Back to Journals » Journal of Inflammation Research » Volume 18
Association Between High-Sensitivity C-Reactive Protein and Longitudinal Changes in Arteriosclerosis Over Time: The Kailuan Prospective Cohort Study
Authors Li W ![]() , Liang P, Han Z, Liu X, An S, Wang X, Gao Y
, Liang P, Han Z, Liu X, An S, Wang X, Gao Y ![]() , Chen S, Wu S
, Chen S, Wu S ![]()
Received 14 June 2025
Accepted for publication 13 September 2025
Published 24 September 2025 Volume 2025:18 Pages 13255—13264
DOI https://doi.org/10.2147/JIR.S541222
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qing Lin
Weizhe Li,1,* Pei Liang,2,* Zhao Han,3 Xiaohui Liu,4 Shasha An,5 Xin Wang,1 Yanling Gao,1 Shuohua Chen,6 Shouling Wu6
1Department of Emergency Internal Medicine No. I, Handan Central Hospital, Handan, Hebei, 056001, People’s Republic of China; 2Rehabilitation Department Three, Handan Mingren Hospital, Handan, Hebei, 056001, People’s Republic of China; 3Department of Dermatology, The Affiliated Hospital of Hebei Engineering University, Handan, Hebei, 056002, People’s Republic of China; 4Department of General Surgery II, Handan Central Hospital, Handan, Hebei, 056001, People’s Republic of China; 5Department of General Medicine, Handan Central Hospital, Handan, Hebei, 056001, People’s Republic of China; 6Department of Cardiology, Kailuan General Hospital, Tangshan, Hebei, 063001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaohui Liu, Department of General Surgery II, Handan Central Hospital, NO. 15, Zhonghuanan Street, Hanshan District, Handan, Hebei, 056001, People’s Republic of China, Tel: +86 18630004402, Email [email protected]
Objective: To investigate the relationship between high-sensitivity C-reactive protein (hs-CRP) and the longitudinal changes in arterial Arteriosclerosis over time.
Methods: Using a prospective cohort study design, 25,336 participants from the Kailuan study cohort, who had completed at least two baPWV measurements and met the inclusion criteria, included in the analysis. Participants were divided into three groups based on baseline hs-CRP levels: hs-CRP< 1 mg/L, 1 mg/L≤hs-CRP≤ 3 mg/L, and hs-CRP > 3 mg/L. The relationship between hs-CRP and the longitudinal changes in baPWV was analyzed using a linear mixed-effects model.
Results: (1) The average follow-up duration was 4.62 ± 2.86 years. At the end of the follow-up, the baPWV of the three groups:hs-CRP < 1 mg/L (n=11,651), 1 mg/L ≤ hs-CRP ≤ 3 mg/L (n=9,369), and hs-CRP > 3 mg/L (n=4,316) increased over time. The average rate of increase in baPWV was 84.26 cm/s, 88.06 cm/s, and 73.92 cm/s, respectively. (2) The linear mixed-effects model analysis of factors affecting the progression of Arteriosclerosis, after adjusting for confounding factors, showed that compared to the hsCRP_1 group, the baPWV increase rate in the hsCRP_2 and hsCRP_3 groups was progressively higher. The effect Estimate were 14.4 cm/s (95% CI 6.54 to 22.34, P< 0.001) and 40.67 cm/s (95% CI 5.28 to 51.02, P< 0.001), respectively. Stratifying by gender showed that the impact was more pronounced in males, with effect Estimate of 20.56 cm/s (95% CI 6.18 to 8.45, P< 0.001) and 43.06 cm/s (95% CI 27.82 to 58.31, P< 0.001), respectively. Sensitivity analysis confirmed that this longitudinal association was more pronounced.
Conclusion: There is a significant “dose-response” relationship between hs-CRP and the longitudinal progression of Arteriosclerosis, with a more pronounced effect observed in the male population.
Keywords: high-sensitivity C-reactive protein, ankle-brachial pulse wave velocity, arteriosclerosis, linear mixed-effects model
Introduction
Arteriosclerosis is an important feature of vascular aging,1 and it is not only a critical pathological foundation for cardiovascular diseases but has also been confirmed by several studies as an effective predictor of newly developed diabetes,2 malignant tumors,3 heart failure,4 cardiovascular events,5 and all-cause mortality.6 The European Society of Hypertension/European Society of Cardiology (ESH/ESC) guidelines for hypertension management have included Arteriosclerosis detection as a key indicator for assessing target organ damage.7 The progression of Arteriosclerosis is a chronic and gradual process. Clinically, non-invasive methods, such as carotid-femoral pulse wave velocity (cfPWV) and baPWV, are commonly used to measure large artery stiffness, reflecting the degree of large artery hardening. The rate of Arteriosclerosis progression is related to traditional risk factors, such as aging and blood pressure.8 Furthermore, epidemiological evidence has shown that the level of inflammation in the body is closely related to the development of Arteriosclerosis.9–11 Previous studies on inflammation and Arteriosclerosis have primarily been cross-sectional.12–18 which do not accurately explain the causal relationship between inflammation and the progression of Arteriosclerosis. Although several large prospective cohort studies have confirmed a positive correlation between inflammation levels and long-term pulse wave velocity (PWV),19–25 these studies often lack baseline and repeated PWV measurements, making it impossible to accurately quantify the relationship between inflammation and the longitudinal changes in PWV over time.
C-reactive protein (CRP) is one of the biomarkers of inflammation that can reflect the level of inflammation in the body,26 while baPWV is a classic indicator of arterial stiffness. Currently, there are no large-sample cohort studies that explore the relationship between hs-CRP and repeated measurements of baPWV. To investigate the relationship between the two, this study utilized data from the Kailuan cohort study27 (Registration number: ChiCTR-TNC-11001489) to explore the longitudinal relationship between hs-CRP and the time-dependent changes in baPWV.
Methods
Study Population and Design
Data Source
The data were collected from the Kailuan General Hospital and its 11 affiliated hospitals, where health check-ups were conducted for both active and retired employees of the Kailuan Group from 2006 to 2007. Subsequently, the second to ninth rounds of health check-ups were carried out from 2008 to 2023. Starting in 2010, baPWV measurements were taken during the third to ninth health check-ups for certain populations. The study aimed to explore the relationship between baseline hs-CRP and arterial stiffness over time. Therefore, individuals who participated in at least two baPWV measurements were selected as the study subjects. Following the Declaration of Helsinki, the Kailuan study was approved by the Kailuan General Hospital’s ethics committee (No. 200605). Written informed consent was obtained from all participants.
Inclusion and Exclusion Criteria
Inclusion Criteria: (1) Participants from the Kailuan study population; (2) No cognitive impairment and able to complete the questionnaires; (3) Participants who have undergone health check-ups and completed at least two baPWV measurements during the same period; (4) Individuals who agreed to participate and signed the informed consent form.
Exclusion Criteria: (1) Participants who completed more than two baPWV measurements but had missing baseline data or hs-CRP values; (2) Individuals with physical disabilities that prevent them from undergoing the tests; (3) Participants with atrial fibrillation or lower limb venous thrombosis; (4) Individuals who did not consent to participate in the study.
Data Collection and Definition
The investigators and examination doctors in this study are fixed personnel who have undergone unified training. They strictly follow the unified standards established by the Kailuan study for conducting questionnaires and various tests. The questionnaire survey is administered by specially trained investigators who conduct face-to-face interviews with participants, filling out the content carefully. The survey includes demographic data, occupational status, behavioral habits (sleep, smoking, alcohol consumption, physical exercise, and diet), medical history, and family history. Physical examinations collect data on systolic blood pressure (SBP) and diastolic blood pressure (DBP), resting heart rate (RHR), height, weight, and waist circumference (WC). Body mass index (BMI) was determined as weight (kg) divided by height (m) squared. The mean arterial pressure (MAP) is calculated as: MAP=DBP+ (SBP-DBP) /3. Smoking is defined as smoking at least one cigarette per day on average over the past year, for at least one year. Alcohol consumption is defined as drinking at least 100 mL of white liquor (with an alcohol content of over 50%) per day on average over the past year, for at least one year. Physical exercise is defined as aerobic activities such as walking, jogging, or ball sports for at least 90 minutes per week.
baPWV Measurement
In the Kailuan study, baPWV was assessed by a BP-203 RPE III networked arterial stiffness detection device manufactured by Omron Health Medical (Omron, Dalian, China) Co., Ltd., with data directly read via network connection. The temperature of the examination room is maintained between 22°C and 25°C. Prior to measurement, participants are instructed not to smoke and to rest for at least 5 minutes. The participant’s age, gender, height, and weight are recorded before the examination. At the start of the test, the participant remains calm, lies flat without a pillow, and positions their palms facing up with arms resting at their sides. Blood pressure cuffs are applied to both the upper arms and the ankles. The cuff’s airbag marker is aligned with the brachial artery on the upper arm, with the lower edge of the cuff placed 2–3 cm above the elbow crease. For the lower limbs, the cuff’s airbag marker is positioned on the inner side of the ankle, with the lower edge of the cuff placed 1–2 cm above the inner ankle. The electrocardiogram (ECG) electrodes are connected to the limbs, and one phonocardiogram (PCG) sensor is placed at the V4 position of the chest leads for the ECG. All four cuffs inflate and deflate simultaneously, and both ECG and PCG are monitored. Each participant undergoes two measurements, with the second measurement being used for the final result. The larger of the baPWV values from the left and right sides is taken for analysis in this study.
Laboratory-Related Tests
All study participants were required to fast for at least 8 hours. Blood samples (5 mL) were collected from the antecubital vein between 7:00 AM and 9:00 AM. The samples were analyzed within 4 hours for total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), fasting blood glucose (FBG), and hs-CRP. Serum hs-CRP levels were measured using the immunoturbidimetric method. From 2006 to 2009, the Ministry of Health’s proficiency testing (Laboratory Proficiency Testing, PT) results for hs-CRP analysis in our laboratory were consistently 100%. Additionally, for each experimental sample, two measurements were conducted daily with a minimum interval of 2 hours, over a span of 20 days, to evaluate measurement precision. The results showed that the intra-assay coefficient of variation (CV) was 6.53%, the inter-assay CV was 4.78%, the intra-day CV was 6.61%, and the total CV was 9.37%. Blood glucose levels were measured using the hexokinase method, with reagents provided by Zhongsheng Beikong Biotechnology (Zhongsheng Beikong, Beijing, china) Co., Ltd., The CV for this method was less than 2%. All analyses were performed using a Hitachi 7600 automatic biochemical analyzer (Hitachi, Tokyo, Japan).
Follow-Up
The follow-up period began with the first measurement of baPWV conducted after the third health check-up in 2010–2011. The follow-up ended at the conclusion of the ninth health check-up in 2023.
Statistical Analysis
Health check-up data were entered by specially trained personnel at each hospital and uploaded to the Kailuan General Hospital’s computer room server via the network, forming an Oracle 10.2 database (Oracle Corporation, Redwood, USA). Statistical analysis was performed using SAS 9.4 software. Normally distributed continuous data are described using the mean and standard deviation (SD), compared with the one- way ANOVA. Skewed continuous data are summarized by the median and interquartile range, compared with the Wilcoxon rank-sum test. Categorical variables are described as frequencies and percentages, compared with the χ2 test. A linear mixed-effects model was used to analyze the longitudinal effect of different baseline hs-CRP levels on the progression of baPWV over time, along with the 95% confidence intervals (CIs). Two multifactorial adjustment models were constructed: Model 1, controlled for age, gender and Follow-up time; Model 2, controlled for age, gender, Follow-up time, MAP, LDL-C, HDL-C, TC, TG, FBG, RHR, BMI, and lifestyle factors (smoking, alcohol intake, physical activity).
Sensitivity analysis: To mitigate the potential confounding effects of acute-phase inflammation (hsCRP>10mg/L), cancer patients, and the use of antihypertensive, lipid-lowering, or glucose-lowering medications on hs-CRP levels, individuals with these conditions were excluded from a subsequent analysis. A bilateral P<0.05 was deemed statistically significant.
Result
Baseline Characteristics
A total of 30,021 subjects underwent at least two baPWV measurements. Baseline data were derived from the most recent health examination conducted before the first baPWV measurement. After excluding 3,949 participants with missing baseline hs-CRP or other health examination data, and 736 participants with ABI < 0.9 or ABI > 1.4, a total of 25,336 participants were included in the statistical analysis. Among them, 16,532 were male (65.25%) and 8,804 were female (34.75%). To ensure the robustness of the results, this study further excluded 3,445 participants with hs-CRP > 10 mg/L, those taking antihypertensive, hypoglycemic, or lipid-lowering medications, and those with tumors. Consequently, a sensitivity analysis was performed on the final cohort of 21,891 participants (Figure 1).
 |
Figure 1 Flowchart of the study participants. Abbreviations: baPWV, brachial-ankle pulse wave velocity; ABI, ankle-brachial Index. |
The mean interval between the first and final baPWV measurements was 4.62 ± 2.86 years. Based on baseline hs-CRP levels, participants were categorized into three groups: hs-CRP < 1 mg/L, 1 mg/L ≤ hs-CRP ≤ 3 mg/L, and hs-CRP > 3 mg/L.28 As baseline hs-CRP levels increased, the following parameters also showed an upward trend: baPWV, age, MAP, SBP, DBP, FBG, LDL-C, BMI, RHR, WC, the proportion of participants using antihypertensive and antidiabetic medications, and tobacco exposure. Conversely, HDL-C levels gradually decreased. All differences were statistically significant (P < 0.05; Table 1).
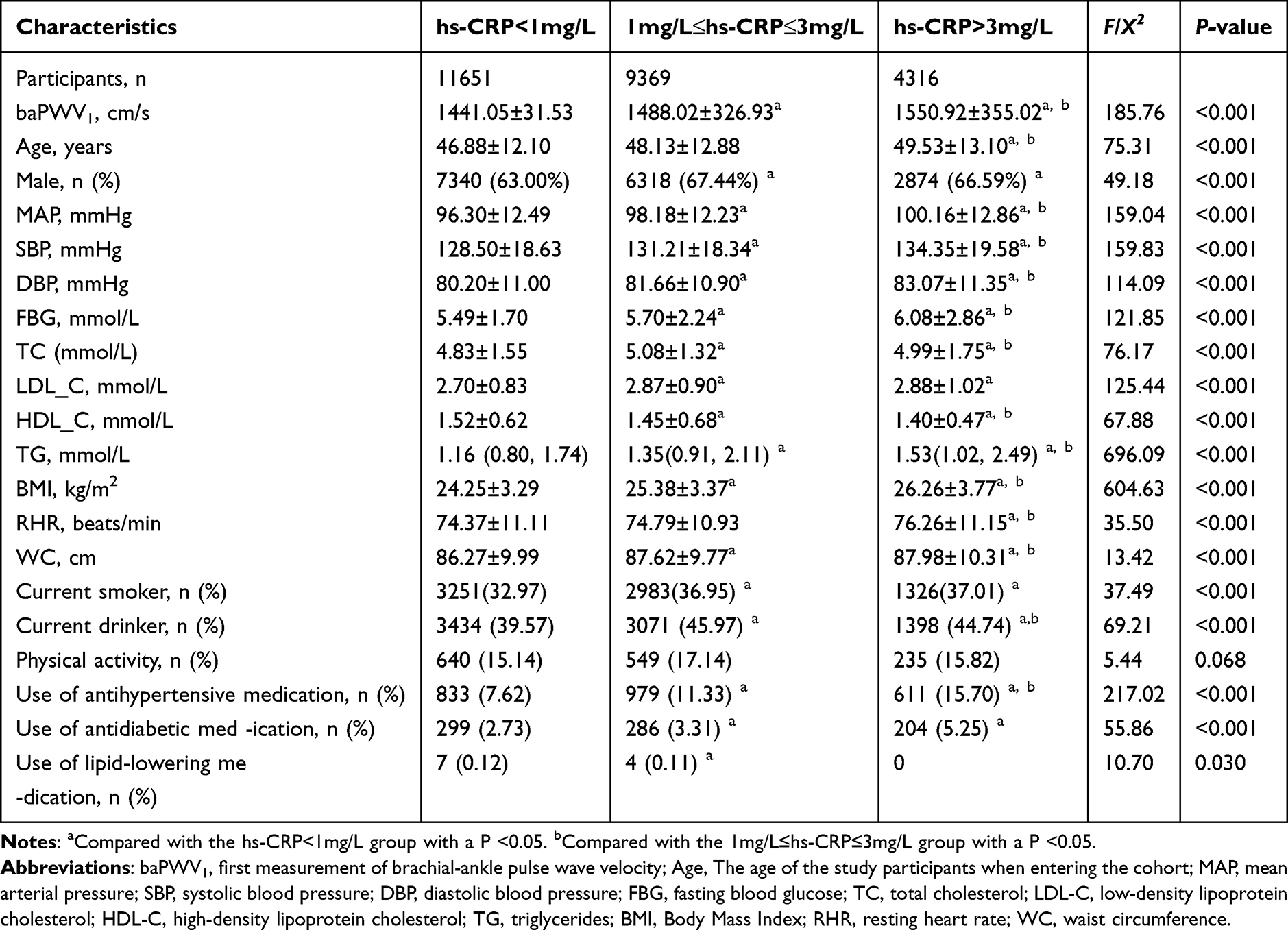 |
Table 1 Comparison of Baseline Characteristics Among Different hs-CRP Groups |
Progression of baPWV in the Study Population
Among the 25,336 study participants included in the statistical analysis, the average baPWV values at the second measurement for the groups with hs-CRP < 1 mg/L, 1 mg/L ≤ hs-CRP ≤ 3 mg/L, and hs-CRP > 3 mg/L were 1525.31, 1576.08, and 1624.84 cm/s, respectively. The differences between the groups were statistically significant (P < 0.05). The average increase in baPWV for each group was 84.26, 88.06, and 73.92 cm/s, respectively, and the inter-group comparisons were also statistically significant (P < 0.05) (Table 2).
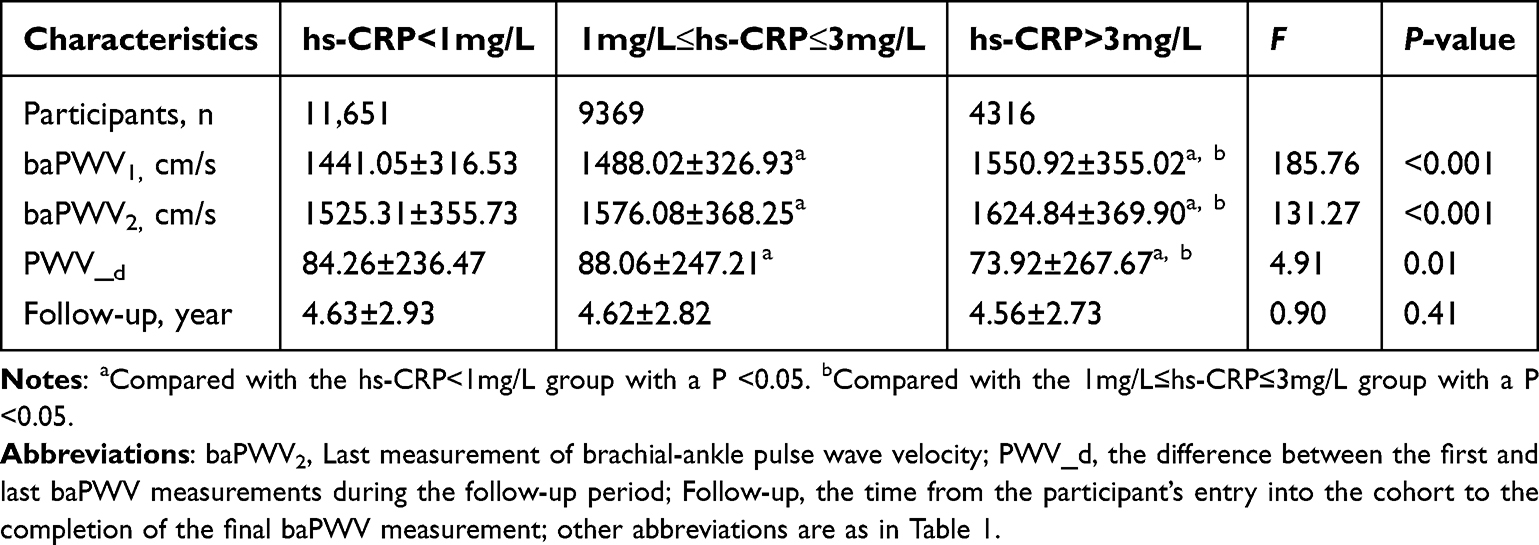 |
Table 2 Progression of baPWV in Different hs-CRP Group Populations |
Linear Mixed-Effects Model Analysis of Factors Affecting Longitudinal Changes in baPWV
Using the hsCRP_1 group as the reference group, Model 1 adjusted for age, gender, and Follow-up time. The results showed that the baPWV increase rate in the hsCRP_2 and hsCRP_3 groups was significantly higher than the control group, with effect Estimate of 27.29 cm/s (95% CI: 22.79 to 31.78, P<0.001) and 63.63 cm/s (95% CI: 57.80 to 69.45, P<0.001), respectively. Model 2 further adjusted for MAP, lipid profiles (LDL-C, HDL-C, TC, TG), FBG, RHR, BMI, and lifestyle factors (smoking, alcohol intake, physical activity). The effect Estimate for hsCRP_2 and hsCRP_3 groups decreased but remained significantly different, with effect Estimate of 14.44 cm/s (95% CI: 6.54 to 22.34, P<0.001) and 40.67 cm/s (95% CI: 5.28 to 51.02, P<0.001), respectively. Subgroup analysis after stratification by gender showed significant gender differences in the effect of hsCRP on baPWV progression, with men exhibiting a significantly faster baPWV progression compared to women. The results suggest that the effect of hsCRP on arterial stiffness differs by gender (Table 3).
 |
Table 3 Analysis of Factors Influencing Longitudinal Changes in baPWV Using a Linear Mixed-Effects Model |
Sensitivity Analysis
To ensure the accuracy of the research results, we excluded other factors that might affect hs-CRP levels, including acute-phase inflammation (hs-CRP > 10 mg/L), cancer patients, and individuals taking antihypertensive, lipid-lowering, and antidiabetic medications, and re-analyzed the data. The results showed that as the hs-CRP levels increased, the rate of increase in baPWV significantly accelerated. In Model 1, the effect Estimate for the hsCRP_2 and hsCRP_3 groups were 24.23 cm/s (95% CI: 19.84 to 28.62, P<0.001) and 57.18 cm/s (95% CI: 51.06 to 63.31, P<0.001), respectively. In Model 2, the effect Estimate for the hsCRP_2 and hsCRP_3 groups were 15.98 cm/s (95% CI: 18.30 to 23.65, P<0.001) and 45.28 cm/s (95% CI: 34.38 to 56.19, P<0.001), respectively. The sensitivity analysis further confirmed that higher hs-CRP levels were significantly positively correlated with the accelerated increase in baPWV (Table 4).
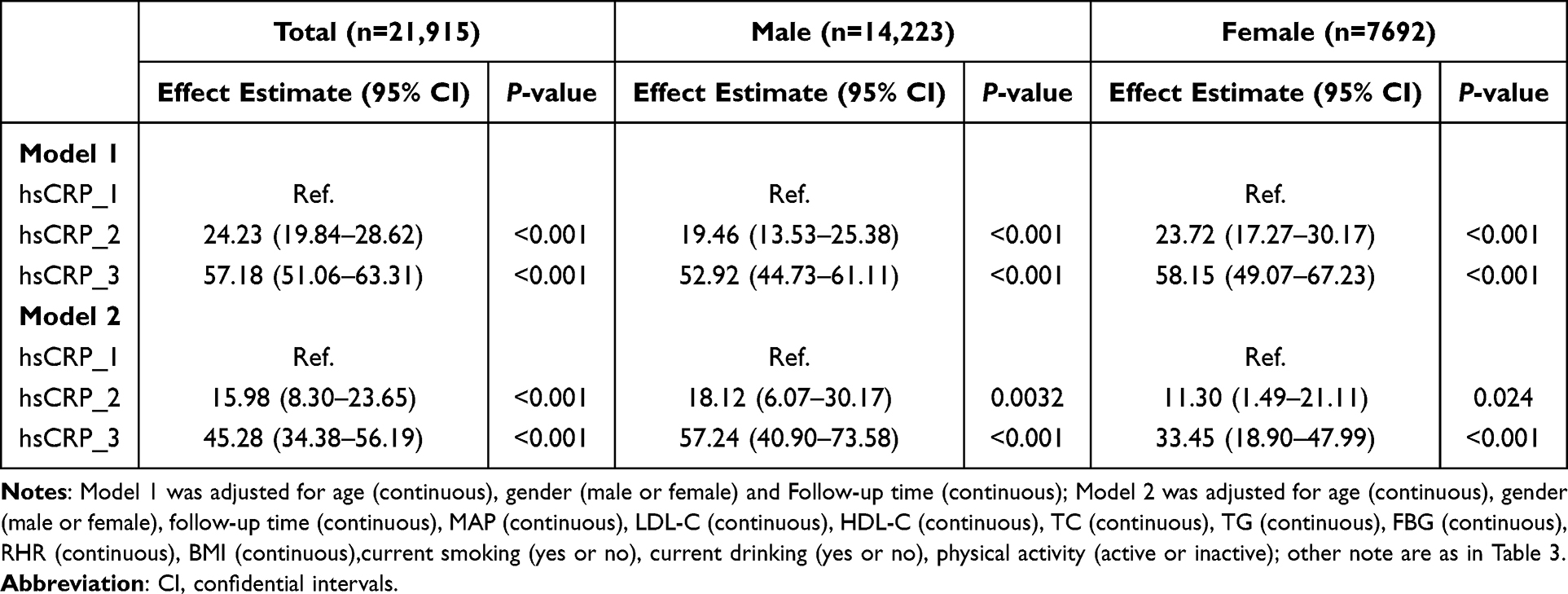 |
Table 4 Sensitivity Analysis Result |
Discussion
This study followed 25,336 participants for an average interval of 4.62 ± 2.86 years and found a positive correlation between hs-CRP levels and the progression of arterial stiffness. Notably, this effect exhibited gender differences, with a more pronounced impact observed in the male population.
First, this study found a positive association between hs-CRP levels and baPWV at baseline. After an average observation period of 4.62 years, the rates of increase in baPWV differed among the hs-CRP groups. In the low-to-medium hs-CRP groups, baPWV increased from 84.26 cm/s in the hsCRP_1 group to 88.06 cm/s in the hsCRP_2 group. In contrast, the increase moderated in the higher-level hsCRP_3 group, reaching only 73.92 cm/s. Our team’s previous research29 found that in individuals with normal arterial stiffness, elevated hs-CRP concentrations were not only associated with faster baPWV at baseline but also showed a significant positive association with the rate of increase in baPWV over time. A similar phenomenon was observed in the Rotterdam study,30 where among middle-aged and elderly individuals aged 55 and over with higher arterial stiffness, the rate of increase in cfPWV tended to moderate as CRP levels increased across tertiles. Given that the average arterial stiffness in all hs-CRP subgroups of our study population was already high at baseline (baPWV ≥ 1400 cm/s),31 Thus, we consider that the impact of hs-CRP on the progression of atherosclerosis may exhibit a “ceiling effect” meaning that when atherosclerosis reaches a certain stage, the influence of inflammation plateaus.
This study not only confirms the longitudinal association between hs-CRP and the progression of Arteriosclerosis but also quantifies the impact of varying inflammation levels on the rate of progression. The linear mixed-effects model analysis, after adjusting for age, gender, follow-up time, MAP, lipid parameters (LDL-C, HDL-C, TC, TG), FBG, HR, BMI and lifestyle factors (smoking, alcohol intake, physical activity), showed that compared to the hsCRP_1 group, the baPWV in the hsCRP_2 and hsCRP_3 groups increased by 14.44cm/s (95% CI: 6.54 to 22.34) and 40.67 cm/s (95% CI: 5.28 to 51.02), respectively. Previous findings from the Caerphilly20 Prospective Cohort Study have shown that in older adults, baseline CRP levels are independently associated with the progression of aortic pulse wave velocity (aPWV) over a 20-year follow-up, as demonstrated by multivariable linear regression analysis (β: 0.35, P = 0.002). Furthermore, the acceleration of aPWV was strongly associated with cumulative CRP exposure. Similarly, the Malmö Diet and Cancer cohort study21 from Sweden found that in a middle-aged population with an average age of 55.97 years, baseline CRP levels, categorized by quartiles, were associated with changes in cfPWV after a median follow-up of 16.9 years. Specifically, the cfPWV in the Q1 and Q4 groups were 9.96 m/s vs 10.37 m/s (P < 0.001). These findings support the existence of a “dose-response” relationship between hs-CRP and the longitudinal progression of Arteriosclerosis.
The subgroup analysis stratified by gender further reveals that hs-CRP has a more significant impact on the male population. Compared to the hsCRP_1 group, the baPWV in the hsCRP_2 and hsCRP_3 groups increased by 20.56 cm/s (95% CI: 6.18 to 8.45) and 43.06 cm/s (95% CI: 27.82 to 58.31), respectively. In contrast, the Whitehall II study22 found that in a cohort of 3,769 European middle-aged individuals, after 16 years of observation, each doubling of baseline CRP concentration was associated with an increase in aPWV of 130 cm/s in men and 140 cm/s in women. Similarly, the ALSPAC study23 found that in a cohort of Caucasian adolescents with an average age of 17.7 years, after 7 years of follow-up, hs-CRP levels were independently positively correlated with cfPWV progression only in the female population (β =0.083, P < 0.001). One potential reason for the gender differences observed is that, compared to men, women have higher baseline hs-CRP concentrations, whereas in this study, the hs-CRP levels were higher in the male population. These findings suggest that the effect of hs-CRP on the progression of Arteriosclerosis varies by gender across different populations.
hs-CRP, as a nonspecific inflammatory marker, is highly susceptible to interference from various factors. To reduce the risk of bias in the study’s results, acute-phase inflammation (hs-CRP > 10 mg/L), cancer patients, and individuals taking antihypertensive, lipid-lowering, or antidiabetic medications were excluded from the analysis. Sensitivity analysis showed a more significant positive correlation between hs-CRP levels and the progression of Arteriosclerosis. Furthermore, baseline data revealed a clustering trend of other traditional risk factors, such as MAP, FBG, BMI and LDL-C, as hs-CRP levels increased. However, after model correction, hs-CRP levels still showed a statistically significant association with the progression of Arteriosclerosis. Several studies using different surrogate indicators of Arteriosclerosis have also confirmed the relationship between CRP and the progression of Arteriosclerosis. A study by Swamynathan et al24 found that, after a 10-year follow-up of a population with an average age of 59 years, baseline CRP levels were negatively correlated with the rate of dilation of both the ascending and descending aorta over time. Additionally, a study in Rotterdam25 discovered that, in a healthy middle-aged and elderly population, hs-CRP levels were positively associated with the risk of developing isolated systolic hypertension as a result of Arteriosclerosis. For each standard deviation increase in hs-CRP, the risk of isolated systolic hypertension increased by 19%. These findings, along with the results from sensitivity analysis, further support a significant longitudinal association between hs-CRP and the progression of Arteriosclerosis.
The current understanding suggests that CRP may contribute to the development of Arteriosclerosis through the following mechanisms: (1) CRP directly inhibits the expression of endothelial nitric oxide synthase (eNOS). Cytokines, such as tumor necrosis factor-α and interleukin-1, produced during inflammation, suppress the activation of eNOS by receptor-dependent agonists, thereby increasing the expression of inducible nitric oxide synthase, which further impairs eNOS activity. (2) Additionally, reactive oxygen species (ROS) generated during inflammation further consume nitric oxide (NO), collectively leading to a reduction in NO bioactivity, decreased vascular dilation, and accelerated progression of Arteriosclerosis.32,33 (3) Prolonged inflammation leads to the activation of matrix metalloproteinases on endothelial and smooth muscle cells by ROS, which degrade tissue inhibitors of metalloproteinases, resulting in elastin degradation and smooth muscle cell proliferation. This impairs the cross-linking of collagen and elastin, ultimately increasing collagen content and promoting Arteriosclerosis.34–37
Strengths and Limitations
This study is a large-sample cohort study that, while confirming the relationship between hs-CRP and the longitudinal changes in arterial stiffness over time, also presents several limitations. (1) The cohort study grouped participants based on their baseline hs-CRP levels at the start of the follow-up, without considering the dynamic changes in hs-CRP levels during the follow-up period and their potential impact on baPWV. Additionally, given that hs-CRP assays were conducted across multiple laboratories with varying reference ranges, this methodological heterogeneity may introduce potential confounding effects on the results.
(2) The study had a relatively short average follow-up time, and given the multitude of factors influencing arterial stiffness, not all potential confounders were included in the statistical analysis, which could affect the accuracy of the results. However, the use of a more robust linear mixed-effects model for analyzing the impact of hs-CRP on baPWV further mitigated the influence of confounding factors. (3) The study utilized baPWV as a surrogate marker for arterial stiffness, rather than cfPWV, which is recognized as the gold standard for arterial stiffness by the European Society of Hypertension and the European Society of Cardiology.38 However, baPWV demonstrates a good correlation with cfPWV and is more widely used in Asian populations. (4) The study predominantly involved male participants, which may limit the generalizability of the results to other populations. Nevertheless, gender analysis was conducted, and the results revealed a significant association between hs-CRP and the progression of arterial stiffness in both men and women.
Conclusion
This study demonstrates that elevated hs-CRP levels exhibit a significant dose-response relationship with the longitudinal progression of arterial stiffness in a general Northern Chinese population, with a more pronounced association observed among males. However, when arterial stiffness reaches a higher level, the magnitude of hs-CRP’s influence may exhibit a “ceiling effect”.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding authors upon reasonable request.
Ethics Approval and Consent to Participate
The Kailuan study was approved by the Kailuan General Hospital’s ethics committee (No. 200605). Before participation, all individuals provided written informed consent.
Acknowledgments
We sincerely express our gratitude to all the staff and participants of the Kailuan Cohort for their invaluable contributions to this project.
Funding
This work was supported by the Hebei Provincial Medical Research Project Plan (2025) (No. 20251339).
Disclosure
The authors declared no conflicts of interest in this work.
References
1. Wu ZG, Wu D, Chen SH, et al. Resting heart rate mediates the association between circulating neutrophil count and arterial stiffness progression: the kailuan study. J Inflamm Res. 2024;21(17):11347–11356. doi:10.2147/JIR.S488928
2. Lou YM, Liao MQ, Wang CY, et al. Association between brachial ankle pulse wave velocity and risk of type 2 diabetes mellitus: results from a cohort study. BMJ Open Diabetes Res Care. 2020;8(1):1317–1326. doi:10.1136/bmjdrc-2020-001317
3. Yu JY, Liu D, Liu T, et al. Relationship between pulse wave velocity of brachial-ankle artery and malignant tumor. Hebei Med. 2024;46(02):231–234. doi:10.3969/j.issn.1002-7386.2024.02.015
4. Zheng HW, Wu SL, Liu XK, et al. Association between arterial stiffness and new-onset heart failure: the kailuan study. Arterioscler Thromb Vasc Biol. 2023;43(2):e104–e111. doi:10.1161/ATVBAHA.122.317715
5. Van Sloten TT, Sedaghat S, Laurent S, et al. Carotid stiffness is associated with incident stroke: a systematic review and individual participant data meta-analysis. J Am Coll Cardiol. 2015;66(19):2116–2125. doi:10.1016/j.jacc.2015.08.888
6. Bäck M, Topouchian J, Labat C, et al. Cardio-ankle vascular index for predicting cardiovascular morbimortality and determinants for its progression in the prospective advanced approach to arterial stiffness (TRIPLE-A-Stiffness) study. EBioMedicine. 2024;5(103):105–107. doi:10.1016/j.ebiom.2024.105107
7. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ ESC guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013;31(7):1281–1357. doi:10.1097/01.hjh.0000431740.32696.cc
8. Corte VD, Antonino Tuttolomondo A, Pecoraro R, et al. Inflammation, endothelial dysfunction and arterial stiffness as therapeutic targets in cardiovascular medicine. Curr Pharm Des. 2016;22(30):4658–4668. doi:10.2174/1381612822666160510124801
9. Yang JY, Nam JS, Choi HJ. Association between high-sensitivity C-reactive protein with arterial stiffness in healthy Korean adults. Clin Chim Acta. 2012;413(19):1419–1423. doi:10.1016/j.cca.2012.06.004
10. Weiss TW, Arnesen H, Seljeflot I. Components of the interleukin-6 transsignalling system are associated with the metabolic syndrome, endothelial dysfunction and arterial stiffness. Metabolism. 2013;62(7):1008–1013. doi:10.1016/j.metabol.2013.01.019
11. Park BJ, Shim JY, Lee HR, et al. Relationship of neutrophil-lymphocyte ratio with arterial stiffness and coronary calcium score. Clin Chim Acta. 2011;412(11):925–929. doi:10.1016/j.cca.2011.01.021
12. Wang X, Du YZ, Fan L, et al. Relationships between HDL-C, hs-CRP, with central arterial stiffness in apparently healthy people undergoing a general health examination. PLoS One. 2013;8(12):81778. doi:10.1371/journal.pone.0081778
13. Pettersson-Pablo P, Cao Y, Bäckström T, et al. Body fat percentage and CRP correlates with a composite score of vascular risk markers in healthy, young adults- The Lifestyle, Biomarkers, and Atherosclerosis (LBA) study. BMC Cardiovasc Disord. 2020;20(1):77. doi:10.1186/s12872-020-01376-6
14. Nakhai-Pour HR, Grobbee DE, Bots ML, et al. C-reactive protein and aortic stiffness and wave reflection in middle-aged and elderly men from the community. J Hum Hypertens. 2007;21(12):949–955. doi:10.1038/sj.jhh.1002255
15. Ojima S, Kubozono T, Kawasoe S, et al. Association of risk factors for atherosclerosis, including high sensitivity C-reactive protein, with carotid intima-media thickness, plaque score, and pulse wave velocity in a male population. Hypertens Res. 2020;43(5):422–430. doi:10.1038/s41440-019-0388-2
16. Aminuddin A, Lazim MRMLM, Hamid AA, et al. The association between inflammation and pulse wave velocity in dyslipidemia: an evidence-based review. Mediators Inflamm. 2020;1(01).
17. McKechnie DGJ, Patel M, Papacosta AO. Associations between inflammation, coagulation, cardiac strain and injury, and subclinical vascular disease with frailty in older men: a cross-sectional study. BMC Geriatr. 2022;22(1):405. doi:10.1186/s12877-022-03106-3
18. Mozos L, Jianu D, Gug C, et al. Links between high-sensitivity c-reactive protein and pulse wave analysis in middle-aged patients with hypertension and high normal blood pressure. Dis Markers. 2019;5(17):2568069. doi:10.1155/2019/2568069
19. Wang KK, Wang Y, Chu C, et al. Joint association of serum homocysteine and high-sensitivity C-reactive protein with arterial stiffness in chinese population: a 12-year longitudinal study. Cardiology. 2019;144(1):27–35. doi:10.1159/000501742
20. McEniery CM, Spratt M, Munnery M, et al. An analysis of prospective risk factors for aortic stiffness in men: 20-year follow-up from the caerphilly prospective study. Hypertension. 2010;56(1):36–43. doi:10.1161/HYPERTENSIONAHA.110.150896
21. Muhammad IF, Borne Y, Ostling G, et al. Acute phase proteins as prospective risk markers for arterial stiffness: the malmo diet and cancer cohort. PLoS One. 2017;12(7):e0181718. doi:10.1371/journal.pone.0181718
22. Johansen NB, Vistisen D, Brunner EJ, et al. Determinants of aortic stiffness: 16-year follow-up of the Whitehall II study. PLoS One. 2012;7(5):e37165. doi:10.1371/journal.pone.0037165
23. Agbaje AO, Barmi S, Sansum KM, et al. Temporal longitudinal associations of carotid-femoral pulse wave velocity and carotid intima-media thickness with resting heart rate and inflammation in youth. J Appl Physiol. 2023;134(3):657–666. doi:10.1152/japplphysiol00701.2022
24. Swamynathan R, Varadarajan V, Nguyen H, et al. Association between biomarkers of inflammation and 10-year changes in aortic stiffness: the multi-ethnic study of atherosclerosis. J Clin Med. 2023;12(15):50–62. doi:10.3390/jcm12155062
25. Mattace-Raso FUS, Verwoert GC, Hofman A, et al. Inflammation and incident-isolated systolic hypertension in older adults: the Rotterdam study. J Hypertens. 2010;28(5):892–895. doi:10.1097/HJH.0b013e328336ed26
26. Corte VD, Tuttolomondo A, Pecoraro R, et al. Inflammation, endothelial dysfunction and arterial stiffness as therapeutic targets in cardiovascular medicine. Curr Pharm Des. 2016;22(30):4658–4668. doi:10.2174/1381612822666160510124801
27. Chinese Clinical Trial Registry. Cardiovascular and cerebrovascular diseases, risk factors, and intervention study (Kailuan Study). Available from: http://www.Chictr.org/cn/proj/show.aspx?proj=1441.
28. Pearson TA, Mensah GA, Alexander RW, et al. Markers of inflammation and cardiovascular disease-application to clinical and public health practice: a statement for healthcare professionals from the centers for disease control and prevention and the American heart association. Circulation. 2003;107(3):499–511. doi:10.1161/01.CIR.0000052939.59093.45
29. Li WZ, Liang P, Ma XL, et al. The association between high-sensitivity C-reactive protein and the progression of arteriosclerosis: the kailuan study. J Inflamm Res. 2025;18:7047–7054. doi:10.2147/JIR.S524495
30. Mattace-Raso FU, van der Cammen TJM, van der Meer IM, et al. C-reactive protein and arterial stiffness in older adults: the rotterdam study. Atherosclerosis. 2004;176(1):111–116. doi:10.1016/j.atherosclerosis.2004.04.014
31. Takashima N, Turin TC, Matsui K, et al. The relationship of brachial-ankle pulse wave velocity to future cardiovascular disease events in the general Japanese population: the Takashima Study. J Hum Hypertens. 2014;28(5):323–327. doi:10.1038/jhh.2013.103
32. Gunnett CA, Lund DD, McDowell AK, et al. Mechanisms of inducible nitric oxide synthase–mediated vascular dysfunction. Arterioscler Thromb Vasc Biol. 2005;25(8):1617–1622. doi:10.1161/01.ATV.0000172626.00296
33. Stewart AD, Millasseau SC, Kearney MT, et al. Effects of inhibition of basal nitric oxide synthesis on carotid-femoral pulse wave velocity and augmentation index in humans. Hypertension. 2003;42(5):915–918. doi:10.1161/01.HYP.0000092882.65699.19
34. Boutouyrie P, Chowienczyk P, Humphrey JD, et al. Arterial stiffness and cardiovascular risk in hypertension. Circ Res. 2021;128(7):864–886. doi:10.1161/CIRCRESAHA.121.318061
35. Yasmin, McEniery CM, Wallace S, Wallace S, et al. C-reactive protein is associated with arterial stiffness in apparently healthy individuals. Arterioscler Thromb Vasc Biol. 2004;24(5):969–974. doi:10.1161/01.ATV.zhq0504.0173
36. Zieman SJ, Melenovsky V, Kass DA. Mechanisms, pathophysiology and therapy of arterial stiffness. Arterioscler Thromb Vasc Biol. 2005;25(5):932–943. doi:10.1161/01.ATV.000016054878317.29
37. Wang M, Lakatta EG. Altered regulation of matrix metalloprotein ase-2 in aortic remodeling during aging. Hypertension. 2002;39(4):865–873. doi:10.1161/01.hyp.0000014506.13322.66
38. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013;34(28):2159–2219.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.