Back to Journals » OncoTargets and Therapy » Volume 11
Association between common polymorphisms in ERCC gene and prognosis of osteosarcoma in patients treated with chemotherapy: a meta-analysis
Authors Li C ![]() , Yu X, Guo D
, Yu X, Guo D ![]() , Liu G, Zhang K, Teng Q, Lin H
, Liu G, Zhang K, Teng Q, Lin H
Received 27 November 2017
Accepted for publication 20 April 2018
Published 18 June 2018 Volume 2018:11 Pages 3495—3504
DOI https://doi.org/10.2147/OTT.S158167
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Geoffrey Pietersz
Chunpu Li,1,2,* Xin Yu,1,* Dongmei Guo,3,4 Guanhua Liu,5 Kaigang Zhang,1 Qingliang Teng,3 Hai Lin4
1Department of Orthopedics, Taian City Central Hospital, Taian, China; 2Department of Orthopedics, Qilu Hospital, Shandong University, Jinan, China; 3Department of Hematology, Taian City Central Hospital, Taian, China; 4Department of Animal Science, College of Animal Science and Veterinary Medicine, Shandong Agricultural University, Taian, China; 5Department of Nutrition and Food Hygiene, School of Public Health, Taishan Medical University, Taian, China
*These authors contributed equally to this work
Purpose: Some previous studies have sought to investigate the roles of excision repair cross complementation group 1 (ERCC1), ERCC2, ERCC4, and ERCC5 gene polymorphisms in the prognosis of osteosarcoma patients. However, their results were inconclusive. Here, we performed a meta-analysis to determine the strength of the association between eight polymorphisms in the ERCC genes (rs11615, rs3212986, rs2298881, rs13181, rs1799793, rs1800067, rs2296147, and rs1047768) and prognosis of osteosarcoma patients treated with chemotherapy.
Materials and methods: We retrieved the relevant studies from PubMed, Embase, and Web of Science in human osteosarcoma published prior to July 2017. Primary outcomes included overall survival (OS) and event-free survival, expressed by hazard ratios (HRs) with their corresponding 95% CIs. STATA software (version 12.0) was utilized to perform data synthesis.
Results: A total of 13 eligible follow-up studies involving 2,303 patients met all the inclusion criteria, conducted in two populations of ethnic descent: 11 Asians and two Caucasians. In the present meta-analysis, we demonstrated that the homozygous variant genotypes in ERCC2 rs1799793 and ERCC5 rs2296147 were significantly associated with OS in osteosarcoma (TT vs GG for rs1799793: HR = 0.62, 95% CI = 0.41–0.93, Pheterogeneity = 0.310, I2 = 15.3%, P = 0.020; TT vs CC for rs2296147: HR = 0.42, 95% CI = 0.23–0.78, Pheterogeneity = 0.708, I2 = 0.0%, P = 0.006). In addition, no evidence of association was observed between prognosis in osteosarcoma and ERCC1 rs11615, ERCC1 rs3212986, ERCC1 rs2298881, ERCC2 rs13181, ERCC4 rs1800067, and ERCC5 rs1047768 polymorphisms.
Conclusion: Our meta-analysis indicated that TT genotype in the ERCC2 rs1799793 and ERCC5 rs2296147 might prolong the survival time of patients with osteosarcoma, suggesting that the rs1799793 and rs2296147 polymorphisms can be used as predictors for prognosis of osteosarcoma patients treated with chemotherapy.
Keywords: ERCC2 rs1799793, ERCC5 rs2296147, polymorphisms, osteosarcoma, chemotherapy, prognosis, meta-analysis
Introduction
Osteosarcoma, the most common malignant bone tumor, is a very devastating neoplasm, with an estimated annual incidence of 3–4 per million people.1 Osteosarcoma frequently occurs in children and adolescents, accounting for ~20% of all primary sarcomas in bone tumor.2 The precise mechanism underlying the developing osteosarcoma remains elusive; nonetheless, genetic factors are proposed to be involved in the progression of this cancer.3 Currently, the standard treatment for osteosarcoma includes neoadjuvant therapy prior to definitive resection with wide margin, followed by multiple postoperative chemotherapeutic agents.4 Cisplatin, a platinum analog that can inhibit cell division and growth through interfering with DNA, is one of the favorable agents for the effective combined chemotherapy in osteosarcoma treatment.5,6 However, over 40% of patients develop a poor response to cisplatin-based chemotherapy.7 In addition, the prognosis for overall long-term survival in these patients remains unsatisfactory, with the overall 5-year event-free survival (EFS) of only 65%.8 It is noteworthy that pharmacogenomics has been perceived as a tool for personalized medicine, which can predict the response to chemotherapy as well as clinical outcome of cancer patients.9 Consequently, comprehensive understanding of the role of pharmacogenetics contributes to selecting individualized chemotherapy for patients to improve their survival. Several recent studies have reported that gene polymorphisms, which are included in the excision repair cross complementation group (ERCC), may influence the prognosis for patients with osteosarcoma.
DNA damage is frequently induced by exogenous carcinogens, including ionizing radiation and ultraviolet rays, which can lead to genomic instability.10 DNA repair, playing a critical role in maintaining genetic stability, is composed of several DNA repair pathways that can enable tumor cells to survive the chemotherapy-induced DNA damage.11 Among all these pathways, the nucleotide excision repair (NER) is the most significant mechanism during the DNA repair process, which can recognize DNA damage and remove the damaged nucleotides.12 As shown in previous studies, genetic variants in the DNA repair pathways may impair the DNA repair capacity and affect the prognosis for tumor patients.13–15
Considered as a significant factor of the DNA repair capacity, ERCC is the key element in the NER pathway. In addition, the ERCC genes are of crucial importance for genetic stability, and genetic alterations are predictive of the survival for tumor patients.16–18 Notably, many recent studies have focused on the correlation of polymorphisms in ERCC1 gene (rs11615, rs2298881, and rs3212986), ERCC2 gene (rs13181 and rs1799793), ERCC4 gene (rs1800067), or ERCC5 gene (rs2296147 and rs1047768) with the prognosis for patients with osteosarcoma. However, the results are inconclusive and conflicting, which can be probably attributed to studies with a small sample size or ethnic differences. Herein, an updated meta-analysis of the published studies was conducted so as to comprehensively evaluate the association of ERCC polymorphisms with the clinical outcome in patients with osteosarcoma, hoping to provide helpful evidence and suggestions for future investigation.
Materials and methods
Search strategy
Studies dealing with prognostic implication of ERCC polymorphisms in patients with osteosarcoma were focused on in this meta-analysis. A comprehensive literature search was conducted in PubMed, Embase, and Web of Science up to July 2017. The following terms were used to search for relevant investigations in the abovementioned databases: “osteosarcoma or bone tumor” and “polymorphism or polymorphisms or variant or mutation” and “ERCC* or XPB or XPD or XPF or XPG”, in combination with “outcome or prognosis or survival”. There was no restriction on population, language, time period, or type of study. References from retrieved articles and previous meta-analysis were examined to avoid any omission of eligible studies.
Inclusion and exclusion
We selected related eligible studies according to the strict inclusion criteria as follows:
- Case–control studies (for humans only);
- Detecting the association between ERCC variants and osteosarcoma prognosis or survival;
- Studies had to provide the information to estimate hazard ratios (HRs) and 95% CIs for prognostic effect of osteosarcoma;
- The study with the largest sample size or most recent publication date from all studies with overlapping data published by the same investigators was chosen.
Our exclusion criteria were as follows:
- Studies with overlapping or incomplete data;
- Literature types such as communications, letters, and reviews.
Data extraction
The following data from each eligible study were collected independently by two investigators: first author’s name, year of publication, ethnicity of patients, sample size, chemotherapy drugs, clinical outcomes, and genotype distribution in cases and controls. In addition, HRs for overall survival (OS) and EFS, and their 95% CIs were extracted for statistical analysis. The corresponding author was contacted for detailed data by email. Disagreements were resolved by discussion with the third investigator.
Quality assessment
The quality of each study was assessed with the Newcastle-Ottawa Scale (NOS) for nonrandomized studies, independently by two investigators. The NOS consists of three parameters: case and control selection, comparability, and exposure. Studies with NOS scores >6 were classified as high quality.19
Statistical analysis
To estimate the relationship between ERCC polymorphisms and the survival in osteosarcoma patients, summary Cox proportional HRs with corresponding 95% CIs were utilized to evaluate EFS and OS by published methods.20 Between-study statistical heterogeneity was assessed using the χ2 test-based Q statistic and the inconsistency index I2.21 According to the Cochrane review guidelines, a fixed-effects model was used in the absence of heterogeneity (P > 0.05 or I2 < 50%), while a random-effects model was applied in existence of severe heterogeneity (P < 0.05 or I2 > 50%). The potential publication bias was tested by Begg’s funnel plot and Egger’s linear regression test; P < 0.05 was deemed as a significantly selective bias.22 STATA software (version 12.0; Stata-Corp, College Station, TX, USA) was utilized to deal with all meta-analyses.
Results
Eligible studies
According to our search strategy we retrieved 24 studies from PubMed, 26 from Embase, and 22 from the Web of Science. Then 45 duplicated articles were removed, leaving 27 studies for further evaluation. The full text of the remainder of the studies was estimated for eligibility in accordance with our inclusion and exclusion criteria. Fourteen articles were excluded: five articles were about other tumors, two articles were reviews, two articles were letters, and eligible data for the meta-analysis were absent in five articles. Finally, a total of 13 studies including 2,303 patients were identified to be eligible for this meta-analysis.23–35 The flowchart of literature selection process and reasons for exclusion are shown in Figure 1.
 | Figure 1 Flowchart of the selection procedure of the studies and reasons for exclusion. |
Clinical characteristics of studies
The main clinical characteristics of all eligible studies associated with the prognosis of osteosarcoma are summarized in Table 1. Among these 13 enrolled studies, two studies were performed in Caucasian populations, while the remainder were based on Asian populations. All studies enrolled patients treated with chemotherapy. Of those, 12 articles focus on the relationship with OS, and three on relationship with EFS. This meta-analysis assessed the variant effect using a homozygous model.
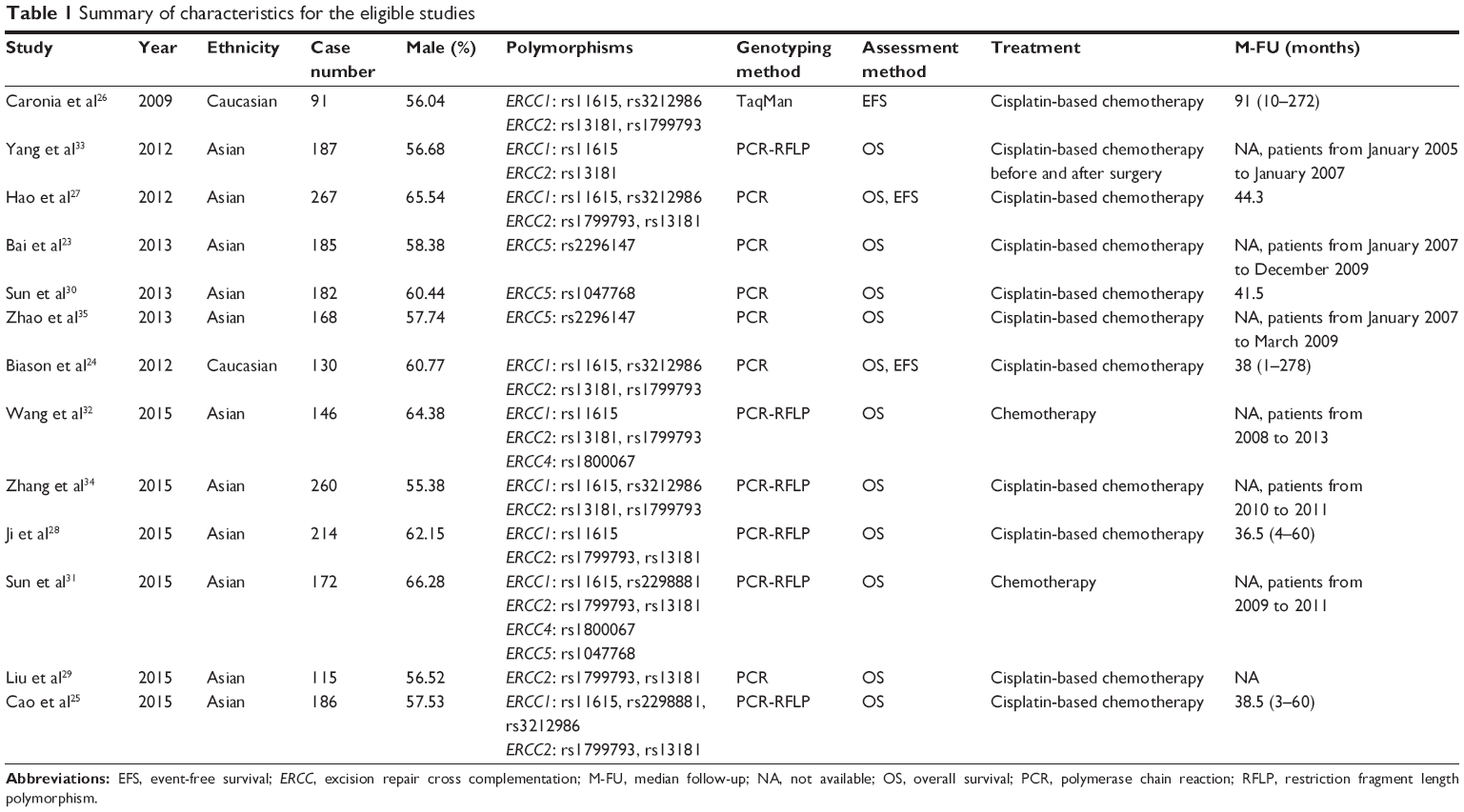 | Table 1 Summary of characteristics for the eligible studies |
ERCC polymorphisms and OS
ERCC1 polymorphisms
Eight studies including 1,562 patients were incorporated to evaluate the association of OS with the ERCC1 polymorphisms in rs11615, rs2298881, and rs3212986. In total, no statistically significant association was found (rs11615: HR = 1.23, 95% CI = 0.65–2.32, Pheterogeneity = 0.002, I2 = 68.3%; rs2298881: HR = 0.77, 95% CI = 0.11–5.39, Pheterogeneity = 0.012, I2 = 84.2%; rs3212986: HR = 0.90, 95% CI = 0.54–1.50, Pheterogeneity = 0.420, I2 = 0.0%). Furthermore, results from stratified analysis by ethnicity indicated that rs11615 and rs3212986 may have no association with OS in both Asians and Caucasians (Table 2).
 | Table 2 Meta-analysis of ERCC polymorphisms with overall survival in osteosarcoma |
ERCC2 polymorphisms
Nine eligible studies consisting of 1,677 patients were included in this evaluation. The rs13181 polymorphism was not significantly associated with OS (HR = 1.07, 95% CI = 0.70–1.65, Pheterogeneity = 0.376, I2 = 7.1%). Stratified analysis by ethnicity also showed no correlation in both Asians and Caucasians (Table 2). However, positive results were found between rs1799793 and OS (TT vs GG: HR = 0.62, 95% CI = 0.41–0.93, Pheterogeneity = 0.310, I2 = 15.3%, P = 0.020), which indicated that patients with TT genotype showed a better survival as compared to GG (Figure 2). Stratified analysis showed that the significance remained in Asians, but not in Caucasians (Asians: HR = 0.63, 95% CI = 0.41–0.96, Pheterogeneity = 0.228, I2 = 26.3%; Caucasians: HR = 0.48; 95% CI = 0.11–2.05) (Table 2).
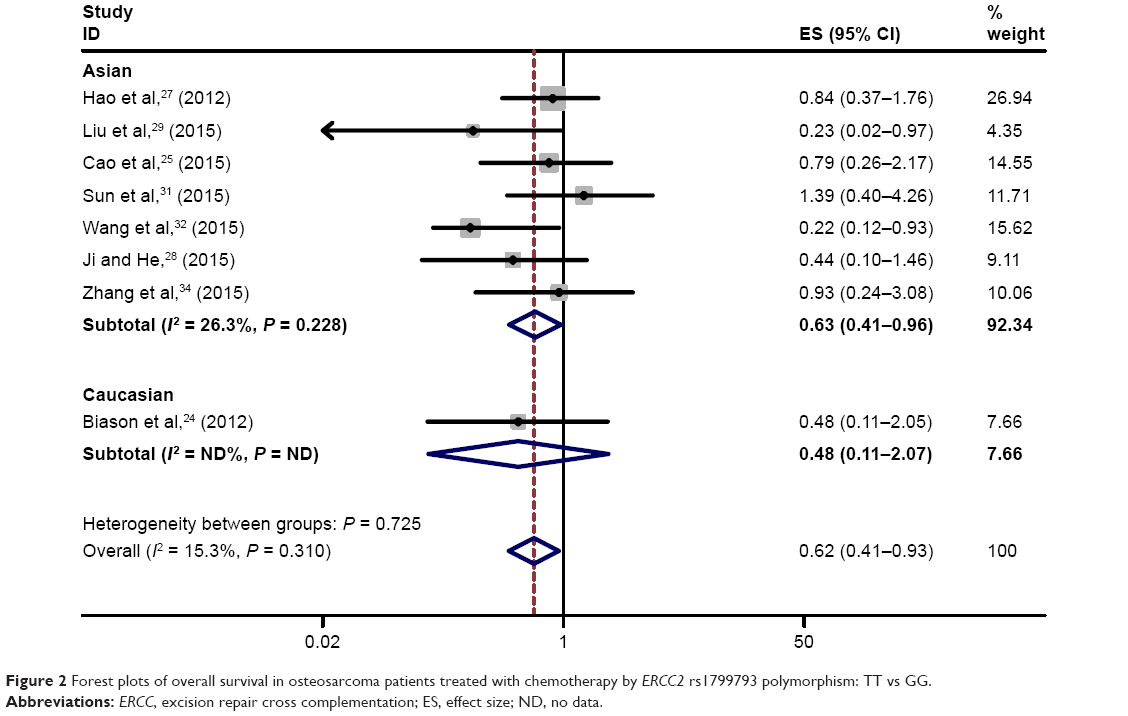 | Figure 2 Forest plots of overall survival in osteosarcoma patients treated with chemotherapy by ERCC2 rs1799793 polymorphism: TT vs GG. |
ERCC4 polymorphisms
Two studies with 318 Asian patients were included in this meta-analysis. There was no evidence to support an association between the ERCC4 rs1800067 polymorphism and OS (HR = 0.56, 95% CI = 0.13–2.39, Pheterogeneity = 0.510, I2 = 0.0%; Table 2).
ERCC5 polymorphisms
Four studies including 707 Asian patients with osteosarcoma were included in the final analysis to reveal the association of OS with the ERCC5 polymorphisms in rs1047768 and rs2296147 (Table 2). The pooled outcome indicated that the rs1047768 polymorphism was not associated with OS in all patients (HR = 0.55, 95% CI = 0.23–1.29, Pheterogeneity = 0.335, I2 = 0.0%). Nevertheless, pooling of data from the rs2296147 polymorphism showed a trend toward an increase in survival of disease with HR of 0.42 (TT vs CC: 95% CI = 0.23–0.78, Pheterogeneity = 0.708, I2 = 0.0%, P = 0.006; Figure 3). The result indicated that patients with rs2296147 TT genotype showed a better survival as compared to CC.
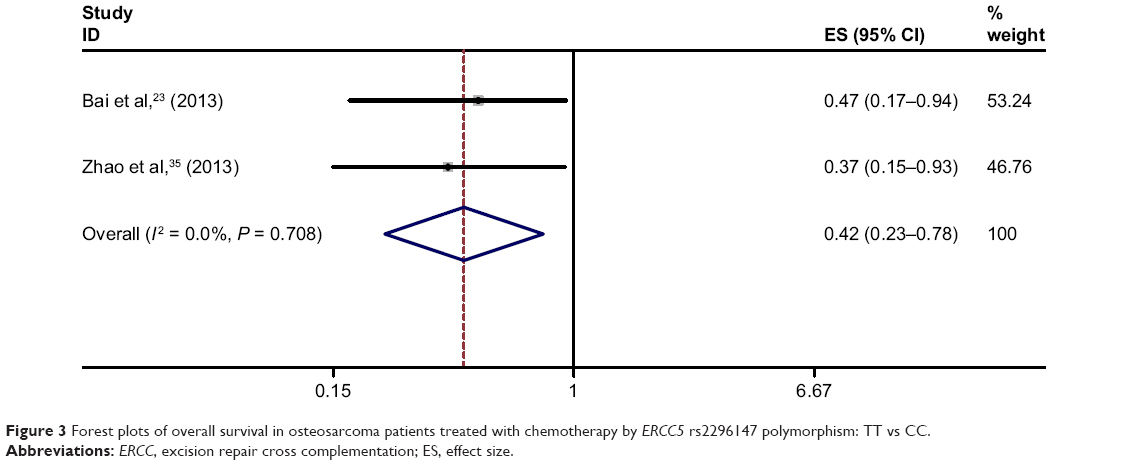 | Figure 3 Forest plots of overall survival in osteosarcoma patients treated with chemotherapy by ERCC5 rs2296147 polymorphism: TT vs CC. |
ERCC polymorphisms and EFS
ERCC1 polymorphisms
Three studies with 488 patients investigating possible associations between the ERCC1 rs11615 polymorphism and EFS were included in the final analysis, one of which included Asians. Overall, there was no statistically significant association in all patients (HR = 0.61, 95% CI = 0.37–1.02, Pheterogeneity = 0.280, I2 = 21.4%). Nevertheless, subgroup analysis by ethnicity showed a positive result in Asian patients (HR = 0.39, 95% CI = 0.14–0.95). These studies also investigated the relationship of the ERCC1 rs3212986 polymorphism and EFS, two of which included Caucasians. In total, no significant correlation was found (HR = 1.04, 95% CI = 0.61–1.75, Pheterogeneity = 0.149, I2 = 47.5%). The ethnic subgroup analysis also demonstrated no association in Asians or Caucasians (Asians: HR = 0.65, 95% CI = 0.43–1.76; Caucasians: HR = 1.86, 95% CI = 0.84–4.09, Pheterogeneity = 0.872, I2 = 0.0%). The results can be found in Table 3.
 | Table 3 Meta-analysis of ERCC polymorphisms with event-free survival in osteosarcoma |
ERCC2 polymorphisms
Three eligible studies of 488 patients were included in the final analysis to investigate the correlation of the ERCC2 rs13181 polymorphism and EFS. Overall, negative results were found in all patients (HR = 1.97, 95% CI = 0.49–8.03, Pheterogeneity = 0.025, I2 = 72.9%). In the subgroup analysis by ethnicity, the results were not significant in Asians or Caucasians (Asians: HR = 2.27, 95% CI = 0.77–6.70; Caucasians: HR = 2.01, 95% CI = 0.15–27.70, Pheterogeneity = 0.010, I2 = 85.1%). These studies were also eligible for the final analysis of association between the ERCC2 rs1799793 polymorphism and EFS. Pooling of data did not show positive results (HR = 0.91, 95% CI = 0.23–3.65, Pheterogeneity = 0.025, I2 = 72.9%). Furthermore, stratified analysis showed negative results in Asian and Caucasian populations (Asians: HR = 0.82, 95% CI = 0.30–1.85; Caucasians: HR = 0.95, 95% CI = 0.06–14.97, Pheterogeneity = 0.007, I2 = 86.3%). Table 3 gives a summary of the results.
Publication bias
Publication bias was assessed in the evaluation of the relationship between ERCC polymorphisms and survival of osteosarcoma by the homozygous model. The shapes of funnel plots showed no evidence of obvious asymmetry (Figure 4). Moreover, the results of Begg’s and Egger’s test confirmed this finding (ERCC1 rs11615: PBegg = 0.71, PEgger = 0.78; ERCC2 rs13181: PBegg = 0.12, PEgger = 0.06; ERCC2 rs1799793: PBegg = 0.39, PEgger = 0.46). For the other ERCC polymorphisms, we did not assess publication bias due to the comparatively smaller number of articles used in the analysis.
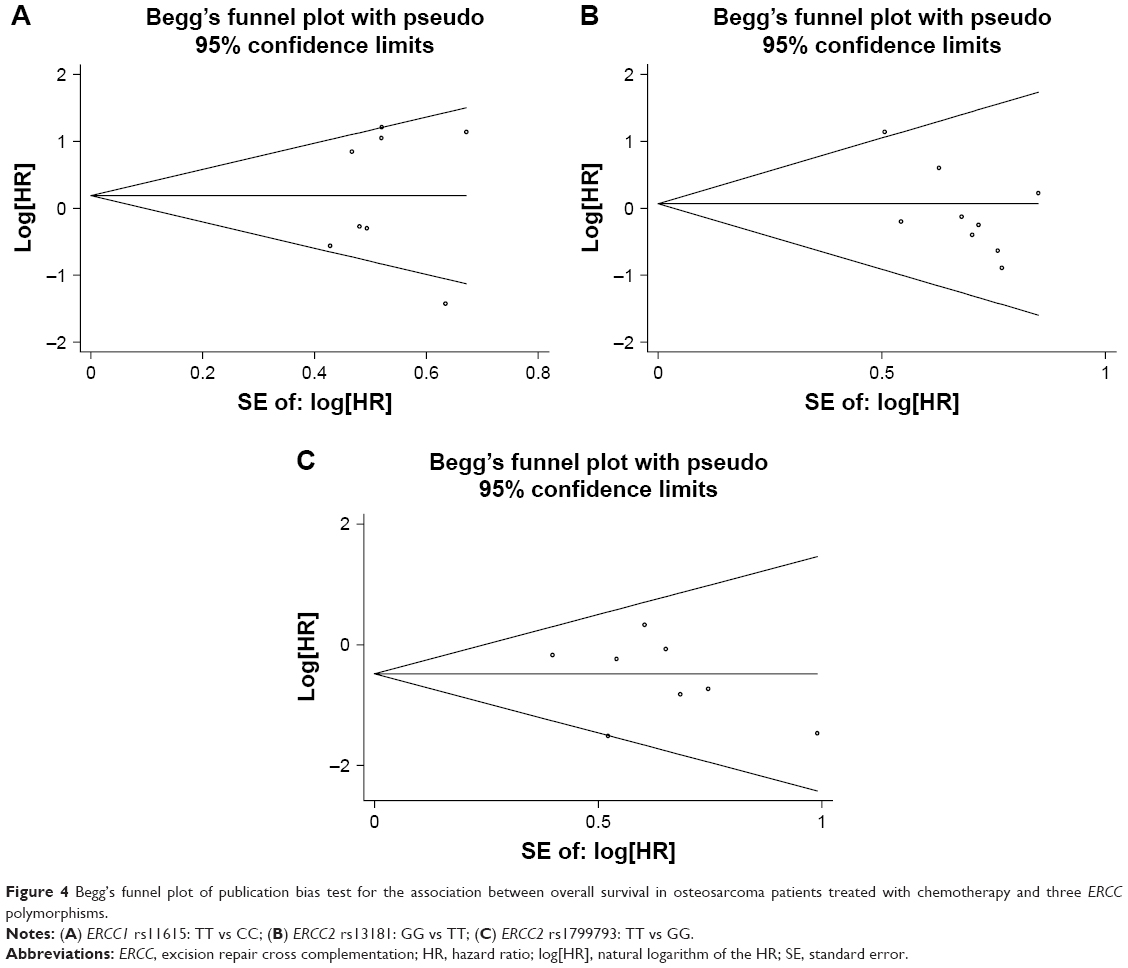 | Figure 4 Begg’s funnel plot of publication bias test for the association between overall survival in osteosarcoma patients treated with chemotherapy and three ERCC polymorphisms. |
Discussion
DNA repair, which is critical to maintain genetic stability, used at least four major pathways, including base excision repair, mismatch repair, NER, and double-strand break repair.36 Among them, NER is the major pathway used by mammals to remove the bulky DNA lesions, which may also prevent the accumulation of DNA damage-induced mutation in humans.37 ERCC1, ERCC2, ERCC4, and ERCC5 are the important factors involved in NER, based on recent studies. During NER, ERCC1 is located at 19q13.2 and can repair the chemical drug-induced DNA damage.38 Moreover, the ERCC1–xenopsin precursor fragment (XPF) complex is a highly conserved endonuclease, which plays a critical role in a variety of other key repair pathways. In addition, McNeil et al39 revealed that ERCC1–XPF might be a novel therapeutic target to overcome chemoresistance in cancer therapy. ERCC2, which maps at 19q13.3, is composed of 23 exons and spans about 54 kb. Furthermore, mutations in ERCC2 gene can lead to defective DNA repair. Chu et al40 observed that the ERCC2 rs13181 TG/GG could prolong the survival time in the Chinese population with gastric cancer. ERCC4, located on chromosome 16p13.12, is composed of 11 exons and spans ~28.2 kb. Moreover, ERCC4 has previously demonstrated to be a human gene correcting the NER deficiency in somatic cell hybrids of mutant hamster cells. In addition, Vaezi et al41 investigated the association of the ERCC4 expression level with the clinical response to DNA damaging agents in head and neck squamous cell carcinoma. Their results identified four ERCC4 single-nucleotide polymorphisms, which revealed a marginal association with treatment failure. Additionally, ERCC5, the central component of NER, participates in the 5′ incision mediated by the ERCC1 and ERCC4 heterodimer. Moreover, Zhao et al35 reported that the ERCC5 mRNA expression level was related to the cytotoxicity of cisplatin; meanwhile, the ERCC5 polymorphisms were correlated with the response to chemotherapy and prognosis of osteosarcoma. Particularly, in recent studies the efficiency of DNA damage repair systems has been shown to be of critical importance and can result in the individual differences in clinical prognosis for osteosarcoma patients treated with chemotherapy.31,42 Furthermore, many clinical studies published within the past several years have extensively investigated the association of ERCC genetic polymorphisms with the prognosis for osteosarcoma patients. However, no consistent results can be obtained from these studies.
Meta-analysis is a statistical analysis that combines a larger sample size than with any individual studies so the results are more precise and robust than any single study. Therefore, we conducted a meta-analysis to elucidate the association between ERCC polymorphisms and the prognosis for osteosarcoma patients from all relevant published studies. OS and EFS, which are intrinsically correlated but not necessarily consistent with each other, were used as the primary parameters after the extracted data were analyzed. Additionally, Li et al43 demonstrated significant correlation between the polymorphisms in ERCC2 rs13181 and the OS in patients with osteosarcoma through assessing the homozygous models. Notably, our updated analysis with more data exactly indicated that the polymorphisms in ERCC2 rs13181 were not necessarily associated with the OS in all patients (HR = 1.17, 95% CI = 0.74–1.83, Pheterogeneity = 0.438, I2 = 0.0%). In our study, an obvious association was found in ERCC2 rs1799793 and ERCC5 rs2296147 polymorphisms with the OS in osteosarcoma patients, indicating that these polymorphisms may be the important prognostic factors of osteosarcoma, especially in Asian populations. However, no significant association was observed between ERCC2 rs1799793 and EFS upon analysis of only three eligible studies. To date, no data are available to assess the relationship between ERCC5 rs2296147 and EFS. Therefore, more future studies are required to confirm the possible prognostic role of rs1799793 and rs2296147 polymorphisms in osteosarcoma. Taking into account the extracted EFS data from some of the studies, we found that genetic polymorphisms in ERCC1 and ERCC2 were not associated with EFS in all patients. However, positive results can be observed in further stratified analyses by ethnicity, in which only one study involving 267 Asian patients examined the relationship between ERCC1 rs11615 and EFS (HR = 0.39, 95% CI = 0.14–0.95). Therefore, further studies regarding the prognosis for osteosarcoma should be performed to draw more reliable results in the future.
We performed a comprehensive meta-analysis to identify the possible association of ERCC polymorphisms with the clinical outcome of osteosarcoma. However, several limitations should be taken into consideration when interpreting our results. First, a relatively small number of studies, as we mentioned above, were included in this meta-analysis. Secondly, studies involving only Asians and Caucasians were included for analysis. Accordingly, future studies enrolling other ethnicities should be carried out to investigate the possibility of a race-specific association. What is more, unpublished relevant articles were excluded from the current meta-analysis. In addition, all Asian studies were performed in the People’s Republic of China. Pan et al44 conducted a study on the interaction of selective reporting and language biases in human genome epidemiology by targeting gene–disease associations. Their findings indicated that a critical and comprehensive global view was needed for human genome epidemiology. Besides, failure to maintain a global outlook may result in bias in medical-scientific literature. Consequently, it is necessary to study more non-Chinese studies of Asian-descent populations, so as to confirm the obvious association in Asians.
Despite the shortages mentioned above, there are many advantages in our meta-analysis. First of all, to our knowledge, the most comprehensive and updated assessment of this association was presented in the current meta-analysis, with the inclusion of new studies. Secondly, the literature retrieval strategy, which includes manual and computer-assisted retrieval, was rigorous enough to identify all the relevant studies with the most comprehensive data possible at the time. Thirdly, data extraction and analysis criteria of the selected literature were designed rationally. Finally, no publication bias was observed in the models of the polymorphisms in rs11615, rs13181, and rs1799793. Consequently, we drew a stable and reliable conclusion. Previous reports of clinical research show that despite tremendous advances in chemotherapy options and surgical procedures, osteosarcoma generally has a poor prognosis, especially in patients with recurrent disease or metastases. Therefore, it is of significant importance to support more research efforts on basic research and clinical translation about osteosarcoma, so as to meet clinical need.
Conclusion
With a pooled dataset of 2,303 patients treated with chemotherapy, we made a comprehensive assessment of prognosis for osteosarcoma by OS and EFS. We observed that the TT genotype in the ERCC2 rs1799793 and ERCC5 rs2296147 can prolong the survival time, suggesting that the rs1799793 and rs2296147 polymorphisms can be used as predictors for prognosis of osteosarcoma patients treated with chemotherapy, especially in Asian populations. Further high-quality and multicenter studies should be conducted to confirm our findings.
Acknowledgments
The present study was supported by grants from the Shandong Province Medical Science and Technology Development Program (No 2016WS0595 and No 2016WS0599), from the Science and Technology Development Plan Project of Tai’an City (No 2016NS1055, No 2016NS1062, and No 2016NS1052).
Disclosure
The authors report no conflicts of interest in this work.
References
Mirabello L, Troisi RJ, Savage SA. Osteosarcoma incidence and survival rates from 1973 to 2004: data from the Surveillance, Epidemiology, and End Results Program. Cancer. 2009;115(7):1531–1543. | ||
Sulzbacher I, Birner P, Trieb K, Pichlbauer E, Lang S. The expression of bone morphogenetic proteins in osteosarcoma and its relevance as a prognostic parameter. J Clin Pathol. 2002;55(5):381–385. | ||
Fuchs B, Zhang K, Schabel A, Bolander ME, Sarkar G. Identification of twenty-two candidate markers for human osteogenic sarcoma. Gene. 2001;278(1–2):245–252. | ||
Longhi A, Errani C, De Paolis M, Mercuri M, Bacci G. Primary bone osteosarcoma in the pediatric age: state of the art. Cancer Treat Rev. 2006;32(6):423–436. | ||
Marsh S, McLeod H, Dolan E, et al. Platinum pathway. Pharmacogenet Genomics. 2009;19(7):563–564. | ||
Keremu A, Aini A, Maimaitirexiati Y, et al. Overcoming cisplatin resistance in osteosarcoma through the miR-199a-modulated inhibition of HIF-1α. Biosci Rep. Epub 2017 Apr 25. | ||
Miwa S, Takeuchi A, Ikeda H, et al. Prognostic value of histological response to chemotherapy in osteosarcoma patients receiving tumor-bearing frozen autograft. PLoS One. 2013;8(8):e71362. | ||
Goorin AM, Schwartzentruber DJ, Devidas M, et al; Pediatric Oncology Group. Presurgical chemotherapy compared with immediate surgery and adjuvant chemotherapy for nonmetastatic osteosarcoma: pediatric Oncology Group Study POG-8651. J Clin Oncol. 2003;21(8):1574–1580. | ||
D’Antonio C, Milano A, Righini R, et al. Pharmacogenomics in lung cancer chemotherapy: a review of what the oncologist should know. Anticancer Res. 2014;34(10):5241–5250. | ||
Chen Y, Williams V, Filippova M, Filippov V, Duerksen-Hughes P. Viral carcinogenesis: factors inducing DNA damage and virus integration. Cancers (Basel). 2014;6(4):2155–2186. | ||
Woods D, Turchi JJ. Chemotherapy induced DNA damage response: convergence of drugs and pathways. Cancer Biol Ther. 2013;14(5):379–389. | ||
Marteijn JA, Lans H, Vermeulen W, Hoeijmakers JH. Understanding nucleotide excision repair and its roles in cancer and ageing. Nat Rev Mol Cell Biol. 2014;15(7):465–481. | ||
Wang C, Nie H, Li Y, et al. The study of the relation of DNA repair pathway genes SNPs and the sensitivity to radiotherapy and chemotherapy of NSCLC. Sci Rep. 2016;6:26526. | ||
Zhou F, Zhu M, Wang M, et al. Genetic variants of DNA repair genes predict the survival of patients with esophageal squamous cell cancer receiving platinum-based adjuvant chemotherapy. J Transl Med. 2016;14(1):154. | ||
Beheshti F, Hassanian SM, Khazaei M, et al. Genetic variation in the DNA repair pathway as a potential determinant of response to platinum-based chemotherapy in breast cancer. J Cell Physiol. 2018;233(4):2752–2758. | ||
Walsh CS, Ogawa S, Karahashi H, et al. ERCC5 is a novel biomarker of ovarian cancer prognosis. J Clin Oncol. 2008;26(18):2952–2958. | ||
Carpagnano GE, Palladino GP, Gramiccioni C, Foschino BMP, Martinelli D. Exhaled ERCC-1 and ERCC-2 microsatellite alterations in NSCLC patients. Lung Cancer. 2010;68(2):305–307. | ||
Lu ZM, Luo TH, Nie MM, et al. Influence of ERCC1 and ERCC4 polymorphisms on response to prognosis in gastric cancer treated with FOLFOX-based chemotherapy. Tumour Biol. 2014;35(4):2941–2948. | ||
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–605. | ||
Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials. 2007;8:16. | ||
Lau J, Ioannidis JP, Schmid CH. Quantitative synthesis in systematic reviews. Ann Intern Med. 1997;127(9):820–826. | ||
Egger M, Davey SG, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. | ||
Bai SB, Chen HX, Bao YX, Luo X, Zhong JJ. Predictive impact of common variations in DNA repair genes on clinical outcome of osteosarcoma. Asian Pac J Cancer Prev. 2013;14(6):3677–3680. | ||
Biason P, Hattinger CM, Innocenti F, et al. Nucleotide excision repair gene variants and association with survival in osteosarcoma patients treated with neoadjuvant chemotherapy. Pharmacogenomics J. 2012;12(6):476–483. | ||
Cao ZH, Yin HP, Jiang N, Yu B. Association between ERCC1 and ERCC2 gene polymorphisms and chemotherapy response and overall survival in osteosarcoma. Genet Mol Res. 2015;14(3):10145–10151. | ||
Caronia D, Patiño-García A, Milne RL, et al. Common variations in ERCC2 are associated with response to cisplatin chemotherapy and clinical outcome in osteosarcoma patients. Pharmacogenomics J. 2009;9(5):347–353. | ||
Hao T, Feng W, Zhang J, Sun YJ, Wang G. Association of four ERCC1 and ERCC2 SNPs with survival of bone tumour patients. Asian Pac J Cancer Prev. 2012;13(8):3821–3824. | ||
Ji WP, He NB. Investigation on the DNA repaired gene polymorphisms and response to chemotherapy and overall survival of osteosarcoma. Int J Clin Exp Pathol. 2015;8(1):894–899. | ||
Liu ZF, Asila AL, Aikenmu K, Zhao J, Meng QC, Fang R. Influence of ERCC2 gene polymorphisms on the treatment outcome of osteosarcoma. Genet Mol Res. 2015;14(4):12967–12972. | ||
Sun XH, Hou WG, Zhao HX, Zhao YL, Ma C, Liu Y. Single nucleotide polymorphisms in the NER pathway and clinical outcome of patients with bone malignant tumors. Asian Pac J Cancer Prev. 2013;14(3):2049–2052. | ||
Sun Y, Wu Y, Li W, Kong Z, Zou X. Genetic polymorphisms in nucleotide excision repair pathway influences response to chemotherapy and overall survival in osteosarcoma. Int J Clin Exp Pathol. 2015;8(7):7905–7912. | ||
Wang MJ, Zhu Y, Guo XJ, Tian ZZ. Genetic variability of genes involved in DNA repair influence treatment outcome in osteosarcoma. Genet Mol Res. 2015;14(3):11652–11657. | ||
Yang LM, Li XH, Bao CF. Glutathione S-transferase P1 and DNA polymorphisms influence response to chemotherapy and prognosis of bone tumors. Asian Pac J Cancer Prev. 2012;13(11):5883–5886. | ||
Zhang Q, Lv LY, Li BJ, Zhang J, Wei F. Investigation of ERCC1 and ERCC2 gene polymorphisms and response to chemotherapy and overall survival in osteosarcoma. Genet Mol Res. 2015;14(3):11235–11241. | ||
Zhao YL, Yang LB, Geng XL, et al. The association of XPG and MMS19L polymorphisms response to chemotherapy in osteosarcoma. Pak J Med Sci. 2013;29(5):1225–1229. | ||
Bartek J, Lukas J. Mammalian G1- and S-phase checkpoints in response to DNA damage. Curr Opin Cell Biol. 2001;13(6):738–747. | ||
Giglia-Mari G, Zotter A, Vermeulen W. DNA damage response. Cold Spring Harb Perspect Biol. 2011;3(1):a000745. | ||
Qixing M, Gaochao D, Wenjie X, et al. Predictive value of Ercc1 and Xpd polymorphisms for clinical outcomes of patients receiving neoadjuvant therapy: a prisma-compliant meta-analysis. Medicine (Baltimore). 2015;94(39):e1593. | ||
McNeil EM, Astell KR, Ritchie AM, et al. Inhibition of the ERCC1-XPF structure-specific endonuclease to overcome cancer chemoresistance. DNA Repair (Amst). 2015;31:19–28. | ||
Chu H, Gu D, Xu M, et al. A genetic variant in ERCC2 is associated with gastric cancer prognosis in a Chinese population. Mutagenesis. 2013;28(4):441–446. | ||
Vaezi A, Wang X, Buch S, et al. XPF expression correlates with clinical outcome in squamous cell carcinoma of the head and neck. Clin Cancer Res. 2011;17(16):5513–5522. | ||
Fu D, Calvo JA, Samson LD. Balancing repair and tolerance of DNA damage caused by alkylating agents. Nat Rev Cancer. 2012;12(2):104–120. | ||
Li J, Liu S, Wang W, et al. ERCC polymorphisms and prognosis of patients with osteosarcoma. Tumour Biol. 2014;35(10):10129–10136. | ||
Pan Z, Trikalinos TA, Kavvoura FK, Lau J, Ioannidis JP. Local literature bias in genetic epidemiology: an empirical evaluation of the Chinese literature. PLoS Med. 2005;2(12):e334. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.