Back to Journals » Infection and Drug Resistance » Volume 15
Association Between Genetic Polymorphisms of lncRNA NEAT1 and Pulmonary Tuberculosis Risk, Clinical Manifestations in a Chinese Population
Authors Li HM, Wang LJ, Tang F, Pan HF ![]() , Zhang TP
, Zhang TP
Received 19 December 2021
Accepted for publication 22 April 2022
Published 12 May 2022 Volume 2022:15 Pages 2481—2489
DOI https://doi.org/10.2147/IDR.S354863
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Suresh Antony
Hong-Miao Li,1,2,* Li-Jun Wang,2,* Fei Tang,3 Hai-Feng Pan,1 Tian-Ping Zhang4
1Department of Epidemiology and Biostatistics, School of Public Health, Anhui Medical University, Hefei, People’s Republic of China; 2Department of Infectious Diseases, The First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 3Anhui Chest Hospital (Anhui Provincial TB Institute), Hefei, Anhui, People’s Republic of China; 4The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Tian-Ping Zhang, The First Affiliated Hospital of USTC, 17 Lujiang Road, Hefei, Anhui, 230001, People’s Republic of China, Email [email protected] Hai-Feng Pan, School of Public Health, Anhui Medical University, Hefei, 230032, Anhui, People’s Republic of China, Email [email protected]
Background: Recent studies have shown that abnormal expression of lncRNA NEAT1 is associated with the progression of pulmonary tuberculosis (PTB). The aim of our study was to analyze the relationship between single nucleotide polymorphisms (SNPs) of NEAT1 gene and susceptibility to PTB.
Methods: Four SNPs (rs2239895, rs3741384, rs3825071, rs512715) in NEAT1 gene were genotyped in 479 patients with PTB and 476 controls by improved multiple ligase detection reaction (iMLDR) in a Chinese population.
Results: We found no significant differences in allele and genotype frequencies of NEAT1 gene rs2239895, rs3741384, rs3825071, rs512715 between PTB patients and controls (all P > 0.05). There was no statistically significant association between genotype frequency distribution of dominant model, as well as recessive model, and genetic susceptibility to PTB patients (all P > 0.05). The TT genotype, T allele frequencies of rs3825071 were significantly increased in sputum smear-positive PTB patients when compared to sputum smear-negative PTB patients (P = 0.010, P = 0.003, respectively). Haplotype analysis shown that NEAT1 haplotype frequency was not associated with PTB susceptibility.
Conclusion: NEAT1 gene polymorphisms were not associated with the risk of PTB in Chinese population, and rs3825071 polymorphism might be related to sputum smear-positive in PTB patients.
Keywords: long non-coding RNA, NEAT1, pulmonary tuberculosis, single nucleotide polymorphisms
Introduction
Tuberculosis (TB) is a common, chronic infectious disease caused by Mycobacterium tuberculosis (MTB), and a serious public health problem around the world, which significantly affect human health.1 According to the latest World Health Organization Global Tuberculosis report, there is approximately 9.9 million new incident TB patients globally in 2021, with an increasing threat.2 The pathogenesis of TB is complex, and the occurrence of TB is relatively slow.3 In addition, the patients normally have sputum smear negative, and no special clinical manifestations besides cough, fever in the early stage. Therefore, it is very important to research the risk factors leading to increased susceptibility to TB and to provide scientific basis for developing disease control strategies. Studies had shown that about a third of the population was infected with MTB, of which 10% would develop TB, while the remaining 90% might never develop symptomatic disease.4 This suggested that the occurrence and progression of this disease was influenced by a variety of factors, such as genetic variation, nutritional status and environmental factors.5 The genetic variation of HLA, killer immunoglobulin-like receptor, Toll-like receptor, vitamin D receptor might play an important role in the susceptibility to pulmonary TB (PTB).6–9
Long noncoding RNAs (lncRNAs) referred to a class of non-coding RNA transcripts with a length of more than 200 nucleotides, which played a key role in many biological processes including transcriptional, posttranslational, and epigenetic regulation of gene expression.10 There was sufficient evidence that lncRNA was also involved in the regulation of host immune response to invasive pathogens, and abnormal expression of lncRNA was associated with a variety of infectious diseases.11 Several studies had been reported on lncRNA effected on acquired and innate immunity responses against MTB, and the differential expression of several lncRNA was also observed in PTB patients.12,13 In addition, the single nucleotide polymorphisms (SNP) in lncRNA genes have been shown to influence the susceptibility and clinical presentation of PTB.14–16 The data of Zhao et al indicated that lncRNA AC079767.4 polymorphism had the potential to serve as a novel biomarker for PTB diagnosis.14
LncRNA NEAT1 was an important inflammatory regulator that not only promoted the activation of inflammasome, but also facilitated the expression of inflammatory cytokines by regulating the expression of miR-17-5p/TLR4 in macrophages.17,18 It had been reported that the up-regulation of NEAT1 played an anti-TB role in MTB-infected patients.19 Our recent study suggested that NEAT1 expression level was abnormally increased in patients with PTB compared to normal controls.20 In addition, previous studies demonstrated that the genetic variations in NEAT1 were significantly associated with risk of multiple diseases, including lung cancer,21 lung squamous cell carcinoma,22 oral squamous cell carcinoma,23 etc. However, no study explored the association between NEAT1 gene variation and susceptibility to PTB. Therefore, we performed this study to investigate the association between NEAT1 gene polymorphism and PTB susceptibility, as well as some clinical manifestations in a Chinese population.
Materials and Methods
Study Design and Subjects
A total of 955 subjects were included in this case-control study, including 479 patients with PTB and 476 healthy controls. All PTB patients were selected from Anhui Chest Hospital, and diagnosed by experienced respiratory physician based on the following criteria: clinical symptoms, chest radiograms, sputum and/or bronchoalveolar lavage fluid MTB culture, microscopic examination of Acid-fast bacilli (AFB), and efficacy of anti-tuberculosis treatment. The PTB patients with HIV infection, hepatitis, cancers, pregnancy, and other respiratory diseases were excluded from the study. All healthy individuals without a previous history of TB, cancer, and HIV were enrolled from health examine center in the same area as the controls. Moreover, healthy controls must also be asymptomatic, sputum smear and culture negative, and chest radiographs normal.
The present study was approved by the Ethics Committee of Anhui Medical University (20200250), and informed consent was acquired from each subject. Then, we collected the demographic data of all subjects, as well as the clinical data of PTB patients including fever, drug resistance, drug-induced liver injury (DILI), etc. from the medical record system of Anhui Chest Hospital. Meanwhile, about 5 mL early morning fasting blood samples from all subjects were collected for DNA extraction.
SNP Selection and Genotyping
At present, the study on NEAT1 gene polymorphism and PTB had not been reported, therefore, we tried to identify the Tag SNP sites in NEAT1 gene. Firstly, we collected the genotype data of NEAT1 in the Han Chinese people in Beijing by using Ensembl Genome Browser 85 and CHBS_1000G. Then, the pairwise option of the HaploView 4.0 software (Cambridge, MA, USA) was used to select the tag SNPs of NEAT1. The tag SNPs, which located in potentially functional regions such as promoters, exons, untranslated regions (UTRs), were preferred for genotyping in this study. In addition, we also searched the previous studies on the association of NEAT1 gene polymorphisms with human diseases.22–24 Finally, we selected four SNPs of NEAT1 gene, including rs2239895, rs3741384, rs3825071, rs512715. These SNPs all met the following two requirements: r2 threshold > 0.8, minor allele frequency (MAF) ≥ 0.05 in CHB.
The Flexi Gene-DNA Kit (Qiagen, Valencia, CA) was used to extract genomic DNA from each peripheral blood sample according to the manufacturer’s instructions, and the improved multiple ligase detection reaction (IMLDR) technique was used for genotyping, with the technical support from Genesky Biotechnologies (Inc., Shanghai).25 The detailed experimental steps were as follows: (1) 1μL DNA sample was extracted, and the quality of the sample was checked and the concentration was estimated by 1% agarose electrophoresis. Then the DNA sample was diluted to 5–10 ng/μL according to the estimated concentration. (2) Multiplex PCR reaction was carried out with 20μL reaction system included 1x HotStarTaq buffer, 3.0 mMMg2+, 0.3mM dNTP, 1U HotStarTaq polymerase (Qiagen Inc.), 1μL sample DNA and 1μL multiple PCR primers. (3) Purification of multiple PCR products: 5U SAP enzyme and 2U Exonuclease I enzyme were added to 20 μL PCR product, 37°C warm bath for 1h, then 75°C inactivated for 15min. (4) Ligating reaction system: 1 μL 10x ligating buffer, 0.25 μL high temperature ligase, 0.4 μL 5’ ligating primer mixture (1μM), 0.4 μL primer 3’ ligating primer mixture (2 μM), 2 μL purifed multiple PCR products, 6 μL ddH2O mixing. (5) The 0.5 μL diluted product was mixed with 0.5 μL Liz500 SIZE STANDARD, 9 μL Hi-Di, denatured at 95°C for 5 min, then placed on the ABI3730XL sequencer. (6) The raw data collected on the ABI3730XL sequencer are analyzed by GeneMapper 4.1 (AppliedBiosystems, USA). The subjects with 100% genotyping success rate for all SNPs were included for final analysis. Those subjects with 100% genotype success for four SNPs were eventually included in our subsequent analysis.
Statistical Analysis
Statistical analysis of our study was performed using SPSS 23.0 software (SPSS Inc., IL, USA). Hardy-Weinberg equilibrium (HWE) of all SNPs genotype distributions among controls was evaluated by Chi-square test. Calculated genotypic and allelic frequencies for all SNPs in PTB patients and controls were compared with Chi-square test, and odds ratios (OR), 95% confidence intervals (CI) were analyzed through logistic regression analyses. In addition, two genetic models (dominant model, recessive model) were also analyzed. The Chi-square test was used to assess the possible association between NEAT1 gene polymorphisms and the patients’ clinical features. Haplotype analysis with NEAT1 polymorphisms was also carried out by SHEsis software.26 P < 0.05 was considered as statistical significance. The Bonferroni correction was used for multiple testing.
Results
Relationship Between NEAT1 Gene SNPs and PTB Risk
The mean age of 479 PTB patients, including 313 males and 166 females, was 45.07±17.74 years. The average age of 476 controls, including 208 males and 268 females, was 43.36±13.84 years (Table 1). The common clinical characteristics of PTB patients were also summarized in Table 1. The allele, genotype frequencies of NEAT1 gene rs2239895, rs3741384, rs3825071, rs512715 in PTB patients and controls were shown in Table 2, and the controls were in Hardy-Weinberg’s equilibrium (all P > 0.05).
 |
Table 1 The Demographic and Clinical Characteristics of PTB Patients and Healthy Controls |
 |
Table 2 Genotypes and Alleles Frequencies of NEAT1 Gene in PTB Patients and Healthy Controls |
Regarding the allele frequency of NEAT1 gene rs2239895, rs3741384, rs3825071, rs512715 between PTB patients and controls, we noted no significant association (all P > 0.05). Similarly, no significant difference was existed in genotype frequency of all SNPs among PTB patients and controls (all P > 0.05). We also constructed dominant model and recessive model to further investigate the differences in the frequencies of different genotypes between PTB patients and the control group, and no significant differences were found (all P > 0.05).
Association of NEAT1 Gene SNPs with Several Clinical Features in PTB Patients
Considering that the clinical manifestations and complications of PTB might affect the disease progression of patients, we determined to explore the potential association between NEAT1 gene polymorphism and the common clinical characteristics of PTB patients in a case-only study (Table 3). We found that the TT genotype, T allele frequencies of rs3825071 were significantly increased in sputum smear-positive PTB patients when compared to sputum smear-negative PTB patients (P < 0.0167, P = 0.003, respectively). The rs512715 CC genotype frequency appeared to be increased in PTB patients with hypoproteinemia, while the significant association disappeared after multiple testing by Bonferroni correction (P > 0.0167). Similarly, no statistically significant association was found between rs512715 gene variation and pulmonary infection in PTB patients after Bonferroni correction (P > 0.0167).
 |
Table 3 The Associations Between NEAT1 Gene Polymorphisms and Several Clinical Features of PTB Patients |
Nonetheless, there was no significant difference between rs2239895, rs3741384 polymorphism and these clinical characteristics of PTB patients (all P > 0:05).
Haplotype Analysis
We used SHEsis software to detect four major haplotypes of NEAT1 gene, including CACC, GGCC, GGCG, GGTG, and analyzed the association between the frequency of these haplotypes and susceptibility to PTB. The results suggested that the association between these haplotype frequencies and susceptibility to PTB was not statistically significant (Table 4).
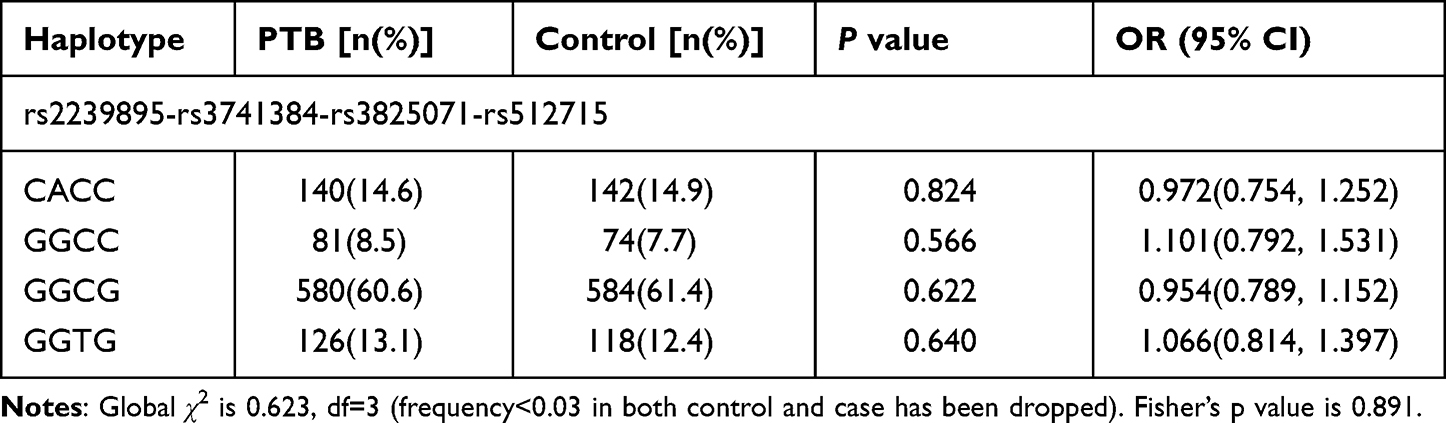 |
Table 4 Haplotype Analysis of NEAT1 Gene in PTB Patients and Controls |
Discussion
Abnormal expression and gene variation of multiple lncRNA had been proved to be closely related to the occurrence and development of tumors, autoimmune diseases, etc.27,28 At the same time, the regulatory roles of lncRNA in PTB had also attracted widespread attention. Yi et al used microarray to detect the expression profile of lncRNA in CD4+T cells, and found that compared with healthy control group, there was abnormal expression of lncRNA in peripheral blood CD4+T cells in patients with active and latent TB.29 According to another recent study, the T-cell inhibitory factor CD244 might control the CD8+T cell immune response during TB infection through inducing the lncRNA CD244 expression.30 One recent study shown that lncRNA NEAT1, which known as a novel regulatory molecule, had two subtypes including NEAT1_1(3.7 kb) and NEAT1_2 (23 kb), and was actively involved in immune regulation.31 Zhang et al found that NEAT1 was increased in T cells infected by HIV-1, whereas NEAT1 knockout stimulated the replication of HIV-1, and this was achieved through promoting the transport of HIV-1 mRNA from the nucleus to the cytoplasm.32 In addition, the results by Huang et al demonstrated that the NEAT1 expression level was higher during MTB infection, and it might be related to the outcome of TB.19 Similarly, our recent study also confirmed that the NEAT1 expression level in peripheral blood mononuclear cells of PTB patients was abnormally elevated.20 These results suggested that NEAT1 might be involved in the development of PTB, however, no study analyzed the association between NEAT1 gene polymorphism and PTB susceptibility. The present study was the first to explore the association between NEAT1 gene rs2239895, rs3741384, rs3825071, rs512715 and the risk of PTB. Our results demonstrated that there was no significant association between these SNPs and PTB.
The expression level of NEAT1 could be affected by genetic variation during the development of disease, thus researchers focused on the role of NEAT1 gene polymorphisms in the risk of many diseases. Wang et al found that NEAT1 gene rs2239895 polymorphism could upregulate its expression, and was associated with the risk of lung squamous cell carcinoma in a Chinese Northeast population.22 Similarly, the NEAT1 gene rs3825071 variant might affect gastric cancer susceptibility by modulated biological effects to improve the NEAT1 expression.24 Another study indicated that NEAT1 gene rs3741384 variant might influence the survival of oral squamous cell carcinoma patients, and identified a predictive role of rs3741384 GG in a worse prognosis of this disease.23 Previous studies had confirmed that a variety of lncRNA gene variants were associated with the genetic risk of PTB, moreover, the expression of NEAT1 in PTB patients was abnormal.14,15 To further analyze the role of NEAT1 gene variation in the pathogenesis of PTB, we explored the role of NEAT1 gene rs2239895, rs3741384, rs3825071, rs512715 variants in PTB. However, no significant result was found. Contrary to the above studies, our result did not seem to support the involvement of NEAT1 gene variation in the pathogenesis of PTB. It was worth noting that study regarding the association between NEAT1 gene variation and PTB was very limited. In addition, this result might be influenced by sample size, experimental methods etc. Thus, relevant studies were very necessary to verify this result.
During the progression of PTB, patients usually accompanied by a variety of complications and clinical manifestations, including pulmonary infection, fever, drug resistance, DILI, hypoproteinemia, which might affect the treatment process of patients. In a previous study, we found that GC gene rs7041, rs3733359 variants were significantly associated with pulmonary infection, fever in the PTB patients, respectively.4 Song et al found a significant association between lncRNA RP11-37B2.1 rs218916, rs160441 and the occurrence of thrombocytopenia among PTB patients.15 In this study, we found that rs3825071 variant TT genotype, T allele frequencies were significantly related to sputum smear-positive in PTB patients. Based on these results, we surmised that this SNP might act as a potential predictor of sputum smear status in PTB patients, thus contributing to make more appropriate treatment choices and management measures.
In conclusion, our study suggested that NEAT1 gene rs2239895, rs3741384, rs3825071, rs512715 polymorphisms might not be related to PTB susceptibility in a Chinese population. While, rs3825071 variant was significantly associated with sputum smear-positive in PTB patients. It was worth noting that several limitations existed in this study, including sample size, ethnic background, disease activity, course of disease, treatment, etc, which might influence the accuracy of these results of our study. Therefore, in order to further clarify the exact role of NEAT1 genetic variation in PTB, it was very necessary to carry out replication studies with larger sample sizes in different populations.
Abbreviations
TB, Tuberculosis; lncRNA, Long noncoding RNA; MAF, minor allele frequency; IMLDR, improved multiple ligase detection reaction; HWE, Hardy-Weinberg equilibrium; SNPs, single nucleotide polymorphisms; MTB, Mycobacterium tuberculosis.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Anhui Medical University (20200250), and the informed consent was obtained from each participant. All methods were carried out in accordance with relevant guidelines and regulations of declaration of Helsinki.
Acknowledgments
We sincerely thank all the participants in this project.
Funding
This work was supported by grants from the National Natural Science Foundation of China (82003515) and Anhui Provincial Natural Science Foundation (1908085QH368). The funder had no role in study design, data collection, analysis, interpretation of data and writing the manuscript.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Kaufmann SHE. New vaccines against tuberculosis. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2020;63:56–64. doi:10.1007/s00103-019-03065-y
2. World Health Organization. Global tuberculosis report 2021; 2021. Available from: https://www.who.int/tb/publications/global_report/en/.
3. Donovan ML, Schultz TE, Duke TJ, Blumenthal A. Type I interferons in the pathogenesis of tuberculosis: molecular drivers and immunological consequences. Front Immunol. 2017;8:1633. doi:10.3389/fimmu.2017.01633
4. Zhang TP, Chen SS, Zhang GY, Shi SJ, Wei L, Li HM. Association of vitamin D pathway genes polymorphisms with pulmonary tuberculosis susceptibility in a Chinese population. Genes Nutr. 2021;16:6. doi:10.1186/s12263-021-00687-3
5. Zhang M, Wang X, Zhu Y, Chen S, Chen B, Liu Z. Associations of genetic variants at TAP1 and TAP2 with pulmonary tuberculosis risk among the Chinese population. Epidemiol Infect. 2021;149:e79. doi:10.1017/S0950268821000613
6. Harishankar M, Selvaraj P, Bethunaickan R. Influence of genetic polymorphism towards pulmonary tuberculosis susceptibility. Front Med. 2018;5:213. doi:10.3389/fmed.2018.00213
7. Tang NL, Wang X, Chang KC, et al. Genetic susceptibility to Tuberculosis: interaction between HLA-DQA1 and age of onset. Infect Genet Evol. 2019;68:98–104. doi:10.1016/j.meegid.2018.12.014
8. Xun X, Shen MH. Associations between vitamin D receptor genetic variants and tuberculosis: a meta-analysis. Innate Immun. 2019;25:305–313. doi:10.1177/1753425919842643
9. Ortega E, Hernández-Bazán S, Sánchez-Hernández B, Licona-Limón I, Fuentes-Dominguez J. TLR4 single nucleotide polymorphisms in affect susceptibility to tuberculosis in Mexican population from the State of Veracruz. J Immunol Res. 2020;2020:2965697. doi:10.1155/2020/2965697
10. Wu H, Yang L, Chen L. The diversity of long noncoding RNAs and their generation. Trends Genet. 2017;33:540–552. doi:10.1016/j.tig.2017.05.004
11. Kazemzadeh M, Safaralizadeh R, Orang AV. LncRNAs: emerging players in gene regulation and disease pathogenesis. J Genet. 2015;94(4):771–784. doi:10.1007/s12041-015-0561-6
12. Fu Y, Gao K, Tao E, Li R, Yi Z. Aberrantly expressed long non-coding RNAs in CD8(+) T cells response to active tuberculosis. J Cell Biochem. 2017;118(12):4275–4284. doi:10.1002/jcb.26078
13. Fang Y, Zhao J, Wang X, et al. Identification of differentially expressed lncRNAs as potential plasma biomarkers for active tuberculosis. Tuberculosis. 2021;128:102065. doi:10.1016/j.tube.2021.102065
14. Zhao Z, Peng W, Wu L, Ying B. Correlation between lncRNA AC079767.4 variants and liver injury from antituberculosis treatment in West China. J Infect Chemother. 2020;26:63–68. doi:10.1016/j.jiac.2019.07.003
15. Song J, Liu T, Zhao Z, et al. Genetic polymorphisms of long noncoding RNA RP11-37B2.1 associate with susceptibility of tuberculosis and adverse events of antituberculosis drugs in west China. J Clin Lab Anal. 2019;33:e22880. doi:10.1002/jcla.22880
16. Wu Q, Zhong H, Bai H, et al. Clinical relevance of the lnc-HNF1B-3:1 genetic polymorphisms in Western Chinese tuberculosis patients. J Clin Lab Anal. 2020;34:e23076. doi:10.1002/jcla.23076
17. Zhang P, Cao L, Zhou R, Yang X, Wu M. The lncRNA Neat1 promotes activation of inflammasomes in macrophages. Nat Commun. 2019;10:1495. doi:10.1038/s41467-019-09482-6
18. Li Y, Guo W, Cai Y. NEAT1 promotes LPS-induced inflammatory injury in macrophages by regulating miR-17-5p/TLR4. Open Med. 2020;15:38–49. doi:10.1515/med-2020-0007
19. Huang S, Huang Z, Luo Q, Qing C. The expression of lncRNA NEAT1 in human tuberculosis and its antituberculosis effect. BioMed Res Int. 2018;2018:9529072. doi:10.1155/2018/9529072
20. Li HM, Chen SS, Bao XD, et al. Expression of long non-coding RNA MALAT1, NEAT1 and NEAT2 in peripheral blood of tuberculosis patients. Chin J Dis Control Prev. 2020;24(2):155–159.
21. Hu Z, Chen J, Meng P, Li M. Association between NEAT1 polymorphism and the risk of lung cancer: a protocol for systematic review and meta-analysis. Medicine. 2021;100:e25478.
22. Wang S, Cui Z, Li H, et al. LncRNA NEAT1 polymorphisms and lung cancer susceptibility in a Chinese Northeast Han Population: a case control study. Pathol Res Pract. 2019;215:152723. doi:10.1016/j.prp.2019.152723
23. Zhu L, He Y, Feng G, et al. Genetic variants in long non-coding RNAs UCA1 and NEAT1 were associated with the prognosis of oral squamous cell carcinoma. Int J Oral Maxillofac Surg. 2020;50(9):1131–1137. doi:10.1016/j.ijom.2020.11.024
24. Ji X, Yan Y, Ma N, et al. Variant of SNPs at lncRNA NEAT1 contributes to gastric cancer susceptibility in Chinese Han population. Int J Clin Oncol. 2021;26:694–700. doi:10.1007/s10147-020-01852-1
25. Zhang T, Li R, Li H, et al. The contribution of genetic variation and aberrant methylation of aryl hydrocarbon receptor signaling pathway genes to rheumatoid arthritis. Front Immunol. 2022. doi:10.3389/fimmu.2022.823863
26. Li Z, Zhang Z, He Z, Tang W, Li T, Zeng Z. A partition-ligation-combination-subdivision EM algorithm for haplotype inference with multiallelic markers: update of the SHEsis (http://analysis.bio-x.cn). Cell Res. 2009;19:519–523. doi:10.1038/cr.2009.33
27. Kim SH, Lim KH, Yang S, Joo JY. Long non-coding RNAs in brain tumors: roles and potential as therapeutic targets. J Hematol Oncol. 2021;14:77. doi:10.1186/s13045-021-01088-0
28. Zhang TP, Zhu BQ, Tao SS, et al. Long non-coding RNAs genes polymorphisms and their expression levels in patients with rheumatoid arthritis. Front Immunol. 2019;10:2529. doi:10.3389/fimmu.2019.02529
29. Yi Z, Li J, Gao K, Fu Y. Identifcation of differentially expressed long non-coding RNAs in CD4+ T cells response to latent tuberculosis infection. J Infect. 2014;69:558–568. doi:10.1016/j.jinf.2014.06.016
30. Wang Y, Zhong H, Xie X, et al. Long noncoding RNA derived from CD244 signaling epigenetically controls CD8+ T cell immune responses in tuberculosis infection. Proc Natl Acad Sci USA. 2015;112:E3883–92. doi:10.1073/pnas.1501662112
31. Zhang F, Wu L, Qian J, et al. Identification of the long noncoding RNA NEAT1 as a novel inflammatory regulator acting through MAPK pathway in human lupus. J Autoimmun. 2016;75:96–104. doi:10.1016/j.jaut.2016.07.012
32. Zhang Q, Chen CY, Yedavalli VS, Jeang KT. NEAT1 long noncoding RNA and paraspeckle bodies modulate HIV-1 posttranscriptional expression. MBio. 2013;4:e00596–12. doi:10.1128/mBio.00596-12
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.