Back to Journals » Psychology Research and Behavior Management » Volume 16
Association Between Family Support and Coping Strategies of People With Covid-19: A Cross-Sectional Study
Authors Chilon-Huaman AM, Camposano-Ninahuanca Á, Chávez-Sosa JV, Huancahuire-Vega S ![]() , De Borba W
, De Borba W
Received 25 February 2023
Accepted for publication 26 June 2023
Published 19 July 2023 Volume 2023:16 Pages 2747—2754
DOI https://doi.org/10.2147/PRBM.S410068
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Aileen M Chilon-Huaman,1 Ángela Camposano-Ninahuanca,1 Janett V Chávez-Sosa,1 Salomon Huancahuire-Vega,2,3 William De Borba1
1Nursing School, Universidad Peruana Unión (UPeU), Lima, Peru; 2Human Medicine School, Universidad Peruana Unión (UPeU), Lima, Peru; 3General Directorate of Research, Universidad Peruana Unión, (UPeU), Lima, Peru
Correspondence: Salomon Huancahuire-Vega, Human Medicine School, Universidad Peruana Unión (UPeU), Carretera Central Km 19 Lurigancho-Chosica, Lima, Peru, Tel +51 997 574 011, Email [email protected]
Purpose: The study aimed to determine the association between family support and coping strategies of people diagnosed with COVID-19.
Methods: The study was analytical and cross-sectional. The sample consisted of 500 participants who were selected by non-probabilistic and snowball sampling and included residents of both sexes who belonged to the city of Lima, with a diagnosis of COVID-19, who lived with relatives, and who accepted to participate in the research. For data collection, the scales “family support” and “Coping and Adaptation Process-Coping Adaptation Processing Scale (CAPS)” were used. The technique used was the survey through the home visit and the questionnaire instrument. To measure the relationship of the study variables, binary logistic regression was chosen, considering coping strategies as the dependent variable and socio-demographic data and family support as independent variables.
Results: Of the 500 participants, 50.4% were women, and 49.6% were men. The results revealed that most participants presented a high capacity for coping strategies and high perceived family support (97.2% and 81%, respectively). In the bivariate analysis, socio-demographic aspects and family support and their dimensions were related to high or low capacity for coping strategies. Significant differences were verified between marital status (p=0.026), having children (p=0.037), family support (p=0.000), and its dimensions with coping strategies. Finally, the multivariate analysis found that people with COVID-19 who perceived high family support were 33.74 times (95% CI: 7266– 156,739) more likely to have a high capacity for coping strategies.
Conclusion: Therefore, it is necessary to promote the development of parental and family support skills in the face of the health emergency caused by COVID-19.
Keywords: family support, coping strategies, coronavirus, health emergency
Introduction
A coping strategy is a cognitive, emotional, or behavioral response to stress related to a particular function: problem-focused or emotion-focused coping.1 Currently, most people who are infected with the virus that causes COVID-19 experience mild to moderate respiratory illness and recover without requiring special treatment. However, older people and those with underlying medical problems, such as cardiovascular disease, diabetes, chronic respiratory disease, and cancer, are more likely to develop severe illnesses that can lead to death.2,3 Consequently, many people diagnosed with COVID-19 experience fear and concern about their health status, worsening of chronic health problems, non-compliance with medical regimens, and increased use of pharmacological substances.4
Several studies have identified a variety of predictors for the use of coping strategies during the COVID-19 pandemic. In Israel, problem-focused coping was positively correlated with social support, openness, extraversion, conscientiousness, and agreeableness.5 Conversely, an Italian study found strong associations between maladaptive personality traits (such as negative affect and antagonism), psychological distress, and coping strategies.6 Similarly, a study in Peru revealed that adults with COVID-19 use self-care, compliance with health measures, relaxation, and entertainment as coping strategies.7
In addition, it has been verified that the greater use of adaptive coping behaviors during the COVID-19 pandemic is associated with greater resilience. The prediction of high levels of resilience was observed through adaptive coping strategies, such as acceptance, thus highlighting the importance of resilience as part of coping strategies.8 Finally, adaptive coping strategies, such as planning, practical support, and reframing, can mediate and predict higher levels of post-traumatic growth. The pandemic can be considered a new type of traumatic stressor; it affected the entire population worldwide, causing severe disruption of daily life.9
Family support is an essential element of social support and refers to perceived support from the family environment. It is positively associated with better adherence to medical treatment, shorter hospital stays, and a speedy recovery; and is inversely related to depression, burnout symptoms, and suicide risk.10,11 Family support will likely become more influential when entire societies are under strict lockdown restrictions.12 Additionally, the importance of family support and face-to-face interactions with COVID-19 patients has been verified.13 However, it has also been shown, in patients in intensive care, that family support, even if virtual, is essential to generate hope and confidence in the treatment and the recovery process.14 Although the family is an essential support for the patient, the family’s response to the presence of a sick member is usually complex, with positive and negative aspects. This family support could be associated with and determine by the coping strategies that the patient uses to overcome the disease.
Since the literature on family support as an influential factor in the use of coping strategies is scarce, the study aimed to determine the association between the perception that the person with COVID-19 has about family support and coping strategies in Lima, Peru.
Materials and Methods
Study Design and Participants
The study was analytical and cross-sectional. It was carried out among the inhabitants of the district of Lima, who represent 29.7% of the total population of Peru. The sample selection was non-probabilistic by snowball sampling. It included residents of legal age, of both sexes, who belonged to Lima, with a diagnosis of COVID-19, who lived with relatives, and who agreed to participate in the investigation. We calculated the sample size based on a population of 10,000,000 inhabitants in Lima. We made a conservative assumption that 50% of participants would have a high capacity for coping strategies, with a confidence level of 95% and a margin of error of 5%, obtaining the necessary sample of 385 participants. We surveyed 500 subjects.
Procedures and Data Collection Instruments
Data collection took place from July to December 2021, ending the second wave of infections in Peru, respecting social distancing and the use of biosafety equipment regulated by the country’s Ministry of Health. The technique used was the survey through the home visit and the questionnaire instrument. The study met the requirements of confidentiality, respect, and justice, requesting informed consent before data collection. The study was approved by the ethics committee of the Universidad Peruana Unión under resolution number 2021-CE-FCS - UPeU-019.
In the evaluation of socio-demographic information, the sex, age, marital status, education, having children, work, religious affiliation, the person who cares for them, the type of family (nuclear, single-parent, extended, and blended), and the use of oxygen support were considered.
For the family support variable, the scale of the same name was used, created by Leyva in Cajamarca, Peru, in 2018.15 It has 22 items distributed in three dimensions: consistent affective (1–7 items), family adaptation (8–15 items), and autonomy (16–22 items). It presents a response scale of three values: yes (3 points), partly (2), and no (1), and categorizes family support as high (33–66 points) and low (22–32 points). The content validity of the scale based on the expert judgment was confirmed (index of 0.96). The internal consistency analysis of the scale was determined by Cronbach’s Alpha coefficient (α= 0.945), showing high reliability.
For the coping strategies variable, the scale “Coping Adaptation Processing Scale (CAPS)” created by Callista Roy was used in Colombia in 2009.16 The instrument is made up of 47 items, grouped into five styles and strategies: recursive and focused (10 items), physical and focused reactions (14 items), alert process (9 items), systematic processing (6 items); and knowing and relating (8 items). It has a Likert-type response format with four criteria: never (1), rarely (2), almost always (3), always (4); and it categorized coping strategies into high capacity (94–184 points) and low capacity (47–93 points). The scale reported a facial validity of 95% and a global content validity index of 0.83. The construct validation of the scale was done through exploratory factor analysis, verifying that it has five factors. In addition, the internal consistency was calculated through Cronbach’s alpha, which reported a reliability of 0.70.
Data Analysis
The SPSS v.24 statistical package was used for data analysis, using simple frequency tables for univariate analysis and contingency tables with a Chi-square test for bivariate analysis. In the bivariate analysis, socio-demographic aspects and family support and their dimensions were related to high or low capacity for coping strategies. Similarly, we opted for binary logistic regression for the multivariate analysis, by backward steps using the Likelihood Ratio (LR) criterion, considering coping strategies as the dependent variable and sociodemographic data and family support as independent variables. In the multivariate analysis, variables with p-value <0.05 were included in the bivariate analysis. The coding carried out has been low capacity=0 and high capacity=1. A p-value< 0.05 was considered statistically significant.
Results
Of the 500 participants, 50.4% were women, and 49.6% were men. Likewise, 63.8% belonged to the adult age group, 57.6% were married or cohabiting, 61.6% had higher education, and 62.4% had children. On the other hand, 73.4% had a job, 54% professed the Catholic faith, 51.4% lived within a nuclear family, 89.2% were cared for by a family member during their convalescence from COVID-19, and 56.4% did not use oxygen support (Table 1).
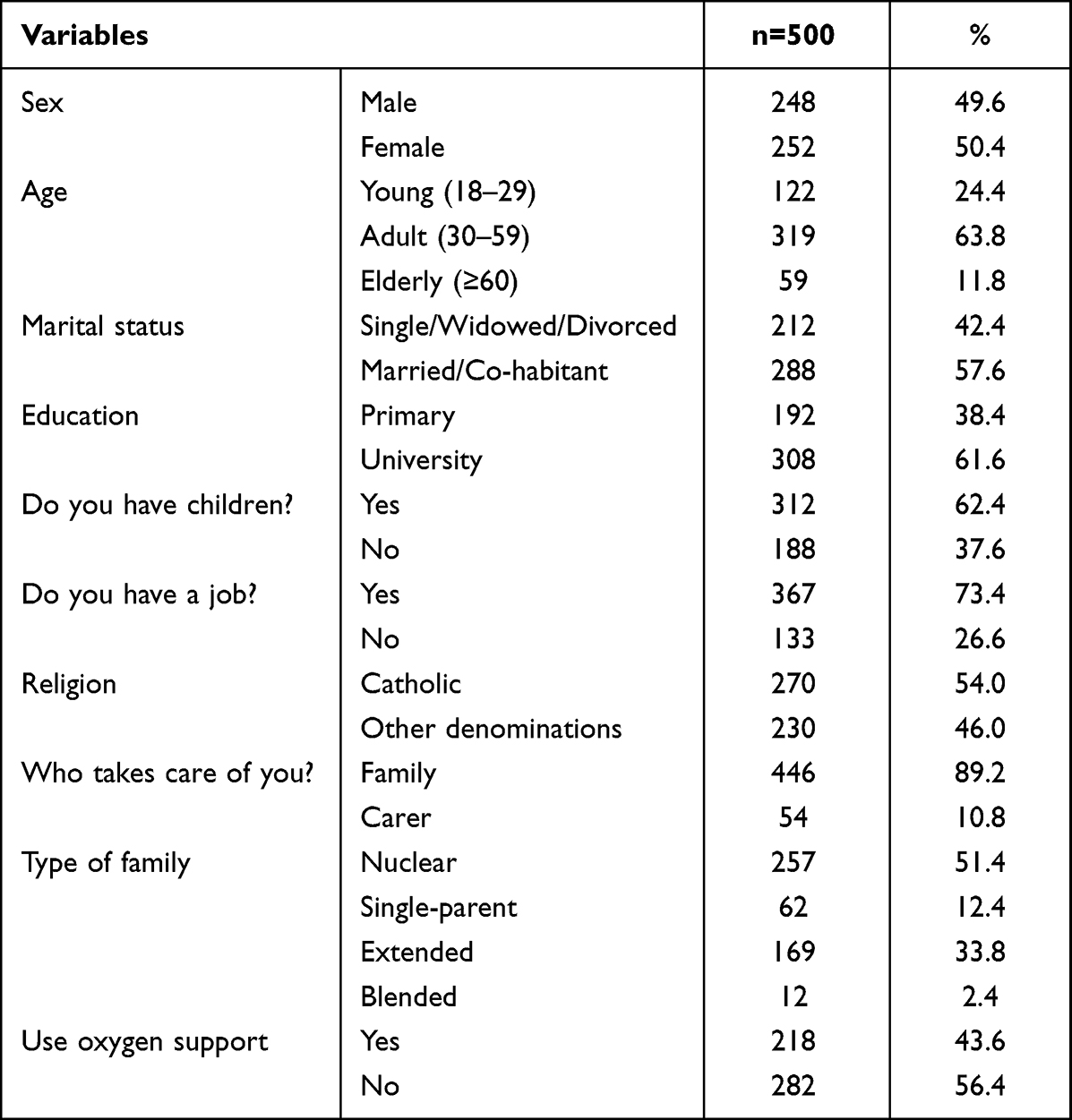 |
Table 1 General Characteristics of the Study Population |
In the descriptive analysis of the study variables, it was found that 97.2% of the participants had a high capacity for coping strategies and 2.8% a low capacity. In the same way, a high capacity was obtained in the recursive and focused alert process, systematic processing, and knowing and relating in 99.6%, 92.2%, 75%, and 80.2%, respectively. However, the physical and focused dimensions presented a low capacity of 89.2%. On the other hand, the family support variable was perceived as high by 81% of the participants and low by 19%. In addition, the consistent affective and family autonomy dimensions were rated as high by 91.8% and 78.6%. On the contrary, the family adaptation dimension was perceived as low at 53.8% (Table 2).
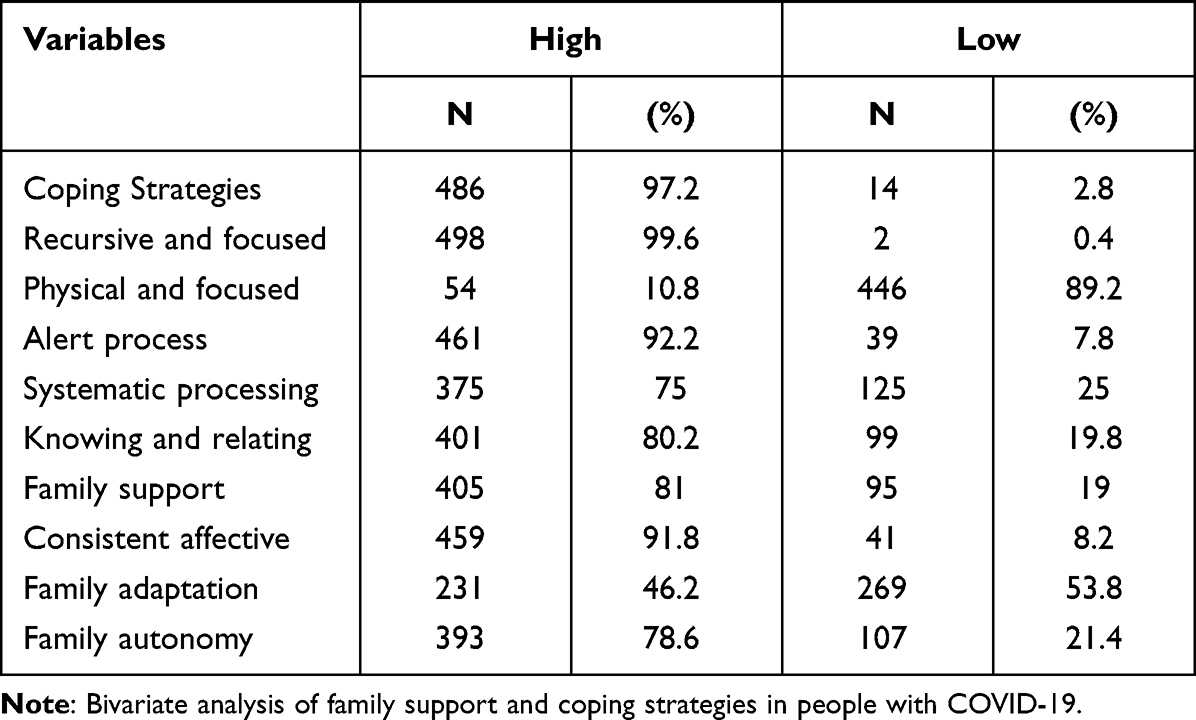 |
Table 2 Descriptive Analysis of the Variables Family Support and Coping Strategies in People with COVID-19 |
In the bivariate analysis with the chi-square test, it was found that there are significant differences between marital status (p=0.026), having children (p=0.037), family support (p=0.000) and its dimensions with coping strategies with a p-value ˂0.05 (Table 3).
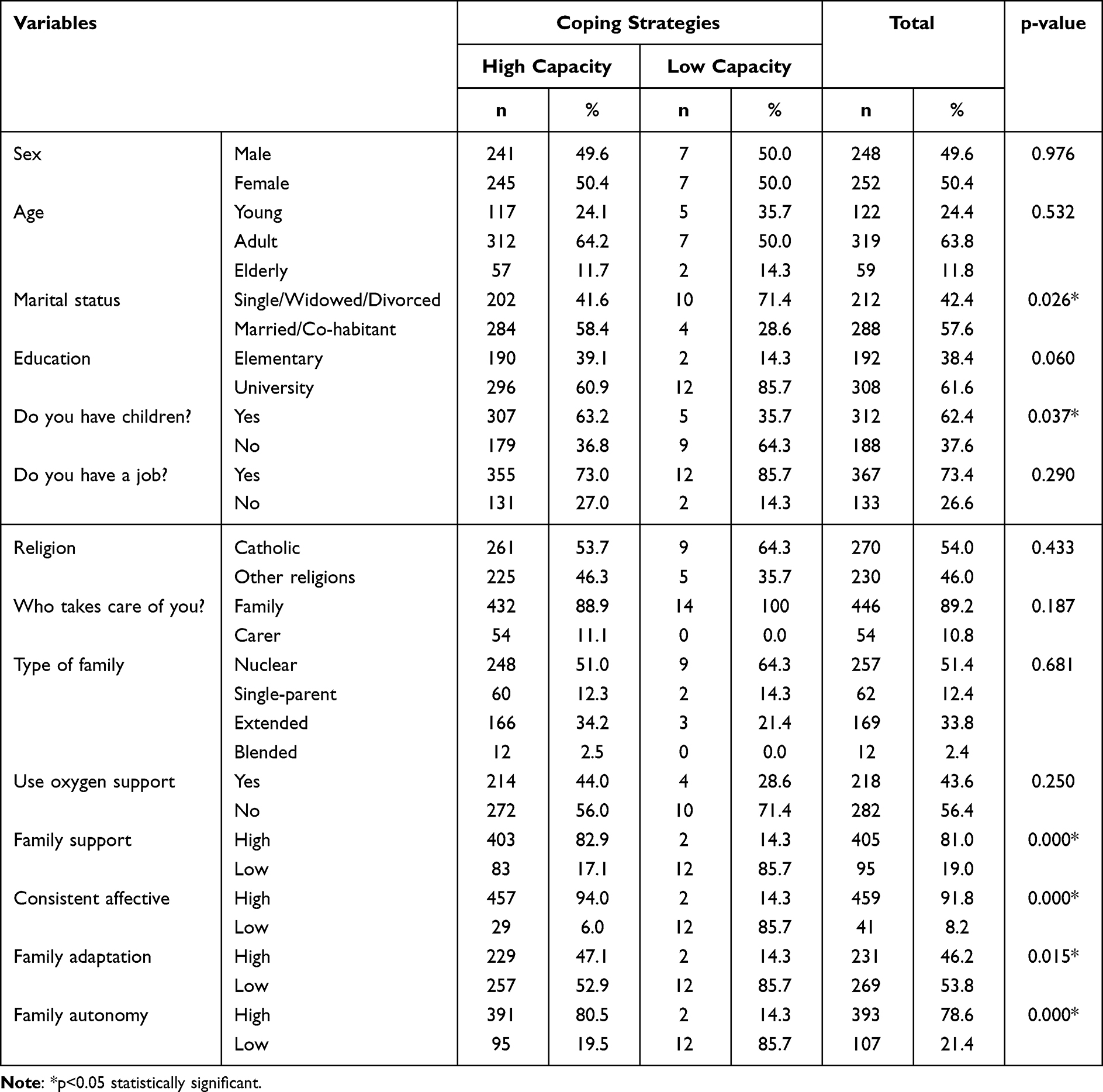 |
Table 3 Bivariate Analysis of Family Support and Coping Strategies in People with COVID-19 |
Lastly, the multivariate analysis found that people with COVID-19 who perceived high family support were 33.74 times (95% CI: 7266–156,739) more likely to have a high capacity for coping strategies (Table 4).
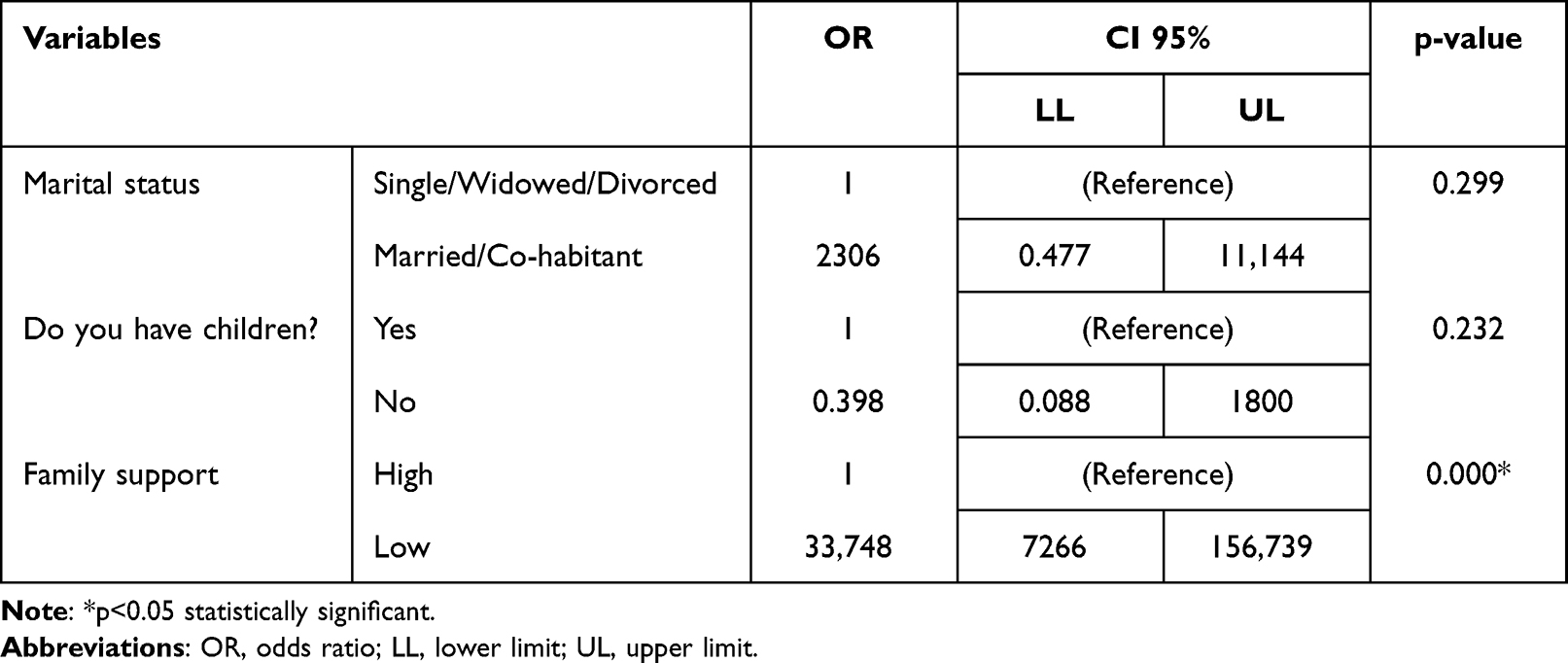 |
Table 4 Multivariate Analysis of Family Support and Coping Strategies in People with COVID-19 |
Discussion
Active coping strategies in stressful situations include positive thinking, optimism, acceptance, purpose in life, humor, positive planning and reframing, and social support.17 An essential element of social support is family support. Due to the negative psychological impact of the COVID-19 outbreak,18 needs to address ways to increase protective coping mechanisms that can improve health and possibly be used as a preventive measure in the future. This study showed that family support and its dimensions are associated with coping strategies. In addition, people with COVID-19 who perceived high family support were 33.74 times more likely to present a high capacity for coping strategies.
Coping strategies appear to have different effects on preventing or promoting psychological symptoms.19 Concerning the pandemic, a previous study showed that the coping strategies used by a sample of Peruvian families are similar to those used by other populations; however, the most prominent cross-cultural differences were observed in religious coping, which was the most common in Peru. The Catholicism practiced by the majority of the Peruvian population and the practices of praying for relief from difficulties and anguish could be the reason for the high prevalence of religious coping in Peru.20. The study found that 97.2% of the participants with COVID-19 presented a high capacity for coping strategies, highlighting their recursive and focused style. (Table 2). This factor is the primary dimension of the coping processing construct, which reflects accepting behaviors and resources used by oneself, focusing on being inventive, and seeking positive results.21 Similar results were found in a study carried out in Pakistan, in which most COVID-19 patients manifested high coping capacity, practicing more acceptance strategies and seeking social support.22 Something similar happened in Romania, where COVID-19 patients used significantly more emotion-focused and engagement coping strategies, in contrast to COVID-19 patients who developed post-traumatic disorder and used emotion-focused and disengagement strategies.23
On the other hand, a significant interaction between marital status and coping strategies was previously evidenced.24 This study found a significant relationship between married and/or cohabiting marital status and a high capacity for coping strategies (p=0.026) (Table 3). Similarly, a study in Turkey on patients with breast cancer revealed that being single and having a delay in diagnosis are related to negative coping, while married patients present positive coping.25 These results indicate the need for more outstanding care for patients without a partner to improve their coping strategies and adaptation to a crisis such as a disease caused by COVID-19.
As part of social support, family support is a multidimensional factor that depends on an individual’s self-perception of “how supported or lonely I feel”. Its importance lies in how to “help to cope” with the adverse effects of stress, which increases self-esteem and the feeling of control over the environment.26 In addition, it has been described that the regular implementation of family support for patients in intensive care increases the perception of the quality of care provided and decreases the length of stay and costs.27 On the other hand, the lack of family support strongly impacts mental and physical health, including premature death at rates comparable to obesity and smoking.28,29
Previous works show high levels of family support in studies carried out in Peruvian families with members with different chronic diseases and mental disorders.30,31 According to the survey applied by the World Values Survey (WVS), the majority of Peruvians consider the family and marriage as valuable institutions; this consideration is higher than the world average and could be a reason for the sound levels of family support observed in Peruvian families. This study found that 81% of the participants with COVID-19 perceived high family support, and family support and its three dimensions were significantly associated with a high capacity for coping strategies (Table 2 and Table 3). Similarly, a study in Indonesia revealed that good family support positively impacts the recovery of patients with COVID-19.32 Likewise, a study in Amsterdam found that patients with COVID-19 perceived family support from their relatives as positive, allowing them to reduce anguish and anxiety.33
Lastly, the multivariate analysis found that people with COVID-19 who perceived high family support were 33.74 times (95% CI: 7266–156,739) more likely to have a high capacity for coping strategies (Table 4). Similarly, a study on cancer patients in Indonesia found a strong and positive association between family support and the problem-focused coping strategy.34 At the same time, there was a significant negative association (p=0.001) and a moderate correlation (r=−0.462) with the coping strategy focused on emotion. Likewise, a study conducted on patients with bipolar disorder in Turkey determined that family functions affected the coping attitudes of patients, and those patients who healthily evaluated family functions made use of adaptive coping strategies to a greater extent.35 Moreover, a study in Semerag, Indonesia demonstrated a relationship between family support and coping mechanisms in patients with heart failure.36 Therefore, we believe that family support can improve the coping mechanisms of patients with COVID-19 because the family acts as a source of coping, so patients have coping mechanisms that are adaptable to deal with the disease and undergo the treatment and recovery process.37
Given the results obtained, some government actions should be carried out to develop family support skills in the population. Governments must implement legislation and finance programs dedicated to strengthening the families of their populations. Projects such as “CLOSE US”, a family-strengthening strategy promoted by the National Comprehensive Program for Family Well-being of the Ministry of Women and Vulnerable Populations of Peru, will help reinforce family functions of affection, training, socialization, care, and economic security; and thus promote family relationships that help its members have better-coping strategies in traumatic situations such as the one caused by the COVID-19 pandemic. For health personnel, the data from this study obtained at the population level show the need for intervention programs to strengthen the internal dynamics of families, especially those in situations of vulnerability and social risk. In addition, clinical staff should develop intervention programs to strengthen coping strategies, which could generate important inputs for mitigating the psychosocial consequences generated by the pandemic.
Our study has some limitations that must be considered. First, family support and coping strategies were assessed using a self-administered questionnaire. Therefore, the results may be vulnerable to bias due to social desirability effects or memory effects and the use of methodologies such as in-depth interviews. However, the fact that validated scales have been Used is a strength of the study. Second, it is a cross-sectional study; due to the health emergency context, it was not feasible to plan a longitudinal study. Therefore, confirming a causal relationship between the variables under study is impossible, and future longitudinal studies are recommended. Finally, the sample was non-probabilistic and did not allow extrapolation of the results. In addition, the sample was limited to one city in the country However, it is true that it is the capital and is home to 30% of the Peruvian population, the results cannot be generalized. Future studies should consider providing evidence that can be generalized to patients nationally and from other regions.
Conclusion
This study showed that family support and its dimensions are associated with coping strategies; in addition, people with COVID-19 who perceived high family support were 33.74 times more likely to present a high capacity for coping strategies. These findings are expected to promote the implementation and development of parental and family support skills to improve coping skills and adaptation to the disease in patients with COVID-19.
Data Sharing Statement
The original data used to support the findings of this study are available from the corresponding authors upon request.
Ethical Statement
All procedures were performed following the 1964 Helsinki Declaration and its later amendments.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stanisławski K. The coping circumplex model: an integrative model of the structure of coping with stress. Front Psychol. 2019;10:694. doi:10.3389/fpsyg.2019.00694
2. Talebi SS, Hosseinzadeh A, Zare F, et al. Risk factors associated with mortality in COVID-19 patient’s: survival analysis. Iran J Public Health. 2022;51(3):652–658. doi:10.18502/ijph.v51i3.8942
3. Bhaskaran K, Bacon S, Evans SJ, et al. Factors associated with deaths due to COVID-19 versus other causes: population-based cohort analysis of UK primary care data and linked national death registrations within the OpenSAFELY platform. Lancet Reg Health Eur. 2021;6:100109. doi:10.1016/j.lanepe.2021.100109
4. Girma A, Ayalew E, Mesafint G. Covid-19 pandemic-related stress and coping strategies among adults with chronic disease in Southwest Ethiopia. Neuropsychiatr Dis Treat. 2021;17:1551–1561. doi:10.2147/NDT.S308394
5. Agbaria Q, Mokh AA. Coping with stress during the coronavirus outbreak: the contribution of big five personality traits and social support. Int J Ment Health Addict. 2022;20(3):1854–1872. doi:10.1007/s11469-021-00486-2
6. Sica C, Latzman RD, Caudek C, et al. Facing distress in Coronavirus era: the role of maladaptive personality traits and coping strategies. Pers Individ Dif. 2021;177:110833. doi:10.1016/j.paid.2021.110833
7. Baca-Romero D, Aiquipa-Tello J, Barboza-Palomino M, Ibañez-Montoya J, Oré-Pacheco L. Psychological impact and coping strategies in peruvian adults during the Covid-19 pandemic. Index de Enfermeria. 2022:31(2):1–9.
8. Sampogna G, Del Vecchio V, Giallonardo V, et al. What is the role of resilience and coping strategies on the mental health of the general population during the COVID-19 pandemic? Results from the Italian Multicentric COMET Study. Brain Sci. 2021;11(9):1231. doi:10.3390/brainsci11091231
9. Menculini G, Albert U, Bianchini V, et al. Did we learn something positive out of the COVID-19 pandemic? Post-traumatic growth and mental health in the general population. Eur Psychiatry. 2021;64(1):e79. doi:10.1192/j.eurpsy.2021.2263
10. Rahimi T, Dastyar N, Rafati F. Experiences of family caregivers of patients with COVID-19. BMC Fam Pract. 2021;22(1):137. doi:10.1186/s12875-021-01489-7
11. Wang YN, Yuan ZJ, Leng WC, et al. Role of perceived family support in psychological distress for pregnant women during the COVID-19 pandemic. World J Psychiatry. 2021;11(7):365–374. doi:10.5498/wjp.v11.i7.365
12. Verberk JDM, Anthierens SA, Tonkin-Crine S, et al. Experiences and needs of persons living with a household member infected with SARS-CoV-2: a mixed method study. PLoS One. 2021;16(3):e0249391. doi:10.1371/journal.pone.0249391
13. Majid A, Suhaff AA, Teli BA, Rafiq F, Bhat A. Impact of COVID-19 pandemic on grief, death, mourning, and coping. Indian J Psychiatry. 2022;64(6):555–559. doi:10.4103/indianjpsychiatry.indianjpsychiatry_124_22
14. Jeitziner MM, Jenni-Moser B, Zante B, et al. Family support in intensive care units during COVID-19 visit ban: a multinational Delphi Study during first COVID-19 wave. Intensive Crit Care Nurs. 2023;74:103308. doi:10.1016/j.iccn.2022.103308
15. Leyva Terrones EF. Percepción del apoyo familiar en los pacientes del Centro de Salud “La Tulpuna”, en la provincia de Cajamarca, periodo 2019 [Perception of family support in patients at the “La Tulpuna” Health Center, in the province of Cajamarca, 2019]; 2019. Spanish.
16. Sarmiento González P, Botero Giraldo J, Carvajal Carrascal G. Validez de constructo de la Escala de Medición del Proceso de Afrontamiento y Adaptación de Roy, versión modificada en español. Index de Enfermería. 2013;22(4):233–236. doi:10.4321/S1132-12962013000300009
17. Rodríguez-Rey R, Palacios A, Alonso-Tapia J, et al. Burnout and posttraumatic stress in paediatric critical care personnel: prediction from resilience and coping styles. Aust Crit Care. 2019;32(1):46–53. doi:10.1016/j.aucc.2018.02.003
18. Olarte-Durand M, Roque-Aycachi JB, Rojas-Humpire R, et al. Estado de Ánimo y Calidad del Sueno˜ de Estudiantes de Medicina Peruanos Durante la Pandemia de COVID-19 [Mood and sleep quality in Peruvian medical students during COVID-19 pandemic]. Rev Colomb Psiquiatr. 2021. Spanish. doi:10.1016/j.rcp.2021.11.010
19. Mariani R, Renzi A, Di Trani M, Trabucchi G, Danskin K, Tambelli R. The impact of coping strategies and perceived family support on depressive and anxious symptomatology during the Coronavirus pandemic (COVID-19) lockdown. Front Psychiatry. 2020;11:587724. doi:10.3389/fpsyt.2020.587724
20. Voronin IA, Manrique-Millones D, Vasin GM, et al. Coping responses during the COVID-19 pandemic: a cross-cultural comparison of Russia, Kyrgyzstan, and Peru. Psychol Russia State Art. 2020;13(4):55–74. doi:10.11621/pir.2020.0404
21. Roy C, Bakan G, Li Z, Nguyen TH. Coping measurement: creating short form of Coping and Adaptation Processing Scale using item response theory and patients dealing with chronic and acute health conditions. Appl Nurs Res. 2016;32:73–79. doi:10.1016/j.apnr.2016.06.002
22. Baloch GM, Kamaludin K, Chinna K, et al. Coping with COVID-19: the strategies adapted by pakistani students to overcome implications. Int J Environ Res Public Health. 2021;18(4):1799. doi:10.3390/ijerph18041799
23. Dehelean L, Papava I, Musat MI, et al. Coping strategies and stress related disorders in patients with COVID-19. Brain Sci. 2021;11(10):1287. doi:10.3390/brainsci11101287
24. Napora E, Andruszkiewicz A, Basińska MA. Types of work-related behavior and experiences and stress coping strategies among single mothers and mothers in relationships differentiating role of work satisfaction. Int J Occup Med Environ Health. 2018;31(1):55–69. doi:10.13075/ijomeh.1896.01052
25. Kelkil BA, Atnafu NT, Dinegde NG, Wassie M. Coping strategies of stress and its associated factors among breast cancer patients in Tikur Anbesa specialized hospital, Ethiopia: institution-based cross-sectional study. BMC Womens Health. 2022;22(1):252. doi:10.1186/s12905-022-01792-0
26. Burke C, Hampel S, Gholson K, Zhang P, Rufkhar B. COVID-19 family support team: providing person and family centered care during the COVID-19 pandemic. J Soc Work End Life Palliat Care. 2021;17(2–3):158–163. doi:10.1080/15524256.2021.1922126
27. Shelton W, Moore CD, Socaris S, Gao J, Dowling J. The effect of a family support intervention on family satisfaction, length-of-stay, and cost of care in the intensive care unit. Crit Care Med. 2010;38(5):1315–1320. doi:10.1097/CCM.0b013e3181d9d9fe
28. Sunday S, Kabir Z. Impact of Carers’ smoking status on childhood obesity in the growing up in Ireland Cohort Study. Int J Environ Res Public Health. 2019;16(15):2759. doi:10.3390/ijerph16152759
29. Compton MT, Daumit GL, Druss BG. Cigarette smoking and overweight/obesity among individuals with serious mental illnesses: a preventive perspective. Harv Rev Psychiatry. 2006;14(4):212–222. doi:10.1080/10673220600889256
30. Pesantes MA, Del Valle A, Diez-Canseco F, et al. Family support and diabetes: patient’s experiences from a public hospital in Peru. Qual Health Res. 2018;28(12):1871–1882. doi:10.1177/1049732318784906
31. Luna Matos ML, Salinas Piélago J, Luna Figueroa A. Depresión mayor en embarazadas atendidas en el Instituto Nacional Materno Perinatal de Lima, Perú. Revista Panamericana de salud pública. 2009;26(4):310–314. doi:10.1590/S1020-49892009001000004
32. Wardani DS, Arifin S. The role of family support in the recovery of Corona Virus Disease-19 patients. Open Access Macedonian J Med Sci. 2021;9(E):1005–1009. doi:10.3889/oamjms.2021.6025
33. Klop HT, Nasori M, Klinge TW, et al. Family support on intensive care units during the COVID-19 pandemic: a qualitative evaluation study into experiences of relatives. BMC Health Serv Res. 2021;21(1):1060. doi:10.1186/s12913-021-07095-8
34. Sari DK, Dewi R, Daulay W. Association between family support, coping strategies and anxiety in cancer patients undergoing chemotherapy at general hospital in Medan, North Sumatera, Indonesia. Asian Pac J Cancer Prev. 2019;20(10):3015–3019. doi:10.31557/APJCP.2019.20.10.3015
35. Çuhadar D, Savaş HA, Ünal A, Gökpınar F. Family functionality and coping attitudes of patients with bipolar disorder. J Relig Health. 2015;54(5):1731–1746. doi:10.1007/s10943-014-9919-y
36. Ryandini FR. Family support and coping mechanism in congestive heart failure patient. Health Sci J. 2020;14(6):1–4.
37. Boatemaa Benson R, Cobbold B, Opoku Boamah E, Akuoko CP, Boateng D. Challenges, coping strategies, and social support among breast cancer patients in Ghana. Adv Public Health. 2020;2020:1–11. doi:10.1155/2020/4817932
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.