Back to Journals » International Journal of Women's Health » Volume 17
Association Between Hepatic Steatosis Index and Endometrial Cancer Risk: A Cross-Sectional Study
Authors Zheng L, Lei H ![]() , Tang X, Zheng Y, Wu Q, Chen P, Chen Y, Cai L
, Tang X, Zheng Y, Wu Q, Chen P, Chen Y, Cai L ![]()
Received 4 November 2024
Accepted for publication 20 February 2025
Published 17 March 2025 Volume 2025:17 Pages 825—833
DOI https://doi.org/10.2147/IJWH.S497621
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Lili Zheng,1,* Huifang Lei,1,* Xiaoyi Tang,2 Yuanyin Zheng,3 Qiuzhen Wu,3 Peixuan Chen,1 Yanhong Chen,1 Liangzhi Cai4,5
1Department of Gynecology, Mindong Hospital Affiliated to Fujian Medical University, Ningde, People’s Republic of China; 2Department of Laboratory, Mindong Hospital Affiliated to Fujian Medical University, Ningde, People’s Republic of China; 3Department of Pathology, Mindong Hospital Affiliated to Fujian Medical University, Ningde, People’s Republic of China; 4Fujian Maternity and Child Health Hospital, College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, People’s Republic of China; 5Fujian Key Laboratory of Women and Children’s Critical Diseases Research, Fuzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liangzhi Cai, Fujian Maternity and Child Health Hospital, College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Daoshan Road 18, Fuzhou, 350001, People’s Republic of China, Tel +86 1 348 910 2656, Fax +86 591 87551247, Email [email protected]
Purpose: To investigate the relationship between hepatic steatosis index (HSI) and endometrial cancer (EC) and its diagnostic value for EC.
Patients and Methods: A total of 114 patients with pathologically diagnosed EC in Mindong Hospital, Ningde City, Fujian Province from 2016 to 2022 were retrospectively included as the EC group. A total of 175 patients with pathologically confirmed benign endometrial lesions (endometrial polyps and uterine submucosal fibroids) in the same hospital during the same period were selected as the control group. Non-parametric test were used to compare the differences in HSI and non-alcoholic fatty liver disease (NAFLD) between the two groups, and the diagnostic value of HSI and NAFLD levels on EC was analysed. The cut-off point of continuous variables was determined by receiver operating characteristic (ROC) curve analysis. Logistic regression analysis was used to calculate odds ratios (ORs).
Results: The results showed that compared with the control group, serum GGT, CA125, HDL-C and HSI were significantly increased in the EC group (P< 0.05). 27.19% of the EC patients (31/114) and 12% of the control group (21/175) had NAFLD, and the difference between the two groups was statistically significant (P< 0.05). The results of univariate logistic regression analysis showed that GGT, CA125, HDL-C, HSI and NAFLD were significantly correlated with the occurrence of EC (P< 0.05). Further multivariate logistic regression analysis showed that CA125 and HSI elevation were independent risk factors for EC (P< 0.05).
Conclusion: NAFLD is closely associated with EC, and elevated HSI is an independent risk factor for EC.
Keywords: nonalcoholic fatty liver disease, hepatic steatosis index, endometrial cancer
Introduction
Endometrial cancer (EC) is one of the three most common malignancies of the female reproductive system.1 According to the American Cancer Society, the incidence of EC increased by 0.6% to 1% per year between 2015 and 2019, and survival decreased, with the 5-year relative survival rate for black women being only 63% compared to 84% for white women.2 The results of a Chinese study also showed that the incidence of EC has increased since 2007.3 EC prevalence and mortality continue to increase with increasing risk factors.4 If EC is diagnosed and treated early, the prognosis is good.5 However, the early symptoms of EC are often insidious, or perimenopausal bleeding may go unnoticed, undiagnosed and untreated, and most patients may be diagnosed at intermediate and advanced stages, with poor outcomes. In addition, clinical practice guidelines do not recommend screening for EC in healthy individuals, so there is still a long way to go to improve the overall survival rate of EC.6
Currently, serum CA125 is the most commonly used biomarker for early diagnosis of EC in clinical practice, but it is elevated in both benign and malignant tumours and lacks specificity. Cytology using urine and vaginal lavage fluid for the diagnosis of EC has also been studied,7 but has not been widely used due to data collection problems. Presently, the clinical diagnosis of EC is mainly based on transvaginal colour ultrasound, segmented diagnosis and curettage, and outpatient hysteroscopic endometrial biopsy, which have good diagnostic sensitivity, but the specificity of transvaginal colour ultrasound and segmented diagnosis and curettage is not high or causes pain to the patient. Hysteroscopic biopsy is limited by its invasive nature.8,9 It is particularly important to reduce the incidence and mortality of EC if new risk factors for EC can be explored to prevent or treat it in advance, or if new non-invasive, convenient and effective indicators for diagnosing EC can be explored.
Previous studies have shown that obesity, diabetes, metabolic syndrome, polycystic ovary syndrome are high risk factors for EC.10–13 It is worth noting that these indicators are also high risk factors for non-alcoholic fatty liver disease(NAFLD). NAFLD involves a range of liver damage, ranging from simple steatosis to non-alcoholic steatohepatitis, advanced fibrosis, and cirrhosis, and can lead to mild to moderate liver dysfunction. In recent years, several studies have shown that NAFLD is associated with a variety of extrahepatic malignancies.14,15 It is well known that type I EC is an estrogen-associated tumour, and estrogen is mainly metabolised in the liver. Meanwhile, estrogen plays an important role in maintaining lipid metabolism and its deficiency is associated with lipid accumulation in liver cells (hepatic steatosis), the development of NAFLD and insulin resistance.16 Meta-analyses of the observational cohort study by Mantovani et al suggest that NAFLD was a long-term risk factor for the development of certain extrahepatic malignancies, particularly gastrointestinal cancers, breast cancers and EC, ovarian cancer.14,15 And this view holds true after adjustment for potential confounders such as age, gender, smoking, obesity and diabetes.17 In recent years, in order to optimise the management of NAFLD, some scientists have proposed a new indicator, the Hepatic Steatosis Index (HSI), a non-invasive, simple, effective and well-performing screening tool for NAFLD, derived by a logistic regression model: HSI= 8 x(ALT/AST ratio)+BMI (+2 if female; +2 if diabetes mellitus). Previous studies have shown that HSI is significantly associated with cervical stromal involvement in type I EC patients without type 2 diabetes mellitus. The results of these previous studies suggest that NAFLD and HSI are closely related to EC, but the specific mechanism and whether HSI is related to the occurrence of EC remain to be explored. Therefore, the main purpose of this study is to investigate the correlation between NAFLD and HSI and the incidence of EC, in order to provide clinicians with a guide to identify high-risk groups for EC at an early stage.
Materials and Methods
Subjects of the Study
A total of 114 EC patients admitted to Mindong Hospital, Ningde City, Fujian Province, from 2016 to 2022 were selected as the EC group, and 175 age- and body mass index (BMI)-matched controls with benign endometrial lesions were selected as the control group. Inclusion criteria: (1) pathological diagnosis following clinical diagnosis and treatment; (2) complete clinical medical records; (3) Informed consent was obtained from all individual participants enrolled in the study. Exclusion criteria: (1) liver disease other than NAFLD; (2) previous radiotherapy, chemotherapy, hormonal and immunosuppressive therapy; (3) previous liver transplantation and carcinogenesis of other organs; (4) history of drug or alcohol abuse (female≥ 20g/d). This study was reviewed and approved by the Ethics Committee of Mindong Hospital, Ningde City, Fujian Province (No: K2024051002).
Sample Size
In our study, 114 patients with EC and 175 normal controls were included for analysis. We use online software http://powerandsamplesize.com to carry out the sample size calculation, results show that the sample size is sufficient, the power was 0.8, prompt the sample size of this study can get reliable results. Due to the small sample size of our study and the long time span, we cannot rule out that type 1 B errors may have been observed in our statistical analysis.
Data Collection
Blood samples, weight, height and hepatobiliary ultrasound results of all enrolled patients were collected in the morning on a fasting basis within 7 days before surgery. Age, menopausal history, pathological tumour type, muscle invasion, pathological grade, depth of muscle invasion, International Federation of Obstetrics and Gynaecology (FIGO) stage and lymph node metastasis of EC patients were recorded.
Blood Biochemistry and Tumor Marker Indicators
Approximately 5 mL of fasting venous blood was collected from the EC group and the benign endometrial lesion group on the same day or early the next morning, and after standing at room temperature for 1 h, the upper serum was separated by centrifugation at 3000 rpm for 15 min (radius 10 cm). The electrochemiluminescence method was used to detect serum CA125 levels, and the Combase411 Roche E601 automatic chemiluminescence analyser and supporting reagents were purchased from Roche in Switzerland. The biochemical immunoassay method was used to determine blood ALT, AST, GGT, and HDL-C levels, and the Beckman biochemical immunoassay analyzer and supporting reagents were purchased from Beckman Instrument Company of the United States. The reference range of CA125 is 0~47U/mL, the reference range of serum AST is 13~45U/L, the reference range of serum ALT is 7~40U/L, the reference range of GGT is 7~45U/L, and the reference range of HDL-C is 1.29~1.55mmol/L. Specimens included in the quality control measures shall be submitted for testing immediately after collection and within 2 hours. After testing, the experienced laboratory physician will perform the test according to the appropriate technical specifications and operating procedures. The test report must be carefully checked against the patient information and reviewed by another qualified testing physician.
Sonographic Features of Ultrasound in the Diagnosis of NAFLD
Studies had shown that sonographic features of NAFLD were the strongest independent predictors of NAFLD.18 Firstly, viral hepatitis, autoimmune liver disease, alcoholic liver disease and hereditary disorders should be excluded. NAFLD could be considered if any 4 of the following 5 sonographic features were present: (1) rapid attenuation of the image within 4–5 cm of depth; (2) diffuse echogenicity, but it is particularly important to note the brightness within the first 2–3 cm of depth; (3) uniformly heterogeneous liver; (4) thick subcutaneous depth (> 2 cm); and (5) liver filling the entire field with no visible edges.19
Hepatic Steatosis Index (HSI)
The Hepatic Steatosis Index (HSI), an indicator derived from standard laboratory tests and anthropometric parameters, is a non-invasive, simple, effective and well-performing screening tool for NAFLD.20 It is obtained by fitting readily available serum alanine aminotransferase (ALT)/aspartate aminotransferase (AST) ratios, body mass index (BMI) and diabetes factors to multiple regression models. The HSI has a sensitivity of up to 93% for excluding NAFLD and a specificity of 92% for detecting NAFLD.21 It is calculated as follows HSI = 8×ALT/AST ratio + BMI (+2 for diabetes; +2 if female).
Statistical Analysis
SPSS 26.0 software was used for statistical analysis. The continuous variables were first tested for normality, the mean (standard deviation) was used to describe the normal distribution and the t-test was used for comparison between the two groups.The non-normal distribution was described by the median (interquartile range) and the rank-sum test was used for comparison between the two groups. The categorical variables were described by the number of cases (percentage) and the chi-squared test was used for comparison between the two groups. The ROC curve was plotted to analyse the diagnostic value of each index for EC. Univariate analysis of risk factors for EC was performed using binary logistic regression. The Hosmer and Lemeshow test was used to test logistic regression model hypotheses. When logistic regression analysis was performed in this study, cases with missing values were automatically excluded from the analysis. Based on the univariate analysis, all variables with P<0.05 were included in the multivariate model to analyse the independent risk factors for EC. P<0.05 was statistically significant.
Results
Comparison of Baseline Data Between the EC Group and the Control Group
In the EC group, there were 42 premenopausal cases (36.84%) and 72 postmenopausal cases (63.16%). In the control group, there were 101 premenopausal cases (57.71%) and 74 postmenopausal cases (42.29%), and there was no significant age difference between the two groups (P>0.05, Table 1). In the EC group, 75 cases (65.79%) had a BMI < 25 kg/m2 and 39 cases (34.21%) had a BMI ≥ 25 kg/m2. In the control group, 136 cases (77.71%) with a BMI < 25 kg/m2 and 39 cases (22.29%) with a BMI ≥ 25 kg/m2, and there was no significant difference in BMI between the two groups (P>0.05, Table 1). Results are detailed in Table 1.
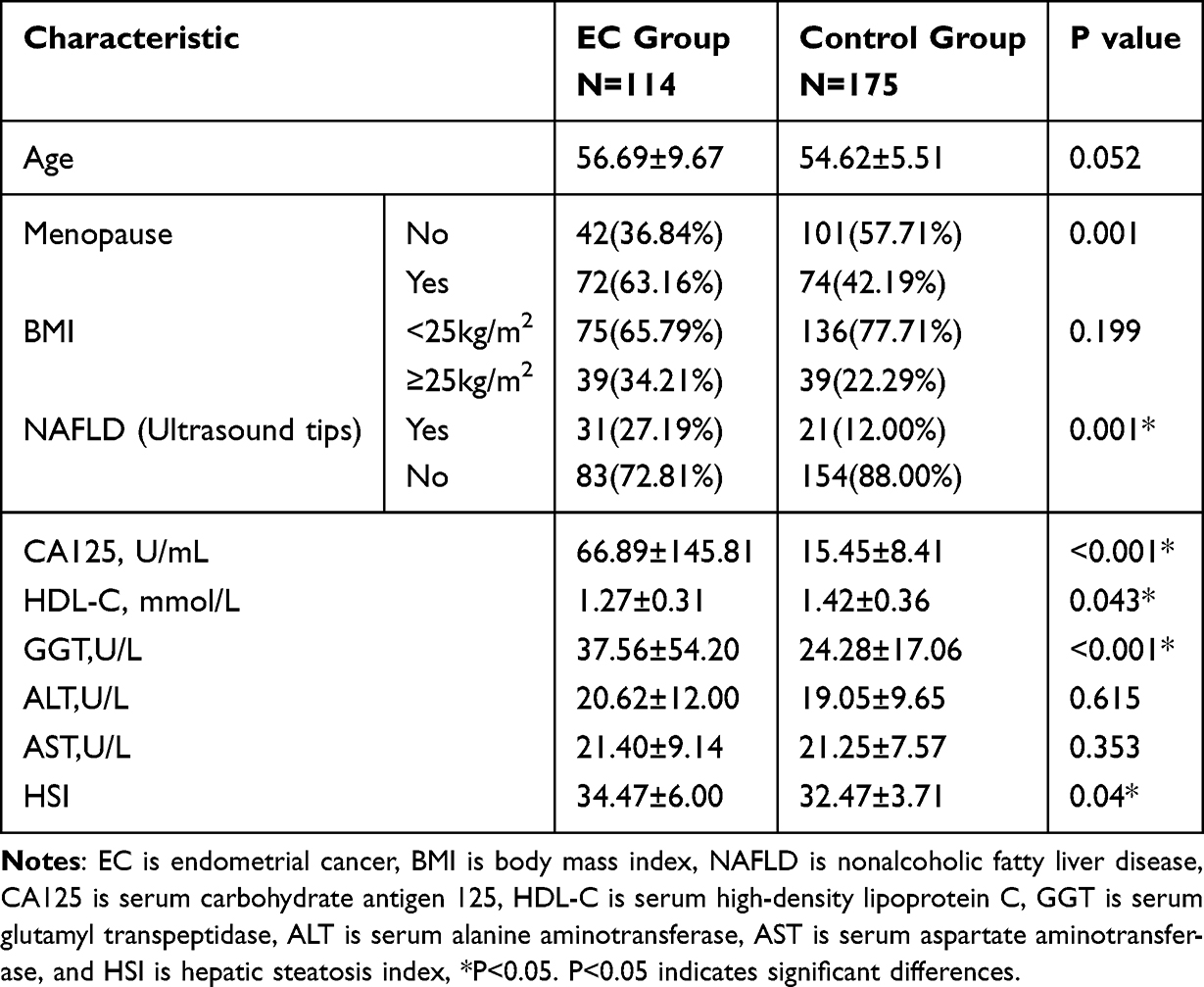 |
Table 1 Comparison of Baseline Data Between the EC Group and the Control Group |
Correlations Between Clinical Features and EC
There was a statistically significant difference in NAFLD between the two groups (P<0.05), there was no statistical difference in serum AST and ALT (P>0.05), and there were significant differences in serum GGT, CA125, HDL-C and HSI between the EC group and the control group (P<0.05), and the above indices were higher in the EC group than in the control group. The specific results are detailed in Table 1 and Figure 1.
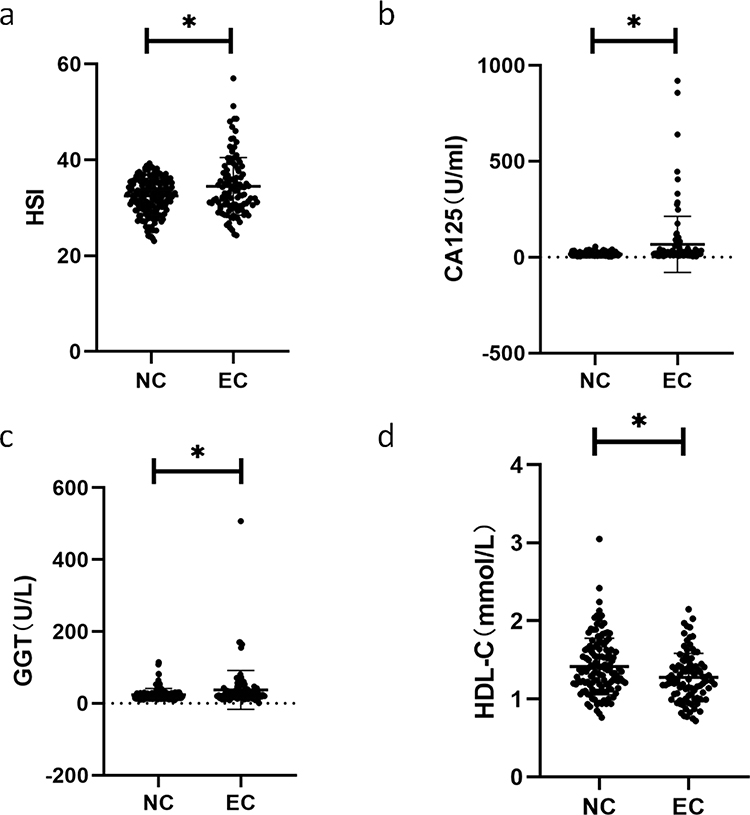 |
Figure 1 HSI levels and serum CA125, GGT and HDL-C levels in the EC group and the benign endometrial lesion group. Notes: The NC was the control group of benign endometrial lesions; The EC was the endometrial cancer case group; HSI is hepatic steatosis index; CA125 is serum carbohydrate antigen 125; GGT is serum glutamyl transpeptidase; HDL-C is serum high-density lipoprotein C; *P< 0.05. P<0.05 indicates significant differences. (a) HSI levels in the EC group and the benign endometrial lesion group; (b) Serum CA125 levels in the EC group and the benign endometrial lesion group; (c) Serum GGT levels in the EC group and the benign endometrial lesion group; (d) Serum HDL-C levels in the EC group versus the benign endometrial lesion group. |
The Independent Risk Factors for EC
Based on the analysis results of the non-parametric test in Table 1, we included the indicators with significant differences between EC and the control group, including GGT, CA125, HDL-C and HSI, in the ROC curve analysis and determined the cut-off value according to the Youden index (all P<0.05, Figure 2). We then included these serum markers and NAFLD in univariate logistic regression analysis. The results of univariate logistic regression analysis showed that GGT, CA125, HDL-C, HSI and NAFLD were significantly correlated with the occurrence of EC (P<0.05, Table 2). Further multivariate logistic regression analysis showed that CA125 and HSI elevation were independent risk factors for EC (P<0.001, Figure 3). The goodness of fit test, multicollinearity test, sensitivity analysis and prediction ability evaluation of logistic regression analysis model in this study all show that the model has good prediction efficiency (Supplement Tables 1–4). In addition, to further evaluate the association between HSI and prognosis in EC patients, we conducted subgroup analysis according to stage, pathological grade, pathological type, muscular invasion, and lymph node metastasis, and the study results showed that HSI and NAFLD were not significantly correlated with these indicators (Supplement Table 5).
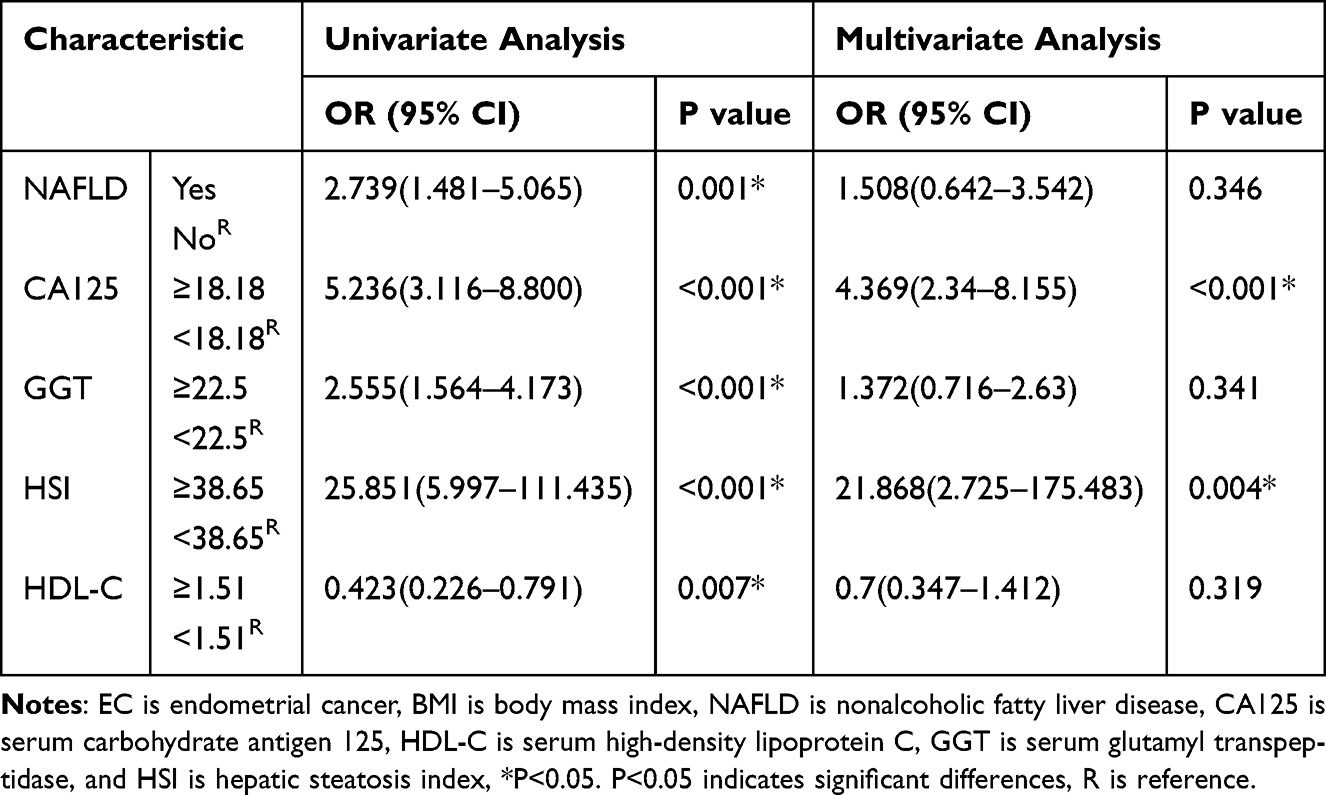 |
Table 2 Univariate and Multivariate Logistics Analysis of Independent Risk Factors for Endometrial Cancer |
 |
Figure 2 The ROC curve. Notes: CA125 is serum carbohydrate antigen 125; GGT is serum glutamyl transpeptidase; HDL-C is serum high-density lipoprotein C; HSI is hepatic steatosis index. (a) The ROC curve for CA125; (b) The ROC curve for GGT; (c) The ROC curve for HDL-C; (d) The ROC curve for HSI. The cutoff values for these indicators were identified. P<0.05 indicates significant differences. |
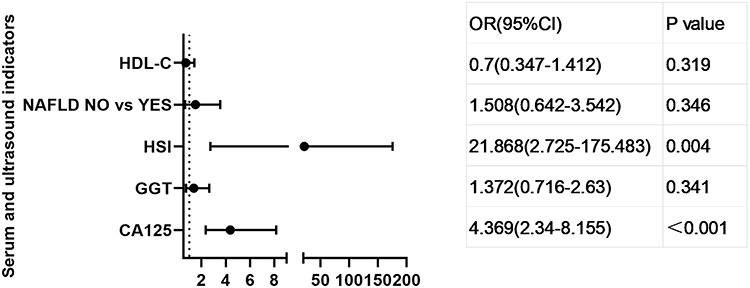 |
Figure 3 Multivariate Logistics regression forest diagram of EC and NC. Notes: CA125 is serum carbohydrate antigen 125; GGT is serum glutamyl transpeptidase; HDL-C is serum high-density lipoprotein C; HSI is hepatic steatosis index. P<0.05 indicates significant differences. |
Discussion
This study aims to elucidate the relationship between NAFLD, HSI and EC. A review of the data of patients diagnosed with benign EC and endometrial lesions in Mindong Hospital, Ningde City, Fujian Province over the past 6 years, non-parametric analysis, ROC curve, univariate and multivariate logistic analysis data showed that women with NAFLD and the higher the HSI, the more likely they were to have EC, and HSI may be an independent risk factor for EC. With the accelerated pace of life and work, high-calorie diet, lack of exercise and other factors, NAFLD is the most common chronic liver disease in the world and has become a serious public health problem worldwide.22 This risk factor continues to increase the prevalence of EC. Although some studies have shown an association between NAFLD and extrahepatic malignancies,15 this study provides an easier way to demonstrate this association by examining the association between HSI and EC. Therefore, raising awareness of NAFLD and EC is essential for the development of EC prevention interventions.
Non-alcoholic fatty liver disease (NAFLD) is a hepatic component of diseases associated with metabolic dysfunction and was first proposed by Ludwig et al in 1980.23 NAFLD is a continuum of disease ranging from more than 5% steatosis with or without mild inflammation (non-alcoholic fatty liver disease) to non-alcoholic steatohepatitis (NASH) in the absence of excessive alcohol consumption (≥30g/day for men and ≥20g/day for women) or other chronic liver disease. NAFLD is currently the most common cause of chronic liver disease worldwide, with a global prevalence of up to 25–30%.24 The data from this study suggest that NAFLD is significantly associated with EC, and previous studies have shown that NAFLD itself is an independent cancer risk factor and is not associated with metabolic disorders such as obesity and type 2 diabetes in NAFLD.25 NAFLD is undoubtedly a global public health problem, and the gold standard for diagnosing NAFLD is liver biopsy. However, its invasive nature and high cost make it difficult to perform routinely in the general population. The Hepatic Steatosis Index (HSI), an indicator derived from standard laboratory tests and anthropometric parameters, is a non-invasive, simple, effective and well-performing screening tool for NAFLD.20 It is obtained by fitting readily available serum alanine aminotransferase (ALT)/aspartate aminotransferase (AST) ratios, body mass index (BMI) and diabetes factors to multiple regression models. The HSI has a sensitivity of up to 93% for excluding NAFLD and a specificity of 92% for detecting NAFLD.21 Overall, the agreement between the HSI and the diagnosis of NAFLD was good,15 but the cut-off value of the HSI in this study was different from the conventional diagnosis of NAFLD. Previous studies have shown that HSI>36 can detect NAFLD by ultrasound,25 and in this study, the prevalence of EC increased with HSI>38.65, which could not exclude the association of single-centre limited studies and differences between northern and southern populations.
However, the mechanism by which NAFLD contributes to endometrial cancer is not well understood. Studies have shown that NAFLD has chronic metabolic inflammation and insulin resistance, and excess fat leads to metabolic imbalance in redox homeostasis and immune dysregulation, resulting in a chronic pro-inflammatory environment that provides tumour cells with a microenvironment for tumour cell proliferation, replication, angiogenesis, invasion and metastasis, thereby promoting tumour initiation and development.17,26,27 In our study, elevated HSI consistently showed a significant correlation with EC in both univariate and multivariate analyses. Therefore, elevated HSI and NAFLD may increase the risk of EC.
In recent years, the management of gynaecological cancers, particularly endometrial and ovarian cancers, has undergone changes based on developments in tumour biology and inheritance patterns, as well as the emergence of the fragility index (a predictor of overall and major complications after EC surgery and a tool to assist clinicians in perioperative management).28,29 If HSI, EC molecular typing and fragility index can be combined to screen, correctly evaluate and diagnose EC, evaluate the complexity of surgical methods, predictability of postoperative complications, prognostic risk stratification, and formulate postoperative adjuvant treatment strategies, it will form a standardised EC management. It has important guiding significance for the screening, evaluation, diagnosis, treatment and prognosis of EC patients.
CA125 is found in the endothelial and mesothelial cells of the female reproductive system and, when stimulated by inflammation or damaged by tumour cells, is released into the blood where it is highly expressed. Therefore, serum CA125 is likely to be elevated in patients with tumour lesions. Previous studies have shown that CA125 is closely associated with the occurrence and development of EC. In agreement with previous studies, our results suggest that CA125 is a high risk factor for the development of EC.30 However, as CA125 can be significantly elevated in patients with inflammation31 and other tumours,32–34 it is not specific. Therefore, in this study, HSI and CA125 were combined for a comprehensive assessment to screen high-risk groups for EC.
This study has several limitations. Firstly, it was a cross-sectional study without causal arguments, and a large prospective cohort study in the population is needed to demonstrate the risk of EC in HSI and even NAFLD; secondly, the sex hormone level status of the study subjects was not included in this study, and EC includes multiple types and is a heterogeneous disease complex, which does not exclude diseases from the source of standard sex hormones, leading to error. In addition, the vast majority of the study population was from the Ningde region of Fujian Province, which may have introduced selection bias and limited regional power. Nevertheless, the main advantage of this study is the use of a simple, convenient, non-invasive method to show the relationship between elevated HSI/NAFLD and endometrium. To date, only a few studies have reported on the relationship between HSI and EC.
Conclusion
In a cross-sectional study, it was concluded that NAFLD was closely associated with the risk of EC and that elevated HSI was one of the independent risk factors for EC. More attention needs to be paid to women with elevated HSI, lifestyle improvement, active EC monitoring, reduction of EC prevalence and improvement of quality of life. However, multicentre, large-sample prospective studies are needed to further investigate the relationship between the occurrence, development and prognosis of elevated HSI and EC, and to confirm the recommendations for EC screening in women with elevated HSI.
Ethics Approval and Informed Consent
This study was conducted in accordance with the tenets of the Declaration of Helsinki. Informed consent was obtained from all individual participants enrolled in the study. This study was reviewed and approved by the Ethics Committee of Mindong Hospital, Ningde City, affiliated to Fujian Medical University (No: K2024051002).
Funding
This work was supported by National Nature Science Foundation of Fujian Province (Grant no. 2024J011061).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Feng X, Li XC, Yang X, et al. Metabolic syndrome score as an indicator in a predictive nomogram for lymph node metastasis in endometrial cancer. BMC Cancer. 2023;23(1):622. doi:10.1186/s12885-023-11053-4
2. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74(1):12–49. doi:10.3322/caac.21820
3. He S, Xia C, Li H, et al. Cancer profiles in China and comparisons with the USA: a comprehensive analysis in the incidence, mortality, survival, staging, and attribution to risk factors. Sci China Life Sci. 2024;67(1):122–131. doi:10.1007/s11427-023-2423-1
4. Shi J, Kraft P, Rosner BA, et al. Risk prediction models for endometrial cancer: development and validation in an international consortium. J National Cancer Inst. 2023;115(5):552–559. doi:10.1093/jnci/djad014
5. Sobel M, Simpson AN, Ferguson SE. Endometrial cancer. CMAJ. 2021;193(36):E1423–E1423. doi:10.1503/cmaj.202731
6. Deng L, Liang H, Han Y. Corrigendum: Cyclooxygenase-2 and β-catenin as potential diagnostic and prognostic markers in endometrial cancer. Front Oncol. 2020;10:582704. doi:10.3389/fonc.2020.582704
7. O’Flynn H, Ryan NAJ, Narine N, Shelton D, Rana D, Crosbie EJ. Diagnostic accuracy of cytology for the detection of endometrial cancer in urine and vaginal samples. Nat Commun. 2021;12(1):952. doi:10.1038/s41467-021-21257-6
8. Barr CE, Njoku K, Jones ER, Crosbie EJ. Serum CA125 and HE4 as biomarkers for the detection of endometrial cancer and associated high-risk features. Diagnostics. 2022;12(11):2834. doi:10.3390/diagnostics12112834
9. Behrouzi R, Barr CE, Crosbie EJ. HE4 as a Biomarker for Endometrial Cancer. Cancers. 2021;13(19):4764. doi:10.3390/cancers13194764
10. King L, Gajarawala S, McCrary MD. Endometrial cancer and obesity. JAAPA. 2023;36(1):28–31. doi:10.1097/01.jaa.0000902884.01725.a3
11. Saed L, Varse F, Baradaran H, et al. The effect of diabetes on the risk of endometrial Cancer: an updated a systematic review and meta-analysis. BMC Cancer. 2019;19(1):19. doi:10.1186/s12885-019-5748-4
12. Yang X, Wang J, Adur MK. The role of metabolic syndrome in endometrial cancer: a review. Front Oncol. 2019;9:9. doi:10.3389/fonc.2019.00744
13. Frandsen C, Gottschau M, Nøhr B, et al. Polycystic ovary syndrome and endometrial cancer risk: results from a nationwide cohort study. Am J Epidemiol. 2024;193(10):1399–1406. doi:10.1093/aje/kwae061
14. Kyrgiou M, Kalliala I, Markozannes G, et al. Adiposity and cancer at major anatomical sites: umbrella review of the literature. BMJ. 2017:j477. doi:10.1136/bmj.j477
15. Mantovani A, Petracca G, Beatrice G, et al. Non-alcoholic fatty liver disease and increased risk of incident extrahepatic cancers: a meta-analysis of observational cohort studies. Gut. 2022;71(4):778–788. doi:10.1136/gutjnl-2021-324191
16. Li L, Liu DW, Yan HY, Wang ZY, Zhao SH, Wang B. Obesity is an independent risk factor for non-alcoholic fatty liver disease: evidence from a meta-analysis of 21 cohort studies. Obesity Rev. 2016;17(6):510–519. doi:10.1111/obr.12407
17. Thomas JA, Kendall BJ, El-Serag HB, Thrift AP, Macdonald GA. Hepatocellular and extrahepatic cancer risk in people with non-alcoholic fatty liver disease. Lancet Gastroenterol Hepatol. 2024;9(2):159–169. doi:10.1016/S2468-1253(23)00275-3
18. Khov N, Sharma A, Riley T. Bedside ultrasound in the diagnosis of nonalcoholic fatty liver disease. World J Gastroenterol. 2014;20(22):6821–6825. doi:10.3748/wjg.v20.i22.6821
19. Riley TR, Mendoza A, Bruno MA. Bedside ultrasound can predict nonalcoholic fatty liver disease in the hands of clinicians using a prototype image. Dig Dis Sci. 2006;51(5):982–985. doi:10.1007/s10620-006-9343-6
20. Lee JH, Kim D, Kim HJ, et al. Hepatic steatosis index: a simple screening tool reflecting nonalcoholic fatty liver disease. Dig Liver Dis. 2010;42(7):503–508. doi:10.1016/j.dld.2009.08.002
21. Riemann A, Blaschke M, Jauho-Ghadimi A, Siggelkow H, Gollisch KSC. Metformin improves the hepatic steatosis index in non-obese patients with polycystic ovary syndrome. J Clin Med. 2022;11(15):4294. doi:10.3390/jcm11154294
22. Zhang S, Gu Y, Bian S, et al. Soft drink consumption and risk of nonalcoholic fatty liver disease: results from the Tianjin Chronic Low-Grade Systemic Inflammation and Health (TCLSIH) cohort study. Am J Clin Nutr. 2021;113(5):1265–1274. doi:10.1093/ajcn/nqaa380
23. Ludwig J, Viggiano TR, McGill DB, Oh BJ. Nonalcoholic steatohepatitis: mayo Clinic experiences with a hitherto unnamed disease. Mayo Clin Proc. 1980;55(7):434–438. doi:10.1016/S0025-6196(24)00530-5
24. Powell EE, Wong VWS, Rinella M. Non-alcoholic fatty liver disease. Lancet. 2021;397(10290):2212–2224. doi:10.1016/S0140-6736(20)32511-3
25. Jones GS, Alvarez CS, Graubard BI, McGlynn KA. Agreement between the prevalence of nonalcoholic fatty liver disease determined by transient elastography and fatty liver indices. Clin Gastroenterol Hepatol. 2022;20(1):227–229.e2. doi:10.1016/j.cgh.2020.11.028
26. Park JH, Choi IS, Han KD, Park H, Kim KH, Kim JS. Association between fatty liver index and risk of breast cancer: a nationwide population-based study. Clin Breast Cancer. 2020;20(4):e450–e457. doi:10.1016/j.clbc.2020.02.004
27. Damba T, Bourgonje AR, Abdulle AE, et al. Oxidative stress is associated with suspected non‐alcoholic fatty liver disease and all‐cause mortality in the general population. Liver Int. 2020;40(9):2148–2159. doi:10.1111/liv.14562
28. Di Donato V, Di Pinto A, Giannini A, et al. Modified fragility index and surgical complexity score are able to predict postoperative morbidity and mortality after cytoreductive surgery for advanced ovarian cancer. Gynecol Oncol. 2021;161(1):4–10. doi:10.1016/j.ygyno.2020.08.022
29. D’Oria O, Giannini A, Besharat AR, Caserta D. Management of endometrial cancer: molecular identikit and tailored therapeutic approach. Clin Exp Obstet Gynecol. 2023;50(10):210. doi:10.31083/j.ceog5010210
30. Hashiguchi Y, Yamauchi M, Kasai M, et al. 409 Serum Ca125 in patients with endometrial cancer. Int J Gynecol Cancer. 2019;29:170. doi:10.1136/ijgc-2019-IGCS.409
31. Bulska-Będkowska W, Chełmecka E, Owczarek A, et al. CA125 as a marker of heart failure in the older women: a population-based analysis. J Clin Med. 2019;8(5):607. doi:10.3390/jcm8050607
32. Funston G, Hamilton W, Abel G, Crosbie E, Rous B, Walter F. The diagnostic performance of CA125 for the detection of ovarian and non-ovarian cancer in primary care: a population-based cohort study. PLoS Med. 2020;17. doi:10.1371/journal.pmed.1003295
33. Xiao M, Zhang Z, Yu X, Fan Y, Chen X. Value of TCT combined with HPV and CA125 in early cervical cancer screening in a medical examination population. Cell mol Biol. 2022;68(9):160–164. doi:10.14715/cmb/2022.68.9.25
34. Zhou S, Wang Z, Li M, Wu L. Elevated preoperative serum CA125 predicts larger tumor diameter in patients with hepatocellular carcinoma and low AFP levels. Biomed Res Int. 2019;2019:1–7. doi:10.1155/2019/6959637
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.