Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 12
Assessment of macrophage migration inhibitory factor in patients with verruca vulgaris
Authors Sorour NE ![]() , Hamed AM, Tabl HAEM, Ahmed AAEA
, Hamed AM, Tabl HAEM, Ahmed AAEA
Received 19 March 2019
Accepted for publication 30 July 2019
Published 22 August 2019 Volume 2019:12 Pages 591—595
DOI https://doi.org/10.2147/CCID.S209269
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Neveen Emad Sorour,1 Ahmed Mohamed Hamed,1 Hala Abd-El Mageed Tabl,2 Amira Abd-El Aziz Ahmed1
1Department of Dermatology, Venereology and Andrology, Faculty of Medicine, Benha Univesity, Benha, Egypt; 2Department of Medical Microbiology and Immunology, Faculty of Medicine, Benha Univesity, Benha, Egypt
Correspondence: Ahmed Mohamed Hamed
Department of Dermatology, Venereology and Andrology Faculty of Medicine, Benha University, El Kobry street, No.5, Benha 13513, Egypt
Tel +20 0 100 523 9888
Email [email protected]
Background: Common warts are caused by human papillomaviruses (HPVs), they are among the most common cutaneous viral infections. Macrophage migration inhibitory factor (MIF) is an essential contributor in many inflammatory and immune skin diseases. Yet, its role in the pathology of common warts is unclear.
Objective: To assess MIF levels in lesional and perilesional skin in patients with common warts in comparison to apparently healthy control group with matching age and sex.
Subjects and methods: A case-control study performed on 60 patients with common warts (group A) and 30 age and sex matching healthy controls (group B). Two biopsies were taken from each patient in group A; one from the lesion (lesional) and the other one from the skin around the wart (perilesional), while biopsies of controls were taken from matched sites to patients. Measurement of MIF in all groups was done by quantitative ELISA kits.
Results: Significant high MIF levels were detected in lesional and perilesional skin biopsies compared to controls (P<0.001). Yet, the difference in MIF levels between lesional and perilesional skin biopsy was non-significant. No significant relations were found between lesional and perilesional MIF levels and clinical characteristics of the studied patients while both lesional and perilesional MIF levels were significantly correlated (rh=0.269, P=0.021).
Conclusion: The significantly elevated MIF levels in lesional and perilesional skin biopsies compared to controls point to its role in wart progression from HPV infected cells.
Keywords: macrophage migration inhibitory factor, common warts, human papillomavirus
Introduction
Cutaneous warts are benign skin proliferations caused by the human papillomavirus (HPV).1 Since papillomaviruses can cause chronic infections, without any apparent systemic manifestations, that rarely kill the host, they are considered very infectious agents.2
Patients suffering from active warts demonstrate both antibody and cellular immune reactions with the latter being proved by a histopathological assessment of spontaneously regressing genital warts.3
Macrophage migration inhibitory factor (MIF) is the first discovered lymphokine4 that holds characteristic structure and biological activities, combining the features of growth factors, chemokines, and cytokines.5,6 Cutaneous MIF is produced in the basal keratinocyte layer.7 MIF is a ligand of cell surface receptor complexes which consists of CD74 and CD44, CXCR2, CXCR4, or CXCR7.8 It is responsible for some pro-inflammatory functions, including chemo-attraction of T cells, neutrophils, and monocytes and activation of T cells and macrophage as well.5,9
Macrophage MIF participates in triggering the innate immune system during infections via stimulating the production of IL-2, IL-6, INF γ, and TNF-α.10 It also exerts major functions in cutaneous wound healing, inflammatory responses, immune reactions, and other skin disorders such as psoriasis vulgaris and atopic dermatitis.11 Yet, data about its role in the pathology of common warts are scanty. So, the aim of this work was to assess MIF in lesional and perilesional skin in patients with common warts (verruca vulgaris) compared with age- and sex-matched control subjects.
Subjects and methods
This case-control study included 60 verruca vulgaris cases who were gathered from the Outpatient Clinic of the Dermatology and Andrology Department of Benha University Hospital between October 2017 and June 2018. The approval of the Research Ethical Committee involving human subjects of Benha Faculty of Medicine was granted before commencing the study which also followed the terms of the Declaration of Helsinki. Each participant signed an informed written consent before joining the study.
Both males and females who were 18 years or older and suffering from verruca vulgaris, yet, did not receive systemic (immunotherapy) or topical treatment for at least a month before collection of the skin biopsies were enrolled in the study. While cases who were pregnant, breast feeding, suffering from other skin disorders which affect the level of MIF like atopic dermatitis and psoriasis vulgaris, or had a history of any systemic disorders like autoimmune disorders, diabetes mellitus, malignancies, or hypertension were excluded from the study.
A purposely designed sheet was filled for each participant demonstrating age, gender, onset, duration of the warts, and medical history. Meticulous general and local examination (focusing on number, and site of warts) was performed for each participant.
Participants were grouped into two groups: group A (patients group including 60 patients with verruca vulgaris) and group B (control group including 30 age- and sex-matched apparently healthy controls).
Two biopsies were taken from each patient in group A; one was the lesional skin biopsy from the verruca vulgaris lesion and the other was the perilesional biopsy taken from skin surrounding the wart (1.5 cm from the edge of the lesion), while biopsies from controls were taken from matched sites to patients.
Skin biopsies were homogenized in 1.5 mL extraction buffer (containing 10 mM Tris pH 7.4, 150 mM NaCl, 1% Triton X-100) per gram of tissue using rotor-stator homogenizer (Art-Miccra D-8 Germany) for 20 s. The resulting homogenate transferred to 1.5 mL Eppendorf tube to be centrifuged at 13.000× g for 10 mins in 4°C and the resulting supernatant was kept in −80°C until analyzed.
MIF levels were measured by the quantitative sandwich ELISA technique using Quantikine® ELISA (DMF00B; R&D Systems, Inc., Minneapolis, MN, USA).
Statistical analysis
Data collection and tabulation were performed using by the 16th version of SPSS software (SPSS Inc., Chicago, ILL Company). Chi-square test (X2) was adopted for analyzing categorical data which were presented as numbers and percentages. While mean±standard deviation, median, and range were used to present continuous data. Shapiro–Wilks test was used to test the normality of data for which P>0.05 was the normality reference. Variables with normal distribution among two independent groups were evaluated using the Student's t- test, while nonparametric variables were evaluated using Man–Whitney U-test. Kruskal–Wallis test was adopted to analyze differences among three independent means of nonparametric variables. Differences in nonparametric data among matched groups were evaluated using Wilcoxon test. Correlation between nonparametric variables was assessed using Spearman’s correlation coefficient (rho). P≤0.05 was considered significant.
Results
The current study included 60 patients; 23 males (38.33%) and 37 females (61.67%). Their ages ranged between 18 and 60 years with a mean±SD for the age of 27.1 years ±8.7. Thirty clinically free individuals served as a control group; 16 males (53.33%) and 14 females (46.67%). Their ages ranged between 19 and 38 years with a mean±SD for the age of 25.4±5.2 years. Both patients and controls were age and sex-matched with no statistically significant difference (P=0.33 and 0.17, respectively).
Macrophage migration inhibition factor was significantly higher in lesional and perilesional skin biopsies than controls (P=0.001 for both); however, the difference in MIF levels between lesional and perilesional skin biopsies was non-significant (P=0.31) (Table1).
 |
Table 1 Comparison between studied groups regarding MIF levels |
No significant relations were found between lesional and perilesional MIF levels and clinical characteristics of the studied patients (Tables 2 and 3) while both lesional and perilesional MIF levels were significantly correlated (rh=0.269, P=0.021) (Table 4).
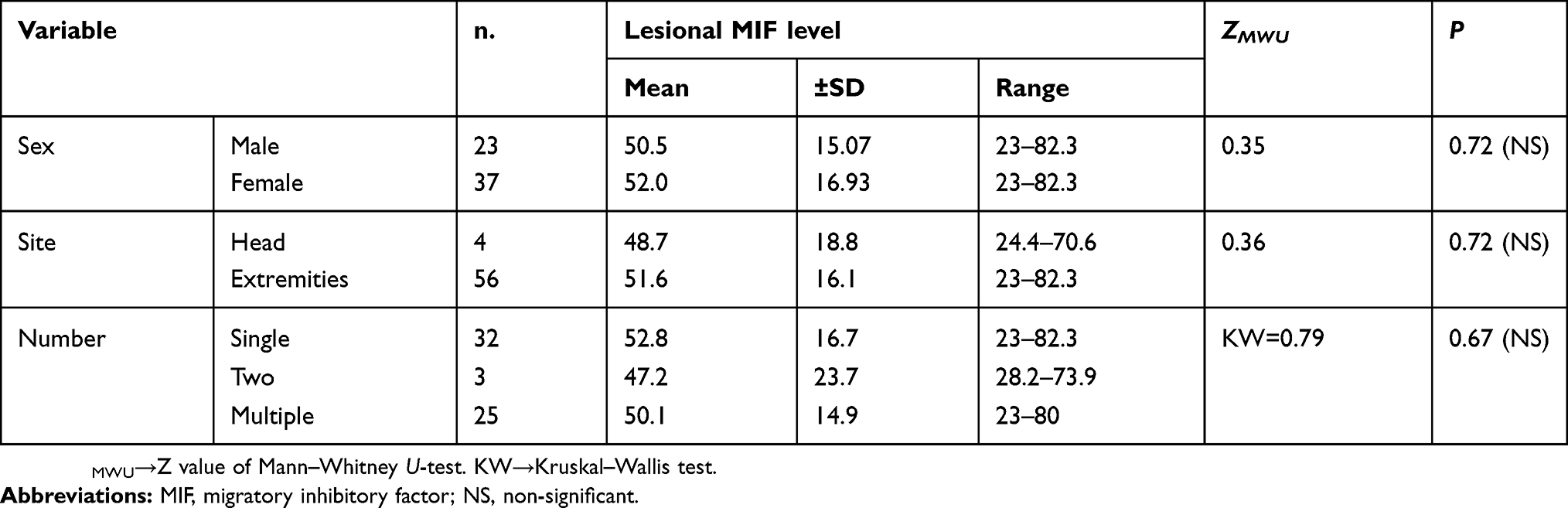 |
Table 2 Level of lesional MIF according to the clinical data of patients group |
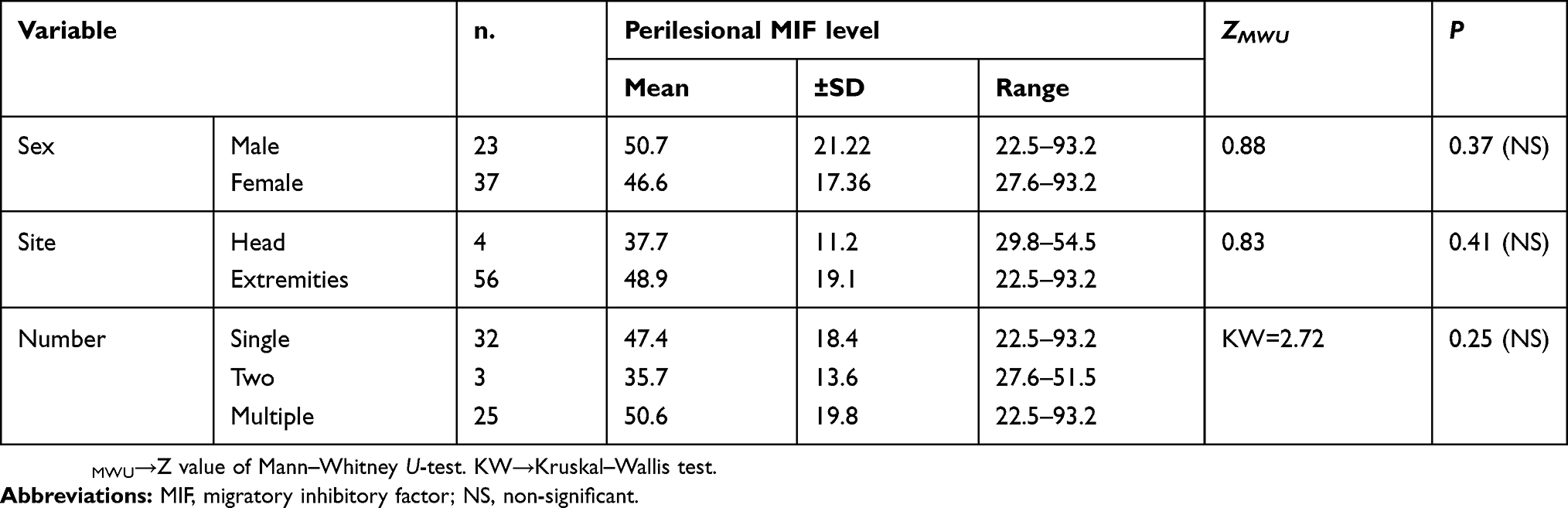 |
Table 3 Level of perilesional MIF according to the clinical data |
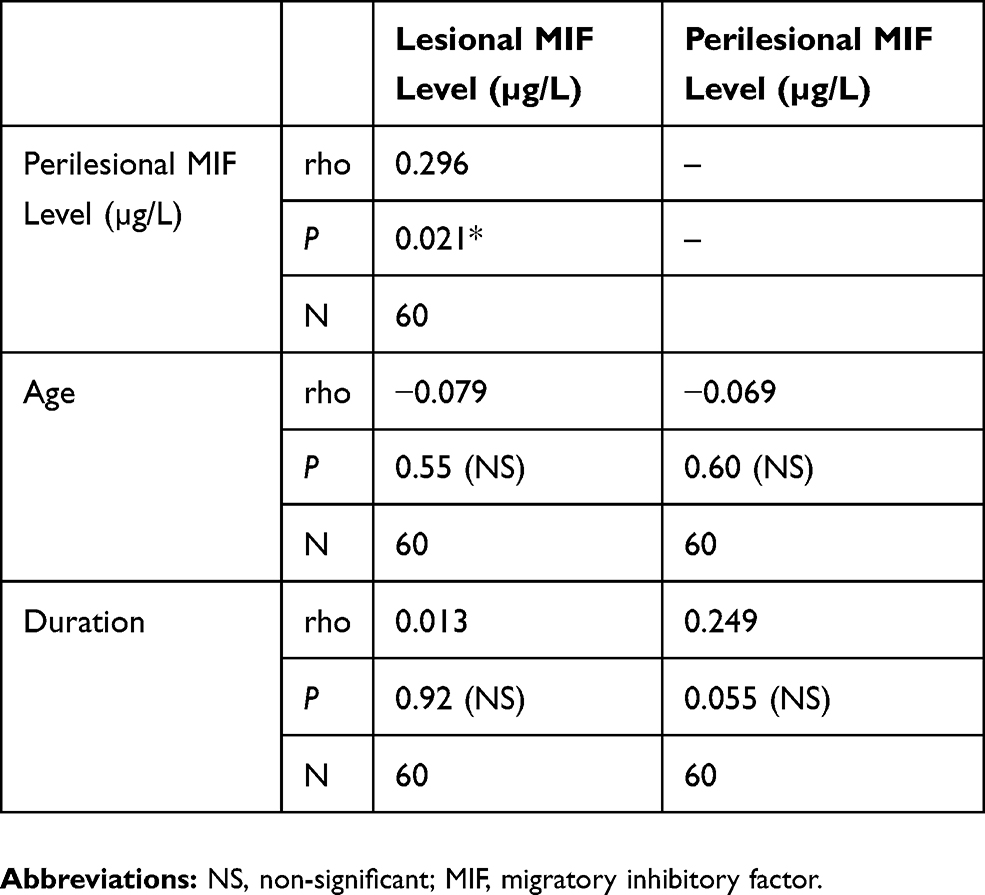 |
Table 4 Correlation between MIF levels with age and duration of warts |
Discussion
The current study was designed to evaluate the level of MIF in lesional and perilesional skin in patients with verruca vulgaris in comparison to age- and sex-matched controls.
As far as we know, this is the first study to assess lesional and perilesional MIF levels in cases suffering from verruca vulgaris compared to their controls.
The increased level of MIF in lesional biopsies could be attributed to its production by many immune and non-immune cells, including fibroblasts, macrophages, and lymphocytes, as well as, cells of endocrine, nervous, and reproductive systems.5 Additionally, histological examination of warts demonstrated an inflammatory cellular infiltration mostly by lymphocytes and mononuclear phagocytes at the destructed epidermal layers which could be the source of MIF.12
The relationship between MIF secretion and HPV infection was studied by Kindt et al.13 They found for the first time that the secretion (not expression) of MIF measured by quantitative analysis to MIF-mRNA was higher in HPV-positive human head and neck squamous cell carcinomas cell lines than in HPV-negative cell lines, an observation which was confirmed by resistance to an inhibitor of MIF (4-iodo-6-phenylpyrimidine). They hypothesized that the acidic environment created by HPV (evidenced by increased lactate production) explained the increase in MIF secretion through the activation of hypoxia-inducible factor 1. Consequently, the MIF-mRNA level increases in human HPV-positive cell lines, thus leading to elevated protein synthesis and the secretion of MIF.
At the cellular level, MIF signaling mainly depends on interaction with the cytokine receptor CD74/CD44. Binding to its cognate receptor triggers the mitogen-activated protein kinase /extracellular signal-regulated kinase signaling cascade, leading to an activation of cyclin D1 transcription and cyclin-dependent kinase-mediated phosphorylation of the Retinoblastomaprotein, resulting in stimulation of cell proliferation.14
The postulated role of MIF in progression of warts could be explained by the fact that high MIF levels may act as a trigger for proliferation of keratinocytes as MIF is a potential enhancer of cellular growth15 and is a pro-inflammatory agent as well, since it stimulates the production of cytokines including IL-1 IL-2, IL-6, IL-8, TNF, interferon IFN- γ, the secretion of nitric oxide, and the induction of the cyclooxygenase-2 pathway.16 IL-8 also stimulates cellular growth and proliferation,17 and angiogenesis.18 MIF induces expression of matrix metalloproteinase 9 which helps in tumor cell invasiveness.19
Clues for the role of MIF in wart progression come from the observation that it has been investigated in many clinical and experimental studies in both inflammatory diseases and cancer20 specifically its role is in stimulating proliferation of keratinocytes in psoriasis animal models.21
Moreover, it plays many roles in the pathogenesis of human cancer stimulating cellular proliferation, growth, progression and escape from the immune system, promoting angiogenesis and cellular migration and inhibiting apoptosis as well as autophagy in tumor cells.22
Results obtained from this study showed that lesional MIF levels were higher than perilesional levels with no statistically significant difference, despite they were correlated which could be explained as a stepwise rise in MIF levels, an observation which needs further studies.
On the other hand, El Hamd et al23 found that serum levels of MIF were significantly lower in patients with cutaneous warts compared to their healthy controls which could be explained by shift of MIF to the wart sites, a result which needs further research.
Limitations of the study
The limitations of this study were the small number of patients and the study of only one type of cutaneous warts which was verruca vulgaris.
Recommendations
We recommend further studies to evaluate MIF in other types of warts, eg, plane, planter, and genital types and correlate it with the type of HPV. Further studies are needed to investigate the genetic polymorphisms.
Conclusion
The significantly elevated MIF levels in lesional and perilesional biopsies compared to controls point to its role in the progression of warts from HPV infected cells through postulated increase in keratinocytes proliferation, enhanced angiogenesis, and cellular invasion.
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Vali A, Ferdowsi F. Evaluation of the efficacy of 50% citric acid solution in plane wart treatment. Indian J Dermatol. 2007;52:96–98. doi:10.4103/0019-5154.33287
2. Medzhitov R, Janeway CAJ. Immunity: the virtues of a non- clonal system of recognition. Cell. 1997;91:295–298. doi:10.1016/s0092-8674(00)80412-2
3. Stanley MA. Immune responses to human papilloma viruses. Indian J Med Res. 2009;130:266–276.
4. Bloom BR, Bennett B. Mechanism of a reaction in vitro associated with delayed-type hypersensitivity. Science. 1966;153:80–82. Quoted from Bezdek et al., 2018. doi:10.1126/science.153.3731.80
5. Calandra T, Roger T. Macrophage migration inhibitory factor: a regulator of innate immunity. Nat Rev Immunol. 2003;3:791–800. doi:10.1038/nri1200
6. Bloom J, Metz C, Nalawade S, et al. Identification of iguratimod as an inhibitor of Macrophage Migration Inhibitory Factor (MIF) with Steroid-sparing potential. J Biol Chem. 2016;291:26502–26514. doi:10.1074/jbc.M116.743328
7. Brocks T, Fedorchenko O, Schliermann N, et al. Macrophage migration inhibitory factor protects from nonmelanoma epidermal tumors by regulating the number of antigen-presenting cells in skin. Faseb J. 2016;31:526–543. doi:10.1096/fj.201600860R
8. Bernhagen J, Krohn R, Lue H, et al. MIF is a non -cognate ligand of CXC chemokine receptors in inflammatory and atherogenic cell recruitment. Nat Med. 2007;13:587–596. doi:10.1038/nm1567
9. Tillmann S, Bernhagen J, Noels H. Arrest functions of the MIF Ligand/Receptor axes in Atherogenesis. Front Immunol. 2013;4:115. doi:10.3389/fimmu.2013.00115
10. Marinho CR, Nunez-Apaza LN, Martins-Santos R, et al. IFN-gamma, but not nitric oxide or specific IgG, is essential for the in vivo control of low-virulence sylvio x10/4 trypanosoma cruzi parasites. Scand J Immunol. 2007;66:297–308. doi:10.1111/j.1365-3083.2007.01958.x
11. Roger T, Schlapbach LJ, Schneider A, et al. Plasma levels of MIF and D-Dopachrome Tautomerase show a highly specific profile in early life. Front Immunol. 2017;8:26. doi:10.3389/fimmu.2017.00026
12. Almalak MK, Abdulhussein H, Alhamdi KI. Viral skin warts: clinical and histopathological characterization. J Pharm Biol Chem Sci. 2014;5:1556–1571.
13. Kindt N, Descamps G, Lechien JR, et al. Involvement of HPV infection in the release of macrophage migration inhibitory factor in head and neck squamous cell carcinoma. J Clin Med. 2019;8:75. doi:10.3390/jcm8010075
14. Shi X, Leng L, Wang T, et al. CD44 is the signaling component of the macrophage migration inhibitory factor-CD74 receptor complex. Immunity. 2006;25:595–606. doi:10.1016/j.immuni.2006.08.020
15. Mitchell RA, Metz CN, Peng T, Bucala R. Sustained mitogen-activated protein kinase (MAPK) and cytoplasmic phospholipase A2 activation by MIF: regulatory role in cell proliferation and glucocorticoid action. J Biol Chem. 1999;18:18100–18106. doi:10.1074/jbc.274.25.18100
16. Baugh JA, Donnelly SC. MIF a neuroendocrine modulator of chronic inflammation. J Endocrinol. 2003;179:15–23. doi:10.1677/joe.0.1790015
17. Tuschil A, Lam C, Haslberger A, Lindley I. Interleukin-8 stimulates calcium transients and promotes epidermal cell proliferation. J Invest Dermatol. 1992;99:294–298. doi:10.1111/1523-1747.ep12616634
18. Xu X, Wang B, Ye C, et al. Overexpression of macrophage migration-inhibitory factor induces angiogenesis in human breast cancer. Cancer Lett. 2008;261:147–157. doi:10.1016/j.canlet.2007.11.028
19. He XX, Chen K, Yang J, et al. Macrophage migration-inhibitory factor promotes colorectal cancer. Mol Med. 2009;15:1–10. doi:10.2119/molmed.2008.00107
20. Kindt N, Journe F, Laurent G, Saussez S. Involvement of macrophage migration inhibitory factor in cancer and novel therapeutic targets. Oncol Lett. 2016;12:2247–2253. doi:10.3892/ol.2016.4929
21. Bezdek S, Leng L, Busch H, et al. Macrophage Migration Inhibitory Factor (MIF) drives murine psoriasiform dermatitis. Front Immunol. 2018;9:2262. doi:10.3389/fimmu.2018.02262
22. Babu SN, Chetal G, Kumar S. Macrophage Migration Inhibitory Factor: a potential marker for cancer diagnosis and therapy. Asian Pac J Cancer Preview. 2012;13:1737–1744. doi:10.7314/APJCP.2012.13.5.1737
23. El Hamd MA, Assaf NA, Nada EA. Possible role of interleukin-17 and macrophage migration inhibitory factor in cutaneous warts. J Cosmet Dermatol. 2018;17:1250–1253. doi:10.1111/jocd.12355
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.