Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Association Between Constipation and Frailty in Maintenance Hemodialysis Patients: A Cross-Sectional Study
Authors Wu S ![]() , Dong T
, Dong T ![]() , Cao P, Hu N
, Cao P, Hu N ![]() , Deng B
, Deng B ![]() , Qiao Q
, Qiao Q ![]()
Received 5 July 2025
Accepted for publication 7 November 2025
Published 21 November 2025 Volume 2025:18 Pages 7659—7666
DOI https://doi.org/10.2147/JMDH.S551776
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Charles V Pollack
Sheng Wu, Ting Dong, Peiyang Cao, Nan Hu, Bingqing Deng, Qing Qiao
Department of Nephrology, The Fourth Affiliated Hospital of Soochow University (Suzhou Dushu Lake Hospital), Suzhou, Jiangsu, People’s Republic of China
Correspondence: Qing Qiao, Email [email protected] Bingqing Deng, Email [email protected]
Purpose: Among patients undergoing maintenance hemodialysis (MHD), constipation and frailty are not only common but also associated with adverse clinical outcomes. The objective of this study was to investigate the relationship between constipation and frailty in this population.
Patients and Methods: This cross-sectional study included patients receiving MHD three times per week in China from November 2023 to November 2024. Rome IV criteria and Fried Frailty Phenotype scale were applied to evaluate constipation and frailty respectively. Multivariate logistic regression analysis was utilized to analyze the correlation between constipation and frailty.
Results: Among the 207 enrolled MHD patients (mean age 58.6 ± 14.7 years; 78 females; median hemodialysis vintage 38.4 months), 100 (48.3%) were diagnosed with constipation and 63 (30.4%) with frailty. After adjusting for clinical characteristics, constipation was associated with frailty (OR: 7.61, 95% CI: 2.74– 21.13). Among the five frailty components, slow gait speed (OR: 2.90, 95% CI: 1.20– 7.00) and low physical activity (OR: 3.51, 95% CI: 1.15– 10.74) were independently associated with constipation.
Conclusion: Frailty is independently associated with constipation in MHD patients. It is important to highlight the significance of monitoring the frailty among MHD patients with constipation.
Keywords: constipation, frailty, maintenance hemodialysis, prevalence
Introduction
Constipation is a prevalent gastrointestinal disorder worldwide, particularly concerning in vulnerable populations such as maintenance hemodialysis (MHD) patients—a life-sustaining renal replacement therapy for individuals with end-stage renal disease.1 It is characterized by dry stools, reduced defecation frequency, excessive straining during defecation, abdominal distension, and abdominal pain.2 Reported prevalence rates of constipation among MHD patients range from 25.9% to 63.1%.3–6 Although constipation is conventionally viewed as a benign and self-limiting condition, emerging evidence indicates its independent association with adverse clinical outcomes, such as all-cause mortality and cardiovascular event.7
Beyond gastrointestinal discomfort, constipation may also reflect systemic vulnerability, raising the question of its potential link with frailty—a multidimensional syndrome highly prevalent in MHD patients. Frailty is a clinical syndrome characterized by progressive decline in physical functioning and cognitive capacity.8 Its prevalence in MHD patients ranges from 29.6% to 82.0%.9 MHD patients with frailty are more prone to adverse outcomes such as mortality, hospitalization, and cardiovascular events and impaired quality of life.10,11
Previous studies have identified an association between constipation and frailty in various populations.12–14 However, to our knowledge, despite the high prevalence of both conditions, no study has specifically examined the association between constipation and frailty among MHD patients, nor identified which frailty components are most strongly linked to constipation.
To address these issues, this study investigates the relationship between constipation and frailty, including its various components, in a cohort of MHD patients.
Materials and Methods
Study Design and Participants
This cross-sectional study screened 260 MHD patients at The Fourth Affiliated Hospital of Soochow University in China, from November 2023 to November 2024. After applying the inclusion and exclusion criteria, 207 patients were included in the final analysis.
Inclusion and Exclusion Criteria
Participants were eligible if they met all of the following criteria: (1) age ≥18 years; (2) diagnosis of end-stage renal disease and receipt of MHD three times per week; (3) hemodialysis vintage exceeding three months. Individuals were excluded for any of the following reasons: (1) documented organic gastrointestinal disorders (eg, colorectal carcinoma, Crohn’s disease); (2) inability or refusal to engage in the protocol-specified assessments or provide complete questionnaire responses. Written informed consent was obtained from all participants prior to enrollment. This study received ethical approval from the Research Ethics Committee of The Fourth Affiliated Hospital of Soochow University and was conducted in accordance with the principles of the Declaration of Helsinki.
Data Collection and Variables
The collected dataset encompassed three domains: Demographic characteristics (age, sex, and body mass index [BMI]), Clinical information (hemodialysis vintage, comorbid conditions, and polypharmacy), and Pre-dialysis laboratory profiles (serum albumin, serum hemoglobin, C-reactive protein, serum calcium, and serum phosphorus). Polypharmacy was defined as the concurrent use of five or more medications for therapeutic purposes.15
Constipation Assessment
The diagnosis of constipation was established according to the Rome IV criteria,16 requiring fulfillment of all three conditions: (1) Symptom criteria (≥2 of the following): hard or lumpy stools in ≥25% of defecations; straining during ≥25% of defecation; sensation of anorectal obstruction in ≥25% of defecation; sensation of incomplete evacuation in ≥25% of defecation; requirement for manual maneuvers (eg, digital disimpaction, pelvic floor support) to facilitate ≥25% of bowel movements; or fewer than three unassisted bowel movements occurring weekly. (2) Diagnostic criteria for irritable bowel syndrome were not met. (3) Loose stools were rarely present without the use of laxatives.
Frailty Assessment
Fried Frailty Phenotype scale was applied to evaluate the frailty of MHD patients,17 a validated tool for predicting adverse outcomes in end-stage renal disease populations.18 This scale comprises five components (scored 0 or 1 per item, total 0–5): (1) Unintentional weight loss: >5% body weight reduction or >4.5 kg over the past year. (2) Slow gait speed: A single 4.57-meter walk test conducted 30 minutes before hemodialysis in a quiet environment. (3) Low grip strength: The mean value of three trials performed on the non-fistula hand using a digital dynamometer in the same pre-dialysis setting. (4) Low physical activity: <383 kcal/week (males) or <270 kcal/week (females). Information on physical activity was collected via a standardized interview using the Minnesota Leisure Time Activities Questionnaire.17 (5) Self-reported exhaustion: based on two items from the Center for Epidemiological Studies Depression scale (CES-D): “Everything I do feels like an effort” and “I could not get going”19 Frailty is categorized into groups of non-frailty (0), pre-frailty (1–2), frailty (≥3).
All evaluators completed standardized protocol training to ensure consistent measurement. They were also blinded to participants’ constipation and frailty status to avoid potential measurement bias.
Statistical Analysis
Statistical analyses were performed using SPSS software, version 27.0.1 (IBM Corporation, Armonk, New York, USA). The normality of continuous variables was assessed using the Kolmogorov–Smirnov test. Normally distributed data (age, body mass index, serum albumin, serum hemoglobin, serum calcium, and serum phosphate) are presented as mean ± standard deviation and were compared using the Student’s t-test. Non-normally distributed data (hemodialysis vintage and C-reactive protein) are expressed as median (interquartile range) and were compared using the Mann–Whitney U-test. Categorical variables are presented as numbers (percentages) and were compared using the chi-square test. A two-tailed p-value < 0.05 was considered statistically significant.
Multivariate binary logistic regression was used to calculate odds ratios (OR) with 95% confidence intervals (CI). The model was adjusted for age, sex, diabetes, polypharmacy, serum albumin, C-reactive protein, and frailty, with the non-frail category serving as the reference. A secondary multivariate binary logistic regression was conducted to examine the associations between constipation and the individual components of the frailty phenotype.
Subgroup analyses were performed to further evaluate the relationship between frailty and constipation. Subgroups were stratified by age (<65 vs ≥65 years), sex, BMI (<22.6 vs ≥22.6 kg/m2), hemodialysis vintage (<38.4 vs ≥38.4 months), and diabetes status.
Results
Characteristics of the Participants
Among the initial 260 patients, 25 were excluded based on exclusion criteria, and 28 did not meet the eligibility criteria, resulting in a final analytical sample of 207 participants according to Figure 1.
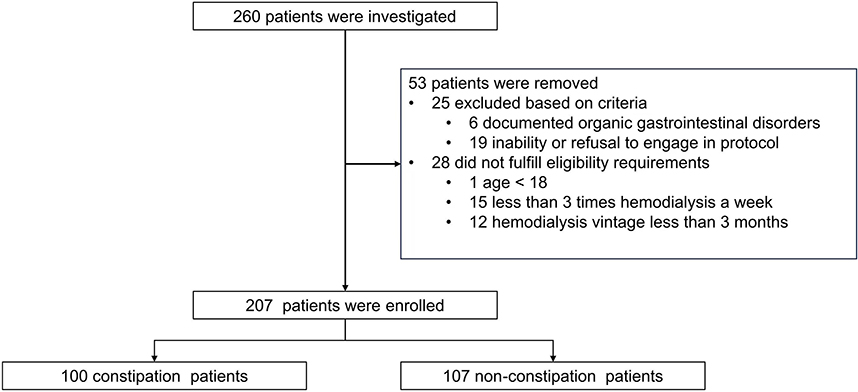 |
Figure 1 Study flow diagram. |
As shown in Table 1, the mean age was 58.6 years, with 37.6% women, a median hemodialysis duration of 38.4 months, a constipation rate of 48.3%, and a frailty rate of 30.4%. The constipation group had older patients, a higher proportion of women, a higher incidence of diabetes, a higher rate of polypharmacy, lower serum albumin levels, and higher C-reactive protein levels compared to the non-constipation group. Furthermore, the constipation group exhibited a higher frailty rate, along with slower gait speed, reduced grip strength, lower physical activity levels, and a greater tendency toward fatigue.
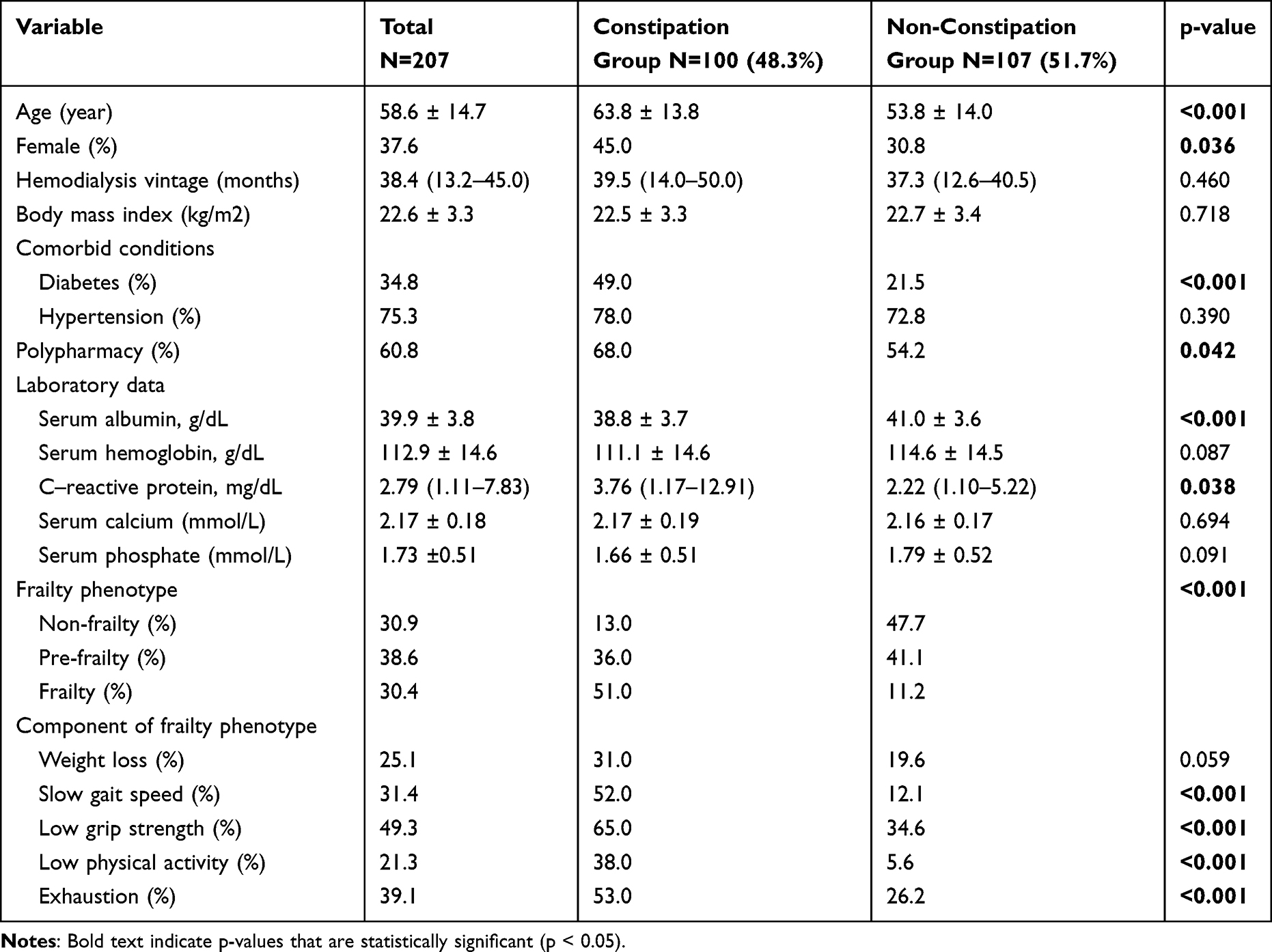 |
Table 1 Characteristics of the Participants |
According to Figure 2, the prevalence of constipation among MHD patients with frailty, pre-frailty, and non-frailty was 80.9%, 45.0%, and 20.3%, respectively. Among patients with constipation, 51.0% were classified as frailty, 36.0% as pre-frailty, and 13.0% as non-frailty. In contrast, non-constipated patients had frailty, pre-frailty, and non-frailty rates of 11.2%, 41.1%, and 47.7%, respectively.
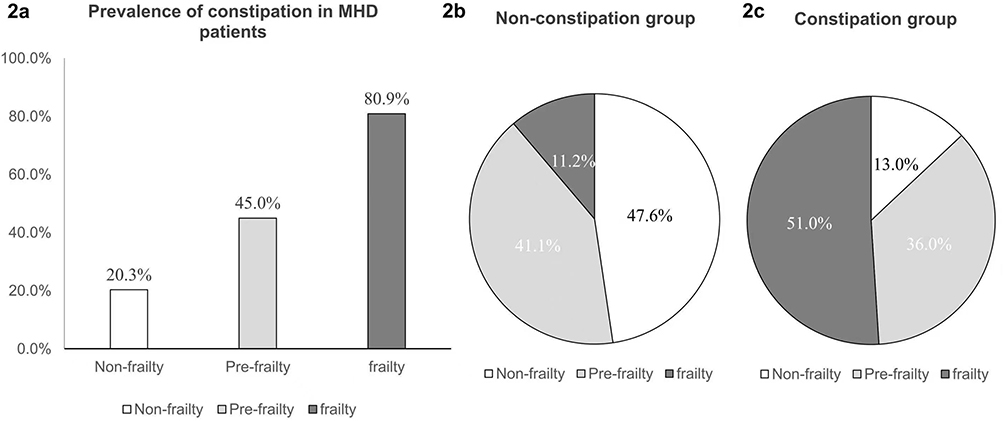 |
Figure 2 Frailty and constipation status in MHD patients. Abbreviations: MHD, maintenance hemodialysis. Notes: (a) Prevalence of constipation in each frailty status; (b) Status of frailty in non-constipation group; (c) Status of frailty in constipation group. |
Association Between Constipation and Frailty
Logistic regression analysis (Table 2) revealed the relationship between constipation and frailty, as well as its association with the five frailty components. After adjusting for age, sex, diabetes, polypharmacy, serum albumin and C-reactive protein levels, constipation remained substantially correlated with frailty (OR: 7.61, 95% CI: 2.74–21.13), while the association with pre-frailty was weaker (OR: 2.43, 95% CI: 1.08–5.48). Among the five frailty components, slow gait speed (OR: 2.90, 95% CI: 1.20–7.00) and low physical activity (OR: 3.51, 95% CI: 1.15–10.74) were independently linked to constipation.
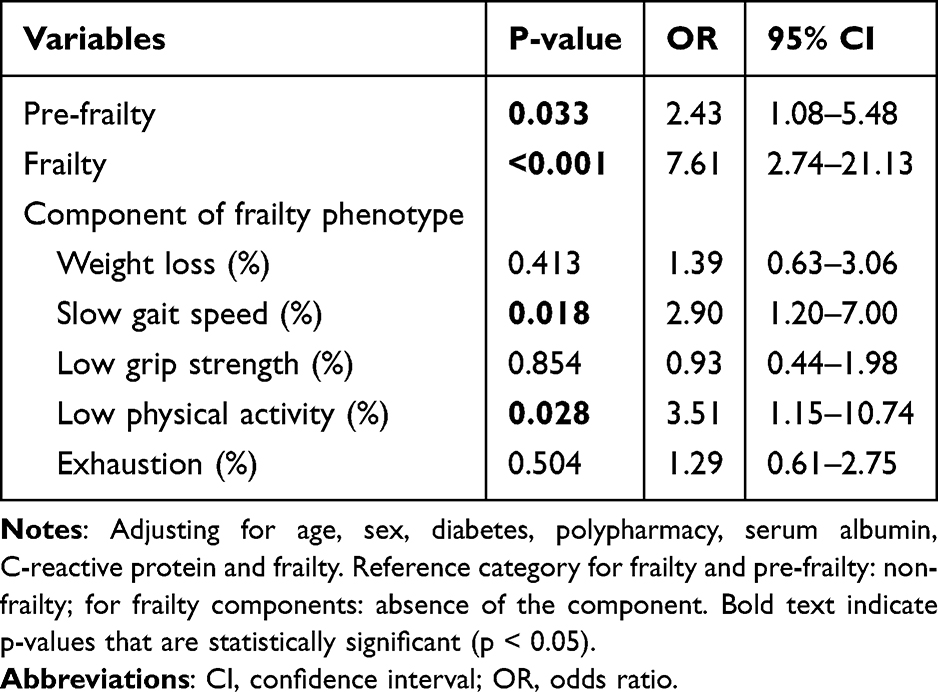 |
Table 2 Association Between Constipation and Frailty with Its Components |
Associations Between Constipation and Frailty: Subgroup Analyses
According to Figure 3, the subgroup analyses showed that in the subgroups age, sex, hemodialysis vintage and diabetes history, frailty is constantly associated with constipation. However, a significant interaction was observed for BMI (interaction p-value = 0.028). Patients with a BMI ≥ 22.6 kg/m2 had a significantly higher odds ratio (OR: 7.174, 95% CI: 3.414–15.075) than those with a BMI < 22.6 kg/m2 (OR: 2.647, 95% CI: 1.515–4.625). This suggests that BMI may be a significant effect modifier in the association between frailty and constipation.
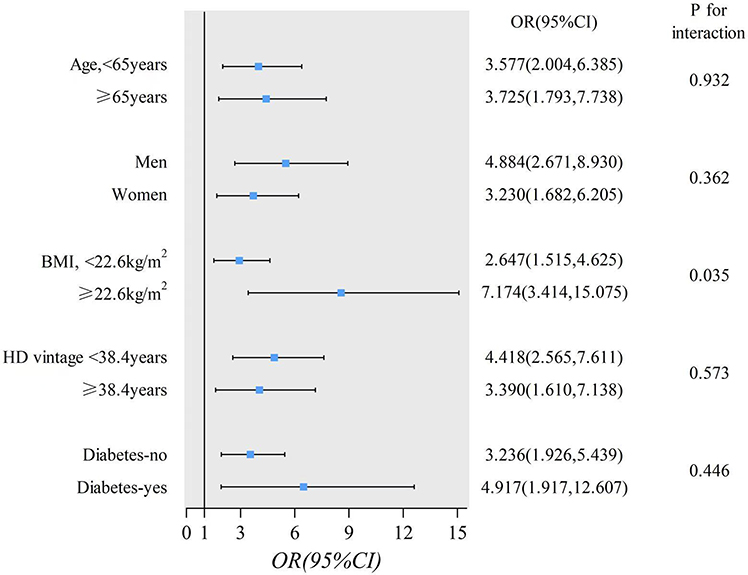 |
Figure 3 Forest plot of odds ratio between constipation and frailty, adjusted for age, sex, BMI, HD vintage and diabetes status. Abbreviations: BMI, body mass index; HD, Hemodialysis; OR, odds ratio; CI, confidence interval. Notes: P for interaction was derived from likelihood ratio tests assessing the interaction between constipation and each subgroup variable. ORs represent the association between constipation and frailty, with reference category: no constipation. |
Discussion
The reported prevalence of constipation among patients undergoing MHD varies considerably across studies, which can likely be attributed to differences in diagnostic criteria and population characteristics.20 The Rome IV criteria, established in 2016 based on extensive clinical research and practical experience, are widely adopted.21 Using these criteria, this study found that 48.3% of MHD patients experienced constipation, a rate substantially higher than the 10.1% reported in the general adult population.22
This study found that constipation was associated with a higher prevalence of frailty after adjusting for relevant patient characteristics. Furthermore, two frailty components—slow gait speed and low physical activity—were independently linked to constipation.
Although data specific to MHD patients remain absent, previous investigations have reported an association between constipation and frailty in older adults. For instance, a cross-sectional study of 1,278 community-dwelling older adults in Korea and an observational epidemiological study of 384 older adults in Spain both identified frailty-constipation correlations.12,14 In addition, a study from Japan involving 102 patients undergoing late Phase II cardiac rehabilitation also revealed a link between constipation and frailty.13 Our study established a significant and independent association between frailty and constipation in MHD patients, a finding that aligned with earlier reports in other populations. However, the unique pathophysiology of MHD—characterized by stringent fluid restrictions and the accumulation of uremic toxins—may amplify the bidirectional relationship between constipation and frailty, making it more pronounced and clinically significant in this vulnerable population than in the general older adults.
Although the specific biochemical link between frailty and constipation remains unclear, several hypotheses can be proposed. First, emerging evidence indicates that frailty is associated with distinct alterations in the gut microbiome.23,24 This frailty-associated dysbiosis may thereby contribute to constipation by slowing intestinal motility and compromising the intestinal barrier.25 Second, prior studies indicate that frailty in MHD patients is associated with polypharmacy.26 These patients frequently require constipation-causing drugs like iron supplements, phosphate binders, potassium-lowering agents, antihypertensives.27 Our research found that patients with constipation used more medications, suggesting that polypharmacy might be a reason behind the relationship between constipation and frailty in MHD patients. Third, our study specifically identified slow gait speed and low physical activity as the frailty components most strongly associated with constipation. Reduced mobility can slow intestinal transit and weaken the muscles involved in defecation, thereby promoting constipation.28,29 Fourth, body composition may act as an effect modifier. Our stratified analysis revealed that the association between constipation and frailty was more pronounced in patients with a higher BMI. This aligns with previous reports linking obesity to an increased risk of constipation,30 suggesting that a higher BMI may exacerbate the underlying pathophysiological processes connecting frailty and constipation.
This study underscores that the management of constipation in MHD patients may require a shift from a sole focus on intestinal symptoms to a more comprehensive strategy that addresses systemic frailty. This approach should integrate proactive frailty screening using tools like the Fried Phenotype for early identification of at-risk patients. Management could include personalized, structured exercise programs—such as intradialytic cycling and resistance training—targeting deficits in gait speed and physical activity. These interventions should be combined with tailored nutritional guidance for weight and fluid management, particularly relevant in individuals with a high BMI, alongside systematic medication reviews to identify and adjust drugs that contribute to constipation. Collectively, this multi-component strategy addresses the systemic nature of frailty to more effectively prevent and alleviate constipation.
To our knowledge, this is the first study to specifically establish a significant and independent association between constipation and frailty in MHD patients. This finding suggests a crucial paradigm shift in clinical understanding, positioning constipation not merely as an isolated gastrointestinal complaint but as a potential indicator of underlying systemic frailty. However, this study has several limitations. First, its cross-sectional design precludes any determination of causality or the dynamic interplay between frailty and constipation. Second, the single-center design and limited sample size may affect the generalizability of the results. Differences across regions and clinical settings may affect the frailty-constipation relationship. Large-scale, multicenter studies are needed to confirm our findings. Third, despite providing standardized, reproducible criteria that enhance comparability across studies, our reliance on the Rome IV questionnaire may introduce subjectivity due to its self-reported nature.
To establish causality and translate these findings into clinical practice, future research should employ longitudinal studies to track the co-evolution of frailty and constipation, complemented by interventional trials testing the efficacy of targeted strategies such as tailored exercise regimens, polypharmacy optimization, and microbiome-targeted therapies.
Conclusion
This study establishes a significant and independent association between constipation and frailty in MHD patients, suggesting a shift from symptomatic to holistic, frailty-centered management. This redefinition opens new avenues for improving patient care and guiding future research.
Funding
This work was supported by the Suzhou Industrial Park Clinical Medical Expert Team Introduction Project (Grant No.: SZYQTD202105) and the Scientific Research Project under the Gusu Health Talent Program of Suzhou (Grant No.: GSWS2022126).
Disclosure
The authors declare that they have no competing interests.
References
1. Sumida K, Yamagata K, Kovesdy CP. Constipation in CKD. Kidney Int Rep. 2020;5(2):121–134. doi:10.1016/j.ekir.2019.11.002
2. Camilleri M, Ford AC, Mawe GM, et al. Chronic constipation. Nat Rev Dis Primers. 2017;3:17095. doi:10.1038/nrdp.2017.95
3. Park SC, Jung J, Kwon YE, et al. Constipation and risk of death and cardiovascular events in patients on hemodialysis. Kidney Res Clin Pract. 2025;44(1):155–163. doi:10.23876/j.krcp.24.174
4. Yasuda G, Shibata K, Takizawa T, et al. Prevalence of constipation in continuous ambulatory peritoneal dialysis patients and comparison with hemodialysis patients. Am J Kidney Dis. 2002;39(6):1292–1299. doi:10.1053/ajkd.2002.33407
5. Zhang L, Tang F, Wang F, et al. The prevalence of constipation in end-stage kidney disease patients: a cross-sectional observation study. Medicine. 2022;101(43):e31552. doi:10.1097/MD.0000000000031552
6. Daniels G, Robinson JR, Walker C, Pennings JS, Anderson ST. Gastrointestinal Symptoms among African Americans Undergoing Hemodialysis. Nephrol Nurs J. 2015;42(6):539–548.
7. Honkura K, Tomata Y, Sugiyama K, et al. Defecation frequency and cardiovascular disease mortality in Japan: the Ohsaki cohort study. Atherosclerosis. 2016;246:251–256. doi:10.1016/j.atherosclerosis.2016.01.007
8. Kim DH, Rockwood K. Frailty in Older Adults. N Engl J Med. 2024;391(6):538–548. doi:10.1056/NEJMra2301292
9. Chan GC, Kalantar-Zadeh K, Ng JK, et al. Frailty in patients on dialysis. Kidney Int. 2024;106(1):35–49. doi:10.1016/j.kint.2024.02.026
10. Cheng M, He M, Ning L, et al. Association between frailty and adverse outcomes in patients undergoing maintenance hemodialysis: a systematic review and meta-analysis. Ren Fail. 2024;46(2):2367716. doi:10.1080/0886022X.2024.2367716
11. Dilek S, Cantekin I. The relationship between frailty levels and quality of life in patients over 65 years of age receiving regular hemodialysis treatment. Psychogeriatrics. 2025;25(1):e13242. doi:10.1111/psyg.13242
12. Lim J, Park H, Lee H, et al. Higher frailty burden in older adults with chronic constipation. BMC Gastroenterol. 2021;21(1):137. doi:10.1186/s12876-021-01684-x
13. Nishitani-Yokoyama M, Shimada K, Yamada M, et al. Association between constipation and frailty components in patients undergoing late phase ii cardiac rehabilitation. Cardiol Res. 2021;12(3):169–176. doi:10.14740/cr1246
14. Arco S, Saldaña E, Serra-Prat M, et al. functional constipation in older adults: prevalence, clinical symptoms and subtypes, association with frailty, and impact on quality of life. Gerontology. 2022;68(4):397–406. doi:10.1159/000517212
15. Hung A, Kim YH, Pavon JM. Deprescribing in older adults with polypharmacy. BMJ. 2024;385:e074892. doi:10.1136/bmj-2023-074892
16. Mearin F, Lacy BE, Chang L, et al. Bowel Disorders. Gastroenterology. 2016;150:1393–1407. doi:10.1053/j.gastro.2016.02.031
17. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–156. doi:10.1093/gerona/56.3.M146
18. Bohm C, Storsley L, Tangri N. The assessment of frailty in older people with chronic kidney disease. Curr Opin Nephrol Hypertens. 2015;24(6):498–504. doi:10.1097/MNH.0000000000000163
19. Yoshikoshi S, Yamamoto S, Suzuki Y, et al. Association between physical frailty and sleep disturbances among patients on hemodialysis: a cross-sectional study. Nephron. 2024;148(3):152–159. doi:10.1159/000533418
20. Zuvela J, Trimingham C, Le Leu R, et al. Gastrointestinal symptoms in patients receiving dialysis: a systematic review. Nephrology. 2018;23(8):718–727. doi:10.1111/nep.13243
21. Drossman DA. Functional gastrointestinal disorders: history, pathophysiology, clinical features and Rome IV. Gastroenterology. 2016;150:1262–1279. doi:10.1053/j.gastro.2016.02.032
22. Barberio B, Judge C, Savarino EV, Ford AC. Global prevalence of functional constipation according to the Rome criteria: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2021;6(8):638–648. doi:10.1016/S2468-1253(21)00111-4
23. Lim MY, Nam YD. Gut microbiome in healthy aging versus those associated with frailty. Gut Microbes. 2023;15(2):2278225. doi:10.1080/19490976.2023.2278225
24. D’Amico F, Barone M, Brigidi P, Turroni S. Gut microbiota in relation to frailty and clinical outcomes. Curr Opin Clin Nutr Metab Care. 2023;26(3):219–225. doi:10.1097/MCO.0000000000000926
25. Yang L, Wang Y, Zhang Y, et al. Gut microbiota: a new avenue to reveal pathological mechanisms of constipation. Appl Microbiol Biotechnol. 2022;106(21):6899–6913. doi:10.1007/s00253-022-12197-2
26. Kimura H, Kalantar-Zadeh K, Rhee CM, Streja E, Sy J. Polypharmacy and frailty among hemodialysis patients. Nephron. 2021;145(6):624–632. doi:10.1159/000516532
27. Cha RR, Park SY, Camilleri M. Constipation in patients with chronic kidney disease. J Neurogastroenterol Motil. 2023;29(4):428–435. doi:10.5056/jnm23133
28. Booth FW, Roberts CK, Laye MJ. Lack of exercise is a major cause of chronic diseases. Compr Physiol. 2012;2(2):1143–1211. doi:10.1002/j.2040-4603.2012.tb00425.x
29. Park H, Lim J, Baek JY, Lee E, Jung HW, Jang IY. Status of constipation and its association with sarcopenia in older adults: a population-based cohort study. Int J Environ Res Public Health. 2021;18(21):11083. doi:10.3390/ijerph182111083
30. Sun X, Zhang S, Zhou X. A causal association between obesity and constipation: a two-sample bidirectional Mendelian randomization study and meta-analysis. Front Nutr. 2024;11:1430280. doi:10.3389/fnut.2024.1430280
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.