Back to Journals » Nature and Science of Sleep » Volume 14
Association Between Habitual Night Sleep Duration and Predicted 10-Year Cardiovascular Risk by Sex Among Young and Middle-Aged Adults
Authors He J ![]() , Wang Y, Zhang L, Li C, Qi X
, Wang Y, Zhang L, Li C, Qi X ![]() , Wang J, Guo P, Chen S, Niu Y
, Wang J, Guo P, Chen S, Niu Y ![]() , Liu F, Zhang R, Li Q, Ma S, Zhang M, Hong C, Zhang M
, Liu F, Zhang R, Li Q, Ma S, Zhang M, Hong C, Zhang M ![]()
Received 7 February 2022
Accepted for publication 4 May 2022
Published 11 May 2022 Volume 2022:14 Pages 911—926
DOI https://doi.org/10.2147/NSS.S359611
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Jiangshan He,1 Yuxue Wang,1 Li Zhang,2 Chunjun Li,3 Xin Qi,3 Jianxiong Wang,4 Pei Guo,1 Shuo Chen,5 Yujie Niu,6,7 Feng Liu,5 Rong Zhang,6,7 Qiang Li,5 Shitao Ma,6,7 Mianzhi Zhang,8,9 Chenglin Hong,10 Minying Zhang1
1School of Medicine, Nankai University, Tianjin, People’s Republic of China; 2Tianjin First Central Hospital, Tianjin, People’s Republic of China; 3Tianjin Union Medical Center, Tianjin, People’s Republic of China; 4Graduate School of Tianjin Medical University, Tianjin, People’s Republic of China; 5Beijing Physical Examination Center, Beijing, People’s Republic of China; 6Hebei Key Laboratory of Environment and Human Health, Shijiazhuang, People’s Republic of China; 7Department of Occupational Health and Environmental Health, Hebei Medical University, Shijiazhuang, People’s Republic of China; 8Dongfang Hospital, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 9Tianjin Academy of Traditional Chinese Medicine Affiliated Hospital, Tianjin, People’s Republic of China; 10Department of Social Welfare, School of Public Affairs, University of California, Los Angeles, CA, USA
Correspondence: Minying Zhang, School of Medicine, Nankai University, 94 Weijin Road, Nankai District, Tianjin, 300071, People’s Republic of China, Tel +86-13752516700, Fax +86-22-23502554, Email [email protected]
Purpose: We hypothesize the association between sleep duration and cardiovascular disease (CVD) risk varies with age category; however, evidence for the relationship between sleep duration and CVD risk among young and middle-aged adults remains scarce. This research aims to assess the association between night sleep duration and cardiovascular risk by sex among young and middle-aged Chinese adults.
Patients and Methods: We used the baseline data of a cohort of adults for physical examination by stratified cluster sampling. The Framingham risk score and the Pittsburgh Sleep Quality Index were used to measure CVD risk and sleep duration, respectively. Demographic characteristics, lifestyle factors, height, weight, total cholesterol (TC), and high-density lipoprotein cholesterol (HDL-C) were collected. We performed multiple logistic regressions to examine the association between night sleep duration and the predicted cardiovascular risk.
Results: We included 27,547 participants aged 18– 64 years free of CVD, cerebral stroke, and not taking lipid-lowering agents. Overall, 12.7%, and 20.4% were at medium and high predicted CVD risk, respectively; 11.9% and 12.3% reported short and long sleep, respectively. Short sleep was independently associated with 23% (95% CI: 1.08– 1.40) increased odds of medium-to-high CVD risk and 26% (95% CI: 1.11– 1.45) increased odds of high CVD risk among females. Whereas long sleep was independently associated with 17% (95% CI: 0.71– 0.98) decreased odds of medium-to-high CVD risk among males.
Conclusion: Among young and middle-aged adults, long sleep was associated with decreased odds of CVD risk in males, whereas short sleep was associated with increased odds of cardiovascular risk in females.
Keywords: predicted 10-year CVD risk, sleep duration, Framingham risk score, young and middle-aged population
Introduction
Normal sleep is essential for maintaining human health. Seven to nine hours of sleep per day is recommended for young and middle-aged adults by the American National Sleep Foundation.1 In modern society, sleep deprivation has become an important but widely ignored health problem. More than one-third of Chinese people have sleep problems, with the majority having less than seven hours of sleep per night.2
Previous studies have suggested that both short sleep and long sleep increases BMI, decrease insulin sensitivity, and induce the production of various inflammatory cytokines, thus affecting the body’s glucose and lipid metabolic homeostasis, therefore induces or accelerates the onset and development of disease.3–5 To data, numerous prospective studies have demonstrated a U-shaped relationship between sleep duration and all-cause mortality and mortality from CVD, with the lowest point at approximately 7–9 hours of sleep per night.5–9 A systematic review of prospective cohort studies showed that the risk of CVD increased by 6% (RR=1.06; 95% CI: 1.03–1.08) for each hour of sleep reduction when sleep duration was <7 hours per day and by 12% (RR=1.12; 95% CI: 1.08–1.16) for each hour of sleep increase when sleep duration was >7 hours per day.9 Although the current evidence consistently suggests that both short and long sleep can elevate the risk of CVD, the studies from which this evidence derived all included older people over 65 years of age. However, factors influencing sleep and CVD risk may differ between older and young and middle-aged people. Chronic comorbidity, infirmity and poor general health may be contributors to adverse impact on sleep and CVD among the elderly. Whereas the sleep patterns of the young and middle-aged population have been particularly changed by the rapid development of science, technology and economy in modern society.10,11 A growing number of young and middle-aged people are shortening their sleep duration in response to prolonged working hours and the introduction of the Internet and smart phone, which enable living “around the clock” and resulting in an elevated CVD risk among this sub-population. Young and middle-aged adults, accounting for the largest proportion of the total population, have a lower prevalence of CVD than their old counterparts, suggesting that predicting cardiovascular risk and exploring the association between sleep duration and the predicted CVD risk in this population may yield great public health and clinical benefit.
Cardiovascular disease risk prediction can be used to estimate cardiovascular risk of individuals without CVD, which not only contributes to early identification of high-risk individuals but also prompts the formulation of public health strategies and the optimization of health resources. Previous studies on the impact of sleep duration on cardiovascular disease were mostly based on cohort data, research on sleep duration and predicted cardiovascular disease risk is still lacking.
Due to the impact of specific culture and region, sleep patterns vary in different countries,12 and sleep duration varies across race and age,13,14 both of which have impact on the association between sleep duration and the predicted 10-year CVD risk. Previous research on the association of sleep duration with the predicted CVD risk has only been conducted in the United States, Korea, Iran, Japan, and Chinese menopausal women.15–18 The studies mentioned above were all conducted in populations including older populations. Though there is considerable evidence of the association between sleep duration and CVD among middle-aged and old populations, the relationship between sleep duration and the predicted 10-year CVD risk among young and middle-aged adults has been rarely explored. The present research aims to examine the relationship between sleep duration and the predicted 10-year cardiovascular risk by sex among a large sample of Chinese young and middle-aged adults free of CVD, cerebral stroke, and not taking lipid-lowering agents.
Materials and Methods
Study Design and Population
We analyzed part of the baseline data of Medical Examination-based Cohort in the Beijing-Tianjin-Hebei Region (MEC-BTH), a National Key R&D Program of China. A multi-stage stratified cluster sampling among attendees at medical examination centers was used in Beijing, and its two neighboring areas-Tianjin municipality and Hebei province, China from July 2017 to December 2020. (For details of the sampling method, see Supplementary Material) Individuals aged 18 years or older and voluntarily participated in the survey and signed the informed consent were included. Individuals who were pregnant, had serious physical and mental illnesses, or were in a state of physical infection such as fever or diarrhea were excluded. Individuals were additionally excluded from the current analyses if they 1) aged 65 years or older; 2) were ever diagnosed with cardiovascular diseases or stroke; 3) were taking lipid-lowering agents.
Measurement of Sleep Duration
We used the Pittsburgh Sleep Quality Index (PSQI)19 and extracted items related to sleep duration, sleep quality, sleep latency, habitual sleep efficiency, sleep disturbance and use of sleep medication. The PSQI has shown to have high validity and reliability with adult respondents.20,21 Subjects were asked, “During the past month, what time have you usually gone to bed at night?”, “During the past month, how long has it usually taken you to fall asleep each night?” and “During the past month, what time have you usually gotten up in the morning?”. Based on the answers, we calculated the subjects’ average daily night sleep duration, then categorized it into short (≤ 6 hours per night), optimal (7–8 hours per night), and long sleep duration (≥ 9 hours per night).22
Clinical and Biochemical Measurements
Clinical and biochemical measurements were performed by professional medical staff of the selected centers. Participants were instructed to fast for ≥ 12 hours before blood sampling the following morning. Sampled blood was immediately sent to the medical testing center, and TC and HDL-C were measured using the Hitachi 7600 automated analyzer (Hitachi, Inc., Tokyo, Japan). Blood pressure was measured using a sphygmomanometer (Kenz-AC OSC, Japan) in a sitting position for the right arm after resting for at least 5 minutes. Two readings were taken, 2 minutes apart, and a third measurement was made if the first two differed by more than 5 mm Hg. The average of the two or three readings was recorded. Hypertension was defined as systolic blood pressure (SBP) ≥ 140 mmHg and/or diastolic blood pressure (DBP) ≥ 90 mmHg or self-reported previous diagnosis of hypertension.23 Height (0.1 cm precision), and weight (0.1 kg precision) was measured using the same device (GL-310, Seoul, Korea). Body mass index (BMI) was expressed as body weight (kg) divided by squared body height (m2). Obesity was defined as BMI ≥ 28 kg/m2.24
Predicted 10-Year Cardiovascular Risk by Framingham Risk Score
We assessed the participants’ 10-year CVD risk using Framingham Risk Score (FRS),25 which was calculated based on the participants’ age, sex, TC, HDL-C, smoking, treated/untreated systolic blood pressure, and diabetic status. The Framingham risk groups were defined as low risk (FRS < 10%), medium risk (FRS = 10–20%), and high risk (FRS > 20%).26
Collection and Definition of Other Variables
Trained investigators conducted a standard questionnaire interview to collect data on sociodemographic characteristics (age, sex, education level, marital status, and occupation), personal history of chronic diseases (hypertension, diabetes, CVD, stroke, hyperlipidaemia, and the respective medication), and lifestyle factors. Participants who reported had been smoking for more than half a year were defined as smokers. Those who consumed alcohol at least once a week were considered as alcohol drinkers. Sitting, reclining or lying down longer than 6 hours per day while awake was defined as being sedentary. Definitions of other lifestyle factors were described in the Supplementary File. If a positive chronic disease history was reported, data on the time of diagnosis and respective medication were further collected. We assessed each participant’s psychological health using The Kessler Psychological Distress Scale (K10).
Statistical Analysis
Continuous variables distributed normally were presented as mean ± standard deviation (SD) and compared using t-test for two groups, one-way analysis of variance (ANOVA) for more than two groups when homogeneity of variances was met. We used Brown and Forsythe’s test where the homogeneity of variances was violated. Non-normally distributed continuous variables were described using median and quartile and compared using the rank-sum test. Rates or percentages were used to describe categorical variables. We used chi-square test, Fisher’s exact test and rank-based test to compare the differences between groups in terms of rates or percentages. Principal component analysis and maximum variance method were used to perform multivariate logistic regression after rotation. Potential confounding factors adjusted in the regression models included age, sex, education, BMI, SBP, smoking status, alcohol consumption, previous diagnosis of diabetes and hypertension, TC, HDL-C, usage of antihypertensive agents, physical exercise, sedentary time, sleep quality and usage of sleep medication. Odds ratio (OR) and 95% confidence interval (CI) were estimated for predicted 10-year CVD risk by sleep duration. Two-sided p <0.05 was considered statistically significant. The Epidata 3.0 and SPSS 23.0 software for Windows (IBM, Armonk, NY, USA) were used to input and clean and analyze the data.
Results
A total of 35,176 adults completed the interview and medical examination. After excluding 3588 aged 65 years or older, 1962 with cardiovascular disease, 679 for currently taking cholesterol-lowering agents, 323 for missing biochemical measurements, 463 for missing blood pressure measurement, 5 for missing sleep duration, 609 for missing other needed variables, 1962 with CVD and 679 for currently taking cholesterol-lowering agents, 27,547 participants aged 18–64 years were included in the analysis (Figure 1). The median age of the subjects was 41 (IQR: 34–51) years, and more than half (52.6%) of the participants were males. The vast majority of participants were of Han ethnicity (95.9%) and 84.7% were in a current marriage. Almost eighty percent (79.1%) had college or above education, and 69.1% were professionals. The proportion of participants who smoked and drank were 20.5% and 26.0%, respectively. Almost seventy percent (66.7%) exercised, and 49.1% reported more than 6 hours of sedentary time per day. In addition, the proportion of the participants with positive family history of CVD was 14.6%, and the prevalence of obesity, hypertension and diabetes was 16.0%, 10.7%, and 3.4%, respectively. The majority (89.3%) of participants reported excellent or good sleep quality, and 97.6% were assessed with good mental health (Table 1).
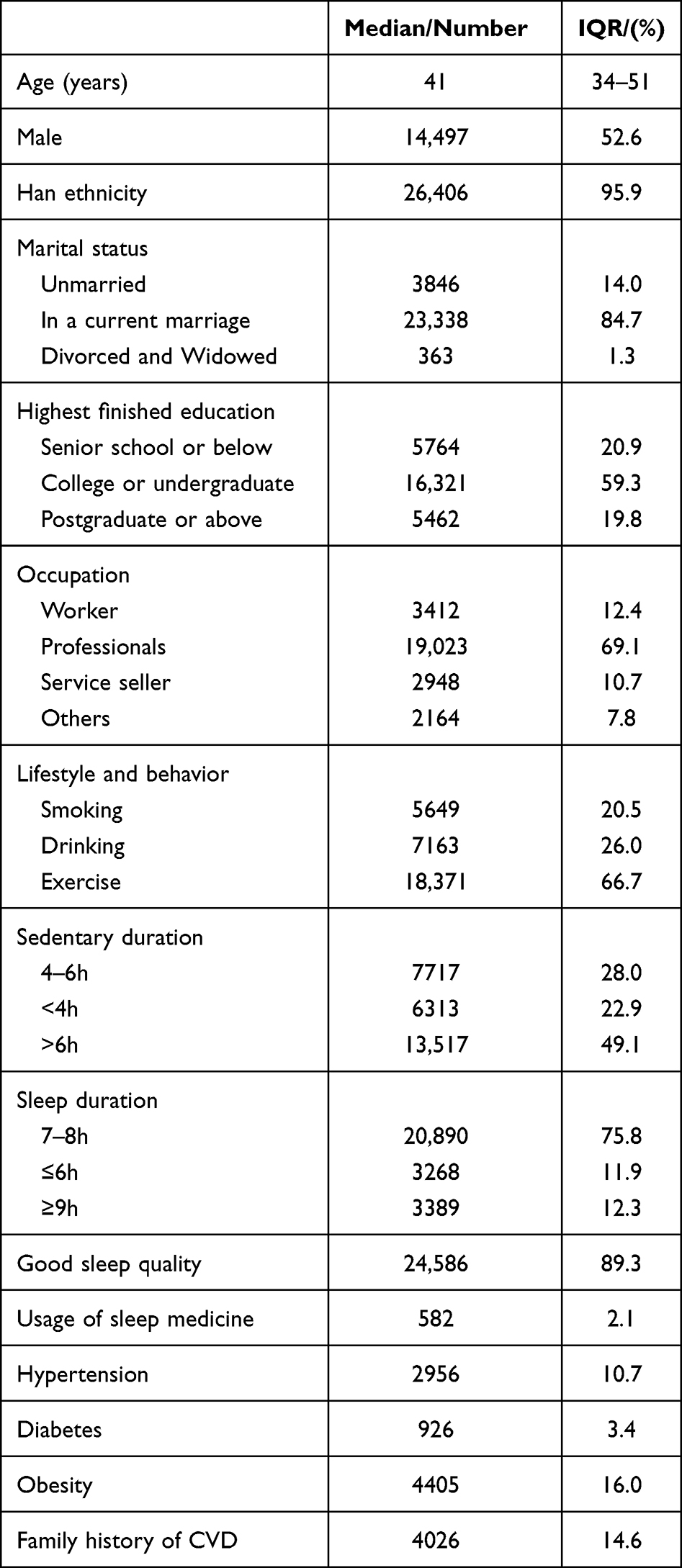 |
Table 1 Baseline Characteristics of the Participants (n = 27,547) |
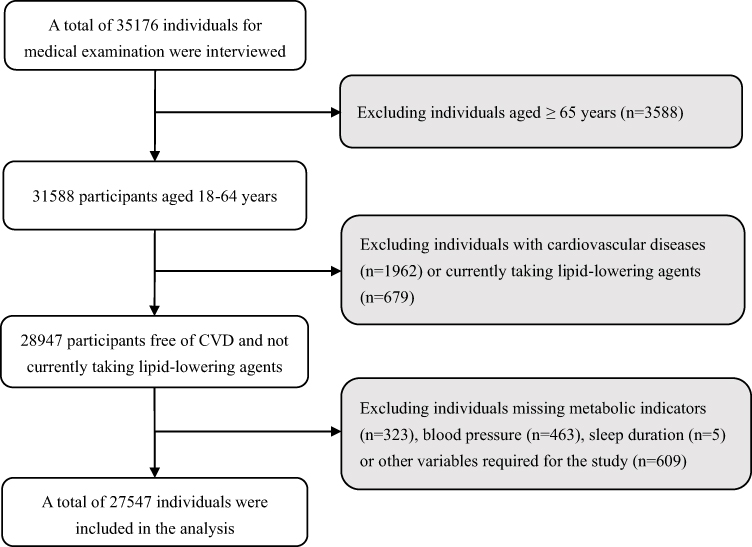 |
Figure 1 Flowchart of study population selection. |
The 10-year CVD risk score ranged from 0% to 31%, with a median of 3.9% (IQR: 2.0–8.6%). Participants at low, medium, and high predicted 10-year CVD risk were 66.9%, 12.7%, and 20.4%, respectively.
Compared with the low predicted 10-year CVD risk, the high predicted 10-year CVD risk was associated with older age, female sex, lower education, smoking, alcohol consumption, doing no exercise, shorter sedentary duration, higher SBP, TC, HDL-C and BMI, hypertension, diabetes and positive family history of CVD; the medium predicted 10-year CVD risk was associated with older age, male sex, lower education, smoking, alcohol consumption, shorter sedentary duration, higher SBP, TC and BMI, lower HDL-C, obesity, hypertension, and diabetes (Table 2).
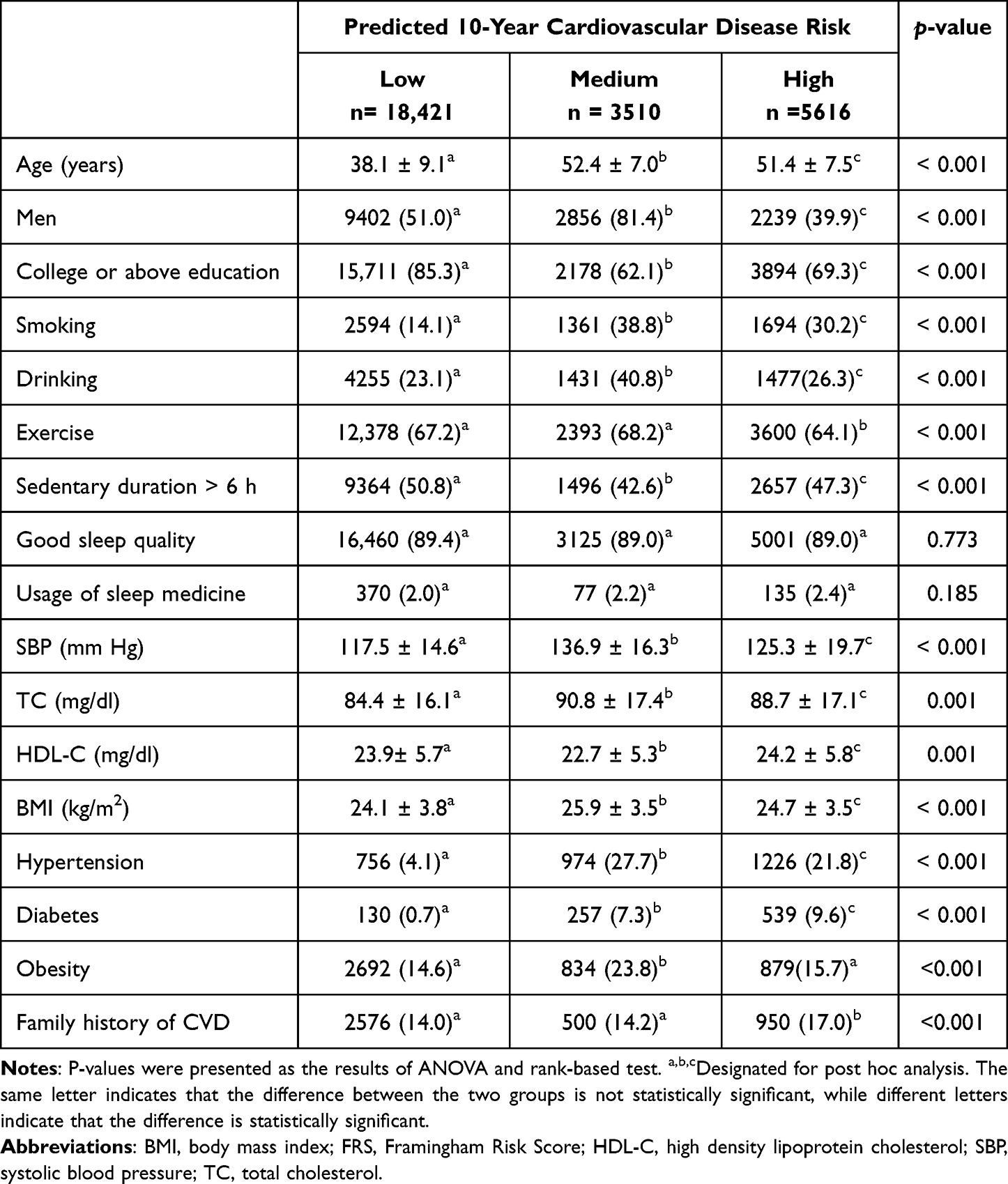 |
Table 2 Mean (Standard Deviation) or Number (Percentage) of Selected Variables Among Adults Aged 18 to 65 Years by Predicted 10-Year Cardiovascular Disease Risk |
Subjects reported short, optimal and long sleep duration accounted for 11.9%, 75.8%, and 12.3%, respectively (Table 3). Compared with optimal sleep duration, short sleep was positively associated with CVD risk factors including age, male sex, lower education, smoking, alcohol consumption, doing no exercise, being sedentary > 6 h, bad sleep quality, usage of sleep medicine, higher SBP and TC, lower HDL-C, higher BMI, previous diagnosis of hypertension or diabetes, obesity, positive family history of CVD and higher FRS; long sleep duration was positively associated with female sex and good sleep quality, but negatively associated with age, education level, smoking alcohol consumption, long sedentary time, TC, BMI, previous diagnosis of hypertension or diabetes, positive family history of CVD and lower FRS. Short sleepers had the highest mean of SBP, TC and BMI, and the lowest mean of HDL-C. Prevalence of hypertension, diabetes and obesity was higher in short sleepers than in optimal sleepers and long sleepers (p < 0.001). But among participants reported long sleep duration, the prevalence of hypertension and diabetes was lower than that of optimal sleepers, while the difference in the prevalence of obesity between long sleepers and optimal sleepers was not statistically significant. The proportion of both medium-to-high and high CVD risk was higher among short sleepers than among optimal and long sleepers. Among long sleepers, the proportion of medium and medium-to-high CVD risk was lower than that of optimal and short sleepers.
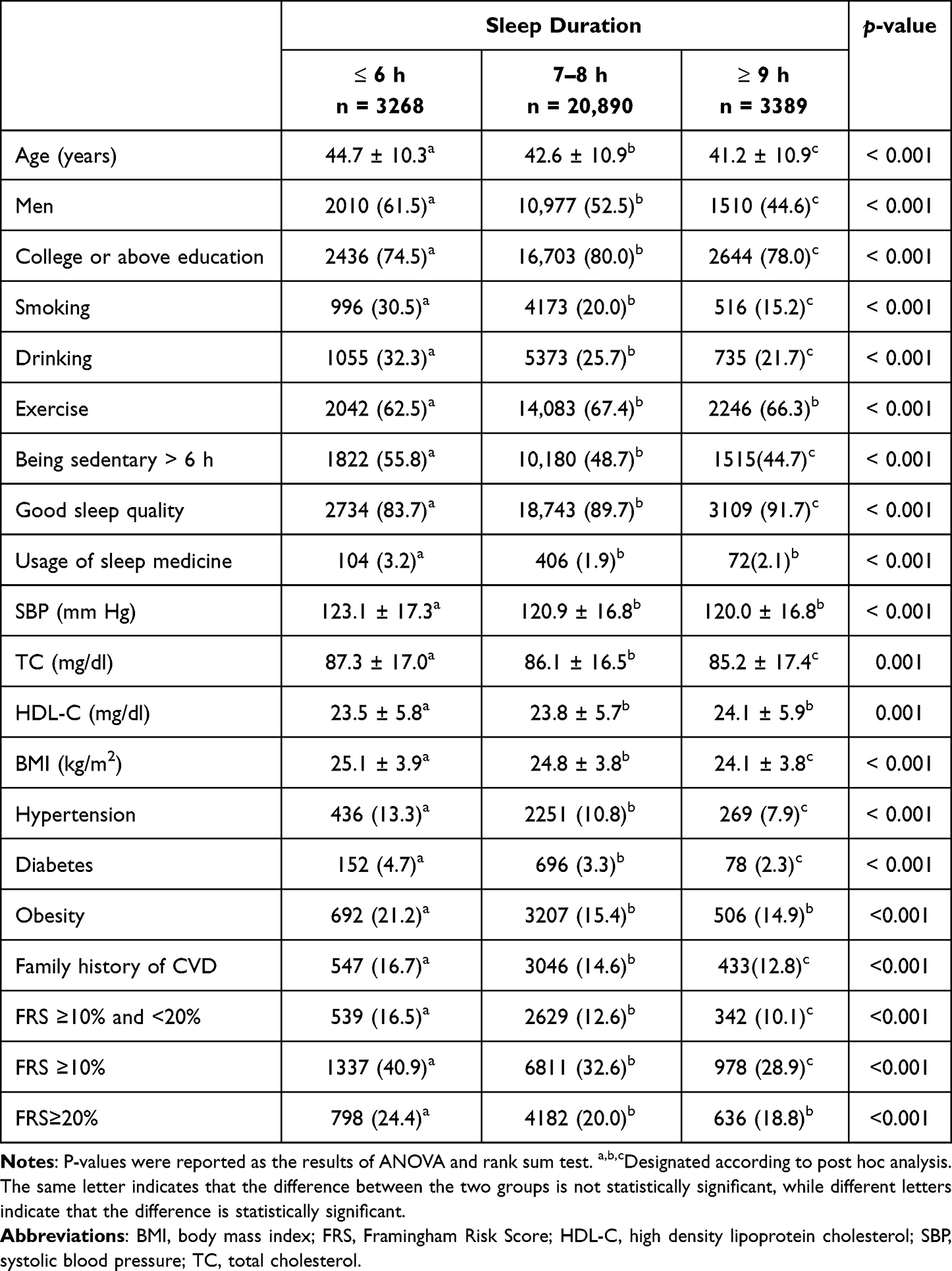 |
Table 3 Mean (Standard Deviation) or Number (Percentage) of Conventional Risk Factors for Cardiovascular Disease Among Adults Aged 18 to 65 Years by Sleep Duration |
As shown in Tables 4 and 5, among the total population, short sleep was significantly associated with increased odds of medium-to-high and high predicted 10-year CVD risk (OR=1.19; 95% CI: 1.08–1.30; OR=1.21; 95% CI: 1.10–1.34) in the fully adjusted regression model (adjusted for age, sex, education level, SBP, TC, HDL-C, smoking, alcohol consumption, sedentary time, physical exercise, BMI, sleep quality, hypertension, diabetes and family history of CVD), while the associations of long sleep with the medium-to-high and high-predicted 10-year CVD risk were not statistically significant in the fully adjusted model, though both odds were less than 1.00 (Figure 2).
 |
Table 4 Odds Ratios of Sleep Duration for Predicted 10-Year Cardiovascular Risk Among Adults Aged 18–65 Years |
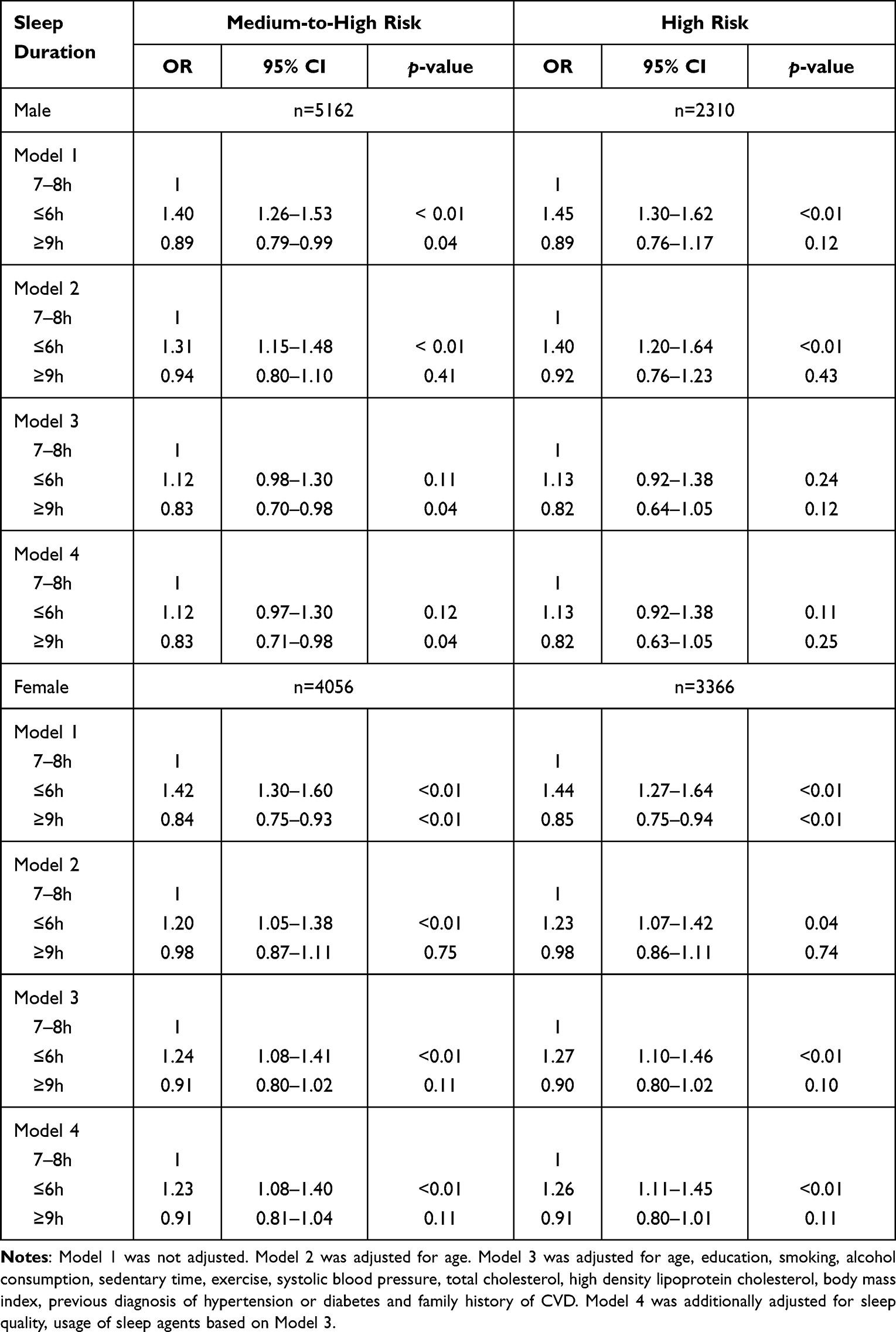 |
Table 5 Odds Ratios of Sleep Duration for Predicted 10-Year Cardiovascular Risk by Sex Among Adults Aged 18–65 Years |
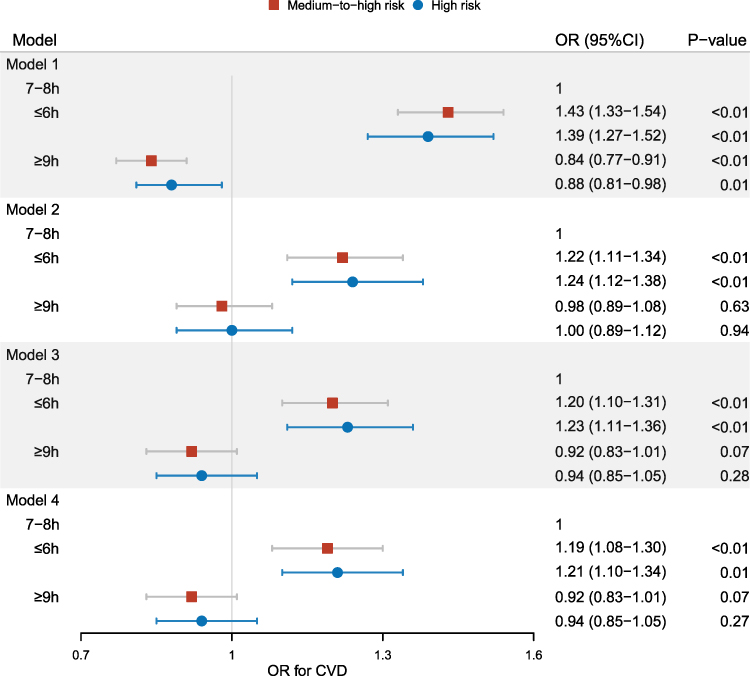 |
Figure 2 Correlations between sleep duration and predicted 10-year CVD risk among the participants aged 18–64 years. Model 1 was not adjusted. Model 2 was adjusted for age and gender (except gender-specific models). Model 3 was adjusted for age, gender (except gender-specific models), education level, systolic blood pressure, total cholesterol, high density lipoprotein cholesterol, smoking, drinking, sedentary duration, exercise, body mass index, history of hypertension, diabetes and family history of CVD. Model 4 was adjusted for sleep quality, usage of sleep agents and all variables in Model 3. |
Sex subgroup analysis demonstrated that short sleep was associated with elevated odds of medium-to-high and high predicted 10-year CVD risk among females (OR=1.23; 95% CI: 1.08–1.40; OR=1.26; 95% CI: 1.11–1.45) and was not associated with predicted 10-year CVD risk among males in the fully adjusted regression models (see in Figures 3 and 4). Though the fully adjusted associations (Model 4) between short sleep and medium-to-high and high cardiovascular risk were not statistically significant among males, the odds were greater than 1.00 and numerically consistent with that among females. In the fully adjusted regression models, long sleep was associated with decreased odds of medium-to-high predicted 10-year cardiovascular risk among males (OR=0.83; 95% CI: 0.71–0.98). Though long sleep was associated with decreased odds of high cardiovascular risk among females in the unadjusted model, the associations became statistically non-significant after adjusting for age (Model 2) and all selected potential confounders (Model 4).
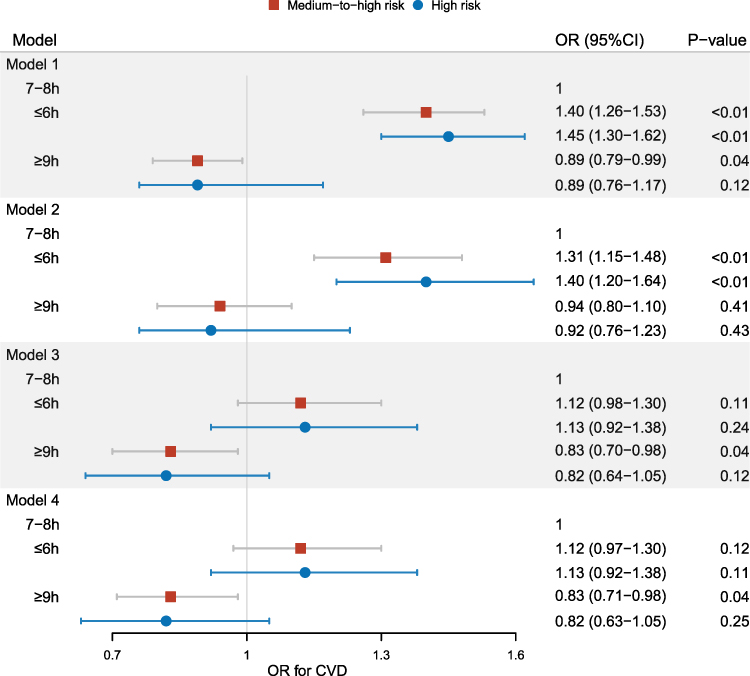 |
Figure 3 Correlations between sleep duration and predicted 10-year CVD risk in men aged 18–64 years. Model 1 was not adjusted. Model 2 was adjusted for age. Model 3 was adjusted for age, education level, systolic blood pressure, total cholesterol, high density lipoprotein cholesterol, smoking, drinking, sedentary duration, exercise, body mass index, history of hypertension, diabetes and family history of CVD. Model 4 was adjusted for sleep quality, usage of sleep agents and all variables in Model 3. |
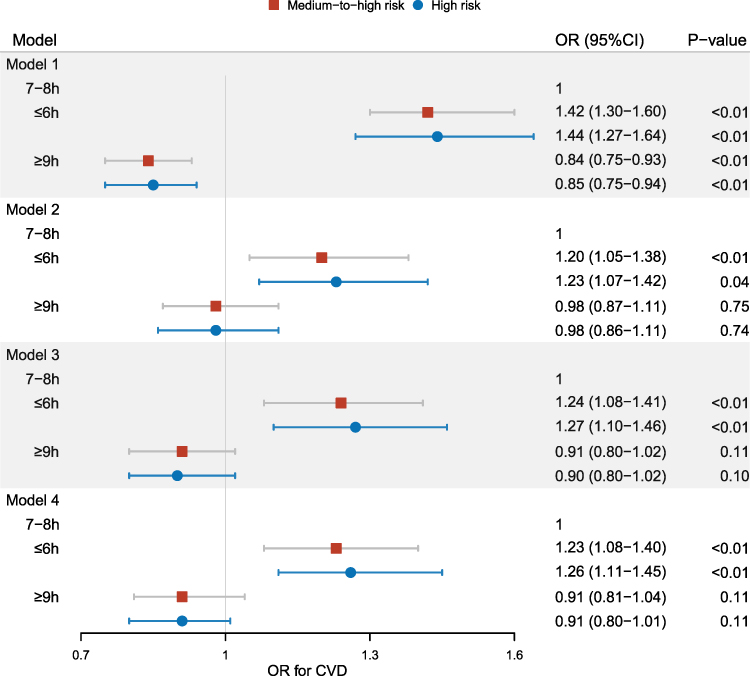 |
Figure 4 Correlations between sleep duration and predicted 10-year CVD risk in women aged 18–64 years. Model 1 was not adjusted. Model 2 was adjusted for age. Model 3 was adjusted for age, education level, systolic blood pressure, total cholesterol, high density lipoprotein cholesterol, smoking, drinking, sedentary duration, exercise, body mass index, history of hypertension, diabetes and family history of CVD. Model 4 was adjusted for sleep quality, usage of sleep agents and all variables in Model 3. |
Discussion
To the best of our knowledge, the current study is the first to identify the protective effect of long sleep on cardiovascular health among young and middle-aged adults. Previous research on this topic has focused on older adults or populations that include older adults. However, compared with the elderly, young and middle-aged adults have sleep patterns more dramatically changed by modern work and lifestyle (long work time and extensive use of social media), resulting in a relatively lower prevalence but a higher risk of CVD. Therefore, predicting cardiovascular risk and examining the association between sleep duration and predicted CVD risk among young and middle-aged adults helps to highlight the need for early interventions on sleep to improve their cardiovascular health. We found 12.7% and 20.4% of the subjects were at medium and high predicted CVD risk, respectively. Compared with optimal sleep duration, short sleep was independently associated with 23% (95% CI: 1.08–1.40) increased odds of medium-to-high CVD risk and 26% (95% CI: 1.11–1.45) increased odds of high CVD risk among females. Whereas long sleep was independently associated with 17% (95% CI: 0.71–0.98) decreased odds of medium-to-high CVD risk among males.
In the present study, long sleep was associated with decreased odds of cardiovascular risk in the total population, males and females in the unadjusted model, but the association was significant only among males after fully adjusting for age and all selected potential confounders. Nevertheless, the odds ratios were all numerically lower than the reference level, suggesting long sleep duration may be associated with decreased cardiovascular risk. The current findings are inconsistent with those of research conducted among populations including the elderly in other countries. Kim et al found that excessive sleep was associated with elevated risk of mortality from CVD in both males (HR: 1.22, 95% CI: 1.09–1.35) and females (HR: 1.29, 95% CI: 1.13–1.47) in a cohort with participants aged 45–75 years.5 Eui Im et al analyzed data of 23,878 people aged 18 and older in the Korean National Health and Nutrition Examination Survey and found that long sleep (≥ 9 h) was also associated with both medium-to-high (OR: 1.142, 95% CI: 1.011–1.322) and high Framingham Cardiovascular Risk Score (OR: 1.276, 95% CI: 1.118–1.457).17 Long sleep duration was found to increase mortality from CVD in both men (HR: 1.58, 95% CI: 1.19–2.12) and women (HR: 2.37, 95% CI: 1.70–3.32) in a cohort of people aged 40 to 79 years.8 All the research mentioned above included participants older than 65 years, whereas we only enrolled adults younger than 65 years. We speculated that the different age span of the study populations might be a key contributor to the inconsistency between their findings and ours. Nevertheless, a cohort conducted in the Netherlands, which included population in a similar age range (aged 20–65 years) to the current research, did not observe an association between long sleep duration and increased risk of CVD,27 which was comparable to our findings.
The inconsistent findings among populations of different age categories indicate that the association between long sleep duration and cardiovascular risk is comprehensive and varied across adults with different age profiles. The positive association of excessive sleep with cardiovascular risk, derived from studies using premature death from cardiovascular disease or the onset of cardiovascular disease as outcome, may be confounded by undiagnosed chronic conditions and unmeasured poor general health in elderly people.28 Therefore, long sleep duration might possibly be a consequence of, rather than a causative risk factor for, unrecognized chronic comorbidity, which could explain the higher risk of mortality, observed in previous research.6,8,29,30 Furthermore, increased sleep fragmentation, changes in cytokine levels (eg, C-Reactive Protein (CRP) and the cytokine IL-6),31 Insufficient physiological challenges and poor general health have all been demonstrated to be associated with long sleep and make it challenging to specify the relationship between sleep duration and adverse health outcomes.28,32 In addition, the associations of long sleep duration with CVD risk may be driven by lack of physical activity as an outcome or impact of infirmity and disease.28 In fact, significant, consistent associations were found between long sleep and age, especially among males, and poorer physical health measured by the SF-36 physical scores in both sexes.28 Therefore, it is reasonable to speculate that the increased cardiovascular risk among old males with long durations of sleep is due to the impact of poor general health and other chronic conditions, which can explain the protective effect of long sleep for CVD risk among young and middle-aged males in the current study. Compared with short or optimal sleepers, long sleepers in the current study were found with lower prevalence of chronic disease (eg, hypertension, diabetes and obesity) and better general health (eg, lower SPB, TC and BMI), reported better sleep quality and shorter sedentary time, which were widely known protective factors of cardiovascular health and may contribute to decreasing the long sleepers’ risk of CVD. The different prevalence of diabetes and hypertension may also be involved in the association between sleep duration and CVD risk. The association between long sleep and decreased odds of high CVD risk among the young and middle-aged men indicates that a larger burden of undiagnosed chronic comorbidities other than CVD, which are highly prevalent in the elderly but not in the young and middle-aged population, may contribute to the association between long sleep and cardiovascular risk. Consequently, the association between long sleep and CVD risk varies across population of different ages with different general health status. The findings suggest sleep patterns and other CVD-related chronic diseases may confound the relationship between sleep and CVD risk; therefore, experimental studies are needed to further explore the mechanisms underlying the associations of long sleep duration and CVD risk.
Being consistent with our findings, a substantial number of studies have indicated that short sleep is independently associated with an increased risk of CVD among adults.16,17 Though the associations between long sleep duration and CVD risk may be driven by the outcome or impact of infirmity and disease, short sleep duration among young and middle-aged adults may be part of an unhealthy lifestyle, which may impair general health and predispose them to CVD. In the current study, compared with optimal or long sleepers, young and middle-aged short sleepers reported the highest prevalence of CVD risk behaviors, such as smoking, alcohol drinking and long sedentary duration. The short sleepers also had the highest means of BMI and SBP, and the highest prevalence of hypertension and diabetes, indicating that short sleepers were of the worst general health compared with optimal and long sleepers.
Overweight and obesity with comorbidities including hypertension and insulin resistance collectively contributes to the development of CVD among short sleepers. Considerable research suggests that adipocytes may play an essential role in overweight and obesity caused by sleep restriction. Reduction in sleep duration can affect leptin release from adipocytes,33 thereby altering the neuroendocrine regulation of hunger. Subjective hunger and appetite increase during sleep restriction, thus altering eating behavior and contributing to the development of obesity. Although leptin levels increase with adiposity, the ability of leptin to reduce food intake may be impaired in the obese status, possibly due to saturated transport systems, suggesting that leptin resistance occurs in addition to insulin resistance in obesity.34 Since adipocytes are the only leptin-producing cells, they may play a crucial role in the development of sleep-induced changes in systemic energy metabolism. Molecular mechanisms underlying sleep curtailment-induced leptin resistance and impaired insulin action are comprehensive and hypothetical. Potential pathways include increased exposure to elevated sympathetic nervous activity either via direct innervation or indirectly via elevated catecholamine levels, stimulation of the stress-responsive hypothalamo-pituitary axis with a resulting increased exposure to glucocorticoids and/or increased inflammation,35 all of which aggravate the development of adipocyte dysfunction and obesity. Increased oxidative stress caused by obesity then leads to inflammation and hypoxia, inducing perivascular adipose tissue (PVAT) dysfunction, which plays a critical role in the development of diseases such as hypertension and atherosclerosis.36–38 PVAT produces biologically active molecules, including cytokines, adipokines, gaseous molecules, prostacyclin, angiotensin, methyl palmitate, and reactive oxygen species (ROS).39,40 It plays a beneficial role by regulating vascular function and homeostasis as long as molecule levels with opposing properties remain in equilibrium. In obesity, PVAT mass and adipocyte size are increased41 and secretes more inflammatory adipokines/cytokines, which may further alter PVAT characteristics and secretomes, and cause dysfunction of the underlying vascular smooth muscle cells (VSMCs) and endothelial cells (ECs),42 eventually affecting vascular homeostasis.43 Dysfunction of vascular homeostasis is an important contributing factor to the development and progression of hypertension37 and atherosclerosis.36,44 In this study, though a higher percentage of short sleep duration was reported among men than women, the odds of short sleep for CVD risk were statistically significant among women but not in men, indicating that women may be more sensitive to the cardiovascular risk associated with short sleep. Evidence from experimental animals also supports the sex-dependent vascular function mediated by PVAT in hypertension and stroke,45,46 suggesting the roles of PVAT-derived adipokines in mediating sex-dependent vascular function in hypertension. The intrinsic differences in PVAT between the sexes need to be further explored in future.47
The strengths of the present study lie in the young and middle-aged sample. The study is the first for this topic worldwide focusing on young and middle-aged adults, whose sleep was dramatically influenced by modern work and lifestyle. Most studies on this issue have focused on middle-aged and older populations for the assumption that younger people have a low or no risk of CVD. In light of the high prevalence of cardiovascular risk factors (eg, being sedentary, less physical exercise, obesity, hyperlipidemia) found among young adults in the previous study,48 we hypothesized that factors contributing to sleep duration and CVD risk are different in young and middle-aged and older adults, and the association of sleep duration with CVD risk is also different in young and middle-aged and older adults. Therefore, we only included adults younger than 65 years to explore whether associations between sleep duration and 10-year CVD risk are different between young and middle-aged adults and general adults. Second, a multi-stage stratified cluster sampling among attendees at physical examination centers was used to obtain a more diverse population on sociodemographic characteristics, duration of sleep, lifestyle, obesity, and metabolic status, thus guaranteeing the representativeness of the sample and the high reliability of the findings. Third, we have collected data on sedentary behavior in addition to conventional cardiovascular risk factors, such as smoking, drinking and lack of exercise. Sedentary behavior is highly prevalent in modern lifestyle, especially among young and middle-aged population. Being sedentary for more than six hours per day was significantly associated with both sleep duration and predicted 10-year cardiovascular risk in the current study, indicating that it might confound the relationship between sleep duration and predicted cardiovascular risk. Including sedentary time into the multivariate regression model helps to exclude its confounding effects, therefore guarantees more reliable results.
The current research has several limitations meriting consideration. First, we only analyzed the baseline data of the cohort, which restricted our ability to make causal inferences about the relationship between durations of sleep and predicted CVD risk. Second, the cohort was constructed by motivated individuals and the vast majority of participants finished higher education and were in a higher socioeconomic status. Therefore, the generalizability of our findings to other populations was uncertain. Lastly, we collect the sleep duration by self-report rather than using polysomnography and reported information bias might be introduced into the current research. Longitudinal studies are needed to further verify the association between durations of sleep and cardiovascular risk.
Conclusion
We have assessed the association between durations of sleep and predicted cardiovascular risk among young and middle-aged Chinese adults. The current findings highlight the beneficial effects of long sleep and the adverse impact of short sleep on cardiovascular health in people younger than 65 years. Given the high prevalence of CVD worldwide, the information may be crucial to further insight into the comprehensive association between durations of sleep and the predicted cardiovascular risk among young and middle-aged adults to guide preventive strategies.
Abbreviations
BMI, body mass index; CI, confidence interval; CVD, cardiovascular disease; DBP, diastolic blood pressure; FRS, Framingham risk score; HDL-C, high-density lipoprotein cholesterol; OR, odds ratio; PSQI, Pittsburgh Sleep Quality Index; SBP, systolic blood pressure; SD, standard deviation; TC, total cholesterol.
Data Sharing Statement
The datasets generated and analysed during the current study are not publicly available due to state restrictions but are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study protocol was approved by the ethics review boards of Nankai University (NKUIRB2016063) and Hebei Medical University (2016021). The research procedures were performed strictly following the Declaration of Helsinki. All methods were conducted in accordance with relevant guidelines and regulations. We obtained written informed consent from all participants.
Acknowledgments
The survey was performed in Tianjin Union Medical Center, Tianjin First Central Hospital, Beijing Physical Examination Center, the First Hospital of Hebei Medical University, the Second Hospital of Hebei Medical University, and Shijiazhuang Changcheng Health Screening Center. We sincerely thank all the study participants and the staff involved in facilitating the study.
Author Contributions
All authors have made significant contributions to the work reported, whether in conception, study design, execution, data acquisition, analysis and interpretation, or in all of these areas. MYZ has concepted, designed and supervised implementation of the study, and led the writing and revision of the article. JH conducted the data acquisition, interpretation and execution of the study, and participated in the writing and revision of the article. YW conducted the data analysis and participated in the data acquisition and the drafting of the article. LZ, CL, XQ, SC, YN and MZZ have organized the investigation and participated in the design of study and the review of the article. PG, JW, FL, RZ, QL, SM and CH have participated in the data acquisition and execution of the study, as well as the drafting or review of the article. All authors have reached an agreement on the Journal of the article, reviewed and agreed on all versions of the article, and agreed to take responsibility and be accountable for the contents of the article.
Funding
This study was funded by the Chinese Key Research & Development Program (Nos. 2016YFC0900600, 2016YFC0900604) from the Chinese Ministry of Science and Technology. The views expressed are those of the authors and not necessarily those of the Foundation.
Disclosure
The authors declare that they have no competing interests.
References
1. Hirshkowitz M, Whiton K, Albert SM, et al. National sleep foundation’s updated sleep duration recommendations: final report. Sleep Health. 2015;1:233–243. doi:10.1016/j.sleh.2015.10.004
2. [Sleep Quality Data in China]. Zhong guo ke ji xin xi. 2020;24:6-9. Chinese.
3. Qureshi AI, Giles WH, Croft JB, Bliwise DL. Habitual sleep patterns and risk for stroke and coronary heart disease: a 10-year follow-up from NHANES I. Neurology. 1997;48:904–911. doi:10.1212/WNL.48.4.904
4. Lakerveld J, Mackenbach JD, Horvath E, et al. The relation between sleep duration and sedentary behaviours in European adults. Obes Rev. 2016;17(Suppl 1):62–67. doi:10.1111/obr.12381
5. Kim Y, Wilkens LR, Schembre SM, Henderson BE, Kolonel LN, Goodman MT. Insufficient and excessive amounts of sleep increase the risk of premature death from cardiovascular and other diseases: the Multiethnic Cohort Study. Prev Med. 2013;57:377–385. doi:10.1016/j.ypmed.2013.06.017
6. Ferrie JE, Shipley MJ, Cappuccio FP, et al. A prospective study of change in sleep duration: associations with mortality in the Whitehall II cohort. Sleep. 2007;30:1659–1666. doi:10.1093/sleep/30.12.1659
7. Hublin C, Partinen M, Koskenvuo M, Kaprio J. Sleep and mortality: a population-based 22-year follow-up study. Sleep. 2007;30:1245–1253. doi:10.1093/sleep/30.10.1245
8. Ikehara S, Iso H, Date C, et al. Association of sleep duration with mortality from cardiovascular disease and other causes for Japanese men and women: the JACC study. Sleep. 2009;32:295–301. doi:10.1093/sleep/32.3.295
9. Yin J, Jin X, Shan Z, et al. Relationship of sleep duration with all-cause mortality and cardiovascular events: a systematic review and dose-response meta-analysis of prospective cohort studies. J Am Heart Assoc. 2017;6. doi:10.1161/JAHA.117.005947
10. Krueger PM, Friedman EM. Sleep duration in the United States: a cross-sectional population-based study. Am J Epidemiol. 2009;169:1052–1063. doi:10.1093/aje/kwp023
11. Akerstedt T, Knutsson A, Westerholm P, Theorell T, Alfredsson L, Kecklund G. Sleep disturbances, work stress and work hours: a cross-sectional study. J Psychosom Res. 2002;2002:741–748. doi:10.1016/S0022-3999(02)00333-1
12. Ahmad A, Didia SC. Effects of sleep duration on cardiovascular events. Curr Cardiol Rep. 2020;22:18. doi:10.1007/s11886-020-1271-0
13. Whinnery J, Jackson N, Rattanaumpawan P, Grandner MA. Short and long sleep duration associated with race/ethnicity, sociodemographics, and socioeconomic position. Sleep. 2014;37:601–611. doi:10.5665/sleep.3508
14. Liu Y, Dong Y, Li X, Mao X, Peng G, Liu L. Meta-analysis of the prevalence of sleep disorder among Chinese elderly aged 60 years and over. Mod Preven Med. 2014;41:
15. Ford ES. Habitual sleep duration and predicted 10-year cardiovascular risk using the pooled cohort risk equations among US adults. J Am Heart Assoc. 2014;3:e001454. doi:10.1161/JAHA.114.001454
16. Yazdanpanah MH, Homayounfar R, Khademi A, Zarei F, Shahidi A, Farjam M. Short sleep is associated with higher prevalence and increased predicted risk of cardiovascular diseases in an Iranian population: Fasa PERSIAN Cohort Study. Sci Rep. 2020;10:4608. doi:10.1038/s41598-020-61506-0
17. Im E, Kim GS. Relationship between sleep duration and Framingham cardiovascular risk score and prevalence of cardiovascular disease in Koreans. Medicine. 2017;96:e7744. doi:10.1097/MD.0000000000007744
18. Li F, Sun K, Lin D, et al. Longtime napping is associated with cardiovascular risk estimation according to Framingham risk score in postmenopausal women. Menopause. 2016;23:950–956. doi:10.1097/GME.0000000000000661
19. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi:10.1016/0165-1781(89)90047-4
20. Potvin O, Lorrain D, Belleville G, Grenier S, Preville M. Subjective sleep characteristics associated with anxiety and depression in older adults: a population-based study. Int J Geriatr Psychiatry. 2014;29:1262–1270. doi:10.1002/gps.4106
21. Backhaus J, Junghanns K, Broocks A, Riemann D, Hohagen F. Test-retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. J Psychosom Res. 2002;53:737–740. doi:10.1016/S0022-3999(02)00330-6
22. Krittanawong C, Tunhasiriwet A, Wang Z, et al. Association between short and long sleep durations and cardiovascular outcomes: a systematic review and meta-analysis. Eur Heart J Acute Cardiovasc Care. 2019;8:762–770. doi:10.1177/2048872617741733
23. Writing Group of 2010 Chinese Guidelines for the Management of Hypertension. [2010 Chinese guidelines for the management of hypertension]. Zhong hua xin xue guan bing za zhi. 2011;39:579–615. Chinese.
24. Chen C, Lu FC. The guidelines for prevention and control of overweight and obesity in Chinese adults. BES. 2004;17:1–36.
25. D’Agostino RB, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117:743–753. doi:10.1161/CIRCULATIONAHA.107.699579
26. Lloyd-Jones DM. Cardiovascular risk prediction: basic concepts, current status, and future directions. Circulation. 2010;121:1768–1777. doi:10.1161/CIRCULATIONAHA.109.849166
27. Hoevenaar-Blom MP, Spijkerman AM, Kromhout D, van den Berg JF, Verschuren WM. Sleep duration and sleep quality in relation to 12-year cardiovascular disease incidence: the MORGEN study. Sleep. 2011;34:1487–1492. doi:10.5665/sleep.1382
28. Stranges S, Dorn JM, Shipley MJ, et al. Correlates of short and long sleep duration: a cross-cultural comparison between the United Kingdom and the United States: the Whitehall II Study and the Western New York Health Study. Am J Epidemiol. 2008;168:1353–1364. doi:10.1093/aje/kwn337
29. Kripke DF, Garfinkel L, Wingard DL, Klauber MR, Marler MR. Mortality associated with sleep duration and insomnia. Arch Gen Psychiatry. 2002;59:131–136. doi:10.1001/archpsyc.59.2.131
30. Patel SR, Ayas NT, Malhotra MR, et al. A prospective study of sleep duration and mortality risk in women. Sleep. 2004;27:440–444. doi:10.1093/sleep/27.3.440
31. Irwin MR, Olmstead R, Carroll JE. Sleep disturbance, sleep duration, and inflammation: a systematic review and meta-analysis of cohort studies and experimental sleep deprivation. Biol Psychiatry. 2016;80:40–52. doi:10.1016/j.biopsych.2015.05.014
32. Signal TL, Gale J, Gander PH. Sleep measurement in flight crew: comparing actigraphic and subjective estimates to polysomnography. Aviat Space Environ Med. 2005;76:1058–1063.
33. Taheri S, Lin L, Austin D, Young T, Mignot E. Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLoS Med. 2004;1:210–217. doi:10.1371/journal.pmed.0010062
34. Caro JF, Kolaczynski JW, Nyce MR, et al. Decreased cerebrospinal-fluid/serum leptin ratio in obesity: a possible mechanism for leptin resistance. Lancet. 1996;348:159–161. doi:10.1016/S0140-6736(96)03173-X
35. Broussard J, Brady MJ. The impact of sleep disturbances on adipocyte function and lipid metabolism. Best Pract Res Clin Endocrinol Metab. 2010;24:763–773. doi:10.1016/j.beem.2010.08.007
36. Hu H, Garcia-Barrio M, Jiang ZS, Chen YE, Chang L. Roles of perivascular adipose tissue in hypertension and atherosclerosis. Antioxid Redox Signal. 2021;34:736–749. doi:10.1089/ars.2020.8103
37. DeMarco VG, Aroor AR, Sowers JR. The pathophysiology of hypertension in patients with obesity. Nat Rev Endocrinol. 2014;10:364–376. doi:10.1038/nrendo.2014.44
38. Hall JE, Do Carmo JM, da Silva AA, Wang Z, Hall ME. Obesity-induced hypertension: interaction of neurohumoral and renal mechanisms. Circ Res. 2015;116:991–1006. doi:10.1161/CIRCRESAHA.116.305697
39. Chang L, Garcia-Barrio MT, Chen YE. Brown adipose tissue, not just a heater. Arterioscler Thromb Vasc Biol. 2017;37:389–391. doi:10.1161/ATVBAHA.116.308909
40. Villacorta L, Chang L. The role of perivascular adipose tissue in vasoconstriction, arterial stiffness, and aneurysm. Horm Mol Biol Clin Investig. 2015;21:137–147. doi:10.1515/hmbci-2014-0048
41. Marchesi C, Ebrahimian T, Angulo O, Paradis P, Schiffrin EL. Endothelial nitric oxide synthase uncoupling and perivascular adipose oxidative stress and inflammation contribute to vascular dysfunction in a rodent model of metabolic syndrome. Hypertension. 2009;54:1384–1392. doi:10.1161/HYPERTENSIONAHA.109.138305
42. Jia G, Sowers JR. Endothelial dysfunction potentially interacts with impaired glucose metabolism to increase cardiovascular risk. Hypertension. 2014;64:1192–1193. doi:10.1161/HYPERTENSIONAHA.114.04348
43. Sowka A, Dobrzyn P. Role of perivascular adipose tissue-derived adiponectin in vascular homeostasis. Cells. 2021;10:1485. doi:10.3390/cells10061485
44. Thanassoulis G, Massaro JM, Corsini E, et al. Periaortic adipose tissue and aortic dimensions in the Framingham Heart Study. J Am Heart Assoc. 2012;1:e000885. doi:10.1161/JAHA.112.000885
45. Ahmad AA, Randall MD, Roberts RE. Sex differences in the regulation of porcine coronary artery tone by perivascular adipose tissue: a role of adiponectin? Br J Pharmacol. 2017;174:2773–2783. doi:10.1111/bph.13902
46. Small HY, McNeilly S, Mary S, Sheikh AM, Delles C. Resistin mediates sex-dependent effects of perivascular adipose tissue on vascular function in the Shrsp. Sci Rep. 2019;9:6897. doi:10.1038/s41598-019-43326-z
47. White UA, Tchoukalova YD. Sex dimorphism and depot differences in adipose tissue function. Biochim Biophys Acta. 2014;1842:377–392. doi:10.1016/j.bbadis.2013.05.006
48. Xue WY, Li Z, Jun LC, et al. Predicted 10-year cardiovascular disease risk and its association with sleep duration among adults in Beijing-Tianjin-Hebei Region, China. Biomed Environ Sci. 2021;34:803–813. doi:10.3967/bes2021.109
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.