")
Back to Journals » Clinical Ophthalmology » Volume 15
Assessment of Knowledge and Attitude of Cataract and Their Associated Factors Among Adults in Arba Minch Zuria Woreda, Southern Ethiopia
Authors Samuel M, Abdulkadir H, Girma M, Glagn M
Received 19 May 2021
Accepted for publication 28 June 2021
Published 6 July 2021 Volume 2021:15 Pages 2913—2920
DOI https://doi.org/10.2147/OPTH.S320873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mesay Samuel,1 Hanan Abdulkadir,2 Meseret Girma,2 Mustefa Glagn2
1Wolayta Zone Health Department, Wolayta Sodo, Ethiopia; 2School of Public Health, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia
Correspondence: Hanan Abdulkadir
School of Public Health, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia
Tel +251923590013
Email [email protected]
Background: Cataract is the major cause of reversible blindness and visual impairment in developing countries. It has been assumed that there is poor access to information related to the cause, prevention, and treatment of cataract in developing countries. There is also a paucity of data on knowledge and attitude towards cataract in Ethiopia.
Purpose: This study aimed to assess the knowledge and attitude of cataract and their associated factors among adults in Arba Minch Zuria Woreda, Southern Ethiopia.
Patients and Methods: A community-based cross-sectional study was conducted among 623 adults from February 6 to April 16, 2020. The study participants were selected by the multi-stage sampling technique. Data were collected with a pre-tested structured questionnaire by using face-to-face interviews. The data were entered into Epi info version 7.2 and exported to SPSS version 23 for analysis. The level of statistical significance was set at a p-value less than 0.05 in multivariable logistic regression.
Results: Among 623 total participants, 54.9% of them had good knowledge about cataract, while 37.9% of them had favorable attitude about cataract. Inability to read and write (AOR=0.104, 95% CI: 0.042– 0.258), primary school educational level (AOR=0.208, 95% CI: 0.091– 0.478), secondary school educational level (AOR=0.199, 95% CI: 0.088– 0.451), earning average monthly income 350– 820 Ethiopian birr (AOR=2.364, 95% CI: 1.277– 4.373), not having previous eye examination (AOR=0.605, 95% CI: 0.425– 0.861) and unavailability of eye clinic (AOR=0.65, 95% CI: 0.446– 0.945) were significantly associated with knowledge of cataract. No history of cataract (AOR=0.257, 95% CI: 0.157– 0.418) was significantly associated with attitude towards cataract.
Conclusion: Significant portion of participants had poor knowledge and an unfavorable attitude towards a cataract. So, it is recommended that stakeholders in different hierarchies need to exert efforts on creating awareness about cataract by considering the education level of the community. Moreover, attention should be given to the availability and accessibility of the primary eye care unit.
Keywords: cataract, knowledge, attitude, associated factors, Arba Minch Zuria Woreda, Southern Ethiopia
Introduction
A cataract is any clouding or opacity of the eye’s lens, which can result in increased scattering of light. Lens opacity can result from the separation of protein process, the aggregation of proteins, or the disruption of the fiber cells’ regular alignment or packing.1 It can be due to congenital, developmental, and acquired causes.2 Symptoms of cataract are blurred/reduced vision, cloudy vision, glare, seeing haloes around light, and inability to see in dim light.3 The most common factors identified to influence cataract development are increasing age, sunlight (UV) exposure, trauma, smoking, steroid use, and genetics.4
In 2010,32.4 million peoples were blind and 191 million people had impaired vision globally. From this 10.8 million and 35.1 million people were blind and visually impaired due to cataract respectively. Cataract caused 33.4% of all blindness worldwide in 2010, and 18.4% of all moderate to severe vision impairment. These rates were lower in the high-income regions (<15%) and higher (>40%) in South and Southeast Asia and Oceania.5 A cataract is the major cause of blindness and visual impairment in developing countries despite it is a preventable and treatable disease.6 In Ethiopia, 50% of blindness is caused by cataract.7
Cataract has a consequent effect on the individual, family, community, and the nation as a whole on visual disability. It reduces the quality of life, independence, economic and social interaction. In developing countries, the economic impact of visual loss from cataract is huge, including loss of jobs and increase custodial care.8 Younger children are often taken out of school to look after the elderly blind, thus the children are deprived of school.9
Different studies around the world showed that there is a gap in knowledge of cataract in both developed and developing countries including Ethiopia.10–12
The lack of knowledge about the disease and its treatment is still a major obstacle in reducing blindness due to cataract in developing countries, particularly in rural areas. However, evidence on public awareness, knowledge, and attitude about cataract is not widely known and done in Ethiopia except in a few communities still these studies are mainly institution-based. Hence, this study aimed to assess the Knowledge and Attitude of adults towards Cataract and associated factors in Arba Minch Zuria Woreda, Ethiopia.
Materials and Methods
Study Area, Design, and Period
A community-based cross-sectional study was conducted from February 6 to April 16, 2020, in Arba Minch Zuria Word (district). It is one of the Gamo Zone woredas which is found around Arba Minch town and 500 km away from the capital city Addis Ababa. According to the 2007 national population and housing census from the Central Statistical Agency of Ethiopia estimated the total population at Arba Minch Zuria woreda was 123,950 of whom 60,736 are men and 63,214 of them are women.13 The woreda has 18 rural kebeles (the smallest administrative unit in Ethiopia) and 25,823 households according to the Arba Minch Zuria woreda information desk affairs office. The woreda has four health centers, twenty-six Health posts, and twenty-nine private Health facilities.
Source and Study Populations
The source population were all households with adults aged ≥ 18 years living in Arba Minch Zuria Woreda. The study population were all households with adults aged ≥ 18 years in the selected kebeles during data collection period.
Inclusion Criteria
Households with adults aged ≥ 18 years, and lived in the study area for greater than 6 months.
Sample Size Determination
A total of 633 sample size was calculated using single population proportion formula by assuming 95% confidence interval, 5% margin of error, the proportion of good knowledge 61.7% taken from Study conducted in Gondar town,11 1.5 design effect (Since multistage systematic sampling was used), and 10% non-response rate.
Sampling Procedures
A multi-stage systematic sampling method was used in the study; the first six kebeles were selected randomly by using the lottery method from a total of 18 kebeles then the sample size (633) was proportionally allocated to selected kebeles based on the size of the households. Participant’s household was selected by using systematic random sampling using k values of five. Finally, one adult is selected for interview using lottery method if there is more than one adult per household.
Operational Definition
Knowledge: To assess the level of knowledge, respondents were asked 14 questions and those who scored greater than the mean value were considered as having “good knowledge” and those who scored less than the mean value were considered as having “poor knowledge”.
Positive attitude: Study participants who score above the mean value from five attitude questions were considered as having a favorable attitude.
Negative attitude: Study participants who score below the mean value from five attitude questions were considered as having unfavorable attitude.
Data Collection Tool and Procedure
A pretested structured questionnaire was used for face-to-face interviews that include Socio-demographic and economic characteristics, knowledge and Attitude of cataract, availability of eye clinic, and previous eye examination which was prepared by reviewing different literature.10,11 Knowledge of cataract was assessed by questions which contain simple definition, symptoms, risk factors, and ways of prevention, effects, and treatment of cataract. The questionnaire was prepared in the English version and translated into Amharic and then translated back to English to maintain its consistency and accuracy. Pretest was done on 10% of the sample in Mirab Abaya woreda. After the pretest, some unclear questions were modified for clarity. Data were collected by 4 diploma nurses and supervised by two BSc Nurses. All data collectors and supervisors were trained for one day and performed practical exercises to be familiar with the questionnaire. All the questionnaires were checked for completeness and consistency on daily basis. Reliability analysis was done for attitude and knowledge measuring questions/items and the result showed a good score of internal consistency between the items with 0.844 and 0.703 Cronbach’s alpha respectively.
Data Processing and Analysis
The data were coded and entered into Epi info version 7.2 and exported to SPSS version 23 for analysis. Descriptive statistics such as mean, percent, and frequency were done. The necessary assumptions of logistic regression were checked using Hosmer and Lemeshow goodness-of-fit-test (p-value > 0.05). Bivariable analysis was done and all explanatory variables which have an association with the outcome variable at p-value <0.25 were selected for multivariable analysis. The level of statistical significance was set at a p-value less than 0.05 in multivariable logistic regression.
Ethical Consideration
Ethical clearance was obtained from Arba Minch University, College of Medicine and Health Science Institutional Review Board with IRB reference number of IRB/213/12. An official letter was written to Arba Minch Zuria Woreda Administrator, then permission was obtained from woreda and selected kebeles. Informed consent was obtained from respondents who participated in the study. All data collectors and supervisors used personal protective equipment based on WHO standards during the training and data collection period to prevent the COVID 19 pandemic disease transmission. Besides, this study was conducted in accordance with the Declaration of Helsinki, and all ethical and professional considerations were followed throughout the study to keep participants’ data strictly confidential.
Result
Socio-Demographic Characteristics
From the total sample size, 623 adults were interviewed giving a response rate of 98%. More than half, 386 (62%) of respondents were male. Greater than one-third 243 (39%) of study participants were at age category of 30–39 and the mean age of respondents was 34.5 years. The educational background of respondents showed that 96 (15.4%) cannot read and write on the other hand 76 (12.2%) were college and above. The majority of respondents 517 (83%) were married. Almost half 283 (45.4%) of the respondents earn between 820 and 1170 Ethiopian birr monthly on average (Table 1).
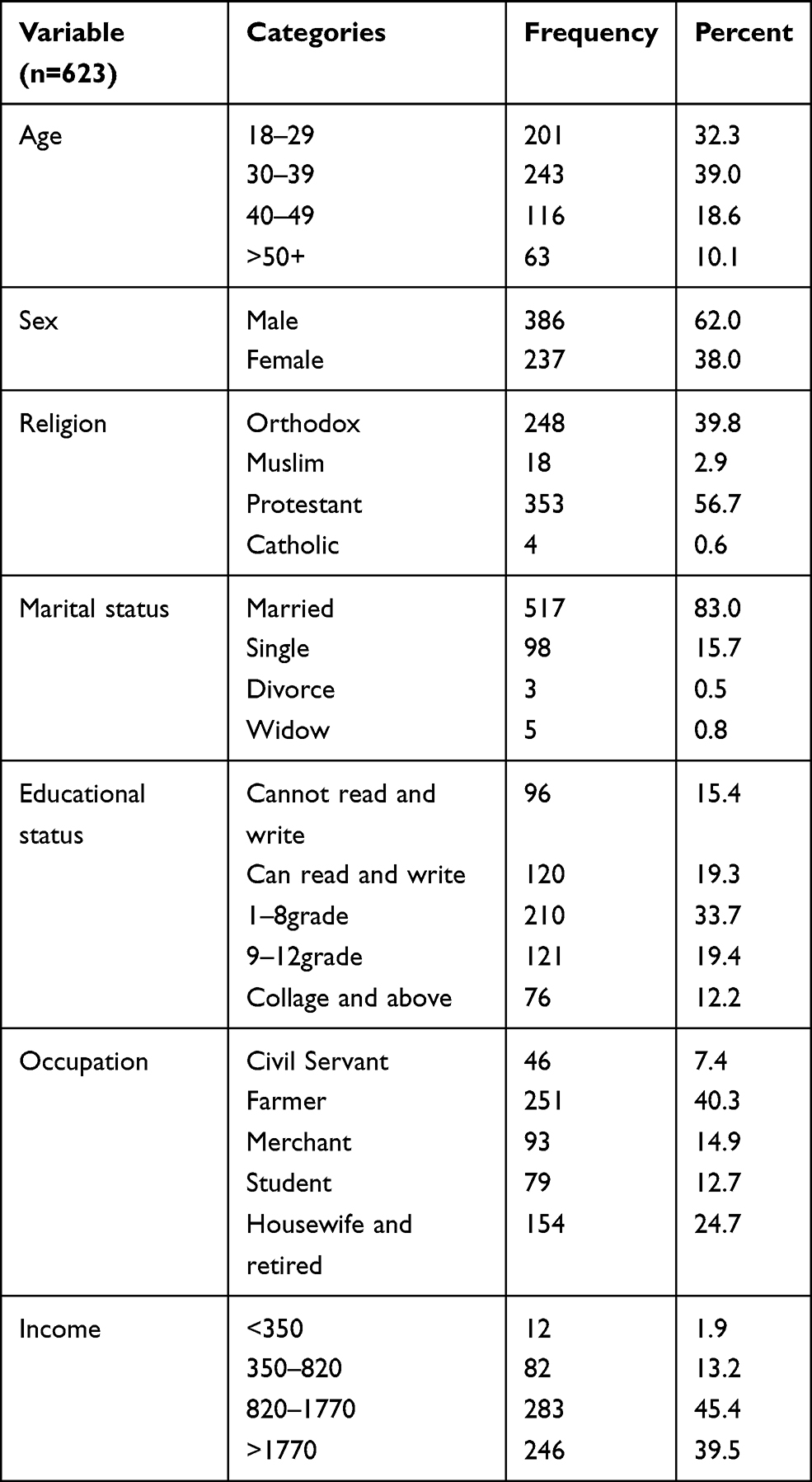 |
Table 1 Socio-Demographic and Economic Characteristics for the Study Assessing Knowledge and Attitude of Cataract and Their Associated Factors Among Adults in Arba Minch Zuria Woreda, Southern Ethiopia, 2020 |
Availability of Eye Clinic and Previous Eye Examination
Almost one-third 208 (33.4%) of respondents reported that there is no eye clinic service nearby. More than one third 280 (44.9%) of respondents have the previous history of examination. From this 78 (27.9%) of them went for eye examination when they felt eye pain and 161 (57.5%) of them had eye examination before two years ago. Less than one-fifth (13.3%) of participants had a previous self-history of cataract and 568 (91.2%) of them had a family history of cataract (Table 2).
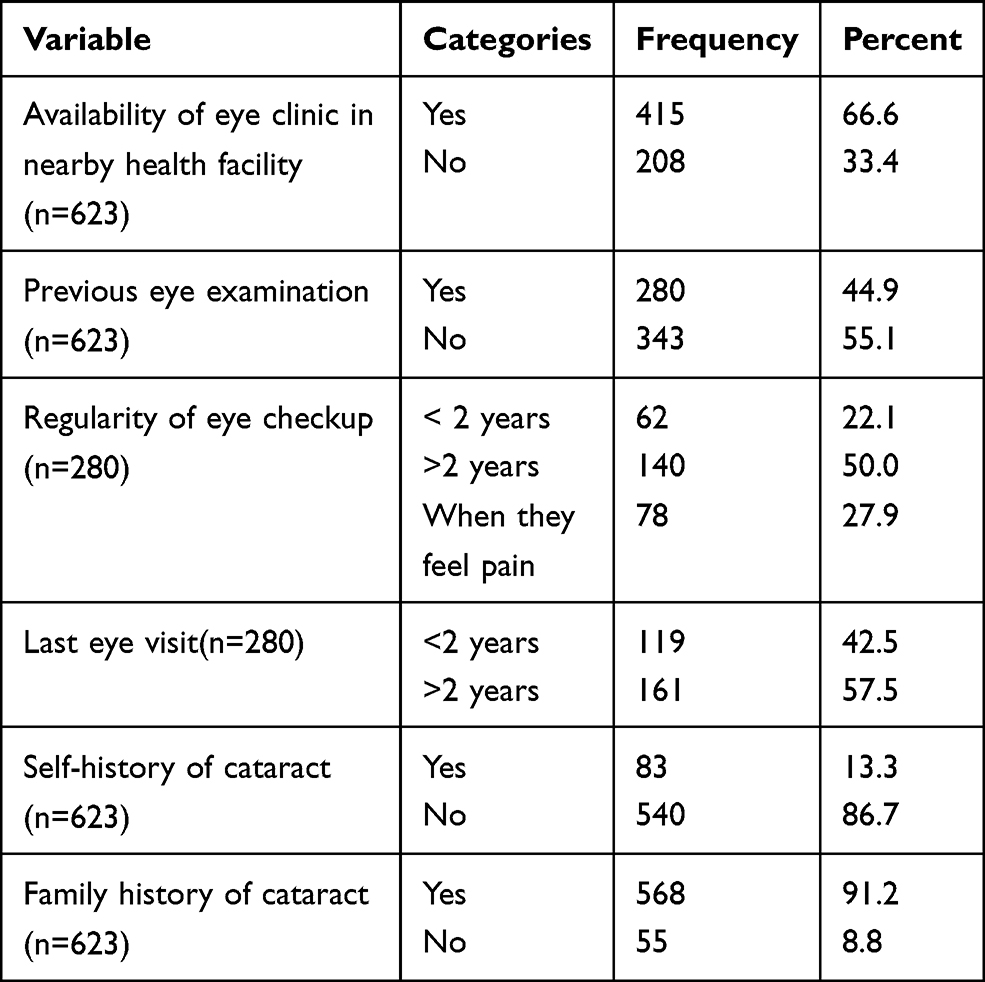 |
Table 2 Health Care System Characteristics and Previous Eye Examination for the Study Assessing Knowledge and Attitude of Cataract and Their Associated Factors Among Adults in Arba Minch Zuria Woreda, Southern Ethiopia, 2020 |
Knowledge of Cataract Among Adults
All of the respondents heard about cataract and 347 (55.7%) of them get this information from health professionals followed by 125 (20.1%) from television, 97 (15.6%) from radio and 54 (8.7%) from family. About 551 (88.4%) of participants answered the correct simple definition of cataract. More than halve 438 (70.3%) of respondents stated reduction of vision as a symptom of cataract. Regarding the risk factors, 362 (58.1%) and 350 (56.2%) of participants were recognized increased age and trauma as risk factors of cataract respectively. Most 552 (88.6%) of respondents identified impaired vision and blindness as the worst effect of cataract. More than halve 465 (74.6%) of them stated surgery as the best treatment for cataract and 40 (6.4%) of respondents cited using sunglass as prevention of cataract. Overall, 342 (54.9%) of participants had good knowledge about cataract (Table 3).
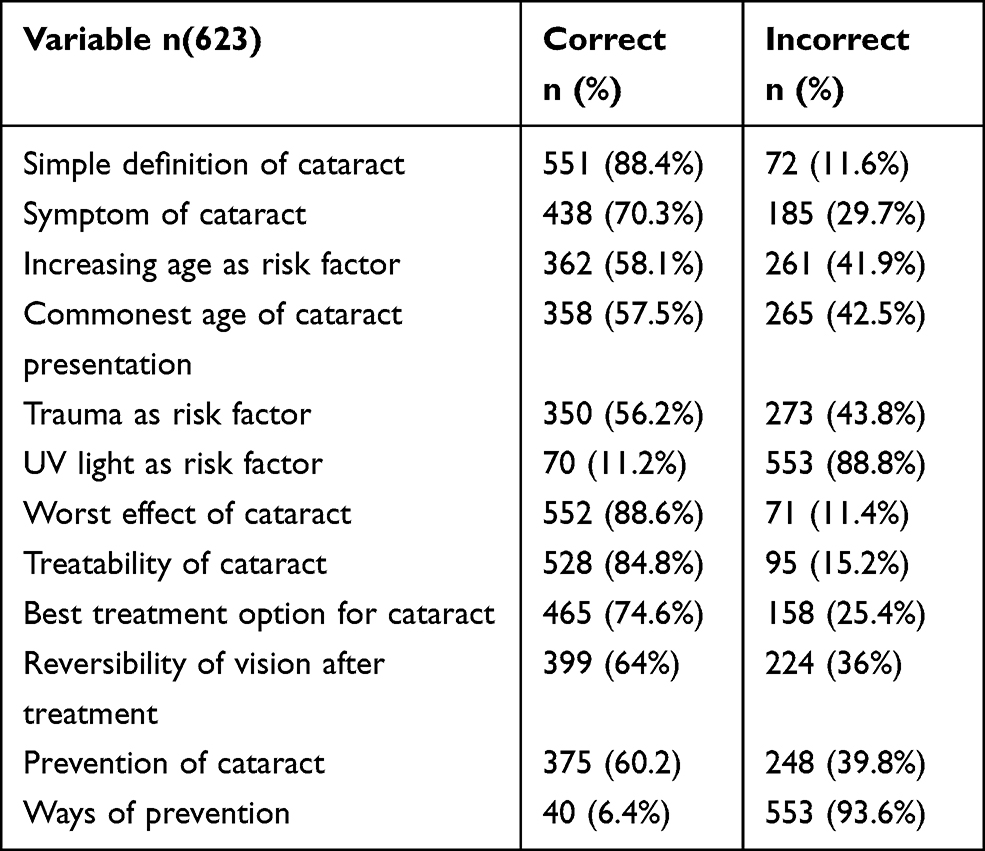 |
Table 3 Knowledge of Cataract for the Study Assessing Knowledge and Attitude of Cataract and Their Associated Factors Among Adults in Arba Minch Zuria Woreda, Southern Ethiopia, 2020 |
The Attitude of Cataract Among Adults
More than one third 218 (35%) of respondents agreed that a person with cataract needs examination and 248 (39.8%) of them agreed on seeking cataract treatment. More than one third 221 (35.5%) of participants agreed that cataract is a serious health problem and 251 (40.3%) of them agreed that people with cataract can get appropriate care in a health institution. Generally, 236 (37.9%) of participants had a positive attitude towards cataract (Table 4).
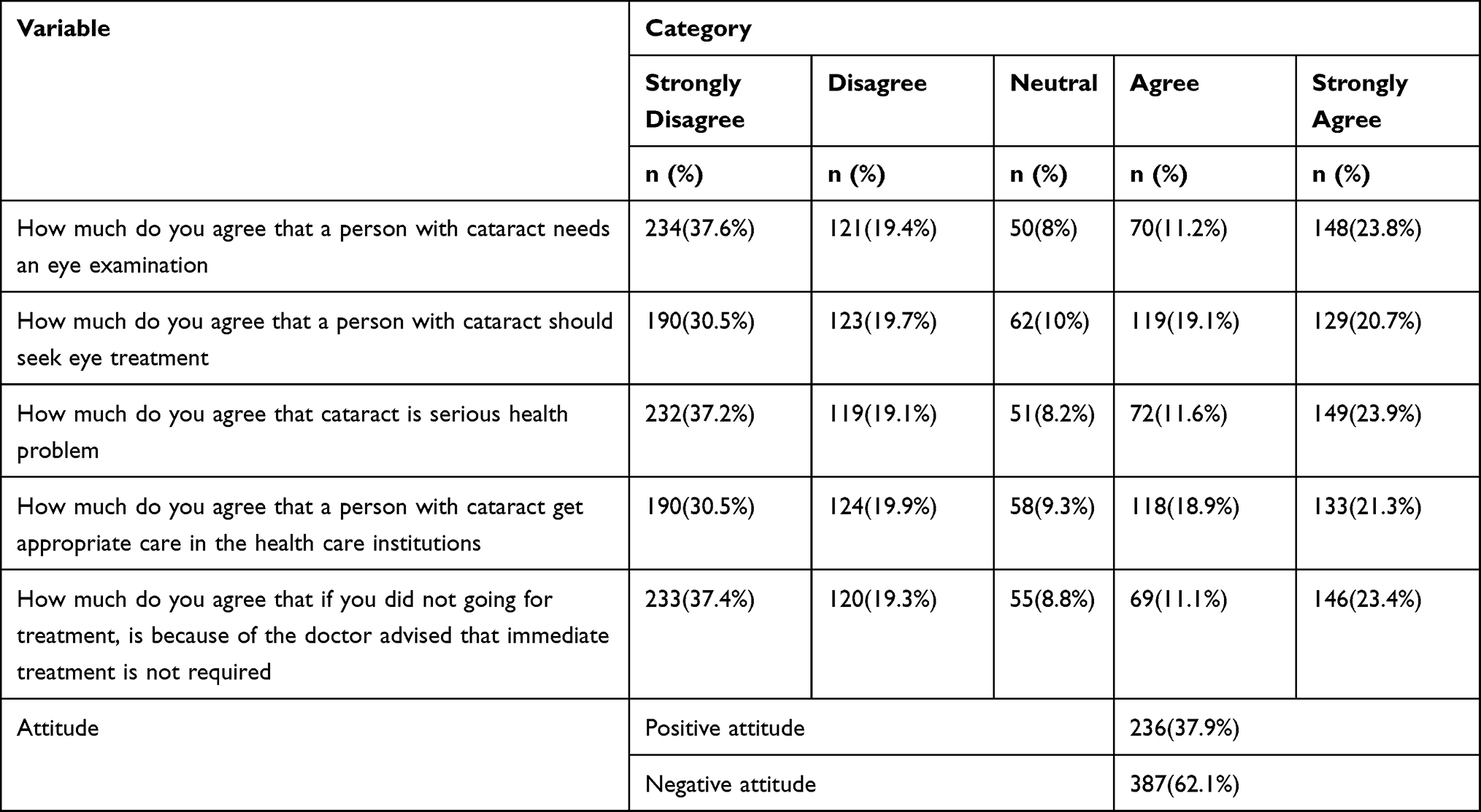 |
Table 4 Attitude of Cataract for the Study Assessing Knowledge and Attitude of Cataract and Their Associated Factors Among Adults in Arba Minch Zuria Woreda, Southern Ethiopia, 2020 |
Associated Factors of Knowledge of Cataract
The result of bivariable logistic regression analysis showed that age, sex, marital status, educational status, occupation, average monthly income, previous eye examination, and availability of eye clinic were selected as a candidate for multivariable logistic regression analysis. Then educational status, earning average monthly income between 350 and 820, previous eye examination, and availability of eye clinic showed statistically significant association with knowledge in multivariable logistic regression analysis.
Those participants who cannot read and write are 89.6% (95% CI 0.042–0.258) less likely to have good knowledge than those whose educational level is college and above. Similarly, those with the educational level of primary school are 79.2% (95% CI 0.91–0.478) less likely to have good knowledge than those whose educational level is college and above. Participants who earned 350–820 Ethiopian birr monthly are 2.36 (95% CI 1.277–4.373) more likely to have good knowledge than those who earned >1770 birr monthly. Respondents who did not have a previous eye examination are 39.5% (95% CI 0.425–0.861) less likely to have good knowledge than those who had a previous eye examination. Those participants who did not have an eye clinic nearby are 35% (95% CI 0.446–0.945) less likely to have good knowledge than those who have an eye clinic nearby (Table 5).
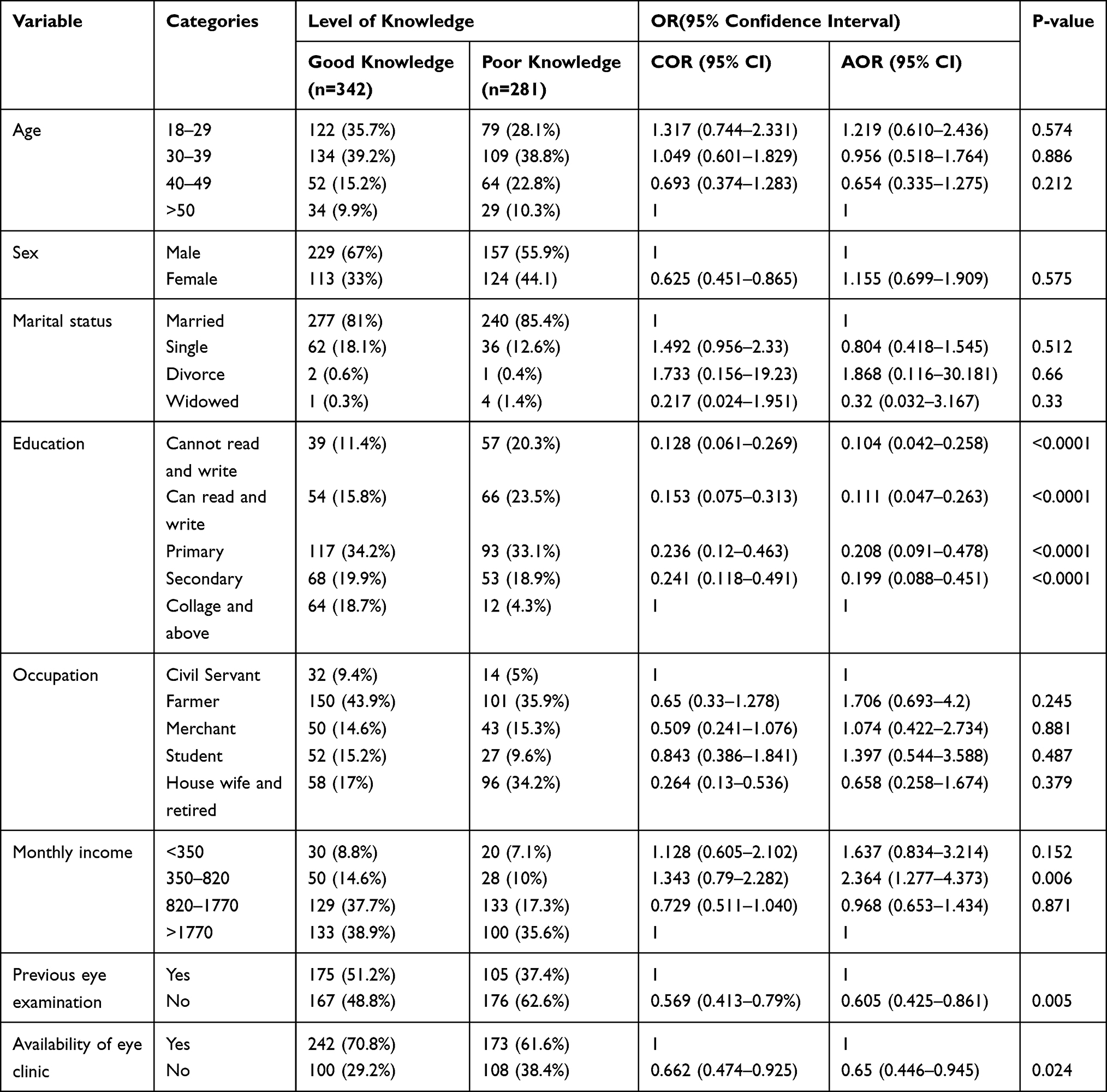 |
Table 5 Associated Factors with Knowledge of Cataract for the Study Assessing Knowledge and Attitude of Cataract and Their Associated Factors Among Adults in Arba Minch Zuria Woreda, Southern Ethiopia, 2020 |
Associated Factors for Attitude of Cataract
In bivariate logistic regression analysis age, educational status, previous eye examination, self-history of cataract, family history of cataract, and availability of eye clinic were selected as a candidate for multivariable logistic regression analysis then self-history of cataract showed statistically significant association with the attitude of cataract. Hence, those participants who did not have a self-history of cataract are 74.3% (95% CI 0.157–0.418) less likely to have a positive attitude than those who had self-history of cataract (Table 6).
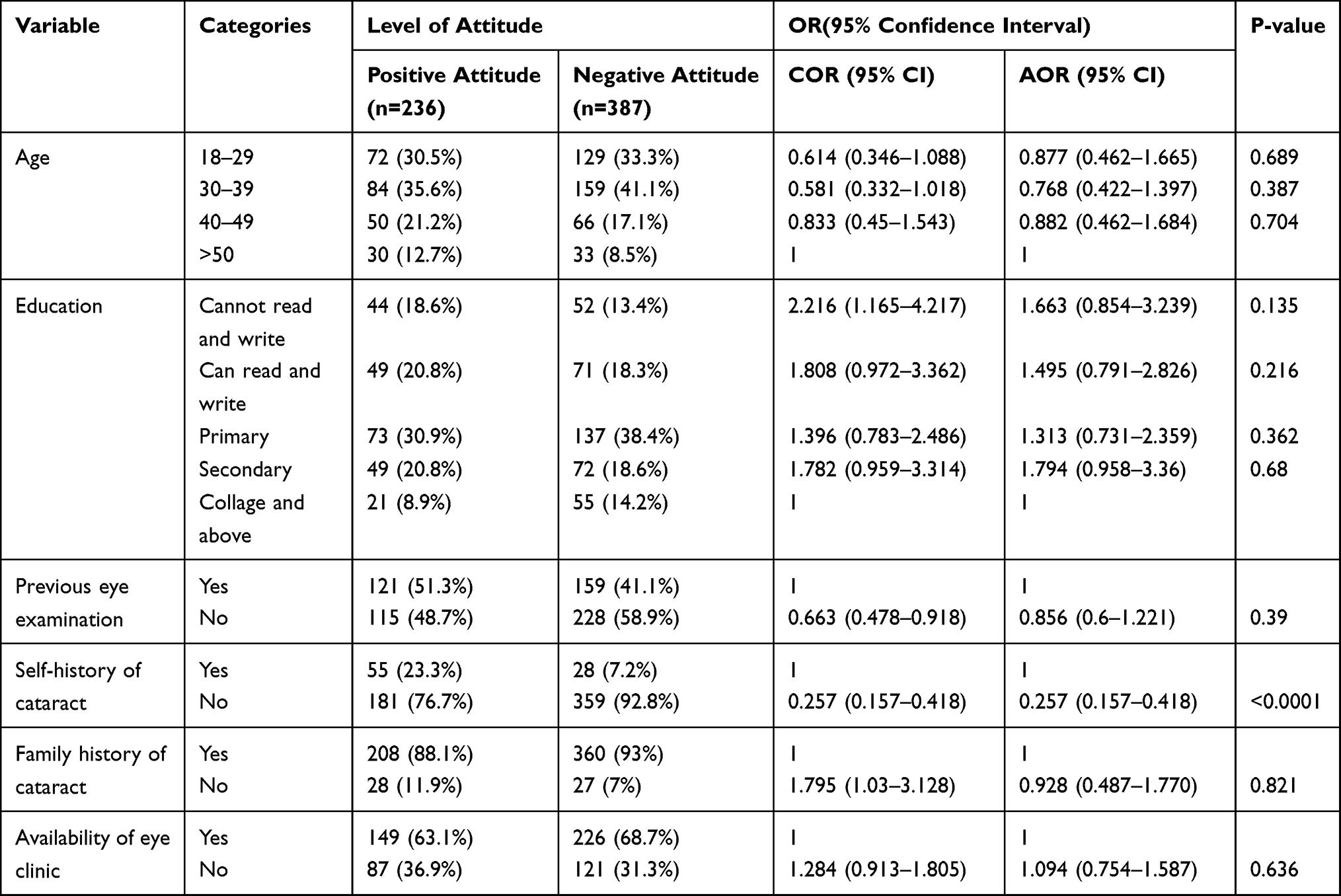 |
Table 6 Associated Factors with the Attitude of Cataract for the Study Assessing Knowledge and Attitude of Cataract and Their Associated Factors Among Adults in Arba Minch Zuria Woreda, Southern Ethiopia, 2020 |
Discussion
This study showed that 54.9% of study participants had good knowledge about cataract. This finding was lower than studies done in China (70.9%),14 Nepal (70.4%),15 Iran (74%),16 Gondar town, North West Ethiopia (61.7%),11 and Yirgalem town, Southern Ethiopia (64.7%).17 But the finding was higher than studies done in Southern India (18%)12 and Nigeria (18.2%).10 These variations can be explained by cut-off points used to measure the composite score of knowledge, the difference in the target population, and the study setting.
Participants who cannot read and write and with primary educational level were 89.6% and 89.2% less likely to have good knowledge than those whose educational level is college and above. This finding is similar to the studies done in Canada,18 Nigeria,10 Gondar town,11 and Yirgalem town.17 This might be due to the reason that individuals with higher educational levels tend to read and explore more. They may also understand information related to cataract easily so that they would become knowledgeable.
Respondents who earned 350–820 Ethiopian birr monthly are 2.36 more likely to have good knowledge than those who earned >1770 monthly. This result is not consistent with the studies done in Bangladesh19 and Gondar town.11 Further research is needed to reason out this discrepancy.
The study finding showed that Respondents who did not have previous eye examinations are 39.5% less likely to have good knowledge than those who had a previous eye examination. This finding is similar to a study done in Gondar town.11 This might explain that individuals who had previous eye examinations may get information from health professionals, posted information in the clinic and from patients.
Those participants who did not have an eye clinic nearby are 35% less likely to have good knowledge than those who have an eye clinic nearby. This might explain that the availability of an eye clinic nearby may help individuals to have an eye examination and also to access information easily.
The study result showed that the overall attitude of the study participants towards cataract was 37.9%. This finding is comparable with the study done in Yirgalem town (35.3%).17
Study participants who did not have a self-history of cataract were 74.3% less likely to have good knowledge than those who have self-history of cataract. This might be due to the reason that an individual with a history of cataract may go to an eye clinic and get information. Also, may experience the consequences and treatment options which may lead the individual to have a positive attitude.
The limitations of this study were recall bias and being cross-sectional in the design, which does not establish a temporal relationship between cause and effect.
Conclusion
A significant portion of study participants had poor knowledge and a negative attitude towards cataract. Which were significantly associated with low educational level, earning an average monthly income of 350–820 Ethiopian birr, not having previous eye examination, unavailability of the eye clinic, and no previous self-history of cataract. So, it is recommended that stakeholders in different hierarchies need to exert efforts on creating awareness about cataract by considering the education level of the community. Moreover, attention should be given to the availability and accessibility of the primary eye care unit.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhao M, Gillani AH, Amirul Islam FM, —. Factors associated with knowledge, attitude and practices of common eye diseases in general population: a multicenter cross-sectional study from Pakistan. Int J Environ Res Public Health. 2019;16:1568.
2. Stevens GA, White RA, Flaxman SR, et al. Global prevalence of vision impairment and blindness: magnitude and temporal trends. Ophthalmology. 2013;120(12):2377–2384. doi:10.1016/j.ophtha.2013.05.025
3. Khurana AK. Comprehensive Ophthalmology.
4. Batlle JF, Lansingh VC, Silva JC, Eckert KA, Resnikoff S. The cataract situation in Latin America: barriers to cataract surgery. Am J Ophthalmol. 2014;158(2):242–250. doi:10.1016/j.ajo.2014.04.019
5. Khairallah M, Kahloun R, Bourne R, Limburg H, Flaxman SR. Number of people blind or visually impaired by cataract worldwide and in world regions. Invest Ophthalmol Vis Sci. 2015;56(11):6762–6769. doi:10.1167/iovs.15-17201
6. Rao GN, Khanna R, Payal A. The global burden of cataract. Curr Opin Ophthalmol. 2011;22(1):4–9. doi:10.1097/ICU.0b013e3283414fc8
7. Berhane Y, Worku A, Bejiga A, et al. Prevalence and causes of blindness and low vision in Ethiopia. Ethiop J Health Dev. 2007;21(3):204–210.
8. Chang JR, Koo E, Agrón E, Hallak J, Clemons T. Risk factors associated with incident cataracts and cataract surgery in the age-related eye disease study (AREDS). Ophthalmology. 2011;118(11):2113–2119. doi:10.1016/j.ophtha.2011.03.032
9. Ellwein LB. Strategic issues in cataract blindness prevention in developing countries. Bull WHO. 2015;73(3):681–690.
10. Onwubiko S, Udeh N, Okoloagu N, Chuka-Okosa C. Knowledge and attitudes towards eye diseases in a rural South-eastern Nigerian population. J Health Care Poor Underserved. 2015;26(1):199–210. doi:10.1353/hpu.2015.0013
11. Alimaw YA, Hussen MS, Tefera TK, Yibekal BT. Knowledge about cataract and associated factors among adults in Gondar town, northwest Ethiopia. PLoS One. 2019;14:e0215809. doi:10.1371/journal.pone.0215809
12. Dandona RDL, John RK, McCarty CA, Rao GN. Awareness of eye diseases in an urban population in southern India. Bull World Health Organ. 2001;79(2):96–102.
13. Central Statistical Authority of Ethiopia (CSA). Population and housing census of Ethiopia: statistical abstract. Addis Ababa, Ethiopia: CSA; 2007.
14. Qiu C, Feng X, Zeng J, Luo H, Lai Z. Discharge teaching, readiness for discharge, and post-discharge outcomes in cataract patients treated with day surgery: a cross-sectional study. Indian J Ophthalmol. 2019;67(5):612–617. doi:10.4103/ijo.IJO_1116_18
15. Thapa SS, Berg RV, Khanal S, et al. Prevalence of visual impairment, cataract surgery, and awareness of cataract and glaucoma in Bhaktapur district of Nepal: the Bhaktapur Glaucoma Study. BMC Ophthalmol. 2011;11(1):2. doi:10.1186/1471-2415-11-2
16. Hashemi H, Pakzad R, Yekta A, et al. Global and regional prevalence of age-related cataract: a comprehensive systematic review and meta-analysis. Eye. 2020;34(8):1357–1370. doi:10.1038/s41433-020-0806-3
17. Anteneh F, Yonatan G, Elias A, Henok B. Knowledge about cataract and associated factors among adults in Yirgalem town. BMC Ophthalmol. 2021;21:79.
18. Noertjojo K, Maberley D, Bassett K, Courtright P. Awareness of eye diseases and risk factors: identifying needs for health education and promotion in Canada. Can J Ophthalmol. 2006;41:617–623.
19. Islam FMA, Chakrabarti R, Islam SZ, Finger RP, Critchley C. Factors associated with awareness, attitudes and practices regarding common eye diseases in the general population in a Rural District in Bangladesh: the Bangladesh population-based diabetes and eye study (BPDES). PLoS One. 2015;10(7):e0133043. doi:10.1371/journal.pone.0133043
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.