Back to Journals » Clinical Ophthalmology » Volume 17
Assessment of Preoperative Risk Factors for Post-LASIK Ectasia Development
Authors El-Naggar MT ![]() , Elkitkat RS
, Elkitkat RS ![]() , Ziada HED, Esporcatte LPG, Ambrósio R Jr
, Ziada HED, Esporcatte LPG, Ambrósio R Jr ![]()
Received 29 June 2023
Accepted for publication 26 September 2023
Published 4 December 2023 Volume 2023:17 Pages 3705—3715
DOI https://doi.org/10.2147/OPTH.S425479
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Mohamed Tarek El-Naggar,1 Rania Serag Elkitkat,2– 5 Hossam El-din Ziada,6 Louise Pellegrino Gomes Esporcatte,7– 9 Renato Ambrósio Jr7– 11
1Refractive Surgery Unit, Ophthalmology Department, Research Institute of Ophthalmology, Giza, Egypt; 2Ophthalmology Department, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 3Watany Eye Hospital, Cairo, Egypt; 4Watany Research and Development Center, Cairo, Egypt; 5Ophthalmology Department, Modern University for Technology and Information, Cairo, Egypt; 6Cornea and Refractive Surgery Unit, Ophthalmology Department, Faculty of Medicine, AL-Azhar University, Cairo, Egypt; 7Rio de Janeiro Corneal Tomography and Biomechanics Study Group, Rio de Janeiro, Brazil; 8Instituto de Olhos Renato Ambrósio, Rio de Janeiro, Brazil; 9Department of Ophthalmology, Federal University of São Paulo, São Paulo, Brazil; 10Brazilian Study Group of Artificial Intelligence and Corneal Analysis - BrAIN, Rio de Janeiro & Maceió, Brazil; 11Department of Ophthalmology, Federal University of the State of Rio de Janeiro (UNIRIO), Rio de Janeiro, Brazil
Correspondence: Mohamed Tarek El-Naggar, Email [email protected]
Purpose: To evaluate preoperative risk factors (mainly those related to corneal topography/tomography) for post-LASIK ectasia development.
Methods: A retrospective case review for post-LASIK ectasia for myopia or myopic astigmatism. The evaluated data included preoperative subjective refraction, method of flap creation, and topometric/tomographic parameters from Oculus Pentacam, including subjective curvature pattern, topometric, elevation, and pachymetric indices from the Belin Ambrosio display “BAD”, and the Pentacam Random Forest Index (PRFI). Moreover, preoperative ectasia detection indices were calculated (including Percentage of Tissue Altered “PTA” index, Randleman Ectasia Risk Score System “ERSS”, and Navarro Index for Corneal Ectasia “NICE”).
Results: Twenty-four eyes of 15 patients were enrolled. Concerning the risk factors, age was lower than 25 in 19 eyes (79%); flaps were created using a microkeratome in 17 eyes (70.8%); thinnest pachymetry was lower than 510μm in eight eyes (33%); total deviation from BAD was higher than 1.6 in 50%; Ambrósio’s relational thickness (ART) max was lower than 340 in 45.83%; PTA index was higher than 40% in 16%; ERSS was more than 3 points in 62.5%; NICE was higher than 8 points in three eyes (12.5%); PRFI index was more than 0.125 in 87.5%; two eyes (8%) had no identifiable risk factors.
Conclusion: Current ectasia risk assessment criteria were insufficient for detecting a relatively large number of cases. There is an unequivocal need for more information, which may be derived from biomechanical assessment and epithelial thickness mapping. Novel corneal tomography indices derived from artificial intelligence may increase accuracy in characterizing ectasia susceptibility.
Keywords: cornea ectasia, preoperative ectasia risk assessment, LASIK screening, Pentacam
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Navarro-Naranjo has been published for this article.
Introduction
Laser in situ keratomileusis (LASIK) is the most frequently performed refractive surgery worldwide, with recognizable efficiency and safety.1 Post-LASIK corneal ectasia has been regarded as one of the most feared complications since the first report by Seiler in 1998.2,3 It is considered in patients who develop keratometric steepening, elevated values of posterior corneal elevation, with or without central and paracentral corneal thinning, and/or topographic evidence of asymmetric inferior corneal steepening following LASIK procedure.4 Its prevention has always been a significant concern for refractive surgeons.5,6
In the published literature, the prevalence of post-LASIK ectasia ranges between 0.04% and 0.9%.7,8 Over the last two decades, the incidence of ectasia has reduced from moderately high levels of 0.66%9 and 0.57%,10 down to 0.2%,11 0.05%,12 and 0.033%.13 Such reduction in this severe complication has resulted from considerable efforts to develop advanced and meticulous preoperative screening strategies.12,14
Notably, some ectasia cases that developed without detectable risk factors have challenged and motivated research in this zone. In a recent systematic review, including LASIK surgeries performed between 1984 and 2021, post-LASIK ectasia in eyes without preoperative recognizable risk factors occurred with an incidence of 0.09%.15
Preoperative risk factors associated with ectasia development have been reported and thoroughly studied for many years. Patients’ age, subjective refraction, and preoperative corneal topographic/tomographic parameters have long been considered benchmarks for evaluating possible ectasia development.7,8,13,14,16 It is also well known that corneal ectasia is a biomechanical decompensation of the corneal stroma that is highly related to the preoperative corneal biomechanical stability and the impact of the refractive surgery on the corneal biomechanics. The current acceptance is that combining preoperative risk factors and the surgical impact on the corneal stroma can define postoperative corneal behavior, either corneal stability or ectasia development after LASIK.17–19 Some cases with low preoperative risk factors can still develop ectasia, while others with high probabilities of developing ectasia remain stable.20 This supports combining the factors above while evaluating ectasia risk. Biomechanical weakening can be caused by the refractive tissue removal procedure or postoperative mechanical trauma or stress, including constant eye rubbing.21
For decades, irregular corneal topography has been regarded as the main factor for identifying ectasia risk. However, new imaging technologies, such as tomography and biomechanical assessment, have enhanced the ability to identify mild preoperative ectatic corneal diseases, as in forme fruste or subclinical ectasia cases.22 Recent studies have demonstrated that typical topography does not exclude a mild or early ectatic corneal disease.5,22,23 Furthermore, combining diagnostic technologies with artificial intelligence (AI) techniques has recently shown higher accuracy in identifying risk factors for ectasia development and distinguishing susceptibility for biomechanical failure and ectasia progression.24
This study aimed to analyze a cohort of cases from Egypt that developed ectasia after LASIK. Preoperative data, including subjective refraction, relevant Oculus Pentacam topographic/tomographic data, and preoperative ectasia risk screening indices, were analyzed to detect the possible preoperative risk factors for developing ectasia after LASIK in these cases.
Materials and Methods
This study was conducted on a cohort of patients from Egypt who developed post-LASIK ectasia. The surgeries were performed by many surgeons all over Egypt, and they were referred for medical consultation following post-LASIK ectasia detection and deterioration of their clinical conditions. Cases sought medical advice at the Watany Eye Hospitals (WEH), Cairo, Egypt, and the Research Institute of Ophthalmology (RIO), Giza, Egypt. The study abided by the tenets of the Declaration of Helsinki and was approved by the Ethical Committee of Watany Eye Hospitals (registration code COR-2020-004) and the Federal University of São Paulo/UNIFESP/SP 2020 (registration code 4.050.934). The Institutional Review Boards granted waivers of informed consent owing to the study’s retrospective nature. Patients’ data were kept anonymous with utmost confidentiality.
The present study analyzed patients’ clinical data and topographic/tomographic parameters. The electronic medical records were searched to attain the relevant data, including age, manifest refraction, spherical equivalent, treated cylinder, method of flap creation (either using a microkeratome or femtosecond laser), and the average flap thickness.
Regarding the topographic/tomographic parameters, all the patients’ pre and postoperative data were exported to U12 files, and they were retrieved using the Pentacam software version 1.21b53 (Oculus, Wetzlar, Germany) and analyzed to detect any preoperative abnormal values that could be identified as risk factors for developing post-LASIK ectasia, either abnormal values of the sole indices or after incorporating them in ectasia risk screening indices.
The evaluated Pentacam parameters included the topometric indices [index of height decentration (IHD), inferior minus superior (IS value), and KISA index], the total deviation value of the Belin / Ambrósio Enhanced Ectasia Display (BAD-D), and the maximum Ambrosio’s Relational Thickness (ARTmax), and the newly introduced AI-based Pentacam Random Forest Index (PRFI). In addition, preoperative ectasia risk detection indices were analyzed, including the Percentage of Tissue Altered (PTA) index, the Ectasia Risk Score System (ERSS), and the Navarro Index for Corneal Ectasia (NICE).
Statistical Analysis
The statistical analysis was done with Microsoft Excel 2023 (Microsoft, Seattle, WA, USA). The quantitative data were presented as mean, standard deviations, median, confidence intervals, and ranges, whereas the qualitative variables were presented as numbers and percentages.
Results
The study enrolled 24 eyes of 15 patients who underwent LASIK for myopia or myopic astigmatism, using either a mechanical microkeratome or femtosecond laser. Two eyes had no identifiable risk factors, and four patients had unilateral ectasia. The retrieved history from the electronic medical records showed that multiple experienced surgeons performed the surgeries.
The enrolled cohort had an average age of 25 ± 4.84 years (range of 21–40 years). Age was lower than 25 in 19 eyes (79%). The chart and topography review revealed that one eye had myopia, while 23 had myopic astigmatism. The average spherical treatment was −3.35 D (range of −5.25 to −0.25 D), the average cylinder was −1,09 CylD (range −2.75 to zero CylD), and the average spherical equivalent was −3.54 D ± 1.34 (range of −5.62 to −1.37 D).
Regarding the method of flap creation, seventeen ectasia cases had a flap created using a mechanical microkeratome (average flap thickness 130 ± 12.4μm). In comparison, in 7 eyes, the flap was created using a femtosecond laser (average flap thickness 117 ± 4.88 μm).
The retrieved Pentacam parameters were evaluated. Atypical topography was detected in 20 eyes, either in the form of asymmetric bowtie (6 eyes, 25%), skewed bowtie (3 eyes, 12.5%), or irregular topography (11 eyes, 45.8%). However, the topometric indexes (including the IHD, IS value, and KISA index) were all within the normal values in all patients.
Regarding the pachymetric indices, which were retrieved from the Belin Ambrosio Enhanced Ectasia Display, the thinnest corneal pachymetry was lower than 510μm in eight eyes (33%), BAD-D was higher than 1.6 in 12 eyes (50%), and ART max was lower than 340 in 11 eyes (45.83%). The AI-based PRFI index showed high accuracy in ectasia detection and was more than 0.125 in 21 eyes (87.5%).
Regarding the calculated preoperative ectasia risk detection indices, the PTA index was higher than 40% in 4 eyes (16%), and the ERSS was more than 3 in 16 eyes (62.5%). For the NICE index, it was higher than 8 points in three eyes (12.5%).
Data from the four stable LASIK eyes (in patients having unilateral ectasia) is presented in Table 1. Table 2 shows the demographics and the incidence of tomographic and clinically recognizable risk factors among patients, and Table 3 shows the summary of clinical parameters from Scheimpflug-based corneal tomography analysis.
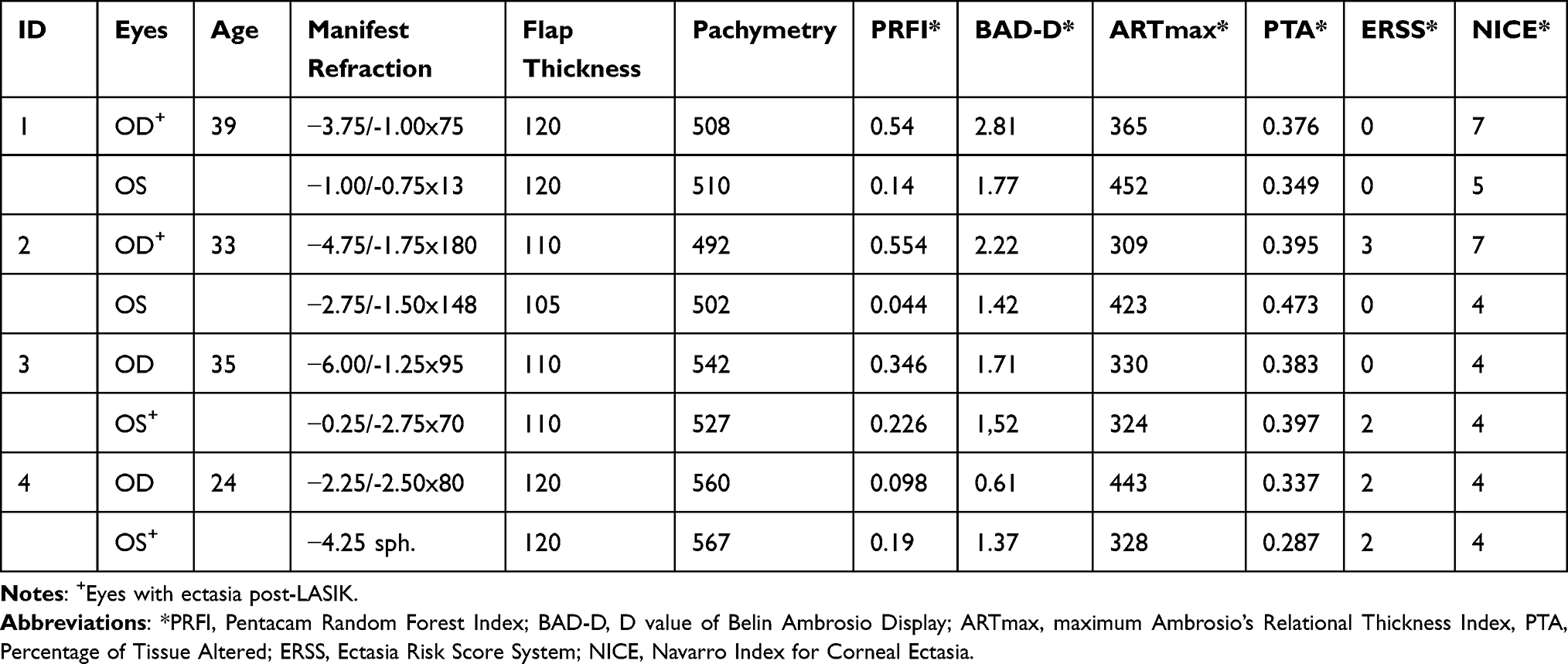 |
Table 1 Demographics and Incidence of Tomographic and Clinically Identifiable Risk Factors Among the Four Patients with One Stable-LASIK Eye |
 |
Table 2 Demographics and Incidence of Tomographic and Clinically Identifiable Risk Factors Among Patients |
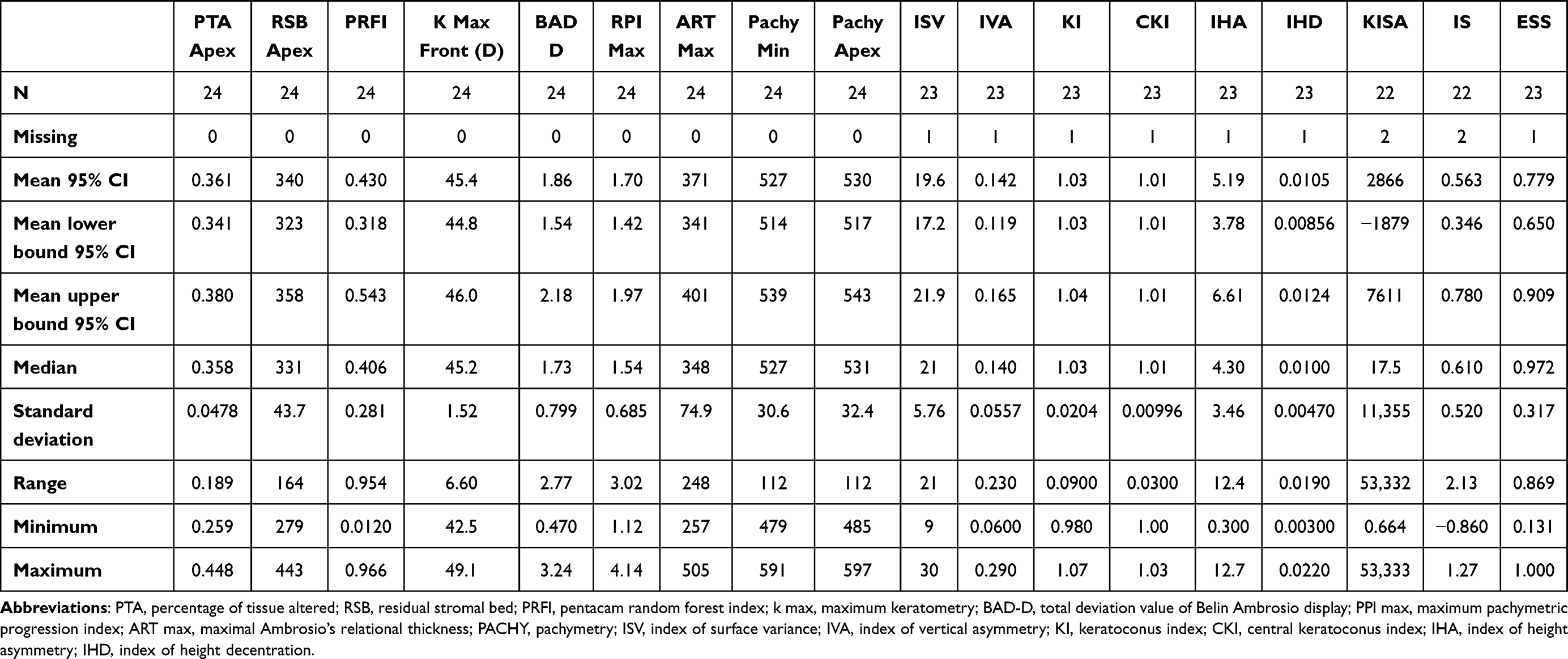 |
Table 3 Summary of Clinical Parameters from Scheimpflug-Based Corneal Tomography Analysis |
Patients’ age, eye laterality, preoperative refraction, PRFI index, and pre - and postoperative Pentacam topometric and Belin Ambrosio displays for patients 1 to 15 included in the study are shown in Supplementary Figures 1–15, respectively. Figure 1 shows the Pentacam topometric parameters of a patient who developed ectasia in the right eye (OD) and remained with a stable left eye (OS). Figure 2 shows the BAD-D from both eyes of the same patient.
 |
Figure 1 The Pentacam topometric indices of a patient who developed ectasia in the right eye (OD) while his left eye (OS) remained stable. We can observe an asymmetric bow tie in OD and a relatively symmetric bow tie in OS in the topography maps. |
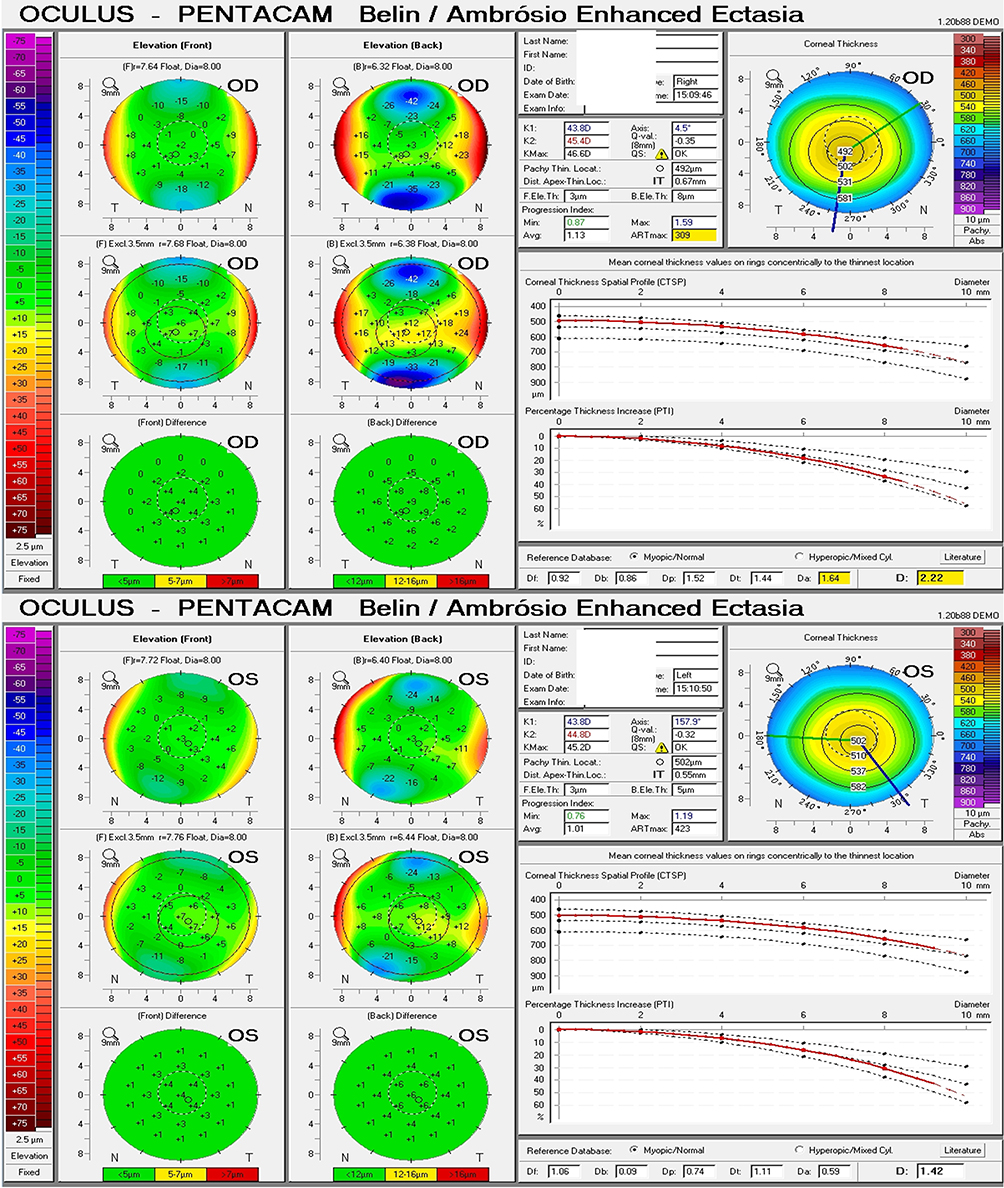 |
Figure 2 The Pentacam Belin/Ambrósio Enhanced Ectasia (BAD-D) in the two eyes of the same patient, with BAD-D of 2.22 in OD and 1.42 in OS. |
Discussion
The development of corneal ectasia is a serious complication following LASIK surgery.2,7,12 In this study, we aimed to evaluate the main preoperative identifiable risk factors that presumably resulted in the development of post-LASIK ectasia.
Most patients (17 out of 24 eyes) had a corneal flap created using a mechanical microkeratome rather than a femtosecond laser. In microkeratome-assisted LASIK, Klein et al25 estimated a rate of post-LASIK ectasia that reached 0.04%, and other reports showed rates of ectasia up to 0.9%.26,27 Furthermore, Spadea et al10 deduced in their study that 0.1% of patients with preoperative zero to low ectasia risk developed ectasia after microkeratome-assisted LASIK. Considering femtosecond-assisted LASIK, Moshirfar et al12 acknowledged that 1 in 2000 patients (0.05%) might develop ectasia. These studies’ results elaborate on the higher risk of ectasia development in mechanical microkeratome cases. This may be attributed to the inaccuracies in flap calculations and the residual stromal bed thickness.
In our study, abnormal PRFI index (0.43 ± 2.81) and abnormal BAD-D (1.86 ± 0.79) were the most encountered risk factors for ectasia development among the recruited cases, followed by ARTmax (371 ± 74.9), a thin cornea (527 ± 30.6 μm), RSB lower than 300 μm (340.39 ± 43.69 μm), and PTA index equal to or higher than 40% (0.361 ± 0.047%). In the relevant published literature, a thin cornea was the most common risk factor, followed by abnormal topography/tomography (eg, anterior map irregularities), low RSB, and PTA equal to or higher than 40%.26,28,29
Bohac et al13 reported that in the cases that developed ectasia, 30% had an RSB lower than 300 μm (none lower than 250 μm), 20% had PTA higher than 40%, and 50% had a cornea thinner than 500 μm. Contrarily, over 15% of stable-LASIK cases had RSB less than 300 μm, and only 20% of such patients had higher than 40% PTA.
A recent study by Elhusseiny et al showed that the ERSS was sensitive, specific, and accurate in screening keratorefractive surgery candidates.30 Similarly, our study results detected a preoperative ERSS higher than three in 62.5% of eyes that developed post-LASIK ectasia.
The NICE index is a cumulative risk index and can be considered a diagnostic test to evaluate LASIK refractive surgery candidates and reduce the risk of postoperative ectasia development. It is based on elevation corneal tomography through Pentacam HR System, Oculus Wetzlar, Germany, including keratometry max (K2), pachymetry, and IS value. Ideal candidates for LASIK are those with NICE equal to or less than 4. Cases with scores of more than four and less than eight could be candidates for laser surface ablation according to the value of their refractive error and the corneal thickness.31 In our cohort of patients, 12.5% of the eyes would have been contraindicated for corneal refractive surgery based on the NICE recommendations, and 50% would have been contraindicated for LASIK. This adds to the significance of considering this index for preoperative patients’ evaluation.
Artificial intelligence (AI) has been developed to improve the ability to screen for ectasia risk.32 Novel parameters such as the Tomographic and Biomechanical (TBI) index, which combine Scheimpflug-based corneal tomography and biomechanics for enhancing ectasia detection, were developed using AI,33 and the Pentacam Random Forest Index (PRFI), which was analyzed in the present study, is another example of AI-based indices.34 Furthermore, the Relational Tissue Altered (RTA) concept was developed considering the biomechanical impact of the LVC procedure.21 A next step would be to train AI to assess the surgery impact based on stable ectatic populations. Future studies should focus on using the uprising benefits and applications of AI for depicting ectasia detection indices and evaluating their accuracy for the detection of this serious complication.
It is essential to have clinical data to train and validate the AI models for developing such algorithms. The ectasia susceptibility score (ESS) was created by the BrAIN (Brazilian Artificial Intelligence Networking in Medicine), considering a cohort that included data from sixty cases that developed ectasia from an international pool. The ESS calculates the relative risk of developing ectasia according to age, flap thickness, IHD, ablation depth, cornea’s thinnest point, and BAD-D. The predicted model leads to a binary outcome from zero to one, representing the relative risk for ectasia. It was able to classify all the cases studied in this work correctly. According to the procedure and corneal tomography data, the ESS provides an individualized risk score for ectasia. An enhanced approach has been developed, and data from such a study has been necessary.21,35
Considering that keratectasia appears due to a blend of preoperative predisposition or susceptibility of the patient’s cornea and the impact of surgery on corneal structure,21 the principal aim of preoperative refractive surgery screening is not only to identify cases with mild ectasia but also to distinguish each cornea in terms of its susceptibility to undergo biomechanical failure and ectasia.36 The integration of tomographic and biomechanical data can increase the accuracy of detecting ectatic disease and identify the susceptibility to develop this complication after LVC. Evaluating ectasia risk should include a combination of patient-related data and procedure-related parameters.21
In our study, four cases had unilateral post-LASIK ectasia. A recently published study by Yang et al focused on cases of unilateral ectasia following LASIK. This work interestingly documented cases with an onset ranging between 4 months and 18 years, which mandates long-term follow-up and is also suspicious of early post-LASIK ectasia occurrence. The study also showed that posterior elevation values and a combined index of front and posterior elevations were higher among the fellow eyes of post-LASIK ectasia cases compared to a group of normal eyes and recommended future longitudinal studies with larger sample sizes to study this entity of unilateral ectasia for longer follow up intervals.37
This study is not without limitations. It is a retrospective study conducted on a single ethnic group of patients. The documented history-taking lacked some essential points, especially the symptoms related to ocular allergies, such as itchy discomfort and irritation. Eye rubbing significantly impacts the “biomechanical stress” applied to the cornea and is strongly associated with ectasia development and progression.16,38 Future longitudinal studies that combine tomographic evaluation with biomechanical corneal assessment and epithelial mapping can be more informative to enrich our understanding of corneal ectasia development following LASIK.
Conclusions
There is a need to go beyond, not over, the classic currently accepted risk factors for detecting the risk of ectasia after LASIK. Corneal topography and tomography increase sensitivity, but some cases demonstrate the need to characterize the corneal structure further. Such data related to the inherent individual susceptibility for ectasia development will be considered along with the impact of the surgical procedure to individualize ectasia risk assessment. Additional integration with multimodal data, including the biomechanical evaluation and corneal epithelial thickness, ocular wavefront, advances related to molecular biology, and genetics, are also promising. In this case, with a vast amount of clinical data, AI will perform an essential role in enlarging the efficacy of patients’ care.39
Data Sharing Statement
Available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Ethical Committee of Watany Eye Hospitals (registration code COR-2020-004) and the Ethical Committee of the Federal University of São Paulo/UNIFESP/SP 2020 (registration code 4.050.934). Both Ethical Committees granted a waiver of informed consent owing to the study’s retrospective nature. Patients’ data were kept anonymous with utmost confidentiality.
Consent for Publication
All the material included in this paper can be published, and the person(s) providing consent has been shown the article contents to be published.
Acknowledgments
We want to thank the surgeons from the Watany Eye Hospitals (WEH), Cairo, Egypt, for sharing with a considerate number of patients enrolled in the study: Dr. Fathy Fawzy Morkos, MD, FRCS (Glasg.), FRCOphth, Chairman WEH, Professor of Ophthalmology, Egyptian Military Medical Academy, and Prof. Dr. Abdallah K. Hassouna, MD, Ph.D., Vice - Chairman WEH, Professor of ophthalmology - Ain Shams University.
Author Contributions
All authors have made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
None to be declared.
Disclosure
Prof. Dr. Renato Ambrósio reports personal fees from Oculus, Alcon, and Mediphacos, during the conduct of the study; personal fees from Oculus, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Sandoval HP, Donnenfeld ED, Kohnen T., et al. Modern laser in situ keratomileusis outcomes. J Cataract Refract Surg. 2016;42(8):1224–1234. doi:10.1016/j.jcrs.2016.07.012
2. Seiler T, Koufala K, Richter G. Iatrogenic keratectasia after laser in situ keratomileusis. J Refract Surg. 1998;14(3):312–317. doi:10.3928/1081-597X-19980501-15
3. Seiler T, Quurke AW. Iatrogenic keratectasia after LASIK in a case of forme fruste keratoconus. J Cataract Refract Surg. 1998;24(7):1007–1009. doi:10.1016/S0886-3350(98)80057-6
4. Binder PS, Lindstrom RL, Stulting RD, et al. Keratoconus and corneal ectasia after LASIK. J Cataract Refract Surg. 2005;31(11):2035–2038. doi:10.1016/j.jcrs.2005.12.002
5. Ambrósio JR, Randleman JB. Screening for Ectasia Risk: What are We Screening for and How Should We Screen for It? NJ: SLACK Incorporated Thorofare; 2013.
6. Ambrosio R Jr, Luz A, Lopes B, Ramos I, Belin MW. Enhanced ectasia screening: the need for advanced and objective data. J Refract Surg. 2014;30(3):151–152. doi:10.3928/1081597X-20140218-03
7. Randleman JB, Russell B, Ward MA, Thompson KP, Stulting RD. Risk factors and prognosis for corneal ectasia after LASIK. Ophthalmology. 2003;110(2):267–275. doi:10.1016/S0161-6420(02)01727-X
8. Santhiago MR, Giacomin NT, Smadja D, Bechara SJ. Ectasia risk factors in refractive surgery. Clinical Ophthalmol. 2016;10:713. doi:10.2147/OPTH.S51313
9. Pallikaris IG, Kymionis GD, Astyrakakis NI. Corneal ectasia induced by laser in situ keratomileusis. J Cataract Refract Surg. 2001;27(11):1796–1802. doi:10.1016/S0886-3350(01)01090-2
10. Spadea L, Cantera C, Cortes C, Conocchia NE, Stewart S. Corneal ectasia after myopic laser in situ keratomileusis: a long-term study. Clin Ophthalmol. 2012;6:1801–1813. doi:10.2147/OPTH.S37249
11. Rad AS, Jabbarvand M, Saifi N. Progressive keratectasia after laser in situ keratomileusis. J Refract Surg. 2004;20(5):S718–22. doi:10.3928/1081-597X-20040903-18
12. Moshirfar M, Smedley JG, Muthappan V, Jarsted A, Ostler EM. Rate of ectasia and incidence of irregular topography in patients with unidentified preoperative risk factors undergoing femtosecond laser-assisted LASIK. Clinical Ophthalmol. 2014;8:35.
13. Bohac M, Koncarevic M, Pasalic A, et al. Incidence and clinical characteristics of post LASIK Ectasia: a review of over 30,000 LASIK Cases. Semin Ophthalmol. 2018;33(7–8):869–877. doi:10.1080/08820538.2018.1539183
14. Randleman JB. Post-laser in-situ keratomileusis ectasia: current understanding and future directions. Curr Opin Ophthalmol. 2006;17(4):406–412. doi:10.1097/01.icu.0000233963.26628.f0
15. Moshirfar M, Tukan AN, Bundogji N, et al. Ectasia After Corneal Refractive Surgery: a Systematic Review. Ophthalmol Ther. 2021;10(4):753–776. doi:10.1007/s40123-021-00383-w
16. Gatinel D. Eye rubbing, a sine qua non for keratoconus. Int J Kerat Ect Cor Dis. 2016;5:6–12.
17. Roberts CJ, Dupps WJ Jr. Biomechanics of corneal ectasia and biomechanical treatments. J Cataract Refract Surg. 2014;40(6):991–998. doi:10.1016/j.jcrs.2014.04.013
18. Dawson DG, Randleman JB, Grossniklaus HE, et al. Corneal ectasia after excimer laser keratorefractive surgery: histopathology, ultrastructure, and pathophysiology. Ophthalmology. 2008;115(12):2181–91e1. doi:10.1016/j.ophtha.2008.06.008
19. Roy AS, Dupps WJ. Effects of altered corneal stiffness on native and postoperative LASIK corneal biomechanical behavior: a whole-eye finite element analysis. J Refract Surg. 2009;25(10):875–887. doi:10.3928/1081597X-20090917-09
20. Meghpara B. Keratectasia after laser in situ keratomileusis: a histopathologic and immunohistochemical study. Arch Ophthalmol. 2008;126(12):1655–1663. doi:10.1001/archophthalmol.2008.544
21. Ambrósio JR, Belin M. Enhanced screening for ectasia risk before laser vision correction. Int J Keratoconus Ectatic Corneal Dis. 2017;6(1):23–33. doi:10.5005/jp-journals-10025-1139
22. Ambrosio R Jr, Valbon BF, Faria-Correia F, Ramos I, Luz A. Scheimpflug imaging for laser refractive surgery. Curr Opin Ophthalmol. 2013;24(4):991–998. doi:10.1097/ICU.0b013e3283622a94
23. Belin MW, Ambrosio R. Scheimpflug imaging for keratoconus and ectatic disease. Indian J Ophthalmol. 2013;61(8):401–406. doi:10.4103/0301-4738.116059
24. Esporcatte DLPG,Salomao DMQ,Sena Jr JDNB Jr, Haddad J, Dawson DDG, Faria-Correia F. Multimodal Imaging in Refractive Surgery. Highlights Ophthalmol. 2020;48(4ESP):4–24. doi:10.5005/hoos-48-4-4
25. Klein SR, Epstein RJ, Randleman JB, Stulting RD. Corneal ectasia after laser in situ keratomileusis in patients without apparent preoperative risk factors. Cornea. 2006;25(4):388–403. doi:10.1097/01.ico.0000222479.68242.77
26. Binder PS. Analysis of ectasia after laser in situ keratomileusis: risk factors. J Cataract Refract Surg. 2007;33(9):1530–1538. doi:10.1016/j.jcrs.2007.04.043
27. Chen MC, Lee N, Bourla N, Hamilton RD. Corneal biomechanical measurements before and after laser in situ keratomileusis. J Cataract Refract Surg. 2008;34(11):1886–1891. doi:10.1016/j.jcrs.2008.06.035
28. Chan CC, Hodge C, Sutton G. External analysis of the Randleman Ectasia risk factor score system: a review of 36 cases of post-LASIK ectasia. Clin Exp Ophthalmol. 2010;38(4):335–340. doi:10.1111/j.1442-9071.2010.02251.x
29. Randleman JB, Trattler WB, Stulting RD. Validation of the Ectasia risk score system for preoperative laser in situ keratomileusis screening. Am J Ophthalmol. 2008;145(5):813–818. doi:10.1016/j.ajo.2007.12.033
30. Elhusseiny FY, Hamed AM, Sinjab MM, Salem TI, Elshahed AF. Ectasia risk score system and practical subjective scoring system in the screening of keratorefractive surgery candidates. Benha Med J. 2022;39(1):95–111.
31. Navarro Naranjo PI. Cumulative risk index (nice) as a diagnostic test based on corneal elevation tomography in the prevention of post-lasik corneal ectasia: Rosario University; 2016.
32. Klyce SD. The future of keratoconus screening with artificial intelligence. Ophthalmology. 2018;125(12):1872–1873. doi:10.1016/j.ophtha.2018.08.019
33. Ambrosio R, Lopes BT, Faria-Correia F, et al. Integration of Scheimpflug-based corneal tomography and biomechanical assessments for enhancing Ectasia detection. J Refract Surg. 2017;33(7):434–443. doi:10.3928/1081597X-20170426-02
34. Lopes BT, Ramos IC, Salomão MQ, et al. Enhanced tomographic assessment to detect corneal ectasia based on artificial intelligence. Am J Ophthalmol. 2018;195:223–232. doi:10.1016/j.ajo.2018.08.005
35. Ambrosio R Jr. Post-LASIK Ectasia: twenty Years of a Conundrum. Semin Ophthalmol. 2019;34(2):66–68. doi:10.1080/08820538.2019.1569075
36. Belin MW, Ambrosio R Jr. Corneal ectasia risk score: statistical validity and clinical relevance. J Refract Surg. 2010;26(4):238–240. doi:10.3928/1081597X-20100318-01
37. Yang K, Fan Q, Xu L, Gu Y, Pang C, Ren S. Accuracy of tomographic and biomechanical parameters in detecting unilateral post-LASIK keratoectasia and fellow eyes. Front Bioeng Biotechnol. 2023;11:1181117. doi:10.3389/fbioe.2023.1181117
38. McMonnies CW. The evidentiary significance of case reports: eye rubbing and keratoconus. Optom Vis Sci Offic Public Am J Optom Physiol Opt. 2008;85(4):262–269. doi:10.1097/OPX.0b013e318169287a
39. Esporcatte LPG, Salomao MQ, Lopes BT, et al. Biomechanical diagnostics of the cornea. Eye Vis. 2020;7(1):9. doi:10.1186/s40662-020-0174-x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.