Back to Journals » Psychology Research and Behavior Management » Volume 16
Association Between Big Five Personality Traits and Hypertension in Saudi Patients: A Case Control Study
Authors Lone A ![]() , Othman Albotuaiba A
, Othman Albotuaiba A
Received 12 April 2023
Accepted for publication 5 August 2023
Published 28 August 2023 Volume 2023:16 Pages 3427—3435
DOI https://doi.org/10.2147/PRBM.S416828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Ayoob Lone,1 Azzam Othman Albotuaiba2
1Department of Clinical Neurosciences, College of Medicine, King Faisal University, AlHasa, 31982, Saudi Arabia; 2College of Medicine, King Faisal University, AlHasa, 31982, Saudi Arabia
Correspondence: Ayoob Lone, Tel +966553039056, Email [email protected]
Background: The association between personality traits and hypertension is complex and has so far not been studied in depth.
Objective: The present study aims to explore the connection between the Big Five personality traits and hypertension.
Methods: This case control study includes 310 participants, and the relationship between personality traits and hypertension was investigated in normotensive and hypertensive patients by the Big Five Inventory-10. We examined the association of each of the Big Five personality traits in hypertensive patients and a control group using binary logistic regression analysis.
Results: The findings of the study revealed that amongst the Big Five personality factors, low conscientiousness (OR: 1.09, 95% CI: 0.92– 1.29, P< 0.005) and high neuroticism (OR: 0.54, 95% CI: 0.45– 0.66, P< 0.001) were related with high risk of hypertension. Male, older people, and physically inactive individuals have been found to be at a higher risk of hypertension. No significant relationship was found between hypertension and marital status, education, or smoking habits.
Conclusion: These results suggested that a low score in conscientiousness trait and a high neuroticism score may be an additional risk factor of hypertension. Thus, it may be worthy to investigate further in order to identify patients at risk and develop a more individual treatment strategy. Cognitive behavioral therapy and pharmacological options can be used preemptively in high-risk patients.
Keywords: Big Five personality, hypertension, conscientiousness, neuroticism
Corrigendum for this paper has been published.
Introduction
Hypertension is a well-known risk factor for cardiovascular disease, and it has been considered as a global disease burden and public health concern.1 Among the various risk factors identified for development of cardiovascular disease, psychosocial determinants have been found to play an important role in the manifestation and outcome of cardiac illness/disease.2,3 In addition, among the many psychological and social factors, an individual’s personality characteristics or traits have been investigated as a significant factor influencing the morbidity of cardiovascular disease. Personality traits are defined as behavioral and psychological tendencies that endure over time and across different contexts.4 The primary indicator of personality functioning is the Big Five personality traits which explains personality into five broad traits: Agreeableness, Extraversion, Conscientiousness, Neuroticism, and Openness to experience. In brief, agreeableness refers to the degree to which a person requires cordial relationship with others. Extraversion is the tendency to be outgoing, active, assertive, and to have positive emotions. Conscientiousness is characterized by the propensity for self-control, task and goal orientation, planning, and rule following. Neuroticism is the tendency to experience negative emotions such as sadness and anxiety, as well as mood swings. Finally, openness to experience refers to originality, complexity, creativity, and receptivity to new ideas.5,6
Multiple pathways exist by which personality may affect health, but the exact mechanisms of these pathways are still unclear.7 Certain personality traits, particularly conscientiousness, may enhance health because those who exhibit high conscientiousness are more likely to engage in healthy behaviors.8,9 Other personality traits, such as extraversion, neuroticism, and agreeableness, may have an impact on individuals' emotional and social lives, including susceptibility to negative experiences,10 poor social support,11 and less ability to adapt to difficult and changing life circumstances.12 As a result, psychosocial stress may increase risk of atherosclerosis, high blood pressure, and other physiological risk factors13,14 and then lead to aggravated risk of cardiovascular mortality.15 There may also be additional personality-related pathways.16 It has been found that a person’s temperament and hypertension are related.17 Previous studies reported that hostile people of different age groups are prone to high blood pressure particularly in adulthood.18,19 In a study of Finnish males, it was found that a threefold increase in the incidence of hypertension was associated with high levels of hopelessness.20 The development of hypertension in normotensive people over a three-year period has been found to be correlated with high levels of defensiveness.21 Although there is conflicting evidence from various studies, it appears that a tendency toward hostile impulses, antagonism, and denial may be related to elevated blood pressure.22
Personality traits have long been linked with physical activity.23 Previous research on the relationships between personality traits and physical activity confirmed the importance of extraversion, neuroticism, and conscientiousness as correlates of physical activity.24 It was also confirmed in meta-analysis that undertaking physical activity was linked with higher conscientiousness, openness, and extraversion, and lower neuroticism.25 Recent research found that moderate exercise is negatively associated with agreeableness and sensitivity to anxiety.26 Personality traits also appear to influence smoking. Previous research reported differences in personality characteristics between smokers and non-smokers.27 A meta-analysis of cross-sectional studies of extraversion and neuroticism reported that smokers had higher neuroticism and higher extraversion than non-smokers.28 Another meta-analysis of published cross-sectional studies on health correlates of conscientiousness reported that smoking was more common among individuals with low compared with high conscientiousness.8 In sum, current smokers are characterized by high neuroticism, high extraversion, low agreeableness, and low conscientiousness.
Studies using the Big Five personality traits have found that extraversion and neuroticism scales have been linked with higher risks of cardiovascular disease.29,30 In contrast, it has been asserted that openness to experience and conscientiousness are cardio-protective traits.29,31 Personality may also have interaction with other factors such as sex and socio-economic status that mediate the risk of cardiovascular disease.32,33 For instance, high neuroticism and low socio-economic status may increase the risk of coronary heart disease mortality in women, whereas high neuroticism and high socio-economic status may lower the risk of coronary heart disease.34 Existing literature suggested that low scores in conscientiousness and agreeableness, high score on neuroticism,35 affective temperaments,17 and type D personality36 are associated with hypertension. However, other studies did not find any significant relationship between personality factors and hypertension.37–39 Although many researchers have explored risk factors in cross-sectional research,17 the predicted values of risk and protective factors can only be determined through case control design. Therefore, the aim of this study was to explore the association between Big Five personality traits and patients with hypertension in Eastern Saudi Arabia.
Materials and Methods
Study Design
In this case control study, the participants were recruited from health care centers of AlHasa, eastern part of Saudi Arabia between January and March 2023. These centers are maintaining a household file of each family under their respective catchment area. These health care centers are run by general physicians and nurses. These centers provide out-patient care and refer the patients to higher level of care. This research was conducted in accordance with the Helsinki Declaration and had received ethical approval from the Deanship of Scientific Research, King Faisal University, AlHasa, Saudi Arabia. Informal verbal consent was taken from all the respondents, and this verbal informed consent was acceptable and approved by the Deanship of Scientific Research King Faisal University prior to their participation in the study.
Participants
In the case group, 164 volunteer hypertensive patients were recruited to participate in this research. Inclusive criteria were as follows: diagnosis primary hypertension, aged >18 years old, and verbal informal consent. Hypertensive patients are defined having blood pressure readings equal to or greater than 140/90 mmHg during three different blood pressure measurements in the clinic. Patients who have one or more of the following are excluded: secondary hypertension, and history of psychiatric illness including neurotic disorder (anxiety, obsessive compulsive disorder, post-traumatic stress disorder) and psychotic disorders (bipolar disorder, mania, schizophrenia, dementia). In the control group, 146 normotensive controls were recruited who also fulfilled the inclusion and exclusion criteria.
Demographic data including age, gender, area of residence, educational level, and marital status were collected with the help of a questionnaire. In addition, information about physical activity (exercise >150 min/week or <150 min/week) and smoking status (never smoked, and current smoking) were also recorded. Physical examination including blood pressure, pulse, weight, height, and waist circumferences were recorded by the trained nurse.
Study Sample Calculation
Presently, there is no research examining Big Five personality traits in patients with hypertension in Saudi Arabia, and there were no previous studies that help us to calculate the sample size. The present study was a case control study, and we used a convenience sampling method which was suitable for this study.
Measures: Big Five Personality Traits
Personality was measured using the Arabic version of the Big Five Inventory-10 (BFI-10).40 This scale comprises five dimensions of personality, ie Extraversion (items 1 and 6), Agreeableness (items 2 and 7), Conscientiousness (items 3 and 8), Neuroticism (items 4 and 9), and Openness to experience (items 5 and 10). Each personality dimension is measured by two items, with one item positively keyed and the other negatively keyed. Responses are obtained on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Total score is produced by adding each subscale score together that ranges from 10 to 50. A high score on this scale indicates a higher trait level. In the present study, internal consistency reliability (Cronbach’s alpha) of different subscales of the Big Five Inventory-10 were 0.76 (Extraversion), 0.42 (Agreeableness), 0.78 (Conscientiousness), 0.68 (Neuroticism), and 0.72 (Openness to experience).
Statistical Analysis
After ensuring the data’s quality and consistency, the data were coded and exported to Statistical Package for Social Sciences (IBM SPSS, version 27) for analysis. To gain clear understanding of socio-demographic characteristics of the study participants, frequency, percentage, mean, standard deviation, and other descriptive statistics were calculated. Student's t-test was performed to examine the differences in the means between the hypertensive and normotensive patients for quantitative variables. For categorical variables, Pearson’s chi-square test for independence was conducted. The Big Five personality factors and demographic and clinical features that were observed to be significantly different between the two groups were treated as independent variables to construct a binary logistic regression model in order to assess the predictive value of personality traits for hypertension, where hypertension and normotension serve as dichotomous dependent variables. Hosmer–Lemeshow and R2 were calculated to test the model for goodness of fit. A P-value of 0.05 was considered as statistically significant.
Results
The current study invited 346 participants, and, from these, 164 of 188 (87.23%) hypertensive patients and 146 of 158 (92.40%) normotensive control patients fulfilled the criteria for the study. A total of 310 participants with valid protocol were included in the final analyses. Table 1 presents mean scores and SDs of the two groups of participants for the measures of the Big Five personality traits along with the independent t-test values. For different personality dimensions, significant differences were found for conscientiousness (t=-4.31, P<0.004) and neuroticism (t=11.13, P<0.001). Mean score clearly indicates that participants with hypertension have shown low score in conscientiousness (M=7.12, SD=1.39) in comparison to the participants without hypertension (M=7.26, SD=1.95). However, participants with hypertension reported high score in neuroticism trait of personality (M=8.24, SD=1.64) in comparison to the participants without hypertension (M=6.10, SD=1.79).
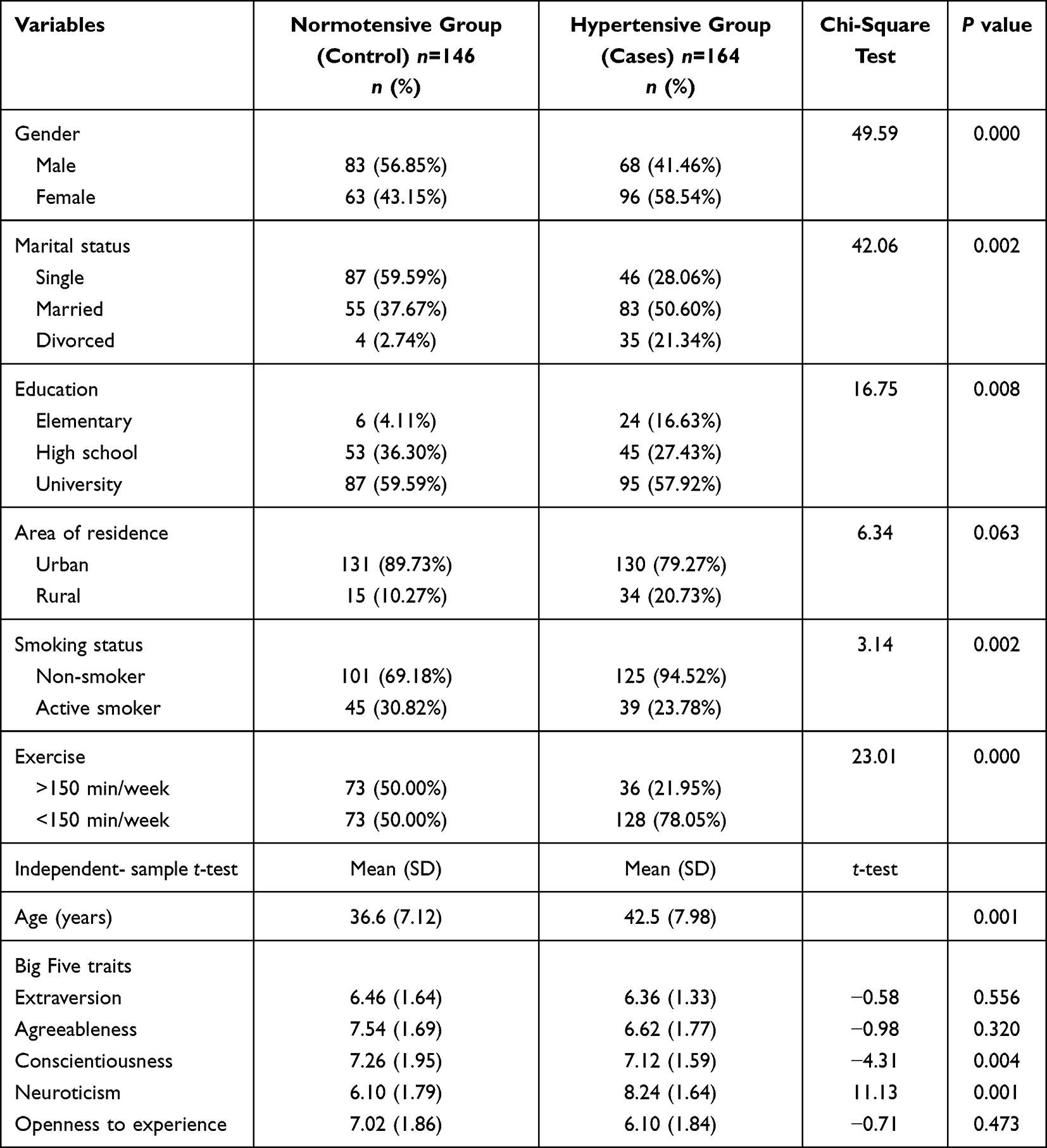 |
Table 1 Sociodemographic and Clinical Features of Participants |
In addition to personality dimensions, demographic and clinical features such as gender, marital status, educational qualification, smoking, physical activity, and age were found to have significant differences between mean scores of normotensive and hypertensive groups. These confounder variables are included together with the Big Five personality factors into a binary logistic regression model as independent variables. The Hosmer–Lemeshow statistic revealed no evidence of poor fit (P=0.089). The predictive values for each of the variables listed above are presented in Table 2.
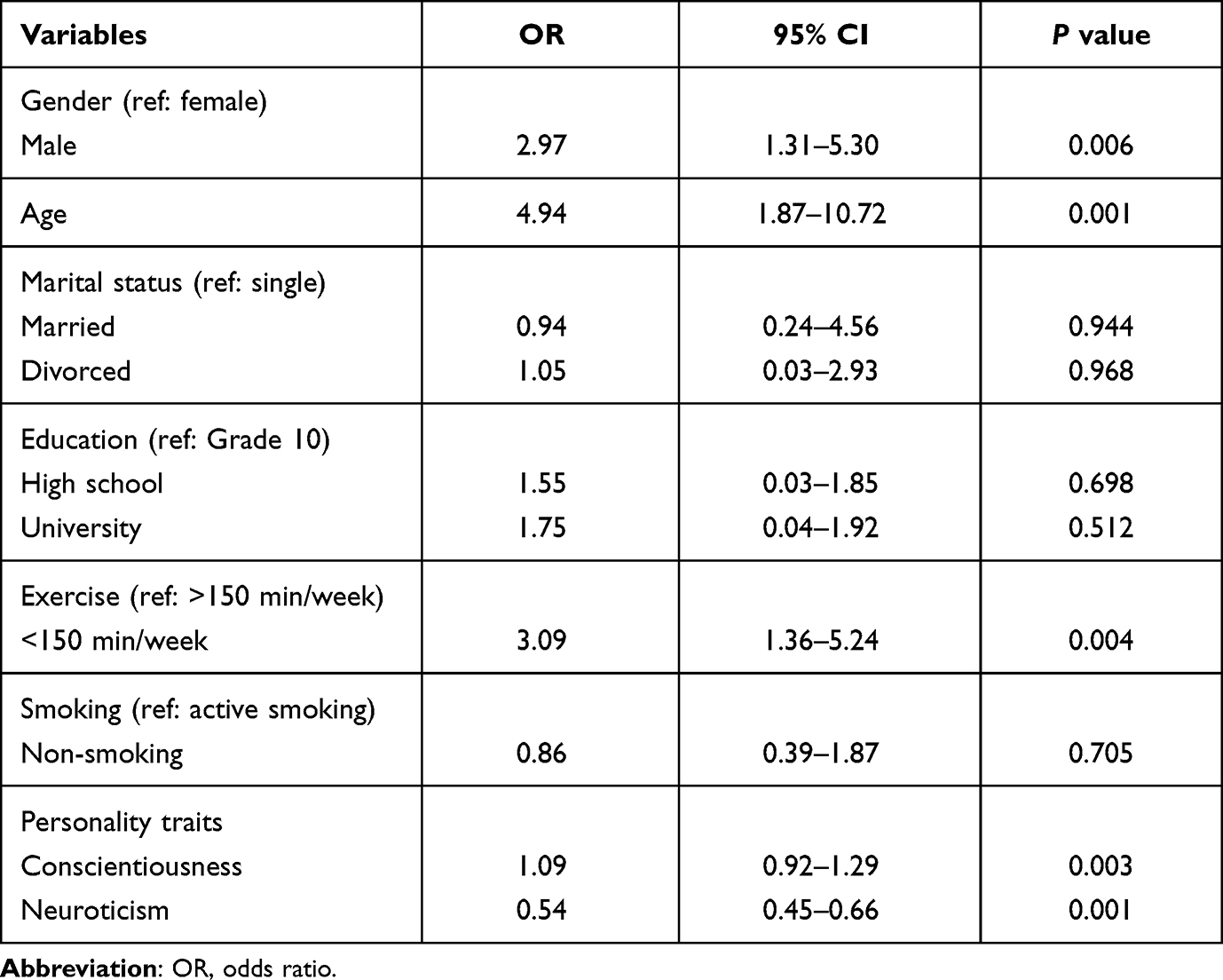 |
Table 2 Result of Binary Logistic Regression Model for Hypertension |
Results of logistic regression analysis presented in Table 2 revealed that gender (OR=2.97; P=0.006), age (OR=4.94; P=0.001), and exercise (OR=3.09; P=0.004) were significantly associated with hypertension. Analysis shows that hypertension was about three times more likely in male patients and approximately five times more likely in older patients. For exercise, participants of the present study were categorized into two groups: those engaging in physical activity for more than 150 min/week, and for less than 150 min/week. Physical activity proved to be a statistically significant predictor, with less active participants being more than three times more likely to be hypertensive in comparison with active participants. However, there was no statistically significant relationship between hypertension and marital status, education, and smoking habits. In the present study it was hypothesized that the Big Five personality dimensions can predict hypertension. Results clearly indicated that conscientiousness and neuroticism were significantly related to hypertension even after adjusting for the important confounders like gender, age, marital status, education, smoking, and physical activity.
Discussion
The current study was conducted to investigate the differences in personality factors between hypertensive and normotensive patients. To our knowledge, this is the first study to examine the association of the Big Five personality traits and hypertension in Saudi Arabia. The results of the study reported a significant relationship between conscientiousness and neuroticism and the development of hypertension. The findings of the study reported that high neuroticism and low conscientiousness trait were the best predictors of hypertension. Direct comparison of this research with past findings exploring the association between personality traits and hypertension was not feasible due to the use of different personality assessment tools and sample characteristics, and studies focused on the relationship between personality dimensions are missing. The current study found that the high neuroticism trait was related to hypertension. This is in line with previous research that individuals who score highly in neuroticism may tend to perceive the world in a negative way. In addition, a person with neuroticism trait, experiencing negative emotions and being overreactive to stress, may have a greater chance to develop hypertension.34,41–43 Previous research reported that negative emotions may have a direct physiologic effect on the development of coronary heart disease by activating the sympathetic nervous system and the hypothalamic-pituitary adrenocortical axis, as well as causing immune dysregulation and inflammation.44–48 Moreover, negative emotions might indirectly influence coronary heart disease by motivating unhealthy behavior. For example, people who experience high levels of anxiety are more likely to smoke and less likely to engage in physical activity.49–51 Both of these factors (biological and behavioral) have a potential to contribute to the development of hypertension and, as a result, the progression of cardiovascular disorders.
The findings of this research suggest that high conscientiousness is linked with lower risk of hypertension. Previous studies offered some clues about the mechanism underlying this trend of relationship.29,50 People with high conscientiousness trait had approximately 40–50% lower cardiovascular-related mortality risk in comparison to people with low conscientiousness.29 Conscientiousness has been linked to a variety of healthy behaviors and outcomes.8,52,53 Conscientiousness proved to be the most important personality trait associated with all-cause mortality,52 diabetes,54 and obesity55 among other health outcomes. Individuals with high conscientiousness are capable of making long-term plans and sticking to them,53 and conscientious people are also more likely to discover and follow health-related information.56 The lower risk of cardiovascular mortality linked to conscientiousness is probably due to these cognitive-behavioral patterns and healthy behaviors.
Additionally, we assessed the relationship of demographic characteristics and hypertension. As a result of this analysis, gender, age, and physical activity were found to be significant predictors of hypertension. Our results indicate that female patients were significantly and substantially less likely to be hypertensive than male patients. Previous studies demonstrated an association between female gender and hypertension.57–60 The observed gender differences in hypertension are caused by both biological and behavioral factors.61–63 The biological factors such as hormones, chromosomal differences, and biological makeup are protective against hypertension in females. These biological factors start to appear in adolescence and continue into adulthood until a woman reaches menopause. High body mass index,64,65 smoking,66,67 and a lack of physical activity64,68 are all behavioral risk factors for hypertension. However, further research is needed to examine other behavioral factors that may explain this disparity.
Regarding age, logistic regression analysis of this study suggested that hypertension occurred more frequently with increasing age which is similar to other studies,69–71 indicating advanced age as an important non-modifiable risk factor for hypertension. The broad consensus is that blood pressure increases with age, although this correlation may be due to a variety of factors such as diet, environmental pollutants, and structural integrity of arteries. Lifestyle factors like physical inactivity were related with higher rates of hypertension in our study. These findings are consistent with earlier studies that examined the association between physical activity and hypertension.72–75 Laboratory investigations and epidemiological researches have reported that more physical activity facilitates post-exercise hypotension, baroreceptor sensitivity, renin angiotensin regulation, endothelial nitric oxide production, and long-term cardiac remodeling.76,77
One of the important strengths of the current study is that the relationship between the Big Five personality factors and hypertension was examined for the first time in Saudi hypertensive patients. The second strength of this study is that the Saudi people are generally eager to participate in studies to advance this growing field in Saudi Arabia. They realize the importance of research and are willing to provide true and unbiased information. This fact has made our data collection journey easier and interesting, and has also increased the likelihood of obtaining valid and reliable data.
Despite the strengths of the present study, there are still some limitations. First, data of the present research were obtained from AlHasa Governorate of Saudi Arabia. Data collected in this region may be unique, and a replication of the study in others parts of the country may yield different outcomes. Second, the sample size of this study was relatively small as we did not find association between some personality traits like agreeableness and extraversion, and hypertension. However, prior findings support the relationship of these personality traits with health.78–81 Nevertheless, this piece of research lays the foundation for longitudinal studies for further evaluation of this association. Third, results of the study would be limited in their generalizability as a convenience sampling technique was used. Finally, the current study focused on participants of Saudi nationality which may make it difficult to generalize the current findings to other nationalities. Further researches should examine populations from other nationalities.
Conclusion
The present study investigated the association between the Big Five personality factors and hypertension. This study found that hypertensive patients had higher neuroticism score and lower conscientiousness score than did normal controls. Several demographic (ie gender, age), physical activity, and personality dimensions were associated with hypertension. However, marital status, education, smoking, and some personality traits such as agreeableness, extraversion, and openness to experience were not found to be significant predictors of hypertension. The current study recommend that health professionals and clinicians should consider sociodemographic factors and personality traits as additional indicators of environmental vulnerability during routine chronic care for high-risk patient screening and improving outcome. A further exploration of these variables may be significant in designing intervention for patients at an early stage of hypertension.
Data Sharing Statement
The data that support our findings can be found through directly asking the corresponding author.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Deanship of Scientific Research King Faisal University, Saudi Arabia (KFU-REC-2022-JAN-ETHICS449).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Author Contributions
All authors made a significant contribution to the work reported whether that is in conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article, gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Deanship of Scientific Research, Vice Presidency for Graduate Studies and Scientific Research, King Faisal University, Saudi Arabia (Grant No. GRANT659).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Liang X, Su S, Hao G, et al. Determinants of pulse wave velocity trajectories from youth to young adulthood: the Georgia Stress and Heart Study. Am J Hypertens. 2019;37(3):563. doi:10.1097/HJH.0000000000001933
2. Everson-Rose SA, Lewis TT. Psychosocial factors and cardiovascular diseases. Annu Rev Public Health. 2005;26(1):469–500. doi:10.1146/annurev.publhealth.26.021304.144542
3. Khayyam-Nekouei Z, Neshatdoost H, Yousefy A, Sadeghi M, Manshaee G. Psychological factors and coronary heart disease. ARYA Atheroscler. 2013;9(1):102–111.
4. Costa PT, McCrae RR. A Five-Factor Model perspective on personality disorders. In: Handbook of Personology and Psychopathology. John Wiley & Sons; 2005:257–270.
5. Costa PT, McCrae RR. Personality in adulthood: a six-year longitudinal study of self-reports and spouse ratings on the NEO Personality Inventory. J Pers Soc Psychol. 1988;54(5):853–863. doi:10.1037/0022-3514.54.5.853
6. McCrae RR, John OP. An introduction to the five‐factor model and its applications. J Pers. 1992;60(2):175–215. doi:10.1111/j.1467-6494.1992.tb00970.x
7. Deary IJ, Weiss A, Batty GD. Intelligence and personality as predictors of illness and death: how researchers in differential psychology and chronic disease epidemiology are collaborating to understand and address health inequalities. Psychol Sci Public Interest. 2010;11(2):53–79. doi:10.1177/1529100610387081
8. Bogg T, Roberts BW. Conscientiousness and health-related behaviors: a meta-analysis of the leading behavioral contributors to mortality. Psychol Bull. 2004;130(6):887–919. doi:10.1037/0033-2909.130.6.887
9. Lodi-Smith J, Jackson J, Bogg T, et al. Mechanisms of health: education and health-related behaviours partially mediate the relationship between conscientiousness and self-reported physical health. Psychol Health. 2010;25(3):305–319. doi:10.1080/08870440902736964
10. Watson D, Clark LA. On traits and temperament: general and specific factors of emotional experience and their relation to the five‐factor model. J Pers. 1992;60(2):441–476. doi:10.1111/j.1467-6494.1992.tb00980.x
11. Connor-Smith JK, Flachsbart C. Relations between personality and coping: a meta-analysis. J Pers Soc Psychol. 2007;93:1080. doi:10.1037/0022-3514.93.6.1080
12. Watson D, Hubbard B. Adaptational style and dispositional structure: coping in the context of the Five‐Factor model. J Pers. 1996;64(4):737–774. doi:10.1111/j.1467-6494.1996.tb00943.x
13. Steptoe A, Kivimäki M. Stress and cardiovascular disease. Nat Rev Cardiol. 2012;9(6):360–370. doi:10.1038/nrcardio.2012.45
14. Steptoe A, Kivimäki M. Stress and cardiovascular disease: an update on current knowledge. Annu Rev Public Health. 2013;34(1):337–354. doi:10.1146/annurev-publhealth-031912-114452
15. Kivimäki M, Nyberg ST, Batty GD, et al. Job strain as a risk factor for coronary heart disease: a collaborative meta-analysis of individual participant data. Lancet. 2012;380(9852):1491–1497. doi:10.1016/S0140-6736(12)60994-5
16. Jonassaint CR, Boyle SH, Williams RB, Mark DB, Siegler IC, Barefoot JC. Facets of openness predict mortality in patients with cardiac disease. Psychosom Med. 2007;69(4):319–322. doi:10.1097/PSY.0b013e318052e27d
17. Eory A, Gonda X, Lang Z, et al. Personality and cardiovascular risk: association between hypertension and affective temperaments—a cross-sectional observational study in primary care settings. Eur J Gen Pract. 2014;20(4):247–252. doi:10.3109/13814788.2013.868431
18. Yan LL, Liu K, Matthews KA, Daviglus ML, Ferguson TF, Kiefe CI. Psychosocial factors and risk of hypertension: the Coronary Artery Risk Development in Young Adults (CARDIA) study. JAMA. 2003;290(16):2138–2148. doi:10.1001/jama.290.16.2138
19. Siegler IC, Peterson BL, Barfoot JC, Williams RB. Hostility during late adolescence predicts coronary risk factors at mid-life. Am J Epidemiol. 1992;136(2):146–154. doi:10.1093/oxfordjournals.aje.a116481
20. Everson SA, Kaplan GA, Goldberg DE, Salonen JT. Hypertension incidence is predicted by high levels of hopelessness in Finnish men. Hypertens. 2000;35(2):561–567. doi:10.1161/01.HYP.35.2.561
21. Rutledge T, Linden W. Defensiveness status predicts 3-year incidence of hypertension. J Hypertens. 2000;18(2):153–159. doi:10.1097/00004872-200018020-00004
22. Leclerc J, Rahn M, Linden W. Does personality predict blood pressure over a 10-year period? Pers. Individ Differ. 2006;40(6):1313–1321. doi:10.1016/j.paid.2005.11.015
23. Karvonen J, Törmäkangas T, Pulkkinen L, Kokko K. Associations of temperament and personality traits with frequency of physical activity in adulthood. J Res Pers. 2020;84:103887. doi:10.1016/j.jrp.2019.103887
24. Wilson KE, Dishman RK. Personality and physical activity: a systematic review and meta-analysis. Pers Individ Differ. 2015;72:230–242. doi:10.1016/j.paid.2014.08.023
25. Sutin AR, Stephan Y, Luchetti M, Artese A, Oshio A, Terracciano A. The five-factor model of personality and physical inactivity: a meta-analysis of 16 samples. J Res Pers. 2016;63:22–28. doi:10.1016/j.jrp.2016.05.001
26. Hearon BA, Harrison TJ. Not the exercise type? Personality traits and anxiety sensitivity as predictors of objectively measured physical activity and sedentary time. J Health Psychol. 2021;26(12):2153–2163. doi:10.1177/1359105320906242
27. Terracciano A, Costa PT. Smoking and the Five Factor Model of personality. Addiction. 2004;99(4):472–481. doi:10.1111/j.1360-0443.2004.00687.x
28. Munafo M, Zetteler JI, Clark TG. Personality and smoking status: a meta-analysis. Nicotine Tobacco Res. 2007;9(3):405–413. doi:10.1080/14622200701188851
29. Jokela M, Pulkki-Råback L, Elovainio M, Kivimäki M. Personality traits as risk factors for stroke and coronary heart disease mortality: pooled analysis of three cohort studies. J Behav Med. 2014;37(5):881–889. doi:10.1007/s10865-013-9548-z
30. Otonari J, Ikezaki H, Furusyo N, Sudo N. Do neuroticism and extraversion personality traits influence disease-specific risk factors for mortality from cancer and cardiovascular disease in a Japanese population? J Psychosom Res. 2021;144:110422. doi:10.1016/j.jpsychores.2021.110422
31. Lee HB, Offidani E, Ziegelstein RC, et al. Five-factor model personality traits as predictors of incident coronary heart disease in the community: a 10.5-year cohort study based on the Baltimore epidemiologic catchment area follow-up study. Psychosomatics. 2014;55(4):352–361. doi:10.1016/j.psym.2013.11.004
32. Ikeda A, Iso H, Kawachi I, Inoue M, Tsugane S. Type A behaviour and risk of coronary heart disease: the JPHC Study. Int J Epidemiol. 2008;37(6):1395–1405. doi:10.1093/ije/dyn124
33. Hagger-Johnson G, Roberts B, Boniface D, et al. Neuroticism and cardiovascular disease mortality: socioeconomic status modifies the risk in women (UK Health and Lifestyle Survey). Psychosom Med. 2012;74(6):596–603. doi:10.1097/PSY.0b013e31825c85ca
34. Turiano NA, Pitzer L, Armour C, Karlamangla A, Ryff CD, Mroczek DK. Personality trait level and change as predictors of health outcomes: findings from a national study of Americans (MIDUS). J Gerontol B Psychol Sci Soc Sci. 2012;67(1):4–12. doi:10.1093/geronb/gbr072
35. Terracciano A, Strait J, Scuteri A, et al. Personality traits and circadian blood pressure patterns: a seven year prospective study. Psychosom Med. 2014;76(3):237–243.
36. Oliva F, Versino E, Gammino L, et al. Type D personality and essential hypertension in primary care: a cross-sectional observational study within a cohort of patients visiting general practitioners. J Nerv Ment Dis. 2016;204(1):43–48. doi:10.1097/NMD.0000000000000421
37. Mommersteeg PM, Herr R, Bosch J, Fischer JE, Loerbroks A. Type D personality and metabolic syndrome in a 7-year prospective occupational cohort. J Psychosom Res. 2011;71(5):357–363. doi:10.1016/j.jpsychores.2011.05.004
38. Ringoir L, Pedersen SS, Widdershoven JW, Pop VJ. Prevalence of psychological distress in elderly hypertension patients in primary care. Neth Heart J. 2014;22(2):71–76. doi:10.1007/s12471-013-0502-z
39. Wiltink J, Beutel ME, Till Y, et al. Prevalence of distress, comorbid conditions and well being in the general population. J Affect Disord. 2011;130(3):429–437. doi:10.1016/j.jad.2010.10.041
40. Tarraf N. Translation within the Psychological Transformation Study Module, TRANSMIT-Project “Transnational Perspectives on Migration and Integration”, at the Humboldt-Universität zu Berlin; 2020. Available from: https://www.gesis.org/fileadmin/upload/SDMwiki/BFI-10/BFI-10_Arabic_Items_Egypt.pdf.
41. Spiro A, Aldwin CM, Ward KD, Mroczek DK. Personality and the incidence of hypertension among older men: longitudinal findings from the Normative Aging Study. Health Psychol. 1995;14(6):563. doi:10.1037/0278-6133.14.6.563
42. Yousfi S, Matthews G, Amelang M, Schmidt-Rathjens C. Personality and disease: correlations of multiple trait scores with various illnesses. J Health Psychol. 2004;9(5):627–647. doi:10.1177/1359105304045339
43. Goodwin RD, Cox BJ, Clara I. Neuroticism and physical disorders among adults in the community: results from the National Comorbidity Survey. J Behav Med. 2006;29(3):229–238. doi:10.1007/s10865-006-9048-5
44. Futterman AD, Kemeny ME, Shapiro D, Fahey JL. Immunological and physiological changes associated with induced positive and negative mood. Psychosom Med. 1994;56(6):499–511. doi:10.1097/00006842-199411000-00005
45. Phillips AC, Carroll D, Burns VE, Drayson M. Neuroticism, cortisol reactivity, and antibody response to vaccination. Psychophysiology. 2005;42(2):232–238. doi:10.1111/j.1469-8986.2005.00281.x
46. Lahey BB. Public health significance of neuroticism. Am Psychol. 2009;64(4):241. doi:10.1037/a0015309
47. Garcia-Banda G, Chellew K, Fornes J, Perez G, Servera M, Evans P. Neuroticism and cortisol: pinning down an expected effect. Int J Psychophysiol. 2014;91(2):132–138. doi:10.1016/j.ijpsycho.2013.12.005
48. Kubzansky LD. Sick at heart: the pathophysiology of negative emotions. Cleve Clin J Med. 2007;74(Suppl_1):67–72. doi:10.3949/ccjm.74.Suppl_1.S67
49. Contrada RJ, Cather C, O’Leary A. Personality and health: dispositions and processes in disease susceptibility and adaptation to illness. In: Handbook of Personality: Theory and Research.
50. Cooper ML, Agocha VB, Sheldon MS. A motivational perspective on risky behaviors: the role of personality and affect regulatory processes. J Pers. 2000;68(1):1059–1088. doi:10.1111/1467-6494.00126
51. Tam HL, Chair SY, Leung ISH, Leung LYL, Chan ASW. US adults practicing healthy lifestyles before and during COVID-19: comparative analysis of national surveys. JMIR Public Health Surveill. 2023;31(9):e45697.
52. Hagger-Johnson G, Sabia S, Nabi H, et al. Low conscientiousness and risk of all-cause, cardiovascular and cancer mortality over 17 years: whitehall II cohort study. J Psychosom Res. 2012;73(1):98–103. doi:10.1016/j.jpsychores.2012.05.007
53. Jokela M, Batty GD, Nyberg ST, et al. Personality and all-cause mortality: individual-participant meta-analysis of 3947 deaths in 76,150 adults. Am J Epidemiol. 2013;178(5):667–675. doi:10.1093/aje/kwt170
54. Martin LR, Friedman HS, Schwartz JE. Personality and mortality risk across the life span: the importance of conscientiousness as a biopsychosocial attribute. Health Psychol. 2007;26(4):428. doi:10.1037/0278-6133.26.4.428
55. Jokela M, Elovainio M, Nyberg ST, et al. Personality and risk of diabetes in adults: pooled analysis of 5 cohort studies. Health Psychol. 2014;33(12):1618. doi:10.1037/hea0000003
56. Jokela M, Hintsanen M, Hakulinen C, et al. Association of personality with the development and persistence of obesity: a meta‐analysis based on individual–participant data. Obes Rev. 2013;14(4):315–323. doi:10.1111/obr.12007
57. Hill PL, Roberts BW. The role of adherence in the relationship between conscientiousness and perceived health. Obes Rev. 2011;30:797.
58. Connelly PJ, Currie G, Delles C. Sex differences in the prevalence, outcomes and management of hypertension. Curr Hypertens Rep. 2022;24(6):185–192. doi:10.1007/s11906-022-01183-8
59. Song JJ, Ma Z, Wang J, Chen LX, Zhong JC. Gender differences in hypertension. J Cardiovasc Transl Res. 2020;13(1):47–54. doi:10.1007/s12265-019-09888-z
60. Santosa A, Zhang Y, Weinehall L, et al. Gender differences and determinants of prevalence, awareness, treatment and control of hypertension among adults in China and Sweden. BMC Public Health. 2020;20(1):1–3. doi:10.1186/s12889-020-09862-4
61. Mohanty P, Patnaik L, Nayak G, Dutta A. Gender difference in prevalence of hypertension among Indians across various age-groups: a report from multiple nationally representative samples. BMC Public Health. 2022;22(1):1524. doi:10.1186/s12889-022-13949-5
62. Sandberg K, Ji H. Sex differences in primary hypertension. Biol Sex Differ. 2012;3:1–21.
63. Vitale C, Fini M, Speziale G, Chierchia S. Gender differences in the cardiovascular effects of sex hormones. Fundam Clin Pharmacol. 2010;24(6):675–685. doi:10.1111/j.1472-8206.2010.00817.x
64. Vitale C, Mendelsohn ME, Rosano GM. Gender differences in the cardiovascular effect of sex hormones. Nat Rev Cardiol. 2009;6(8):532–542. doi:10.1038/nrcardio.2009.105
65. Brown CD, Higgins M, Donato KA, et al. Body mass index and the prevalence of hypertension and dyslipidemia. Obes Res. 2000;8(9):605–619. doi:10.1038/oby.2000.79
66. Hu G, Barengo NC, Tuomilehto J, Lakka TA, Nissinen A, Jousilahti P. Relationship of physical activity and body mass index to the risk of hypertension: a prospective study in Finland. Hypertens. 2004;43(1):25–30. doi:10.1161/01.HYP.0000107400.72456.19
67. Halimi JM, Giraudeau B, Cacès E, Nivet H, Tichet J. The risk of hypertension in men: direct and indirect effects of chronic smoking. J Hypertens. 2002;20(2):187–193. doi:10.1097/00004872-200202000-00007
68. Niskanen L, Laaksonen DE, Nyyssönen K, et al. Inflammation, abdominal obesity, and smoking as predictors of hypertension. Hypertens. 2004;44(6):859–865. doi:10.1161/01.HYP.0000146691.51307.84
69. Haapanen N, Miilunpalo S, Vuori I, Oja P, Pasanen M. Association of leisure time physical activity with the risk of coronary heart disease, hypertension and diabetes in middle-aged men and women. Int J Epidemiol. 1997;26(4):739–747. doi:10.1093/ije/26.4.739
70. Addo J, Smeeth L, Leon DA. Hypertension in sub-saharan Africa: a systematic review. Hypertens. 2007;50(6):1012–1018. doi:10.1161/HYPERTENSIONAHA.107.093336
71. Musinguzi G, Nuwaha F, Ashton N. Prevalence, awareness and control of hypertension in Uganda. PLoS One. 2013;8(4):62236. doi:10.1371/journal.pone.0062236
72. Olack B, Wabwire-Mangen F, Smeeth L, Montgomery JM, Kiwanuka N, Breiman RF. Risk factors of hypertension among adults aged 35–64 years living in an urban slum Nairobi, Kenya. BMC Public Health. 2015;15(1):1–9. doi:10.1186/s12889-015-2610-8
73. Diaz KM, Shimbo D. Physical activity and the prevention of hypertension. Curr Hypertens Rep. 2013;15(6):659–668. doi:10.1007/s11906-013-0386-8
74. Gamage AU, Seneviratne RD. Physical inactivity, and its association with hypertension among employees in the district of Colombo. BMC Public Health. 2021;21(1):1–11. doi:10.1186/s12889-021-12013-y
75. Bairapareddy KC, Kamcheh MM, Itani RJ, et al. Low physical activity levels are linked to early hypertension risk in College-Going Young Adults. Healthcare. 2021;9(10):1258. doi:10.3390/healthcare9101258
76. Hegde SM, Solomon SD. Influence of physical activity on hypertension and cardiac structure and function. Curr Hypertens Rep. 2015;17(10):1–8. doi:10.1007/s11906-015-0588-3
77. Wagenmakers AJ, McAllister RM, Laughlin MH, Wagenmakers AJM. Vascular nitric oxide: effects of physical activity,-importance for health. Essays Biochem. 2006;42:119–131. doi:10.1042/bse0420119
78. Liang X, Hao G, Xiao L, et al. Association between extraversion personality with the blood pressure level in adolescents. Front cardiovasc Med. 2022;9:711474. doi:10.3389/fcvm.2022.711474
79. Kang W. Personality traits predict life satisfaction in Coronary Heart Disease (CHD) patients. J Clin Med. 2022;11(21):6312. doi:10.3390/jcm11216312
80. Lachmann B, Sariyska R, Kannen C, et al. Contributing to overall life satisfaction: personality traits versus life satisfaction variables revisited—is replication impossible? Behav Sci. 2017;8(1):1, 1. doi:10.3390/bs8010001
81. Steel P, Schmidt J, Shultz J. Refining the relationship between personality and subjective well-being. Psychol Bull. 2008;134(1):138–161. doi:10.1037/0033-2909.134.1.138
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Interactive Effect of Stressor Appraisals and Personal Traits on Employees’ Procrastination Behavior: The Conservation of Resources Perspective
Huang Q, Zhang K, Huang Y, Bodla AA, Zou X
Psychology Research and Behavior Management 2023, 16:781-800
Published Date: 14 March 2023
Personality Traits Associated with Treatment Choice with an Explicit Statistical Prediction After an Explanation in a Negative Context: A Study in Patients with Glaucoma
Kodaka F, Noro T, Kishimoto N, Kurosawa M, Itoh Y, Ogawa S, Watanabe T, Kubota M, Hori K, Shigeta M, Nakano T
Clinical Ophthalmology 2023, 17:3685-3691
Published Date: 1 December 2023