Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Association Between High-Sensitivity C-Reactive Protein and Prognosis of Patients with Acute Cerebral Infarction
Authors Pu Y ![]() , Li S, Wang L, Fang B, Bai X
, Li S, Wang L, Fang B, Bai X ![]()
Received 7 June 2022
Accepted for publication 17 August 2022
Published 20 August 2022 Volume 2022:18 Pages 1771—1778
DOI https://doi.org/10.2147/NDT.S376440
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Yuting Pu,1,2 Shuangyang Li,2 Lingxue Wang,2 Bangjiang Fang,1 Xue Bai2
1LongHua Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, 200032, People’s Republic of China; 2Department of Neurology and National Traditional Chinese Medicine Clinical Research Base, The Affiliated Traditional Chinese Medicine Hospital of Southwest Medical University, Luzhou, 646000, People’s Republic of China
Correspondence: Xue Bai, Department of Neurology and National Traditional Chinese Medicine Clinical Research Base, The Affiliated Traditional Chinese Medicine Hospital of Southwest Medical University, Luzhou, Sichuan, 646000, People’s Republic of China, Email [email protected]
Purpose: To investigate the association of serum high-sensitivity C-reactive protein (hs-CRP) with the severity of neurological deficits and prognosis in patients with acute cerebral infarction (ACI).
Patients and Methods: In this retrospective analysis, 119 patients with ACI were recruited from January to December 2020. The serum hs-CRP level was measured by a latex-enhanced immunoturbidimetric assay. The severity of neurological deficits and prognosis of ACI patients were assessed using the National Institutes of Health Stroke Scale (NIHSS) and the modified Rankin Scale (mRS). Multivariate logistic analysis was performed and receiver operating characteristic (ROC) curves were plotted to evaluate the value of hs-CRP in predicting the prognosis of ACI.
Results: The patients with a more favorable prognosis (mRS score 0– 2) had a lower median serum hs-CRP level than those with a worse prognosis (mRS score 3– 6) (3.32 IQR: 1.51, 8.04 to 17.93 IQR:16.02, 19.01; P< 0.001). After adjusting for potential confounders, multivariable linear regression showed that serum hs-CRP level was independently associated with NIHSS score (Beta = 0.952, P< 0.001) and mRS score (Beta=0.878, P< 0.001). Multivariate logistic analysis revealed that high hs-CRP level was an independent predictor of the poor prognosis in patients with ACI (adjusted1 OR = 1.995; 95% CI = 1.499– 2.655; adjusted2 OR = 2.75; 95% CI = 1.015– 7.457). ROC curve analysis indicated that the area under the curve for hs-CRP to predict poor prognosis was 0.986. The cutoff value, sensitivity, and specificity were 11.835 mg/L, 95%, and 92.5%, respectively. In terms of ischemic stroke subtypes, the serum hs-CRP level was higher in large-artery atherosclerosis (LAA) patients than in those with small-artery occlusion (SAO) and cardioembolism (CE). In addition, the patients with LAA had higher scores of NIHSS and mRS than those with SAO and CE.
Conclusion: Serum hs-CRP level is an independent predictor of prognosis, and an efficient index to discriminate patients with ACI, especially for those with LAA.
Keywords: acute cerebral infarction, high-sensitivity C-reactive protein, neurological deficits
Introduction
Stroke is the second leading cause of death and the third leading cause of disability in patients with cerebrovascular diseases worldwide.1 Acute cerebral infarction (ACI) accounts for 69.6–70.8% of all stroke cases. The high morbidity, disability, and mortality due to ACI pose a heavy burden on public health.2 Early prediction of ACI risk and prognosis is essential to the successful management of ACI.
ACI manifests brain tissue necrosis caused by ischemia and hypoxia.3 Cerebral atherosclerosis is the most common cause of ACI.4,5 Inflammation affects cerebral atherosclerosis and plays a critical role in the pathogenesis of ACI.6–8 High-sensitivity c-reactive protein (hs-CRP) is a marker of acute nonspecific inflammation in the course of ACI.9 Previous studies have revealed that a high hs-CRP level predicts a poor prognosis for ACI patients.10 However, the association between hs-CRP and the degree of neurological deficits and prognosis is unclear in different stroke subtypes. This study aimed to investigate the hs-CRP level in different ischemic stroke subtypes and their associations with the scores measured with the National Institutes of Health Stroke Scale (NIHSS) and the 3-month modified Rankin Scale (mRS).
Materials and Methods
Participants
A total of 119 patients diagnosed with ACI and hospitalized from January 2020 to December 2020 in the Department of Neurology of the Affiliated Traditional Chinese Medicine Hospital of Southwest Medical University were enrolled. Included were those aged >18 years, with symptoms setting on within 72 hours and confirmed by imaging data (CT or MRI). The Trial of Org 10,172 in Acute Stroke Treatment (TOAST) is a system for classification of subtypes of ischemic stroke based on etiology, including large-artery atherosclerosis (LAA), cardioembolism (CE), small-artery occlusion (SAO), stroke of other determined etiology (SOE), and stroke of undetermined etiology (SUE).11 The patients were classified into different subtypes by at least two experienced senior neurologists. Excluded were those with (1) a history of surgery or trauma in the previous three months, (2) autoimmune diseases, malignancies, or infectious diseases, and (3) severe liver failure or acute or chronic renal insufficiency.
Measurement of Hs-CRP
At admission before treatment, 5 mL of fasting venous blood was obtained from the patient, left to stand for 30 minutes, and centrifuged at 3000 rpm for 15 minutes; then, the serum was collected. Serum hs-CRP level was measured by latex-enhanced immunoturbidimetric assay. The suspension was prepared according to the instruction of the High Sensitivity C-reaction Protein (HS-CRP) Kit (Myriad), and then tested using a fully automated biochemical analyzer (model: BS-400). All operations were performed by a physician from a clinical laboratory of the Affiliated Traditional Chinese Medicine Hospital of Southwest Medical University.
Assessment of Neurological Deficits and Outcomes
The severity of neurological deficits was estimated at admission using the NIHSS score. The deficit was classified as follows:2 mild (<5, the patient’s daily activities are not limited); moderate (5–15, the patient’s movements are partially limited, with limb, speech or sensory disorders); severe (>15, the patient is completely incapable to care for themselves).
Clinical outcomes were scored using the modified Rankin scale (mRS) at 90 days after stroke onset. Criteria were as follows: 0, completely asymptomatic; 1, no significant disability (the patient can perform all daily activities despite the presence of symptoms); 2, slight disability (the patient is unable to perform daily activities, but able to manage personal affairs without assistance); 3, moderate disability (the patient needs some assistance, but can walk independently); 4, moderately severe disability (the patient is unable to walk and perform daily activities independently without help); 5, severe disability (the patient is bedridden and in need of constant care). An mRS score of ≤2 predicted a favorable prognosis, and an mRS score of >2 predicted a poor prognosis.12
Statistical Analysis
All data were analyzed by IBM SPSS 25.0 software, and images were evaluated by GraphPad Prism 8 (GraphPad Software, San Diego, USA). The normality of data was confirmed by using the Kolmogorov–Smirnov test. Non-normality variables were expressed as median with interquartile range (IQR) and processed by nonparametric Mann–Whitney U-tests or Kruskal-Walis H. Categorical data were compared using chi-squared tests.
The association between serum hs-CRP level and NIHSS score or mRS score was assessed through multivariate linear regression analysis with adjustment for potential confounders. The association between hs-CRP level and ACI prognosis was evaluated by the multivariable binary logistic regression analysis; odds ratios (OR) with 95% CI were calculated. Potential confounding factors were adjusted in the multivariable model, including age, sex, smoking, alcohol consumption, hypertension, NIHSS score, and stroke subtype. P values <0.05 were considered statistically significant. The receptor operating characteristic (ROC) curves were generated and the area under the curve (AUC) was calculated to evaluate the ability of hs-CRP in predicting ACI prognosis.
Results
Baseline Clinical Characteristics
A total of 119 patients were enrolled in this study, including 75 (63.0%) men and 44 (37.0%) women, with an average age of 68 (IQR 58, 72) years. Among the patients, 57 (47.9%) had a smoking history, 52 (43.7%) of alcohol consumption, 82 (68.9%) of hypertension, 62 (52.1%) of diabetes mellitus, 32 (26.9%) of atrial fibrillation, and 48 (40.3%) of coronary artery disease. According to the etiological classification of TOAST, 59 cases (49.6%) were classified as LAA, 37 cases (31.1%) as SAO, and 23 cases (19.3%) as CE. The median values of hs-CRP and NIHSS scores were significantly lower in patients with a favorable prognosis than those with an unfavorable prognosis (P<0.001). The incidence of hypertension was also lower in the group with a favorable prognosis. The baseline clinical characteristics are presented in Table 1.
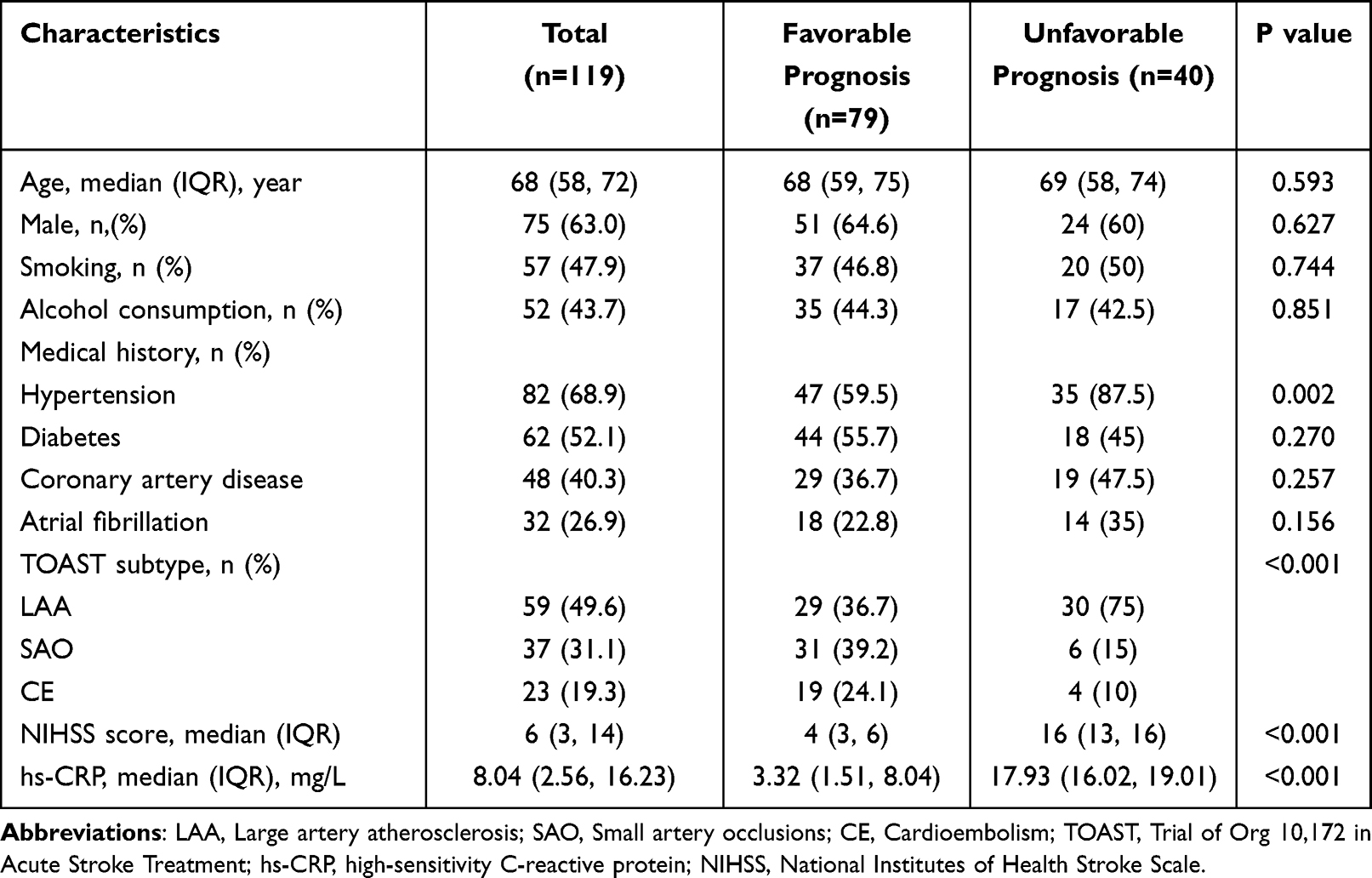 |
Table 1 Baseline Clinical Characteristics |
Association of Hs-CRP Level with NIHSS Score at Admission and mRS Score at 90 Days After Stroke Onset
Age, sex, smoking, alcohol consumption, comorbid diseases (hypertension, diabetes, Coronary artery disease, Atrial fibrillation), and stroke subtype were incorporated into a multivariate linear regression analysis. The results suggested that hs-CRP level was positively affected NIHSS score (P < 0.001) and mRS score (P < 0.001) (Table 2).
 |
Table 2 Association Between Hs-CRP and NIHSS Score at Admission and mRS Score at 90 Days After Stroke Onset |
Association Between Hs-CRP Level and ACI Prognosis
Significant factors (P<0.05) in the univariate analysis and identified risk factors were subjected to the multivariable binary logistic regression analysis. The results indicated that hs-CRP level independently affected the prognosis of patients with ACI after adjusting for age, sex, NIHSS score, stroke subtype, smoking, drinking, and hypertension at baseline (Table 3).
 |
Table 3 Favorable Outcome at 90 Days |
ROC curves showed that the area under the curve (AUC) of hs-CRP in predicting the prognosis of ACI at 90 days was 0.986, with a cutoff value of 11.835 mg/L (sensitivity, 95%; specificity, 92.5%), indicating that high serum hs-CRP level had a strong ability to predict the poor prognosis of ACI (Figure 1).
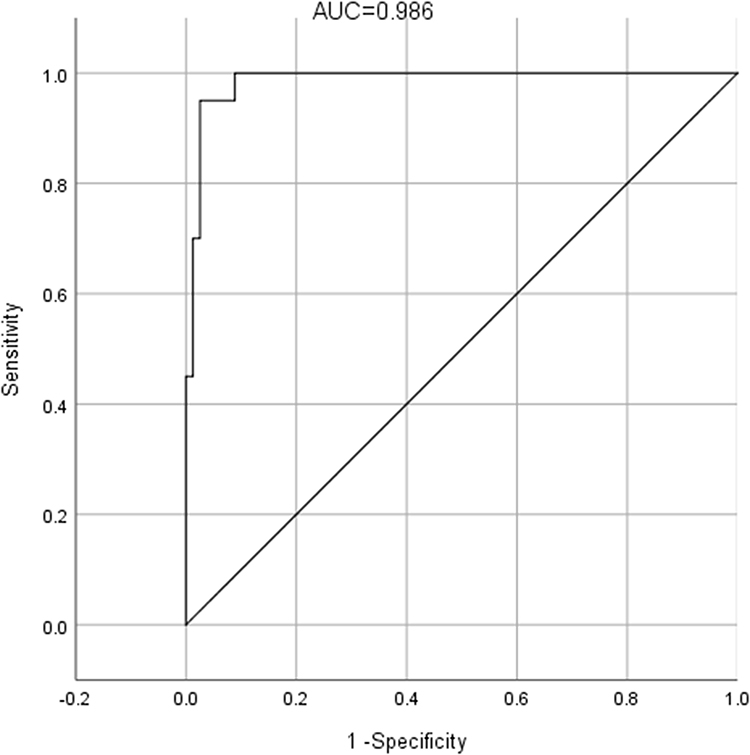 |
Figure 1 ROC curves of hs-CRP for a poor outcome at 90 days after stroke onset. |
Increased Serum Hs-CRP Level in Patients with the LAA Subtype
The hs-CRP level in patients with LAA subtype was statistically higher than those in patients with SAO and CE (Figure 2A). Moreover, the NIHSS and mRS scores of LAA patients were significantly higher than those of patients with subtypes of SAO and CE (Figures 2B and C).
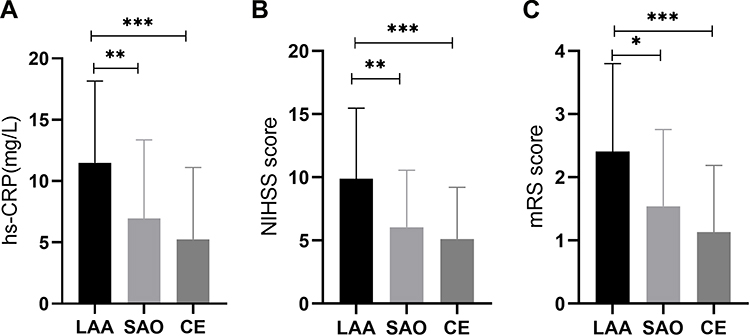 |
Figure 2 Levels of hs-CRP, NIHSS scores as well as mRS scores in patients with different TOAST subtypes (A) hs-CRP levels in patients with ischemic stroke subtypes. **P<0.01 and ***P<0.001 from Kruskal-Walis H by Dunn’s multiple comparisons tests. (B) NIHSS scores in patients with ischemic stroke subtypes. **P<0.01 and ***P<0.001 from Kruskal-Walis H by Dunn’s multiple comparisons tests. (C) mRS scores in ischemic stroke subtypes. *P<0.05 and ***P<0.001 from Kruskal-Walis H by Dunn’s multiple comparisons tests. |
Discussion
Postischemic inflammation plays a vital role in the progression of cerebral ischemic injury.13,14 Inflammatory cascade can be activated immediately after ischemic stroke.8,15 Interactions between inflammatory cell may lead to long-term vascular inflammation and ischemic brain injury.16,17 Our findings lays a foundation for designing an early intervention strategy based on Hs-CRP.
Hs-CRP is a common nonspecific inflammatory factor primarily secreted by the liver. Serum hs-CRP level elevates in response to trauma, inflammation, or stress.18 Previous studies have shown that hs-CRP is sensitive to ischemic stroke, and can be used to predict the risk of cerebrovascular events and mortality in the general population.19,20 However, it remains controversial whether hs-CRP level can serve as an independent predictor of prognosis in patients with ischemic stroke.21 Therefore, it becomes important to verify the efficiency of serum hs-CRP in predicting the clinical prognosis of ACI.
In this study, multivariable binary logistic regression analysis suggested that serum hs-CRP was an independent prognostic factor of ACI. The ROC curve also showed that the AUC of hs-CRP was 0.986 to predict the poor ACI prognosis at 90 days after onset. The above results suggest that serum hs-CRP level at admission can predict the short-term prognosis of patients with ACI. Therefore, detecting hs-CRP may help predict the overall clinical outcome of ACI.
The potential mechanisms of high hs-CRP in worsening the prognosis of ACI are as follows: (1) High hs-CRP level reflects the instability of atherosclerotic plaques. Hs-CRP can bind to lipoproteins, activate the classical complement pathway, directly potentiate resting vascular endothelial cells, mediate the rolling, adsorption, and exudation of leukocytes in endothelial cells, and form unstable plaques, a process that finally induces ischemic stroke.22 (2) Hs-CRP can bind to hs-CRP receptors on monocytes and granulocytes, and damages brain cells through direct infiltration and aggregation or indirect action (cytokine production). Elevated hs-CRP level can reflect chronic and persistent damage to vascular endothelial cells. (3) Hs-CRP can lead to abnormal coagulation. Hs-CRP can induce abnormal platelet aggregation and release to disrupt coagulation and hemostasis, thus increasing the risk of cerebrovascular accidents.23
Currently, TOAST is most commonly used to classify stroke, and the risk factors for each stroke subtype are listed in this system.24 This classification aids much in the clinical management of stroke.25 In this study, we observed that the patients with LAA had a significantly higher hs-CRP level than those with SAO and CE. In addition, the patients with LAA had also higher NIHSS and mRS scores than those SAO and CE. The above results indicate that patients with LAA are more prone to severe neurological deficit and poor prognosis. Therefore, hs-CRP level may be a valuable biomarker for identifying LAA subtype and predict the destiny of ACI.
This study also has certain limitations. First, this is a single-center, small-sample retrospective study, and the results may need to be reconfirmed in a multicenter, large-sample, long follow-up study. Second, we measured serum hs-CRP after admission and before treatment, but not during hospitalization, at discharge, and during follow-up, and we did not monitor the changes in hs-CRP, and evaluate their relationship with the prognosis of ACI. Lastly, although multivariate logistic regression analysis was conducted to adjust for potential confounders, unmeasured and residual confounders might remain.
Conclusion
Serum hs-CRP level was positively associated with the severity of neurological deficits in patients with ACI. It can be used to predict the prognosis of ACI and identify the etiological subtypes, especially the LAA subtype.
Abbreviations
hs-CRP, high-sensitivity C-reactive protein; ACI, acute cerebral infarction; NIHSS, National Institutes of Health Stroke Scale; mRS, modified Rankin Scale; LAA, large artery atherosclerosis; SAO, small artery occlusions; CE, cardioembolism; SOE, stroke of other determined etiology; SUE, stroke of undetermined etiology; AUC, area under the curve.
Data Sharing Statement
The original data supporting the findings of this article are available from the corresponding authors on reasonable request.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of the Affiliated Traditional Chinese Medicine Hospital of Southwest Medical University (Review No: KY2019089). Written informed consent was obtained from every patient or their relatives.
Author Contributions
All authors contributed significantly to conception and study design, drafting or revising the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Innovation Team and Talents Cultivation Program of the National Administration of Traditional Chinese Medicine (ZYYCXTD-C-202207), Innovation Team of Sichuan Provincial Administration of Traditional Chinese Medicine (2022C007), and Innovation Team of the Affiliated Traditional Chinese Medicine Hospital of Southwest Medical University (2022-CXTD-05).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Feigin VL, Stark BA, Johnson CO, et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795–820. doi:10.1016/s1474-4422(21)00252-0
2. Lin Y, Wang K, Ji D, Gong Z, Wang Z. Correlation between plasma high mobility group protein N1 level and the prognosis of patients with acute cerebral infarction: preliminary findings. Neuropsychiatr Dis Treat. 2022;18:907–913. doi:10.2147/ndt.S359879
3. Gao HH, Gao LB, Wen JM. Correlations of MCP-1 −2518A>G polymorphism and serum levels with cerebral infarction risk: a meta-analysis. DNA Cell Biol. 2014;33(8):522–530. doi:10.1089/dna.2013.2263
4. Fu X, Liu Q, Zeng X, Huang S, Huang R, Gao Q. Association between cerebral arterial stiffness and large artery atherosclerosis in acute ischemic stroke. J Stroke Cerebrovasc Dis. 2018;27(11):2993–3000. doi:10.1016/j.jstrokecerebrovasdis.2018.06.033
5. Li S, Song X, Hu Q, et al. Association of plaque features with infarct patterns in patients with acutely symptomatic middle cerebral artery atherosclerotic disease. J Stroke Cerebrovasc Dis. 2021;30(5):105724. doi:10.1016/j.jstrokecerebrovasdis.2021.105724
6. Ridker PM, Silvertown JD. Inflammation, C-reactive protein, and atherothrombosis. J Periodontol. 2008;79(8 Suppl):1544–1551. doi:10.1902/jop.2008.080249
7. Ponsaerts L, Alders L, Schepers M, et al. Neuroinflammation in ischemic stroke: inhibition of cAMP-specific Phosphodiesterases (PDEs) to the rescue. Biomedicines. 2021;9(7). doi:10.3390/biomedicines9070703
8. Iadecola C, Anrather J. The immunology of stroke: from mechanisms to translation. Nat Med. 2011;17(7):796–808. doi:10.1038/nm.2399
9. Zhang X, Huang WJ, Yu ZG. Relationship between the hypersensitive c-reactive protein (hs-CRP) level and the prognosis of acute brainstem infarction. Cell Biochem Biophys. 2015;72(1):107–110. doi:10.1007/s12013-014-0414-6
10. Cai Z, He W, Zhuang FJ, Chen Y. The role of high high-sensitivity C-reactive protein levels at admission on poor prognosis after acute ischemic stroke. Int J Neurosci. 2019;129(5):423–429. doi:10.1080/00207454.2018.1538139
11. Adams HP
12. Zhang XG, Xue J, Yang WH, et al. Inflammatory markers as independent predictors for stroke outcomes. Brain Behav. 2021;11(1):e01922. doi:10.1002/brb3.1922
13. Iadecola C, Buckwalter MS, Anrather J. Immune responses to stroke: mechanisms, modulation, and therapeutic potential. J Clin Invest. 2020;130(6):2777–2788. doi:10.1172/jci135530
14. Anrather J, Iadecola C. Inflammation and Stroke: an Overview. Neurotherapeutics. 2016;13(4):661–670. doi:10.1007/s13311-016-0483-x
15. De Meyer SF, Denorme F, Langhauser F, Geuss E, Fluri F, Kleinschnitz C. Thromboinflammation in stroke brain damage. Stroke. 2016;47(4):1165–1172. doi:10.1161/strokeaha.115.011238
16. Maida CD, Norrito RL, Daidone M, Tuttolomondo A, Pinto A. Neuroinflammatory mechanisms in ischemic stroke: focus on cardioembolic stroke, background, and therapeutic approaches. Int J Mol Sci. 2020;21(18). doi:10.3390/ijms21186454
17. Jayaraj RL, Azimullah S, Beiram R, Jalal FY, Rosenberg GA. Neuroinflammation: friend and foe for ischemic stroke. J Neuroinflammation. 2019;16(1):142. doi:10.1186/s12974-019-1516-2
18. Park SW, Park SS, Kim EJ, Sung WS, Ha IH, Jung B. Sex differences in the association between self-rated health and high-sensitivity C-reactive protein levels in Koreans: a cross-sectional study using data from the Korea National Health and Nutrition Examination Survey. Health Qual Life Outcomes. 2020;18(1):341. doi:10.1186/s12955-020-01597-5
19. Makita S, Nakamura M, Satoh K, et al. Serum C-reactive protein levels can be used to predict future ischemic stroke and mortality in Japanese men from the general population. Atherosclerosis. 2009;204(1):234–238. doi:10.1016/j.atherosclerosis.2008.07.040
20. Zhou Y, Han W, Gong D, Man C, Fan Y. Hs-CRP in stroke: a meta-analysis. Clin Chim Acta. 2016;453:21–27. doi:10.1016/j.cca.2015.11.027
21. Bustamante A, Simats A, Vilar-Bergua A, García-Berrocoso T, Montaner J. Blood/brain biomarkers of inflammation after stroke and their association with outcome: from C-reactive protein to damage-associated molecular patterns. Neurotherapeutics. 2016;13(4):671–684. doi:10.1007/s13311-016-0470-2
22. Zhang XL, Dong YT, Liu Y, Zhang Y, Li TT, Hu FY. Effects of dl-3-n-butylphthalide on serum lipoprotein-associated phospholipase A2 and hypersensitive C-reactive protein levels in acute cerebral infarction. Brain Behav. 2019;9(12):e01469. doi:10.1002/brb3.1469
23. Tohgi H, Konno S, Takahashi S, Koizumi D, Kondo R, Takahashi H. Activated coagulation/fibrinolysis system and platelet function in acute thrombotic stroke patients with increased C-reactive protein levels. Thromb Res. 2000;100(5):373–379. doi:10.1016/s0049-3848(00)00356-x
24. Lv P, Jin H, Liu Y, et al. Comparison of risk factor between lacunar stroke and large artery atherosclerosis stroke: a cross-sectional study in China. PLoS One. 2016;11(3):e0149605. doi:10.1371/journal.pone.0149605
25. Knight-Greenfield A, Nario JJQ, Gupta A. Causes of acute stroke: a patterned approach. Radiol Clin North Am. 2019;57(6):1093–1108. doi:10.1016/j.rcl.2019.07.007
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.