Back to Journals » Integrated Pharmacy Research and Practice » Volume 11
Assessment of Inventory Management Practice and Associated Challenges of Maternal, Newborn, and Child Health Life-Saving Drugs in Public Hospitals of Southwest Ethiopia: A Mixed-Method Approach
Authors Bekele A ![]() , Kumsa W, Ayalew M
, Kumsa W, Ayalew M ![]()
Received 18 June 2022
Accepted for publication 2 September 2022
Published 7 September 2022 Volume 2022:11 Pages 139—149
DOI https://doi.org/10.2147/IPRP.S378340
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Jonathan Ling
Azmeraw Bekele,1,2 Wondwosen Kumsa,3 Mihret Ayalew4
1Department of social and administrative pharmacy, Jimma University, Jimma, Ethiopia; 2School of Pharmacy, Institute of Health, Jimma University, Jimma, Ethiopia; 3Jimma University Medical Center, Jimma University, Oromia, Ethiopia; 4Department of Pharmacology, Institute of Health Science, Jimma University, Jimma, Ethiopia
Correspondence: Azmeraw Bekele, Department of social and administrative pharmacy, Institute of Health, Jimma University, Jimma, Ethiopia, Email [email protected]
Introduction: Maternal, newborn, and child health is a global priority, while most countries in sub-Saharan Africa have a poor implementation of maternal, newborn, and child health programs.
Objective: To assess inventory management practice and associated challenges of maternal, newborn, and child health life-saving drugs in public hospitals of Jimma zone and Jimma city.
Methods: Hospital-based mixed-method cross-sectional study was conducted from October 1 to 30, 2020. The quantitative data was collected using physical inventory and document reviews. Thus, seventy-eight bin cards and annual report and resupply forms were reviewed, and the collected data was analyzed using SPSS |Version 24| software. Statistical significance was determined at p < 0.05. Twelve semi-structured in-depth interviews were conducted to collect qualitative data and analysed manually using a thematic analysis technique.
Results: About half of the evaluated drugs experienced 22 stock-outs per year with a stock-out rate and mean stock-out duration of 83.3% and 1.69 months, respectively. All hospitals placed at least one emergency order. The wastage rate of products was 13.1%. The data quality of report and resupply forms such as the average data accuracy of 396 (84.61%) had a significant association with the increasing level of education, X2 (16, N = 13) = 297.7, p = 0.019. Thirty-five (97.22%) reports and resupply forms were complete, while 24 (66.67%) of them were submitted to suppliers as per the predetermined timeline with an annual reporting rate of 94.44%.
Conclusion: Data quality of bin card records was more promising than report and resupply form reports. All hospitals encountered at least one stock-out and one emergency order per year. The wastage rate was twice more than the national normal. Storage management, human asset, and capacity building challenges were identified as inventory management challenges.
Keywords: inventory management practice, challenge, MNCH, Ethiopia
Introduction
Sustainable Development Goal 3.2 aims to end preventable child mortality, reduce neonatal mortality to less than 12 per 1000 live births, and reduce under-child mortality to less than 25 children per 1000 live births per country by 2030.1 On the other hand, neonatal and under five mortality remains slower in developing countries, which suffers from 80% of women’s deaths and 44% of all childhood deaths every single day from preventable causes.2 Indeed, most sub-Saharan African countries had a low implementation of maternal, newborn, and child health programs due to operational and management inefficiency, poor quality of health services, inequities in the distribution of the health workforce, and low capacity of planning, budgeting, and controlling programs.3 Accordingly, the main Global Strategy for Women’s and Children’s Health should be improving financing, policy, and service delivery for the most vulnerable women and children.4 Suitably, in 2012, the United Nations Commission on the life-saving commodity for every woman and child movement started5 and endorsed an initial list of 13 unnoticed life-saving drugs that, if more commonly accessed and properly used, could save the lives of more than 6 million women and children.6 Yet, there are persistent disparities in the availability and accessibility of life-saving drugs due to the costly and complex nature of pharmaceutical supply chain management.7 A fragile drug supply management system and inappropriate ways of managing inventories results in wastage, over- or under-stocking, loss, increased out-of-pocket expenditure, and a decline in the quality of MNCH services.8 Studies conducted in Zambia and Nigeria identified a limited storage capacity, lack of reliable data, lack of adequate human resources, and poor performance of health care workers.9 Likewise, in Kenya, inappropriate use, wastage, and MNCH drugs were reported out of stock following inadequate procurement and inventory management practices and poor data quality of logistic records and reports.10 Studies showed that maintaining the optimal stock level and avoiding wastages are major challenges of pharmaceutical inventory management, and successful interventions are required to ensure usable stocks and reduce preventable wastages of life-saving drugs.7,11,12 Correspondingly, in Ethiopia, the data quality of logistic records and reports was low and resulted from drug stock-out and wastage.11 Furthermore, assessing the existing inventory management practice is required13 to intervene and achieve health sector targets.14 Thus, this study aimed to assess the inventory management practice and associated challenges of Life-Saving MNCH drugs in selected public hospitals of Jimma zone and Jimma city.
Methods
Study Area
The study was conducted in Jimma city and Jimma Zone public hospitals. Jimma city is surrounded by Jimma Zone, and it is one of 17 Zones in the Oromia region located in southwest Ethiopia, 365 km away from the capital city Addis Ababa. A total of 770 health facilities are found in the Zone and the City. Out of them, 7 public hospitals were found in both Jimma Zone and City serving a total population of 2,486,155 (Source: human resource and program offices of Jimma zone and city).
Study Design and Period
A hospital-based mixed-method cross-sectional study was conducted from October 1 to 30, 2020. The qualitative concurrent explanatory approach was used for the triangulation to advance the results of the quantitative research with qualitative findings.15
Study Units and Participants
The study parts were all public hospitals in Jimma City and the Jimma zone including bin card records, reporting and resupply forms (RRFs), internal facility reporting and resupply forms (IFRRs), and selected MNCH life-saving drugs. As well, pharmacy heads, store managers, and dispensary unit coordinators participated in the study.
Eligibility Criteria
All public hospitals functioned at least for a year before data collection and respondents involved in inventory management of MNCH drugs for six years and above were included. On the other hand, private and army hospitals in both Jimma zone and Jimma City were excluded from the study because program drugs were resupplied differently. One hospital (Shene Gibe general hospital) used as a coronavirus-19 service center at the time of data collection was excluded. Respondents unwilling to participate and absent during the data collection period were excluded from the study.
Sample Size and Sampling Process
Out of the total seven public hospitals found in both Jimma city and zone, six hospitals were eligible for this study. Thus, six hospitals were included in the actual study excluding the one (Shene Gibe general hospital) used for the coronavirus-19 service center. Based on the United Nations endorsement of 2016, all of the 13 MNCH life-saving drugs16 were considered. The sample size of logistics records and reports was determined by the Ethiopian Integrated Pharmaceutical Logistics System, which states that hospitals and health centers should submit RRF reports every two months to their corresponding suppliers.17 Furthermore, the Logistics Indicators Assessment Tool (LIAT) revealed that a quantitative logistics health facilities assessment is recommended to review RRF reports for a minimum of six months18 which is about three reports (1 RRF bimonthly is equivalent to three RRF reports within six months) from each hospital. To increase the generalizability of the study, the 6-monthly reports (generated per year) were included in the study. Thus, 36 RRF reports (6 RRF reports from each facility and a total of 6 hospitals ie 6 × 6=36) and 78 bin cards (13 drugs per hospital ie 13 × 6= 78) were reviewed.
Data Collection Procedures
The data were collected by three data collectors, who had received two hours of training about study objectives and questionnaire administration, using semi-structured questionnaires and checklists adapted from LIAT and inventory management assessment tools.18,19 The data were gathered through in-depth interviews, observation, a physical count of drugs, and a review of selected logistics management information system (LMIS) tools (one-year RRFs, bin card records, and IFRRs).
The Qualitative Study
Regarding the qualitative data, twelve in-depth interviews were conducted with the key informants. Thus, six store managers and six pharmacy heads based on their position for information to identify challenges related to inventory management of MNCH life-saving drugs. Interviews were interactive and conducted by one of the researchers with a witness among the data collectors, using a semi-structured interview guide (Supplementary File-1) adapted from the logistics system assessment tool,20 a tool designed to guide a qualitative logistics system assessment, and each key informant interview lasted between 25 and 30 minutes. The collected data were analysed manually using a thematic approach after authors closely examined and familiarized themselves with responses by taking notes, then coded using an Excel sheet. Finally, results were reported using texts.
Data Quality Assurance
A pilot study was conducted in a hospital excluded from the actual study to check the content and consistency of the data collection tools. Two hours of training were given for data collectors regarding the data collection tools and processes. The data collection was closely supervised throughout the data collection process by one of the researchers for data consistency and completeness.
Data Processing and Analysis
After checking for completeness and consistency of information, the computable data were entered into Epi-data software version 3.1. Then, the output was exported to a statistical package for Social Science (SPSS) version 24 for analysis. Statistical values were determined significant at p < 0.05. Finally, results were presented using texts, tables, and graphs. The following standard indicators were used to measure quantifiable variables but it is difficult to measure the overall inventory management practice using a single indicator.21
Operational Definitions
Stock Wastage: unusable item over the total items value during the review period and the acceptable standard was <2%.22
Data quality of RRF reports: It is the measurement of data accuracy, completeness, timeliness, and facility reporting rate.23
Completeness of reports: a report is considered complete if all the columns for each product listed in the report are filled unless the facility does not manage the product.23
Timelines of reports: as per the standard operating procedure of the integrated pharmaceutical logistics system of Ethiopia;17
- Hospitals and health centers should submit their RRF report to the Ethiopian pharmaceutical agency or zone health department until the 10th day of the next month.
- Health centers that send their RRF report via the district health office should submit their RRF to the district health office until the 5th day of the next month of the reporting period.
Bin card updated: if the bin card was last updated with a balance of zero and the facility has not received any of those products within the previous 30 days.23
Data accuracy: Data is accurate when there is no discrepancy between stock balances on the bin card record (manual, electronic) compared with the physical count and the balance on the bin card to the balance on the RRF report; inventory accuracy was good if (≥80%).22
Near accurate report: The report is considered to be near accurate if a ±10% discrepancy between the balance on the bin card to the physical count and the RRF report is considered near accurate.23
Acceptable storage conditions: Health facility storage condition is said to be acceptable if that facility has fulfilled at least 80% of the criteria for acceptable storage conditions.22
Results
Availability and Utilization of LMIS Tools
The availability and utilization of LMIS tools such as bin card records, RRF, and IFRR reports were available and used by all study facilities.
Bin Card Updating Practice
Out of the total bin cards, 65 (83.33%) of them were updated. It was determined that bin card updating practice had statistically significant association with the increasing the level of education, X2 (1, N = 13) = 79.02, p = 0.048, years of experience, X2 (1, N = 13) = 193.60, p = 0.004 and receiving LMIS training, X2 (1, N = 13) = 54.1, p = 0.025. Furthermore, the range of bin card updating practices varied among lifesaving MNCH drugs (Table 1).
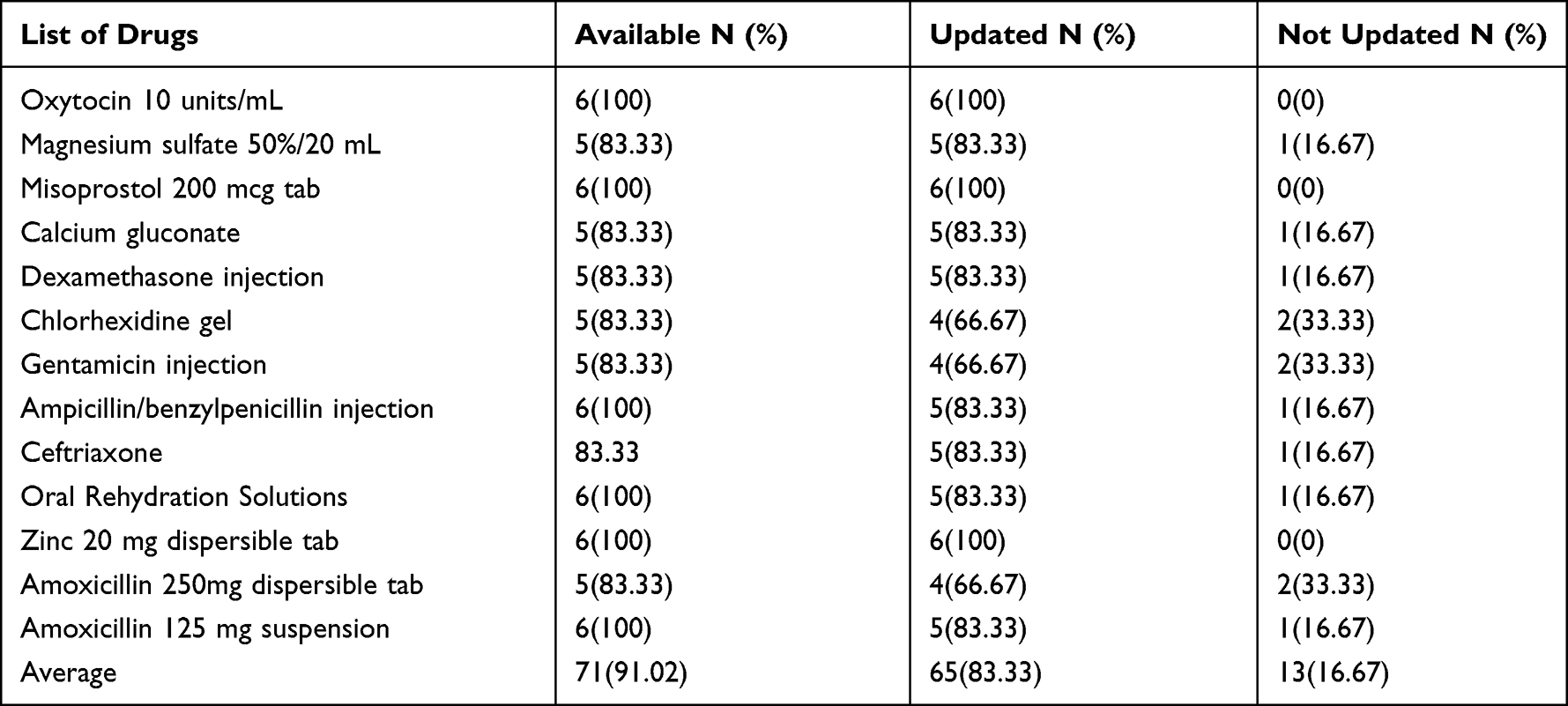 |
Table 1 Bin Card Updating Practice in Hospitals of Jimma City and Jimma Zone, 2020 |
Data Accuracy of Bin Cards
The average bin card accuracy was 59 (90.77%) ranging from 75% for Chlorhexidine gel and Gentamicin injection to 100% for Magnesium sulfate 50%/20 mL, Misoprostol 200 mcg tablet, and Amoxicillin 250mg dispersible tablet (Table 2).
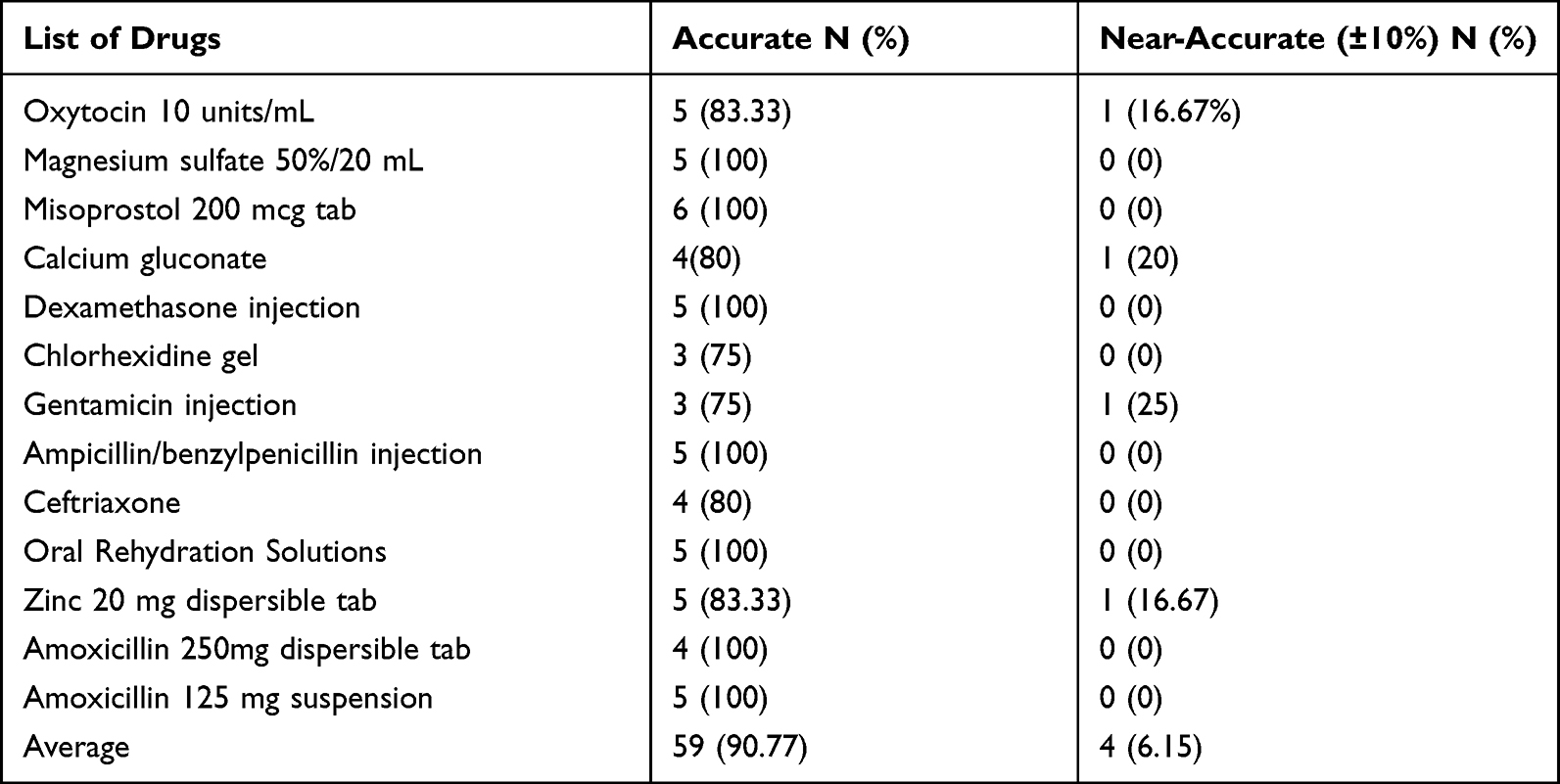 |
Table 2 Data Accuracy of Bin Cards in Hospitals of Jimma City and Jimma Zone, 2020 |
Data Accuracy of RRF Reports
The average data accuracy of RRF reports was 396 (84.61%) and ranging from 36 (100%) to 24 (66.66%) (Table 3). The annual average data accuracy of RRF reports was 84.61% with a reporting rate of 34 (94.44%). Most of the RRF reports were completed 35 (97.22%) and timely reported 24 (66.67%). The chi-square test was computed and found that the accuracy of RRF reports was significantly associated with the increasing level of education, X2 (16, N = 13) = 297.7, p = 0.019. Yet, there was no statistically significant association between the accuracy of RRF reports and years of experience, X2 (8, N = 13) = 134.4, p = 0.097, and LMIS training, X2 (5, N = 13) = 54.1, p = 0.368.
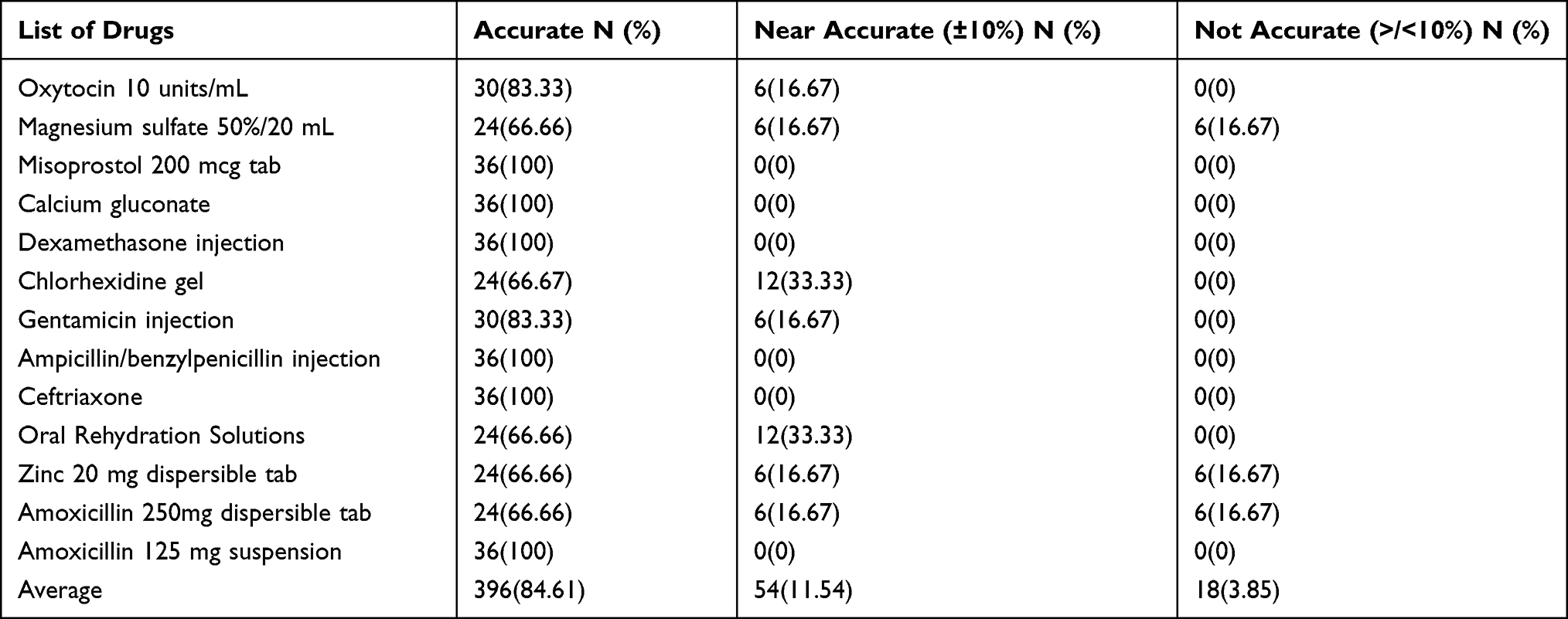 |
Table 3 Data Accuracy of RRF Reports in Hospitals of Jimma City and Jimma Zone, 2020 |
Availability of MNCH Drugs
The availability of lifesaving MNCH drugs was 59 (75.64%). Oxytocin 10 units/mL and Ampicillin or benzylpenicillin injection were mostly found in the normal stock level. Calcium gluconate 4 (66.66%) and oral rehydration solutions 5(83.33%) were the most overstocked products (Table 4).
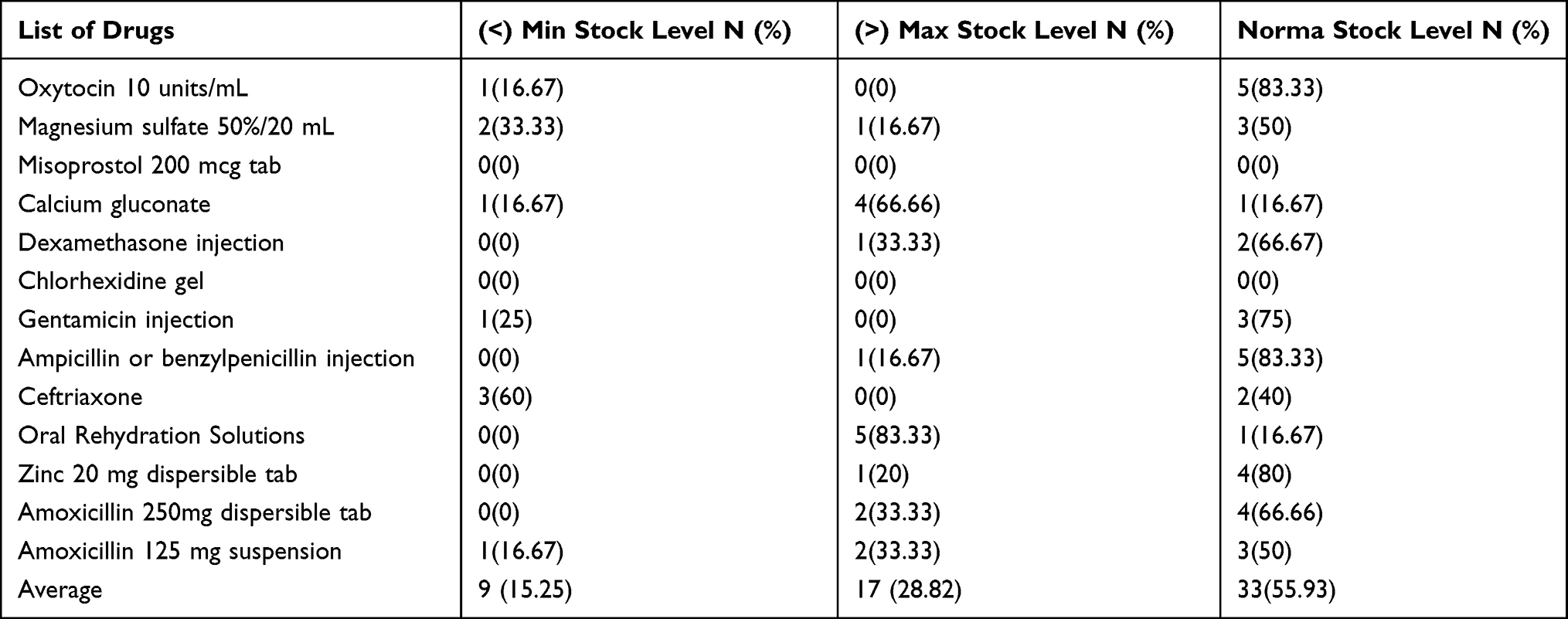 |
Table 4 Stock Status During the Hospital Visit of Jimma City and Jimma Zone, 2020 |
Stock-Out of MNCH Drugs
About half of the drugs had 22 stock-outs in a year with a stock-out rate and mean stock-out duration of 83.3% and 1.69 months, respectively. Misoprostol 200 mcg and Chlorhexidine gel were the most stocked-out items (Table 5).
 |
Table 5 Number of drug stock out within the past six months in Hospitals of Jimma City and Jimma Zone, 2020 |
Emergency Ordering
This study revealed that all hospitals placed at least one emergency order a year. The majority, 4 (66.67%) of the hospitals placed one or two emergency orders and the other 2 hospitals placed 2 and more emergency orders per year. Two-thirds of the hospitals waited for one to two months to receive their orders, and the fastest orders were filled between two to four weeks.
Wastage of MNCH Drugs
About half of the lifesaving MNCH drugs were wasted due to expiration, damage or failure to practice the first expired first out (FEFO) stock rotation principle. The wastage rate was determined by using unusable stock divided by the sum of the usable and unusable stock value obtained from model 19 (receiving voucher). The total value of usable stocks was 14,534 Ethiopian Birr (ETB), while unusable stock (expired or damaged) accounted for 2183 ETB per year (Figure 1) with a wastage rate of 13.1%.
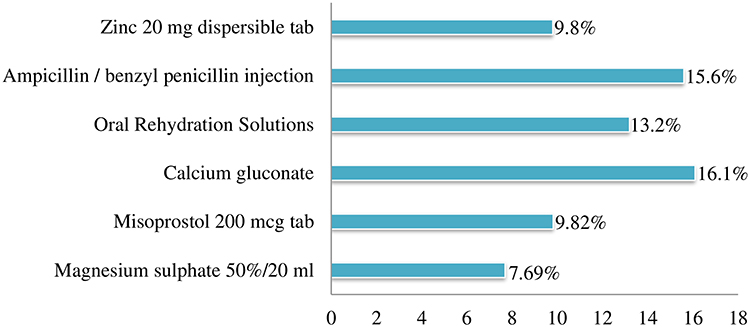 |
Figure 1 Percentage of wasted drugs in hospitals of Jimma city and Jimma zone, 2020. |
Reasons for Product Wastage
This study identified three major reasons for the wastage of lifesaving MNCH drugs such as product expiration, receiving near the expired product, and failure to practice FEFO (Figure 2) stock rotation, which varies among the type of drugs.
 |
Figure 2 Reasons of drugs wastage in hospitals of Jimma city and Jimma zone, 2020. |
Storage Conditions
Five (83.33%) out of the six hospitals fulfilled the criteria of acceptable storage condition (at least 80% of 13 criteria) with an average fulfilled criteria of 65 (83.33%). Out of the 13 criteria for acceptable storage conditions, products stacked at least 30 cm away from the walls were the least fulfilled criteria (Table 6).
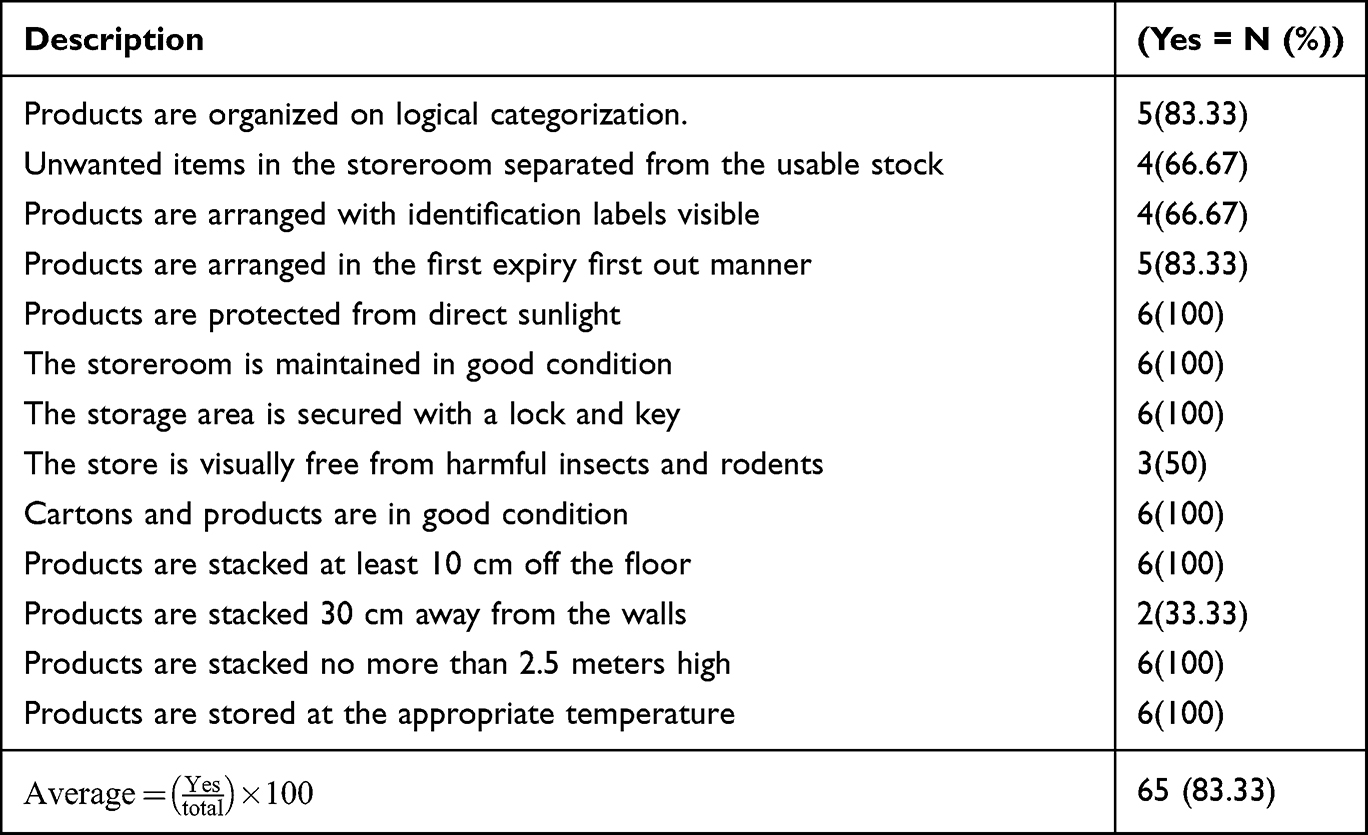 |
Table 6 Storage Practices of Selected Drugs in Hospitals of Jimma City and Zone, 2020 |
Qualitative Findings
Twelve in-depth interviews were conducted with store managers and pharmacy heads based on their position for information to identify challenges related to storage management and inventory control with immediate possible solutions.
Storage Management-Related Challenges
The results from the in-depth interview identified inadequate human resources following high staff turnover and a lack of financial incentives. Almost all hospitals experienced deprived staff commitment in updating bin card records, lack of supportive supervision, and inadequate storage space. A pharmacy head in one of the study hospitals replied that;
We are required to submit RRF reports every two months, but suppliers do not fulfill orders according to our requirements, especially in terms of item quantities. This has an undesirable effect that we have identified as misappropriation of information.
Human Resource-Related Challenges
Assessment of the current study identified the lack of close monitoring and frequent staff turnover. Furthermore, lack of supportive supervision, weak management cooperation, and lack of incentives are identified across all hospitals. One of the key informants reacted as follows;
Our staff has to endure heavy workload and sometimes one member is required to work as store manager and dispenser in pharmaceutical service units. In addition, dispensing units send their request to the store as an urgent order outside the predetermined schedule. So, we don’t have time to save and compile reports.
Capacity Building-Related Challenges
The present study found that on-job training, supportive supervision, and experience sharing with good-performing institutions were unsuccessfully implemented. Even though the hospitals tried to create decent working conditions using a kaizen approach, minimum efforts were made by higher health facilities and hospital administrations. Thus, disengagement of staff, manipulating reports, and lack of commitment were common among hospitals. One of the pharmacy heads replied to the situation as follows;
We do not have enough qualified personnel to compute e-registration tools in a complete and timely manner. As we believe that training can fill these skills gaps, some training has been provided in limited numbers and most of them have been misused by the management as a tool of income.
Discussions
Appropriate inventory management practices are critical to avoiding stock-out and ensuring the data quality of logistics records and reports.24 Bin card updating practice is one of the key measures to convey reliable and consistent logistic information. The present study showed that the overall bin card updating practice was 65(83.33%), which is significantly associated with the increasing the level of education, X2 (1, N=13) = 79.02, p=0.048, years of experience, X2 (1, N=13) = 193.60, p=0.004 and LMIS training, X2 (1, N=13) = 54.1, p=0.025. Proper implementation of LMIS is 3.3 times more likely to be efficient than in the case where there are no proper LMIS services.25 To this point, the current figure, 83.3% is higher than the previous similar practice (33.5%) but below the national normal (100%).22 The larger the current figure might be because of the expansion of electronic health commodity management information systems as indicated by the qualitative finding. Regarding the data quality of RRF reports, an average of 396 (84.61%) reports were filled correctly with a reporting rate of 34(94.44%). This is nearly similar to the accuracy of RRF reports reported in Cameroon 75% and Burundi 90%.26 As well, our finding found that most RRF reports were complete 35 (97.22%) and timely reported 24 (66.67%), which implies that some RRF reports were submitted late and remain incomplete. Our study showed more promising results than a similar study in that 69 (59.48%) reports were accurate with a reporting rate of 116 (84.06%) in which 47 (40.52%) reports were reported on time and 73 (62.93%) were complete reports.27 The difference might be due to the difference in sample size that the previous study included more health facilities including health centers so that more low-performing health facilities could be involved. On the other hand, the difference could be related to the counter agreement with the qualitative finding that some hospitals manipulated their reports. As well, our study showed that the average bin card accuracy was 59 (90.77%), ranging from 75% to 100%, therefore, there is some inconsistent data among the physical stock and stock balance in the bin card record that could lead to under or over-reporting. Still, the current figure is higher than the previous study that 374 (52.45%) bin cards were accurate27 that the difference might be to the difference in sample size and settings while both studies encounter similar challenges and another finding indicated that there was poor to no visibility of stock position for most dispensed products.28 No doubt increasing access and use of essential drugs ensures women and children are protected from preventable causes of death and disease. Our finding indicated that the average availability of MNCH drugs was 59(75.64%), which is fairly high but below the normal (100%), with a mean stock-out duration of 1.69 months in which at least one stock-out per month for one or more of closely half of life-saving MNCH drugs mainly due to inadequate supply. This finding shows that mothers, neonates, and children lost or endangered their life following the stock-out of some lifesaving drugs given that all hospitals placed at least one emergency order within a year. With its gaps, this study indicated a stock-out 59(75.64%) which is higher than the previous studies, 14 (61.30%),27 54.3%,29 and 74.3%30 with a mean stock-out duration of 70.7127 and 2629 days. The new kaizen approach and enactment of Dagu 2.0 were the possible means for the availability of MNCH drugs over the previous studies. Developing countries not only have limited resources but are also mismanaged. Deprived inventory management in public hospitals results in wastage of financial resources.31 In this study, the overall wastage rate was 13.1% which is more than twice the national normal,22 and higher than a similar previous study where wastage due to expiration was 8.04%.32 The difference from the standard may be attributed to poor adherence to the Federal Hospitals Pharmacy directive33 and lower commitment of the store managers. Furthermore, medicines stored in acceptable conditions enable the maintenance of the quality of medicines and reduce the wastage of scarce resources. In our study, 5(83.33%) hospitals fulfilled the criteria of acceptable storage conditions, which is optimal but below the national maximum of22 and closely similar to the result of the previous survey, in which 80% of hospitals met the acceptable storage conditions. It is higher than a finding in Lesotho (57.43%)34 but lower than a finding from the west of the Wollega zone that 4(100%)32 hospitals met storage criteria. The study is not without limitation, and it was limited to public hospitals. Therefore, to get to the overall conclusion, higher-level and lower level (medical centers and clinics) public health facilities shall be the subject of future studies. This study is suggested to be helpful for healthcare facility leaders, non-governmental organizations, and product service managers to make informed decisions so that they could take policy measures.
Conclusion
In conclusion, both bin card accuracy and the data quality of report and resupply forms were lower than the maximum target value (100%) and need significant improvement. The availability of life-saving MNCH drugs was low. Almost all hospitals placed an emergency order and encountered at least one stock-out per year. The wastage rate was twice more than the national normal and failed to first-expiry-first-out stock rotation, whereas most of the hospitals met acceptable storage conditions. Findings from the in-depth interview identified scanty storage management practice, inadequate human resources, and unreliable capacity building. Effective storage management, retaining sufficient human resources, and increasing the capacity of hospital staff could boost efforts of inventory management practice. Further study is recommended to identify factors associated with poor inventory management practices.
Abbreviations
EPSA, Ethiopia Pharmaceutical Supply Agency; IPLS, Integrated Pharmaceutical Logistics System; LIAT, Logistics Indicator Assessment Tool; LMIS, Logistics Management Information System; LSAT, Logistics System Assessment Tool; MNCH, Mother, Neonates and Child Health; UN, United Nations; USAID, United States Agency for International Development; WHO, World Health Organization.
Data Sharing Statement
All the necessary data were included in the manuscript.
Ethical Declarations
Ethical approval was received from the institutional review board of Jimma University, and then hospital administrative staff were communicated using letters of support obtained from the school of pharmacy and the Jimma zone health office approved it as ethical. The study was conducted according to the criteria set by the declaration of Helsinki. Both written and verbal informed consent were obtained from all participants, before enrolling them in the study, including publication of anonymized responses and personal profiles that were not used during reporting and publishing of the result.
Acknowledgments
All authors would like to thank the facility directors and health facilities staff for providing relevant information. We also thank Jimma University for facilitating the study.
Disclosure
The authors declared that they have no competing interests in this work.
References
1. Paulson KR, Kamath AM, Alam T, et al. Global, regional, and national progress towards Sustainable Development Goal 3.2 for neonatal and child health: all-cause and cause-specific mortality findings from the Global Burden of Disease Study 2019. Lancet. 2021;398(10303):870–905.
2. Wardlaw T, You D, Hug L, Amouzou A, Newby H. UNICEF report: enormous progress in child survival but greater focus on newborns urgently needed. Reprod Health. 2014;11(1):1–4. doi:10.1186/1742-4755-11-82
3. Pronyk PM, Nemser B, Maliqi B, et al. The UN Commission on life saving commodities 3 years on: global progress update and results of a multicountry assessment. Lancet Global Health. 2016;4(4):e276–e286. doi:10.1016/S2214-109X(16)00046-2
4. Ababa A. Federal Democratic Republic of Ethiopia Ministry of Health. Ethiopia: Postnatal Care; 2003.
5. Black RE, Levin C, Walker N, et al. Reproductive, maternal, newborn, and child health: key messages from disease control priorities 3rd edition. Lancet. 2016;388(10061):2811–2824. doi:10.1016/S0140-6736(16)00738-8
6. World Health Organization. Survey of the Quality of Medicines Identified by the United Nations Commission on Life-Saving Commodities for Women and Children. World Health Organization; 2016.
7. Droti BO, Mathai M, Dovlo DY, Robertson J, Robertson J. Poor availability of essential medicines for women and children threatens progress towards Sustainable Development Goal 3 in Africa. BMJ Global Health. 2019;4(Suppl 9):e001306. doi:10.1136/bmjgh-2018-001306
8. You D, Jones G, Hill K, Wardlaw T, Chopra M. Levels and trends in child mortality, 1990–2009. Lancet. 2010;376(9745):931–933. doi:10.1016/S0140-6736(10)61429-8
9. The Global AR. Fund’ s in -country supply chain processes, GF-OIG-17-008, 28 April 2017 Geneva, Switzerland; 2017. Available from: http://apps.who.int/medicinedocs/documents/s17997en/s17997en.pdf.
10. Bourret POC, Gitau L, Mwangi J, et al. HCSM assists Kenya’s MOH to develop Essential Medical Lab Commodities List. Health Commodity and Supply Management; 2014.
11. Gurmu TG, Ibrahim AJ. Inventory management performance of key essential medicines in health facilities of east Shewa zone, Oromia regional state, Ethiopia. Cukurova Med J. 2017;42(2):277–291. doi:10.17826/cutf.322908
12. Semu E. Inventory Management Practices for Pharmaceuticals Items at Health Facilities in Addis Ababa. St. Mary’s University; 2018.
13. Carter J. Role of laboratory services in health care: the present status in Eastern Africa and recommendations for the future. East Afr Med J. 1999;76(5):1–2.
14. Ethiopian hospital services transformation guidelines Addis Ababa; 2016:1–6.
15. Zheng M. Conceptualization of cross-sectional mixed methods studies in Health science. Int j Quant Qual Res Methods. 2015;3:66–87.
16. Getahun W, Tadeg H, Ejigu E, Korra A. Health Facility Assessment on Availability of the 13 Reproductive, Maternal, Newborn, and Child Health Commodities Prioritized by the UN Commission on Life-Saving Commodities for Women and Children. Arlington, VA: United States Agency for International Development; 2015.
17. Standard operating procedure manual for the integrated pharmaceutical logistics system in health facilities of Ethiopia. 2nd ed. Addis Ababa; 2015.
18. John Snow Inc./DELIVER. Logistics Indicators Assessment Tool (LIAT). Arlington, VA; 2005 [cited January 5, 2021]. Available from: https://pdf.usaid.gov/pdf_docs/Pnade735.pdf.
19. Inventory management assessment tool [Internet]. Available from: https://www.msh.org/resources/inventory-management-assessment-tool-imat.
20. USAID. Logistics System Assessment Tool (LSAT). Arlington: USAID | DELIVER PROJECT; 2009.
21. Monitoring and evaluation indicators for assessing logistics systems performance. Arlington, VA: DELIVER, for the U.S. Agency for International Development; 2008.
22. Federal Ministry of Health. National pharmaceutical SCM, pharmacy service and medical device monitoring and evaluation framework. Addis Ababa; 2018.
23. Shewarega A, Dowling P, Necho W, Tewfik S, Yiegezu Y. Ethiopia: national survey of the integrated pharmaceutical logistics system. Arlington: USAID/DELIVER PROJECT, Task Order; 2015.
24. Mkoka DA, Goicolea I, Kiwara A, Mwangu M, Hurtig A-K. Availability of drugs and medical supplies for emergency obstetric care: experience of health facility managers in a rural District of Tanzania. BMC Pregnancy Childbirth. 2014;14(1):1–10. doi:10.1186/1471-2393-14-108
25. Mbatia EM, Muthoni Mwangi E, Mwaura-Tenambergen W. Determinants of efficient health commodity management in maternal child health: a case of Meru County, Kenya. Int J Sci Res Publ. 2021;11(8):434–440. doi:10.29322/IJSRP.11.08.2021.p11654
26. SIAPS. Systems for improved access to pharmaceutical services annual report: project year 3, October 2013-September 2014. Arlington: Management Sciences for Health; 2014.
27. Kebede O, Tilahun G. Inventory management performance for family planning, maternal and child health medicines in public health facilities of West Wollega zone, Ethiopia. J Pharm Policy Pract. 2021;14(1):20. doi:10.1186/s40545-021-00304-z
28. PROJECT UD. Supply chains for reproductive, maternal, newborn, child, and adolescent health. Haryana; 2014.
29. Bassoum O, Ba A, Tall AB, et al. Availability, management and use of priority life-saving medicines for under-five children in two health districts in senegal: a cross-sectional study. Health. 2020;12(02):204–218. doi:10.4236/health.2020.122017
30. Damtew D, Worku F, Tesfaye Y, Jemal A. Availability of lifesaving maternal and child health commodities and associated factors in public and private health facilities of Addis Ababa, Ethiopia. Health Serv Res Manag Epidemiol. 2019;6:2333392819892350. doi:10.1177/2333392819892350
31. Matowe LWP, Adome RO, Kibwage I, Minzi O, Bienvenu E, Bienvenu E. Human Resources for Health A strategy to improve skills in pharmaceutical supply management in East Africa: the regional technical resource collaboration for pharmaceutical management. Hum Resour Health. 2008;6:1–6. doi:10.1186/1478-4491-6-30
32. Kebede O, Tilahun G, Feyissa D. Storage management and wastage of reproductive health medicines and associated challenges in west Wollega zone of Ethiopia: a mixed cross-sectional descriptive study. BMC Health Serv Res. 2021;21(1):297. doi:10.1186/s12913-021-06291-w
33. Ayalew MB, Taye K, Asfaw D, et al. Patients’/clients’ expectation toward and satisfaction from pharmacy services. J Res Pharm Pract. 2017;6(1):21. doi:10.4103/2279-042X.200995
34. Pharasi B. Assessment of the HIV/AIDS medical supplies and laboratory commodities supply chain in Lesotho. USA Arlington, VA: USAID/RPM Plus, for management science for health; 2007.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.