Back to Journals » Clinical Interventions in Aging » Volume 17
Association Between Dynapenic Abdominal Obesity and Fall Risk in Older Adults
Received 31 October 2021
Accepted for publication 28 February 2022
Published 7 April 2022 Volume 2022:17 Pages 439—445
DOI https://doi.org/10.2147/CIA.S347053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi-Ying Wu
Danmei Lv, Shanshan Shen, Xujiao Chen
Department of Geriatrics, Zhejiang Hospital, Hangzhou, 310013, People’s Republic of China
Correspondence: Xujiao Chen, Department of Geriatrics, Zhejiang Hospital, Lingyin Road #12, Hangzhou, 310013, People’s Republic of China, Email [email protected]
Background: In recent years, dynapenic abdominal obesity has received more and more attention. This article aimed to explore the relationship between dynapenic abdominal obesity and fall risk in older adults.
Methods: In this cross-sectional study, according to waist circumference (≥ 90 cm for men and ≥ 85 cm for women) and handgrip strength (< 28 kg for men and < 18 kg for women), 551 older adults were divided into four groups: dynapenic abdominal obese (D/AO), dynapenic nonabdominal obese (D/NAO), nondynapenic abdominal obese (ND/AO) and nondynapenic nonabdominal obese (ND/NAO). Fall risk was measured by the Tinetti performance-oriented mobility assessment (POMA). Binary logistic regression was used to explore the relationship between D/AO and fall risk.
Results: D/AO was related to POMA score (odds ratio [OR]=3.39; 95% confidence interval [CI]: 1.47– 7.81; P=0.004) after adjusting the confounding variables. However, D/NAO (OR=1.51; 95% CI:0.69– 3.32; P=0.302) and ND/AO (OR=1.48; 95% CI:0.74– 2.99; P=0.272) were not associated with POMA score.
Conclusion: This study suggests that older adults with D/AO have a higher risk of falls. Therefore, it is necessary to strengthen the attention to D/AO and relevant interventions should be implemented.
Keywords: dynapenic abdominal obesity, fall risk, older adult
Introduction
The global population is aging. At present, about 11% of the world’s population is over 60 years old, and it is expected that this proportion will rise to 22% by 2050.1 As we all know, balance and gait disturbance is common in older people and is the potential cause of falls.2,3 Tinetti performance-oriented mobility assessment (POMA), which includes balance and gait subscales, is widely used to assess a patient's fall risk.43 Among older adults, falls are the main cause of accidental injuries and injury-related deaths, consuming a lot of medical resources.4,5 Therefore, fall risk assessment need to be taken seriously in older adults.
At present, the prevalence of overweight and obesity worldwide is increasing and almost a third of the world’s population is classified as overweight or obese.6 Obesity is related to functional limitation, disability and poorer quality of life.7 In older adults, the proportion of body fat, especially abdominal fat, increases with age. Therefore, based on height and weight, body mass index (BMI) cannot accurately measure the changes in body fat.8,9 Waist circumference is considered to be a substitute for measuring fat distribution. It is widely used to diagnose abdominal obesity and may be a better measure of obesity in older adults.9
With age, human muscle strength and muscle mass decrease. Previous studies have suggested that age-related muscle mass decrease is the main cause of insufficient muscle strength,10,11 but recent studies have shown that muscle mass decrease has a relatively small effect on the loss of muscle strength.12,13 The relationship between muscle strength and muscle volume is not linear14 and the decline in muscle strength is much faster than the decline in muscle mass.15 Studies have shown that physical function is more affected by muscle strength, rather than muscle mass.16,17 Newman et al18 pointed out that muscle strength rather than muscle mass was related to mortality. In predicting health-related outcomes in older people, muscle strength was better than muscle mass.19,20 Therefore, dynapenia was proposed to define age-related loss of muscle strength.21,22
Previous studies separately explored the effects of abdominal obesity and dynapenia. It was found that abdominal obesity had a greater impact on metabolic disorders,23 had independent effects on functional limitations and disability,24–26 and was associated with mortality.27 And dynapenia increased the risk for functional limitations, disability, and mortality.22 However, recent studies have found that the simultaneous presence of abdominal obesity and dynapenia have a greater adverse effect. Studies have shown that patients with dynapenic abdominal obese (D/AO) had a higher prevalence of metabolic syndrome,28,29 a higher risk of falls and fall events,30–32 a faster decline in walking speed,32,33 a higher risk of functional decline,34,35 and a higher rate of disability, mortality and hospitalization.36–38 Among older women, patients with D/AO were associated with increased risk and fear of falls and reduced dynamic balance.39
As we known that falls affect the clinical prognosis of older adults. And D/AO has an important impact on physical function. However, only a few studies have directly investigated the relationship between D/AO and fall risk, and there are no previous studies conducted in Asian population. Therefore, this article tries to explore the relationship between D/AO and fall risk in Chinese people, so as to find potential ways to prevent falls in older people.
Methods
Participants
This was a cross-sectional study. The 551 participants were selected from inpatients and outpatients in the geriatric department of Zhejiang Hospital in China from October 2014 to July 2019, who had completed a comprehensive geriatric assessment (CGA). The CGA was performed by a professional geriatric assessment team. The inclusion criteria were as follows: (1) Aged 65 years or older; (2) Ability to walk independently (walking aids such as cane were allowed); (3) Able to understand and communicate in Chinese. The exclusion criteria were as follows: (1) severe acute infection, uncontrolled malignant tumor, severe heart, lung or kidney disease, Parkinson’s disease or Parkinson’s syndrome, cerebellar disease, acute cerebrovascular disease, delirium, terminal illness; (2) severe vision or hearing impairment; (3) severe cognitive impairment (Mini-Mental State Examination (MMSE) score ≤10 points). This study was in compliance with the Declaration of Helsinki and was approved by the medical ethics committees of Zhejiang Hospital. Each subject signed a written informed consent.
Classification of the Groups
Waist circumference was measured at the level of umbilicus. According to the unique standards of abdominal obesity in Asia, abdominal obesity is defined as WC≥90 cm for men and WC≥85 cm for women.40,41 And handgrip strength was measured using a dynamometer (the Camry EH101 Electronic Hand Dynamometer). Participants did it three times with their dominant hand, and the best result of the test was recorded. According to Asian Working Group for Sarcopenia (AWGS), low muscle strength is defined as handgrip strength <28 kg for men and <18 kg for women.42 According to the grouping criteria of waist circumference and handgrip strength, the participants were divided into four groups: D/AO, D/NAO, ND/AO and ND/NAO.
Fall risk Assessment
The fall risk was measured with POMA, which includes balance and gait subscales.43 The balance subscale includes nine components: sitting balance, arises, attempts to arise, immediate standing balance, standing balance, nudged, eyes closed, turning 360°, and sitting down, with a maximum score of 16 points. And the gait subscale consists of seven components: initiation of gait, step length, step symmetry, step continuity, path, trunk, and walking stance, with a maximum score of 12 points. The total score is the sum of the two subscale scores with a maximum score of 28. The total score is associated with different levels of fall risks, from low risk (>24) to medium or high risk (0–24).
Covariates
The covariates included in this analysis constitute a broad range of factors related to fall risk.3 The demographic data were collected including: age, gender, education level, marital status, BMI, smoking, drinking, hearing, vision, comorbidity, polypharmacy and orthostatic hypotension. The oldest old was defined as 80 years old and over.44 So the cut-off point for age here was 80 years old. BMI was calculated by weight/height2. The World Health Organization recommends that the definition of overweight is BMI ≥ 25 kg/m2.45 Comorbidity was referred to the clinical diagnosis of 5 or more diseases.46 Polypharmacy was defined as the patient taking 5 or more oral prescription drugs.47 Orthostatic hypotension was defined as a at least 20 mmHg drop in systolic blood pressure or 10 mmHg drop in diastolic blood pressure within 3 minutes of standing position in the orthostatic test.48 The history of falls in the past year, fear of falling and walking aids were also recorded. A fall is a sudden, involuntary, or unintentional change in body position, falling to the ground or a lower surface.49 Furthermore, the gait speed (m/s) was calculated using a four-meter gait speed test. Slow gait speed was defined as <1 m/s.42
In addition, the 15-item Geriatric Depression Scale (GDS-15) was used to screen for the symptoms of depression in older people, and the sum of score≥6 points was considered to have depressive symptoms.50 Cognitive function was assessed using the MMSE and the score ≤24 was considered to have cognitive impairment.51 Nutritional status was assessed by the Mini Nutritional Assessment-Short Form (MNA-SF), and patients with the score≤11 points was considered to be at risk of malnutrition.52
Statistical Analysis
Statistical analysis was performed using SPSS 23.0 software. All the data was expressed as a percentage or constituent ratio and the chi-square was used to determine the significant difference among the four groups. In addition, binary logistic regression conducted with 2 models was used to analyze the relationship between D/AO and POMA score, expressed in odds ratios (ORs) and 95% confidence intervals (CIs). Model 1 was not adjusted for covariates and Model 2 was adjusted for age, sex, marital status, education, BMI, smoking, drinking, hearing, eyesight, orthostatic hypotension, comorbidities, polypharmacy, walking aids, history of falls, fear of falling, four-meter walk, MMSE scores, GDS-15 scores, MNA-SF scores. Two-tailed tests were used for all significance tests, and P <0.05 was considered a significant difference.
Results
A total of 551 people were included in the study, including 105 people with D/AO, 79 with D/NAO, 194 with ND/AO and 173 with ND/NAO. As can be seen in Table 1, the four groups had differences in age, gender, marriage status, BMI, comorbidities, polypharmacy, walking aids, history of falls, fear of falling, four-meter gait speed, MMSE scores, MNA-SF scores and POMA scores (all with P<0.05). And there were no significant differences in education level, smoking history, alcohol drinking history, hearing, eyesight, orthostatic hypotension or GDS-15 scores (all with P>0.05).
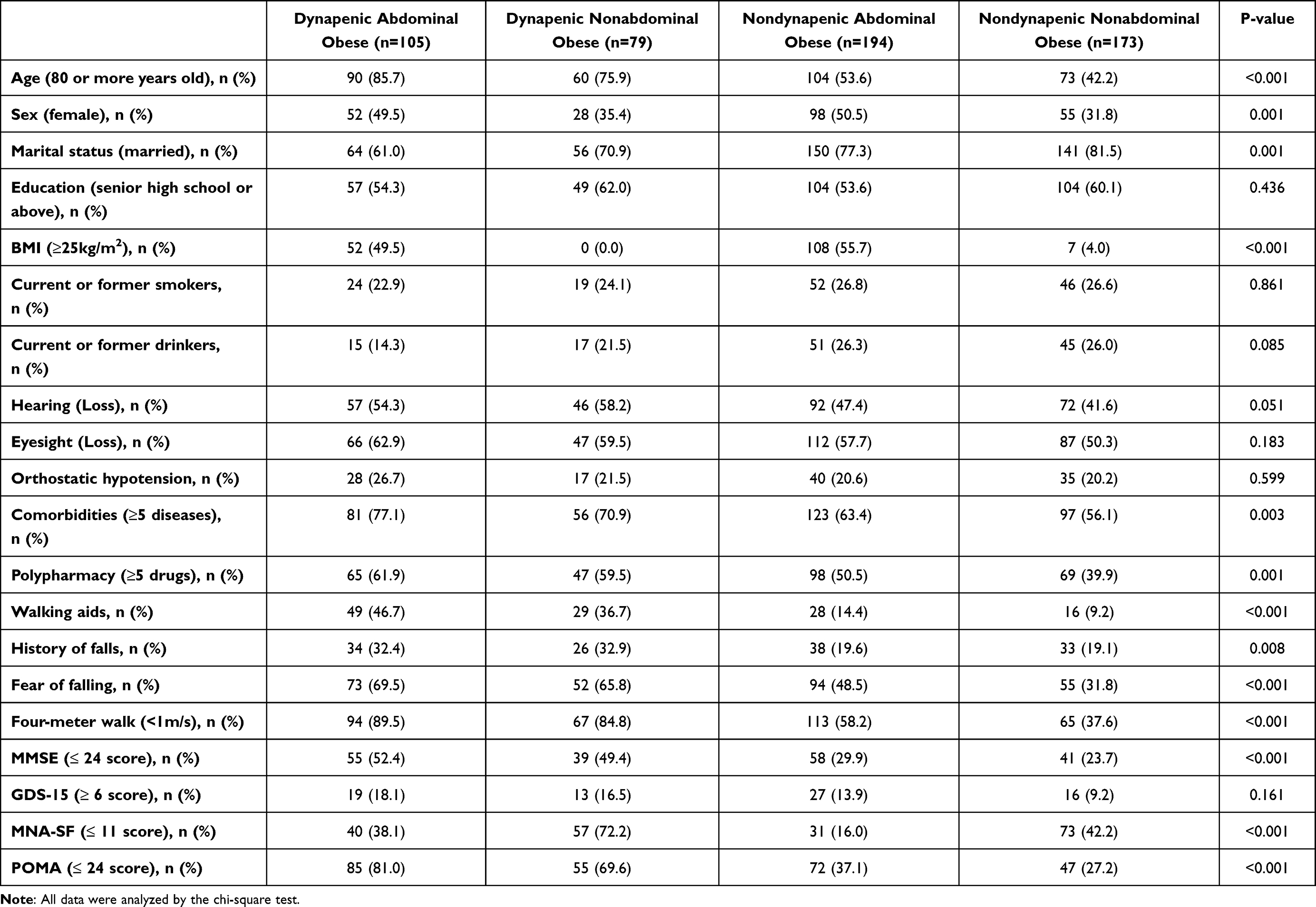 |
Table 1 Characteristics of Older Adults According to Abdominal Obesity and Dynapenia Status |
Then, binary logistic regression analysis was performed between fall risk (POMA score≤ 24) and D/AO (Table 2). Model 1 without adjusting covariates was a crude model and it was showed that D/AO (OR: 11.39, 95% CI: 6.31–20.58; P<0.001), D/NAO (OR: 6.14, 95% CI: 3.42–11.03; P<0.001) and ND/AO (OR:1.58, 95% CI: 1.02–2.47; P=0.043) were all associated with increased fall risk. Model 2 found that only D/AO (OR:3.39, 95% CI: 1.47–7.81; P=0.004) was associated with increased fall risk adjusted for age, sex, marital status, education, BMI, smoking, drinking, hearing, eyesight, orthostatic hypotension, comorbidities, polypharmacy, walking aids, history of falls, fear of falling, four-meter walk, MMSE scores, GDS-15 scores, MNA-SF scores.
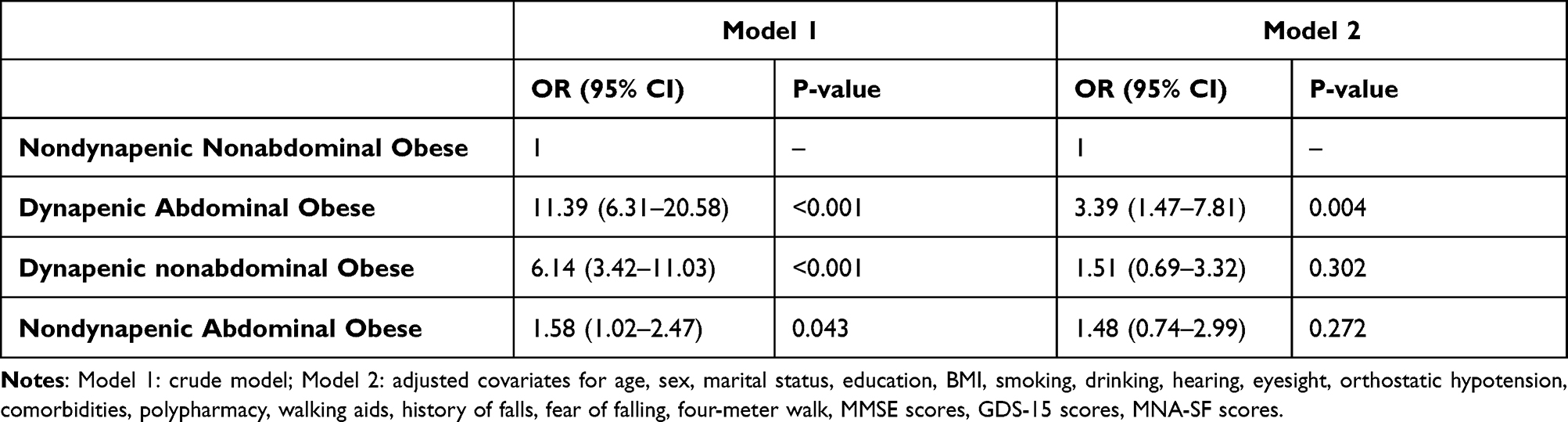 |
Table 2 Association Between Fall Risk and Dynapenic Abdominal Obesity |
Discussion
This article found that D/AO was associated with increased fall risk in older adults, and the result remained unchanged even after adjusting for confounding variables. It suggests that the coexistence of decreased muscle strength and central obesity may have more important clinical application value in older people.
Previous studies have found that abdominal obesity is related to falls.53 The possible mechanism is that the weight center of obese people is farther from the ankle joint. Therefore, compared with people of normal weight, they need a larger corrective ankle joint torque to offset the greater gravitational torque.54 And dynapenia is the age-associated loss of muscle strength,21 which is an important contributor to balance and gait problems, causing the occurrence of falls.55 Our research found that D/AO, D/NAO and ND/AO were all associated with increased fall risk. However, when the confounding variables were controlled, only D/AO was related to increased fall risk. This may be related to the characteristics of our subjects, and it was also showed that D/AO had a greater impact on fall risk.
Falls have caused a heavy economic burden on society.4 Previous articles have attempted to explore the relationship between D/AO and falls. Gadelha et al30 found that in a total of 201 older women, D/AO was more closely related to falls than either dynapenia or abdominal obesity alone, and was independently associated with an increased incidence of falls. And Máximo et al31 analyzed the data from 1046 community-dwelling participants and discovered that there was a stronger association between D/AO and a single fall. The above results are consistent with our study.
In addition, studies have tried to explore the relationship between D/AO and falls-related phenotype. Pereira et al39 found that D/AO was associated with increased risk and fear of falls and reduced dynamic balance in 217 older women. Zhang et al.32 found that D/AO exhibited worse gait speed and increased the risk of fall events in older adults.Our article found that D/AO was related to increased fall risk in Chinese older adults. Fall risk was assessed by POMA, which includes balance and gait subscales. It suggested that D/AO may have poorer balance and gait, which may provide a potential direction for prevention of falls in older adults.
This article has some advantages. Firstly, the data measuring method in the article is easy, which is convenient for clinical implementation. Secondly, we grouped D/AO, D/NAO, ND/AO and ND/NAO according to Asian demographic standards, which is more in line with the characteristics of Chinese people. Also, this study has some limitations. First of all, this is a cross-sectional study and we cannot determine the causal relationship between D/AO and fall risk. Second, our subjects were selected from inpatients and outpatients in the same hospital, and the differences between inpatients and outpatients were not analyzed, which affected the generalizability of our results. Therefore, prospective studies with more representative subjects are needed to further explore the relationship between D/AO and fall risk.
Conclusions
This article found that older adults with D/AO had a higher risk of falls. Therefore, D/AO in older adults should be taken seriously and corresponding intervention measures such as increasing muscle strength and controlling abdominal obesity should be taken, which will help prevent falls in older people.
Acknowledgments
The study was supported by the Science Technology Department of Zhejiang Province (2014C33241), the National Health and Family Planning Commission of Scientific Research Fund of People’s Republic of China (WKJ2013–2-001) and National Key R&D Program of China (Grant 2020YFC2008606).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Newgard CB, Sharpless NE. Coming of age: molecular drivers of aging and therapeutic opportunities. J Clin Invest. 2013;123(3):946–950. doi:10.1172/JCI68833
2. Ambrose AF, Paul G, Hausdorff JM. Risk factors for falls among older adults: a review of the literature. Maturitas. 2013;75(1):51–61. doi:10.1016/j.maturitas.2013.02.009
3. Cuevas-Trisan R. Balance problems and fall risks in the elderly. Phys Med Rehabil Clin N Am. 2017;28(4):727–737. doi:10.1016/j.pmr.2017.06.006
4. Heinrich S, Rapp K, Rissmann U, et al. Cost of falls in old age: a systematic review. Osteoporos Int. 2010;21(6):891–902. doi:10.1007/s00198-009-1100-1
5. Gelbard R, Inaba K, Okoye OT, et al. Falls in the elderly: a modern look at an old problem. Am J Surg. 2014;208(2):249–253. doi:10.1016/j.amjsurg.2013.12.034
6. Chooi YC, Ding C, Magkos F. The epidemiology of obesity. Metabolism. 2019;92:6–10. doi:10.1016/j.metabol.2018.09.005
7. Samper-Ternent R, Al Snih S. Obesity in older adults: epidemiology and implications for disability and disease. Rev Clin Gerontol. 2012;22(1):10–34. doi:10.1017/S0959259811000190
8. Rothman KJ. BMI-related errors in the measurement of obesity. Int J Obes. 2008;32(Suppl 3):S56–S59. doi:10.1038/ijo.2008.87
9. Zamboni M, Mazzali G, Zoico E, et al. Health consequences of obesity in the elderly: a review of four unresolved questions. Int J Obes. 2005;29(9):1011–1029. doi:10.1038/sj.ijo.0803005
10. Frontera WR, Hughes VA, Lutz KJ, et al. A cross-sectional study of muscle strength and mass in 45- to 78-yr-old men and women. J Appl Physiol. 1991;71(2):644–650. doi:10.1152/jappl.1991.71.2.644
11. Reed RL, Pearlmutter L, Yochum K, et al. The relationship between muscle mass and muscle strength in the elderly. J Am Geriatr Soc. 1991;39(6):555–561. doi:10.1111/j.1532-5415.1991.tb03592.x
12. Beliaeff S, Bouchard DR, Hautier C, et al. Association between muscle mass and isometric muscle strength in well-functioning older men and women. J Aging Phys Act. 2008;16(4):484–493. doi:10.1123/japa.16.4.484
13. Barbat-Artigas S, Rolland Y, Vellas B, et al. Muscle quantity is not synonymous with muscle quality. J Am Med Dir Assoc. 2013;14(11):852 e1–7. doi:10.1016/j.jamda.2013.06.003
14. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European working group on sarcopenia in older people. Age Ageing. 2010;39(4):412–423. doi:10.1093/ageing/afq034
15. Goodpaster BH, Park SW, Harris TB, et al. The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study. J Gerontol a Biol Sci Med Sci. 2006;61(10):1059–1064. doi:10.1093/gerona/61.10.1059
16. Pisciottano MV, Pinto SS, Szejnfeld VL, et al. The relationship between lean mass, muscle strength and physical ability in independent healthy elderly women from the community. J Nutr Health Aging. 2014;18(5):554–558. doi:10.1007/s12603-013-0414-z
17. Schaap LA, Koster A, Visser M. Adiposity, muscle mass, and muscle strength in relation to functional decline in older persons. Epidemiol Rev. 2013;35(1):51–65. doi:10.1093/epirev/mxs006
18. Newman AB, Kupelian V, Visser M, et al. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J Gerontol a Biol Sci Med Sci. 2006;61(1):72–77. doi:10.1093/gerona/61.1.72
19. Menant JC, Weber F, Lo J, et al. Strength measures are better than muscle mass measures in predicting health-related outcomes in older people: time to abandon the term sarcopenia? Osteoporos Int. 2017;28(1):59–70. doi:10.1007/s00198-016-3691-7
20. Visser M, Goodpaster BH, Kritchevsky SB, et al. Muscle mass, muscle strength, and muscle fat infiltration as predictors of incident mobility limitations in well-functioning older persons. J Gerontol a Biol Sci Med Sci. 2005;60(3):324–333. doi:10.1093/gerona/60.3.324
21. Clark BC, Manini TM. Sarcopenia =/= dynapenia. J Gerontol a Biol Sci Med Sci. 2008;63(8):829–834. doi:10.1093/gerona/63.8.829
22. Clark BC, Manini TM. What is dynapenia? Nutrition. 2012;28(5):495–503. doi:10.1016/j.nut.2011.12.002
23. Janssen I, Katzmarzyk PT, Ross R. Waist circumference and not body mass index explains obesity-related health risk. Am J Clin Nutr. 2004;79(3):379–384. doi:10.1093/ajcn/79.3.379
24. Houston DK, Stevens J, Cai J. Abdominal fat distribution and functional limitations and disability in a biracial cohort: the atherosclerosis risk in communities study. Int J Obes. 2005;29(12):1457–1463. doi:10.1038/sj.ijo.0803043
25. Corona LP, Alexandre TDS, de Oliveira Duarte YA, Lebrão ML, et al. Abdominal obesity as a risk factor for disability in Brazilian older adults. Public Health Nutr. 2017;20(6):1046–1053. doi:10.1017/S1368980016003505
26. Angleman SB, Harris TB, Melzer D. The role of waist circumference in predicting disability in periretirement age adults. Int J Obes. 2006;30(2):364–373. doi:10.1038/sj.ijo.0803130
27. Koster A, Leitzmann MF, Schatzkin A, et al. Waist circumference and mortality. Am J Epidemiol. 2008;167(12):1465–1475. doi:10.1093/aje/kwn079
28. Alexandre TDS, Aubertin-Leheudre M, Carvalho LP, et al. Dynapenic obesity as an associated factor to lipid and glucose metabolism disorders and metabolic syndrome in older adults - findings from SABE study. Clin Nutr. 2018;37(4):1360–1366. doi:10.1016/j.clnu.2017.06.009
29. Sénéchal M, Dionne IJ, Brochu M. Dynapenic abdominal obesity and metabolic risk factors in adults 50 years of age and older. J Aging Health. 2012;24(5):812–826. doi:10.1177/0898264312440324
30. Gadelha AB, Neri SGR, Vainshelboim B, et al. Dynapenic abdominal obesity and the incidence of falls in older women: a prospective study. Aging Clin Exp Res. 2020;32(7):1263–1270. doi:10.1007/s40520-019-01318-z
31. Maximo RO, Santos JLF, Perracini MR, et al. Abdominal obesity, dynapenia and dynapenic-abdominal obesity as factors associated with falls. Braz J Phys Ther. 2019;23(6):497–505. doi:10.1016/j.bjpt.2018.10.009
32. Zhang L, Liu S, Wang W, et al. Dynapenic abdominal obesity and the effect on long-term gait speed and falls in older adults. Clin Nutr. 2022;41(1):91–96. doi:10.1016/j.clnu.2021.11.011
33. De oliveira maximo R, de Oliveira DC, Ramírez PC, et al. Dynapenia, abdominal obesity or both: which accelerates the gait speed decline most? Age Ageing. 2021;50(5):1616–1625. doi:10.1093/ageing/afab093
34. Alexandre TDS, Scholes S, Santos JLF, et al. Dynapenic abdominal obesity as a risk factor for worse trajectories of ADL disability among older adults: the ELSA cohort study. J Gerontol a Biol Sci Med Sci. 2019;74(7):1112–1118. doi:10.1093/gerona/gly182
35. Alexandre TDS, Scholes S, Ferreira santos JL, et al. The combination of dynapenia and abdominal obesity as a risk factor for worse trajectories of IADL disability among older adults. Clin Nutr. 2018;37(6):2045–2053. doi:10.1016/j.clnu.2017.09.018
36. Rossi AP, Bianchi L, Volpato S, et al. Dynapenic abdominal obesity as a predictor of worsening disability, hospitalization, and mortality in older adults: results from the inchianti study. J Gerontol a Biol Sci Med Sci. 2017;72(8):1098–1104. doi:10.1093/gerona/glw203
37. Rossi AP, Fantin F, Caliari C, et al. Dynapenic abdominal obesity as predictor of mortality and disability worsening in older adults: a 10-year prospective study. Clin Nutr. 2016;35(1):199–204. doi:10.1016/j.clnu.2015.02.005
38. Rossi AP, Urbani S, Fantin F, et al. Worsening disability and hospitalization risk in sarcopenic obese and dynapenic abdominal obese: a 5.5 years follow-up study in elderly men and women. Front Endocrinol. 2020;11:314. doi:10.3389/fendo.2020.00314
39. Pereira JC, de Moraes Elias J, Neri SGR, et al. Dynapenic abdominal obesity as a risk factor for falls in older women. Top Geriatr Rehabil. 2019;35(2):149–155. doi:10.1097/TGR.0000000000000225
40. Lee SY, Park HS, Kim DJ, et al. Appropriate waist circumference cutoff points for central obesity in Korean adults. Diabetes Res Clin Pract. 2007;75(1):72–80. doi:10.1016/j.diabres.2006.04.013
41. Bao Y, Lu J, Wang C, et al. Optimal waist circumference cutoffs for abdominal obesity in Chinese. Atherosclerosis. 2008;201(2):378–384. doi:10.1016/j.atherosclerosis.2008.03.001
42. Chen LK, Woo J, Assantachai P, et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21(3):300–307 e2. doi:10.1016/j.jamda.2019.12.012
43. Tinetti ME. Performance-oriented assessment of mobility problems in elderly patients. J Am Geriatr Soc. 1986;34(2):119–126. doi:10.1111/j.1532-5415.1986.tb05480.x
44. Guilley E, Bopp M, Faeh D, et al. Socioeconomic gradients in mortality in the oldest old: a review. Arch Gerontol Geriatr. 2010;51(3):e37–40. doi:10.1016/j.archger.2009.12.009
45. Consultation WHOE. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–163.
46. Salive ME. Multimorbidity in older adults. Epidemiol Rev. 2013;35:75–83. doi:10.1093/epirev/mxs009
47. Viktil KK, Blix HS, Moger TA, et al. Polypharmacy as commonly defined is an indicator of limited value in the assessment of drug-related problems. Br J Clin Pharmacol. 2007;63(2):187–195. doi:10.1111/j.1365-2125.2006.02744.x
48. The Consensus Committee of the American Autonomic Society and the American Academy of Neurology. Consensus statement on the definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy. Neurology. 1996;46(5):1470. doi:10.1212/WNL.46.5.1470
49. Lamb SE, Jørstad-Stein EC, Hauer K, et al. Development of a common outcome data set for fall injury prevention trials: the prevention of falls network Europe consensus. J Am Geriatr Soc. 2005;53(9):1618–1622. doi:10.1111/j.1532-5415.2005.53455.x
50. Dennis M, Kadri A, Coffey J. Depression in older people in the general hospital: a systematic review of screening instruments. Age Ageing. 2012;41(2):148–154. doi:10.1093/ageing/afr169
51. Galea M, Woodward M. Mini-Mental State Examination (MMSE). Aust J Physiother. 2005;51(3):198. doi:10.1016/S0004-9514(05)70034-9
52. Rubenstein LZ, Harker JO, Salva A, et al. Screening for undernutrition in geriatric practice: developing the short-form mini-nutritional assessment (MNA-SF). J Gerontol a Biol Sci Med Sci. 2001;56(6):M366–72. doi:10.1093/gerona/56.6.M366
53. Cho BY, Seo DC, Lin HC, Lohrmann DK, Chomistek AK. BMI and Central Obesity With Falls Among Community-Dwelling Older Adults. Am J Prev Med. 2018;54(4):E59–E66.
54. Simoneau M, Teasdale N. Balance control impairment in obese individuals is caused by larger balance motor commands variability. Gait Posture. 2015;41(1):203–208. doi:10.1016/j.gaitpost.2014.10.008
55. Wolfson L, Judge J, Whipple R, et al. Strength is a major factor in balance, gait, and the occurrence of falls. J Gerontol a Biol Sci Med Sci. 1995;50:64–67. doi:10.1093/gerona/50a.special_issue.64
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.