")
Back to Journals » Journal of Healthcare Leadership » Volume 7
Assessment of the management factors that influence the development of preventive care in the New South Wales public dental service
Authors Masoe A, Blinkhorn A, Taylor J, Blinkhorn F
Received 29 December 2014
Accepted for publication 8 January 2015
Published 2 March 2015 Volume 2015:7 Pages 1—11
DOI https://doi.org/10.2147/JHL.S80011
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Russell Taichman
Angela V Masoe,1 Anthony S Blinkhorn,2 Jane Taylor,1 Fiona A Blinkhorn1
1Faculty of Health and Medicine, School of Health Sciences, Oral Health, University of Newcastle, Ourimbah, 2Department of Population Oral Health, Faculty of Dentistry, University of Sydney, Sydney, NSW, Australia
Background: Oral diseases, particularly dental caries, remain one of the most common chronic health problems for adolescents, and are a major public health concern. Public dental services in New South Wales, Australia offer free clinical care and preventive advice to all adolescents under 18 years of age, particularly those from disadvantaged backgrounds. This care is provided by dental therapists and oral health therapists (therapists). It is incumbent upon clinical directors (CDs) and health service managers (HSMs) to ensure that the appropriate clinical preventive care is offered by clinicians to all their patients. The aims of this study were to 1) explore CDs’ and HSMs’ perceptions of the factors that could support the delivery of preventive care to adolescents, and to 2) record the strategies they have utilized to help therapists provide preventive care to adolescents.
Subjects and methods: In-depth, semistructured interviews were undertaken with 19 CDs and HSMs from across NSW local health districts. A framework matrix was used to systematically code data and enable key themes to be identified for analysis.
Results: The 19 CDs and HSMs reported that fiscal accountability and meeting performance targets impacted on the levels and types of preventive care provided by therapists. Participants suggested that professional clinical structures for continuous quality improvement should be implemented and monitored, and that an adequate workforce mix and more resources for preventive dental care activities would enhance therapists’ ability to provide appropriate levels of preventive care. CDs and HSMs stated that capitalizing on the strengths of visiting pediatric dental specialists and working with local health district clinical leaders would be a practical way to improve models of preventive oral health care for adolescents.
Conclusion: The main issue raised in this study is that preventive dentistry per se lacks strong support from the central funding agency, and that increasing prevention activities is not a simple task of changing regulations or increasing professional education.
Keywords: public oral health management, clinical leadership, preventive strategies, dental/oral health therapist
Introduction
Despite increased access to water fluoridation, widespread use of fluoride toothpaste, and health-promotion efforts, oral diseases, particularly dental caries and periodontal disease, remain a public health challenge.1–4 The Australian Institute of Health and Welfare’s Australians Health 2014 reported that oral disease is one of the four most expensive preventable chronic diseases, and in most cases these dental diseases are preventable.3 In the state of New South Wales, the Health Centre for Epidemiology and Evidence stated that dental disease was the fourth-most common reason for hospitalization in 2012–2013 for a disease that can be prevented.4 Australian epidemiological studies of 14- to 15-year-olds have reported that 50% of adolescents suffer from dental caries, with increased prevalence among vulnerable and disadvantaged groups.1,2 Dental disease is a gradually progressive disease that causes serious problems to adults, and hence it is important to institute the appropriate preventive oral health care in adolescents to avoid dental health problems in adulthood.5–8
The primary focus of any system of oral health care should focus on the prevention of disease, with particular attention given to the social determinants of health, underpinned by a suite of strategies encompassing the common risk-factor approach.9,10 The public dental service is an integral part of the NSW public health system, and offers free oral health care to children and adolescents according to criteria that prioritize those individuals in most need and at highest risk of disease.11 The NSW Ministry of Health is the purchaser and system administrator of the public dental service, with local health districts (LHDs) responsible for utilizing the funds provided to deliver services to address local needs.11 Public dental services to children and adolescents are mainly provided by dental therapists and oral health therapists (therapists). They have a pivotal role in the prevention of dental caries and periodontal disease, because of their academic qualification and expertise in providing oral health care to children and adolescents. Therapists are well placed to engage and support adolescent patients’ self-efficacy toward good oral health.12–14 A strategic framework for dental health in NSW – Oral Health 2020 – encourages the development of targeted models of care for identified groups that promote patient centric service provision and prevention, and integration with other health care and community groups.11
Brocklehurst et al discussed the growing importance of clinical leadership in dentistry as a key component for the transitioning and development of clinician-led services where local clinicians drive forward a quality agenda with a focus on patient outcomes.15 Therefore, the public dental service should develop interventions to improve patient health outcomes.11 LHD clinical directors (CDs) and health service managers (HSMs) as oral health leaders should translate state public oral health strategies into practical goals that will improve the oral health of people living in their communities.11,16,17
Leadership in organizations is important in influencing workers’ perceptions, response to organizational change, acceptance of health innovations, and scientific informed practice.18 However, there is little information on how public dental service CDs and HSMs provide support to therapists to enable them to embed scientific preventive care into clinical practice, such as the use of fissure sealants, application of topical fluoride, oral hygiene instruction, offering of dietary and smoking-cessation advice, and utilizing motivational interviewing techniques to improve compliance with preventive care guidance.5,19–24 Therefore, this study was undertaken to explore and identify 1) what CDs and HSMs perceive as factors influencing therapists to provide clinical preventive care to their patients, and to 2) record their recommendations supporting mechanisms for therapists to increase their clinical preventive activities.
Subjects and methods
Qualitative in-depth semistructured face-to-face interviews were used to explore the two study aims. Open questions were employed to gain insight into participants’ understanding of real workplace situations and processes.25 CDs and HSMs were recruited by purposive sampling from the 15 NSW LHD rural and metropolitan locations to answer the research questions.25
All NSW LHD oral health CDs (n=13) and all HSMs (level four and five) (n=9) were formally invited by email to participate in the research study. The one-on-one interviews were undertaken at convenient locations for the participants. They were requested to reflect and respond to key open questions that were used to explore 1) influencing factors that could support therapists to offer preventive care, and 2) to identify and record their proposed strategies to enhance therapists’ clinical preventive practices to ensure quality oral health care is provided for their patients.
Consent was obtained from the CDs and HSMs to record the interview to facilitate the note taking and support the data collection and analysis. During the interviews, some participants spontaneously opted to use whiteboards and drawings and provide documentation as evidence to illustrate LHD processes. Although not a grounded-theory research study, this technique is aligned with Glaser and Holton’s dictum that “all is data” relevant to answer the research questions.26
The qualitative data analysis continued after the face-to-face interview sessions, using the thematic analysis inductive approach.27 Systematic steps pertaining to thematic analysis were followed: 1) familiarization with data by synthesizing all data into a framework matrix using Microsoft Excel, 2) creating codes that identified unique features of the data relevant to the research questions, 3) review and further development of themes as dictated by the collected data, 4) comprehensive, inclusive, and thorough examination of the codes to identify patterns of meaning (generating themes), 5) data analyzed and interpreted, and a narrative composed of key themes, and 6) verification of processes by academic principal investigators.27
Ethics approval was obtained from the lead Health and Research Ethics Committee, Hunter New England LHD: HNEHREC12/02//15/5.04 and the 15 LHDs (LHD site-specific assessment ethics approval numbers are available on request).
Results
Of the 15 LHDs, 12 CDs (seven rural and five metropolitan LHDs) participated in the study. Two CDs represented two rural LHDs each (Northern NSW and Mid North Coast, and Southern NSW and Murrumbidgee LHDs), and one LHD (Far West) did not have a CD at the time. The Far West LHD was represented by their HSM. Nine LHD HSMs were invited to join the study, and seven (three metro and four rural) agreed to participate. The main theme that emerged from this study was “Resourcing preventive oral health care for adolescents”; the theme was underpinned by key subthemes shown in Figure 1. Each of the subthemes are presented in more detail.
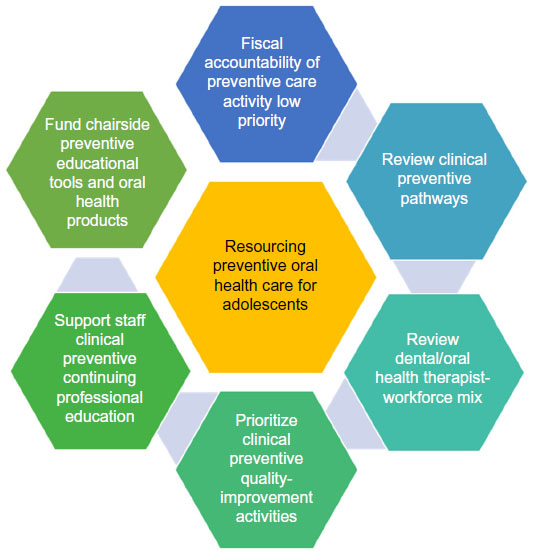 | Figure 1 Resourcing preventive oral health care for adolescents accessing public oral health services in NSW illustrated and reported by clinical directors and health service managers. |
Fiscal accountability and policy
Fiscal accountability and meeting public dental demands according to NSW health policy were reported by participants as a major influencing factor that impacted on the support and provision of preventive care to adolescents.28 Performance agreements between LHDs and the funding agency NSW Ministry of Health are based on activity targets that impact on CD and HSM management decisions and affect the way clinical services are arranged.11 Clinical care, such as extractions and restorations, carry more weight with the funding agency than preventive care, such as fissure sealants, fluoride therapy, oral hygiene instruction, and dietary and smoking-cessation advice:
The bottom line is, invasive treatment such as extractions and restorative treatment have more kudos than preventive treatment such as fissure sealants and remineralising agents. [HSM06]
Although the scientific evidence highlighted the importance of providing preventive care, the respondents were being forced by the system to place greater emphasis on pain relief and restorative care. Conversely, some respondents stated that complaints generated from patients needing preventive care were unknown, compared to the level of complaints received from patients requiring emergency and immediate dental care:
Structuring several preventive appointments a day for therapists is unsustainable. You can’t have appointments to monitor whether patients complied with your oral hygiene instructions, when a mum rings in that her child has been up all night with a raging toothache and there are no appointments available. We can’t afford patient complaints. [CD02]
The Australian government’s benefit scheme Teen Dental Program (TDP) provided a preventive voucher for disadvantaged adolescents whose families were eligible for family tax A, which could be used for private and public dental services.29 Funding from the vouchers enabled some LHDs to provide extra clinical sessions for adolescents, for example, in the evenings or Saturday mornings. Figure 2 depicts the prioritized clinical pathway for eligible TDP adolescents as informed by some LHD respondents. However, with time and streamlining of clinical access to preventive care, these LHDs were able to incorporate the TDP adolescents’ clinical pathway into their general weekly core business, and the extra sessions were not required. Figure 2 illustrates work in progress by these LHDs toward improved prioritized preventive pathways for adolescents. Additionally, Figure 3 illustrates a comprehensive care clinical pathway for patients, incorporating a focus on preventive care as relayed by respondents in some LHDs. Many CDs stated the prescriptive nature of the voucher acted as a catalyst for the majority of therapists to provide preventive care and advice:
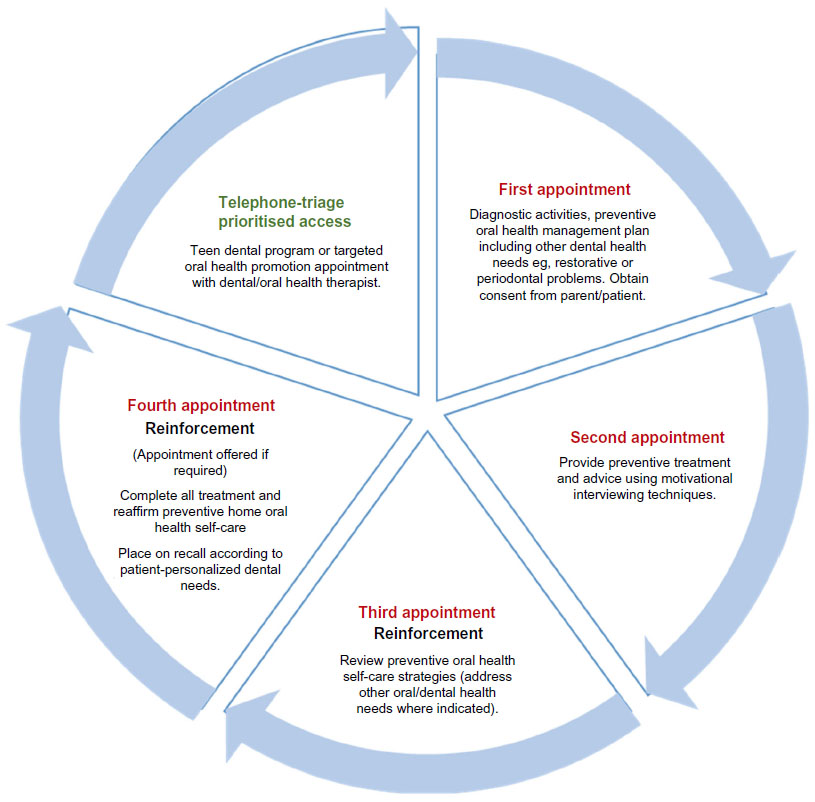 | Figure 2 Adolescents on government benefit scheme and prioritized high-risk groups clinical pathway to preventive care depicted by clinical directors and health service managers in four local health districts. |
 | Figure 3 Comprehensive clinical pathway for adolescents prioritized for relief of pain in some local health districts. |
The implementation of the Teen Dental Program was very positive from the preventive care aspect, as it removed the financial aspect for the patient to access dental care and limitations for patients to return regularly. It’s motivating for therapists, patients, and the service as well in terms of economics. [CD04]
Conversely, most participants reported that often the TDP-eligible adolescents required restorative or invasive treatment at a cost beyond the allocated government funds, and so could not stay with the private sector and returned to seek restorative treatment with the public system, causing longer waiting lists.
Resourcing clinical preventive care pathways
Some participants stated there was a public misconception of “long waiting lists to access public dental care” for adolescents across the LHDs. With a focus on managing waiting lists utilizing the clinical LHD professional team-support structures depicted in Figure 4, regular monitoring of administration processes supported by government benefit scheme funding enabled some LHDs to provide timely preventive care for adolescents (Figures 2 and 3).
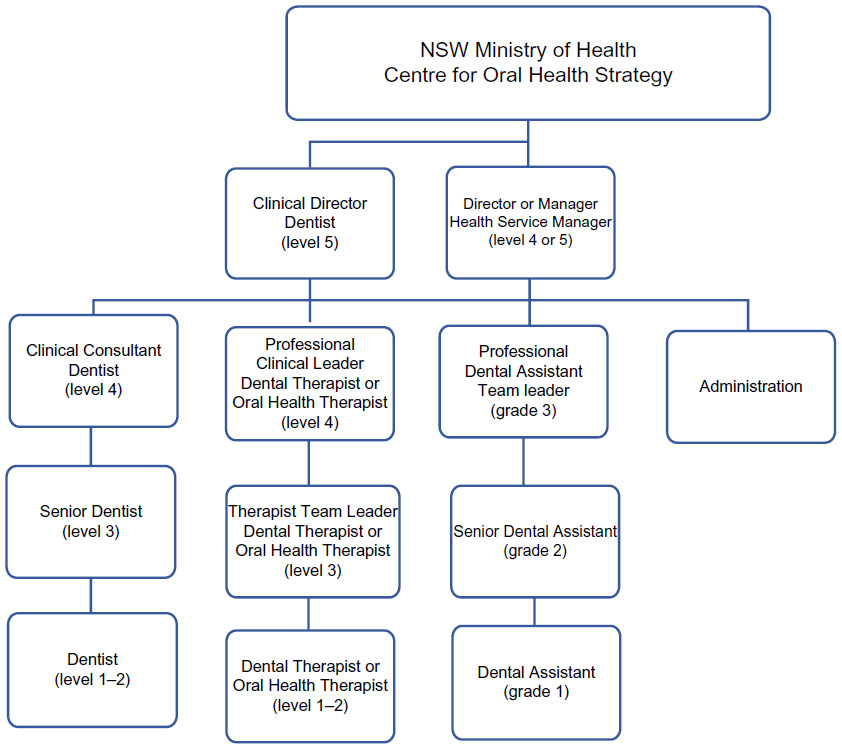 | Figure 4 Professional clinical support structure for therapists, as outlined by clinical directors and health service managers in most local health districts. |
The importance of effective communication between triaging call centers with clearly defined processes for monitoring and measuring clinical activities ensured emergency patients had precedence over patients with less demanding needs. Well-structured appointment-roster systems for relief of pain utilizing all clinicians’ daily “unable to attend”-type appointments were processes that gave therapists leeway to insert preventive care appointments in some LHDs. Several participants argued that adolescent services were markedly different to adult services; therefore, therapists were able to provide full courses of treatment incorporating preventive care.
Our therapists draw up their rosters with the responsibility to structure their day with a balance of emergency and new appointments for the call centre. Follow-up appointments are available for them to manage and complete their patient’s treatment. The electronic appointment system (Information System for Oral Health – ISOH) has a “force booking flexibility” for either parties to meet daily emergency demands. [HSM05]
Whereas others argued to maintain consistency and equity for patient access across LHDs, oral health management mandated structured appointment rosters to support patient access to dental care, with little flexibility for therapists to offer preventive care at specific visits.
Where staffing levels were adequate, some respondents stated therapists were able to provide timely preventive care for all their patients. Figure 3 illustrates some LHDs’ versions of adolescents’ dental care clinical pathways incorporating prevention, with others stating that the current health restructure is an opportunity for clinical quality improvement. Community partnerships whereby therapists collaborated with allied health and primary community health services enabled timely referral of adolescents to preventive care:
Developing partnerships with Aboriginal health professionals, youth agencies, opioid treatment programs and following similar prioritized clinical referral pathways can provide timely preventive care for adolescents. [CD04]
Professional clinical structure
The provision of preventive oral health care to all patients must be informed by scientific evidence and according to NSW health policies – “providing what is right for the individual patient and not what they as a therapist prefer to do” (CDR05) – synthesized the majority of CD viewpoints. In their capacity as primary health care providers, several CDs argued the key role and function of therapists is uniquely focused on preventive care and oral health promotion, which is much needed in the NSW public dental health system. All participants reported therapists were the main advocates and drivers for preventive oral health care activities in their LHD clinical community settings:
Therapists’ rhythm of work is prevention and oral health promotion; it’s their field of expertise. [CDM09]
Figure 4 clarifies the relationships between the different levels of clinical oral health professionals. Organizational operational structures (Figure 4) were similar across the LHDs to support therapists and clinical oral health teams, with most CDs commenting it was work in progress. Therapist clinical leaders (TCLs) shown in the LHD hierarchical structure had a key role to uphold and account for therapists’ clinical preventive and oral health promotion activities. They functioned as advocates for therapists to access appropriate resources. These TCLs, in consultation with staff dentists (and HSMs where applicable), provided clinical support to frontline therapists. A few CDs commented that their pivotal role in providing clinical support to therapists was gradually being recognized, as LHDs moved toward strengthening multidisciplinary structures within clinical settings.
The majority of CDs and HSMs stated that the daily management and communication with therapists was the TCLs’ responsibility. Several CDs reported TCLs obtained clinician preventive data from patient electronic health-activity reports and patient clinical oral health records to conduct peer-review sessions with therapists. They reported that to their knowledge, the lack of clinical preventive care offered by therapists was not highlighted as a major concern.
Resourcing clinical quality-improvement activities
Identifying “interfering factors” that impacted on a therapist’s ability to provide preventive care to adolescents was reported by most participants as raising their awareness of areas for clinical quality improvement.
Giving access to adolescents for timely care was a key barrier to provision of preventive care:
Accessing adolescents, meaning they don’t come in the first place, is a key barrier for therapists to provide preventive care. Most teenagers attend seeking relief of pain, and are given further appointments which may include preventive care, they often fail to attend, some due to prolonged waiting times between appointments. [CD03]
A concern raised by several participants was that the therapists had been conditioned by the public system to systematically “look for holes in teeth” (HSM07). Caries detection followed by focusing on restorative treatment was a clinical practice “norm”. Others stated that therapists often provided ad hoc oral hygiene instruction and dietary advice while performing other clinical tasks:
Therapists often provide oral hygiene instructions whilst providing a restoration or waiting for LA to work. The majority account these activities as preventive care; well, that’s not effective oral hygiene instruction or dietary advice, but I guess it’s better than nothing, as sometimes it’s all kids get in their course of care. [HSM07]
A few CDs argued that a major gap for therapists at the chairside was their level of knowledge and skills to change behavior. New caries-management systems (CMSs) require therapists to understand adolescent psychology, and this requires in-service training to enhance each clinician’s skills to modify adolescents’ behavior:
… it’s about changing behavior, or modify adolescents’ inappropriate diet or oral hygiene behaviors if we are to control dental disease, which is what therapists should be focusing on. [CD09]
A few CDs stated that therapists’ confidence and behavior-management capacity to communicate effectively with adolescents in the health context and manage assertive parents and special needs adolescents were impediments that impacted on therapists’ stress levels, motivation to work, and ability to provide appropriate levels of preventive care to patients and families:
A challenge for therapists with preventive sessions, we often have parents complain and become very aggressive towards clinicians because they only provided education, or they didn’t perform any of the restorative work required; their time [parent] attending the appointment was not effectively utilized. [CD01]
Nonetheless, others stated that despite therapists’ attending funded continuing professional development, upon their return knowledge application often did not occur or was not feasible, as mechanisms to implement new concepts were lacking, such as saliva-testing kits, periodontal screening-record templates, preventive remineralizing agents, and oral health products. Conversely, some participants argued that it was a matter of someone taking the lead, organizing clinical staff forums and in-house training sessions for staff, and improving processes for change implementation:
Our senior clinicians should take the lead enabling all clinicians to share updated clinical knowledge using consistent processes, learning together, clinical best practice methods for implementation; it’s something we plan to undertake with our teams. [CD04]
A few participants stated part-time clinicians lacked sufficient time to see patients or read health policies and meet mandatory training requirements, which could impact on their clinical preventive practice. For example, the participants were not sure whether staff participated in motivational interviewing training sessions held for therapists, or whether they attended LHD scientific conference programs.
Several HSMs stated that the restructure of LHDs and the improvement in processes had reduced waiting lists to manageable levels, therapists were permitted and encouraged to focus on preventive care. Clinical quality-improvement work was in progress at some LHDs to shift the therapists’ clinical frame of reference:
… giving therapists permission, allowing them follow-up appointments for preventive care, shifting their clinical frame of reference from relief of pain to prevention. [HSM07]
Resourcing continuing professional education
Professional development activities for therapists and clinical quality-improvement activities reported tended to intertwine and interrelate. Several respondents discussed recent graduating therapists’ knowledge base of the CMS and minimal intervention-dentistry philosophies and the uneven application in public health settings. The CMS for adolescents in public health settings was a concern for several CDs, considering the unpredictability of public dental demands, including adolescent’s psychosocial determinants of health. Nonetheless, several CDs highlighted the importance of professional clinical structures to support clinicians to introduce CMS and minimal intervention-dentistry concepts into clinical practice, thereby sharing knowledge with other colleagues.
A few respondents commented on their LHDs’ prevention clinics as benchmark models of care for all high-risk patients, established in consultation with pediatric dental specialists and dieticians, the variations of referral pathways into prevention clinics, or standalone prevention sessions (Figures 2 and 3). Delegated therapist leaders were responsible for coordinating, monitoring, and providing LHD preventive care-orientation support. A few metropolitan CDs stated professional development facilitated by pediatric dental specialists was open to therapists across the state; however, whether therapists attended was subject to LHD management approval and support.
Pediatric dental specialists’ clinical sessions provided therapists in rural settings with referral pathways and opportunities for consultation on the management of special cases:
[For] early management of hypomineralised permanent molars, there is still confusion over whether to refer, apply fluoride varnish and how often, place GICs [glass ionomer cements] in them, use stainless steel crowns, all preventive techniques that they are aware of and want to practice, but need further clinical support …. [CD09]
HSMs all reported that external professional development to access contemporary preventive modalities was supported with funding or conference leave in consultation with therapists as a strategy to assist clinicians maintain annual professional registration.
Legislation and clinical governance
Taking advantage of NSW Health reforms to “create a culture of clinical excellence” (CD04), establishing learning environments to encompass preventive care was seen as a way forward by some participants. Reviewing the therapist-workforce mix aligned with the Oral Health Therapist Award and NSW Dental Board legislation were opportunities to strengthen professional clinical networks. Figure 4 demonstrates proposed professional clinical structures reported by a few CDs for LHD clinical governance processes for therapists, whereas other CDs reported it as work in progress, dependent on funding. Several participants quoted clinical governance processes to support their vision, while other CDs provided clear evidence of professional accountability for the provision of preventive care:
We have fairly robust, clear peer-review mechanisms in place. Patient clinical case reports are presented to clinicians (dentists and therapists). There are opportunities for clinician sessions, whereby they discuss a particular clinical problem and someone always comes up with a solution. [CD 12]
Conversely, it was argued that there was a public misconception of what public dental services represented:
Therapists offer high-quality services in public health supported by our team of dentists and paediatric dental specialists. It’s a caring profession for them, not driven by monetary values. Meeting health-accreditation standards and performance indicators are LHD governance requirements, which clinicians have to meet; if not – then we need to address these issues. [CD04]
Some CDs and HSMs acknowledged the private sector versus public health system dichotomy, especially as new NSW legislation had been passed that allows therapists to work in the private sector. Therapists practicing in the private sector were reported to be able to offer incentives, such as fluoride toothpaste and toothbrushes, to support a patient’s compliance with the home care preventive program, thereby enhancing the long-term working relationship with their patients. These factors impacted on therapists’ practices in public health, resulting in requests/demands for preventive oral health products to support oral health self-efficacy for their adolescent patients:
We have to cater for these changes, as they are positive influencing factors for public health. Therapists enjoy providing quality care supported with the offer of oral health products for their patients, so someone in my position can do something about these requests, but realistically it comes down to balancing the money, how much can we afford …. [CD03]
Resourcing chairside preventive care
The majority of CDs and a few HSMs highlighted the lack of appropriate oral health education resources for therapists’ use at the chairside as a major impediment. Most CDs reported that it was NSW Health’s responsibility to provide scientific-based preventive guidelines for LHD consistency:
… there’s a lack of appropriate oral health education materials for therapists, consistent scientific dental disease management guidelines, which is the state’s responsibility. Therapists need to use marketing strategies to make adolescents want to brush their teeth twice a day; hard to keep saying reduce the cola, but provide them with attractive incentives to drink more water. [CD09]
Preventive guidelines for different patient age-groups provided by pediatric dental specialists and endorsed by one periodontist were available in three LHDs. Referral pathways to dieticians were available in two LHDs with teaching hospitals. Two rural HSMs were considering how they could fund dietician positions for their LHDs.
Some HSMs stated that therapists were conditioned not to request chairside preventive materials and resources, as the dictum for so long had been:
… there is no funding to purchase necessary fluoride toothpaste and toothbrushes for patients. [HSM06]
Nonetheless, access to fluoride toothpaste and toothbrushes was a norm for some LHDs, and a few LHDs also provided 5,000 ppmF toothpaste through state priority oral health promotion-funded youth and opioid-treatment programs. One other LHD was involved with a research project that enabled them to access family fluoride toothpaste and toothbrushes.
A few CDs highlighted scientific evidence for 5,000 ppmF toothpaste to control dental caries, and argued therapists should be able to offer this high-fluoride toothpaste to all identified at-risk adolescents as a major public health preventive strategy:
We should be issuing Neutrafluor 5,000 ppmF toothpaste to identified high-risk teenagers in conjunction with the family toothpaste; you keep promoting that message to brush twice a day with it, I guarantee it would be one of our most effective preventive strategies. [CD011]
Several CDs commented that funding was essential to support preventive strategies; however, they were reliant on the LHD HSMs’ funding approval.
Discussion
This study had two objectives: first to record CDs’ and HSMs’ views on factors influencing how therapists provided clinical preventive dentistry, and second to note how therapists could increase their preventive activities. The results show that these two objectives were inextricably combined, such that the themes identified in the data covered both objectives. The main issue raised is that preventive dentistry per se lacks strong support from the central funding agency and that increasing prevention activities is not a simple task of changing regulations or increasing professional education.
Resourcing of preventive care for adolescents is a continual balancing act for NSW public dental health care leaders in association with meeting LHD performance targets. System processes to ensure equity and fairness of patient access to clinical care and changes to workforce legislation were other factors that influenced oral health leaders’ resourcing of preventive care activities. This is consistent with Marks and Mertz’s dental leadership research brief, where they reported that dental directors faced such challenges as maintaining or ensuring sustainable funding, increased emphasis on providing quality care, and the movement toward a pay-for-performance model and workforce changes.30 Conversely, it is noteworthy that participants in our study counteracted these challenges by viewing health reforms as opportunities for reviewing professional clinical leadership structures, improving clinical governance processes, and incorporating scientific oral health preventive measures for public health patients. This study illustrated various levels of a CD’s dependency on HSMs to approve and fund scientific-based preventive strategies.
Nicol provided an insight into challenges or tensions health care leaders and managers faced within the British National Health Service (NHS).31 The focus is on shifting to a locally led, patient-centered, clinically driven change, placing stronger emphasis on a health and well-being service, with a paradigm shift from the traditional illness service to a health care system that is receptive to its consumers and funders, prioritizing quality care according to professionals, patients, and other agencies.31 To underpin this goal, Nicol outlined fundamental concepts, structures, and phases for consideration to enable frontline health professionals to provide leadership and take responsibility for implementing and delivering the NHS’s vision.31 The recently released NSW Health Plan: Towards 2021 is aligned with this vision.11,17
Strategies for therapists’ professional development was a work in progress, not only to enhance offering of clinical preventive care for adolescents, but inclusive of a holistic oral health service vision for the future. However, participants in this study omitted to comment on strategies to underpin therapists’ clinical leadership-development needs, as discussed by Brocklehurst et al15 and Nicol,31 as fundamental to building clinical leadership capacity in health systems.
It would therefore be judicious for LHD CDs and HSMs to encourage and sponsor therapists to enroll and participate in clinical leadership professional development courses and clinical redesign programs offered by the NSW Clinical Excellence Commission, Agency of Clinical Innovation, and Health Education and Training Institute. These three key NSW Health pillars are to assist LHDs in building clinical leadership capacity, enabling CDs and HSMs to collaborate effectively with clinical teams to develop/redesign sponsored scientific-based models of oral health care, if the vision of a world-class clinical service is to be realized.11,17 Adopting this strategy may address concerns raised by CDs and HSMs with their efforts towards shifting therapists’ frame of reference from “relief of pain” toward an NSW Health-sponsored scientific-based preventive care culture at LHD level. Blinkhorn alluded to dental health systems that leaned toward creating “emergency-only operators”, rather than highly trained and skilled clinicians, a concern consistent with our study’s findings.32
The government benefit scheme was a significant enabler in improving clinical pathways for adolescents to access preventive dental care as prescribed by the voucher.29 Skinner et al referred to the Child Dental Benefit Scheme as solutions for adolescents under 18 years of age to access dental care from the private sector.2 Interestingly, this study found that NSW public dental services are also heavily reliant on government benefit-scheme funding to support preventive care pathways for adolescents, an area for future public oral health research in terms of funding stability and direct funding for preventive care for adolescents under 18 years of age, as per its core purpose.
The differentiation argument of adolescent care from adult services was an interesting point noted by some participants in this study. Clinical pathways for adolescents were distinctive, with therapists having the scope to provide quality oral health care. Illustrating installation of specific prevention clinics and sessions within the current health care system solidified the few participants’ stance for potential adolescent preventive models of care in their LHDs.
Cashmore et al’s study reorienting NSW pediatric oral health services toward prevention recommended the involvement and engagement of entire dental teams during all planning phases when establishing programs.33 Our study’s participants planned to incorporate clinical teams in the health reforms to improve delivery of patient/client-centered care; however, they reported that funding parameters were often difficult to overcome. We found CDs and HSMs intended to enhance current clinical services internally, scoping better funding mechanisms to resource therapist preventive chairside activities. This is consistent with Cashmore et al’s suggestions for implementing preventive strategies that build on existing services.33
The respondents had a vision of creating a culture of clinical excellence for oral health, incorporating therapists’ timely provision of oral health care and preventive advice for adolescent patients in accordance with the NSW State Health Plan to deliver “world class clinical care”.17 NSW Health have devolved decision making to a local and regional level to augment transparency of funding and monitoring of performance.17 Although participants illustrated professional structures underpinned by strategies to enhance therapists’ preventive clinical practice, the complexities and interrelationships governing NSW clinical oral health services appeared uneven across LHDs in terms of human resources and funding for goods and services.
Conclusion
Resourcing and supporting therapists to provide timely and appropriate levels of preventive care to adolescents attending public dental services was important to CDs and HSMs. The main issue raised in this study is that preventive dentistry per se lacks strong support from the central funding agency, and that increasing prevention activities is not a simple task of changing regulations or increasing professional education.
Acknowledgments
Funding was received from the NSW Ministry of Health Rural and Remote Allied Health Professionals Postgraduate Scholarship Scheme and Centre for Oral Health Strategy. Appreciation is extended to NSW local health districts oral health clinical directors and health service managers for participating in this study.
Author contributions
All authors contributed toward the design of the study, preparing and critically revising the paper, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work. The findings from this study are those of the authors and do not reflect the views of the funding body or the NSW Ministry of Health.
References
Armfield JM, Spencer AJ, Brennan DS. Dental Health of Australia’s Teenagers and Pre-teen Children: The Child Dental Survey, Australia 2003–2004. Canberra: Australian Institute of Health and Welfare; 2009. | |
Skinner J, Johnson G, Phelan C, Blinkhorn A. Dental caries in 14- and 15-year-olds in New South Wales, Australia. BMC Public Health. 2013;13:1060. | |
Australian Institute of Health and Welfare. Australia’s Health 2014. Canberra: AIHW; 2014. | |
Health Statistics New South Wales [homepage on the Internet]. Available from: http://www.healthstats.nsw.gov.au. Accessed August 26, 2014. | |
Moynihan PJ, Kelly SA. Effect on caries of restricting sugars intake: systematic review to inform WHO guidelines. J Dent Res. 2014;93(1):8–18. | |
Bernabé E, Sheiham A. Extent of differences in dental caries in permanent teeth between childhood and adulthood in 26 countries. Int Dent J. 2014;64(5):241–245. | |
Spencer AJ, Harford J. Improving Oral Health and Dental Care for Australians: Prepared for the National Health and Hospitals Reform Commission. Canberra: Ministry of Health; 2008. Available from: http://www.health.gov.au/internet/nhhrc/publishing.nsf/Content/16F7A93D8F578DB4CA2574D7001830E9/$File/Improving%20oral%20health%20&%20dental%20care%20for%20Aust.pdf. Accessed May 30, 2011. | |
American Academy of Pediatrics. Guideline on caries-risk assessment and management for infants, children, and adolescents. Pediatr Dent. 2012;34(6):118–125. | |
Nash DA. Envisioning an oral healthcare workforce for the future. Community Dent Oral Epidemiol. 2012;40 Suppl 2:141–147. | |
Watt RG. Strategies and approaches in oral disease prevention and health promotion. Bull World Health Organ. 2005;83(9):711–718. | |
NSW Ministry of Health. Oral Health 2020: A Strategic Framework for Dental Health in NSW. Sydney: NSW MoH; 2013. Available from: http://www.health.nsw.gov.au/oralhealth/Documents/oral-health-2020.pdf. Accessed September 23, 2014. | |
Centre for Oral Health Strategy NSW. Pit and Fissure Sealants: Use of In Oral Health Services NSW. Sydney: NSW Ministry of Health; 2013. Available from: http://www0.health.nsw.gov.au/policies/pd/2013/pdf/PD2013_025.pdf. Accessed December 8, 2015. | |
Centre for Oral Health Strategy, NSW. Oral health. 2008. Available from: http://www.health.nsw.gov.au/oralhealth/pages/default.aspx. Accessed May 23, 2011. | |
Ford PJ, Farrah CS. Oral health therapists: what is their role in Australian health care? Int J Dent Hyg. 2012;11(1):22–27. | |
Brocklehurst P, Ferguson J, Taylor N, Tickle M. What is clinical leadership and why might it be important in dentistry? Br Den J. 2013;214(5):243–246. | |
Australian Dental Association. Dentists… Part Of a Caring Profession: Become a Dentist – Your Passport to a Brighter Future. Sydney: ADA; 2014. Available from: http://www.ada.org.au/app_cmslib/media/umlib/documents/products_publications/other%20publications/dentists%20...%20part%20of%20a%20caring%20profession.pdf. Accessed August 26, 2014. | |
NSW Ministry of Health. NSW State Health Plan: Towards 2021. Sydney: NSW MoH; 2014. Available from: http://www.health.nsw.gov.au/statehealthplan/Publications/NSW-State-Health-Plan-Towards-2021.pdf. Accessed August 26, 2014. | |
Aarons GA. Transformational and transactional leadership: association with attitudes towards evidence-based practice. Psychiatr Serv. 2006; 57(8):1162–1169. | |
Ahovuo-Saloranta A, Hiiri A, Nordblad A, Mäkelä M, Worthington HV. Pit and fissure sealants for preventing dental decay in the permanent teeth of children and adolescents. Cochrane Database Syst Rev. 2008;(4):CD001830. | |
Jenson L, Budenz AW, Featherstone JD, Ramos-Gomez FJ, Spolsky VW, Young DA. Clinical protocols for caries management by risk assessment. J Calif Dent Assoc. 2007;35(10):714–723. | |
Clarkson JE, Young L, Ramsay CR, Bonner BC, Bonetti D. How to influence patient oral hygiene behavior effectively. J Dent Res. 2009;88(10):933–937. | |
Centre for Oral Health Strategy NSW. Smoking Cessation Brief Intervention at the Chairside: Role of Public Oral Health/Dental Service. Sydney: NSW Ministry of Health; 2009. Available from: http://www0.health.nsw.gov.au/policies/pd/2009/pdf/PD2009_046.pdf. Accessed September 23, 2011. | |
Watt RG, Sheiham A. Integrating the common risk factor approach into a social determinants framework. Community Dent Oral Epidemiol. 2012;40(4):289–296. | |
Yevlahova D, Satur J. Models for individual oral health promotion and their effectiveness: a systematic review. Aust Dent J 2009;54(3):190–197. | |
O’Leary Z. The Essential Guide to Doing Research. London: Sage; 2004. | |
Glaser B, Holton J. Remodeling grounded theory. Forum Qual Soc Res. 2004;5(2):4. | |
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. | |
Centre for Oral Health Strategy NSW. Priority Oral Health Program and List Management Protocols. Sydney: NSW Ministry of Health; 2008. Available from: http://www0.health.nsw.gov.au/policies/pd/2008/pdf/PD2008_056.pdf. Accessed December 29, 2014. | |
Australian Government Department of Human Services. Medicare teen dental plan. 2012. Available from: http://www.humanservices.gov.au/customer/services/medicare/medicare-teen-dental-plan. Accessed May 3, 2014. | |
Marks A, Mertz E. Leadership Development: A Critical Need in the Dental Safety Net. San Francisco: Center for the Health Professions; 2012. Available from: http://futurehealth.ucsf.edu/Content/5763/Dental%20Director%20Issue%20Brief_FINAL.pdf. Accessed September 23, 2014. | |
Nicol ED. Improving clinical leadership and management in the NHS. J Healthc Leadersh. 2012;4:59–69. | |
Blinkhorn AS. Comparison of the dental health of adults and children living in NSW with their counterparts in the US and UK. N S W Public Health Bull. 2009;20(3–4):52–55. | |
Cashmore AW, Noller J, Ritchie J, Johnson B, Blinkhorn AS. Reorienting a paediatric oral health service towards prevention: lessons from a qualitative study of dental professionals. Health Promot J Austr. 2011;22(1):17–21. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.