")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Assessment of Occipital Involvement Among a Large Population of Females with Pattern Hair Loss in Saudi Arabia
Authors Zari S
Received 11 June 2023
Accepted for publication 16 September 2023
Published 27 September 2023 Volume 2023:16 Pages 2687—2696
DOI https://doi.org/10.2147/CCID.S422283
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Shadi Zari
Department of Dermatology, College of Medicine, University of Jeddah, Jeddah, Saudi Arabia
Correspondence: Shadi Zari, Department of Dermatology, College of Medicine, University of Jeddah, Jeddah, Saudi Arabia, Email [email protected]
Background: Cumulative evidence suggests the involvement of the occipital region in female pattern hair loss (FPHL). However, most of the studies that have been published so far concerned relatively small samples of patients.
Purpose: To assess the occipital involvement in FPHL and analyze its correlation with disease severity among a large sample of patients.
Patients and Methods: A retrospective study involved 1000 adult women with FPHL, between January 2020 and August 2022. Occipital involvement was defined as more than 10% of thin hairs (< 0.03 mm). Baseline trichometry parameters in the frontal and occipital regions were analyzed.
Results: Occipital involvement was observed in 32.4% of the patients. Positive correlations between frontal and occipital regions were observed for all trichometry parameters; the strongest concerned average hair shaft thickness (Pearson’s coefficient r=0.708), cumulative hair thickness (r=0.673), and trichometry-derived Sinclair scale (r=0.656). The risk of occipital involvement increased independently with the disease severity in frontal region; however, the disease progression was slower in the occipital compared to frontal region.
Conclusion: One-third of females in our study with FPHL had occipital involvement. This has a major impact on the methods used to diagnose pattern hair loss in females and their treatment plan including hair restoration surgery.
Plain Language Summary: This study provides the largest evidence of occipital involvement in females with pattern hair loss among one-third of the study patients.This has a major clinical implication in the diagnosis of pattern hair loss in females when the occipital region is used as a normal reference, besides limiting hair transplantation as a treatment option.
Keywords: pattern hair loss, female androgenetic alopecia, occipital donor area, donor area, donor supply
Introduction
Female pattern hair loss (FPHL), also termed female androgenetic alopecia, is a highly prevalent hair loss condition characterized by progressive hair follicle miniaturization leading to hair thinning and shedding.1,2 The scalp distribution of the hair thinning follows characteristic patterns such as Ludwig’s type affecting the crown region,3 “Christmas tree” pattern mostly affecting the frontal region,4 and Hamilton type affecting the temporal regions.5
Pathogenically, FPHL differs from male pattern hair loss in that it is less associated with androgen metabolism alteration. Instead, female patients with pattern hair loss have increased sensitivity to normal androgen levels.6,7 This results in differential features between male and female pattern hair loss. Among these specificities is the involvement of the occipital region, which was previously demonstrated to concern a significant percentage (25%) of afflicted women.8 Clinical observations supported by trichometric analysis evidenced significant reductions in hair density, hair diameter, and terminal-to-vellus hair ratio in the occipital region among women with FPHL compared to healthy controls. These findings were more remarkable in advanced stages of the disease, such as in stage Ludwig II.9,10 This has significant implications notably because it impacts the donor area, which compromises the success of hair transplant surgeries.11–13
However, most of the studies that have been published so far concerned relatively small samples of patients. Furthermore, since the prevalence of FPHL differs across ethnic groups,14 it can be hypothesized that the levels and patterns of occipital involvement may also differ with ethnicity. Therefore, it is interesting to investigate the occipital involvement in different ethnic groups.
To address this issue, the present study was designed to explore the occipital involvement in FPHL among a large sample of Saudi women by comparing levels of trichometry parameters in frontal and occipital regions in females with different levels of FPHL severity. Such data have implications in deciding the best course of action in the management of patients who are candidates for hair transplantation, besides other implications in the diagnosis and assessment of patients.
Materials and Methods
Design
A retrospective chart review was carried out at the author’s hair clinic in Jeddah, Saudi Arabia. The ethical approval was obtained from the Bioethics Committee of Scientific & Medical Research of the University of Jeddah (UJ-REC-122). The study was carried out in compliance with the Declaration of Helsinki.
Population
The study involved adult women who attended the clinic for the assessment or management of FPHL between January 2020 and August 2022. Both patients who have never been treated before (untreated group) and those with treatment failure (failed treatment group) have been included. Treatment failure was defined as patients who presented to the clinic and expressed dissatisfaction with the outcomes of the previous treatment they had received. In addition, patients who underwent hair transplantation were excluded.
Trichometric Examination
In this study, trichometry parameters of participants were determined from trichoscopic images captured using a Medicam 800 computerized video dermatoscope (FotoFinder Systems GmbH, Bad Birnbach, Germany), in conjunction with TrichoScan digital image analysis (TrichoScan, Tricolog GmbH, Freiburg, Germany). For each participant, an image was acquired at a 20x magnification and four additional images at a 70x magnification from both the frontal midline and occipital midline regions. This standardized image acquisition protocol ensured consistent and reliable measurements of trichometry parameters throughout the study population.
Diagnostic Criteria for Female Pattern Hair Loss
The diagnosis of FPHL, involving the frontal area, was established based on trichometry parameters, in compliance with the criteria proposed by Rakowska et al.15
Definition of Occipital Involvement
Occipital involvement was defined as more than 10% of thin hairs (below 0.03 mm), which reflects hair miniaturization.
Data Collection
A pre-formatted Excel data sheet was used to collect the following data: patient’s age; treatment status (never treated vs post-treatment failure); FPHL severity level indicated by trichoscopy-derived Sinclair scale (TDSS) in the frontal region divided into four classes (mild [TDSS<2.00], moderate [2.00–2.99], severe [3.00–3.99], and extremely severe [≥4.00]); baseline trichometry parameters by scalp region including hair density (N/cm2), average hair shaft thickness (AHST, μm), percentage of thin, medium, and thick hair, cumulative hair thickness (CHT, mm/cm2); number of follicular units (%); and percentage of single, double, and triple follicular units.
Statistical Methods
Data were cleaned and analyzed using SPSS version 21.0 for Windows (SPSS Inc., Chicago, IL, USA); duplicates were removed, outliers were corrected, and observations with significant data missing were excluded. Frequencies and percentages were used to present categorical variables, while means ± standard deviations (SD) were used to summarize continuous variables. The prevalence of occipital involvement was estimated as the percentage of patients who had more than 10% of thin hairs (below 0.03 mm), with 95% confidence interval (95% CI). Baseline data were compared between untreated group and those who were in treatment failure; independent t-test was used to compare age and chi-square was used to compare FPHL severity and occipital involvement.
Pearson’s correlation was used to analyze the correlation between frontal and occipital regions regarding the different trichometry parameters; results are presented in scatter plots with the fit line, as well as the value of Pearson’s correlation coefficient (r).
Independent t-test was used to analyze the variance of the different trichometry parameters between patients with occipital involvement and those without, with calculation of the effect size using Cohen’s D coefficient. Parameters showing both statistical significance and clinical significance (large effect size) were considered key parameters to indicate occipital involvement.
The population was divided by level of severity into three groups including mild, moderate, and severe+ FPHL. Within each group, paired t-test was used to analyze the intrasubject variance of each parameter between occipital and frontal regions; results are presented as the mean difference (SD) with the effect size and the correlation coefficient.
Finally, a multivariate logistic regression model was carried out to analyze occipital involvement as a function of age, previous treatment status, and FPHL severity; results were presented as odds ratio (OR) with 95% CI. Statistical significance was indicated by a p-value <0.05.
Results
Participants’ Characteristics
Of 1000 patients included, six were duplicates and one patient had significant data missing in trichometry parameters. Hence, 993 women with FPHL were included, 65.9% of them have never been treated and 34.1% were in treatment failure. The mean age was 34.66 years (SD=11.25) with no significant difference between untreated and failed treatment groups (p=0.738). Majority (69.9%) of the patients had a moderate form (TDSS 2–2.99) and 16.6% had a severe or extremely severe form (TDSS ≥3) of FPHL, with no significant difference between untreated and failed treatment groups (p=0.288) (Table 1).
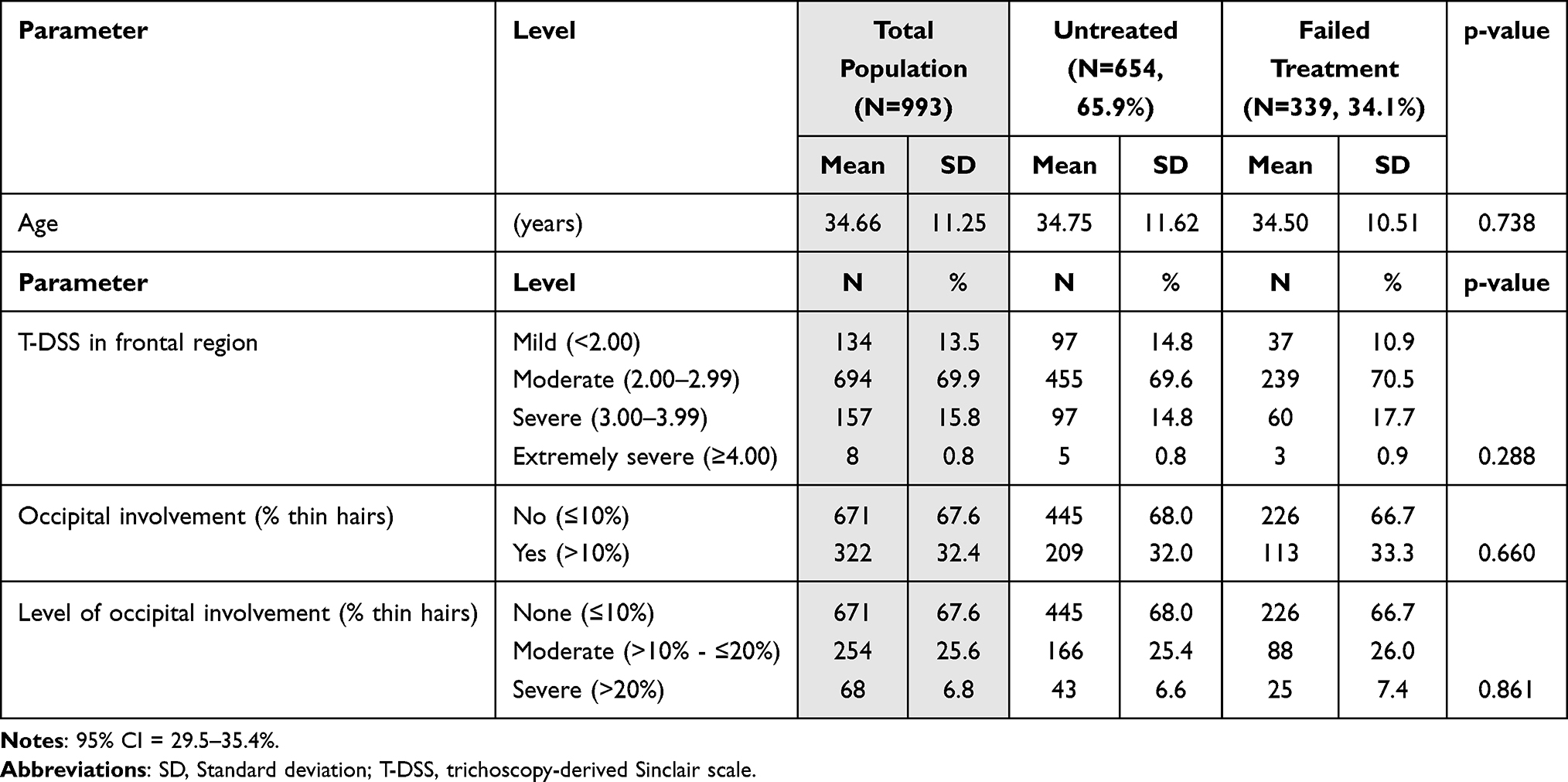 |
Table 1 Participants’ Main Demographic and Clinical Characteristics (N=993) |
Occipital Involvement
The prevalence of occipital involvement was estimated as 32.4% (95% CI = 29.5–35.4%), with no significant difference between untreated (32.0%) and treated (33.4%) women (p=0.660) (Table 1). Of the total participants, 6.8% had a severe occipital involvement defined as % thin hairs >20%; this percentage increased with the disease severity (mild 0.7%, moderate 7.3%, severe 9.7%; p<0.001 [Results not presented in tables]).
Occipital-Frontal Correlations of Trichometry Parameters
Pearson’s correlation analysis showed significantly positive correlations of all trichometry parameters between frontal and occipital regions. The strongest correlation was observed for AHST (r=0.708), followed by CHT (r=0.673) and TDSS (r=0.656), while double follicular units (r=0.172) and number of follicular units (r=0.460) showed the weakest correlations (Figure 1, Supplemental Table 1).
 |
Figure 1 Correlations between occipital and frontal regions regarding the different trichometry parameters including: (a) hair density; (b) average hair shaft thickness; (c) percentage of thin hairs; (d) percentage of medium hairs; (e) percentage of thick hairs; (f) single follicular units; (g) double follicular units; (h) triple follicular units; (i) number of follicular units; (j) cumulative hair thickness; (k) trichometry derived Sinclair scale. Abbreviations: r, Pearson’s correlation coefficient; p, p-value. |
Occipital Involvement and Trichometry Findings
Occipital involvement was associated with a higher hair density and number of follicular units (including a higher number of single follicular units) in the occipital but not in the frontal region. In addition, occipital involvement was associated with significantly lower AHST, % thick hairs, double follicular units, and CHT in both scalp regions. Additionally, patients with occipital involvement had a higher percentage of thin and medium hairs with higher TDSS scores in both regions. However, the effect size was large (Cohen’s D ≥0.8) only for AHST, % thin hairs, and % thick hairs in both regions, while the other parameters showed small-to-medium effect size (Table 2).
 |
Table 2 Trichometry Findings in All Three Scalp Regions Among Patients with Occipital Involvement Compared to Those Without Occipital Involvement |
The Levels of Occipital Involvement as a Function of the Disease Severity
The disease severity was associated with slower alterations in the occipital compared to frontal region in terms of decrease in hair density, AHST, % thick hair, CHT, and number of follicular units. On the other hand, as the disease severity increases, the % thin and medium hairs, as well as TDSS, increased less in the occipital region compared to the frontal region (Figure 2).
 |
Figure 2 Difference in trichometry parameters between occipital and frontal as a function of the disease severity level. Lines represent the mean levels of the given trichometry parameter, in occipital (black line) versus frontal (light blue line) regions, in mild, moderate, and severe disease. Trichometry parameters include: (a) hair density; (b) average hair shaft thickness; (c) percentage of thin hairs; (d) percentage of medium hairs; (e) percentage of thick hairs; (f) single follicular units; (g) double follicular units; (h) triple follicular units; (i) number of follicular units; (j) cumulative hair thickness; (k) trichometry derived Sinclair scale. |
Predictors of Occipital Involvement
Occipital involvement was independently increased in case of moderate (OR=2.64; 95% CI = 1.63–4.38) or severe+ (OR=4.72; 95% CI = 2.68–8.32) form of FPHL, while no significant association was found with the patient’s age or previous treatment status (Table 3).
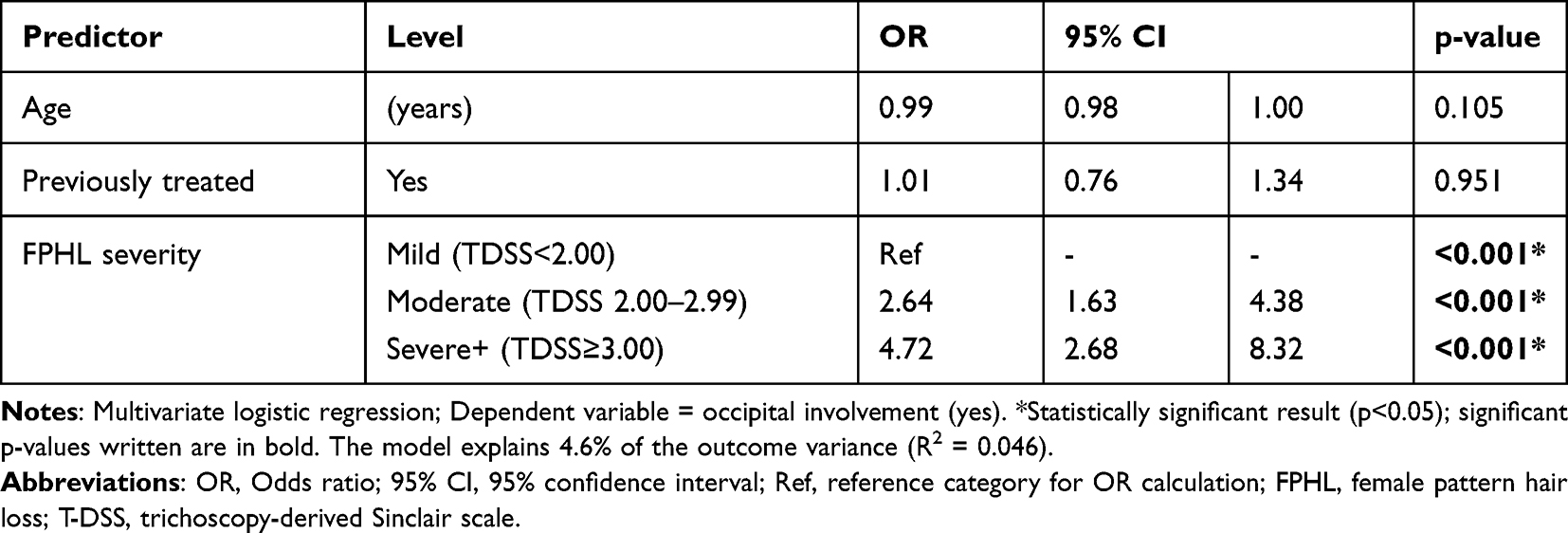 |
Table 3 Prediction of Occipital Involvement as a Function of Age, Treatment Status, and the Level of FPHL Severity in Frontal and Temporal Regions |
Discussion
The present study estimated the prevalence of occipital involvement in FPHL and its correlations with the disease severity. We found that the occipital region is involved in FPHL among one-third of the patients, and the level of involvement was found to be severe in 6.8%. The level of occipital involvement was independently associated with disease severity, and moderate-to-strong positive correlations were observed between the occipital and frontal regions in majority of the trichometry parameters. On the other hand, occipital involvement was paradoxically associated with an increased hair density and number of follicular units in the occipital area, with a higher number of single follicular units and a lower number of double follicular units. Additionally, the increased hair density was composed mainly of thin and medium, miniaturized hairs. Furthermore, we note a slower progression of the disease in the occipital region, from mild to severe forms, compared to in frontal region, suggesting a delayed pathological process in the occipital area compared to the frontal area.
To our knowledge, the present report provides the largest evidence of occipital involvement in female patients with FPHL. In the literature, data regarding occipital hair miniaturization in FPHL are scarce, and the few available studies reported comparable figures to those reported in the present study. Ekmekci et al studied occipital involvement in FPHL among 60 untreated women and found stage Ludwig I and II of thin hairs in the occipital scalp in 32% versus 38%, respectively, which was significantly different from the 22 controls.10 Another study by the same authors involving 40 patients found occipital involvement in 10 (25%) patients, who had fewer vellus follicles (9.60 versus 11.00) and follicles in telogen phase (10.46 versus 16.57) in the occiput when compared to the midscalp area, respectively.8 A more recent study observed increased vellus hairs in the occipital area in 74% of females with FPHL, although the dermoscopic findings showed a statistically significant gradient of hair loss between the frontal and occipital regions with a greater maximal severity noted in the frontal scalp.16 The latter findings are compatible with our findings, showing a slower impact of trichometry findings on the occipital compared to the frontal region as the disease progresses.
Female pattern hair loss (FPHL) typically manifests in one of two ways. The first presentation involves a diffuse thinning of hair across the mid-frontal area of the scalp, while preserving the frontal hairline. This thinning becomes particularly evident when the hair is parted down the middle. This pattern can be categorized using two scales. Ludwig’s scale separates it into three stages, ranging from mild thinning in the first stage to a complete lack of hair in the affected area in the third stage.3 Similarly, Sinclair’s scale categorizes the condition into four severity levels (ranging from grade 2 to 5), based on comparison with a normal scalp (grade 1).17 The second presentation is characterized by a diffuse thinning process, with accentuation of the central line that expands into a triangle, with its base at the anterior hairline. This is often referred to as the “Christmas tree pattern”, a term coined by Olsen.18
In contrast, male pattern hair loss (MPHL) is marked by a significant recession of the frontal-temporal hairline and baldness in the vertex region. This pattern was first proposed by Hamilton,19 and later adapted by Norwood,20 resulting in the Hamilton-Norwood scale. It is worth noting that this pattern is atypical in FPHL, where females generally experience diffuse thinning without the extensive baldness often seen in men.
The exact etiopathogenesis of FPHL is not fully understood; however, accumulating evidence suggests multiple and complex interactions between genetic, hormonal, and environmental factors.21 Usually, the diagnosis of FPHL in females is supported by the predominance of hair balding in the frontal/parietal scalp area with less focus on the occipital scalp area.22 In both males and females with androgenetic alopecia, Marty et al previously demonstrated that the scalp occipital region contains lower levels of the androgen receptors and 5α-reductase type I and II, the enzymes responsible for the conversion of testosterone into its more active form, dihydrotestosterone, than in the frontal region of the scalp. Also, authors revealed higher levels of cytochrome P-450 aromatase in occipital hair follicles, which signifies a greater local transformation (aromatization) of androgens to estrogens.23 Together, these findings suggest a lower androgens-dependent activity of hair follicles in the occipital area, which may result in lesser androgens-mediated hair regression during androgenetic alopecia.24 However, such mechanisms are probably more determinant in male androgenetic alopecia, where androgens play a major role.25
Generally, females are described to have a more protective profile against androgenic-induced hair miniaturization through greater conversion of the potentially alopecic androgens to estrogens.24 This supports the tendency for diffuse hair miniaturization in FPHL as demonstrated in our study, where the levels of occipital involvement are high and positively correlated with the disease severity. Thus, FPHL seems to induce a more generalized distribution of hair regression than the traditional, area-specific pattern hair loss.
Another interesting observation from the present study is that the likelihood and severity of occipital involvement is significantly increased in advanced forms of FPHL. In agreement, Khunkhet et al found that occipital involvement was associated with advanced forms of androgenetic alopecia, which was more observed in females than in males.24 This has important implications in the management of FPHL patients, highlighting the necessity of assessing the level of occipital involvement to adapt the therapeutic approach and improve the patient’s outcome.
One of these therapeutic implications is the impact of occipital involvement as a potential donor site for hair transplantation.26 Reduced donor sites are a major limitation for transplantation surgery outcomes, regardless of the technique used.27 Rassman and Carson provided a description of the donor region, which encompasses three important limits. The front boundary is positioned higher than that of the external acoustic meatus in a vertical orientation. An upper limit can be found 2 cm beyond the upper edge of the helical rim on a horizontal plane, while the lower limit of the donor area is subject to some debate as it potentially shifts upward over time.28 A modified version of Unger’s theory conceptualized alopecia as an ongoing and progressive state, determined by assessing the likelihood of the most severe outcome.13,28 Consequently, when hair in the occipital donor area is affected by miniaturization, the feasibility and effectiveness of hair transplantation are profoundly compromised.8,29 In some cases, when the usual donor sites are not available, it remains possible to consider transplantation from other parts of the body.30 However, these alternative sites are only available for hirsute men, but not for females. Consequently, the occipital hair miniaturization in FPHL constitutes a major limitation for hair transplantation in female patients.29
Another implication of these findings is to consider FPHL as a distinct entity of androgenetic alopecia from males, where the classical description of PHL cannot be applied. It is worth noting that the occipital area is not taken into consideration by the grading systems developed by Ludwig, Olsen, Savin and Sinclair, which may underestimate the hair thinning involvement in many FPHL patients.8 Another major clinical implication is the validity of FPHL diagnostic criteria that use the occipital scalp as a reference for the frontal region,15,24 which may result in underdiagnosis or delayed diagnosis in case of early occipital involvement. The present study has shown that the occipital area might serve as a “dynamic” diagnostic and prognostic indicator for FPHL, rather than a “static” reference for normality.
Limitations
Our study was limited by retrospective design as well as its failure to investigate other factors that may influence severity and topography of the disease such as personal co-morbidities, familial history of similar cases, biological test results, reproductive status, disease duration, etc. In addition, histopathological analysis of the cases was not performed, although it would have added value to the study findings.
Conclusion
One-third of patients with FPHL have significant occipital miniaturization. The extent and severity of the occipital involvement is proportional to the disease severity and correlates with levels of impact in the frontal region. This has major clinical implications, notably in the diagnosis when the occipital region is used as a normal reference for the assessment of the frontal region, besides limiting hair transplantation as a treatment option. A systematic assessment of the occipital region is critical to determine the staging and extensiveness of the disease and to guide the best therapeutic approach.
Ethical Statement
This study was reviewed and approved by the Bioethics Committee of Scientific & Medical Research of the University of Jeddah, approval #UJ-REC-122. Before participating, all patients underwent the standard practice of signing an informed consent form and granting permission for their data to be used for research purposes.
Acknowledgments
Author thanks Dr. Mohamed Amine Haireche for his support in analyzing the data of this study.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Birch MP, Messenger JF, Messenger AG. Hair density, hair diameter and the prevalence of female pattern hair loss. Br J Dermatol. 2001;144(2):297–304. doi:10.1046/j.1365-2133.2001.04018.x
2. Herskovitz I, Tosti A. Female pattern hair loss. Int J Endocrinol Metab. 2013;11(4):e9860. doi:10.5812/ijem.9860
3. Ludwig E. Classification of the types of androgenetic alopecia (common baldness) occurring in the female sex. Br J Dermatol. 1977;97(3):247–254. doi:10.1111/j.1365-2133.1977.tb15179.x
4. Olsen EA. Disorders of Hair Growth: Diagnosis and Treatment. Androgenetic Alopecia. New York: McGraw-Hill; 1994.
5. Venning VA, Dawber RPR. Patterned androgenic alopecia in women. J Am Acad Dermatol. 1988;18(5, Part 1):1073–1077. doi:10.1016/S0190-9622(88)70108-5
6. Glaser RL, Dimitrakakis C, Messenger AG. Improvement in scalp hair growth in androgen-deficient women treated with testosterone: a questionnaire study. Br J Dermatol. 2012;166(2):274–278. doi:10.1111/j.1365-2133.2011.10655.x
7. Griffin JE, McPhaul MJ, Russell DW, Wilson JD. The androgen resistance syndromes: Steroid 5α-Reductase 2 deficiency, testicular feminization, and related disorders. In: Valle DL, Antonarakis S, Ballabio A, Beaudet AL, Mitchell GA, editors. The Online Metabolic and Molecular Bases of Inherited Disease. McGraw-Hill Education; 2019.
8. Ekmekci TR, Sakiz D, Koslu A. Occipital involvement in female pattern hair loss: histopathological evidences. J Eur Acad Dermatol Venereol. 2010;24(3):299–301. doi:10.1111/j.1468-3083.2009.03411.x
9. Mai W, Sun Y, Liu X, Lin D, Lu D. Characteristic findings by phototrichogram in southern Chinese women with female pattern hair loss. Skin Res Technol. 2019;25(4):447–455. doi:10.1111/srt.12672
10. Rezan Ekmekci T, Koslu A. Phototrichogram findings in women with androgenetic alopecia. Skin Res Technol. 2006;12(4):309–312. doi:10.1111/j.0909-752X.2006.00196.x
11. Caroli S, Pathomvanich D, Amonpattana K, Kumar A. Current status of hair restoration surgery. Int Surg. 2011;96(4):345–351. doi:10.9738/cc31.1
12. Park JH, Park JM, Kim NR, Manonukul K. Hair diameter evaluation in different regions of the safe donor area in Asian populations. Int J Dermatol. 2017;56(7):784–787. doi:10.1111/ijd.13638
13. Unger W, Solish N, Giguere D, et al. Delineating the “safe” donor area for hair transplanting. Am J Cosmet Surg. 1994;11(4):239–243. doi:10.1177/074880689401100402
14. Carmina E, Azziz R, Bergfeld W, et al. Female pattern hair loss and androgen excess: a report from the multidisciplinary androgen excess and PCOS committee. J Clin Endocrinol Metab. 2019;104(7):2875–2891. doi:10.1210/jc.2018-02548
15. Rakowska A, Slowinska M, Kowalska-Oledzka E, Olszewska M, Rudnicka L. Dermoscopy in female androgenic alopecia: method standardization and diagnostic criteria. Int J Trichology. 2009;1(2):123. doi:10.4103/0974-7753.58555
16. Bains P, Kaur S, Kaur K. Comparison of dermoscopic findings in female androgenetic alopecia and telogen effluvium and female controls in a tertiary care center. J Clin Aesthet Dermatol. 2022;15(5):29–34.
17. Sinclair R, Wewerinke M, Jolley D. Treatment of female pattern hair loss with oral antiandrogens. Br J Dermatol. 2005;152:466–473. doi:10.1111/j.1365-2133.2005.06218.x
18. Olsen EA. The midline part: an important physical clue to the clinical diagnosis of androgenetic alopecia in women. J Am Acad Dermatol. 1999;40:106–109. doi:10.1016/S0190-9622(99)70539-6
19. Hamilton JB. Patterned loss of hair in man; types and incidence. Ann NY Acad Sci. 1951;53:708–728. doi:10.1111/j.1749-6632.1951.tb31971.x
20. Norwood OT. Male pattern baldness: classification and incidence. South Med J. 1975;68:1359–1365. doi:10.1097/00007611-197511000-00009
21. Bhat YJ, Saqib NU, Latif I, Hassan I. Female pattern hair loss—an update. Indian Dermatol Online J. 2020;11(4):493. doi:10.4103/idoj.IDOJ_334_19
22. Price VH. Androgenetic alopecia in women. J Investig Dermatol Symp Proc. 2003;8(1):24–27. doi:10.1046/j.1523-1747.2003.12168.x
23. Sawaya ME, Price VH. Different levels of 5α-reductase type I and II, aromatase, and androgen receptor in hair follicles of women and men with androgenetic alopecia. J Invest Dermatol. 1997;109(3):296–300. doi:10.1111/1523-1747.ep12335779
24. Khunkhet S, Chanprapaph K, Rutnin S, Suchonwanit P. Histopathological evidence of occipital involvement in male androgenetic alopecia. Front Med. 2021;8:790597. doi:10.3389/fmed.2021.790597
25. Fabbrocini G, Cantelli M, Masarà A, Annunziata MC, Marasca C, Cacciapuoti S. Female pattern hair loss: a clinical, pathophysiologic, and therapeutic review. Int J Womens Dermatol. 2018;4(4):203–211. doi:10.1016/j.ijwd.2018.05.001
26. Sinclair R, Patel M, Dawson TLJ, et al. Hair loss in women: medical and cosmetic approaches to increase scalp hair fullness. Br J Dermatol. 2011;165:12–18. doi:10.1111/j.1365-2133.2011.10630.x
27. Zito PM, Raggio BS. Hair Transplantation; 2022.
28. Rassman WR, Carson S. Micrografting in extensive quantities. The ideal hair restoration procedure. Dermatol Surg. 1995;21(4):306–311. doi:10.1111/j.1524-4725.1995.tb00178.x
29. Bernstein RM, Rassman WR. Densitometry and Video-microscopy. Hair Transp Forum Int. 2007;17(2):41–51. doi:10.33589/17.2.0041
30. Umar S. Use of body hair and beard hair in hair restoration. Facial Plast Surg Clin North Am. 2013;21(3):469–477. doi:10.1016/j.fsc.2013.05.003
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.