Back to Journals » Risk Management and Healthcare Policy » Volume 16
Assessment of MRI Safety Practices in Saudi Arabia
Authors Alghamdi SA ![]()
Received 6 December 2022
Accepted for publication 31 January 2023
Published 10 February 2023 Volume 2023:16 Pages 199—208
DOI https://doi.org/10.2147/RMHP.S398826
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Sami A Alghamdi
Radiological Sciences Department, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia
Correspondence: Sami A Alghamdi, Email [email protected]
Aim: The aim of this study is to investigate the safety practices used by MRI departments in Saudi Arabia.
Methods: A cross-sectional study across 113 private and public hospitals was conducted in Saudi Arabia. A survey questionnaire was designed and sent to 113 MRI units. The questionnaire consisted of 43 items under 14 sections for the assessment of MRI safety practices. These 14 sections are related to (i) MRI and its safety, (ii) MRI usage and its safety, and (iii) safety of the MRI technologists and reporting of adverse effects during the usage. The American College of Radiology (ACR) guidance document on MRI safety practices was used as a template for this survey. Data were analyzed using IBM SPSS Statistical software for Windows version 26.0 (IBM Corp., Armonk, NY, USA).
Results: Of the 43 items assessed, only 3 items’ binary responses (Yes & No) did not differ much. A greater proportion of positive responses for 40 items (93%) regarding MRI safety practices. More than 50% of the participants claimed that their departments lacked a Magnetic Resonance Safety Officer (MRSO). Regarding regular safety training programs, less than 50% received training in MRI safety. Handheld metal detectors were found in only 39% of the MRI units.
Conclusion: The majority of MRI units in Saudi Arabia have demonstrated compliance with majority of ACR MRI safety recommendations; nonetheless, there are two main items for which the guidelines may not be attained: MRSO and regular MRI safety training programs. By taking into account the limitations of this study, it is strongly recommended to assign MRSO and implement annual MRI safety training to improve MRI safety practices for both patients and healthcare workers.
Keywords: magnetic resonance imaging, MRI, safety, Saudi Arabia, 2020 American College of Radiology guidelines, ACR
Introduction
Magnetic resonance imaging (MRI) is one of the most advanced imaging modalities that provides high resolution and detailed anatomical images of the human body. It is considered as a non-invasive procedure and does not modify the structure, composition, or physical properties of atoms in the same way that other imaging methods, such as ionizing radiation, do.1 However, it is extremely important to maintain MRI safety to protect not only patients but also MRI staff, other medical personnel, and equipment.2
The use of clinical MRI comes with a number of potential dangers, one of which is that the presence of powerful static magnetic fields may increase the likelihood of injury caused by projectile effects. In addition, time-varying gradient fields have significant effects on humans, such as acoustic noise.2,3 Tissue heating and issues with the specific absorption rate (SAR) are two of the risks connected with Radiofrequency (RF) field. Furthermore, due to the growing usage of numerous medical devices and implants within the human body, the subjects of MRI safety has become more challenging than ever, with greater potential dangers linked with implants and foreign objects.4 The foreign implants that composed of ferromagnetic metals are drawn into the MRI scanner’s static magnetic field and might cause complications during scans. Objects that are elongated and ferromagnetic are subject to torsion forces. In addition, RF can cause heating of metallic implants. Some of the aforementioned incidents resulted in severe injuries.5
Pre-MRI screening is the initial step in ensuring that only approved individuals are permitted to enter the MRI area. Several incidents have been documented due to inadequate screening methods and lack of disclosure of the presence of ferromagnetic elements. However, numerous studies have justified the use of ferromagnetic detectors.6,7
MRI safety is also influenced by the design of MRI units and signage within them, as the nature and structure of these units necessitate specific precautions. The American College of Radiology (ACR) requirements include a zoning system with four distinct zones, each with its own design and signs, and numerous studies have emphasized the necessity of this safety measure. Furthermore, all zones must be supervised by MRI staff.8 Other suggestions for signs include ones warning of the powerful magnetic fields, “danger” alerts, and notices indicating that the magnet is always on. Therefore, all healthcare professionals working in an MRI unit should be aware of the purpose of safety zones and MRI appropriateness criteria.9
An ACR standard divides MRI equipment into three categories: MR-Safe, MR-Conditional, and MR-Unsafe. This eliminates the risk of injury from projectile effect injuries. Therefore, MR-safe equipment such as contrast media injector is essential, but some projectile impacts have also been documented. When non- MR-Unsafe or mislabeled MR-safe equipment is accidentally introduced into the MRI room, projectile effects with the potential for damage can occur. In addition, any emergency equipment, such as fire extinguishers or resuscitation equipment, must be thoroughly tested to ensure its compatibility with the MR setting.10
Contrast media, and specifically gadolinium chelates, are quite useful. Contrast administration is utilized for two primary reasons: enhanced lesion sensitivity and enhanced lesion characterization. However, contrast media have had a lower incidence of acute adverse responses, such as nausea and headache, and MRI staff should be prepared and aware of such adverse effects of gadolinium.11 Moreover, contrast media reaction must be stated as an emergency response and medical staff should know how to engage the emergency response system to escalate the level of care if necessary.12
As various events might occur in the MR environment, emergency preparedness is another critical aspect of MRI safety. Communication is regarded as the biggest issue in formulating emergency preparations for radiological situations.13 Many emergencies occur in radiology departments, the majority of which are caused by heart problems.14 Consequently, emergency response procedures must be devised in the event of a fire, cardiac arrest, water damage, or quench. Local responders must receive the necessary training. Drills must also be conducted on a regular basis to guarantee the level of preparedness.
All MRI technologists should take MRI safety training. This training should be part of the annual orientation program for MRI employees. A technical and medical background should be included in MRI safety training. Hands-on demonstrations of ferromagnetic missile impact assist in comprehending MRI hazards.15 Moreover, the person in charge of MRI safety should outsource some of their responsibilities to an MRI safety officer, who is in charge of enforcing the site’s safety policies on a daily basis. The MRI safety officer must have adequate training and expertise in MRI and MRI safety.9
It is important to display signs detailing the presence of magnetic fields as well as warnings that the magnet is always on. An ACR standard divides MRI equipment into three categories: MR-Safe, MR-Conditional, and MR-Unsafe. This eliminates the risk of injury from projectile effect injuries.16,17
In 2020, the ACR published guidelines (updated) on how to use MRI safely. The guidelines cover several safety pillars, such as access control, zoning, roles, and annual training. MRI safety guides mostly address the jobs of MRI staff, how to prepare patients for MRI procedures, and where to put safety warnings, like zoning and signs. MR personnel are in charge of four zones with signs of solid magnetic field presence and equipment compatibility.9 This study’s objective is to investigate the safety practices used by Saudi MRI departments. The study’s justification is based on the fact that MRI clinical applications have substantially expanded while the number of safety-related events has also increased. Therefore, strict steps must be taken to improve safety in the MR environment, since it’s been proven that only strict safety policies can reduce the number of safety-related events.18 To best of our knowledge, there have been no previous national studies regarding MRI safety in Saudi Arabia.
Materials and Methods
This online questionnaire-based cross-sectional study was conducted from March to May 2022 in different hospitals across Saudi Arabia that are using MRI scanners. The questionnaire was sent to the MRI supervisor of each hospital through an online request for their institution to participate by explaining the objectives and utility of the study. A total of 113 hospitals were approached to participate in this study. The questionnaire was developed according to the ACR guidelines on MRI safety practices. The questionnaire consisted of demographic information (region, type of health facility, magnetic field strength of the scanners, and the number of MRI scanners) and 43 items under 14 sections for the assessment of MRI safety practices. These 14 sections are related to (i) MRI and its safety, (ii) MRI usage and its safety, and (iii) safety of the MRI technologists and reporting of adverse effects during the usage of MRI across the hospitals. The responses for these 43 items were collected on a binary scale as Yes/No.
Data were analyzed using IBM SPSS Statistical software for Windows version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics (frequencies and percentages) were used to describe the categorical variables. For the bivariate analysis, the Chi-square test was used to compare the proportions of responses to the 43 items in relation to the type of health facility (private and public) and the number of MRI scanners (1 and ≥2). A p-value ≤0.05 was used to report the statistical significance of the results.
The ethical approval was not required as the study does not involve the individuals who had undergone MRI across the hospitals. This study was conducted an audit of MRI safety practices followed by the hospitals. But the consent was obtained from the MRI supervisors across the hospitals to participate in the study.
Results
This study managed to obtain responses from 113 hospitals regarding their MRI scanner facilities. Out of the 113 hospitals, 86 (76.1%) are public hospitals, and the remaining ones are private. More than 60% of these hospitals use a 1.5T-magnetic field strength MRI scanner, while 17.7% use both 1.5T and >1.5T-strength MRI scanners. Only one MRI scanner is available in 48.7% of the hospitals, whereas 15.9% use three or more MRI scanners. The distribution of these 113 hospitals are 28.3% from Riyadh Region, 15.9% from the Eastern Province, 15.9% from the Makkah Region, and the remaining ones are from Asir, Jizan, Madinah, Qassim and other places (Table 1).
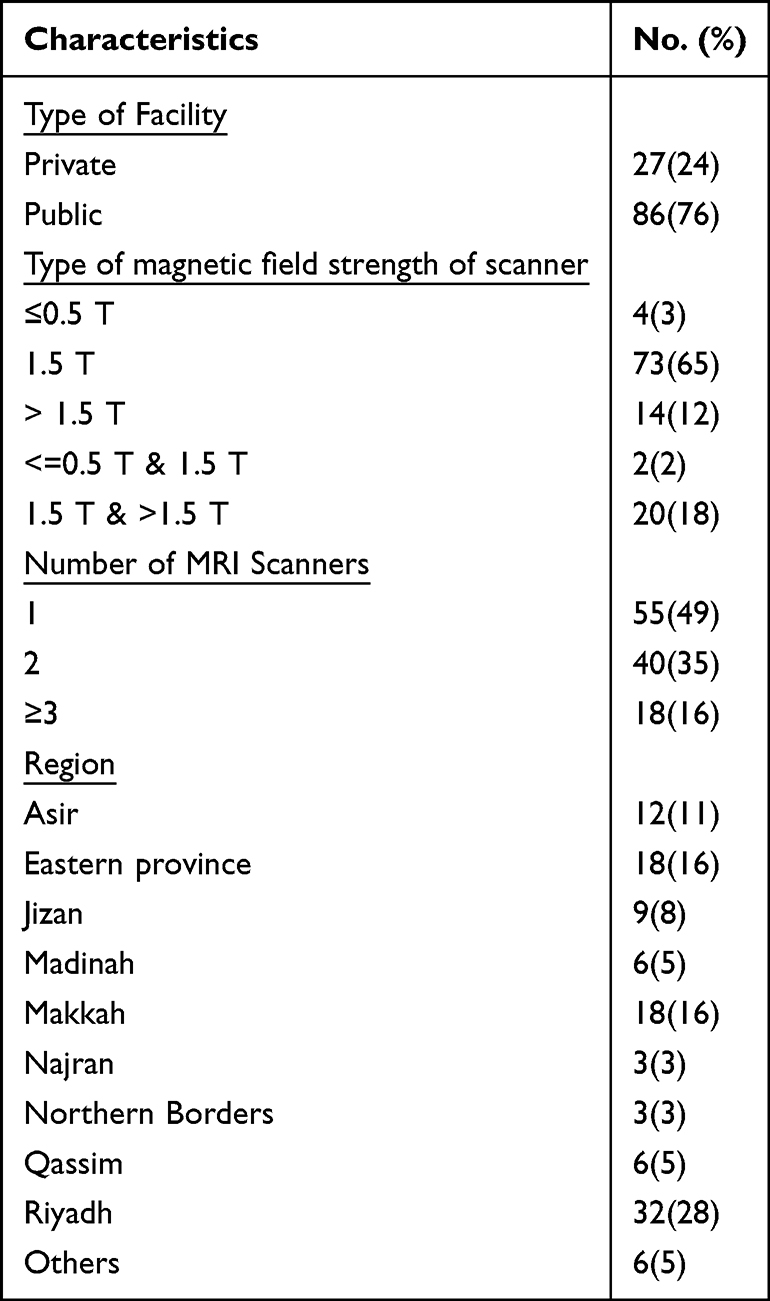 |
Table 1 Distribution of Characteristics of MRI Scanners Facilities (n=113) |
The univariate analysis in Table 2 shows the binary responses (Yes/No) provided by the 113 hospitals regarding their MRI facilities and their level of safety. A total of 16 items were used to assess the safety of the MRI scanners. The proportions of positive responses for the 16 items range from 66.4% (for the item “Is there any emergency exit door to the MRI suite?”) to 97.3% (for the item “Does the site have a written MRI safety policy?”). Out of the 16 items, the following four items generated more than 90% positive responses: “Are written policies present and readily available to facility staff?” “Are all equipment brought into the MRI suite checked to be MRI safe?” “Availability of headphones”, and “Are all MRI entrances marked to indicate the presence of a magnetic field hazard?” In addition, seven items had positive responses between 80% and 89%, whereas four items had positive responses of 77.9%, 75.1%, 72.6%, and 66.4% (Table 2).
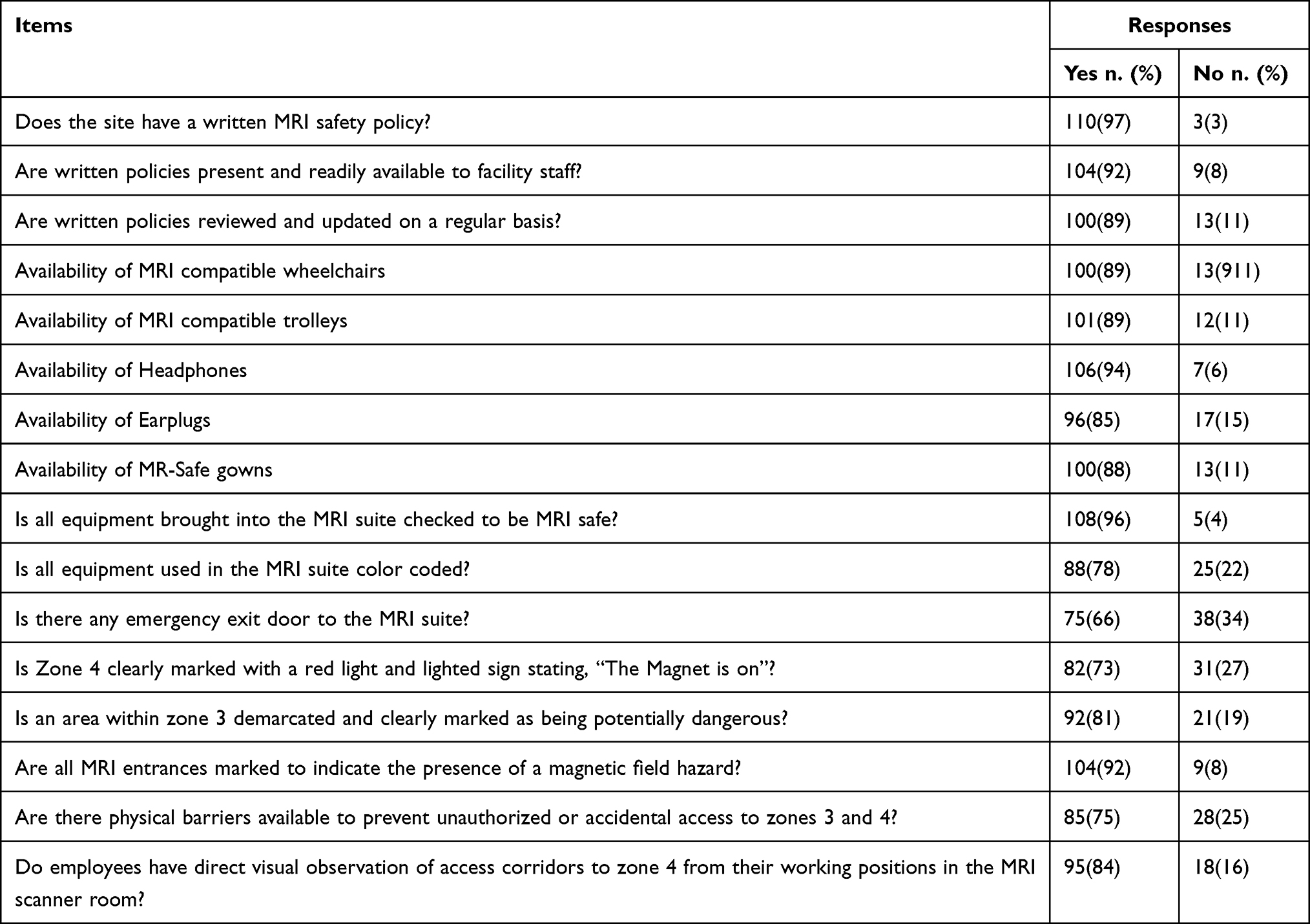 |
Table 2 Distribution of Responses Towards MRI and Its Safety |
The distribution of the responses (Yes/No) to the 14 items of MRI usage and its safety across the 113 hospitals is given in Table 3. For one item, namely, “Availability of handheld magnet”, only 38.9% of the hospitals responded positively (Yes), whereas 61.1% responded negatively (No). This indicates that most of the hospitals (61.1%) did not have this safety facility (“Availability of handheld magnet”). For the other 13 items, the positive responses range from 71.7% (for the item “Is there any document to show evidence of drills?”) to 99.1% (for the item “Availability of fire tender”). The proportion of positive responses for the 13 items is higher than the proportion of negative responses. Out of the 13 items, six had positive responses of more than 90%, four had positive responses between 80% to 90%, and the remaining three had positive response rates of 71.7%, 72.6%, and 75.2% (Table 3).
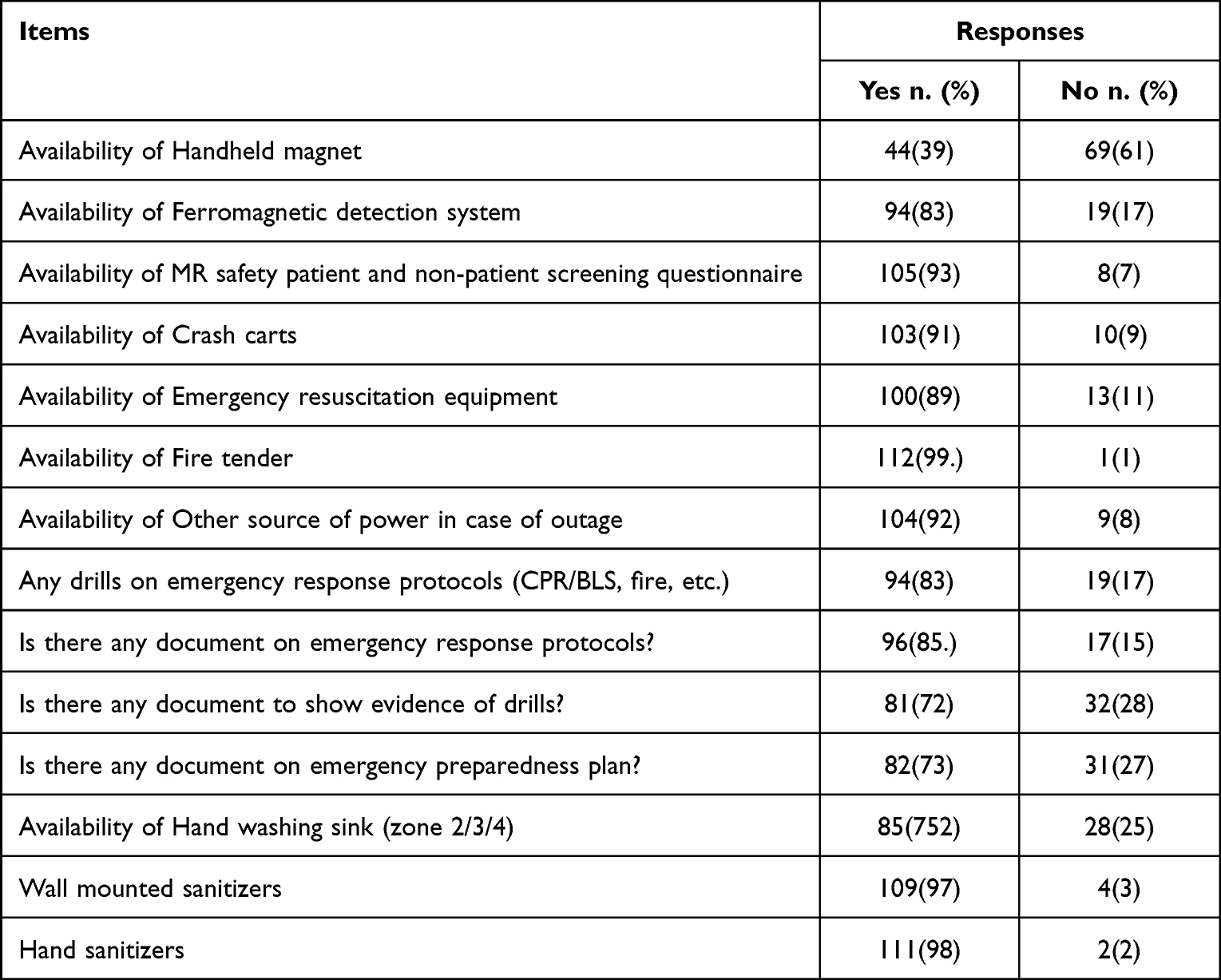 |
Table 3 Distribution of Responses Towards MRI Usage and Its Safety |
The distribution of responses associated with the safety of MRI technologists and the reporting of adverse effects during usage of MRI provided by the 113 hospitals in which there were four out of the six items related to the safety of MRI technologists and six out of the seven items related to the reporting of adverse effects during usage of MRI.
For the items related to the safety of the MRI technologists, highly positive responses 93.8%, 85.8%, 71.7%, and 77% were found for the following items: (i) Do you report MR safety incidents to the medical director in a timely manner?; (ii) Are the MRI technologists in compliance with the technologist qualifications listed in the MR Accreditation Program Requirements?; (iii) Do you have a safety training program in place for new MRI personnel?; and (iv) Do the MRI technologists in your hospital rotate in other units in the department, such as the CT? (Fixed/Rotate). For the two items, Do you have a regular safety training program in place for MRI personnel? and Do you have an MRI safety officer (MRSO) assigned in your department? The proportion of positive responses were moderate (53.1% and 42.5%.). For the six items related to reporting adverse effects during MRI usage, a higher negative response was observed, with the proportion ranging from 61.1% to 97.3%. This indicates that most of the hospitals did not experience adverse effects during MRI usage. It should be mentioned that 93.8% negative response was related to “patient death”, 61.1% to “projectile effect”, 95.6% to “fire outbreak”, 92.9% to “thermal burns”, 97.3% to “electrical shock”, and 76.1% to “Has the facility ever invited police/fire reps to MR safety presentations/facility tours?” All these proportions of negative responses (No) higher than the positive responses (Yes) (Table 4).
 |
Table 4 Distribution of Responses Towards Safety of MRI Technologists and Reporting of Adverse Effects During Usage of MRI |
Bivariate Analysis
In this analysis, two study variables (type of health facility: private and public; the number of MRI scanners: 1 and ≥2) were used to compare the responses to the 43 items of the 113 hospitals regarding (i) MRI and its safety, (ii) MRI usage and its safety, and (iii) safety of MRI technologists and reporting of adverse effects during usage of MRI.
Table 5 shows the statistical significance of nine items, the binary responses (Yes/No), and the comparison between private and public hospitals. The corresponding p-values indicate statistically significant differences in the proportion of responses for the nine items between private and public hospitals. For the five items associated with MRI and its safety, three items associated with MRI usage and its safety, and one item associated with the safety of MRI technologists and the reporting of adverse effects during usage of MRI, the proportion of positive responses (Yes) is statistically significantly higher in public hospitals compared with the proportion of positive responses in private hospitals. Meanwhile, there is no statistically significant difference in the proportion of responses for the remaining 34 items between private and public hospitals (Table 5).
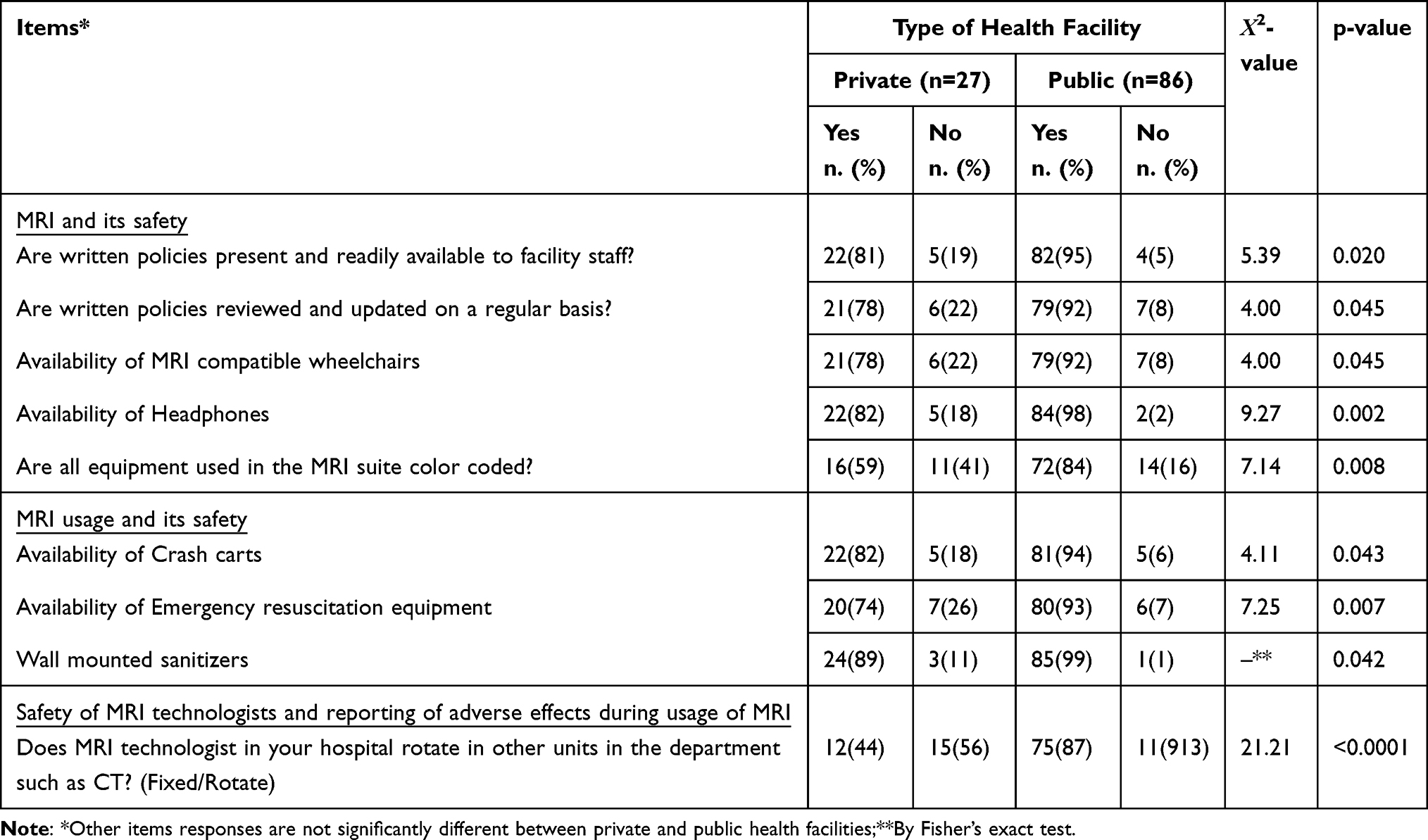 |
Table 5 Comparison of Responses Towards (i) MRI and Its Safety, (ii) MRI Usage and Its Safety Related to Patients and (iii) Safety of MRI Technologists and Reporting of Adverse Effects During Usage of MRI Between Private and Public Health Facilities |
The comparison of responses to (i) MRI and its safety, (ii) MRI usage and its safety, and (iii) safety of MRI technologists and reporting of adverse effects during usage of MRI in relation to the number of MRIs showed statistically significant difference in the proportion of responses for seven out of 43 items. For the four items related to MRI and its safety, one item related to MRI usage and its safety, and two items related to the safety of the MRI technicians and reporting of adverse effects during usage of MRI, the proportion of positive responses (Yes) is statistically significantly higher in hospitals using ≥2 MRI scanners compared with hospitals using just one MRI scanner. For the remaining 36 items, no statistically significant difference in the proportion of responses was observed in relation to the number of MRI scanners used by the hospitals (Table 6).
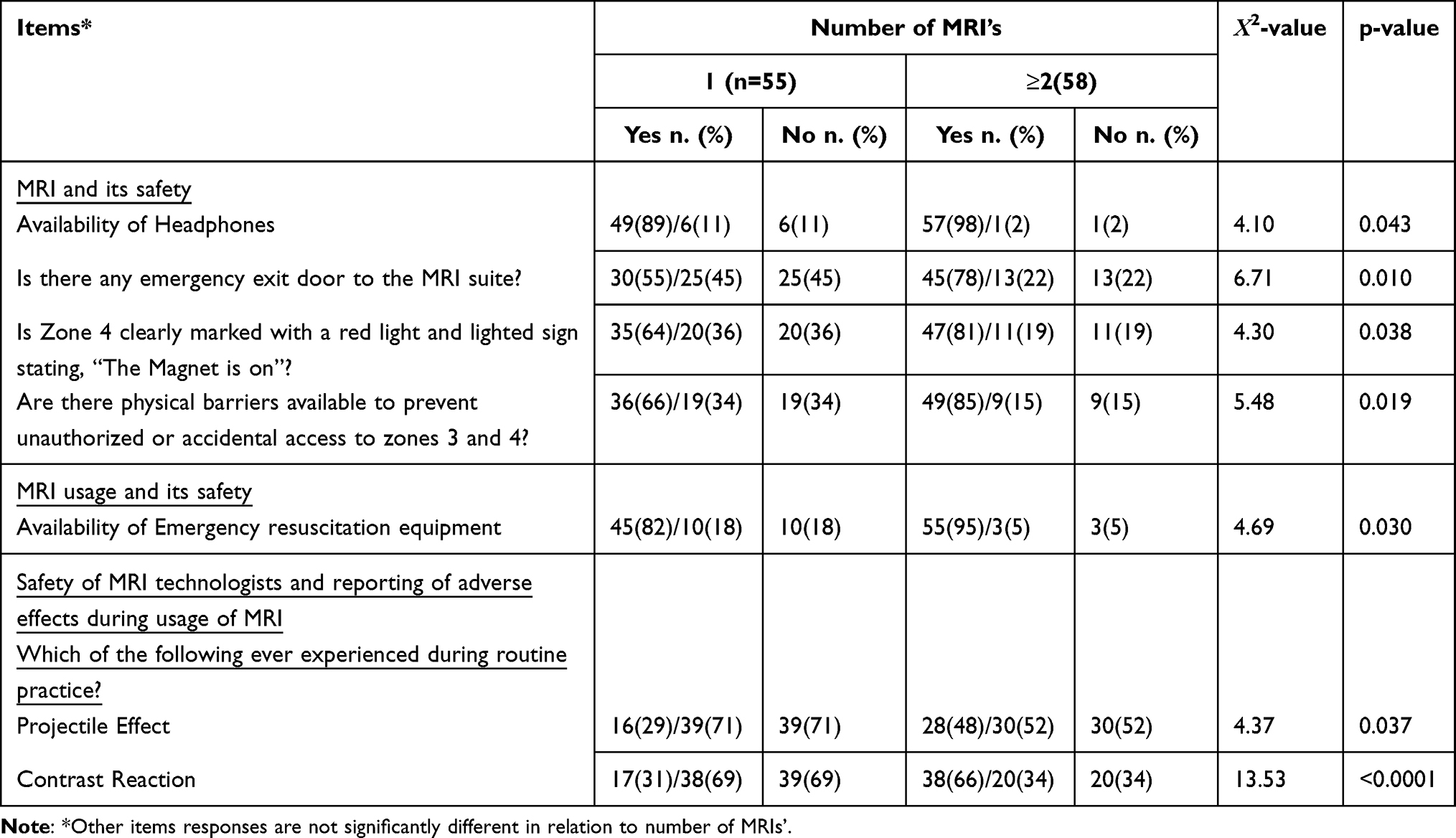 |
Table 6 Comparison of Responses Towards (i) MRI and Its Safety, (ii) MRI Usage and Its Safety Related to Patients and (iii) Safety of MRI Technicians and Reporting of Adverse Effects During Usage of MRI in Relation to the Number of MRI’s |
Discussion
Even though MRI does not employ ionizing radiation, it has its safety concerns, such as projectiles, which require safety criteria for clinical MRI situations.1 The online survey in this study summarizes the outcomes of Saudi’s existing MRI safety practices. The ACR guidance document on MRI safety practices was used as a template for this survey.9 This cross-sectional study of 113 private and public hospitals in Saudi Arabia has obtained higher proportion of positive responses regarding MRI installation safety, MRI’s usage and its safety, the safety of MRI technologists and reporting of adverse effects during usage of MRI. Of the 43 items assessed, only 3 items’ binary responses (YES/NO) had moderate positive responses. A higher proportion of positive responses (40/43; 93%) regarding MRI safety practices indicates that both private and public hospitals in Saudi Arabia are following most of the guidelines, as recommended by ACR.
MRI safety is influenced by the design of MRI units and their signage. Four separate zones around the MRI scanner are indicated in the ACR recommendation document.19 Zones 3 and 4 are MRI-monitored and controlled entry zones. The results of this study indicate that MRI departments employ their zoning systems optimally. Moreover, ferromagnetic detection systems should be used to physically screen for the presence of metallic material in zone 3.20 The vast majority of study respondents (83.2%) reported that MRI units were equipped with metal detectors. However, handheld metal detectors were found in only 39% of the MRI units.
Pre-MRI screening is the initial step in ensuring that only qualified people may access the MRI areas. Many occurrences of ferromagnetic elements not being disclosed have been reported as a result of faulty screening techniques; for example, more than a quarter of screening-related incidents contain an object that should not have been in the MRI unit.21 Opoku et al22 noted that accompanying family members and other clinical professionals, such as nurses, were not subject to required screening other than removing their metallic items before entering the scanner room. However, the present study showed that most hospitals follow the optimal use of pre-MRI screening.
This study demonstrated that all MRI units had access to emergency preparedness equipment, such as a stretcher, fire extinguisher, safe wheelchair, trolley, anesthetic, and alternative power sources in the event of a power outage. In addition, three-quarters of the respondents reported that their units had emergency exits. These results reflect that the vast majority of MRI units in Saudi Arabia are prepared for disasters. Moreover, within zones 3 and 4, all movable equipment should be clearly labeled and color-coded as follows: MRI safe (green), MRI conditional (yellow), and MRI unsafe (red).23 Eighty percent of respondents stated that all MRI equipment was color-coded in the present study.
Healthcare-associated infections harm more than a million patients each year, and infection control measures must be implemented to reduce their risks.24 The majority of respondents reported the availability of wall-mounted hand sanitizers and hand washing sinks.
The presence of MRSOs in MRI departments to continuously monitor safety procedures is crucial.8 More than 50% of the participants claimed that their departments lacked an MRSO. Regarding regular safety training programs for MRI personnel, less than 50% received training in MRI safety. This is possibly due to the burden of financial commitment to organize periodic safety training, appoint an MRSO, or because Saudi Arabia’s Ministry of Health (MOH) does not mandate MRI safety training or an MRSO.25 Ayasrah26 found that only 4 of 38 facilities implemented MRI safety training courses in Jordan.
The vast majority of the respondents in our result reported that they have an MRI safety policy document that is reviewed and updated regularly. This is contrary to a study from Ghana that revealed that approximately half of the MRI units did not have a written MRI safety policy document.27
Regarding adverse effects associated with MRI, we found that there was a negative response related to patient death, projectile effects, fire outbreaks, thermal burns, and electrical shock. This shows that most hospitals have safety measures for their MRIs. Delfino et al28 found in their study of examine the MRI adverse event reports submitted to Food and Drug Administration from 1 January 2008 to 31 December 2017 in 1568 reports in which the thermal injuries were the most often reported adverse event with 59% were documented as examined reports. The 9% of projectile events was also observed. The only exception in this study was contrast media reactions; 48.7% of hospitals experienced this type of adverse effect. Potential adverse reactions associated with the delivery of MRI contrast media have been reported,29,30 including acute allergic reactions, rashes, nausea, and anxiety. MRI should be considered safe in terms of frequency, presentation, and severity of acute reactions.
In our study, a comparison between private and public hospitals showed no statistically significant difference for 34 of the 43 items that were used to assess the safety practices of MRI. Only for nine items was there a statistically significant difference, as public hospitals maintain better safety practices than private hospitals (Table 5). This indicates that public hospitals are utilizing the best safety practices when compared to private hospitals. This is logical, as currently, there are safety guidelines issued by the MOH related to MRI safety practices for its hospitals. Our results also show a statistically significant difference in responses for 7 of 43 items, revealing that hospitals that use more than 1 MRI scanner utilize better safety practices than hospitals with only 1 MRI scanner.
The main limitation of this study was the method of data collection, which was a self-administered questionnaire rather than a collection of events/accidents, due to hospital or institution legislative or policy restrictions regarding data collection. The self-administered questionnaire study had a low response rate. However, I was not following up repeatedly so as to annoy the working colleagues. Another limitation of this study was the omission of qualitative evaluation.
Conclusion
The majority of MRI units have demonstrated compliance with the majority of the ACR MRI safety recommendations, though work remains to better assure MRI patients and caregivers of safety; nonetheless, there are two main items for which the guidelines may not be attained: MRSO and regular MRI safety training programs. Therefore, it is strongly recommended to assign MRSO and implement annual MRI safety training to improve MRI safety practices for both patients and healthcare workers.; nonetheless, there are two main items for which the guidelines may not be attained: MRSO and regular MRI safety training programs. Therefore, it is strongly recommended to assign MRSO and implement annual MRI safety training to improve MRI safety practices for both patients and healthcare workers.
Acknowledgment
Author thanks the College of Applied Medical Sciences Research Center and Deanship of Scientific Research at King Saud University for support and providing resources.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Hartwig V, Giovannetti G, Vanello N, Lombardi M, Landini L, Simi S. Biological effects and safety in magnetic resonance imaging: a review. Int J Environ Res Public Health. 2009;6:1778–1798. doi:10.3390/ijerph6061778
2. Stafford RJ. The physics of magnetic resonance imaging safety. Magnet Resonance Imaging Clin. 2020;28:517–536. doi:10.1016/j.mric.2020.08.002
3. Stogiannos N, Westbrook C. Investigating MRI safety practices in Greece. A national survey. Hellenic J Radiol. 2020;5:547.
4. Smith JA. Hazards, safety, and anesthetic considerations for magnetic resonance imaging. Top Companion Anim Med. 2010;25:98–106. doi:10.1053/j.tcam.2010.01.003
5. Steinbacher J, McCoy M, Klausner F, Wallner W, Oellerer A, Machegger L. Do patients with implants experience strong sensations that lead to early termination of MRI examinations? Concepts Magnet Resonance Part A. 2019;2019:215.
6. Weidman EK, Dean KE, Rivera W, Loftus ML, Stokes TW, Min RJ. MRI safety: a report of current practice and advancements in patient preparation and screening. Clin Imaging. 2015;39:935–937. doi:10.1016/j.clinimag.2015.09.002
7. Keene MN, Watson RE. Ferromagnetic detectors for MRI safety: toy or tool? Curr Radiol Rep. 2016;4:1–6. doi:10.1007/s40134-016-0146-z
8. Kanal E, Barkovich AJ, Bell C, et al. ACR guidance document on MR safe practices: 2013. J Magnetic Resonance Imaging. 2013;37:501–530. doi:10.1002/jmri.24011
9. ACR Committee on MR Safety. 2022 ACR manual on MR safety version 1.0, 2020.
10. Gowing JR, Walker KN, Elmer SL, Cummings EA. Disaster preparedness among health professionals and support staff: what is effective? An integrative literature review. Prehosp Disaster Med. 2017;32:321–328. doi:10.1017/S1049023X1700019X
11. Thomsen HS. European Society of Urogenital Radiology (ESUR) guidelines on the safe use of iodinated contrast media. Eur J Radiol. 2006;60:307–313. doi:10.1016/j.ejrad.2006.06.020
12. Rivers B. ACR manual on contrast media. 2021.
13. Ingram RJ. Emergency response to radiological releases: have we communicated effectively to the first responder communities to prepare them to safely manage these incidents? Health Phys. 2018;114:208–213. doi:10.1097/HP.0000000000000757
14. Ott LK, Pinsky MR, Hoffman LA, et al. Medical emergency team calls in the radiology department: patient characteristics and outcomes. BMJ Qual Saf. 2012;21:509–518. doi:10.1136/bmjqs-2011-000423
15. Sammet S, Sammet CL. Implementation of a comprehensive MR safety course for medical students. J Magnetic Resonance Imaging. 2015;42:1478–1486. doi:10.1002/jmri.24993
16. Tsai LL, Grant AK, Mortele KJ, Kung JW, Smith MP. A practical guide to MR imaging safety: what radiologists need to know. Radiographics. 2015;35:1722–1737. doi:10.1148/rg.2015150108
17. Jaimes C, Biaggotti D, Sreedher G, Chaturvedi A, Moore MM, Danehy AR. Magnetic resonance imaging in children with implants. Pediatr Radiol. 2021;51:748–759. doi:10.1007/s00247-021-04965-5
18. Medicines and Healthcare Products Regulatory Agency. (2015) Safety guidelines for magnetic resonance imaging equipment in clinical use.
19. Fuentes MA, Trakic A, Wilson SJ, Crozier S. Analysis and measurements of magnetic field exposures for healthcare workers in selected MR environments. IEEE Trans Biomed Eng. 2008;55:1355–1364. doi:10.1109/TBME.2007.913410
20. Chandra T, Chavhan GB, Sze RW, et al. Practical considerations for establishing and maintaining a magnetic resonance imaging safety program in a pediatric practice. Pediatr Radiol. 2019;49:458–468. doi:10.1007/s00247-019-04359-8
21. Cynthia Field, B. S. N., and Pennsylvania Patient Safety Authority. MRI Screening: What’s in Your Pocket?. 2022.
22. Opoku S, Antwi W, Sarblah SR. (2013) Assessment of safety standards of magnetic resonance imaging at the Korle Bu Teaching Hospital (KBTH) in Accra, Ghana. Imaging and Radioanalytical Techniques in Interdisciplinary Research—Fundamentals and Cutting Edge Applications.
23. Sammet S. Magnetic resonance safety. Abdomin Radiol. 2016;41:444–451. doi:10.1007/s00261-016-0680-4
24. Haque M, Sartelli M, McKimm J, Bakar MA. Health care-associated infections–an overview. Infect Drug Resist. 2018;11:2321. doi:10.2147/IDR.S177247
25. Almalki MJ, Shubayr N, Alomair OI, et al. Safety related for lone working magnetic resonance technologists in southern Saudi Arabia. J King Saud Univ Sci. 2022;102178. doi:10.1016/j.jksus.2022.102178
26. Ayasrah M. MRI safety practice observations in MRI facilities within the Kingdom of Jordan, compared to the 2020 manual on MR safety of the American College of Radiology. Med Devices. 2022;15:131.
27. Piersson AD, Gorleku PN. A national survey of MRI safety practices in Ghana. Heliyon. 2017;3:e00480. doi:10.1016/j.heliyon.2017.e00480
28. Delfino JG, Krainak DM, Flesher SA, Miller DL. MRI‐related FDA adverse event reports: a 10‐yr review. Med Phys. 2019;46:5562–5571. doi:10.1002/mp.13768
29. Choi MH, Choi J-I, Jung SE, Ahn K-J, Lee HG. Acute adverse reactions to gadolinium-based intravenous contrast agents for MRI: retrospective analysis using computed reporting system. J Korean Soc Magnet Resonance Med. 2011;15:139–145. doi:10.13104/jksmrm.2011.15.2.139
30. Bruder O, Schneider S, Nothnagel D, et al. Acute adverse reactions to gadolinium-based contrast agents in CMR: multicenter experience with 17,767 patients from the EuroCMR registry. JACC. 2011;4:1171–1176. doi:10.1016/j.jcmg.2011.06.019
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of the Accreditation Program of the Saudi Central Board for Accreditation of Healthcare Institutions on the Safety Dimension of the Institute of Medicine Quality
Alsaedi A, Sukeri S, Yaccob NM, Almazroea A
Journal of Multidisciplinary Healthcare 2023, 16:1179-1190
Published Date: 28 April 2023