Back to Journals » International Journal of Women's Health » Volume 17
Association Between Hysterectomy and Accelerated Aging: Protective Effect of Dietary Fiber and Mediating Role of Creatinine
Authors Qian W, Xu B, Fang Y, Wu X
Received 3 April 2025
Accepted for publication 5 July 2025
Published 11 July 2025 Volume 2025:17 Pages 2015—2024
DOI https://doi.org/10.2147/IJWH.S532242
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Wen Qian,1,* Binkai Xu,2,* Yuan Fang,1 Xian Wu1
1Department of Operation, Changzhou Maternal and Child Health Care Hospital, Changzhou Medical Center of Nanjing Medical University, Changzhou, Jiangsu Province, People’s Republic of China; 2Department of Surgery, Changzhou Maternal and Child Health Care Hospital, Changzhou Medical Center of Nanjing Medical University, Changzhou, Jiangsu Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xian Wu, Email [email protected]
Objective: To investigate the association between hysterectomy and accelerated aging, with a focus on the mediating effect of renal function and protective role of dietary fiber intake.
Methods: The cross-sectional study utilized data from the National Health and Nutrition Examination Survey (NHANES) from 2007 to 2010. The effects of serum creatinine, dietary fiber, vitamin C and vitamin D intake were evaluated.
Results: A total of 4974 participants were included in this study, and 1151 women accepted hysterectomy. The rates of accelerated aging of the women accepted hysterectomy were significantly increased (13.55% vs 10.62%, p = 0.007), and their levels of serum creatinine were also significantly increased (75.56 vs 66.41, p < 0.01). Logistic regression analysis confirmed that the risk of accelerated aging of women undergoing hysterectomy increased significantly (OR 1.32, CI 1.08, 1.60, p = 0.0060). A nonlinear (L-shaped) relationship was observed between creatinine and the odds ratio by RCS curves. Mediation analysis demonstrated that creatinine accounted for 16.7% of observed association between hysterectomy and accelerated aging (p = 0.044). Additionally, the accelerated aging after hysterectomy would be reduced with the intake of dietary fiber, and it accounted for 5.92% of the association between hysterectomy and accelerated aging (p = 0.05).
Conclusion: Women who underwent hysterectomy will face the increased risk of accelerated aging, with a focus on renal function as a mediating factor and dietary fiber intake as a potential protective factor. It will contribute to the long-term health management after hysterectomy.
Keywords: hysterectomy, accelerated aging, renal function, creatinine, dietary fiber
Introduction
Hysterectomy is one of the most common gynecological procedures worldwide.1 Its medical indications are common gynaecological diseases, mainly including endometrial cancer, abnormal uterine bleeding, endometriosis, uterine fibroids and pelvic organ prolapse,2 while in the obstetric field due to postpartum hemorrhage.3 Despite the prevalence of hysterectomy has declined, hysterectomy continues to carry significant long-term health implications.4–6 It is generally believed that the health status is slightly below population norms post-surgery, and rehabilitation interventions to optimize physical function are essential.7 The trend toward ovarian conservation during hysterectomy has introduced complexities in understanding its systemic effects. While ovarian preservation aims to mitigate hormonal disruptions, studies report that even ovary-conserving hysterectomy may disrupt pelvic blood flow, pelvic infection, neuroendocrine signalling, and pelvic floor integrity.8 These alterations could indirectly influence women’s long-term health. Recent studies suggested there were associations between hysterectomy and increased risks of cardiovascular disease,9 metabolic disorders,10 and osteoporosis.11 However, its potential role in accelerating biological aging remains underexplored.
Recently, accelerated aging has become an important health issue, and can have a significant impact on human’s quality of life and longevity, especially for women. Accelerated aging refers to the premature decline in physiological function that manifests as increased frailty, chronic inflammation, and heightened vulnerability to age-related pathologies such as cardiovascular disease, neurodegeneration, and renal dysfunction. Phenotypic age is a biomarker calculated from clinical parameters and is considered a more accurate reflection of an individual aging process compared to chronological age.12 When the phenotypic age exceeds the actual age, it is considered to accelerate aging. To women, aging is uniquely influenced by hormonal transitions, particularly the decline in estrogen during menopause, which exacerbates oxidative stress, mitochondrial dysfunction, and epigenetic alterations.13 It is not clear whether the hysterectomy will accelerate the aging of women. At present, only the Wilson’ group has similar research. They reported that women with hysterectomy-bilateral oophorectomy were at increased risk of substantial limitations of age-associated decline in physical function.14 Undoubtedly, it is a brand-new study field that the association between hysterectomy and accelerated aging of women, as well as the long-term impact on health.
It is generally acknowledged that estrogen deficiency accelerates telomere shortening, impairs DNA repair mechanisms, and promotes cellular senescence. Recently, non-hormonal factors, including chronic inflammation, metabolic dysregulation, and impaired renal function were increasingly recognized as critical contributors to accelerated aging. Notably, renal function plays a pivotal role in accelerated aging.15 The kidneys regulate homeostasis by filtering metabolic waste, maintaining electrolyte balance, and producing hormones such as erythropoietin. Serum creatinine, a byproduct of muscle metabolism and a biomarker of renal filtration efficiency, has emerged as a predictor of aging-related outcomes.16 Elevated creatinine levels, indicative of reduced renal clearance, correlate with increased mortality and cardiovascular risk in aging populations. On the other side, emerging clinical data suggested that hysterectomy was associated with the increased risk of kidney disease.17 Proposed mechanisms include surgical trauma-induced inflammation, oxidative stress, and RAAS activation. Furthermore, hysterectomy may exacerbate age-related declines in glomerular filtration rate (GFR), accelerating the accumulation of uremic toxins and pro-aging factors.18 Despite this, the interplay between gynaecological surgeries, renal function, and aging remains unexplored.
Dietary fiber, a non-digestible carbohydrate found in fruits, vegetables, and whole grains, has garnered attention for its anti-inflammatory, antioxidant, and prebiotic properties. High fiber intake is associated with improved renal outcomes, including slower GFR decline and reduced kidney disease risk,19,20 likely via modulation of gut microbiota, reduction of uremic toxin production, and suppression of systemic inflammation. Despite these benefits, no studies have specifically examined whether dietary fiber attenuates accelerated aging in hysterectomized women. Existing research on post-hysterectomy nutritional interventions focuses predominantly on bone health or metabolic syndrome, neglecting renal and aging-related outcomes.
Given the complexity of the relationship between hysterectomy, kidney function, accelerated aging and dietary fiber, there is a need for comprehensive studies that can elucidate these associations. The National Health and Nutrition Examination Survey (NHANES)21,22 provides a comprehensive platform for the formulation of public health policies, the design and evaluation of health promotion plans and epidemiological study. In present study, we investigated the relationship between hysterectomy and accelerated aging, explore the protective effect of dietary fiber and mediating the role of creatinine. This study offers new insights into potential health risks associated with post-hysterectomy and hope to contribute to improving public health outcomes.
Materials and Methods
Data Source and Study Population
The cross-sectional study was from the NHANES. The participant’s selection is illustrated in Figure 1. Of 20686 initial subjects from NHANES (2007–2010), 10321 were excluded due to gender. Four thousand one hundred and forty-four were excluded due to incomplete data of body mass index (BMI), education level, race, poverty ratio, smoking status. About 1247 were excluded due to missing the information of hysterectomy and the data of accelerating aging, creatinine and so on. Finally, 4974 adults were included in this study. According to whether they had undergone hysterectomy or not, the subjects were divided into two groups: G1 (n = 3823, not having undergone hysterectomy) and G2 (n = 1151, having undergone hysterectomy).
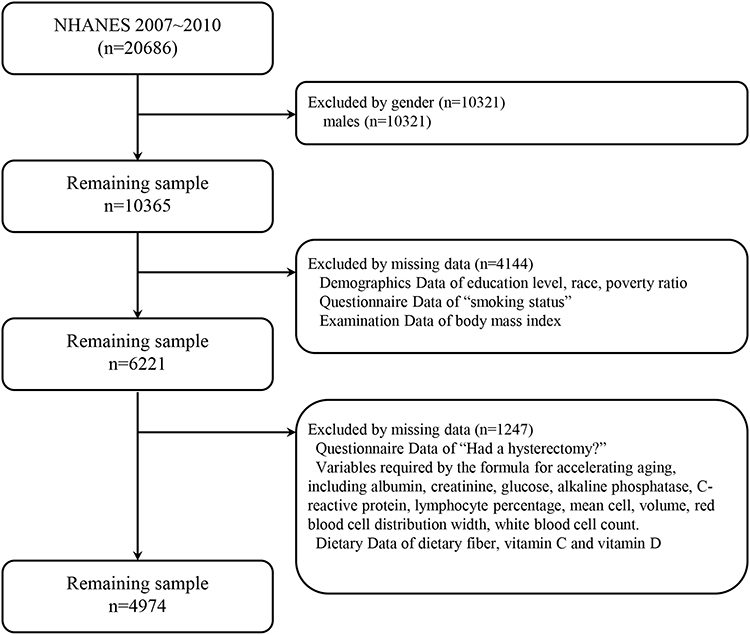 |
Figure 1 Flowchart of participants selection from the NHANES 2007–2010. |
Definition of Hysterectomy
Just as the previous study,17 hysterectomy was measured by the following question: “Had a hysterectomy? (RHD280)”. Women who answer yes were considered as having hysterectomy.
Definition of Accelerated Aging (PhenoAge)
For deriving the phenotypic age, the laboratory data were utilized from NHANES, including albumin, serum creatinine, glucose, C-reactive protein (CRP), percentage of lymphocytes, mean cell volume, red blood cell distribution width, alkaline phosphatase, and white blood cell count. Next, the phenotypic age was calculated in accordance with the method described previously.23,24 Then, aging acceleration was assessed by comparing the phenotypic age with the chronological age of participants. Acceleration in senescence was considered present if the difference between phenotypic age and chronological age was greater than zero.
Measurements of Total Nutrient Intakes
Related dietary parameters were derived from the Dietary Interview – Total Nutrient Intakes, First Day (DR1TOT). The dietary nutrients investigated in our study included the following: Dietary Fiber (g), Vitamin C (mg), and Vitamin D (D2 + D3) (mcg).
Other Covariates
Similar to some other studies,25,26 age, gender, race education level, race and poverty ratio were obtained from demographics data. BMI and weight were collected from examination data. Smoking status was collected during in-home interviews.
Statistical Analysis
DecisionLinnc1.0 software27 was employed for data analysis, which is a platform that integrates multiple programming language environments. Cox hazards regression model was employed to across three distinct models to examine the relationship between hysterectomy and accelerated aging. Model 1 was not adjusted for covariates. Model 2, additionally adjusted for age, race, education level, poverty. Model 3 was additionally adjusted for BMI, smoking status. Subgroup analyses were also conducted. Next, restricted cubic splines (RCS) were utilized to explore potential non-linear relationships between creatinine, dietary fiber and accelerated aging. P < 0.05 was considered statistically significant.
Results
Baseline Participant Characteristics
A total of 4974 participants with complete data from NHANES (2003–2020) were included in this study, and 1151 women accepted hysterectomy. Their average postoperative time was 20.93 years. Table 1 presents the baseline characteristics of the participants according to hysterectomy. Of 4974 participants, 562 (11.30%) women experienced accelerated aging. Compared to G1 group, the rates of accelerated aging of the participants with having undergone hysterectomy (G2) were significantly increased (13.55% vs 10.62%, p = 0.007). At the same time, the levels of serum creatinine were also significantly increased (75.56 vs 66.41, p < 0.01). It suggests that there is a relationship between hysterectomy and the renal function.
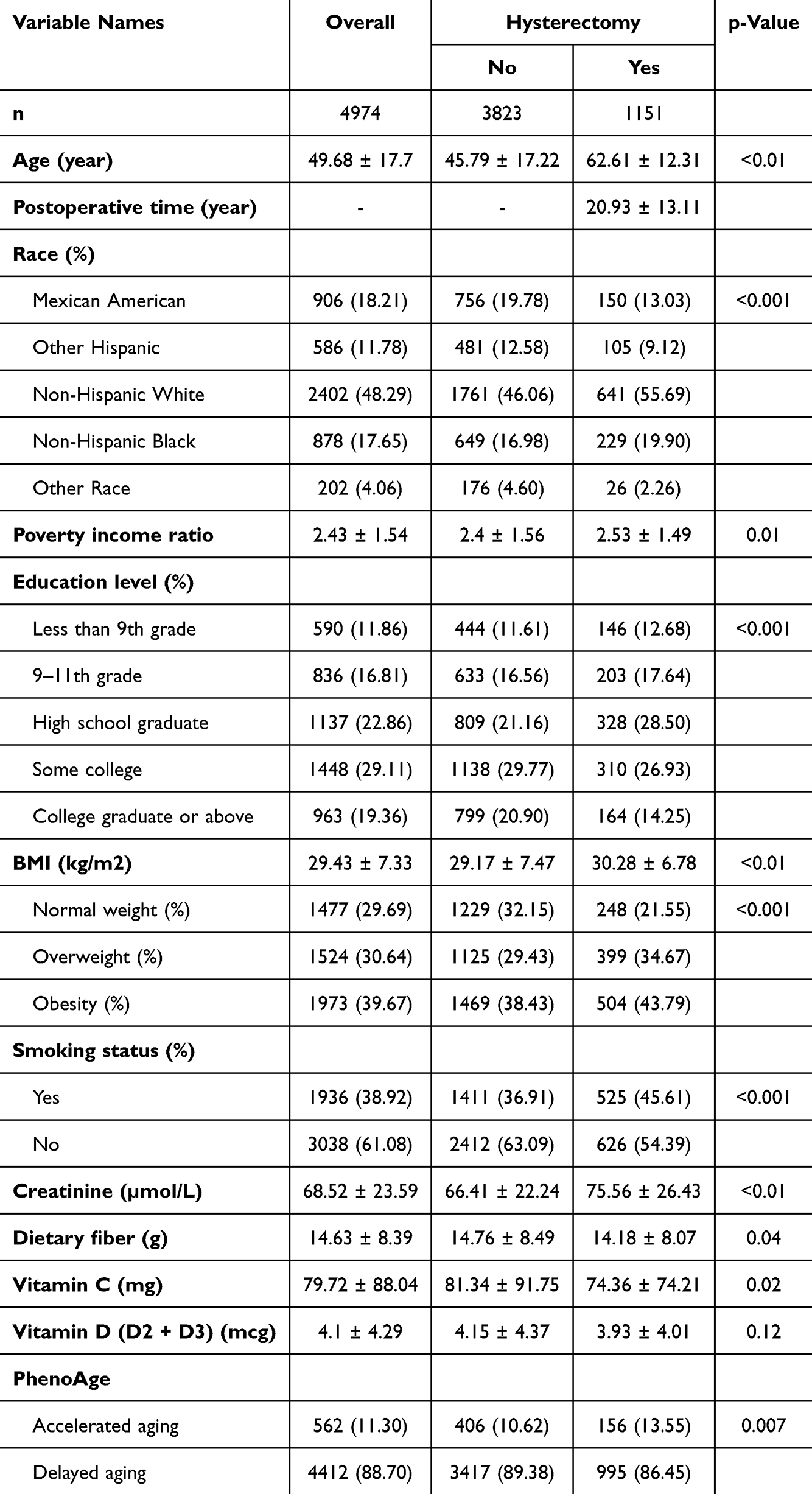 |
Table 1 Baseline Participant Characteristics According to Hysterectomy |
Associations Between Hysterectomy and Accelerated Aging
We have established three models before and after adjusting for confounding factors, respectively. As shown in Table 2, three models established a statistically significant association between hysterectomy and accelerated aging. In the unadjusted model (Model 1), the risk of accelerated aging for the women with having undergone hysterectomy was significantly increased. The odds ratio (OR) and 95% confidence intervals (CIs) were 1.32 (1.08, 1.60) (p = 0.0060). After adjusting for general data confounding factors such as race, education, poverty income ratio (Model 2), hysterectomy was still associated with an increased risk of accelerated aging (OR = 1.26, p = 0.0244). However, there was no significant difference after adjusting for BMI and smoking status (Model 3).
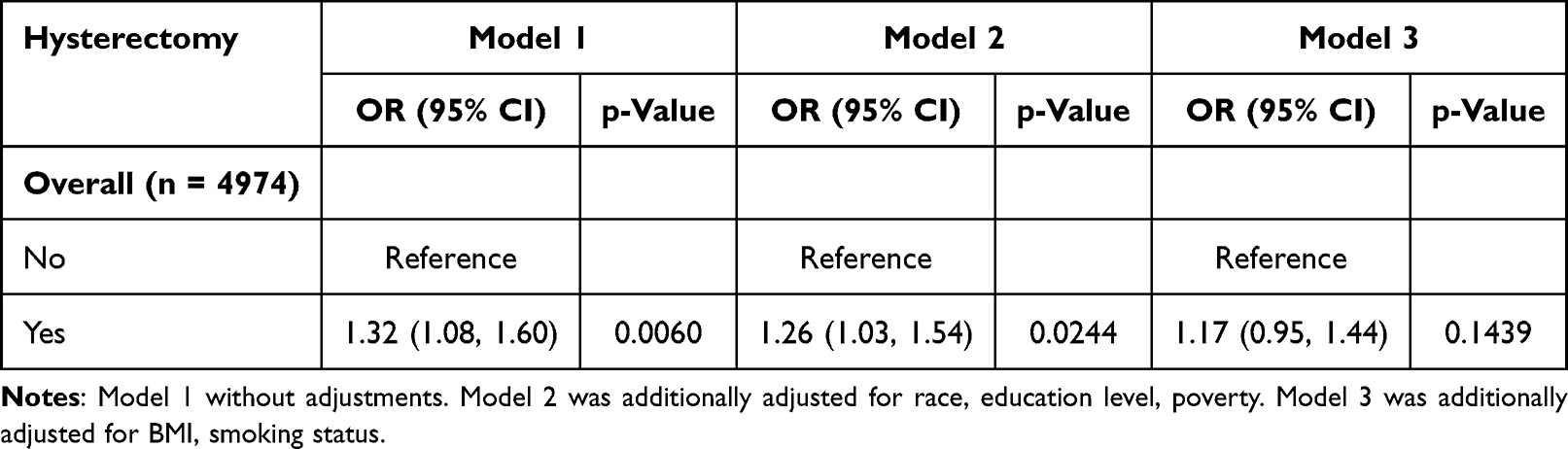 |
Table 2 Multivariable-Adjust ORs and 95% CI of Hysterectomy and Accelerated Aging |
To examine potential differences in the relationship between hysterectomy and accelerated aging in specific populations, we conducted subgroup analyses and interaction tests by age, race, education level, poverty ratio, BMI and smoking status. As showed in Table 3 and Supplement Figure 1, significant interactions were found in education level, poverty ratio and BMI. Women with having undergone hysterectomy had a greater impact on accelerated aging among those with high education level, lower poverty ratio and lower BMI.
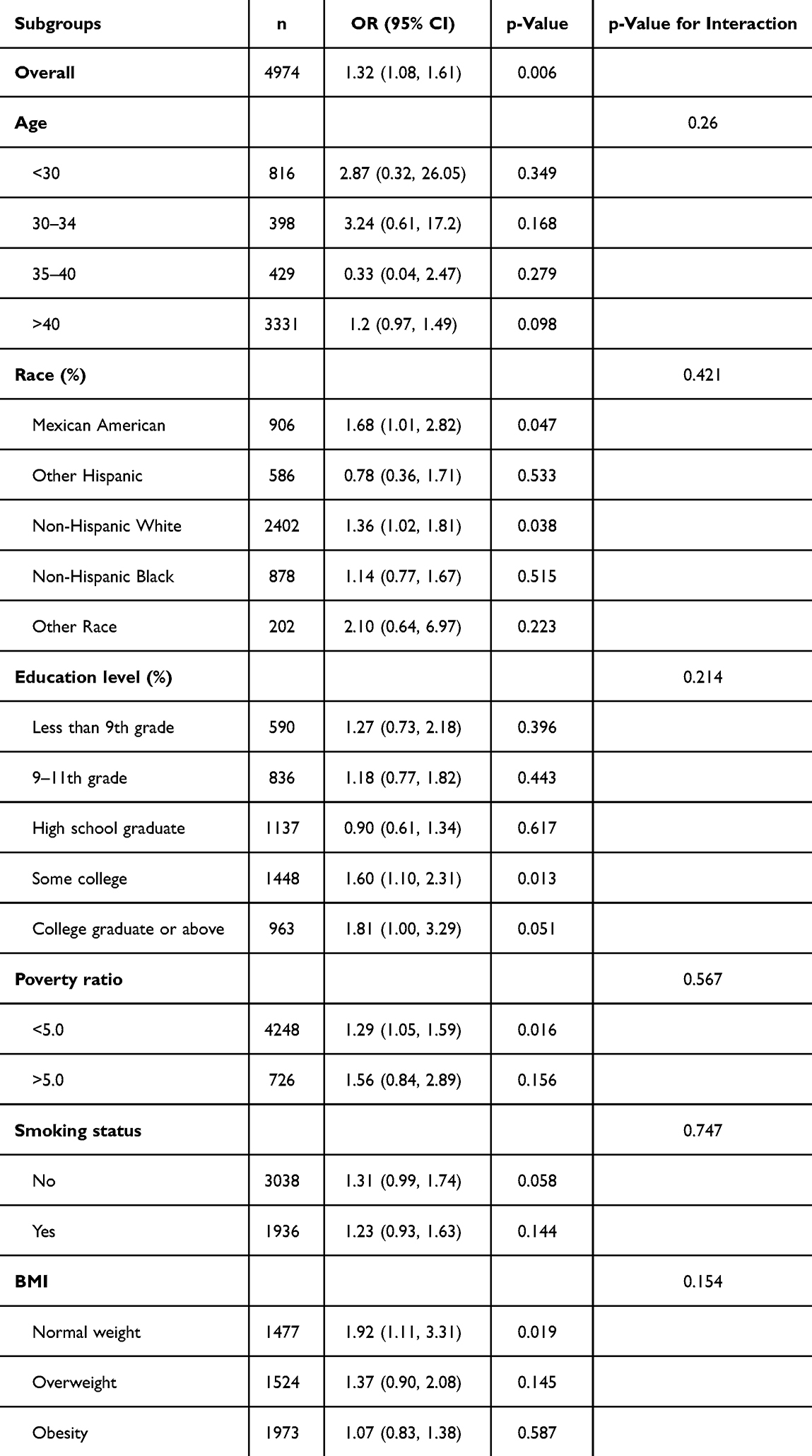 |
Table 3 Subgroup Analysis of Associations Between Hysterectomy and Accelerated Aging |
Mediation Effects of Creatinine
Firstly, RCS curves were adopted to display the association between the level of creatinine and the risk of accelerated aging caused by hysterectomy. After adjusting for multiple variables, evidence for a nonlinear (L-shaped) relationship was observed between creatinine (p for nonlinearity < 0.001) and the odds ratio (Figure 2A). Secondly, smooth curve fitting was employed to clarify the relationship between creatinine and accelerated aging risk. As showed in Figure 2B, both appeared to be the U-shaped association. Furthermore, an inflection point (53.92 µmol/L) was determined by threshold effect analysis. Combined with the normal level of creatinine in the general population, it was particularly noteworthy that when the level of creatinine exceeds 53.92 µmol/L, it will increase the accelerated aging caused by hysterectomy. Thirdly, to clarify whether creatinine play an intermediary role between hysterectomy and accelerated aging, the parallel mediation analysis was carried out. Mediation analysis demonstrated that creatinine accounted for 16.7% of observed association between hysterectomy and accelerated aging (p = 0.044, Figure 2C). The relationship between creatinine and the risk of accelerated aging due to hysterectomy were proved again.
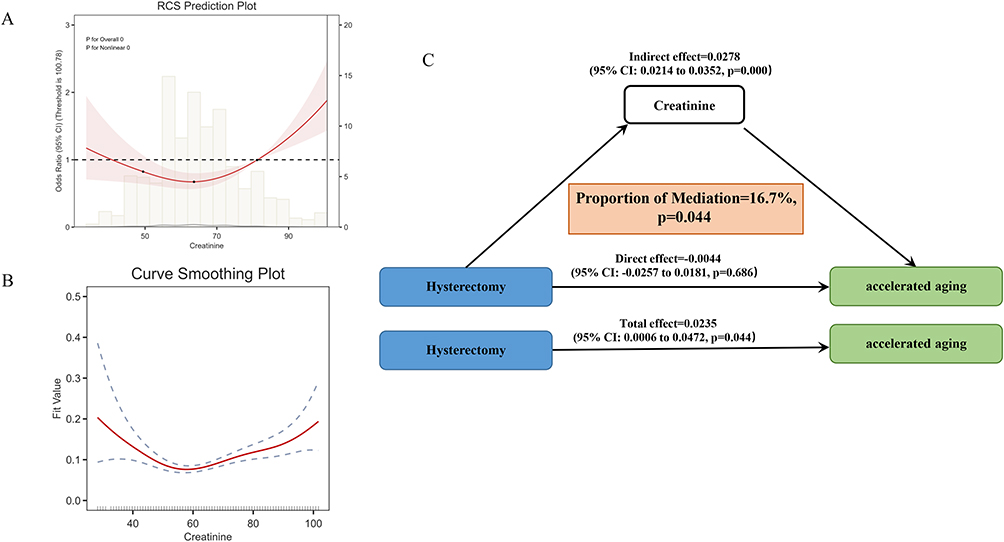 |
Figure 2 Mediation effect for the association between creatinine and the risk of accelerated aging caused by hysterectomy. (A). Restricted cubic splines curves of creatinine. (B). Smooth curve fitting of creatinine. (C) Mediation of creatinine in the association between hysterectomy and accelerated aging. Results were adjusted for gender, race, education level, smoking status and BMI. |
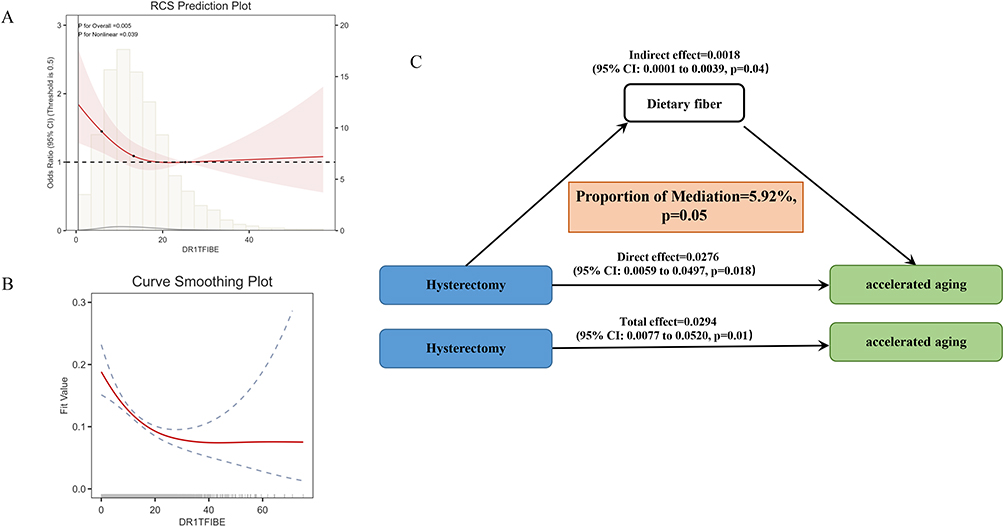 |
Figure 3 Dietary fiber intake reduce the risk of accelerated aging. (A) Restricted cubic splines curves of dietary fiber intake. (B) Smooth curve fitting of dietary fiber intake. (C) Mediation of dietary fiber intake in the association between hysterectomy and accelerated aging. Results were adjusted for gender, race, education level, smoking status and BMI. |
Improvement of Nutrient Intakes
We evaluated the potential of nutrient intakes in retarding the risk of accelerated aging caused by hysterectomy. Based on existing literature, data of dietary fiber, vitamin C, vitamin D (D2 + D3) were extracted and analysed. RCS curves were confirmed that there was a nonlinear (L-shaped) relationship between dietary fiber (p for nonlinearity =0.030) and the risk of accelerated aging caused by hysterectomy odds ratio (Figure 3A). Additionally, smooth curve fitting also clarified that the accelerated aging after hysterectomy would be reduced with the intake of dietary fiber (Figure 3B). Meanwhile, according to the data of diet survey from NHANES, the intake of dietary fiber in women undergoing hysterectomy was obviously insufficient (Table 1). An optimal dietary fibres intake (>4.4 g) was suggested with threshold effect analysis. Furthermore, mediation effect analysis demonstrated that dietary fiber intake played a mediating factor in reducing the risk of accelerated aging due to hysterectomy, with an effect ratio of 5.92% (p = 0.05) (Figure 3C).
Discussion
The present study represents one of the first comprehensive investigations into the relationship between hysterectomy and accelerated aging, with a focus on renal dysfunction as a mediating pathway and dietary fiber intake as a potential protective factor. Leveraging data from the NHANES 2007–2010 cohort, our findings revealed that women who underwent hysterectomy would face a 32% increased risk of accelerated aging compared to those without the procedure. This association was partially mediated by elevated serum creatinine levels, accounting for 16.7% of the observed effect. Furthermore, dietary fiber intake emerged as a modifiable factor, with optimal consumption (>4.4 g/day) attenuating the risk of accelerated aging in hysterectomized women. These results advance our understanding of the long-term health consequences of hysterectomy, highlighting the interplay between gynaecological surgery, renal physiology, and aging trajectories.
Our observation that hysterectomy is associated with accelerated aging aligns with emerging evidence linking gynaecological surgeries to systemic health risks. While prior studies have established connections between hysterectomy and cardiovascular disease, metabolic disorders, and osteoporosis, the relationship with biological aging has remained unexplored. Phenotypic age, a composite biomarker integrating inflammatory, metabolic, and haematological parameters serves as a robust indicator of biological aging.23 The 13.55% prevalence of accelerated aging in hysterectomized women (vs 10.62% in controls) underscores the clinical significance of this association. Notably, this risk persisted even after adjusting for sociodemographic factors but attenuated when accounting for BMI and smoking, suggesting that lifestyle factors may partially confound the relationship. Subgroup analyses further revealed heightened vulnerability among women with higher education, lower poverty ratios, and lower BMI—a paradoxical finding that may reflect differential access to healthcare or variations in post-surgical health behaviors.
The identification of serum creatinine as a mediator bridges a critical gap in understanding how hysterectomy influences aging. Elevated creatinine levels in hysterectomized women (75.56 µmol/L vs 66.41 µmol/L, p < 0.01) align with prior reports linking hysterectomy to chronic kidney disease (CKD) risk. The nonlinear (L-shaped) relationship between creatinine and accelerated aging suggests a threshold effect, where creatinine levels exceeding 53.92 µmol/L significantly amplify aging risk. This threshold aligns with population-based studies defining early renal dysfunction, reinforcing the clinical relevance of our findings.
Mechanistically, hysterectomy may impair renal function through multiple pathways. First, surgical disruption of pelvic vasculature and neural networks could reduce renal blood flow, exacerbating age-related declines in glomerular filtration rate (GFR). Second, estrogen deficiency—even with ovarian conservation—may dysregulate renal vasodilation and sodium balance via estrogen receptor signalling. Third, post-surgical inflammation and oxidative stress could activate the renin-angiotensin-aldosterone system (RAAS), accelerating renal fibrosis and uremic toxin accumulation. These pathways collectively elevate creatinine levels, which in turn drive systemic aging through chronic inflammation, oxidative damage, and metabolic dysregulation.
Recent studies indicated that biological aging is modifiable, mainly including physical activity, dietary intake and lifestyle.28–30 Our study is the first to demonstrate that dietary fiber intake mitigates accelerated aging risk in hysterectomized women. The L-shaped relationship between fiber intake and aging risk, with a protective threshold of >4.4 g/day, aligns with population studies linking fiber to slower GFR decline and reduced CKD progression.19,20,31 Fiber’s benefits likely stem from its prebiotic effects, which enhance short-chain fatty acid (SCFA) production,32 suppress systemic inflammation, and reduce uremic toxins like indoxyl sulfate. Notably, hysterectomized women in our cohort had insufficient fiber intake, highlighting a critical opportunity for dietary intervention. The mediation effect of dietary fiber (5.92%, p = 0.05) suggests that nutritional strategies could partially offset the renal and aging consequences of hysterectomy. This finding is particularly relevant given the lack of existing guidelines addressing post-hysterectomy nutritional care.
However, there are some limitations in present study. The study’s cross-sectional design limits the ability to establish causality. Phenotypic age was calculated based on CRP, WBC, and other laboratory tests. But we indeed failed to take into account the influence of inflammation and infectious diseases. Serum creatinine is widely used marker relating to kidney. However, it still may not capture the full spectrum of renal health. More comprehensive assessments of kidney function could provide a more nuanced understanding of the relationship between hysterectomy and kidney health. Besides, this study only analysed the dietary fiber, vitamin C and vitamin D intake based on the literature, which could not fully reflect the role of diet in accelerating aging.
In conclusion, women who underwent hysterectomy will face the increased risk of accelerated aging, with emphasis on renal function as an intermediary factor. As a potential protective factor, dietary fiber intake will contribute to long-term health management after hysterectomy. However, due to the limitation of cross-sectional design, it is very important to establish causal associations with further prospective study.
Data Sharing Statement
The questionnaire and datasets used are available from the corresponding author on request.
Ethics Approval and Consent to Participate
The National Center for Health Statistics (NCHS) Ethics Review Board (ERB) has approved each NHANES study protocol. Meanwhile, the study was reviewed and approved by the ethics committee of Changzhou Maternal and Child Health Care Hospital.
Acknowledgments
We thank all of the project participants for their contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Bretschneider CE, Jallad K, Paraiso MFR. Minimally invasive hysterectomy for benign indications: an update. Minerva Ginecol. 2017;69(3):295–303. doi:10.23736/S0026-4784.17.04017-5
2. Chang OH, Saldanha IJ, Encalada-Soto D, et al. Associations between hysterectomy and pelvic floor disorders: a systematic review and meta-analysis. Am J Obstet Gynecol. 2025. doi:10.1016/j.ajog.2025.03.018
3. Nguyen PN, Nguyen VT. Evaluating Clinical Features in Intracavitary Uterine Pathologies among Vietnamese Women Presenting with Peri-and Postmenopausal Bleeding: a Bicentric Observational Descriptive Analysis. J Mid-Life Health. 2022;13(3):225–232. doi:10.4103/jmh.jmh_81_22
4. Kim KH, Lee KA. Symptom experience in women after hysterectomy. JOGNN. 2001;30(5):472–480. doi:10.1111/j.1552-6909.2001.tb01566.x
5. Dedden SJ, Werner MA, Steinweg J, et al. Hysterectomy and sexual function: a systematic review and meta-analysis. J Sexual Med. 2023;20(4):447–466. doi:10.1093/jsxmed/qdac051
6. Kim KH, Lee KA. Sleep and fatigue symptoms in women before and 6 weeks after hysterectomy. JOGNN. 2009;38(3):344–352. doi:10.1111/j.1552-6909.2009.01029.x
7. Brennen R, Lin KY, Denehy L, et al. Physical Activity, Quality of Life, and Pelvic Floor Disorders Before and After Hysterectomy for Gynecological Cancer: a Prospective Cohort Study. Int Urogynecol J. 2025. doi:10.1007/s00192-025-06157-3
8. Chen J, Luan T, Zhang Y, et al. Analysis of pathogen distribution, drug sensitivity and inflammatory indicators related to pelvic infection after hysterectomy. Eur J Obstet Gynecol Reprod Biol. 2025;306:210–218. doi:10.1016/j.ejogrb.2025.01.024
9. Chen Y, Li F, Liang L, et al. Examining the association of hysterectomy with and without oophorectomy on cardiovascular disease and all-cause, cardiovascular or cancer mortality: a systematic review and meta-analysis. Bjog. 2024;131(11):1444–1455. doi:10.1111/1471-0528.17843
10. Broni EK, Echouffo-Tcheugui JB, Palatnik A, et al. Associations between hysterectomy and metabolic syndrome: the Multi-Ethnic Study of Atherosclerosis. Am J Obstet Gynecol. 2024;231(4):448.e441–448.e412. doi:10.1016/j.ajog.2024.04.035
11. Seo YS, Yuk JS. Osteoporosis and Fracture Risk Following Benign Hysterectomy Among Female Patients in Korea. JAMA Netw Open. 2023;6(12):e2347323. doi:10.1001/jamanetworkopen.2023.47323
12. Yoo J, Kim Y, Cho ER, Jee SH. Biological age as a useful index to predict seventeen-year survival and mortality in Koreans. BMC Geriatr. 2017;17(1):7. doi:10.1186/s12877-016-0407-y
13. Lozupone M, Solfrizzi V, Sardone R, et al. The epigenetics of frailty. Epigenomics. 2024;16(3):189–202. doi:10.2217/epi-2023-0279
14. Wilson LF, Pandeya N, Byles J, Mishra GD. Hysterectomy and perceived physical function in middle-aged Australian women: a 20-year population-based prospective cohort study. Qual Life Res. 2018;27(6):1501–1511. doi:10.1007/s11136-018-1812-9
15. Goyal K, Afzal M, Altamimi ASA, et al. Chronic kidney disease and aging: dissecting the p53/p21 pathway as a therapeutic target. Biogerontol. 2024;26(1):32. doi:10.1007/s10522-024-10173-z
16. van der Burgh AC, Rizopoulos D, Ikram MA, Hoorn EJ, Chaker L. Determinants of the Evolution of Kidney Function With Age. Kidney Int Rep. 2021;6(12):3054–3063. doi:10.1016/j.ekir.2021.10.006
17. Yuan Y, Tan W, Huang Y, et al. Association between hysterectomy and kidney stone disease: results from the National Health and Nutrition Examination Survey 2007–2018 and Mendelian randomization analysis. World J Urol. 2023;41(8):2133–2139. doi:10.1007/s00345-023-04465-1
18. Komatsu H, Oishi T, Osaku D, et al. Long-term evaluation of renal function and neurogenic bladder following radical hysterectomy in patients with uterine cervical cancer. J Obstet Gynaecol Res. 2020;46(10):2108–2114. doi:10.1111/jog.14394
19. Zhang C, Yan W, Sun X, Lin F. Association between dietary fiber intake and chronic kidney disease in adults with and without hypertension in the United States: a cross-sectional study of NHANES 2009–2020. Renal Failure. 2024;46(2):2415514. doi:10.1080/0886022X.2024.2415514
20. Wathanavasin W, Cheungpasitporn W, Thongprayoon C, Fülöp T. Effects of Dietary Fiber Supplementation on Modulating Uremic Toxins and Inflammation in Chronic Kidney Disease Patients: a Systematic Review and Meta-Analysis of Randomized Controlled Trials. Toxins. 2025;17(2):57. doi:10.3390/toxins17020057
21. Fang J, Alderman MH. Serum uric acid and cardiovascular mortality the NHANES I epidemiologic follow-up study, 1971–1992. JAMA. 2000;283:2404–2410.
22. Alderman MH, Cohen H, Madhavan S. Dietary sodium intake and mortality: the National Health and Nutrition Examination Survey (NHANES I). Lancet. 1998;351(9105):781–785. doi:10.1016/S0140-6736(97)09092-2
23. Levine ME, Lu AT, Quach A, et al. An epigenetic biomarker of aging for lifespan and healthspan. Aging. 2018;10(4):573–591. doi:10.18632/aging.101414
24. Liu Z, Kuo P-L, Horvath S, et al. A new aging measure captures morbidity and mortality risk across diverse subpopulations from NHANES IV: a cohort study. PLoS Med. 2018;15(12):e1002718. doi:10.1371/journal.pmed.1002718
25. Dang K, Wang X, Hu J, et al. The association between triglyceride-glucose index and its combination with obesity indicators and cardiovascular disease: NHANES 2003–2018. Cardiovascular Diabetol. 2024;23(1):8. doi:10.1186/s12933-023-02115-9
26. Guo HJ, Ye YL, Gao YF, Liu ZH. Age at first birth is associated with the likelihood of frailty in middle-aged and older women: a population-based analysis from NHANES 1999–2018. Maturitas. 2024;181:107904. doi:10.1016/j.maturitas.2023.107904
27. Chen HL, Wu C, Cao L, et al. The association between the neutrophil-to-lymphocyte ratio and type 2 diabetes mellitus: a cross-sectional study. BMC Endocr Disord. 2024;24(1):107. doi:10.1186/s12902-024-01637-x
28. Thomas A, Belsky DW, Gu Y. Healthy Lifestyle Behaviors and Biological Aging in the U.S. National Health and Nutrition Examination Surveys 1999–2018. J Gerontol a Biol Sci Med Sci. 2023;78(9):1535–1542. doi:10.1093/gerona/glad082
29. Jin S, Li C, Cao X, et al. Association of lifestyle with mortality and the mediating role of aging among older adults in China. Arch Gerontol Geriatrics. 2022;98:104559. doi:10.1016/j.archger.2021.104559
30. Li J, Wu Z, Xin S, et al. Body mass index mediates the association between four dietary indices and phenotypic age acceleration in adults: a cross-sectional study. Food Funct. 2024;15(15):7828–7836. doi:10.1039/D4FO01088D
31. Xu H, Huang X, Risérus U, et al. Dietary fiber, kidney function, inflammation, and mortality risk. CJASN. 2014;9(12):2104–2110. doi:10.2215/CJN.02260314
32. Yan F, Wang X, Du Y, et al. Pumpkin Soluble Dietary Fiber instead of Insoluble One Ameliorates Hyperglycemia via the Gut Microbiota–Gut–Liver Axis in db/db Mice. J Agric Food Chem. 2025;73(2):1293–1307. doi:10.1021/acs.jafc.4c08986
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.