Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Association Between Dietary Salt and Plasma Glucose, Insulin and Hemoglobin A1c Levels Among Type 2 Diabetes Patients in Eastern China
Authors Lin Y ![]() , Chattopadhyay K
, Chattopadhyay K ![]() , Yang X
, Yang X ![]() , Li JL
, Li JL ![]() , Chen YS
, Chen YS ![]() , Zhou Y
, Zhou Y ![]() , Li L
, Li L ![]()
Received 12 September 2021
Accepted for publication 12 November 2021
Published 19 December 2021 Volume 2021:14 Pages 4811—4818
DOI https://doi.org/10.2147/DMSO.S338915
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Yi Lin,1 Kaushik Chattopadhyay,2 Xi Yang,3 Jia-Lin Li,4 Yan-Shu Chen,4 Ye Zhou,4 Li Li4
1Center for Health Economics, Faculty of Humanities and Social Sciences, University of Nottingham, Ningbo, Zhejiang Province, People’s Republic of China; 2Division of Epidemiology and Public Health, School of Medicine, University of Nottingham, Nottingham, UK; 3Department of Nutrition, Ningbo First Hospital, Ningbo, Zhejiang Province, People’s Republic of China; 4Department of Endocrinology and Metabolism, Ningbo First Hospital, Ningbo, Zhejiang Province, People’s Republic of China
Correspondence: Li Li
Department of Endocrinology and Metabolism, Ningbo First Hospital, 59, Liuting Street, Ningbo, 315010, Zhejiang Province, People’s Republic of China
Tel +86 13757426626
Email [email protected]
Yi Lin
Center for Health Economics, Faculty of Humanities and Social Sciences, University of Nottingham, 199, Taikang East Road, University Park, Ningbo, 315100, People’s Republic of China
Tel +86-13916608572
Email [email protected]
Purpose: Type 2 diabetes (T2D) is one of the major public health concerns in China. Studies on the association between dietary salt intake and the glycemic response of T2D are lacking in China. The aim was to investigate the association between the levels of dietary salt intake and the plasma glucose, insulin and hemoglobin A1c (HbA1c) levels in T2D patients.
Methods: Patients with T2D, who accepted management and treatment by the National Standardized Metabolic Disease Management Center at Ningbo First Hospital from March 2018 to January 2020, were included in this study. Dietary salt intake was assessed through a standardized food frequency questionnaire. Anthropometry, blood pressure and biomarkers were measured by well-trained endocrinology nurses. Generalized linear models (GLMs) were used to examine the associations.
Results: A total of 1145 eligible T2D patients with a mean age of 51.4 years were included in the study. Fasting plasma glucose (FPG), 2-hour postprandial plasma glucose and 2-hour postprandial insulin were significantly increased across dietary salt categories. The GLMs further showed that dietary salt intake > 8 g/day was positively associated with FPG and HbA1c.
Conclusion: Higher daily salt intake was found to be associated with FPG and HbA1c in T2D patients. Lifestyle education and promotion of salt reduction should be provided to T2D patients.
Keywords: dietary salt, type 2 diabetes, blood glucose, insulin, glycated hemoglobin A1c, China
Introduction
Over the past four decades, the rapidly increasing prevalence of type 2 diabetes (T2D) has become a public health concern in China, due to economic development and changes in diet, lifestyle and culture influenced by westernization. The prevalence of diabetes rose from less than 1% in 19801 to 12.8% in 2017.2 T2D has been the main driver for the increased prevalence of diabetes in China.3 T2D patients in the tertiary hospital in Ningbo were reported to have poor glycemic control.4 In addition, a study conducted by Li et al, which included 3370 T2D patients from the tertiary hospital in Ningbo, indicated that patients with T2D were at high risk of further chronic complications, including hypertension, dyslipidemia, nephropathy, retinopathy, coronary heart disease, stroke and cerebrovascular diseases.5
T2D is a lifestyle disorder and progression is highly correlated with aging, dietary and lifestyle behavior, and genetic factors.6 Although dietary salt as an essential seasoning contributes to eating pleasure and satisfaction,7 many guidelines have promoted dietary salt restriction in patients with diabetes.8,9 Higher intake of sodium is an established risk factor for stroke and cardiovascular diseases.10 Dietary sodium intake is evidenced to be positively associated with increased blood pressure in the general population.11,12 However, the connection between dietary salt and glucose homeostasis remains elusive and has not been drawn the same attention as hypertension. The majority of dietary interventions do not focus on the relationship between dietary salt/sodium intake and the prognosis of diabetes.
To the best of our knowledge, few studies have explored the relationship between dietary salt and indicators of T2D in China, patients in particular. The objective of this study was to investigate the association between the levels of dietary salt and blood glucose, insulin and hemoglobin A1c (HbA1c) in T2D patients in Ningbo, China.
Methods
Study Design and Patients
An ongoing innovation study of the management of metabolic diseases and complications is a national standardized project, implemented by the Metabolic Management Center (MMC). The National Standardized MMC called “One Center, One Stop, and One Standard Model” was established as a platform for the standardized diagnosis and treatment of metabolic diseases and their long-term follow-up.13 In the MMCs, patients can receive a comprehensive series of services including registration, tests, evaluation, prescriptions and health education. Under the guidance of the MMC Experts Committee, more than 400 stringent standard operating procedures were set up for quality control of the MMC operation. The details of the national MMC are reported elsewhere.13
The present study included 2313 patients with T2D, registering in the MMC for the first time from March 2018 to January 2020, at the outpatient Department of Endocrinology, Ningbo First Hospital, Zhejiang Province, China and the National Standardized MMC. T2D was diagnosed based on the definition proposed by the World Health Organization (WHO).14 Patients were excluded from this study if they met any of the following criteria: (1) age >75 years or age <18 years; (2) diagnosis with any kind of cancer; (3) positive islet autoantibodies; (4) glomerular filtration rate (eGFR) <30 mL/minute; (5) severe liver dysfunction; (6) acute infectious diseases; (7) pregnancy or lactation; (8) incompleting standardized questionnaires on food frequency, demography and lifestyle.
The study was approved by the Research Ethics Committee of Ningbo First Hospital, China (no. 2019-R057). Written informed consent was obtained from all participants.
Dietary Assessment
Dietary information was collected through a nationwide standardized food frequency questionnaire (FFQ), following the guidelines proposed by MMC and Ningbo First Hospital during outpatient visits. All of the dietary information was collected by well-trained nurses. Quantitative dietary information was collected on how many usual foods (vegetables, fruits, soya and soya products) were consumed (in grams per day), how often meat (red meat, poultry, fish and shrimps) and soft drinks were consumed per week, and how much seasoning (salt and sugar) was consumed per day. Patients were provided with a standard brochure with colorful photographs for description of the portion sizes, following the Chinese dietary guideline.15 Considering the psychological responses of patients, all of the information on dietary intake was collected through multiple-choice questions.
Dietary salt was categorized into three groups: ≤6, 6–8 (excluding 6g/d) and >8 g/day, according to the Chinese dietary guideline for prevention and control of diabetes in primary care.16,17 Patients with missing reports were asked to fill them in during outpatient visits, and misreported information was evaluated and corrected based on daily reasonable consumption.
Demography and Lifestyle
All adults diagnosed with T2D who were willing to participate in the study were invited to complete the MMC standard questionnaires on their demography [education (low education: lower than college/university; and high education: college/university or above)], lifestyle [current smoking status (no and yes); current alcohol drinking status (no and yes); physical activity], medical history and medication records.
Anthropometric Measurements and Blood Pressure
Anthropometric measurements, including height, body weight and waist circumference (WC), were measured with the patient wearing light clothing by well-trained endocrinology nurses. Height to the nearest 0.1 cm and body weight to the nearest 0.1 kg were measured using an electronic scale (OMRON HNH-318; Dalian, Liaoning Province, China). WC was measured at the midpoint between the inferior costal margin and the iliac crest in the midaxillary line. Body mass index (BMI), defining general obesity, was calculated as weight (kg)/height (m2). Patients were classified into four BMI categories according to the China Obesity Task Force, as follows: underweight (<18.5 kg/m2), normal weight (18.5–23.9 kg/m2), overweight (24.0–27.9 kg/m2) and obesity (≥28.0 kg/m2).18 Abdominal obesity was defined according to WC values: WC >90 cm in men or >85 cm in women.18 Blood pressure was measured using an electronic sphygmomanometer (ORMON HBP-9020; Dalian, Liaoning Province, China) on the right or left arm after a 10-minute rest.
Biomarker Measurements
After a 10–12-hour overnight fast, blood samples were obtained in the early morning to measure the levels of biomarkers, including fasting plasma glucose (FPG), fasting insulin (FINS), HbA1c, total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), uric acid (UA) and serum creatinine (SCr). Then, the 100 g carbohydrate (steamed bread meal) test was used to assess 2-hour postprandial plasma glucose (2hPG) and 2-hour postprandial insulin (2hINS) concentrations. Lipid profiles were analyzed by enzymatic procedures. FPG and 2hPG were assessed by the glucose oxidase method and chemiluminescence immunoassay, respectively. FINS was measured by radioimmunoassay. HbA1c was determined by high-pressure liquid chromatography. UA was examined by enzymatic spectrophotometry. Biomarkers were analyzed using an auto-analyzer (Beckman Coulter AU5800; Shizuoka, Japan). Details of biomarker measurements have been reported elsewhere.19
Statistical Analysis
The percentage of patients, mean with standard deviation (SD) and median values with interquartile range among the categories of dietary salt were presented as descriptive analyses. Continuous and categorical variables of patients’ characteristics were examined by analysis of variance (ANOVA) and chi-square test, respectively. ANOVA with Bonferroni correction/Games–Howell, and the Mann–Whitney U-test and Kruskal–Wallis test were used to examine mean and median values of anthropometric measurements and biomarkers within and between the categories of dietary salt.
Generalized linear models (GLMs) were used to assess the associations between salt intake and biomarkers (FPG, 2hPG, FINS, 2hINS and HbA1c) after adjusting for confounding factors (sex, age and educational levels), lifestyle factors (physical activity, smoking status and drinking status), BMI, WC, systolic blood pressure (SBP), diastolic blood pressure (DBP), UA, SCr, medication and interactions. Only significant interactions between dietary salt and confounding factors were examined in the model. Results were considered statistically significant at a two-tailed level of 0.05. Statistical analyses were conducted using IBM SPSS Statistics version 26.0.
Results
Study Population
In total, 1145 out of 2313 T2D patients (65.2% men) with a mean age of 51.4 years were included in the present study. They were divided into three groups according to salt intake: ≤6, 6–8 and >8 g/day (Table 1).
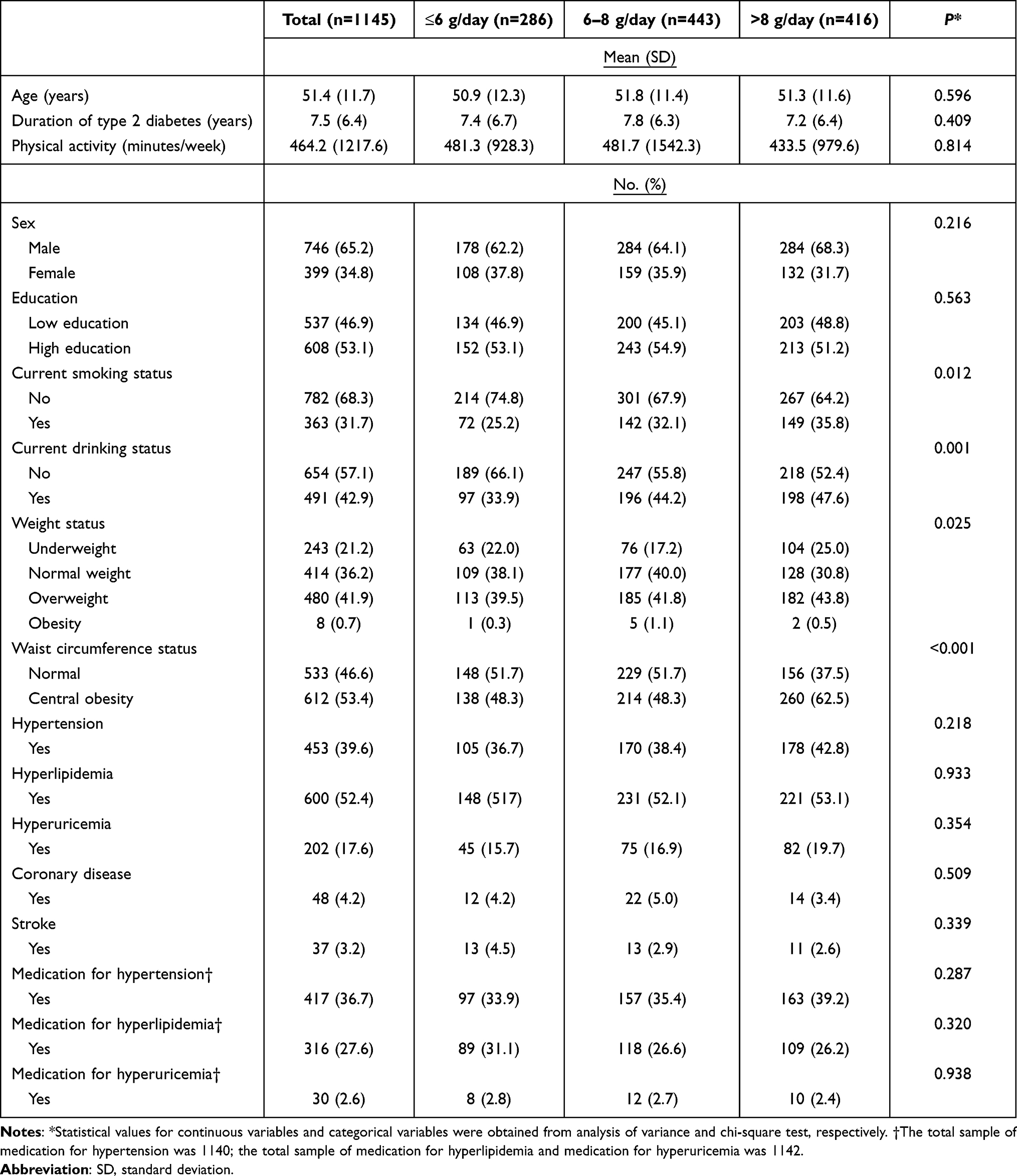 |
Table 1 Patient Characteristics According to Levels of Salt Intake |
Among all patients, around 25.0% had dietary salt intake less than or equal to 6g/day. Compared to lower salt intake (≤6 g/day), a higher prevalence of patients with overweight and central obesity was observed in the groups with higher salt intake (6–8 and > 8 g/day). Similarly, higher prevalences of hypertension, hyperlipidemia, hyperuricemia and coronary disease were seen in the groups with higher salt intake.
Risk Factors Among Salt Intake Categories
In T2D patients, direct risk factors, including FPG, 2hPG, 2hINS and HbA1c, and indirect risk factors, including BMI, WC, VFA, SFA, TC, TG and LDL-C, were significantly different across dietary salt categories (Table 2), whereas 2hINS, SBP, DBP, HDL-C and UA were not significantly different. Within dietary salt categories, mean values of FPG, 2hPG and HbA1c were significantly higher in the group with dietary salt >8 g/day than in the groups with lower salt intake (≤6 and 6–8 g/day).
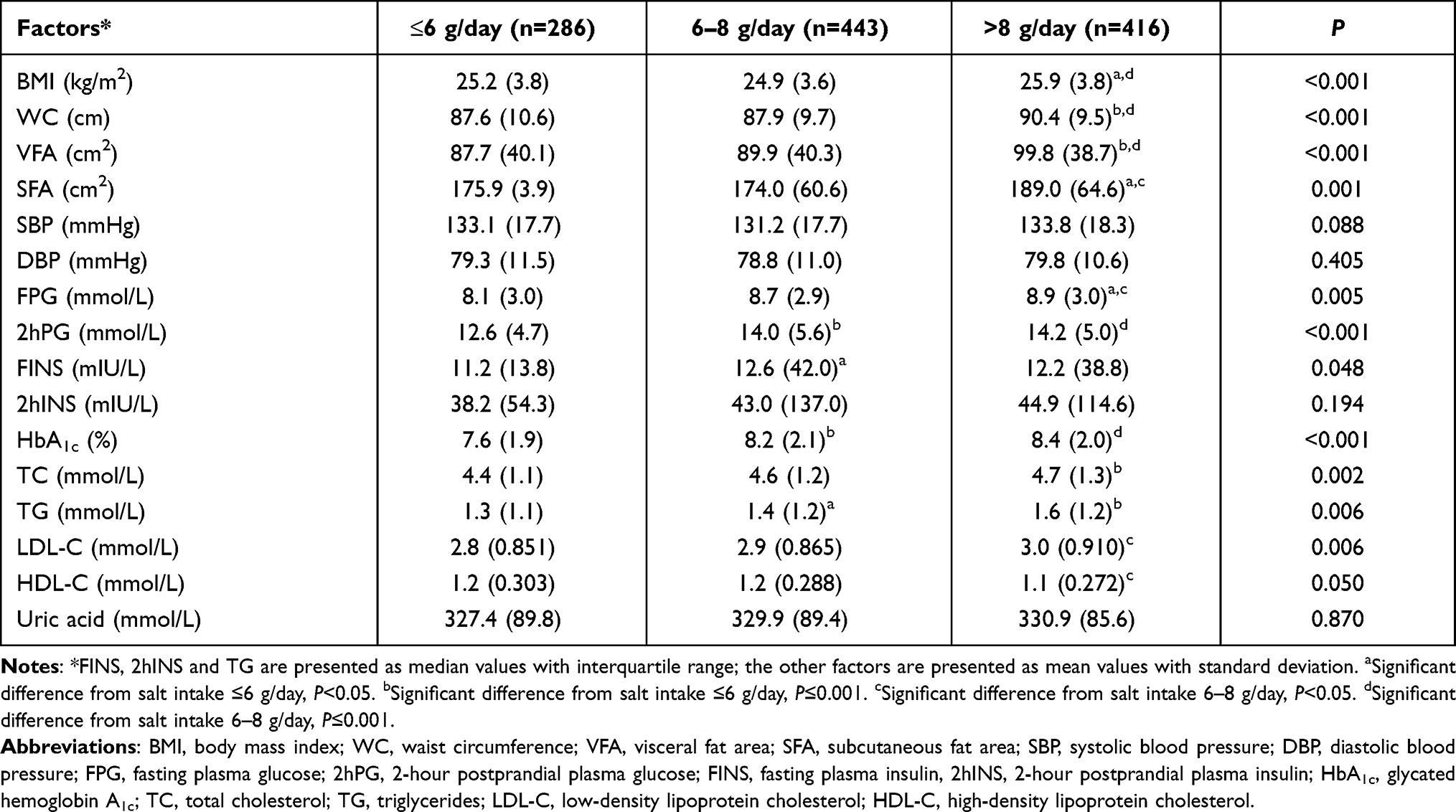 |
Table 2 Mean and Median Values of Risk Factors for Type 2 Diabetes According to Salt Intake Levels |
Associations Between Dietary Salt Intake and Blood Glucose, Insulin and HbA1c
Associations between dietary salt and plasma glucose, insulin and HbA1c among T2D patients were further investigated by GLMs (Tables 3–5). Dietary salt (6–8 and >8 g/day) was significantly associated with all of the dependent variables (FPG, 2hPG, FINS, 2hINS and HbA1c) in the crude model. After further adjusting for confounding factors, lifestyle factors, BMI, WC, SBP, DBP, UA, SCr, medication and interactions, dietary salt (>8 g/day) remained statistically significant in the model and positively associated with FPG (β=2.3, P=0.013) and HbA1c (β=0.67, P=0.032). Thus, the results showed that higher dietary salt (>8 g/day) increased FPG by 2.3 mmol/L and HbA1c by 0.67%, compared to lower dietary salt (≤6 g/day).
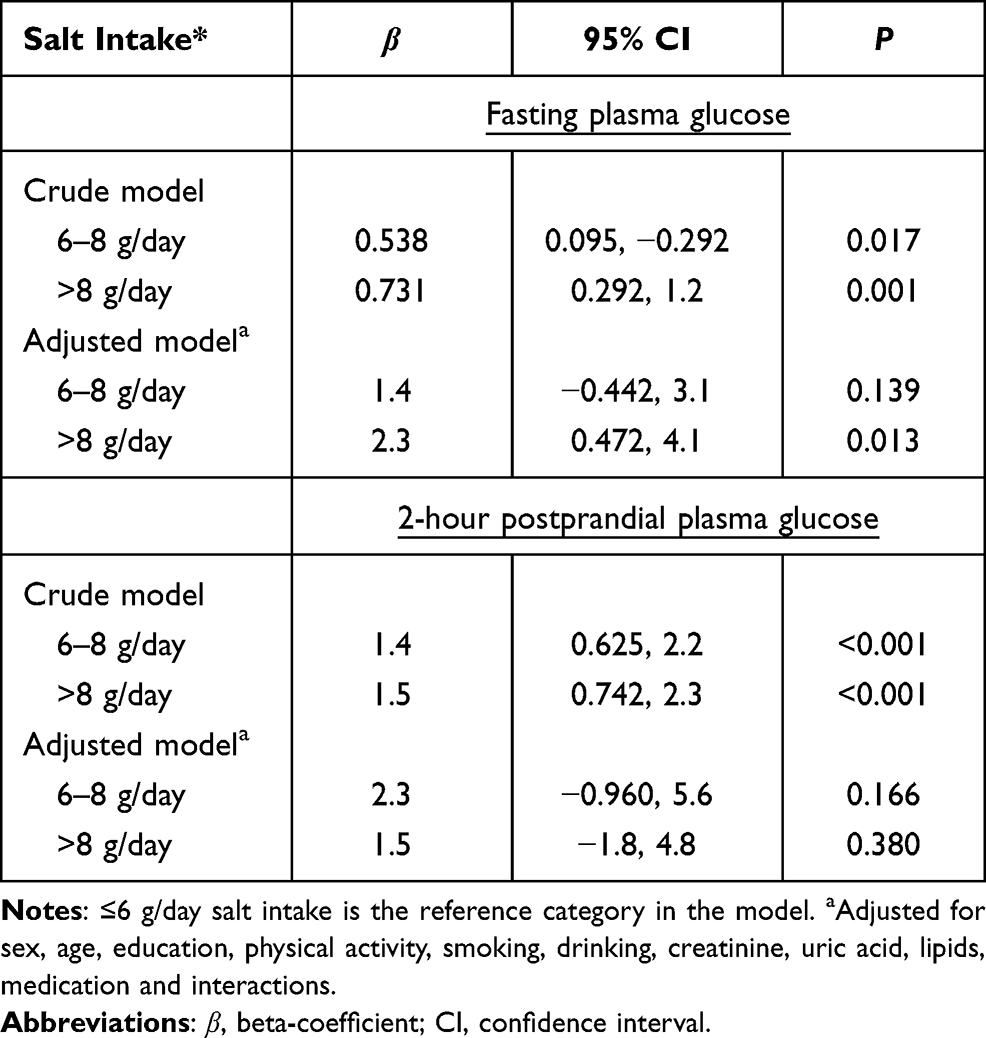 |
Table 3 Association Between Dietary Salt Intake and Plasma Glucose |
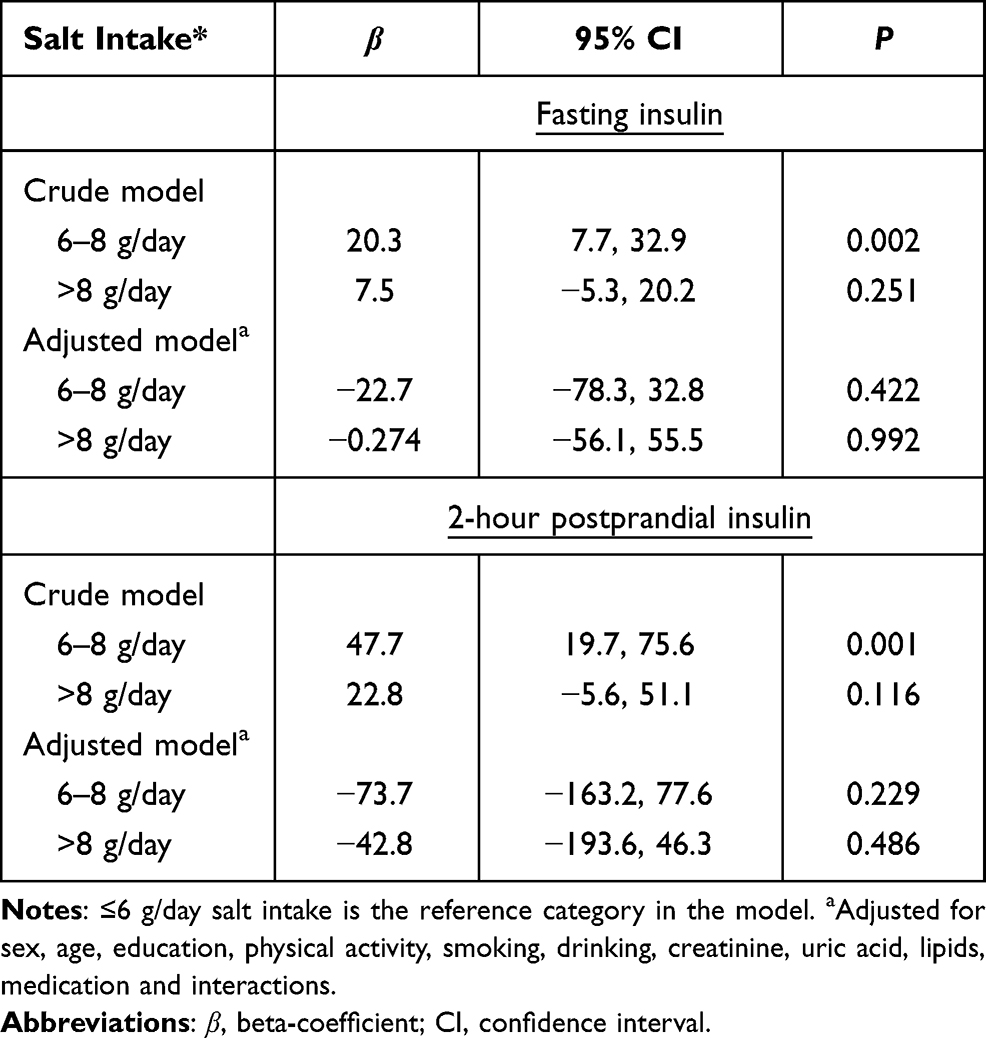 |
Table 4 Association Between Dietary Salt Intake and Insulin |
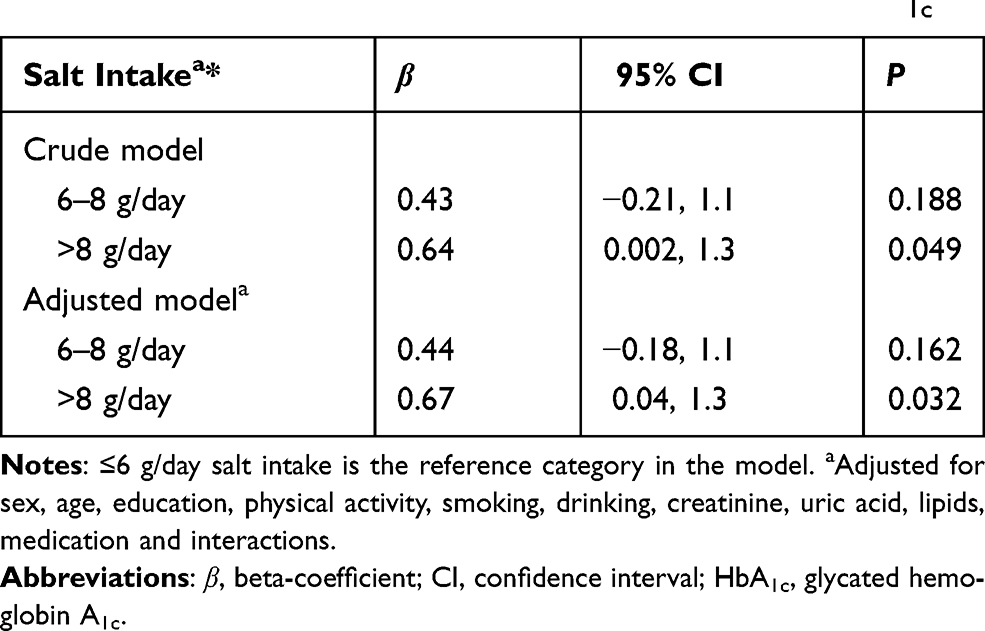 |
Table 5 Association Between Dietary Salt Intake and HbA1c |
Discussion
To date, the association of dietary salt intake with the glycemic response has not been adequately investigated and understood in China, in T2D patients in particular. The present study, using clinical data from the outpatient Department of Endocrinology and the MMC, analyzed the association between dietary salt and the glycemic response (plasma glucose, insulin and HbA1c) in T2D patients in Ningbo. The findings indicated that higher dietary salt was positively associated with increased FPG and HbA1c.
A previous study conducted on healthy residents in Ningbo found a higher fasting blood glucose level in the group with a higher dietary salt intake (≥6 g/day) than in the group with lower dietary salt intake (<6 g/day).12 The results of that Chinese study are in line with our findings on FPG among Chinese patients in Ningbo, although the target populations are different. The mechanism of the association between dietary salt and the glycemic response in T2D patients is unclear. Increased dietary salt intake may suppress the activity of the renin–angiotensin–aldosterone system,20,21 stimulate sympathetic activity22 and cause insulin resistance.23,24 Therefore, it may contribute to the development and progression of T2D complications.
In the majority of studies, the relationship between dietary salt and the glycemic response of T2D has been explored through observational studies, intervention studies and meta-analyses in healthy populations.12,25,26 However, few studies have been conducted on T2D patients. Our findings showed that dietary salt was positively associated with HbA1c, which is consistent with the results from a randomized controlled trial (RCT) on salt reduction.26 This observer-blind RCT, recruiting 70 patients with acute non-cardioembolic mild ischemic stroke, reported that HbA1c decreased more in the lifestyle intervention group, providing a reduction in salt intake, compared to the control group, although no significant difference was found between the two groups.26 Likewise, Strazzullo et al conducted a meta-analysis including 13 studies with 177,025 participants, which indicated an association between the HbA1c level and dietary sodium in the development of cardiovascular disease.27
Higher dietary salt was found to be related to a high prevalence of overweight and obesity compared to lower dietary salt in the present study. In addition, high blood lipid levels were significantly related to increased dietary salt intake in our study. The potential hypothesis is that high dietary salt may increase plasma glucose and postprandial plasma glucose in T2D patients through weight gain due to increased appetite and overconsumption of energy, fat and cholesterol.28 Eventually, the increased fat free acid level in the blood can inhibit insulin suppression of hepatic glucose production.29 Dietary salt is a key factor in increasing the feeling of thirst, resulting in greater intake of fluid drinks.30 An increase in the dietary salt intake of 1 g/day was positively associated with an increase of 100 g/day total fluid and 27 g/day sugar-sweetened soft drink consumption.31 In this way, it may contribute to high blood pressure/hypertension.
Several dietary guidelines recommend and advocate that patients with T2D should decrease their dietary salt intake for lowing a modest blood pressure.8,9 In the present study, the results derived from descriptive analysis showed that no significant differences in SBP and DBP were found across dietary salt categories. The WHO Cardiovascular Diseases and Alimentary Comparison (WHO-CARDIAC) Study, conducted on pre- and post-menopausal women from 17 countries, reported that 24-hour sodium excretion was positively associated with blood pressure.32 In T2D patients, hypertension is associated with a range of adverse outcomes for further developing cardiovascular disease and premature mortality.33 The different result in our study could be attributed to the cross-sectional study design.
In this study, dietary salt was not found to be significantly associated with postprandial plasma glucose and postprandial insulin. Few studies have investigated the relationship between dietary salt and postprandial plasma glucose and insulin responses in T2D patients. An intervention study including six healthy adults, who were randomly assigned to take meals with or without added salt, suggested that moderate dietary salt intake increased postprandial plasma glucose and insulin levels.25 Sodium can facilitate the absorption of glucose in the small intestine.34 The potential reason for the difference between studies may be that most of our participants had been diagnosed with T2D for a certain period, so that postprandial plasma glucose and insulin responses to dietary salt were not the same as in healthy participants owing to their weak digestive system.
The relationship between dietary salt intake and hypertension is well understood in the Chinese population. In addition, there is a high level of knowledge on glycemic control through the duration and quantity of carbohydrate consumption from foods.35 Patients with diabetes are recommended to restrict their total consumption of energy and carbohydrates in order to control body weight and blood glucose levels. However, more attention needs to be paid to the effect of dietary salt intake on the glycemic response in T2D patients. Therefore, hospital-based education and community-based education are required regarding the health effects of excess salt intake, food labeling and food sources.
This is the first study on the association between dietary salt intake and the glycemic response in T2D patients in Ningbo with standard national management and treatment by MMC. Nevertheless, several study limitations need to be considered. First, causality between dietary salt intake and factors of T2D cannot be assessed owing to the cross-sectional study design. Second, because of the structure of the FFQ, quantitative dietary salt intake could not be obtained, although the categories of salt intake could be collected from the patients. Therefore, it may not accurately reflect daily dietary salt intake among T2D patients. Third, total energy intake was not adjusted in the model owing to the FFQ. In addition, the reported dietary salt level could be biased towards misreporting because of the patients’ psychology. Furthermore, the patients were from eastern China, so the findings may not be representative for the entire Chinese population with T2D.
Conclusion
High dietary salt intake was found to be associated with FPG and HbA1c among T2D patients. Hospital-based lifestyle education with the promotion of salt reduction should be provided to T2D patients. Future research should involve intervention studies on salt reduction to investigate the impact of the dose of dietary salt intake on the glycemic response of T2D patients.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement
The study was ethically approved by the Ethics Committee of Ningbo First Hospital, China (ethics approval no. 2019-R057) and followed the principles of the Declaration of Helsinki.
Acknowledgments
The authors thank all the patients who participated in the study. We thank Ningbo First Hospital for their support of the research project. We thank the Faculty of Humanities and Social Sciences, University of Nottingham, Ningbo, China, for supporting this research collaboration.
Funding
This study was supported by the Medical Health Science and Technology Project of Zhejiang Provincial Health Commission (grant no. 2019331427), Major Program of Social Development of Ningbo Science and Technology Bureau (grant no. 2019C50094) and Ningbo Science and Technology Bureau (grant no. 2019A610391).
Disclosure
The authors declared no conflicts of interest for this work.
References
1. National Diabetes Research Cooperative Group. [A mass survey of diabetes mellitus in a population of 300,000 in 14 provinces and municipalities in China (author’s transl)]. Zhonghua Nei Ke Za Zhi. 1981;20(11):678–683. Chinese.
2. Li Y, Teng D, Shi X, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ. 2020;369:m997. doi:10.1136/bmj.m997
3. Jia W, Weng J, Zhu D, et al. Standards of medical care for type 2 diabetes in China 2019. Diabetes Metab Res Rev. 2019;35(6):e3158. doi:10.1002/dmrr.3158
4. Li J, Chattopadhyay K, Xu M, et al. Glycaemic control in type 2 diabetes patients and its predictors: a retrospective database study at a tertiary care diabetes centre in Ningbo, China. BMJ Open. 2018;8(3):e019697. doi:10.1136/bmjopen-2017-019697
5. Li J, Chattopadhyay K, Xu M, et al. Prevalence and associated factors of vascular complications among inpatients with type 2 diabetes: a retrospective database study at a tertiary care department, Ningbo, China. PLoS One. 2020;15(6):e0235161. doi:10.1371/journal.pone.0235161
6. Murea M, Ma L, Freedman BI. Genetic and environmental factors associated with type 2 diabetes and diabetic vascular complications. Rev Diabet Stud. 2012;9(1):6–22. doi:10.1900/rds.2012.9.6
7. Duffy VB, Hayes JE, Sullivan BS, Faghri P. Surveying food and beverage liking: a tool for epidemiological studies to connect chemosensation with health outcomes. Ann N Y Acad Sci. 2009;1170:558–568. doi:10.1111/j.1749-6632.2009.04593.x
8. Graham I, Atar D, Borch-Johnsen K, et al. European guidelines on cardiovascular disease prevention in clinical practice: full text. Fourth Joint Task Force of the European Society of Cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of nine societies and by invited experts). Eur J Cardiovasc Prev Rehabil. 2009;14(Suppl 2):S1–113. doi:10.1097/01.hjr.0000277983.23934.c9
9. Bantle JP, Wylie-Rosett J, Albright AL, et al. Nutrition recommendations and interventions for diabetes: a position statement of the American Diabetes Association. Diabetes Care. 2008;31(Suppl 1):S61–78. doi:10.2337/dc08-S061
10. Strazzullo P, D’Elia L, Kandala NB, Cappuccio FP. Salt intake, stroke, and cardiovascular disease: meta-analysis of prospective studies. BMJ. 2009;339:b4567. doi:10.1136/bmj.b4567
11. Santos JA, Webster J, Land MA, et al. Dietary salt intake in the Australian population. Public Health Nutr. 2017;20(11):1887–1894. doi:10.1017/s1368980017000799
12. Lin Y, Mei Q, Qian X, He T. Salt consumption and the risk of chronic diseases among Chinese adults in Ningbo city. Nutr J. 2020;19(1):9. doi:10.1186/s12937-020-0521-8
13. Zhang Y, Wang W, Ning G. Metabolic management center: an innovation project for the management of metabolic diseases and complications in China. J Diabetes. 2019;11(1):11–13. doi:10.1111/1753-0407.12847
14. World Health Organization. Reducing salt intake in populations –report of a WHO forum and technical meeting. Geneva: WHO Document Production Services; 2007.
15. Wang SS, Lay S, Yu HN, Shen SR. Dietary guidelines for Chinese residents (2016): comments and comparisons. J Zhejiang Univ Sci B. 2016;17(9):649–656. doi:10.1631/jzus.B1600341
16. Chinese Diabetes Society. National Office for Primary Diabetes Care. National guidelines for the prevention and control of diabetes in primary care (2018). Chin J Intern Med. 2018;57(12):9.
17. Chinese Nutrition Society. The Chinese dietary guideline; 2016. Available from: http://dg.cnsoc.org/article/04/8a2389fd5520b4f30155be1475e02741.html.
18. Department of Diseases Control, Ministry of Health, People’s Republic of China. The guideline of prevention and control of overweight and obesity among Chinese adults. Acta Nutri Sin. 2004;26(1):1–36.
19. Yang X, Lin Y, Xu GD, et al. Optimal cut-off values of visceral fat area for predicting metabolic syndrome among type 2 diabetes patients in Ningbo, China. Diabetes Metab Syndr Obes. 2021;14:1375–1383. doi:10.2147/dmso.S304164
20. Charytan DM, Forman JP. You are what you eat: dietary salt intake and renin-angiotensin blockade in diabetic nephropathy. Kidney Int. 2012;82(3):257–259. doi:10.1038/ki.2012.148
21. Graudal NA, Galløe AM, Garred P. Effects of sodium restriction on blood pressure, renin, aldosterone, catecholamines, cholesterols, and triglyceride: a meta-analysis. JAMA. 1998;279(17):1383–1391. doi:10.1001/jama.279.17.1383
22. Grassi G, Dell’Oro R, Seravalle G, Foglia G, Trevano FQ, Mancia G. Short- and long-term neuroadrenergic effects of moderate dietary sodium restriction in essential hypertension. Circulation. 2002;106(15):1957–1961. doi:10.1161/01.cir.0000033519.45615.c7
23. Garg R, Williams GH, Hurwitz S, Brown NJ, Hopkins PN, Adler GK. Low-salt diet increases insulin resistance in healthy subjects. Metabolism. 2011;60(7):965–968. doi:10.1016/j.metabol.2010.09.005
24. Petrie JR, Morris AD, Minamisawa K, et al. Dietary sodium restriction impairs insulin sensitivity in noninsulin-dependent diabetes mellitus. J Clin Endocrinol Metab. 1998;83(5):1552–1557. doi:10.1210/jcem.83.5.4835
25. Thorburn AW, Brand JC, Truswell AS. Salt and the glycaemic response. BMJ (Clinical Research Ed). 1986;292(6537):1697–1699. doi:10.1136/bmj.292.6537.1697
26. Kono Y, Yamada S, Yamaguchi J, et al. Secondary prevention of new vascular events with lifestyle intervention in patients with noncardioembolic mild ischemic stroke: a single-center randomized controlled trial. Cerebrovasc Dis. 2013;36(2):88–97. doi:10.1159/000352052
27. Takahashi K, Yoshimura Y, Kaimoto T, Kunii D, Komatsu T, Yamamoto S. Validation of a food frequency questionnaire based on food groups for estimating individual nutrient intake. Jpn J Nutr. 2001;59:221–232. doi:10.5264/eiyogakuzashi.59.221
28. Meneton P, Jeunemaitre X, de Wardener HE, MacGregor GA. Links between dietary salt intake, renal salt handling, blood pressure, and cardiovascular diseases. Physiol Rev. 2005;85(2):679–715. doi:10.1152/physrev.00056.2003
29. Boden G, Cheung P, Stein TP, Kresge K, Mozzoli M. FFA cause hepatic insulin resistance by inhibiting insulin suppression of glycogenolysis. Am J Physiol Endocrinol Metab. 2002;283(1):E12–9. doi:10.1152/ajpendo.00429.2001
30. He FJ, Markandu ND, Sagnella GA, MacGregor GA. Effect of salt intake on renal excretion of water in humans. Hypertension. 2001;38(3):317–320. doi:10.1161/01.hyp.38.3.317
31. He FJ, Marrero NM, MacGregor GA. Salt intake is related to soft drink consumption in children and adolescents: a link to obesity? Hypertension. 2008;51(3):629–634. doi:10.1161/hypertensionaha.107.100990
32. Yamori Y, Liu L, Ikeda K, Mizushima S, Nara Y, Simpson FO. Different associations of blood pressure with 24-hour urinary sodium excretion among pre- and post-menopausal women. WHO Cardiovascular Diseases and Alimentary Comparison (WHO-CARDIAC) Study. J Hypertens. 2001;19(3 Pt 2):535–538. doi:10.1097/00004872-200103001-00003
33. Intersalt Cooperative Research Group. Intersalt: an international study of electrolyte excretion and blood pressure. Results for 24 hour urinary sodium and potassium excretion. Intersalt Cooperative Research Group. BMJ. 1988;297(6644):319–328. doi:10.1136/bmj.297.6644.319
34. Gray GM. Carbohydrate digestion and absorption. Role of the small intestine. NEJM. 1975;292(23):1225–1230. doi:10.1056/nejm197506052922308
35. Feinman RD, Pogozelski WK, Astrup A, et al. Dietary carbohydrate restriction as the first approach in diabetes management: critical review and evidence base. Nutrition. 2015;31(1):1–13. doi:10.1016/j.nut.2014.06.011
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.