")
Back to Journals » Journal of Asthma and Allergy » Volume 16
Assessment of the Current Practice of Managing Depression in Patients with Asthma in Saudi Arabia: Physicians’ Views
Authors Siraj RA , Alrajeh AM , Alhaykan AE, Alqarni AA , Alahmadi FH, Aldhahir AM , Alqahtani JS , Bakhadlq S, Alghamdi SM, Algarni SS , Alghamdi AS, Alwadeai KS , Alsulami AS, Alsindi TH, Alahmari MA
Received 8 March 2023
Accepted for publication 16 June 2023
Published 23 June 2023 Volume 2023:16 Pages 637—647
DOI https://doi.org/10.2147/JAA.S411614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Rayan A Siraj,1 Ahmed M Alrajeh,1 Ahmad E Alhaykan,1 Abdullah A Alqarni,2 Fahad H Alahmadi,3 Abdulelah M Aldhahir,4 Jaber S Alqahtani,5 Samah Bakhadlq,5 Saeed M Alghamdi,6 Saleh S Algarni,7,8 Abdulrhman S Alghamdi,9 Khalid S Alwadeai,9 Abdulelah S Alsulami,10 Tawah H Alsindi,11 Mushabbab A Alahmari12
1Department of Respiratory Care, College of Applied Medical Sciences, King Faisal University, Al-Ahasa, Saudi Arabia; 2Department of Respiratory Therapy, Faculty of Medical Rehabilitation Sciences, King Abdulaziz University, Jeddah, Saudi Arabia; 3Respiratory Therapy Department, College of Medical Rehabilitation Sciences, Taibah University, Madinah, Saudi Arabia; 4Respiratory Therapy Department, Faculty of Applied Medical Sciences, Jazan University, Jazan, Saudi Arabia; 5Department of Respiratory Care, Prince Sultan Military College of Health Sciences, Dammam, Saudi Arabia; 6Clinical Technology Department, Respiratory Care Program, Faculty of Applied Medical Sciences, Umm Al-Qura University, Makkah, 21961, Saudi Arabia; 7Department of Respiratory Therapy, College of Applied Medical Sciences, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 8King Abdullah International Medical Research Center, Riyadh, 12271, Saudi Arabia; 9Department of Rehabilitation Science, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia; 10Department of Respiratory Care Services, King Abdulaziz Medical City, Ministry of National Guard, Jeddah, Saudi Arabia; 11Department of Respiratory Therapy Program, Inaya Medical College, Riyadh, Saudi Arabia; 12Department of Respiratory Therapy, College of Applied Medical Sciences, University of Bisha, Bisha, Saudi Arabia
Correspondence: Rayan A Siraj, Department of Respiratory Care, College of Applied Medical Sciences, King Faisal University, Al-Ahasa, 31982, Saudi Arabia, Email [email protected]
Objective: Depression is a common comorbidity in patients with asthma with a significant impact on clinical management. However, little information is available about physicians’ perceptions and current practices in identifying and managing depression in individuals with asthma in Saudi Arabia. Thus, this study aims to assess physicians’ views and current practices of identifying and managing depression in patients with asthma in Saudi Arabia.
Methods: A cross-sectional study was employed. Between September 2022 and February 2023, an online survey was distributed to physicians (general practitioners and family, internal and pulmonary medicine specialists) in Saudi Arabia. Descriptive statistics were performed to analyze the collected responses.
Results: Out of 1800 invited participants, a total of 1162 physicians completed the online survey. Nearly 40% of the respondents received adequate training for managing depression. More than 60% of physicians reported that depression interferes with self-management and worsens asthma symptoms, while 50% viewed the importance of regular screening for depression. Less than 40% (n=443) aim to identify depression during patients’ visits. Of those, only 20% always screen for depression in asthma patients. Physicians show a low level of confidence when asking patients about their feelings (30%), being able to recognize depression (23%), and knowing if patients have depression (23%). The most common barriers linked to recognizing depression are high workload (50%), lack of time to screen for depression (46%), limited knowledge about depression (42%), and poor training (41%).
Conclusion: The rate of recognizing and confidently managing depression in asthmatic patients is significantly low. This is attributed to high workload, poor training, and limited knowledge about depression. There is a need to support psychiatric training and implement a systematic approach to depression detection in clinical settings.
Keywords: asthma, depression, management
Introduction
Asthma, an airway inflammation disease, is characterized by variable airflow limitation and respiratory symptoms, with a prevalence ranging from 1% to 21% globally. In Saudi Arabia, it is estimated that 11.3% of population are diagnosed with asthma by a physician and that asthma is undiagnosed in 18.2% of the Saudi general population.1 The common respiratory symptoms in patients with asthma include wheezing, shortness of breath, chest tightness, and/or cough. Worsening of these symptoms comes as a result of the presence of risk factors as well as comorbidities. Delays in identifying and managing comorbidities can ultimately lead to poor asthma management, a decline in pulmonary function, and an increased risk of unpredictable exacerbation and hospitalization.2
Depression, a common mental disorder, is among the comorbidities frequently observed in patients with asthma.3 It has been reported that the prevalence of depression in patients with asthma is variable around the world, ranging from 11% to 13%.4,5 Recent findings from our group showed that depression is also prevalent (16%) among patients with asthma in Saudi Arabia.6 Given that depression is associated with poor asthma control and adherence to inhalers,6 these findings suggest that the presence of depression in patients with asthma may lead to poor control of asthma symptoms and that early recognition and treatment of depression, by the implementation of routine screening for mental illness, may improve asthma symptoms and overall quality of life. Although international and national asthma guidelines encourage routine assessment for comorbidities,2,7 more than 50% of potential cases of depression remain underdiagnosed and consequently undertreated among patients with chronic diseases.8,9 The most commonly reported barriers are poor training that physicians and healthcare providers receive about depression as well as the absence of diagnostic tools and therapeutic strategies to identify and treat depression.10
Although physicians who are in direct contact with asthma patients play a key role in identifying the presence of depression and referring those with depressive symptoms to psychological consultation, there is no evidence that mental health assessment is currently part of the standard assessment for patients with asthma. In addition, the current practice of identifying and managing depression among patients with asthma in Saudi Arabia is not well determined. Given that there are currently not much research studies on depression in asthmatic patients in Saudi Arabia and that early recognition and interventions to effectively address depression in patients with asthma, may improve clinical outcomes, it is important to determine healthcare providers’ views on depression in patients with asthma. Therefore, this study hypothesized that 1) The prevalence of identifying and confidently managing depression in asthmatic patients is suboptimal and 2) There are multiple barriers which interfere with recognizing depression in patients with asthma. The objectives of this study are 1) To assess the physicians’ current practice of identifying and managing depression among patients with asthma and 2) To identify barriers as well as facilitators linked to physicians’ practice.
Method
Study Design and Study Participants
This study was conducted using an online survey to assess physicians’ attitudes, current practices, and barriers and facilitators for managing depression in patients with asthma. The survey was carried out from 01 September 2022 to 28 February 2023.
Ethical Consideration
Ethical approval was obtained from an independent research committee at King Faisal University (ID: KFU-REC-2022-SEP-ETHICS183).
Questionnaire Tool
The questionnaire was divided into five sections, each of which included closed-ended questions and free text spaces for further comments. The questionnaires used in this study were adopted from previous studies, which have investigated the current practice of managing depression in other populations (COPD and low vision patients).4,9,10 The questionnaires were revised to meet the objective of the current study (management of depression in patients with asthma). A group of experts from different specialities (eg respiratory medicine and respiratory epidemiology) has reformulated the original questionnaires. A pilot study was then conducted on 15 physicians (GPs, internal medicine, family medicine, and pulmonary medicine), to ensure the validity of the questionnaire was maintained. Participants who took part in the pilot testing were eliminated from the study. The questionnaire was structured as follows:
Section 1 involves questions on participants’ backgrounds, which include sex, current job, clinical experience (years), average time spent with patients, number of asthma patients seen each month, and whether physicians have ever received training for depression management.
Section 2 involves 7 statements that assess physicians’ perspectives on depression in asthma patients utilizing a 5-point Likert scale ranging from 1 to 5, with 1 being strongly disagreed and 5 strongly agreeing.
In Section 3, the current practice of working with patients with asthma and depression is evaluated. It includes three questions on the following points: 1) The desire of the physicians to recognize depression in asthmatics, 2) The application of screening tools and 3) The likelihood that actions will be taken if depression in asthma patients is assumed.
Section 4 contains nine statements to assess the level of confidence of the physicians in dealing with asthma patients, graded on a 5-point Likert scale from 1 (not confident) to 5 (completely confident).
Section 5 includes two questions that assess perceived facilitators and barriers to diagnosing depression in asthma patients.
Study Participants
Physicians were recruited for the study using a convenience sampling technique. The targeted participants were physicians who were likely to conduct a standard assessment for asthma patients, such as GPs, family medicine, internal medicine, and pulmonologist/respirologists. Professional Saudi committees (eg Saudi Society of Internal Medicine, the Saudi Thoracic Society, the Saudi Society for Respiratory Care and the Saudi Society of Family and Community Medicine) were approached, via emails, to distribute the survey among physicians. Furthermore, authors from multiple institutions in various regions participated in the data collection process to cover all geographical areas in Saudi Arabia, by approaching and following up with hospital officials to fill in survey. The survey was sent through social media networks (Twitter, WhatsApp and Telegram) to reach a greater number of participants. Each author was assigned to a specific area of the country to make sure that all regional areas are covered and samples are representative. A total of 1800 questionnaires were sent and 1162 were completed, with a response rate of 64.5%.
Before the study was conducted, participants were aware of the study’s purpose and the identity of the principal investigator. Moreover, it was clearly stated that involvement in the survey was entirely voluntary and that participants might withdraw at any time. The confidentiality of the data and that no personal information will be shared or used were also disclosed to the participants. Participants give their consent to participate in this study by answering “yes” to the following question “Do you agree to participate in the study?” The survey takes approximately 5–7 minutes to complete.
Statistical Analysis
STATA version 16.0 software StataCorp LP, College Station, TX, US) was used for statistical analyses. All variables included in this study were categorical; thus, results were reported and presented as numbers and percentages. No sample size calculation was done, as this was an exploratory study. Missing and incomplete questionnaires were removed and have not been included in the study results.
Results
Out of 1800 surveys sent, a total of 1162 physicians completed the online survey between 1 September 2022 and 28 February 2023, with a response rate of 64.5%. Most of the respondents were working in government hospitals (75.7%) and categorized based on their specialty as follows: general practitioners (41.1%) followed by family medicine practitioners (26.5%), internal medicine (17.3%), and pulmonologists (14.9%). The majority of the respondents had one to four years of clinical experience in caring for asthmatics (39.5%), with most seeing less than ten patients with asthma on a monthly basis. Unexpectedly, 60.1% of participants received no proper training for managing depression in asthma patients. The characteristics of the respondents are summarised in Table 1.
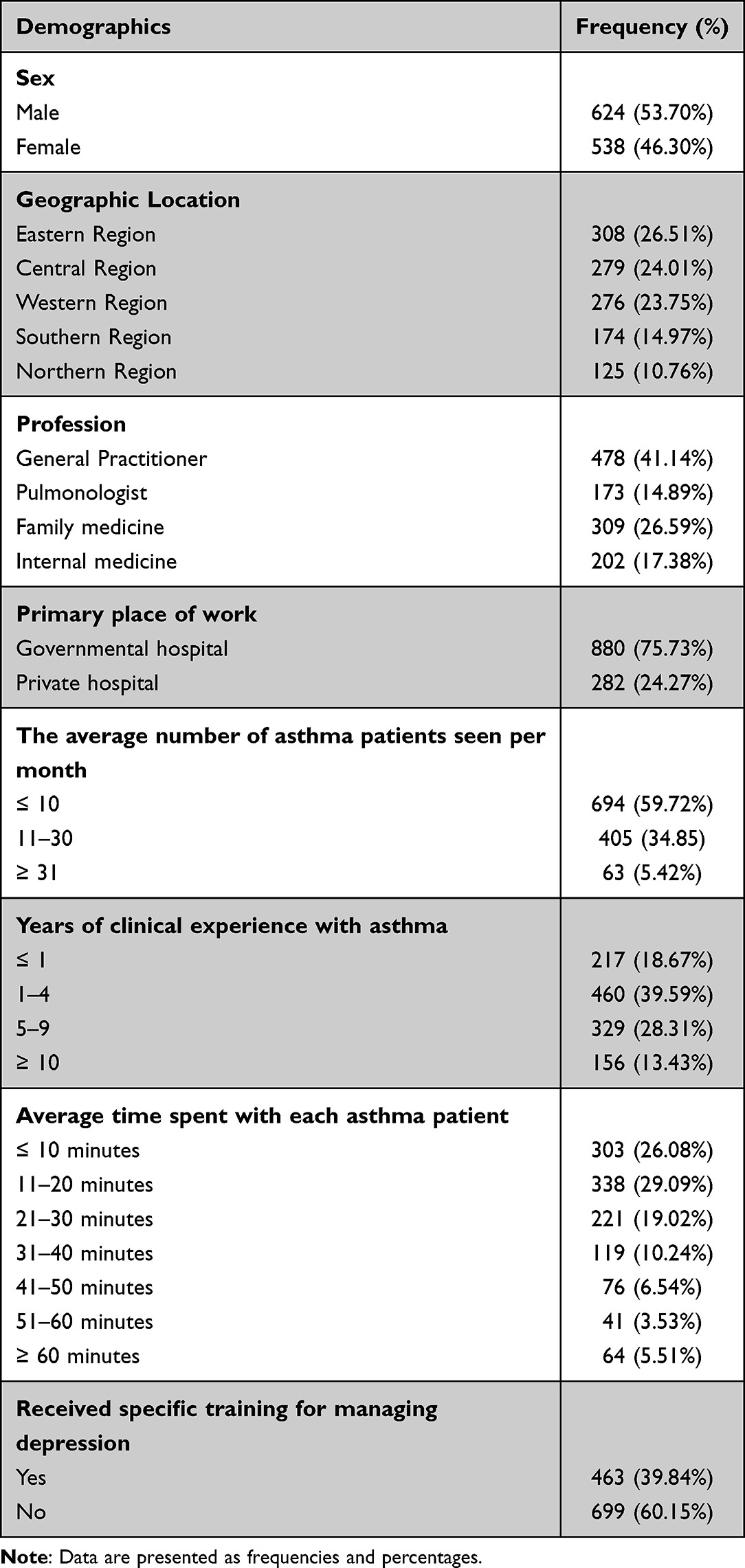 |
Table 1 Demographics and Professional Background of the Study Respondents (n= 1162) |
Physicians’ Views on Depression in Patients with Asthma
Of the 1162 respondents, 58% (Agree = 40.6%; Strongly agree = 17.3%) that depression develops as a consequence of limitations of physical illness in asthma patients. Additionally, 65.66% (Agree = 38%; Strongly agree = 27.6%) that controlling asthma symptoms is the best way of improving depression in patients. In patients with asthma and depression, 66.8% of surveyed physicians recommended prioritizing asthma treatment. However, more than half of the participants (57.4%) reported difficulty convincing asthma patients to seek treatment for depression. Furthermore, the majority of the respondents noted that depression exacerbates asthma symptoms (59.7%) and impairs self-management of asthma (67.1%). Table 2 provides a summary of the physicians’ views on depression in patients with asthma.
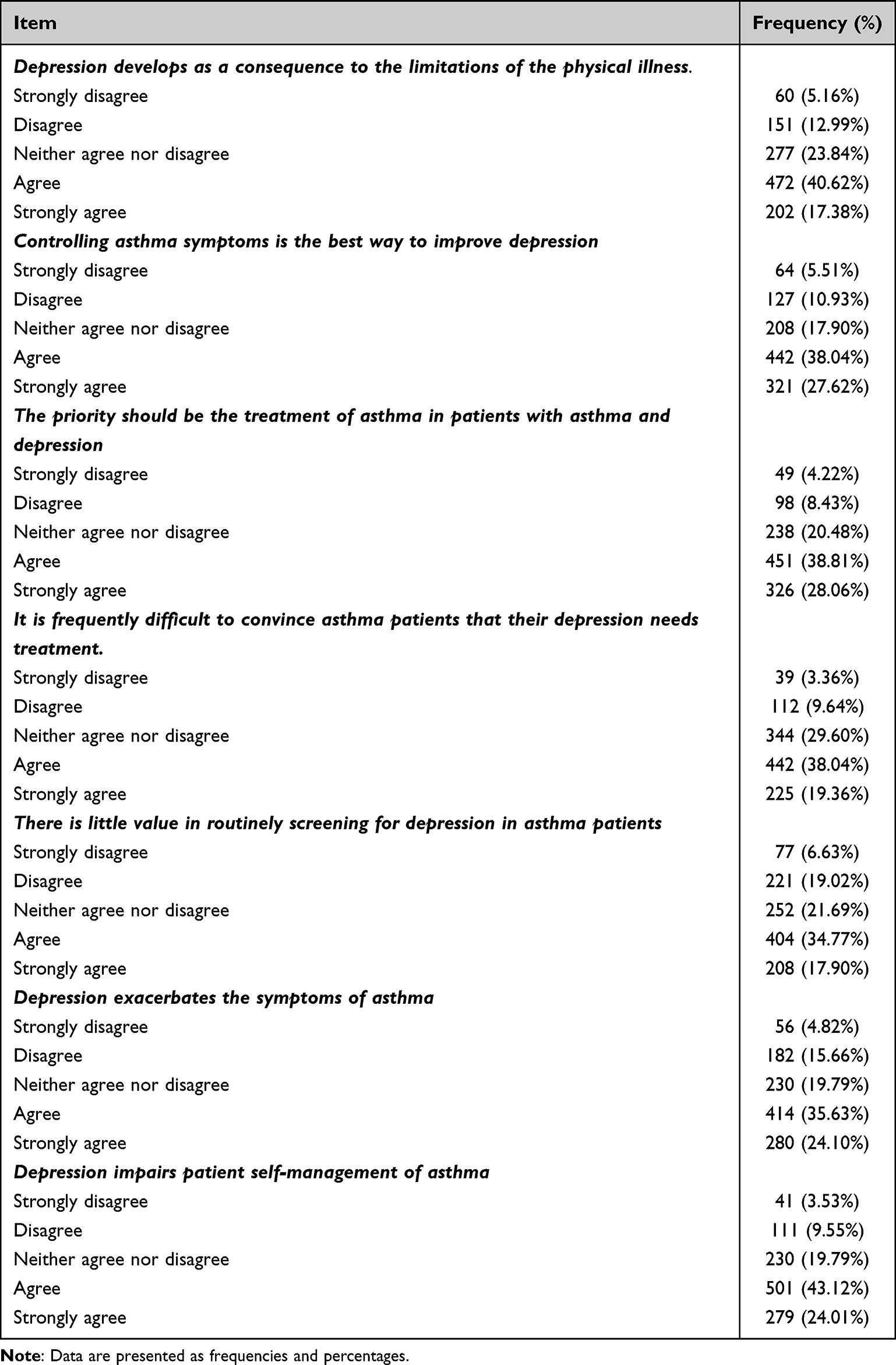 |
Table 2 Physicians’ Views About Depression in Asthmatic Patients (n= 1162) |
Current Practices and Confidence Level for Managing Depression in Patients with Asthma
The physicians were asked about their current practices and confidence in managing depression in asthma patients. Of the 1162 physicians, less than 40% (n=443) aim to identify possible depression in asthma patients, Table 3. Of those, 20.5% always use screening tools. When physicians were asked what actions they were likely to take when depression is suspected, less than half reported referrals to mental health services or using formal diagnostic questionnaires. However, Only a small proportion (30.4%) would provide medication.
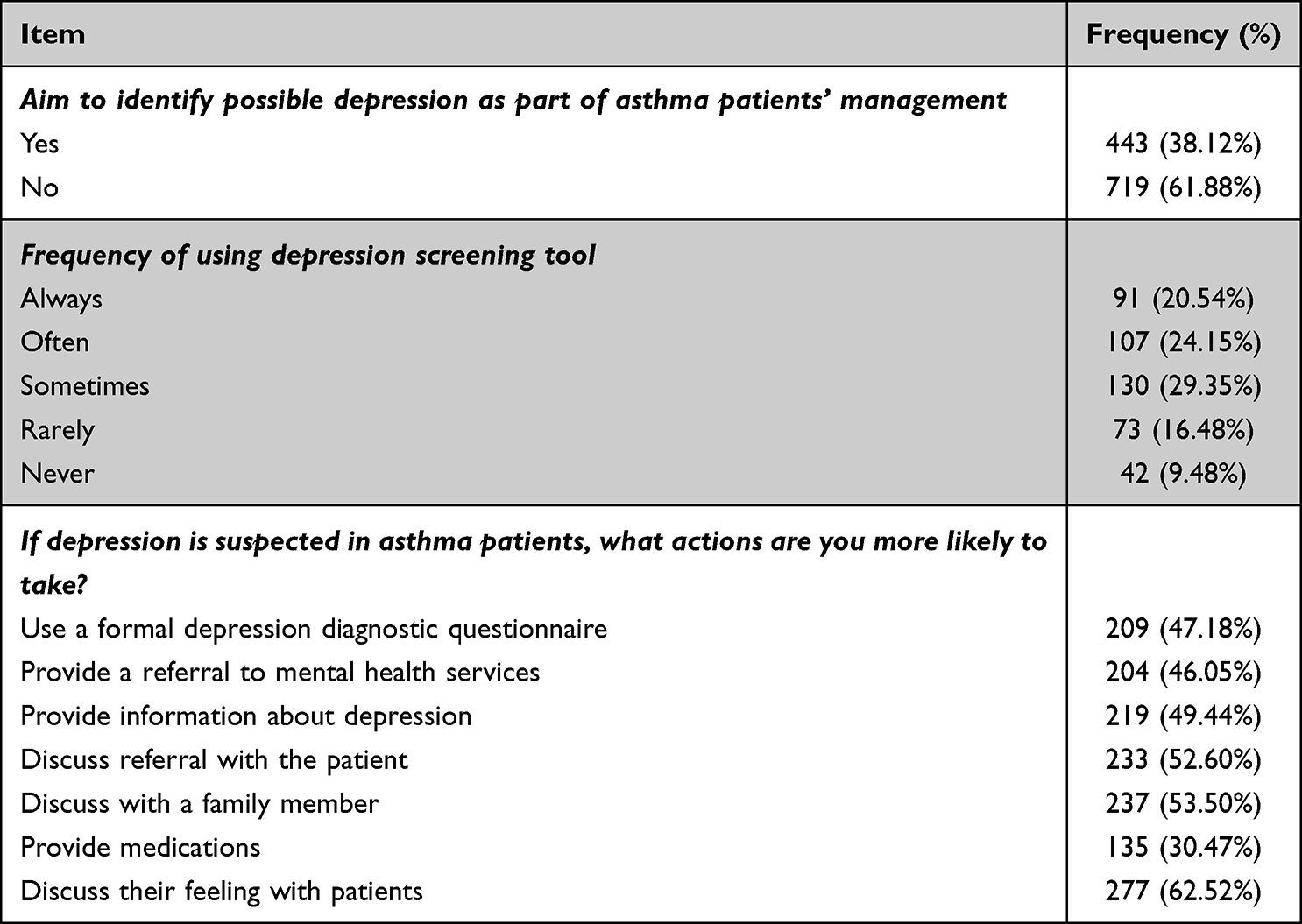 |
Table 3 Current Practice and Confidence in Working with Asthma Patients and Depression (n=443) |
Multiple questions assessed physicians’ confidence in working with patients with asthma and depression. Physicians (n=443) who were completely or fairly confident in asking the patients about their moods or feelings accounted for 54.4%. A little over 20% of the study participants showed complete confidence in recognizing depression in asthma patients. Almost half of the study participants reported a complete or fair level of confidence in discussing depression with patients’ families, providing education about depression, and knowing if the patient has depression. The level of confidence of the respondents in managing asthma patients with depression is summarised in Table 4.
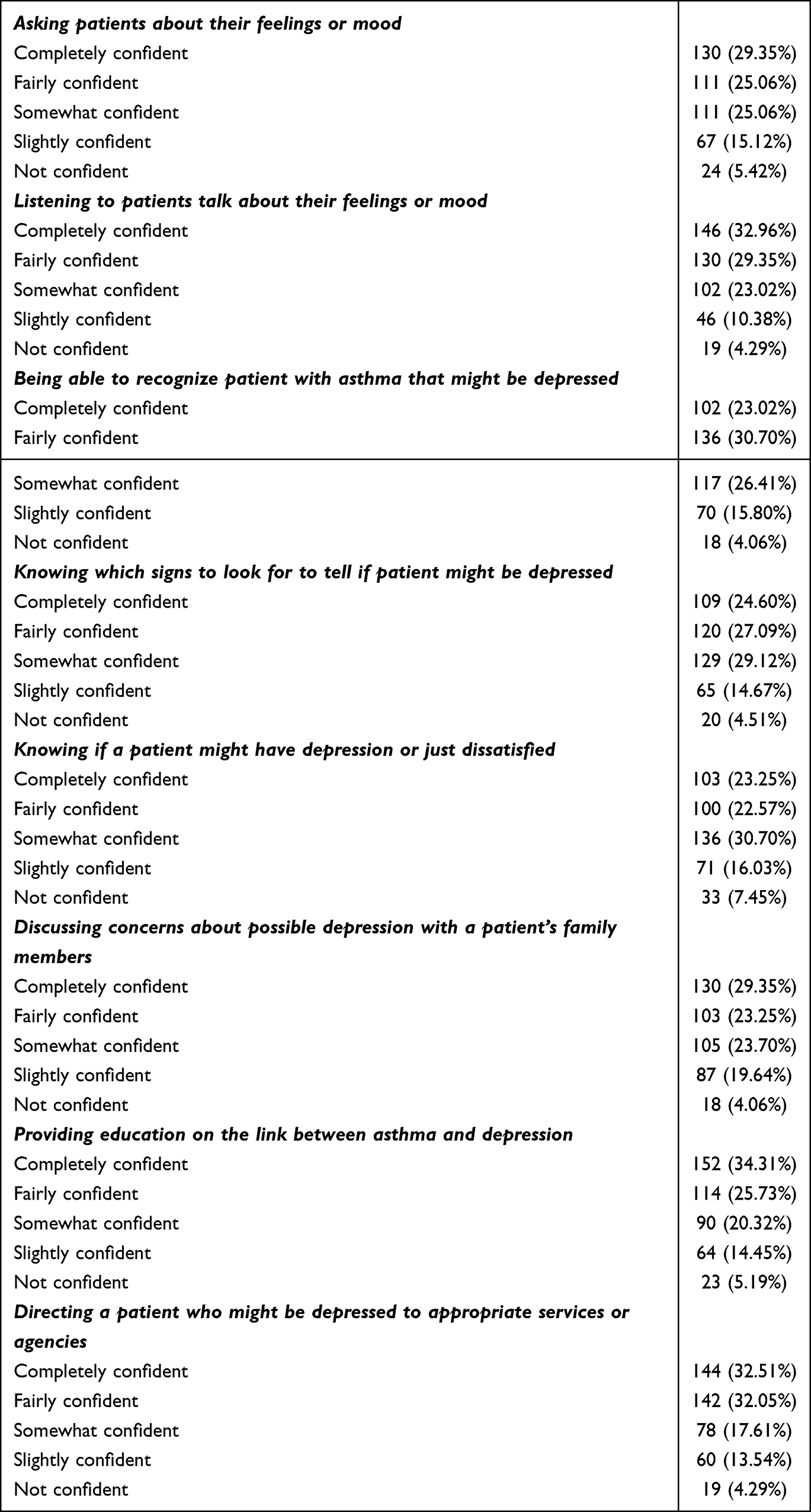 |
Table 4 Confidence in Working with Asthma Patients and Depression (n=443) |
Barriers to Identifying and Managing Depression in Asthma Patients
The most commonly reported barriers of identifying and managing depression in asthma reported by respondents to include high workload (50.2%), and as a result, it is expected that lack of time to screen every patient will also be a barrier (46%), limited knowledge about depression (42%), and poor training in depression identification and management in asthma patients (41%) Figure 1.
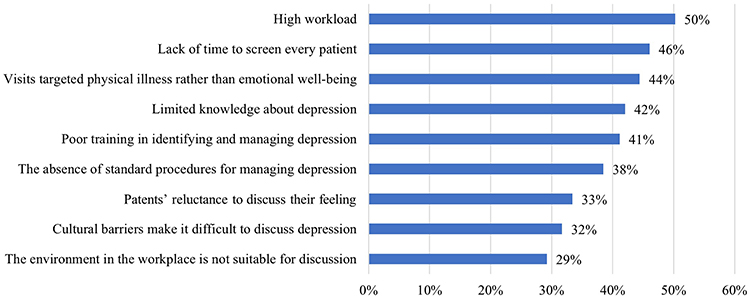 |
Figure 1 The most common barriers to identifying and managing asthma patients (n=1162). |
Factors That Facilitate the Identification and Managing Depression in Asthma Patients
The most commonly reported factors that facilitated the identification and management of depression in patients with asthma were spending adequate time with patients (56.10%) and having a reasonable workload (50.3%). The other frequently reported enabling factors were appropriate training (48%), the presence of standardized management procedures (47.2%), adequate knowledge of depression (44.4%), and the patient’s willingness to discuss feelings (41.7%) Figure 2.
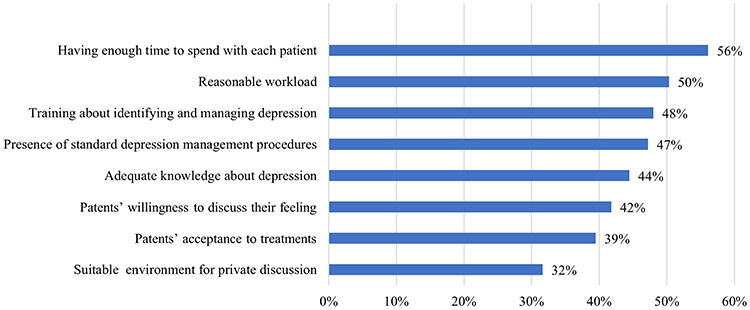 |
Figure 2 The most common factors that facilitate identifying and managing depression in asthma patients (n=1162). |
Discussion
This study aimed to assess the physicians’ current practice of recognizing and managing depression among asthmatic patients, and identify barriers and facilitators for depression management in patients with asthma. The study results showed that many physicians agreed that monitoring or controlling asthma symptoms is an effective way to prevent or ameliorate depressive symptoms. Despite this, a significant proportion of physicians have not received proper training for managing depression in patients with asthma, nor do they aim to identify depression during patients’ visits. High workload and lack of time to screen every patient were reported as the most common barriers to managing depression in asthma patients.
Depression is among the common comorbidities among patients with asthma, with a considerable impact on clinical management. Indeed, evidence suggests that asthma increases the risk of depression.4 Our findings show that over half of the study participants believed that the physical limitations caused by asthma is associated with increased depressive symptoms in asthma patients. Moreover, our participants show positive attitudes towards the impact of depression on asthma exacerbation and self-management. Indeed, there is evidence to show that depression in asthma patients is linked to serious clinical outcomes such as poor asthma control,11 higher use of rescue inhalers,12 poor adherence to medications,13 high exacerbation rate,12 and health care utilization.14 Therefore, it is essential to identify and manage depression in patients with asthma so that proper interventions can be delivered. It is worth noting that patients with asthma and depression may benefit from other non-pharmacological interventions.15 This may also be seen as a strategy to facilitate the management of the situation (eg if the depression condition improves, it may be possible to reduce rescue medications use and asthma outcomes).
Poorly controlled asthma patients are at high risk of psychological disorders, depression, and anxiety.16 Indeed, international guidelines recommend screening for depression in those who are at high risk, as it may help the healthcare provider to broaden the scope when providing the appropriate treatment. However, even with the high prevalence of depression in the asthma population, only 38% of the physician in our study aim to screen for depression during a patient visit. Moreover, 44% of them intend to assess a validated depression screening tool. Screening for depression symptoms in asthma patients using validated scales can be reported by the patient or physician17 (eg Patient Health Questinnaire-9), which can be completed by the patient addressing multiple symptoms. However, it is also necessary to note that physician assessment for depression is also needed to verify that symptoms are because of mental health aetiology. Therefore, depression screening and discussion with the patient should be part of the comprehensive respiratory assessment for asthma patients as it is practical and feasible to be also implemented in primary care settings.18
Our results indicated more than half of the physicians had not received proper training for managing depression in asthma patients. This, in turn, may explain why depression remains undiagnosed and thus untreated in a significant proportion of patients with chronic respiratory disease.8,9 Moreover, there is little preference for prescribing medication for depression (eg antidepressants) in asthma patients when depression is suspected. This may express a deep concern about the confidence level and the ability to manage depression in the absence of training. In line with this, Becker et al reported a poor ability of Saudi physician working in primary care to recognize and detect mental health disorders.19 Hence, this suggests that proper training and general awareness for physicians will enhance and change their performance level towards asthmatic patients with depression. These include involving social services specialists in the management of supporting community and social engagement, familiarising themselves with depression screening tools, and establishing a therapeutic relationship with asthmatic patients.
Barriers to identifying and managing depression in patients with asthma include high workload and lack of knowledge regarding depression in asthmatics. Providing sufficient time to interact appropriately with asthma patients will facilitate the identification and management of depression in asthmatic patients, and this explains the reason behind the high numbers of undiagnosed depression in asthma patients. With the current load, physicians’ ability to discuss possible interpersonal or psychological stressors like the patient’s feelings becomes challenging. It is important to mention that in the Saudi community, social stigma is common, which may limit many patients from discussing their mental health issues.20 Physicians should nevertheless encourage patients to discuss their feelings without taking into consideration the social stigma attached to psychological disorders. Thus, mental health screening tools are crucial to be used in clinical practice in order to timely detect depression and, therefore, intervene accordingly.
The lack of training and knowledge provided to the physicians also makes it difficult for them to correctly identify depression in asthmatics. A lack of standardized protocols may also lead to a missed opportunity to identify depression during patients’ visits. There needs to be a strategy to incorporate depression screening during the respiratory assessment. Moreover, there is also the role of the patients to be open to discussing their feelings with their physicians. Therefore, patients should be educated about the signs, symptoms and risks of depression. System issues such as time constraints and heavy workloads may prevent physicians from performing a comprehensive medical assessment. These barriers should be facilitated in order to improve patients’ outcomes. Such includes supporting healthcare providers to Implement frequent screening and allowing more time per patient’s visit to discuss psychosocial stressors with asthmatic patients.
Strengths and Limitations
This study has some potential points which strengthen our study It is the first study to report the current practice of identifying and managing depression in asthmatic patients in Saudi Arabia. Moreover, this study included physicians from different disciplines and from different regions across the country who are working with asthma patients, therefore, increasing the external validity of the study. However, the study also has some limitations. The study’s cross-sectional design prevents any causality from being evaluated. Second, the survey approach does not include the same applications, experiences, and real-world occurrences because daily practices are challenging to explore, record, and evaluate. In addition, the results could have been influenced by subspecialty care, as the majority of our participants were GP practitioners working in primary care settings. In fact, we have not asked about whether physicians work at primary, secondary, or tertiary care centres. Moreover, this study aimed to assess the current practice of Saudi Arabia, and the results may not be applicable to other healthcare systems elsewhere.
Conclusion
Depression is a common comorbidity in patients with asthma, contributing to worse clinical outcomes and making the clinical management more challenging; thus, should be recognized and managed as early as possible. However, the rate of physicians who have received adequate training, and thus, aim to identify depression in patients with asthma is of a significant concern. Factors such as considerable workload and lack of time to screen every patient are likely to interfere with the intention to recognize depression among patients with asthma. There is a need for aggressive training in psychiatric care to allow for the early detection and timely interventions of depressive symptoms. Future research should also focus on the role of frequent screening of depression in this population.
Acknowledgement
The author acknowledges the Deanship of Scientific Research, Vice Presidency for Graduate Studies and Scientific Research at King Faisal University, Al-Ahsa, for providing financial support under the Promising Researcher Track “Grant No. 3693”.
Funding
This work was supported by the Deanship of Scientific Research, Vice Presidency for Graduate Studies and Scientific Research, King Faisal University, Saudi Arabia (Grant No. 3693).
Disclosure
The authors report no conflicts of interest in this work.
References
1. AlAhmari M. Asthma prevalence among adults in Saudi Arabia. Saudi Med J. 2018;39(7):740. doi:10.15537/smj.2018.7.23170
2. Reddel HK, Bacharier LB, Bateman ED, et al. Global initiative for asthma strategy 2021: executive summary and rationale for key changes. Am J Respir Crit Care Med. 2022;205(1):17–35. doi:10.1164/rccm.202109-2205PP
3. Lomper K, Chudiak A, Uchmanowicz I, Rosinczuk J, Jankowska-Polanska B. Effects of depression and anxiety on asthma-related quality of life. Pneumonol Alergol Pol. 2016;84(4):212–221. doi:10.5603/PiAP.2016.0026
4. Choi HG, Kim JH, Park JY, Hwang YI, Jang SH, Jung KS. Association between asthma and depression: a national cohort study. J Allergy Clin Immunol Pract. 2019;7(4):1239–45 e1. doi:10.1016/j.jaip.2018.10.046
5. de Miguel Diez J, Hernandez Barrera V, Puente Maestu L, Carrasco Garrido P, Gomez Garcia T, Jimenez Garcia R. Psychiatric comorbidity in asthma patients. Associated factors. J Asthma. 2011;48(3):253–258. doi:10.3109/02770903.2011.554943
6. Alqarni AA, Aldhahir AM, Alqahtani JS, et al. Association of anxiety and depression with adherence to inhaler in patients with asthma. In: C102 Asthma and Copd: Advancing Behavioral Sciences and Health Services Research. American Thoracic Society; 2023:A6007–A600.
7. Al-Moamary MS, Alhaider SA, Alangari AA, et al. The Saudi initiative for asthma - 2021 update: guidelines for the diagnosis and management of asthma in adults and children. Ann Thorac Med. 2021;16(1):4–56.
8. Faisal-Cury A, Ziebold C, Rodrigues DMO, Matijasevich A. Depression underdiagnosis: prevalence and associated factors. A population-based study. J Psychiatr Res. 2022;151:157–165. doi:10.1016/j.jpsychires.2022.04.025
9. Mitchell AJ, Vaze A, Rao S. Clinical diagnosis of depression in primary care: a meta-analysis. Lancet. 2009;374(9690):609–619. doi:10.1016/S0140-6736(09)60879-5
10. Searle K, Blashki G, Kakuma R, Yang H, Zhao Y, Minas H. Current needs for the improved management of depressive disorder in community healthcare centres, Shenzhen, China: a view from primary care medical leaders. Int J Ment Health Syst. 2019;13:47. doi:10.1186/s13033-019-0300-0
11. Sastre J, Crespo A, Fernandez-Sanchez A, Rial M, Plaza V. Anxiety, depression, and asthma control: changes after standardized treatment. J Allergy Clin Immunol Pract. 2018;6(6):1953–1959. doi:10.1016/j.jaip.2018.02.002
12. Ahmedani BK, Peterson EL, Wells KE, Williams LK. Examining the relationship between depression and asthma exacerbations in a prospective follow-up study. Psychosom Med. 2013;75(3):305–310. doi:10.1097/PSY.0b013e3182864ee3
13. Krauskopf KA, Sofianou A, Goel MS, et al. Depressive symptoms, low adherence, and poor asthma outcomes in the elderly. J Asthma. 2013;50(3):260–266. doi:10.3109/02770903.2012.757779
14. Feldman JM, Siddique MI, Morales E, Kaminski B, Lu SE, Lehrer PM. Psychiatric disorders and asthma outcomes among high-risk inner-city patients. Psychosom Med. 2005;67(6):989–996. doi:10.1097/01.psy.0000188556.97979.13
15. Depression: management of depression in primary and secondary care London National Institute for Health and Clinical Excellence (NICE); 2004 Available from: https://www.nice.org.uk/guidance/cg23.
16. Di Marco F, Verga M, Santus P, et al. Close correlation between anxiety, depression, and asthma control. Respir Med. 2010;104(1):22–28. doi:10.1016/j.rmed.2009.08.005
17. Mancuso CA, Wenderoth S, Westermann H, Choi TN, Briggs WM, Charlson ME. Patient-reported and physician-reported depressive conditions in relation to asthma severity and control. Chest. 2008;133(5):1142–1148. doi:10.1378/chest.07-2243
18. Williams JW Jr, Noël PH, Cordes JA, Ramirez G, Pignone M. Is this patient clinically depressed? JAMA. 2002;287(9):1160–1170. doi:10.1001/jama.287.9.1160
19. Becker SM. Detection of somatization and depression in primary care in Saudi Arabia. Soc Psychiatry Psychiatr Epidemiol. 2004;39(12):962–966. doi:10.1007/s00127-004-0835-4
20. Hasan AA, Musleh M. Self-stigma by people diagnosed with schizophrenia, depression and anxiety: cross-sectional survey design. Perspect Psychiatr Care. 2018;54(2):142–148. doi:10.1111/ppc.12213
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.