Back to Journals » Patient Preference and Adherence » Volume 20
Assessment of Participant Satisfaction and Overall Experience: A Cross-Sectional Survey to Inform Trial Conduct
Authors Al-Maqbali JS, Al Alawi AM, Al-Zakwani I ![]() , Al Za'abi M
, Al Za'abi M ![]()
Received 16 December 2025
Accepted for publication 5 March 2026
Published 12 March 2026 Volume 2026:20 589554
DOI https://doi.org/10.2147/PPA.S589554
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Ramón Morillo-Verdugo
Juhaina Salim Al-Maqbali,1 Abdullah M Al Alawi,2 Ibrahim Al-Zakwani,1,3 Mohammed Al Za’abi1
1Department of Pharmacology and Clinical Pharmacy, College of Medicine and Health Sciences, Sultan Qaboos University, Muscat, Oman; 2Department of Medicine, Sultan Qaboos University Hospital, University Medical City, Muscat, Oman; 3Department of Pharmacy, Sultan Qaboos University Hospital, University Medical City, Muscat, Oman
Correspondence: Juhaina Salim Al-Maqbali, Sultan Qaboos University, Muscat, Oman, Tel +968-2414 4422, Email [email protected]
Purpose: This study assessed participants’ experience with their clinical trial and explored perceived health improvements to support quality improvement initiatives.
Patients and Methods: A cross-sectional survey was conducted among participants of a randomized, double-blind clinical trial on magnesium supplementation in type 2 diabetes. All participants were invited to complete a 25-item survey after providing informed consent. The survey covered general information, core trial experience (Five-Point-Likert-Scale), symptom improvement, overall satisfaction, and open-ended questions. The tool was bilingually developed, culturally adapted, and psychometrically tested for consistency and validity. Both quantitative and qualitative thematic analysis were performed.
Results: The survey demonstrated a high internal consistency (Cronbach’s alpha=0.93), and a strong construct validity characterized by a predominant unidimensional structure (Kaiser–Meyer–Olkin value=0.897). Of 227 contacted participants, 132 completed the survey (response rate: 58.15%). Satisfaction scores were consistently positive, especially for staff professionalism, respect for time, and informed consent clarity. Most respondents (75%) were willing to join future trials, and 87.88% would recommend participation. Over half reported symptom improvements, particularly in muscle cramps, energy, and sleep quality. No significant association was found between satisfaction and symptom improvement. Satisfaction was high across all educational levels. Open-ended responses emphasized staff professionalism, clear communication, and perceived health benefits as key factors to the overall reported satisfaction.
Conclusion: Respondents reported a consistently high satisfaction level, with perceived symptom improvements and strong willingness to future participation. This internally reliable and structurally valid survey captured meaningful feedback and may serve as a valuable quality improvement initiative to enhance patient engagement and optimize trial conduct, however, within the study’s limitations.
Keywords: participant satisfaction, clinical trials, survey, trial conduct, patient engagement, quality improvement
Introduction
Healthcare organizations that conduct clinical trials play vital roles in driving medical innovation and advancing evidence-based care. These institutions serve as key platforms for testing new therapies, diagnostics, and interventions that ultimately shape clinical practice. Clinical trials are widely acknowledged by healthcare professionals, policymakers, and the public as essential to improving current treatment options and discovering new ones for future patients. However, the success of these trials, centers not only on rigorous methodology but also on the active participation and satisfaction of trial participations.1,2 When patients have a positive trial experience, they are more likely to remain engaged, adhere to study protocols, and advocate for future participants. Therefore, enhancing patient experience is not only ethically important but also strategically critical to the validity and impact of clinical trials.3
Previous systematic reviews, suggest that clinical trial participation is generally safe and may even yield clinical benefits for some subgroup of patients, and no evidence of harm was found.1 As of 2024, over 480,000 clinical trials are registered globally,4 and the focus of clinical research has expanded from trial efficacy and safety to include the participant experience, recognized now as both a quality and ethical imperative.
Evidence suggests that satisfaction with clinical trial participations is shaped by several interconnected domains, including the quality of interaction with research staff, the service environment, trial design, personal motivations, trial logistics, and perceived health outcomes.4–8 Among these, positive and respectful interactions with research staff, characterized by professionalism, trust, and clear communication, are consistently cited as top drivers of satisfaction and willingness to recommend or rejoin future trials.2,4,8 High-quality service environments, efficient procedures, and organized facilities also enhance the trial experience.4,9 Although financial incentives are occasionally acknowledged, participants are more often motivated by the hope of personal health improvement, humanity, and the desire to contribute to scientific advancement.5,8,10 Furthermore, satisfaction was found to be improved with well-communicated informed consent, flexible scheduling, and minimal logistical burden.2,11 Conversely, dissatisfaction arises from unmet expectations, logistical challenges such as transportation, or family-related concerns.5,9 Additionally, to ensure reliability and validity of clinical trial experience surveys, it is essential that core domains undergo psychometric testing, including assessment of internal consistency.12,13
Despite growing international evidence, and some regional studies in GCC countries exploring knowledge and attitudes toward clinical trials,14 limited regional studies have systematically assessing participant satisfaction using validated and culturally adapted tools. Most regional research has focused on public perceptions rather than the lived experiences of enrolled trial participants. To address this gap, the present study aimed primarily to assess participant satisfaction and secondly to assess overall experience and perceived health benefits among individuals who had recently completed a randomized controlled trial (RCT), using a bilingual culturally adopted instrument aligned with global best practices and aiming to inform future trial methodology and quality improvement initiatives. Quantitative and qualitative components were added to the current study’s tool to allow a structured measurement of participant satisfaction levels and identification of patterns across domains and to provide a deeper insight into participants’ experiences, perceptions, and contextual factors that cannot be fully captured through structured survey items alone. By integrating both approaches, the study aims to generate a more comprehensive understanding of trial conduct and identify actionable areas for quality improvement.
Materials and Methods
Study Design and Population
A cross-sectional survey incorporating both quantitative and qualitative analytical approaches was conducted among all participants who were enrolled in the randomized, double-blind clinical trial titled “The Effect of Oral Magnesium Supplements on The Control and Outcomes of Type 2 Diabetes Mellitus: A Double-Blinded Randomized Control Trial” registered on 3rd July, 2023, under the ID number NCTO5774015.15 All individual who participated in the trial, regardless of the treatment arm allocation, were eligible and invited to voluntarily complete the satisfaction survey. Respondents included direct trial participants and, where applicable, caregivers or family members who were involved in the participant’s care or overall trial experience.
Summary of the Trial
It was a prospective, double-blind RCT (NCT05774015)15 evaluated the effect of oral magnesium on glycemic control, prognosis and metabolic outcomes in adults with T2DM. Recruited 247 participants who had HbA1c ≥7.0% and creatinine clearance >30 mL/min and were allocated to Mg-oxide (302 mg elemental Mg) or placebo, with biochemical assessments conducted at baseline and at 4-month intervals over 12 months. The median age was 58 years, 53% were female, and median diabetes duration was 16 years.
Survey Instrument Development
The participant satisfaction survey was developed to capture multiple dimensions of the clinical trial experience, guided by established frameworks for evaluating satisfaction in clinical research.2–4,9,16 The questionnaire was structured around five core domains that included: 1. service quality and staff interaction, evaluating professionalism, communication, and respect for participant time; 2. physical environment and operational efficiency, assessing the ease, safety, and timeliness of access to the trial site; 3. -trial procedures and participant experience, covering the clarity of informed consent, alignment between expectations and actual procedures, and overall process transparency; 4. health outcomes and perceived benefits, exploring perceived improvements in health, understanding of the illness, and contribution to scientific knowledge; and 5. motivations and willingness for future participation, addressing participants’ reasons for enrolling and their likelihood to recommend or rejoin future clinical studies.4,17–20 The domains were conceptualized as higher-order experiential constructs, each including closely related subcomponents reflecting different but complementary aspects of participant satisfaction.
The original questionnaire was developed in English by the team based on different satisfaction surveys frameworks. It was then translated into Arabic. To ensure accuracy and cultural relevance, the translated version underwent a number of adaptation steps. First it was reviewed by two bilingual clinical research experts, who performed the cultural adaptation into the Arabic version, and further evaluated the Arabic version and conducted the back-translation into English. Then, all revisions were incorporated to enhance clarity and ensure the appropriateness of the content for the target population.
Finaly, the initial survey questionnaire was pilot tested with a sample of 30 respondents to assess its clarity and relevance. Minor modifications in language were made accordingly, reaching the final version.
Survey Structure and Content
The survey instrument consisted of five sections, with a total of 25 main questions/items. 1. General information (3 items). Three domines were included in the quantitative analysis, assessing structured dimensions of participant satisfaction and preserved health outcomes. 2. Core domains of trial satisfaction (Five-Point Likert-scale with 15 items). 3. Additional health effects and symptom relief (2 items with multi-response options). 4. Overall satisfaction (2 items with multi-response options). The last domine was included in the qualitative analysis exploring participant experiences. 5. Open feedback (3 optional, open-ended questions). The survey combined a mix of multiple-choice, five-point Likert-scale questions (strongly disagree, disagree, neutral/neither agree nor disagree, agree, and strongly agree), symptom improvement checklist (not experienced before, no change, slight improvement, marked improvement), which were only positively worded items and did not require reverse scoring. Open-ended items were also included to provide participant freedom to add additional reflections. These elements align with recommended international frameworks to ensure reliability, relevance, and in generating meaningful insights into participants’ perspectives on clinical trial participation.
Informed Consent Statement
Providing consent was a required step before accessing and completing the survey. Participants informed consent included publication of anonymized responses/direct quotes.
Collection Procedure
Given that all participants enrolled in the original RCT were routinely connected via electronic messaging (WhatsApp Inc., founded in 2009, Menlo Park, California, USA) from the outset of the study, the survey was administered electronically using contact information obtained during the clinical trial. Responses were collected anonymously. The survey was distributed over a two-week period. A minimum response rate of 50% was targeted to ensure adequate representation of the trial population and to yield a meaningful and reliable results.21 Reminders were sent periodically to non-respondents to improve participation rate.
Data Analysis
To evaluate the internal consistency of the five-point Likert-scale with 15 items covering core domains of trial satisfaction, Cronbach’s alpha (α) was performed. This coefficient ranges from 0 to 1, with higher values reflecting greater internal consistency; values above 0.70 are generally considered acceptable, while values above 0.90 suggest excellent reliability.12,13 While construct validity was assessed using exploratory factor analysis (EFA) using principal factor extraction. Sampling adequacy was assessed using the Kaiser–Meyer–Olkin measure, A KMO value ≥0.60 was considered acceptable Items were considered to demonstrate adequate loading if factor loadings were ≥0.40 on their primary factor. Items with loadings <0.40 or with substantial cross-loading (≥0.40 on more than one factor) were evaluated for potential misfit. To assess unidimensionality, a one-factor solution was additionally examined and compared against the multidimensional model by evaluating eigenvalues and the proportion of total variance explained. Further, a mixed-methods analytical approach was performed, integrating both quantitative and qualitative data.
Quantitative Analysis
A priori two-tailed level of significance was set at the 0.05 level. Data analysis was conducted using STATA version 16.1 (StataCorp, College Station, TX, USA).
Descriptive statistics were used to summarize demographic variables. Frequencies, and percentages were calculated for all Likert-scale and multiple-choice questions. Inferential bivariate statistics were performed to assess the associations between categorical groups using Chi-square test or Fisher’s exact test when expected event rate was lower than 5.
Qualitative Analysis
The three open-ended questions were examined using manual thematic content analysis inspired by the Braun and Clarke’s six-step thematic analysis approach.22 Responses by respondents were coded, and codes that shared common meanings or patterns were grouped together to form key themes and further categorized under three primary sections. Representative quotes were selected to illustrate major themes and provide depth to the quantitative findings.
Results
Internal Consistency and Construct Validity
The overall internal consistency calculated by Cronbach’s alpha was excellent (α=0.93), indicating strong reliability across the full set. Domain-specific analysis also demonstrated good internal consistency: staff interaction and communication (α=0.85), physical environment and operations (α=0.79), trial procedure and experience (α=0.83), health outcomes and perceived benefits (α=0.83), and motivations and willingness for future participation (α=0.84). All domain scores exceeded the acceptable threshold of 0.70, supporting the reliability of the instrument in capturing respondents’ perceptions across core dimensions of the clinical trial satisfaction (Supplementary Tables).
Sampling adequacy for EFA was excellent, with an overall KMO value of 0.89. The likelihood ratio test comparing the independent and saturated models was statistically significant (χ2(105) = 1657.09, p < 0.001), indicating that the correlation matrix was appropriate for factor analysis. Initial eigenvalue inspection demonstrated a dominant first factor (eigenvalue = 8.41) accounting for 79.17% of the total variance, while subsequent eigenvalues were below 1.0. Suggesting the presence of a strong general satisfaction dimension underlying the instrument. A five-factor solution showed that all items demonstrated adequate factor loadings (≥0.40), with no items exhibiting substantial cross-loading or misfit. Communalities were acceptable across all items, supporting adequate shared variance within the factor structure (Supplementary Tables).
General Demographics
Out of 227 participants contacted, 132 completed the survey, yielding a response rate of 58.15%, which exceeded the target threshold of 50%.
As shown in Table 1, out of a total of 132 respondents, the majority (84.85%) were patients themselves, while 15.15% were relatives on behalf of patients. The relatives who completed the questionnaire were primary caregivers directly involved in the participants’ care and were present during trial counseling and follow-up from the beginning of the study. Among the 18 respondents who were not patients themselves, 61.11% responded for their mothers (n = 11), 33.33% responded for their fathers (n = 6), and only one responded for their wife. The educational background varied, with 15.15% being illiterate (n = 20), 21.21% having less than high school education (n = 28), 31.06% being high school graduates (n = 41), 21.97% having completed university degrees (n = 29), and 10.61% holding higher degrees (n = 14).
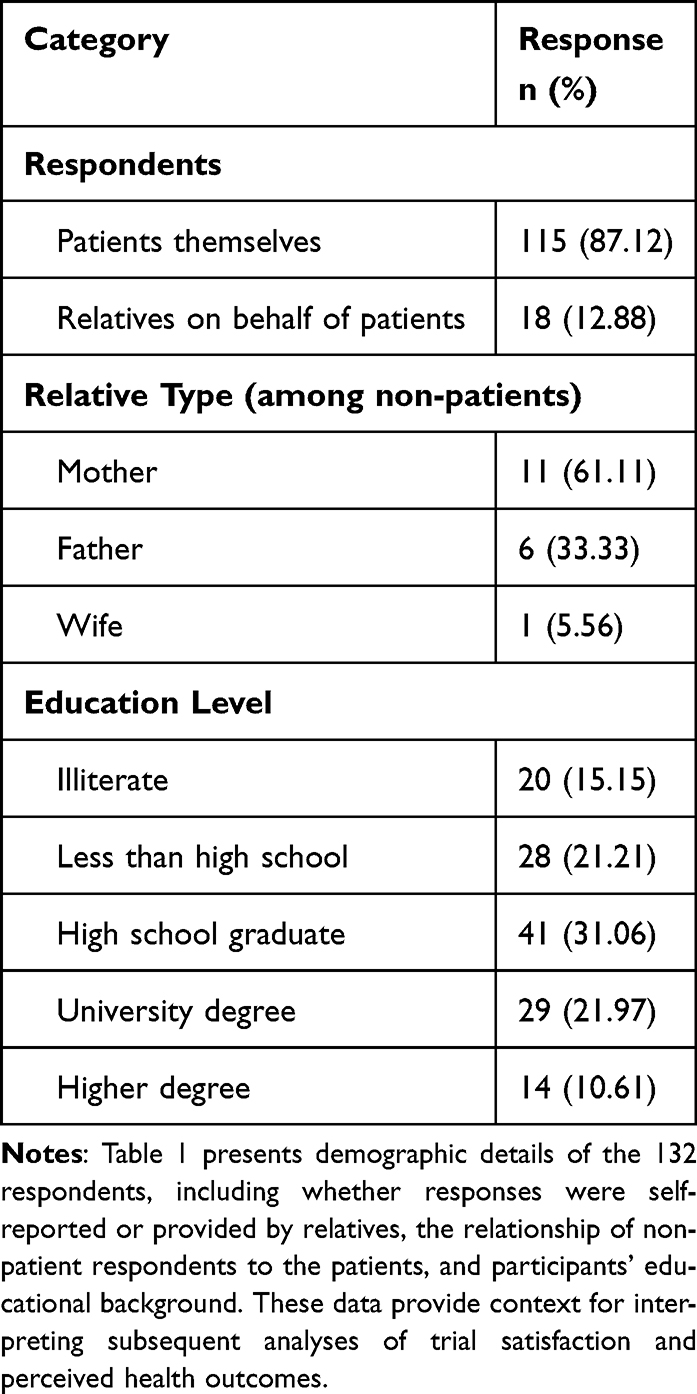 |
Table 1 Participant Demographics: Respondents, Relationship of Respondents, and Educational Background (n = 132) |
Quantitative Outcomes Participant Satisfaction
Table 2 presents participants’ responses to the clinical trial satisfaction assessed by the Five-point Likert scale with 15 items. Overall, responses indicated a high level of satisfaction, with most respondents selecting either “agree” or “strongly agree” for nearly all survey items. Across all items, neutral, disagree, and strongly disagree responses were rare, generally totaling less than 5–7% per item, which further emphasizes the consistently positive satisfaction reported by the respondents.
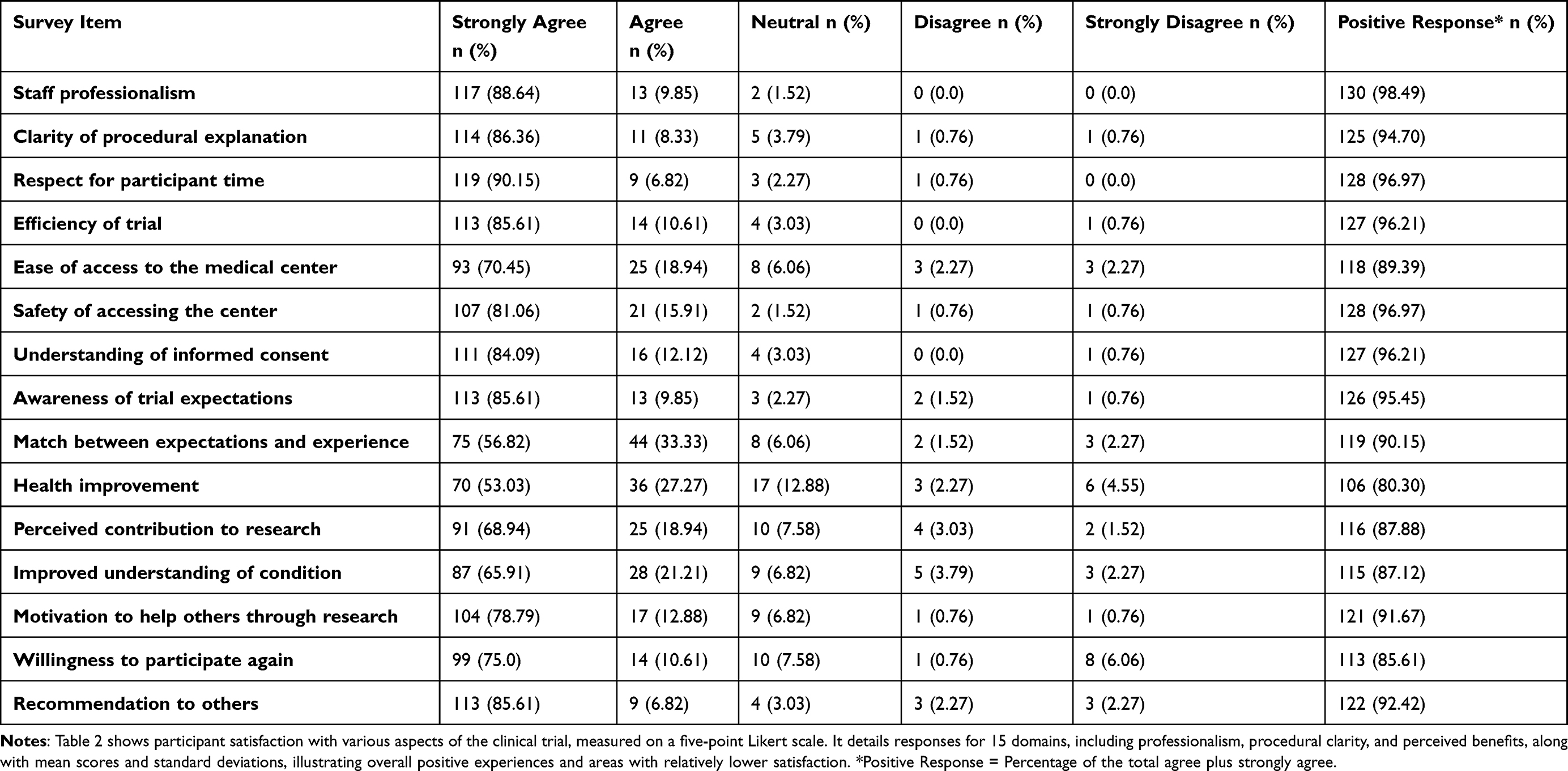 |
Table 2 Participant Satisfaction with Clinical Trial Experience Based on Five-Point Likert-Scale Responses (1 = Strongly Disagree to 5 = Strongly Agree) (n = 132) |
The highest-rated item was “staff professionalism”, with 98.5% of respondents indicating a positive response (88.64% strongly agree and 9.85% agree). Similarly, “respect for participant time” demonstrated a 96.97% positive response, with 90.15% strongly agreeing. Responses to other domains also reflected strong satisfaction. For instance, “willingness to participate again in clinical trials” showed an 85.61% positive response (75.00% strongly agree and 10.61% agree) “Safety of accessing the center” demonstrated a 96.97% positive response (81.06% strongly agree and 15.91% agree). Also, “understanding of informed consent” and awareness of trial expectations were highly rated, with positive response of 96.21% and 95.45%, respectively. Motivational factors were also prominent, with “motivation to help others through research” (positive response = 91.67%) and “recommendation to others” (positive response = 92.42% both showing high levels of endorsement, where over 85% strongly agreed in each (Table 2).
While most items showed uniformly strong positive responses, a few showed variations in response. For example, “health improvement (changes in my health status)” had the lowest proportion of positive responses, with 80.30% indicating agreement (53.03% strongly agree and 27.27% agree) e), while 12.88% selected a neutral response and 6.82% reported disagreement. Additionally, “match between expectations and experience” demonstrated a 90.15% positive response (56.82% strongly agree and 33.33% agree), however this item had a slightly higher proportion of neutral or negative responses compared to other items (Table 2).
Perceived Health Benefits
Table 3 shows the response of the respondents when they were asked to assess perceived changes in a set of common symptoms experienced during or after the clinical trial. The findings suggest that participation in the trial was associated with perceived improvements in a range of physical and neurological symptoms, especially among those who were symptomatic at baseline. Overall, a substantial proportion of respondents reported improvements across multiple symptom domains. Muscle cramps or spasms showed improvement in 57.6% of respondents, with 40.9% reporting slight and 16.7% marked improvement, while 28% had not experienced such symptoms. Similarly, 51.5% of respondents reported improvement in neuropathic symptoms, and 34.9% had not previously experienced them. Constipation improved in 55.3% of respondents, with similar proportions reporting slight (27.3%) and marked (28.0%) improvement. Sleep quality improved in 57.6% of respondents, although 27.3% had no prior sleep issues. Over half of respondents (53.0%) had not experienced headaches, and 34.8% of those who had reported some level of improvement. Energy levels improved in 57.6% of respondents, while 44% reported better mood or reduced anxiety symptoms. Improvements in joint-related pain were noted in 52.3% of respondents.
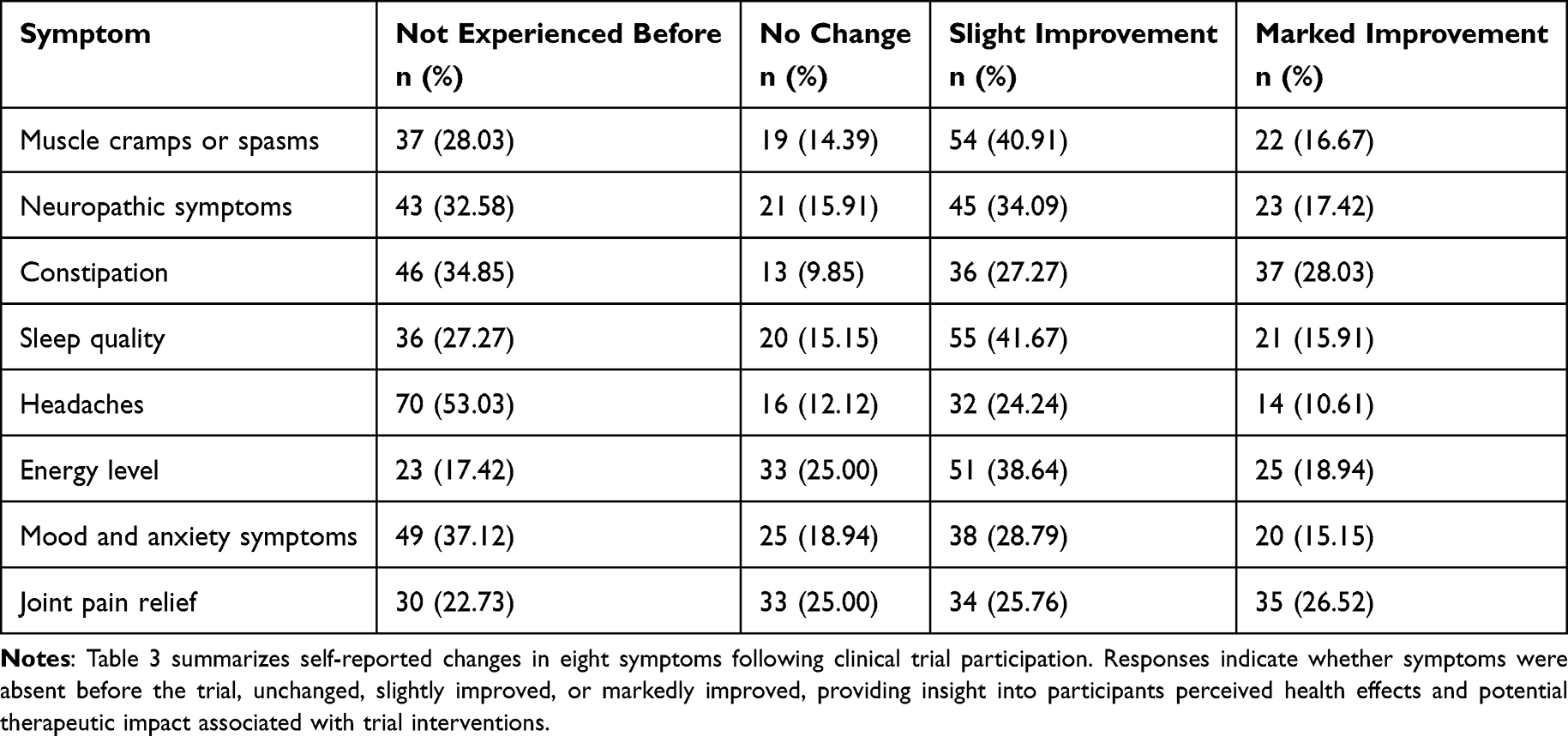 |
Table 3 Self-Reported Changes in Symptoms Following Clinical Trial Participation (n = 132) |
Overall Satisfaction
In the overall satisfaction section, respondents reported high levels of positive experience with the clinical trial. When asked about their overall satisfaction, 75.76% indicated they were very satisfied, 21.97% were satisfied, and only 2.27% selected a neutral response; notably, no respondents reported being dissatisfied or very dissatisfied. Moreover, when asked whether they would recommend participation in a clinical trial to others, 87.88% responded “yes,” 11.36% were “not sure,” and only 0.76% answered “no.”
Additionally, overall satisfaction was consistently high across all educational levels, with no statistically significant differences observed (p=0.613). Respondents across all levels of education, predominantly rated their experience as “very satisfied.”
Most respondents who reported improvement (scores either slight improvement or marked improvement) across all symptoms were more likely to rate their overall experience as very satisfied. For instance, 54/54 respondents with slight improvement in muscle cramps, 55/55 who reported slight improvement in sleep and 38/38 with slight mood improvement, and 51/51 with slight energy level improvement rated their experience as very satisfying. Although these associations suggest that there is a positive alignment between perceived health improvement and satisfaction level, statistical analysis showed no statistically significant associations (p>0.05).
Qualitative Outcome (Participants’ Experience)
A thematic analysis of the open-ended survey responses revealed six prominent themes to explore participants’ experience. Many respondents highlighted “1-ethical and respectful care”, “2-empowerment and participation”, and “3-smoothness of the process”. Although majority of respondents reported no challenges, few reported “4-some logistical concerns”, and others suggested “5-calls for broader testing”, and “6-sustainability and access to the trial program”. Finally, the six initial themes were further categorized into three primary sections; positive experiences, challenges encountered, and recommendations for improvement.
In terms of positive aspects of trial participation “What did you like most about participating in this clinical trial?”, respondents frequently praised the professionalism, kindness, and continuous support from the research team. Many appreciated the clear communication, respectful treatment, and the sense of contribution to scientific knowledge as well as helping others. Others highlighted the perceived health improvements, especially better blood sugar control and increased awareness of magnesium’s role in health. Several respondents found the experience to be emotionally uplifting, noting positive energy, improved motivation, and trust in the care team. Examples of responses include; “The investigator was very kind and genuinely cared about my health.”, “The research team was cooperative, clear, and kind in communication, and explained the purpose and importance of the study well.”, “I became more aware of health and nutrition.”, “Participating in the trial benefited me greatly.”, and “I felt proud to contribute to research that may help develop a more effective treatment.”.
While for challenges reported “what challenges or concerns did you encounter during the trial?”, most respondents reported no significant challenges. However, among the few who did, common concerns included logistical issues, such as transportation difficulties, long distances to the study site, and parking availability. A few respondents mentioned timing of medication intake, missed laboratory tests, or lack of continuity after the trial, particularly when a treatment had proven effective for them. Examples of responses include “parking at the university was a challenge.”, “The distance from my residence to the study site was a barrier.”, “I was anxious about forgetting to take the medication every day.”, and “Unfortunately, after the medication was discontinued, complications reappeared.”
Lastly, suggestions for improvement “do you have suggestions for improving the clinical trial experience?”, respondents suggested offering follow-up care or continued access to effective interventions, increasing recruitments across regions, and providing more frequent testing and updates. A few proposed using digital tools, such as glucose sensors, for better data collection. Others emphasized the importance of participant education, group support sessions, and even material recognition to encourage future participation. Examples of responses include; “I suggest that tests required for the research be done in the dedicated clinic for the research.”, “If the results are positive, I hope to continue being part of the program.”, “Sample selection should reflect regional diversity, with follow-up by local teams.”, and “Using big data could yield better insights and predictions.”.
Discussion
This survey-based evaluation provides important insights into participants’ satisfaction, perceived health benefits and overall experience following participation in a randomized, double-blind clinical trial by incorporating both quantitative and qualitative analytical approaches. The findings revealed consistently positive satisfaction across all key domains, including research staff professionalism, respectful communication, accessibility, trial logistics, and perceived health improvement. Additionally, there were few challenges that were reported mainly involving logistical burdens. The psychometric evaluation demonstrated that the survey instrument possesses strong internal consistency and robust construct validity. The tool consistently assesses distinct satisfaction domains without duplication, while reflecting a strong general satisfaction construct reinforced by meaningful domain-level clustering.
The overall satisfaction level among respondents aligns with a growing body of literature emphasizing the value of patient-centered approaches in clinical research. Prior umbrella review of six systematic reviews from 292 RCTs, by Bouzalmate-Hajjaj et al (2022) reported that 18.7% of comparisons favored trial participation and reported significantly better outcomes, while 71.7% showed no difference and only 9.5% favored non-participation, with no evidence of harm noted, which potentially attributed to enhanced monitoring, structured care, and closer follow-up embedded in trial designs.1 Similarly, Tantoy et al (2021) found that satisfaction in clinical trials is often driven by huminitic motivations, positive research-patient interactions, and perceived benefits. These findings support the importance of professionalism, informed communication, and time respect domains included in our survey, which were all rated highly by the respondents.2 Our findings also align with those of Lee et al (2024), who demonstrated that respondents’ perceptions of service quality, including; interaction quality, environment, and operational efficiency, strongly predict overall satisfaction and respondents retention.4
Notably, the results confirm that high satisfaction was not solely driven by clinical outcomes but is also shaped by interpersonal factors. Respondents in this survey cited clear communication, and collaboration with the research team, which may be contributors to their positive experience. These themes echo observations by Jeon et al (2019), Paidipati et al (2023), and Adler et al (2020), who identified trust and supportive interactions as essential for satisfaction and future trial engagement.6,8,23
Respondent motivation remains another vital determinant of satisfaction. Several studies indicated that individuals often join trials for personal health improvement, to help others, or to contribute to science, rather than for financial gain.8,24 In our cohort, perceived health benefits were common, particularly improvements in energy, mood, and symptom relief. Although descriptive alignment was observed with the overall satisfaction levels, satisfaction scores demonstrated limited variability, which may have reduced the ability to detect statistical associations. Additionally, satisfaction appears to be multidimensional and may be more strongly influenced by interpersonal and procedural aspects of trial conduct than by perceived symptom improvement alone. Further, they reinforced the idea that personal benefit and meaningful contribution are powerful motivators as evidenced from literature.1,4,5 Yet, these findings should be interpreted with caution, as symptom-related responses reflect subjective perceptions rather than objectively measured outcomes. No baseline-adjusted analyses or comparator-group evaluations were conducted within this survey component, and therefore these findings must not be interpreted as evidence of treatment effect. Psychological and emotional benefits, such as increased self-awareness, empowerment, and pride in contributing to science, were also frequently expressed in open-ended responses. This supports earlier findings that participation often brings emotional rewards beyond physical health outcomes.8,25 These perceived gains may positively influence health behaviors, especially in chronic conditions like diabetes, where self-management is key factor for better health outcomes.
On the other hand, respondents valued logistical ease, environmental comfort, and procedural clarity. Prior studies indicate that heavy trial procedures often lower satisfaction and increase dropouts.9 Equally, satisfaction improves when trial designs incorporate flexible scheduling, efficient consent processes, and ongoing respondent support.11,26 This is reflected in our study’s high satisfaction ratings in domains related to procedural efficiency and informed consent clarity.
Despite the high satisfaction levels, the study also highlighted areas for improvement. A small subgroup of respondents cited logistical burdens as major barriers, including travel distance, parking, and scheduling follow-up appointments. Such concerns, which have been reported across multiple studies, represent a persistent challenge to enrolment in clinical trial.9,16 In our study, respondents who experienced a mismatch between expectations and actual outcomes, such as post-trial medication discontinuation due to protocol obligations, also expressed concern, aligning with findings from other studies.5,27 These feedbacks highlight the importance logistical flexibility, improved expectation management, and strategies to ensure continuity of care or access to effective interventions when ethically and practically feasible.4,10
This study emphasizes that clinical trial satisfaction is a multidimensional construct shaped by interpersonal, logistical, and outcome-related factors. The high response rate and use of a culturally adapted instrument further strengthen the credibility of these findings. This evaluation adds meaningful evidence to support the integration of patient-reported satisfaction tools into clinical trial processes, not only as a measure of respondent engagement but also as a vehicle for improving trial delivery and institutional quality assurance. Future trials should continue to prioritize patient-centered design, incorporate structured satisfaction assessments, address logistical barriers, and strengthen post-trial continuity of care to enhance participant trust and sustained engagement. Embedding culturally adapted, psychometrically evaluated satisfaction tools within trial protocols may serve not only as a measure of participant satisfaction but also as a mechanism for continuous quality improvement and institutional accountability. The high response rate and use of a validated bilingual instrument further support the credibility of these findings and their relevance to optimizing future trial delivery.
While this study has notable strengths, several limitations must be acknowledged. First, the potential for response bias. Participants who had more favorable experiences may have been more inclined to complete the survey, whereas those who were dissatisfied or less engaged may have been less likely to respond. This possibility, combined with the restriction to trial completers, may have contributed to the consistently high satisfaction scores observed across domains. Second, respondent motivators for trial participation were not systematically captured through specific open-ended questions or structured multiple-choice items, limiting the ability to analyze underlying reasons for engagement. Third, while the survey instrument was culturally adapted and demonstrated internal consistency, further testing in other settings is needed to establish broader applicability and cross-trial comparability. Fourth, although the survey was conducted electronically and included open-ended response options with full fairness and accessibility, it may still lack the depth that could be captured through more interactive qualitative methods such as interviews or focus groups and missed opportunities to inform the co-design of future trials. Also, it may be associated with digital access bias. Fifth, a small proportion of surveys were completed by relatives acting, and they may introduce some variability in perceived satisfaction. Lastly, the findings may not be generalizable to other populations beyond adults with T2DM. Furthermore, due to sample size and scope of the study it was not possible to perform in depth validation analysis for Likert-scale items such as Rasch modeling and Andrich thresholds.
Conclusion
The survey demonstrated excellent reliability and strong construct validity, supporting a robust underlying satisfaction construct with complementary multidomain structure. By integrating quantitative findings with qualitative insights that provided contextual depth, the study offers a comprehensive understanding of participant experience. Overall, respondents reported consistently high levels of satisfaction across all assessed domains, along with perceived improvements in common symptoms and a strong willingness to participate in future clinical trials. These findings highlight the value of incorporating structured satisfaction assessments into clinical research to inform trial conduct and guide quality improvement initiatives aimed at enhancing patient engagement. Nonetheless, continued efforts to address logistical challenges and strengthen post-trial follow-up remain important. Further validation of the instrument in different geographic and clinical settings is warranted to confirm its broader applicability beyond this specific trial setting.
Abbreviations
RCT, Randomized Controlled Trial; SD, Standard Deviation; MREC, Medical and Research Ethics Committee; STATA, Stata Statistical Software; NCT, National Clinical Trial (as part of clinicaltrials.gov ID); α (Alpha), Cronbach’s Alpha (used for internal consistency/reliability).
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Ethical approval for this study was granted by the Medical and Research Ethics Committee at the College of Medicine and Health Sciences, Sultan Qaboos University, Muscat, Oman (MREC #2951; dated 22 February 2023), in accordance with the Declaration of Helsinki. Providing consent was a required step before accessing and completing the survey. Informed consent to participate was obtained from all patients prior to their involvement in the study.
Consent for Publication
The content of this manuscript has not been previously published or submitted for publication elsewhere. All authors have reviewed the final version and have made substantial intellectual contributions to its preparation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Ministry of Higher Education, Research and Innovation through the Block Funding Program (Grant No. RC/RG-MED/PHAR/23/01), approval date; 1st November 2022.
Disclosure
The authors declare that there are no conflicts of interest associated with this work.
References
1. Bouzalmate-Hajjaj A, Guijarro M, Khan K, Bueno-Cavanillas A, Cano-Ibáñez N. Benefits of participation in clinical trials: an umbrella review. Int J Environ Res Public Health. 2022;19:15368. doi:10.3390/ijerph192215368
2. Tantoy I, Bright A, Paelmo E, et al. Patient satisfaction while enrolled in clinical trials: a literature review. Patient Exp. J. 2021;8:125–12. doi:10.35680/2372-0247.1509
3. Manton K, Gauld C, White K, Griffin P, Elliott S. Qualitative study investigating the underlying motivations of healthy participants in Phase I clinical trials. BMJ Open. 2019;9:e024224. doi:10.1136/bmjopen-2018-024224
4. Lee GE, Kim S, Chu SH, Seok JH, Kim SY, Kim S. Improving patient satisfaction based on service quality in clinical trials: a cross-sectional study. PLoS One. 2024;19(12):e0313340. doi:10.1371/journal.pone.0313340
5. Kozakiewicz A, Mazur J, Szkultecka-Dębek M, Białorudzki M, Izdebski Z. Public perception of clinical trials and its predictors among polish adults. J Clin Med. 2025;15:14. doi:10.3390/jcm15010014
6. Adler P, Otado J, Kwagyan J. Satisfaction and perceptions of research participants in clinical and translational studies: an urban multi-institution with CTSA. J Clin Transl Sci. 2020;4:317–322. doi:10.1017/cts.2020.20
7. Cummings M, Pradhan S, Madhavan S. Understanding factors contributing to participant satisfaction in stroke walking recovery clinical trials. Contemp. Clin. Trials Commun. 2022;28.
8. Paidipati C, Foxwell A, Mooney-Doyle K, Tiller D, Pinto-Martin J, Ulrich C. Caregiver perspectives on the benefits, burdens, and moral distress of participation in cancer clinical trials. J Fam Nurs. 2022;29:89–98. doi:10.1177/10748407221098187
9. Xiao S, Androulakis A, Skelton W, et al. Assessing compliance and satisfaction among participants in clinical trials on traditional chinese medicine. Open Access J. Clin. Trials. 2024;Volume 16:23–39. doi:10.2147/OAJCT.S456933
10. Fisher J, McManus L, Wood M, et al. Healthy Volunteers’ Perceptions of the Benefits of Their Participation in Phase I Clinical Trials. J Empir Res Hum Res Ethics. 2018;13:494–510. doi:10.1177/1556264618804962
11. Gouveia R, Cruz V, Almeida L. Sociodemographic and psychological characteristics influencing patients’ willingness to participate in clinical trials. BMJ Open Quality. 2022;11.
12. Amirrudin M, Nasution K, Supahar S. Effect of variability on cronbach alpha reliability in research practice. Jurnal Matematika, Statistika dan Komputasi. 2020;17:223–230.
13. Edelsbrunner P, Simonsmeier B, Schneider M. The cronbach’s alpha of domain-specific knowledge tests before and after learning: a meta-analysis of published studies. Educ Psychol Rev. 2025;37. doi:10.1007/s10648-024-09982-y
14. Al-Rawashdeh N, Damsees R, Al-Jeraisy M, Al Qasim E, Deeb AM. Knowledge of and attitudes toward clinical trials in Saudi Arabia: a cross-sectional study. BMJ Open. 2019;9(10):e031305. doi:10.1136/bmjopen-2019-031305
15. USNLo M. Effect of oral magnesium supplementation on type ii diabetes mellitus guided by serum ionized magnesium level 2023. Available from: https://clinicaltrials.gov/study/NCT05774015.
16. Escritt K, Mann M, Nelson A, Harrop E. Hope and meaning-making in Phase 1 oncology trials: a systematic review and thematic synthesis of qualitative evidence on patient-participant experiences. Trials. 2022;23(1):409. doi:10.1186/s13063-022-06306-9
17. Doyle C, Lennox L, Bell D. A systematic review of evidence on the links between patient experience and clinical safety and effectiveness. BMJ Open. 2013;3(1):e001570. doi:10.1136/bmjopen-2012-001570
18. Pflugeisen BM, Rebar S, Reedy A, Pierce R, Amoroso PJ. Assessment of clinical trial participant patient satisfaction: a call to action. Trials. 2016;17(1):483. doi:10.1186/s13063-016-1616-6
19. Kraft SA, Cho MK, Gillespie K, et al. Beyond consent: building trusting relationships with diverse populations in precision medicine research. Am J Bioeth. 2018;18(4):3–20. doi:10.1080/15265161.2018.1431322
20. Kim M, Oh Y, Lee JY, Lee E. Job satisfaction and moral distress of nurses working as physician assistants: focusing on moderating role of moral distress in effects of professional identity and work environment on job satisfaction. BMC Nursing. 2023;22(1):267. doi:10.1186/s12912-023-01427-1
21. Karakaya S, Alparslan Z. Sample size in reliability studies: a practical guide based on cronbach’s alpha. Psychiatry Behav Sci. 2022;12:150. doi:10.5455/PBS.20220127074618
22. Cernasev A, Axon D. Research and scholarly methods: thematic analysis. J Am Coll Clin Pharm. 2023;6:751–755. doi:10.1002/jac5.1817
23. Jeon J, Kim JH, Kim K. Perception and satisfaction of cancer patients in clinical trials. Ann Oncol. 2019;30:ix182. doi:10.1093/annonc/mdz423.001
24. Rosser JI, Njoroge B, Huchko MJ. Changing knowledge, attitudes, and behaviors regarding cervical cancer screening: the effects of an educational intervention in rural Kenya. Patient Educ Couns. 2015;98(7):884–889. doi:10.1016/j.pec.2015.03.017
25. Jiang S, Velasquez-Garcia H. The role of education in colorectal cancer screening participation: updated evidence from Canadian Community Health Survey (2011–2012). Cancer Treat Res Commun. 2017;10:1–5. doi:10.1016/j.ctarc.2016.10.001
26. Voss T, Li J, Cummings J, et al. Randomized, controlled, proof-of-concept trial of MK-7622 in Alzheimer’s disease. Alzheimers Dement. 2018;(4):173–181.
27. Squires KE, Feinberg J, Bridge DA, et al. Insights on GRACE (Gender, Race, And Clinical Experience) from the patient’s perspective: GRACE participant survey. AIDS Patient Care and STDs. 2013;27(6):352–362. doi:10.1089/apc.2013.0015
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.