Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 18
Association Between Dental Aesthetics and Psychosocial Well-Being: A Cross-Sectional Study Among Health Sciences Students in Yemen
Authors AL-Huthaifi BH ![]() , Al-Hababi AH, Aldhorae K, Muharram A, Dahaba A, Ghaleb A, Tareq R, Taha R, Abdu EM
, Al-Hababi AH, Aldhorae K, Muharram A, Dahaba A, Ghaleb A, Tareq R, Taha R, Abdu EM ![]() , Abdullah BM
, Abdullah BM ![]() , Al Moaleem MM
, Al Moaleem MM
Received 11 May 2026
Accepted for publication 25 June 2026
Published 3 July 2026 Volume 2026:18 619857
DOI https://doi.org/10.2147/CCIDE.S619857
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Basem H AL-Huthaifi,1,2,* Ahlam H Al-Hababi,3,* Khalid Aldhorae,1,4 Asala Muharram,1 Abeer Dahaba,1 Asmaa Ghaleb,1 Rawan Tareq,1 Rawan Taha,1 Ehab M Abdu,1,5 Baker M Abdullah,5 Mohammed M Al Moaleem,6
1Faculty of Dentistry, Ibn Al-Nafis University for Medical Sciences, Sana’a, Yemen; 2Orthodontic Department, Faculty of Dentistry, University of Sciences and Technology, Sana’a, Yemen; 3Department of Periodontology, Faculty of Dentistry, Sana’a University, Sana’a, Yemen; 4Orthodontic Department, Faculty of Dentistry, Thamar University, Thamar, Yemen; 5Department of Oral and Maxillofacial Surgery, College of Dentistry, Sana’a University, Sana’a, Yemen; 6Department of Prosthetic Dental Science, College of Dentistry, Jazan University, Jazan, 45142, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Basem H AL-Huthaifi, Faculty of Dentistry, Ibn Al-Nafis University for Medical Sciences, Sana’a, Yemen, Email [email protected]
Baker M Abdullah, Faculty of Dentistry, Ibn Al-Nafis University for Medical Sciences, Sana’a, Yemen, Email [email protected]
Background and Aim: Dental aesthetics has an increasing effect on young adults’ psychosocial well-being; this effect is particularly true for patient-facing professions, in which people’s appearance influences how others interact with them. However, there is currently limited evidence from conflict-affected, resource-poor settings regarding this relationship. The current study aimed to explore the relationship between the psychosocial effects of dental aesthetics and self-esteem and perceived need for orthodontic treatment among health sciences students in Sana’a, Yemen.
Methodology: A cross-sectional, Internet-based survey was conducted among 300 health sciences students (18– 25 years) from public and private universities in Sana’a between August and September 2025. The survey included the Psychosocial Impact of Dental Aesthetics Questionnaire (PIDAQ), Rosenberg Self-Esteem Scale (RSES), and Aesthetic Component of the Index of Orthodontic Treatment Needs (IOTN-AC). Data were analyzed using SPSS version 26.0.
Results: Of 385 targeted participants, 300 responded (70.7% female; mean age 22.3 years). The mean PIDAQ score was 2.40 ± 0.62, indicating a mild psychosocial impact based on established PIDAQ scoring conventions. Male students had significantly higher PIDAQ scores than females (2.52 ± 0.69 vs. 2.35 ± 0.56; p = 0.026). No statistically significant correlation was detected between PIDAQ and RSES scores in this sample (r = − 0.012, p = 0.834). Academic year progression predicted higher self-esteem (β = 0.281, p = 0.002). Self-perceived orthodontic need (IOTN-AC) showed a dose-response relationship with PIDAQ scores (definite need: 2.82 ± 0.41 vs. no need: 2.34 ± 0.35; p < 0.05).
Conclusion: Dental aesthetics significantly affects psychosocial well-being among health sciences students in Yemen, with unexpectedly higher impact among male students. No direct association was found between dental aesthetics and global self-esteem in this sample. Academic achievement emerged as a predictor of self-esteem. Gender-sensitive screening and integrated wellness programs are recommended for resource-limited settings.
Keywords: dental aesthetics, psychosocial impact, self-esteem, health sciences students, Yemen, gender differences, orthodontic treatment need
Introduction
Dental aesthetics is becoming increasingly important with respect to personal image and overall psychosocial health.1 Globally, there are an estimated 60–75% of adults between the ages of 18 and 35 who have some form of malocclusion, which can vary in severity and affect social relationships, psychological health, and a person’s overall quality of life.2,3 The effects of malocclusion extend beyond functional impairment, because individuals with this condition often find themselves feeling less confident, withdrawn from society, and at a higher risk of being subjected to psychological distress; this situation is especially evident during the formative years of young adulthood.4,5 These effects are likely magnified in professional and scholarly environments, where personal relationships and first impressions are particularly important.
A unique group of students enrolled in health sciences programs is preparing for a future in patient-facing careers that will require them to demonstrate high levels of interpersonal competence and professional presence.6 Therefore, many of these individuals possibly place heightened importance on how their teeth look to others (ie., dental aesthetics). Furthermore, an established fact is that health science students learn within an environment placing emphasis on the importance of clinical excellence, professional appearance, and effective communication, all of which may lead to heightened awareness of one’s dental aesthetic.7,8
Several recent studies have shown that dental and medical students have higher levels of aesthetic sensitivity and are more likely to perceive a need for orthodontics compared with students enrolled in non-health-related degree programs.7 However, despite the known associations between dental aesthetics and psychosocial health, the exact relationship of perceived dental appearance, perceived orthodontic treatment need, and global self-esteem among dental and medical students is still poorly defined.8–10
Current data on the psychosocial effects from dental aesthetics are primarily from Western countries with relatively developed healthcare systems, and representation among low- and middle-income countries (LMIC), which have limited access to orthodontics, is lacking.11,12 Even though validated instruments, such as the Psychosocial Impact of Dental Aesthetics Questionnaire (PIDAQ) and Rosenberg Self-esteem Scale (RSES), are routinely used separately, limited studies have evaluated these instruments together with objective measures of orthodontic treatment need, which are assessed using the Aesthetic Component of the Index of Orthodontic Treatment Need (IOTN-AC).10,13,14
Prior findings on the relationship between dental aesthetic perceptions and self-esteem are inconsistent, influenced by cultural contexts.10,15 Some studies show lower dental self-confidence correlates with decreased self-esteem,14 while others report no significant gender differences in psychosocial impact owing to educational attainment.16 These discrepancies suggest the need for further investigation in settings like Yemen, which are underrepresented in the literature.
Based on the above, this study tested the following hypotheses: (1) there is a negative association between perceived dental aesthetic distress (PIDAQ scores) and global self-esteem (RSES scores); (2) male and female health sciences students differ in the psychosocial impact of dental aesthetics; and (3) higher self-perceived orthodontic treatment need (IOTN-AC) is associated with greater psychosocial impact. The primary outcome of this study was the total PIDAQ score. Secondary outcomes included PIDAQ subscale scores (Dental Self-Confidence, Social Impact, Psychological Impact, Aesthetic Concern), RSES total score, and IOTN-AC category distribution.
In Yemen, where healthcare services are significantly challenged and orthodontic care providers are limited, no systematic investigations have been conducted on the psychosocial effects of dental aesthetics among university students. Therefore, this study aimed to evaluate these associations among undergraduate health sciences students in Sana’a.
Methodology
Study Design and Ethical Approval
A cross-sectional study was conducted between August and September 2025 to determine the psychosocial effects of dental aesthetics on the psychosocial well-being of undergraduate health sciences students in Sana’a City. Ethical approval for this study was obtained from the Research Ethics Committee of the Faculty of Dentistry, Ibn Al-Nafis University for Medical Sciences, Sana’a, Yemen (Approval No. 196, dated 02 July 2025). The study was conducted in accordance with the Declaration of Helsinki.17 All participants provided informed consent after being fully informed about the study objectives, procedures, and their right to withdraw at any time.
Selection Criteria
This study involved undergraduate students from health sciences faculties in public and private universities in Sana’a City. Inclusion criteria were: age 18–25 years, current enrollment in a health science program (medicine, dentistry, pharmacy, nursing), and willingness to participate. Students who had received orthodontic or cosmetic treatment, had congenital craniofacial deformities, or submitted incomplete responses were excluded.
Sample Size Determination
Sample size was calculated using Cochran’s formula for categorical data,18 applying a 95% confidence interval (Z = 1.96), a 5% margin of error (e = 0.05), and a 50% response distribution, yielding a minimum target of 385 participants. Ultimately, 300 health sciences students participated (response rate 77.9%). The achieved sample size remained below the calculated target; this limitation is acknowledged in the Discussion section, as it may reduce statistical power and increase the risk of Type II error. A post-hoc power analysis using G*Power (version 3.1) with a medium effect size (Cohen’s w = 0.3) and α = 0.05 showed statistical power above 80% for the chi-square tests performed, though caution is warranted for secondary analyses.
Questionnaire Development, Validity, Reliability, and Pilot Testing
The structured, self-administered questionnaire contained three standardized instruments: PIDAQ, RSES, and IOTN-AC, developed from previously validated survey tools13,16,19–21 with minor modifications for clarity and cultural appropriateness. Specifically, minor wording adjustments were made to three PIDAQ items to improve comprehension in the Yemeni context (eg., “I envy people with nice teeth” was rephrased to “I feel envious when I see people with attractive teeth”; these changes did not alter the core meaning or response structure). No modifications were made to the RSES or IOTN-AC. Although PIDAQ has been validated for Arabic-speaking adolescents,22 its use to investigate connections between dental aesthetics, self-esteem, and treatment need in young adults remains unexplored.
Content validity of the adapted questionnaire was assessed by a panel of multidisciplinary experts (orthodontists, public health researchers, clinical psychologists) to ensure cultural appropriateness, despite the use of previously validated instruments. Each reviewer independently rated clarity, relevance, and simplicity on a 4-point scale, yielding a Content Validity Index of 0.94, indicating good validity for the Yemeni context.
A pilot study with 30 students (excluded from final analysis) assessed feasibility, clarity, and completion time (8–10 minutes). Minor wording edits were made based on pilot feedback. Internal consistency was good: total PIDAQ (α = 0.80), Dental Self-Confidence (α = 0.92), Social Impact (α = 0.90), Psychological Impact (α = 0.84), Aesthetic Concern (α = 0.91), and RSES (α = 0.86). Test-retest reliability at two weeks (n=30) showed excellent temporal stability (ICC = 0.91). Figure 1 presents the participant recruitment and exclusion process.
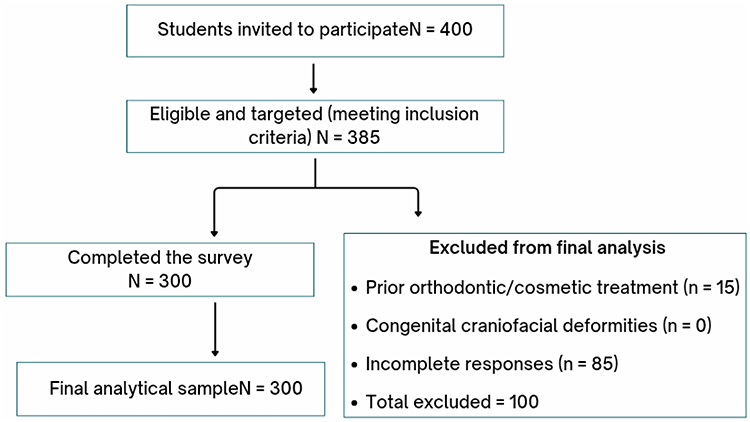 |
Figure 1 Flowchart of Participant Recruitment. |
Questionnaire Parts
The final version of the questionnaire comprised 42 questions and was divided into four sequential parts to assess the psychosocial impact of dental aesthetics, evaluate levels of global self-esteem, and examine their association among undergraduate health sciences students in Sana’a City.
The first part consisted of eight questions addressing participants’ sociodemographic and academic profiles, including age (18–21 years or 22–25years), gender (male or female), type of university attending (public or private), academic major (medicine, dentistry, pharmacy, nursing), academic level (1st, 2nd, 3rd, 4th, or 5th year), and academic performance (excellent, very good, good, acceptable, or needs improvement). The first part also contained two dichotomous (Yes/No) screening questions used to determine eligibility: “Have you ever had, or are you currently wearing orthodontic appliance?” and “Have you ever had a cosmetic treatment to improve the appearance of your teeth?”
The second part of the questionnaire examined the psychosocial impact of dental aesthetics using PIDAQ,16,19,20 with 23 items across four subscales: Dental Self-Confidence (6 items, measuring positive feelings), Social Impact (8 items, evaluating social interaction effects), Psychological Impact (6 items, assessing emotional responses), and Aesthetic Concern (3 items, focusing on negative feelings when seeing one’s teeth). Items are rated on a 5-point Likert scale (0 = “Not at all” to 4 = “Very much”). Subscale scores are mean item scores. Total PIDAQ scores were interpreted as follows based on the scale’s theoretical range (0–4): scores <1.5 considered low impact, 1.5–2.5 mild impact, 2.5–3.5 moderate impact, and >3.5 severe impact.19
The third part of the questionnaire evaluated global self-esteem by using the standardized version of RSES.21,23 This unidimensional scale consists of 10 items and involves 5 with positive-worded and 5 with negative-worded statements, which are rated on a 4-point Likert-type agreement scale, ranging from “strongly disagree” to “strongly agree.” The total score for each individual who completes RSES may range from 0 to 40, and cut-off scores are established at low (<15), moderate (15–25), or high (>25) self-esteem.
The fourth part of the questionnaire aimed to evaluate self-reported need for orthodontic treatment based on IOTN-AC.24,25 Assessment was performed under standardized conditions, in which participants viewed digital high-quality reproductions of the 10-grade photographic scale depicting various dental aesthetic impairments. After showing the images, they were instructed to select the image that most closely matches their own dentition, indicating their perceived need for orthodontic treatment. Aesthetic grades were classified into three levels of treatment need (ie., “no need”-grades, 1–4; “borderline need”-grades, 5–7; “definite need”-grades, 8–10) according to clinical-based criteria.26
Data Collection
Data were collected through self-reporting online questionnaires administered using the Google Forms platform and circulated through social media channels frequently used by students (eg., WhatsApp, Facebook, and Telegram). Prior to data collection, the aims of this study and the importance of voluntary and anonymous participation were clearly expressed to participants. After the initial survey link was distributed, two follow-up reminders were sent weekly to encourage participants to complete the survey.27 This multi-wave approach is identified to significantly improve participation rates in digital survey research among student populations.28,29 Technical safeguards in Google Forms limited responses to one per Email and excluded incomplete submissions with over 10% missing data in essential sections.
Statistical Analysis
SPSS version 26 (IBM Corp., Armonk, NY, USA), was used for data analysis. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were calculated for participants’ demographic characteristics and their associated scale scores. Analysis for normality of the distribution of the variables was completed using the Shapiro–Wilk test. Group differences were analyzed using independent-sample t-tests and one-way ANOVA with Tukey’s HSD post-hoc comparisons. Pearson’s correlation examined the relationship between the PIDAQ and RSES scores. Multiple linear regression analysis indicated the predictors of self-esteem with associated sociodemographic variables and relevant academic variables. A p-value of < 0.05 indicated statistically significant results for all analyses.
Results
Participants’ Demographics
Of the 400 undergraduate health sciences students invited, 385 were eligible and targeted, and 300 completed the questionnaire. The majority were female (70.7%, n = 212), aged 22–25 years (59.3%, n = 178), and attending private universities (60.0%, n = 180). Pharmacy was the most common discipline (25.7%, n = 77), followed by medicine (23.7%, n = 71) and nursing (20.7%, n = 62). Nearly one-third (32%, n = 96) were in their fourth year. Academic performance was self-reported as excellent (37.3%, n = 112) or very good (32.3%, n = 97).
Descriptive Statistics of the PIDAQ Scores
Table 1 shows PIDAQ descriptive statistics. The total PIDAQ mean score was 2.40 ± 0.62, which falls within the mild psychosocial impact range (1.5–2.5) according to established PIDAQ scoring conventions.19 Dental Self-Confidence had the highest subscale score (3.40 ± 1.04), indicating positive self-perception of dental aesthetics. Social Impact (1.94 ± 0.93) and Aesthetic Concern (2.08 ± 1.22) were lower, reflecting perceived negative psychosocial impact.
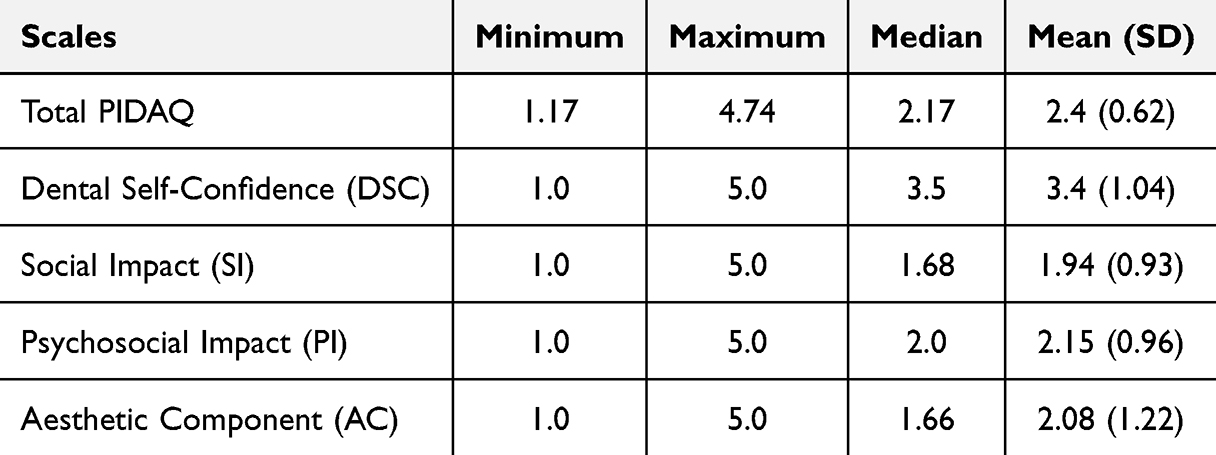 |
Table 1 Descriptive Statistics of the Psychosocial Impact of Dental Aesthetics Questionnaire (PIDAQ) Scores (n = 300) |
Distribution of PIDAQ Scores Across Demographic Variables
Table 2 presents PIDAQ scores by demographic variables. Male students had significantly higher total PIDAQ scores than females (2.52 ± 0.69 vs. 2.35 ± 0.56; p = 0.026), indicating greater psychosocial impact among males. No significant differences were found for age, university type, academic level, or academic performance (all p > 0.05). Differences across academic majors were not statistically significant (p = 0.091). Gender was the key sociodemographic variable associated with psychosocial outcomes related to dental aesthetics.
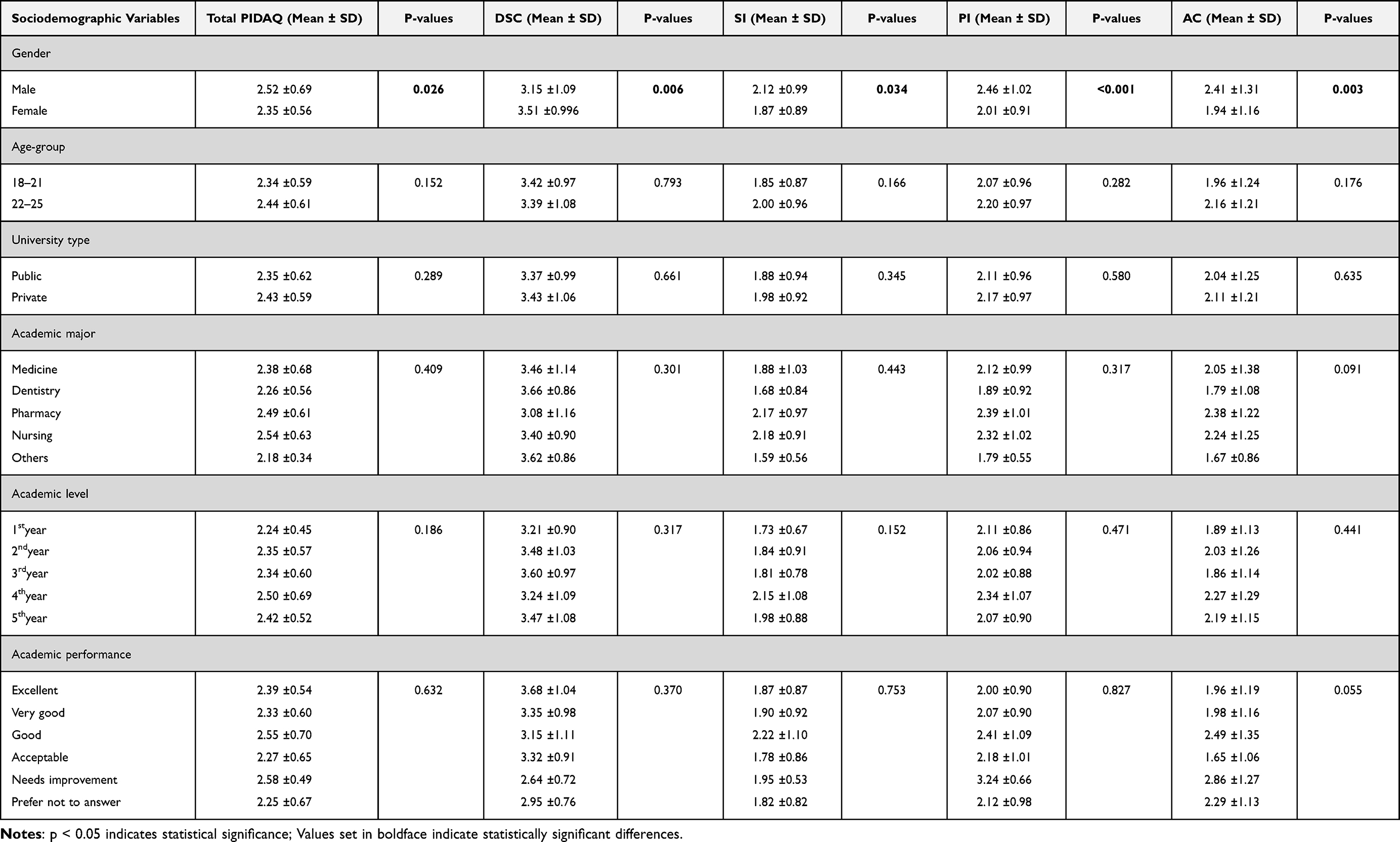 |
Table 2 Comparison of PIDAQ Scores Across Sociodemographic Variables (n = 300) |
Self-Esteem Scores and Sociodemographic Associations
Table 3 presents RSES scores by participant characteristics. The mean RSES score was 3.30 ± 0.49 (range 0–40), representing generally positive global self-esteem. No statistically significant differences in self-esteem were found for any sociodemographic or academic variable (all p > 0.05).
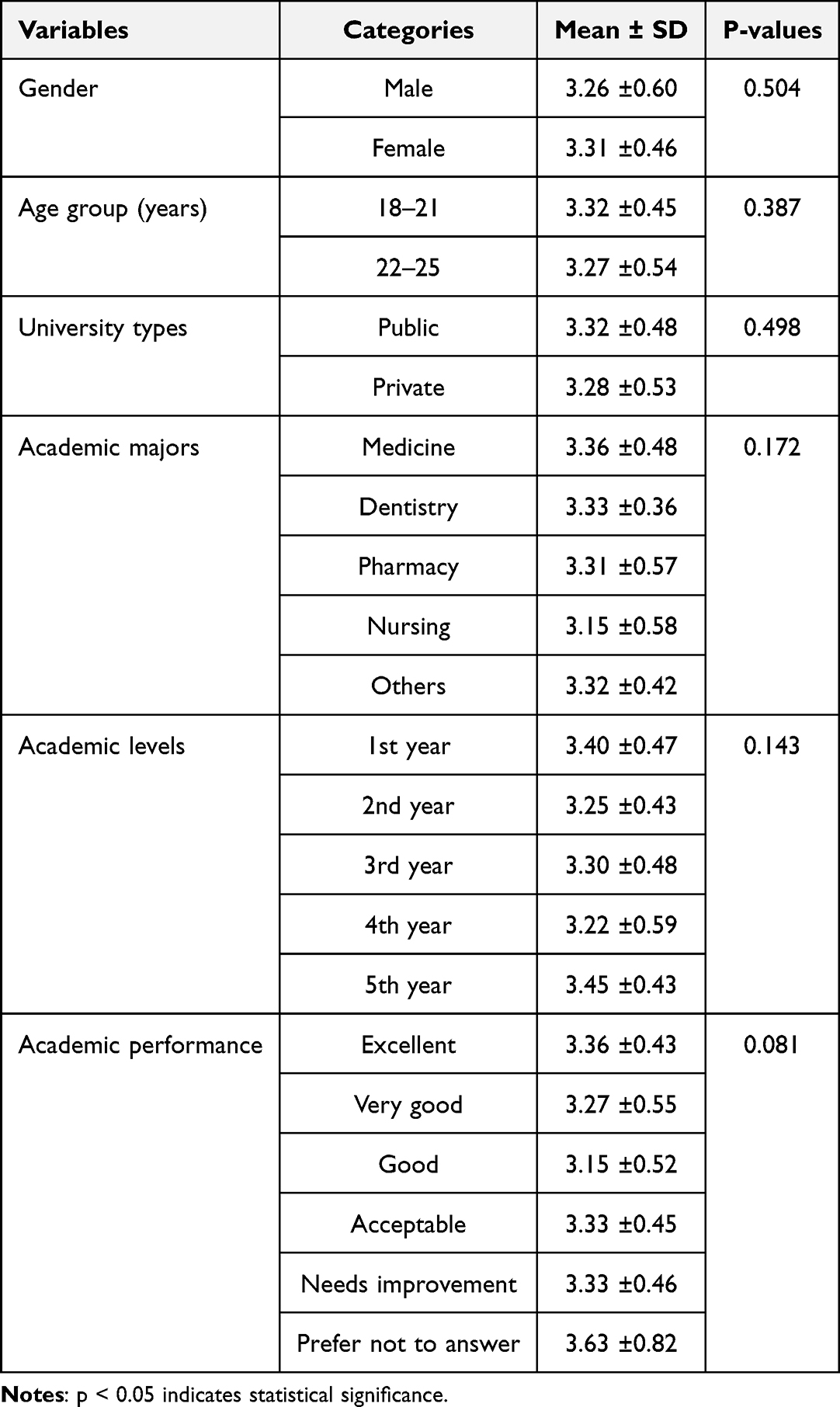 |
Table 3 Self-Esteem (RSES) by Sociodemographic Characteristics (n = 300) |
Self-Esteem Predictors
Table 4 presents the multiple linear regression analysis for predictors of self-esteem. Academic year (β = 0.281, p = 0.002) and grade point average (β = 0.095, p = 0.047) were significant predictors of RSES scores. Neither gender nor age significantly predicted self-esteem (p > 0.05).
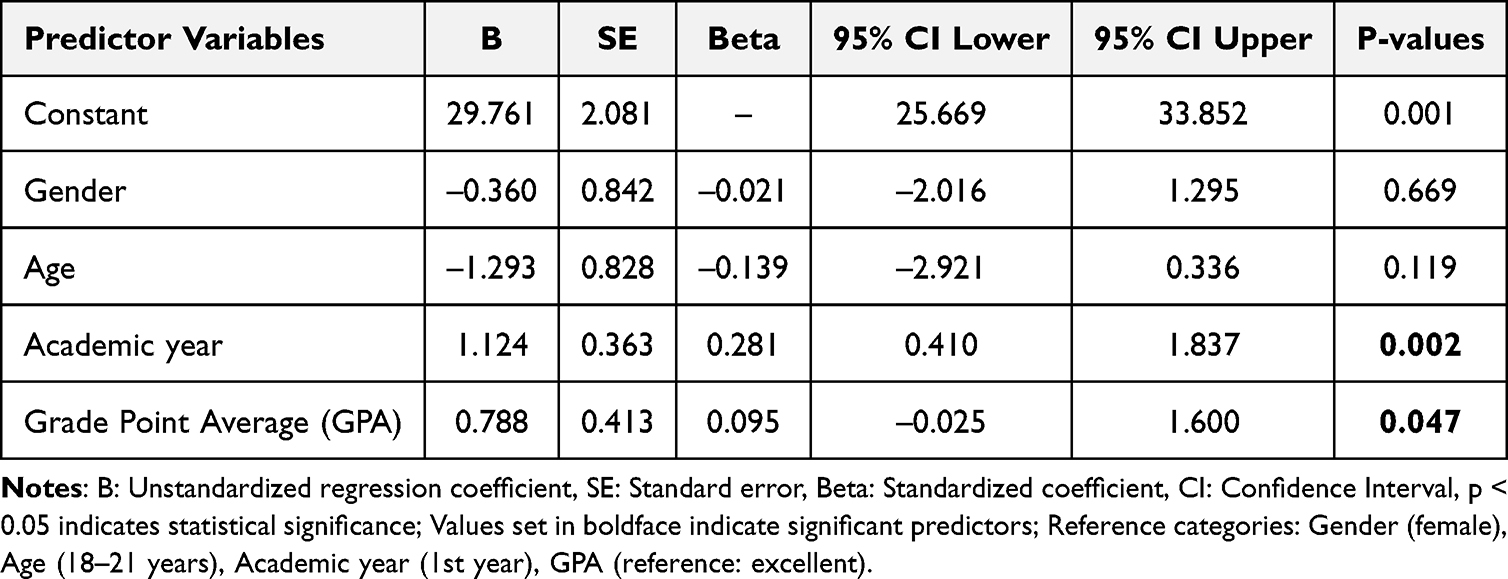 |
Table 4 Multiple Linear Regression Model: Rosenberg’s Self-Esteem Scale in Relation to Sociodemographic Variables (n = 300) |
Correlation Between Dental Aesthetics and Self-Esteem
Table 5 presents Spearman correlation coefficients between PIDAQ scales and RSES. No statistically significant association was detected between total PIDAQ scores and self-esteem in this sample (r = −0.012, p = 0.834). Similarly, no PIDAQ subscale showed a statistically significant correlation with RSES (all p > 0.05). These findings indicate that within the studied sample, the perceived psychosocial impact of dental aesthetics did not demonstrate a direct linear relationship with overall self-esteem.
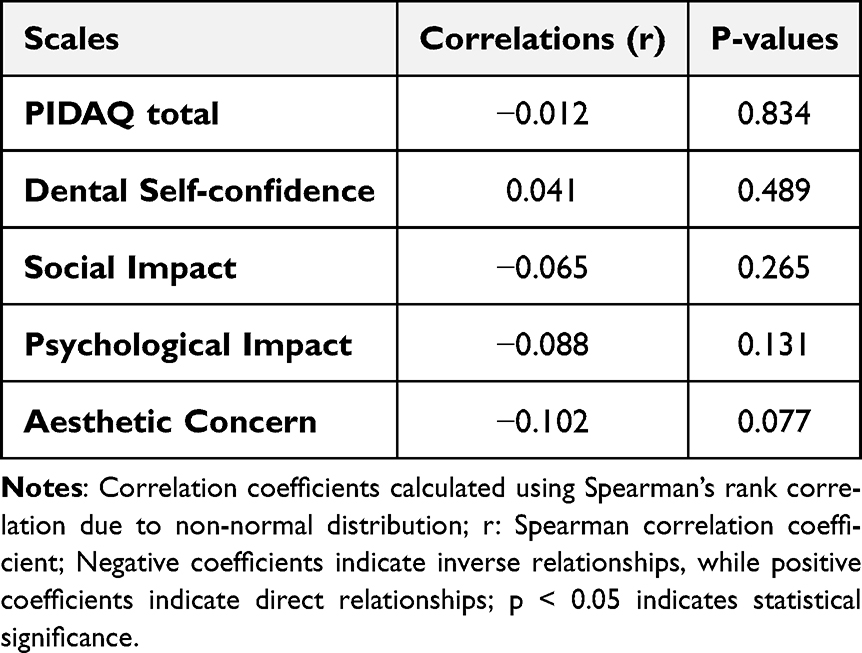 |
Table 5 Spearman Correlation Coefficients Between Psychosocial Impact of Dental Aesthetics (PIDAQ) Scales and Self-Esteem (RSES) (n = 300) |
Distribution of Aesthetic Component (IOTN-AC) Categories
Table 6 presents the distribution of IOTN-AC categories. The majority (84.7%, n = 254) had “no need” for orthodontic treatment (grades 1–4), while 10.3% (n = 31) were borderline (grades 5–7) and 5.0% (n = 15) had definite need (grades 8–10). A statistically significant association was found between AC grades and gender (p = 0.002) and academic performance (p = 0.009).
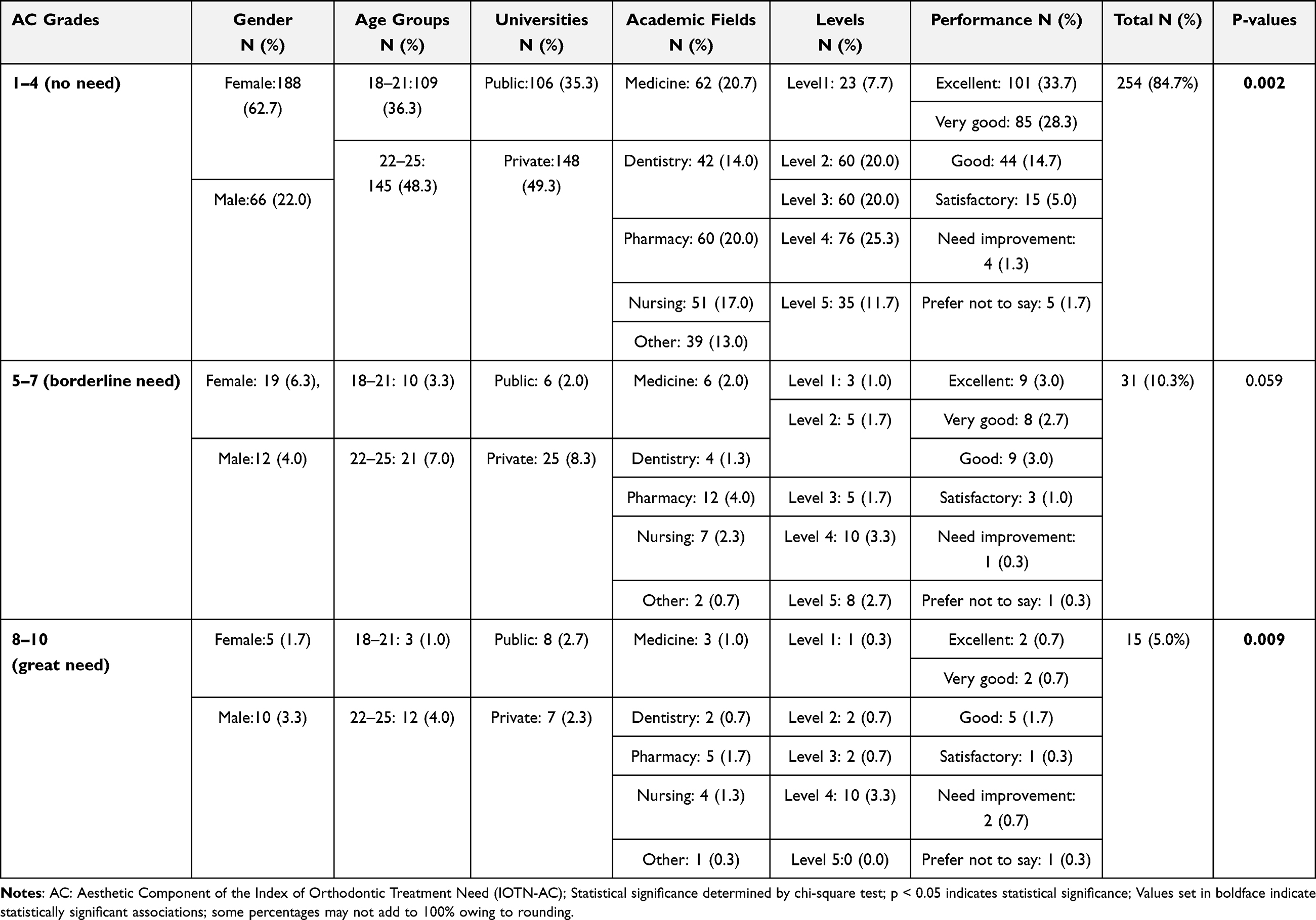 |
Table 6 Distribution of Aesthetic Component by Sociodemographic Variables (n = 300) |
Association Between Orthodontic AC, PIDAQ, and Self-Esteem
Table 7 shows the relationship between AC categories and psychosocial measures. Mean total PIDAQ scores increased with higher AC categories: 2.34 ± 0.35 (no need), 2.67 ± 0.37 (borderline need), and 2.82 ± 0.41 (definite need). Post-hoc analyses revealed significant differences between the no-need group and both other groups (p < 0.05). Self-esteem (RSES) scores did not vary significantly across AC categories (p = 0.724). The imbalance in AC category distribution (84.7% “no need”) is acknowledged in the Discussion as a potential attenuating factor for observed associations.
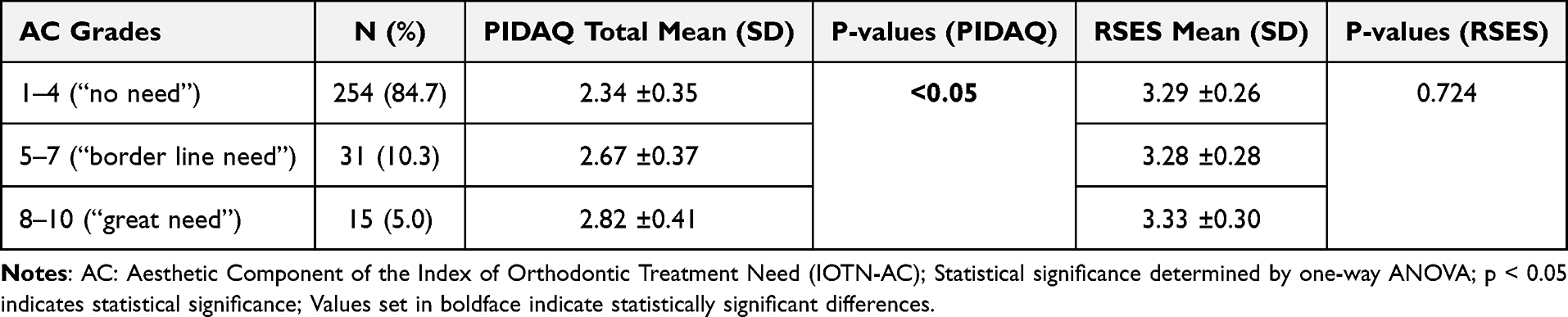 |
Table 7 Mean Scores of Psychosocial Impact (PIDAQ) and Self-Esteem (RSES) by Aesthetic Component (IOTN-AC) Category (n = 300) |
Discussion
Summary of Key Findings
The current research is the first to examine the psychosocial effects of appearance in health science students in Yemen. The findings present distinct patterns that differ from the Western and regional Middle Eastern literature.11,12 The findings can be summarized in three parts. The first finding is related to gender discrepancy, with men having reported significantly higher levels of anxiety across all of the PIDAQ measures than women. The second finding relates to the fact that no relationship exists between level of dental distress and global self-esteem as measured by RSES. Lastly, the finding supports the idea that as the self-perceived need for orthodontic treatment increases (dose-response), so does the psychosocial burden associated with it, which is then compounded by the fact that academic progress was found to be the primary indicator of self-worth in this population affected by conflict.
Gender Paradox in the Yemeni Context
Although traditional Western studies have established females’ considerable interest in appearance-based issues,30,31 our findings demonstrate that this idea is not the case in Yemen. Male health science students in Yemen reported significantly higher scores than their female counterparts on the new PIDAQ when broken down into the four subscales of SI, PI, AC, and overall. Although this unexpected finding is not unique to Yemen, multiple studies from other patriarchal countries in the Middle East demonstrate similar findings.32,33 Accordingly, this finding suggests that male healthcare trainees in the aforementioned patriarchal countries may experience different pressures relating to professional expectations.
In Yemen, owing to traditional gender roles and limited financial resources, male students who plan on working with patients perceive such factors as dental aesthetics as an element of their own appearance and also as a significant factor in their ability to establish themselves as professionals and develop trust with patients they will work with.6,7 These different pressures resulting from the intersection of cultural expectations, professional socialization, and financial limitations may create a unique set of gender dynamics with respect to the psychology of appearance.
Difference Between Global Self-Esteem and Dental Aesthetics
No significant correlation was found between students’ dental aesthetic distress as measured by PIDAQ and their global self-esteem as measured by RSES. This finding contrasts with studies conducted elsewhere, which have found significant negative correlations between the two variables.14,15 Theoretically, the differences may be explained based on the concept of the distinction between domain-specific and global levels of self-worth. PIDAQ focuses on distress associated with dental-specific social and aesthetic areas, while RSES assesses a markedly global and stable concept of self-esteem. Our results suggest that students’ perceptions of dental aesthetics are compartmentalized from their overall self-perception, at least in Yemen, where an unstable society may cause individuals to be more concerned about the more immediate needs of safety and education rather than developing concerns about aesthetics.34 Accordingly, we may conclude a disconnect between dental aesthetics and global self-esteem, but we cannot make definitive statements on the relationship between dental aesthetics and global self-esteem in this population based on the current sample.
Orthodontic Need and Psychosocial Burden
A dose-response relationship was observed between IOTN-AC categories and PIDAQ scores, consistent with previous findings.13,14,35 Even individuals with “borderline need” reported significantly higher psychological distress than the “no need” group, suggesting that even mild aesthetic concerns can create meaningful psychosocial burden when perceived as important. Given the limited orthodontic access in Yemen, this finding has important implications for health policy. However, the imbalance in AC category distribution (84.7% “no need”) may have attenuated the strength of observed associations, and this limitation should be considered.
Clinical and Translational Implications
The implications of this study’s findings have several implications for health practice Yemen and in similar communities. First, health services in universities need to create protocols for screening that reflect the fact that men are also at risk for aesthetic-related distress.36 Traditionally, screening protocols have only considered aesthetic-related distress among women. Second, the idea that a dissociation exists between individuals’ dental aesthetics and their overall self-esteem means that screening needs to include an understanding of how dental aesthetics impact people’s social life, and not just viewing the psychological impact in terms of people/individuals.37 Third, a strong association between academic achievement and self-esteem indicates the need for universities to establish integrated programming to address dental health, mental health, and academic success as one unit.38,39 Lastly, although relatively few participants indicated they were in need of orthodontic treatment, the numerous individuals who expressed concern about the aesthetics of their teeth emphasizes the need for early prevention education and intervention. These types of education/intervention will help reduce the long-term financial and psychosocial burdens related to dental aesthetic problems.19
Limitations
Several limitations should be acknowledged. First, the cross-sectional design precludes causal inferences. Second, the sample size (n=300) fell below the calculated target (n=385), potentially reducing statistical power and increasing Type II error risk, particularly for secondary analyses. Third, convenience sampling via Internet-based survey may have introduced selection bias; students without internet access or those less concerned about dental aesthetics may have been underrepresented. Fourth, the sample was predominantly female (70.7%) and recruited only from Sana’a, limiting generalizability to rural areas or male-dominated health sciences programs. Fifth, reliance on self-reported measures (including IOTN-AC without clinical examination) may introduce social desirability and recall biases, although anonymity was maintained. Sixth, potential confounding variables such as socioeconomic status, prior orthodontic awareness, and mental health conditions were not measured. Seventh, the IOTN-AC distribution was heavily skewed toward “no need” (84.7%), which may have attenuated observed associations. Eighth, the study did not include a comparison group of non-health sciences students. Future studies should address these limitations through clinical examinations, larger and more representative samples, and inclusion of comparison groups.
Conclusion
Based on this cross-sectional study of health sciences students in Yemen, dental aesthetics significantly affects psychosocial well-being, with a greater impact observed among male students than typically reported in Western literature. Self-perceived orthodontic need showed a dose-response association with psychological distress. However, no statistically significant association was detected between dental aesthetics and global self-esteem in this sample. Academic achievement emerged as a significant predictor of self-esteem. Authors recommend gender-sensitive oral health screening and integrated wellness programs addressing both aesthetic concerns and mental health in resource-limited academic settings.
Data Sharing Statement
The datasets created and/or analyzed during the current study are not publicly available due to confidentiality but can be made available by the corresponding author (Baker M. Abdullah) upon reasonable request.
Ethics Approval and Consent to Participate
Ethical approval for this study was obtained from the Research Ethics Committee of the Faculty of Dentistry, Ibn Al-Nafis University for Medical Sciences, Sana’a, Yemen (Approval No. 196, dated 02 July 2025). All participants provided informed consent after being fully informed about the study objectives, procedures, and their right to withdraw at any time.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xiao L, Mai W, Chen S, et al. Psychosocial impact of dental aesthetics in adolescent: an evaluation of a latent profile and its associated risk factors. BMC Oral Health. 2024;24(1):1076. doi:10.1186/s12903-024-04844-z
2. Doughan MB, Khandakji M, Khoury B, Ghafari JG. Assessment of psychosocial parameters in adolescents seeking orthodontic treatment. BMC Oral Health. 2024;24(1):1299. doi:10.1186/s12903-024-04875-6
3. Claudino D, Traebert J. Malocclusion, dental aesthetic self-perception and quality of life in a 18 to 21 year-old population: a cross section study. BMC Oral Health. 2013;13:3. doi:10.1186/1472-6831-13-3
4. Yamini Priyanka JS, Bhavya P, Srinivas B, Singaraju GS, Vivek Reddy G, Mandava P. An assessment of the subjective psychological and social effects of malocclusion-related dental aesthetics and its influence on body self-image and oral health-related quality of life in young adults. Cureus. 2024;16(5):e60120. doi:10.7759/cureus.60120
5. Sicari F, Merlo EM, Gentile G, et al. Body image and psychological impact of dental appearance in adolescents with malocclusion: a Preliminary Exploratory Study. Children. 2023;10(10):1691. doi:10.3390/children10101691
6. Negm LMMA, Mersal FA, Fawzy MS, Rajennal AT, Alanazi RS, Alanazi LO. Challenges of nursing students during clinical training: a nursing perspective. AIMS Public Health. 2024;11(2):379–13. doi:10.3934/publichealth.2024019
7. Kovačić I, Miloš M, Kurkutović M, Čelebić A, Petričević N. Influence of education level and gender of dental students on perception of dental aesthetics. BMC Oral Health. 2024;24(1):398. doi:10.1186/s12903-024-04115-x
8. Nazir MA, Alaqili FA, Alnajjar LS, et al. Aesthetic and orthodontic treatment desires and their psychosocial impact in dental students: a Questionnaire Study. Patient Prefer Adherence. 2025;19:1487–1495. doi:10.2147/PPA.S524287
9. Militi A, Sicari F, Portelli M, et al. Psychological and social effects of oral health and dental aesthetic in adolescence and early adulthood: an Observational Study. Int J Environ Res Public Health. 2021;18(17):9022. doi:10.3390/ijerph18179022
10. Bahar AD, Sagi MS, Mohd Zuhairi FA, Wan Hassan WN. Dental aesthetics and self-esteem of patients seeking orthodontic treatment. Healthcare. 2024;12(16):1576. doi:10.3390/healthcare12161576
11. Hassan AH, Hel-S A. Association of orthodontic treatment needs and oral health-related quality of life in young adults. Am J Orthod Dentofacial Orthop. 2010;137(1):42–47. doi:10.1016/j.ajodo.2008.02.024
12. Alhokair RA, Alanzan AS, Alamery GH. Socioeconomic status and its effect on the dental esthetics: a survey-based study in Saudi Arabia. Inter J Medic Devel Count. 2021;5(1):006–011. doi:10.24911/IJMDC.51-1600602889
13. Brook PH, Shaw WC. The development of an index of orthodontic treatment priority. Eur J Orthod. 1989;11(3):309–320. doi:10.1093/oxfordjournals.ejo.a035999
14. Stojilković M, Gušić I, Berić J, et al. Evaluating the influence of dental aesthetics on psychosocial well-being and self-esteem among students of the University of Novi Sad, Serbia: a cross-sectional study. BMC Oral Health. 2024;24(1):277. doi:10.1186/s12903-024-04002-5
15. Ghorbani Z, Esmaeili S, Shahbazi S, Jarrahzadeh M, Madihi S. Self-esteem and its influence on the inclination toward esthetic dental treatments: a cross-sectional study. BMC Psychol. 2025;13(1):140. doi:10.1186/s40359-025-02423-7
16. Faraj M, Shobha S, Latheef V, Nivedita P. Does Psychosocial Impact of Dental Aesthetics Questionnaire (PIDAQ) reflect the impact of malocclusion on facial aesthetics? Dental Press J Orthod. 2023;28(4):e232211. doi:10.1590/2177-6709.28.4.e232211oar
17. Parums DV. Editorial: the 2024 revision of the declaration of helsinki and its continued role as a code of ethics to guide medical research. Med Sci Monit. 2024;30:e947428. doi:10.12659/MSM.947428
18. Cochran WG. Sampling Techniques.
19. Klages U, Claus N, Wehrbein H, Zentner A. Development of a questionnaire for assessment of the psychosocial impact of dental aesthetics in young adults. Eur J Orthod. 2006;28(2):103–111. doi:10.1093/ejo/cji083
20. Gómez-Polo C, Sánchez de Martín MA, Curto A, Montero J, Martín Casado AM. Validation of a new questionnaire for assessing the Psychosocial Impact of Gingival Aesthetics (PIGAQ). J Clin Periodontol. 2025;52(3):399–407. doi:10.1111/jcpe.14081
21. Abbasi A, Moradkhani A, Shahri B, Khosravi H, Sohrabi A, Mirhosseini S. Psychometric evaluation of the Persian version of the rosenberg self-esteem scale among medical sciences students. Front Psychol. 2024;15:1451862. doi:10.3389/fpsyg.2024.1451862
22. Alsanabani AAM, Yusof ZYM, Wan Hassan WN, Aldhorae K, Alyamani HA. Validity and reliability of the arabic version of the psychosocial impact of dental aesthetics questionnaire for yemeni adolescents. Children. 2021;8(6):448. doi:10.3390/children8060448
23. Jiang C, Zhu Y, Luo Y, et al. Validation of the Chinese version of the rosenberg self-esteem scale: evidence from a three-wave longitudinal study. BMC Psychol. 2023;11(1):345. doi:10.1186/s40359-023-01293-1
24. Anagnostou C, Zogakis IP, Pagkozidis I, Dardavesis T, Matiakis A, Tsimtsiou Z. Predictors of willingness to uptake orthodontic treatment and qualitative insights into the reasons for its postponement in young adults. Angle Orthod. 2025;95(3):290–295. doi:10.2319/070724-541.1
25. Kapoor P, Singh H. Evaluation of esthetic component of the index of orthodontic treatment need: the orthodontists’ perspective. Indian J Dent. 2015;6(4):181–184. doi:10.4103/0975-962X.170368
26. Jasim ES, Kadhom ZM, Al-Groosh D. Comparative evaluation of orthodontic treatment needs index and the dental aesthetic index to assess the need for orthodontic treatment from the participants’ perspective: a cross-sectional study. J Orthod Sci. 2025;14:30. doi:10.4103/jos.jos_24_25
27. Jankowski J, Krokosz S, Zięba S, et al. Self-assessed preparedness of final-year dental students and dental interns in Poland: a multi-institutional study. BMC Med Educ. 2025;25(1):627. doi:10.1186/s12909-025-07215-6
28. Jezek AH, Ekholm O, Thygesen LC, Christensen AI. The impact of reminders on representativeness and survey estimates among web-mode invited in the Danish National Health Survey. Eur J Public Health. 2025;35(2):256–262. doi:10.1093/eurpub/ckae176
29. Joseph AM, Alsalman RA, Almasoud WA, et al. Predicting the employment of teledentistry in clinical practice by the Saudi dental community using a theoretical model. Digit Health. 2024;10:20552076241253739. doi:10.1177/20552076241253739
30. Tin-Oo MM, Saddki N, Hassan N. Factors influencing patient satisfaction with dental appearance and treatments they desire to improve aesthetics. BMC Oral Health. 2011;11:6. doi:10.1186/1472-6831-11-6
31. Akarslan ZZ, Sadik B, Erten H, Karabulut E. Dental esthetic satisfaction, received and desired dental treatments for improvement of esthetics. Indian J Dent Res. 2009;20(2):195–200. doi:10.4103/0970-9290.52902
32. Al-Zarea BK. Satisfaction with appearance and the desired treatment to improve aesthetics. Int J Dent. 2013;2013:912368. doi:10.1155/2013/912368
33. Ghazi OM, Alhashimi AH, Jasim GM. Assessment of the psychological impact of dental aesthetics among undergraduate university students in Iraq. J Orthod Sci. 2023;12:34. doi:10.4103/jos.jos_110_22
34. Al-Ja’afreh SA-H, Algoma AA, Al-Habies FA, Abudoush AN, Aloran OIH. The impact of psychosocial support and psychological well-being among expatriate students. J Inter Students. 2025;15(3):183–202.
35. Muniz-Junior AB, De Moraes CN, De Lima Gomes S, et al. Psychosocial impact of dental aesthetics, orthodontic treatment needs, and self-esteem in amazonian adolescents. Biosc J. 2025;41:e41010. doi:10.14393/BJ-v41n0a2025-76534
36. Birkeland K, Bøe OE, Wisth PJ. Relationship between occlusion and satisfaction with dental appearance in orthodontically treated and untreated groups. A longitudinal study. Eur J Orthod. 2000;22(5):509–518. doi:10.1093/ejo/22.5.509
37. Venete A, Trillo-Lumbreras E, Prado-Gascó VJ, Bellot-Arcís C, Almerich-Silla JM, Montiel-Company JM. Relationship between the psychosocial impact of dental aesthetics and perfectionism and self-esteem. J Clin Exp Dent. 2017;9(12):e1453–e1458. doi:10.4317/jced.54481
38. Albagawi BS, Alsalamah YS, Dabosi S, et al. The mediating role of self-esteem and mental wellbeing in the association between emotional intelligence and motivation among saudi nursing students. SAGE Open Nurs. 2025;11:23779608251365315. doi:10.1177/23779608251365315
39. Samir AA, Elamir AH, Basyouni Helal M, et al. Sociodemographic, lifestyle, and psychological factors as controllable predictors of academic self-efficacy after reforming a medical education system; the Egyptian Nationwide experience. BMC Med Educ. 2025;25(1):211. doi:10.1186/s12909-025-06805-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.