")
Back to Journals » Journal of Asthma and Allergy » Volume 16
Assessment of Fraction of Exhaled Nitric Oxide and Soluble Receptor for Advanced Glycation End Products Biomarkers for Jordanian Asthmatic Children
Authors Alzayadneh EM , Al Bdour SA, Elayeh ER, Ababneh MM, Al-ani RA, Shatanawi A, Al-Iede M, Al-Zayadneh E
Received 26 April 2023
Accepted for publication 12 July 2023
Published 4 August 2023 Volume 2023:16 Pages 793—811
DOI https://doi.org/10.2147/JAA.S415481
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Ebaa M Alzayadneh,1 Suzan A Al Bdour,1 Eman R Elayeh,2 Mai M Ababneh,3 Ruqaya A Al-ani,3 Alia Shatanawi,4 Montaha Al-Iede,3 Enas Al-Zayadneh3
1Department of Physiology and Biochemistry, School of Medicine, The University of Jordan, Amman, Jordan; 2Department of Biopharmaceutics and Clinical Pharmacy, School of Pharmacy, The University of Jordan, Amman, Jordan; 3Department of Pediatrics, School of Medicine, The University of Jordan, Amman, Jordan; 4Department of Pharmacology, School of Medicine, The University of Jordan, Amman, Jordan
Correspondence: Ebaa M Alzayadneh, Tel +962796972717, Fax +96265300820, Email [email protected]
Purpose: Fraction of exhaled nitric oxide (FeNO) and soluble advanced glycation end-product receptor (sRAGE) are proposed as biomarkers of asthma, therefore we sought to assess their use in asthmatic children of Jordan.
Patients and Methods: We conducted a case-control study at The University of Jordan Hospital. A total of 141 asthmatic children followed by respiratory pediatricians and 118 healthy children aged 4– 18 years were recruited. FeNO was measured by NObreath device and serum sRAGE by ELISA that detect endogenously soluble isoform (esRAGE) and total soluble RAGE (sRAGE).
Results: sRAGE in asthmatic was half of the control (p < 0.001). In addition, ratio of esRAGE/sRAGE was two-fold higher in asthmatic (p = < 0.001). Neither FeNO nor esRAGE levels were significantly different between groups. FeNO and asthma control test (ACT) score were negatively correlated corrected for age and body mass index (BMI), (r = − 0.180, p= 0.034). For the uncontrolled asthma group, esRAGE/sRAGE negatively correlated with ACT score (r = − .329, p = 0.038). Receiver operating curve (ROC) analysis revealed significant predictive value (PV) for sRAGE and esRAGE/sRAGE in asthma detection with area under the curve (AUC) of (0.751 ± 0.031) and (0.711± .033), consequently. However, no biomarker had a significant PV for lack of control.
Conclusion: The current study supports utilizing sRAGE as a marker for asthma and present a potential therapeutic target. However, our results indicate that both FeNO and sRAGE have a limited role in the management of asthmatic children or assessment of asthma control.
Keywords: childhood asthma, allergy, inflammation, asthma control test
Introduction
Asthma is the most common chronic lung disease affecting children worldwide. It is a heterogenous disease comprising a range of different clinically recognized phenotypes that are characterized by bronchial hypersensitivity, chronic airway inflammation and reversible airway narrowing. Asthma is mainly diagnosed based on clinical history and physical findings that are linked to distinct, yet complex underlying molecular pathways known as endotypes.1 Two major endotypes of asthma were identified, T-helper 2-high (TH2-high) that is elicited mainly by TH2 which is typically seen in childhood-onset asthma due to allergens sensitization. TH2-high endotype is characterized by airway eosinophilic inflammation and is highly responsive to steroids treatment. On the other hand, asthmatics lacking the TH2 endotype (TH2-low) has much fewer clear mechanisms and more severe outcomes hallmarked with airway neutrophilia, which is not well-responsive to steroids.1
In Jordan, asthma prevalence was estimated by 9% among children in Amman and northern Jordan.2–4 Importantly, asthma affects children growth, development, and quality of life and poses a great burden on healthcare systems.5 Currently, commonly used methods in the diagnosis and management of asthma are peak expiratory flow, lung function test (spirometry), bronchodilator responsiveness, and bronchial provocation.5 The difficulty of application and invasiveness in most of the aforementioned methods for young children led to agreed consensus on the urgent need to validate novel and applicable methods for improving asthma outcomes especially among children.6 Therefore, other complementary assessment methods are currently proposed as specific asthma biomarkers including fractional exhaled nitric oxide (FeNO) and soluble receptor for advanced glycation end products (sRAGE).6,7
FeNO test is used to measure expiratory nitric oxide gas level, which is produced by inflammatory cells of allergic or eosinophilic asthma.8 FeNO is being increasingly used worldwide as a complementary tool to either identify asthma phenotype, to determine level of control, or to predict exacerbations and medication plan.9 However, its validity is still questioned due to its various confounders, thus more investigation is mandated. To our knowledge, no previous studies have been conducted in Jordan on utilization of FeNO in asthma diagnosis or management at any age group, and a few were conducted in the middle east.9 In Jordan, FeNO is rarely used in clinical practice partly due to its controversial role as a diagnostic tool or as management biomarker. Asthma is often inadequately diagnosed or treated, particularly in low- and middle-socioeconomic countries.9–11 In Jordan for an example, asthma control was achieved in only 45.2% of the sample of a study performed in south of Jordan, having severe asthma and atopy defined as main risk factors for uncontrolled asthma.12 Previous reports have shown that FeNO utilization may improve diagnosis and management of allergic childhood asthma due to its non-invasive and non-laborious measurement methods.9,13,14 However, there is no consensus established till now for using FeNO in asthma diagnosis, it’s more likely to rule in rather than rule out allergic asthma.9
On the other hand, a growing body of evidence suggests that advanced glycation-end products receptor (RAGE)- multi-ligand receptor belonging to the cell surface immunoglobulin superfamily- is highly expressed in the lungs and is implicated in asthma pathogenesis and suggested as a biomarker.15–17
Current experimental findings indicate that RAGE plays a key role in type 2 inflammatory reactions evident in TH2-high asthmatic subtype.15 Moreover, previous clinical studies demonstrated that increased RAGE ligands and signaling strongly correlate with asthma severity, especially in severe neutrophilic asthma (TH2-low).18–21 The soluble form of the receptor (sRAGE) is produced from proteolytic cleavage of the extracellular domain of the plasma membrane bound receptor (mRAGE) or from the alternative splicing of the RAGE gene leading to production of the endogenously secreted soluble isoform (esRAGE).22,23 Serum or bronchial lavage levels of sRAGE correlated with asthma previously by several reports. Serum sRAGE levels were negatively correlated to FeNO levels and low sRAGE was associated with wheezing children at high risk of asthma.24 Interestingly, inhalation of steroids, decreased FeNO and increased sRAGE levels and improved asthma.24 Another study highlighted an association of low serum sRAGE with acute and chronic morbidities of bronchiolitis including recurrent wheeze in hospitalized infants.25 Several reports investigated the pathophysiological mechanisms of RAGE axis, however, the variable expression of RAGE, the diversity of RAGE ligands, along with the overly complex nature of asthma disease, merit further research.17 It has been previously shown that binding of mRAGE to its ligands such as high mobility group box 1 (HGMB1) results in activation of a myriad of inflammatory signaling cascades in various cell types including alveolar cells.26 Currently, it is suggested that sRAGE can function as a decoy receptor that reduces binding of various RAGE ligands to mRAGE thus reducing downstream pro-inflammatory signaling pathways (eg, nuclear factor kappa B (NFκB), Janus kinase/signal transducer and activator of transcription (JAK/STAT)) in the lungs.17
Taken together, there is a growing rationale for investigating RAGE as a biomarker of asthma.
The main goal of this study was to assess utility of more applicable non-invasive biomarkers such as FeNO or minimally invasive biomarkers such as serum sRAGE in asthma management among Jordanian population. We compared levels of FeNO and sRAGE in both asthmatic and healthy children (control) and investigated the relationship between these levels and various variables such as demographic data, gestational age, environmental exposure to tobacco and pet dander (cats), vitamin D supplementation, concomitant allergies, and asthma medications. Additionally, we investigated correlations between FeNO and sRAGE biomarkers and asthma control measured by asthma control test (ACT). Moreover, we evaluated the diagnostic value of FeNO and sRAGE to diagnose asthma or to aid in assessment of asthma control in children.
Materials and Methods
Study Population
The study recruited 141 asthmatic children that were clinically diagnosed by respiratory pediatricians, who visited pediatric respiratory clinic at the Jordan University Hospital’s (JUH), in the city of Amman, Jordan, from July 2021 until July 2022. Additionally, 118 healthy children who visited the pediatric clinics for routine check-up were recruited as controls. Clinical history, FeNO measurement and a blood sample were taken for all study subjects.
Study Design
The study is a case-control study. Asthmatic children or children with recurrent wheezing who were aged between 4 and 18 years old were included. These children were diagnosed according to the Global Initiative for Asthma GINA criteria and were followed up by pediatric pulmonary specialists. The following were the exclusion criteria: patients presented with asthma exacerbation treatment before FeNO measurement, presence of respiratory viral infection or other acute respiratory concomitant disease in the 12 weeks before medical care. Healthy children of matched age and sex who did not have any respiratory diseases were included as controls in this study. An extensive chart review was conducted to extract the study variables, including demographic information such as age and sex for all participants. Perinatal history and social history including gestational age, pets, and smoking exposure. Medication history includes inhaled salbutamol, inhaled and systemic steroids, and previous vitamin D supplementation. In addition, medical history was taken to record presence of other concomitant allergies, the severity of asthma within the last 2 months and the treatment regimen used for asthma. We conducted logistic regression analysis to identify variables that affect asthma and to identify factors affecting FeNO levels, esRAGE/sRAGE among all participants, control group and asthmatic patients. In addition, we compared levels of FeNO and sRAGE in both asthmatic and control healthy children and investigated the relationship between these levels and various variables such as demographic data, gestational age, environmental exposure to tobacco and pet dander(cats), vitamin D supplementation, concomitant allergies and asthma medications. Additionally, we investigated correlations between FeNO and sRAGE biomarkers and asthma control measured by asthma control test (ACT).24 Moreover, we evaluated the diagnostic value of FeNO and sRAGE to diagnose asthma or to aid in assessment of asthma control in children.
FeNO Device
FeNO was measured by NObreath device (Wales, UK) according to American Thoracic Society /European Respiratory Society (ATS/ERS) and manufacturer recommendations.27 For analysis purposes, asthmatic children based on the value of FeNO were categorized according to ATS clinical practice guidelines as the following: high (>35 ppb), intermediate (20–35) and low (<20).9
Measurement of Serum sRAGE and esRAGE
A sample of five milliliters (5 mL) of venous blood was collected by venipuncture. The serum was separated by centrifugation (10 mm, 3000 × g, 10 min), and stored at −80 °C until used. The levels of sRAGE and esRAGE in serum were measured by two distinct Enzyme-Linked Immunosorbent Assay (ELISA) kits. For sRAGE, (OmniKine Human RAGE Colorimetric ELISA Kit (My BioSource, San Diego, LA, California, Cat. NO. MBS9502071) was utilized to detect total sRAGE including cleaved form of membrane bound full length RAGE and endogenously soluble esRAGE, while for esRAGE directed kit (esRAGE ELISA Kit, My BioSource, Cat. NO. MBS3801084) was used to specifically detect esRAGE by using an antibody directed against the unique COOH-terminal sequence of RAGE-v1(splice variant lacking transmembrane domain) and does not cross-react with the cleaved form of full RAGE. Both immunoassays used the quantitative technique of a “Sandwich” ELISA with different capture antibodies. The serum was assayed according to the protocol described by the manufacturers. The sRAGE kit and esRAGE kit were capable to detect and quantify RAGE proteins within range of (63–4000 pg/mL) and (0–1600 ng/mL), respectively. All sera’s measurements fell within detection range. The optical densities were measured by a microplate reader set to 450 nm. (Synergy HTX, multi-mode order), from Biotech. The software program was Gen5, version 2.07.
Asthma Control
The level of asthma control was assessed by medical evaluation before a patient underwent FeNO level measurements. Asthma Control Test (ACT) was used to assess control level of asthma for teens of 12 years and older.28 It comprises five questions assessing the frequency of shortness of breath, frequency of asthma night-time symptoms, degree of functional limitation, frequency of using rescuers, and patient’s self-assessment of their level of asthma control. Each item has five response choices each with a score ranging from (1–5). Accordingly, the levels of asthma control are as follows: well-controlled (scores of 20–25), partially controlled (15–19), and uncontrolled asthma (5–14).28 For Children up to 11-years-old, children ACT (cACT) was used which has a total score of 27, where poor controlled children had lower than 19 score.29
Statistical Analysis
All collected data were organized, coded, and imported to the Statistical Package for Social Sciences (SPSS) version 22. Continuous variables were expressed as median and interquartile range while categorical variables were expressed as frequency and percentage. Statistical comparisons among the FeNO values, sRAGE and esRAGE serum levels were performed using the Mann–Whitney test and Kruskal–Wallis test. Spearman’s rho test was used to find correlations between continuous variables. P values less than 0.05 were considered statistically significant. Logistic regression analysis was conducted to identify variables that affect asthma, FeNO level and esRAGE/sRAGE among all participants, control group and asthmatic patients. A receiver operating characteristic (ROC) curve was constructed, presenting the sensitivity and specificity to find the best cut-off values for the diagnosis of asthma or detection of lack of control. In which an asymptotic p values of less than 0.05 were considered significant.
Ethical Considerations
The study was conducted in compliance with the Declaration of Helsinki, and the study’s protocol and proposal were reviewed and accepted by the Jordan University Hospital’s Institutional Review Board (IRB) # 2022/33 and the University of Jordan’s research ethics committee. A written informed consent was obtained from the parents or legal proxies of all participants of this study.
Results
Characteristics of Study Children
The study group included 141 asthmatic (5- to 18-years-old) or wheezing (under 5-years-old) children and 118 healthy controls. Of study children, 65.2% were males and 34.8% were females. The median age of children was 11 years. Demographic and clinical characteristics of all study children are listed in Table 1. For asthmatic children, clinical characteristics are shown in Table 2. Among asthma risk factors, family history of asthma and presence of allergy other than asthma showed significant association with asthma diagnosis as observed from logistic regression analysis (Table S1).
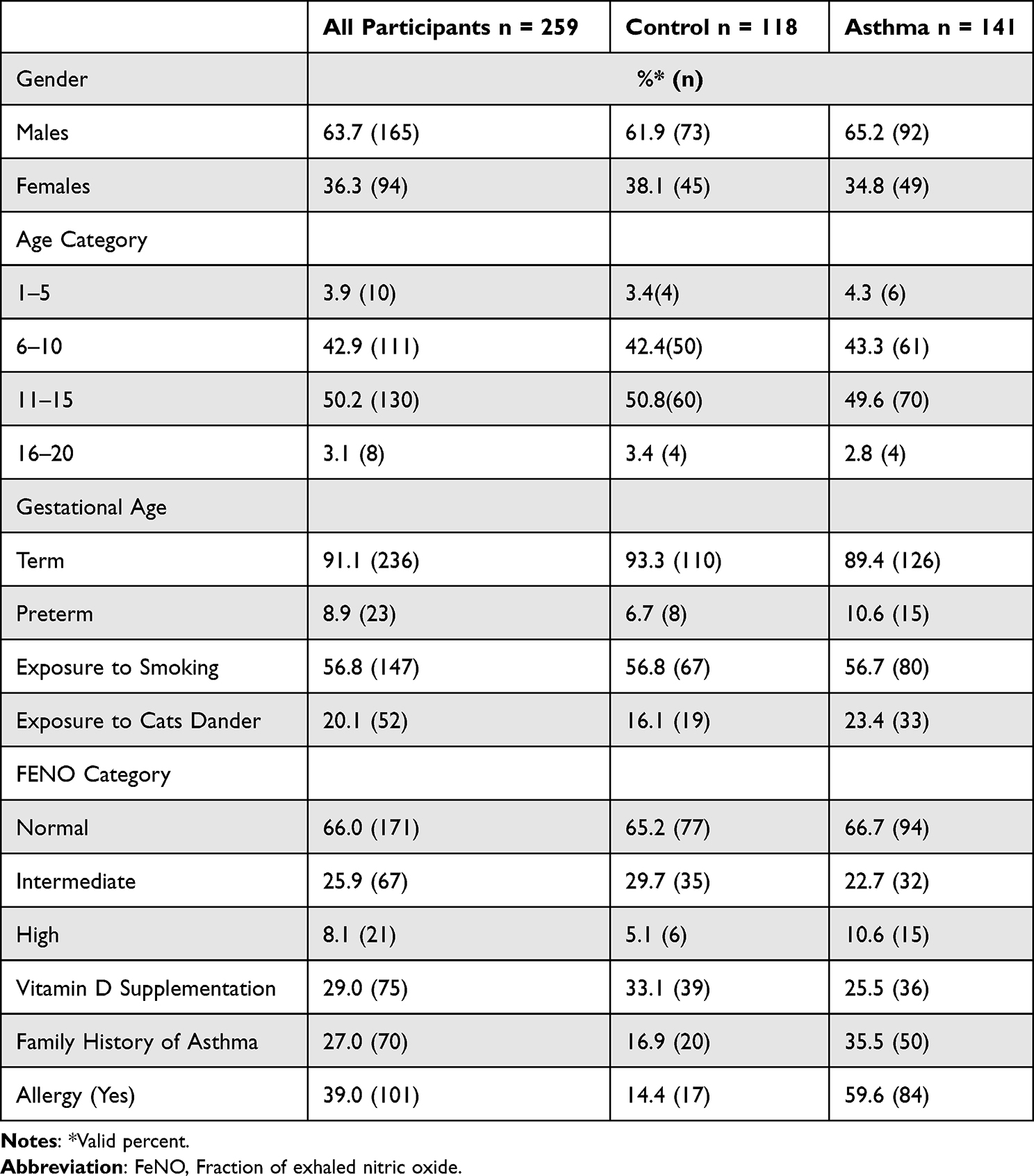 |
Table 1 Characteristics of the of All Participants (Control and Asthma Groups) |
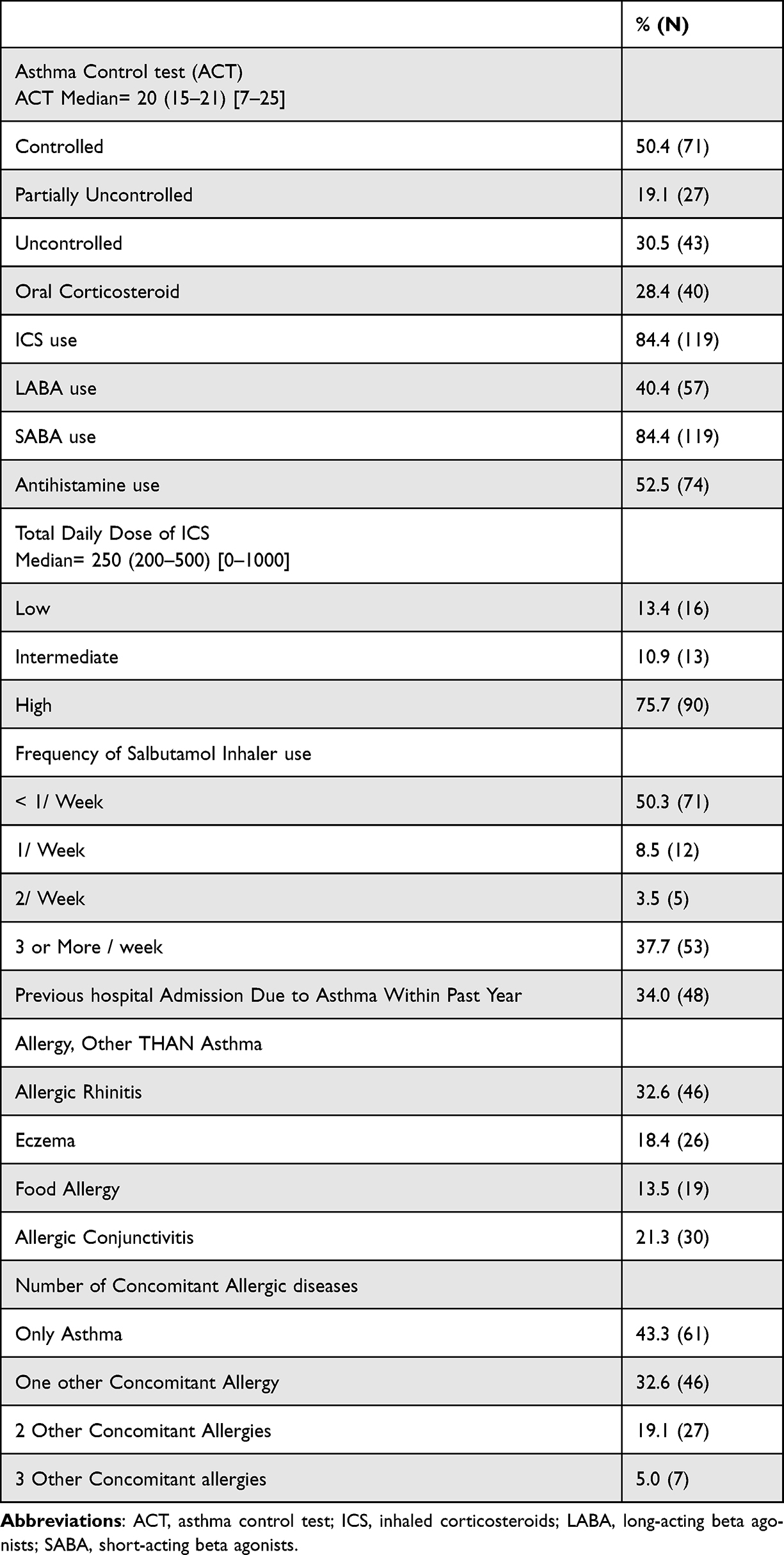 |
Table 2 Clinical Characteristics of Asthma Patients (n = 141) |
Measurements of FeNO, sRAGE, esRAGE and Ratio of esRAGE/sRAGE
The median (Interquartile range (IQR)) FeNO levels (ppm) were not significantly different between asthmatic and control children (14.0, (8.0–22.0) vs. 15.0, (7.8–23.5)), p = 0.987), however, median serum sRAGE (pg/mL) was reduced in asthmatic to almost half that of control (673.8 (417.2–1017) vs. 1363.0 (774.0–2065), p <0.001) (Table 3). Although only 28.4% are taking systemic corticosteroids, 84.4% used inhaled corticosteroids (ICS), which could explain the blunted difference in FeNO measurements between asthmatic and control children.
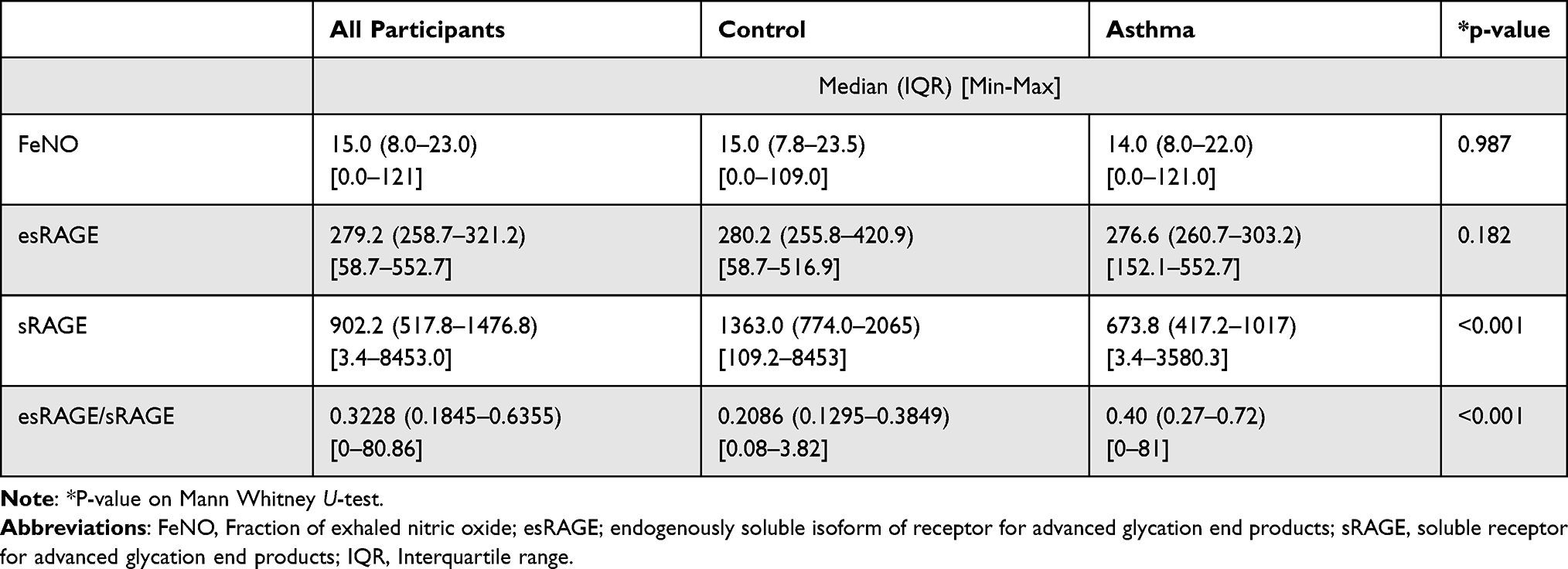 |
Table 3 Differences Between Asthmatic and Control in Studied Biomarkers |
In addition, median of esRAGE was not different between the groups (280.2 (255.8–420.9) vs. 276.6 (260.7–303.2), p = 0.182) (Table 3). In contrast, median of ratio of esRAGE/sRAGE (IQR) was significantly higher in asthmatic compared to control (0.40 (7.8–23.5) vs. 0.2086 (8.0–22.0), p <0.001) (Table 3).
For the different asthma control groups, no statistically significant differences were found regarding FeNO levels or serum RAGE markers (sRAGE, esRAGE, or esRAGE/RAGE) (Table 4), indicating they could not provide a useful tool to assess level of control of asthma in children as compared to ACT.
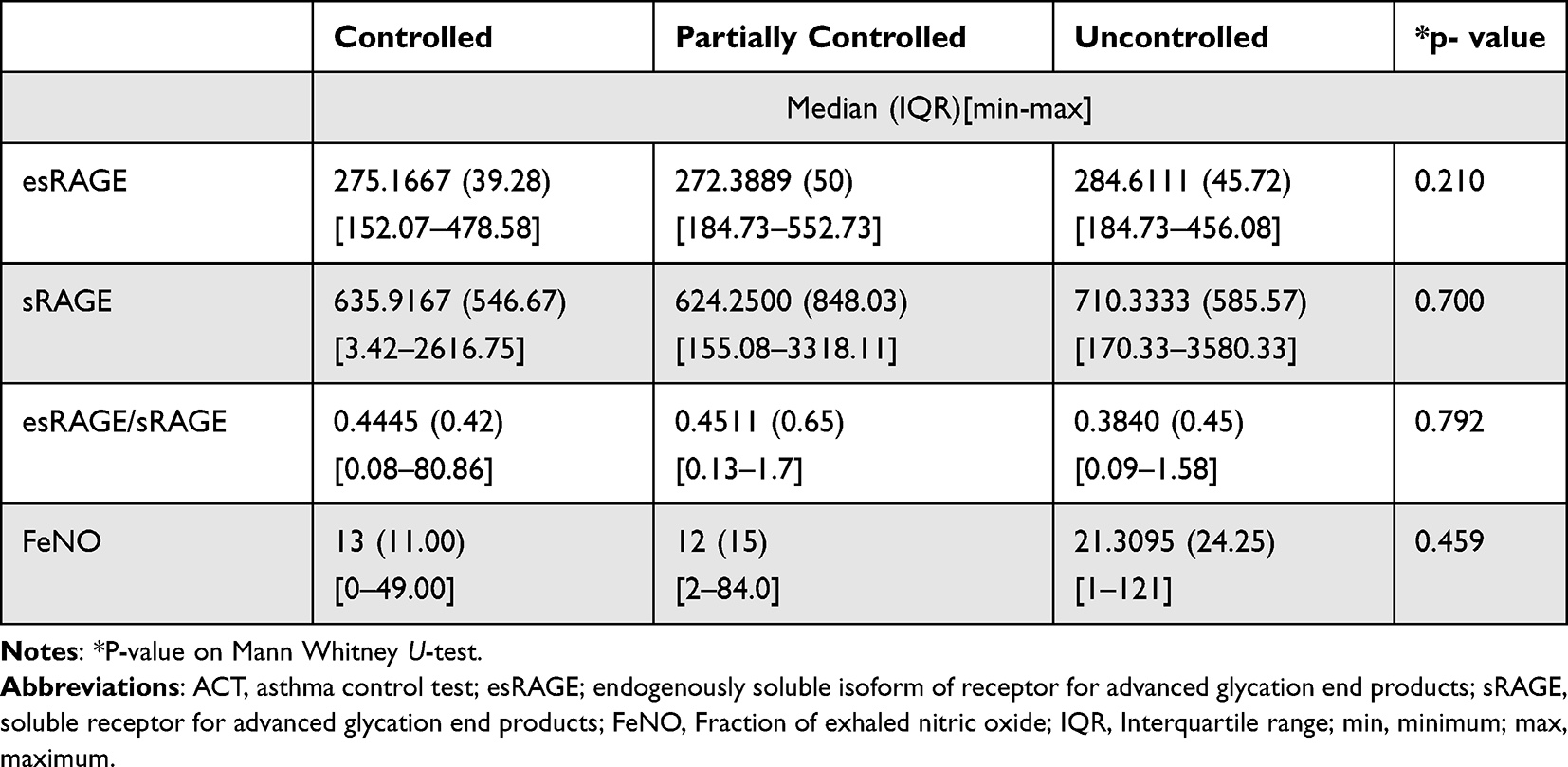 |
Table 4 Differences Between Asthmatic Groups According to ACT Score in Studied Biomarkers |
Regarding ICS and systemic steroids use, asthmatic children who were taking ICS had significantly higher ACT scores than those who did not (chi square = 8.705, p = 0.003, degree of freedom (df) = 1) which might be related to better control of the disease with use of ICS (Figure 1A). In contrast, asthmatic children who were treated with systemic steroids had significantly lower ACT scores which is explained by the need to treat more severe asthma with systemic steroids (chi square = 11.813, p =0.001, df = 1) (Figure 1E).
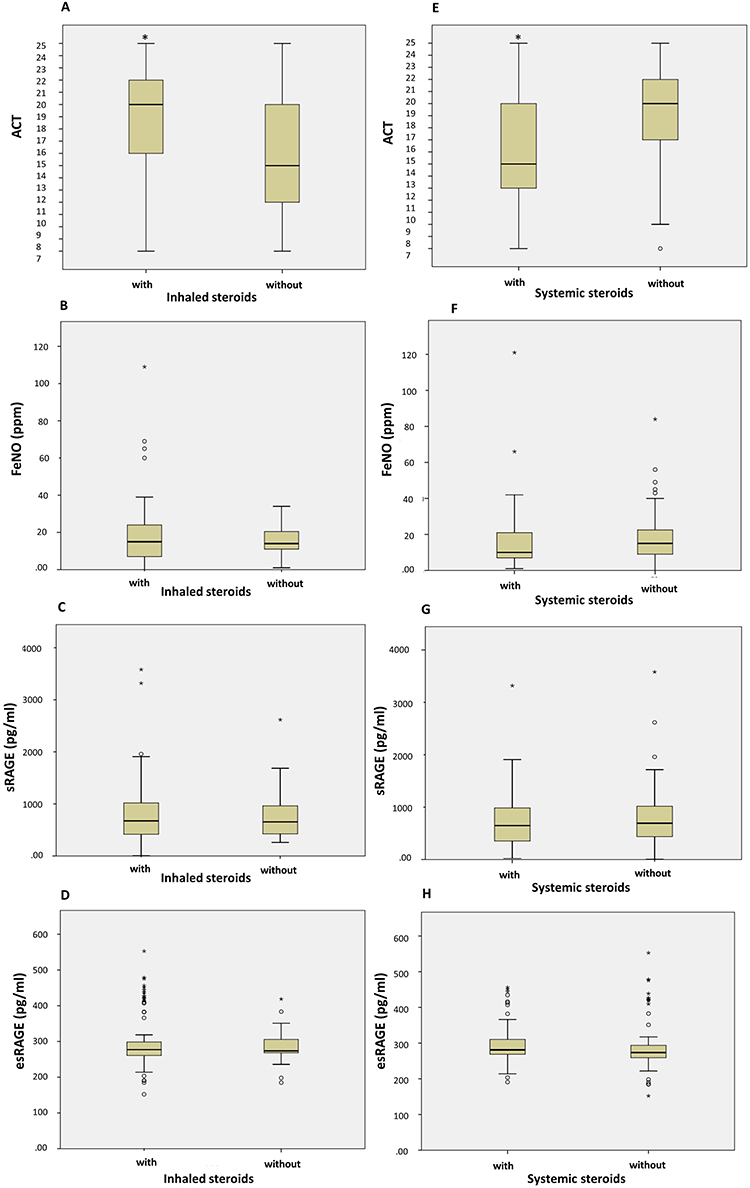 |
Figure 1 Box plots demonstrating comparisons between asthmatic children who take inhaled corticosteroids (ICS) and who do not (A–D), and between asthmatic children who take systemic steroids and who do not (E–H) in terms of ACT score, FeNO, sRAGE and esRAGE levels. ACT score was significantly different between children who are under ICS and who are not (chi square = 8.705, p = 0.003, df = 1) as in (A). However, asthmatic children who were treated with systemic steroids had significantly lower ACT scores (chi square = 11.813, p = 0.001, df = 1) as in (E). On the other hand, FeNO level, sRAGE, or esRAGE were not significantly affected by ICS or systemic steroids (chi square = 3.71, p = 0.39, df = 6) as in (B–D and F–H; consequently); *P value of ≤.05 is considered significant. Abbreviations: ICS, inhaled corticosteroids; FeNO, Fraction of exhaled nitric oxide; sRAGE, soluble receptor for advanced glycation end products; esRAGE, endogenously soluble isoform of receptor for advanced glycation end products; ACT, asthma control test. |
However, FeNO, sRAGE, or esRAGE were not significantly affected by ICS or systemic steroids (chi square = 3.71, p = 0.39, df = 6). (Figure 1B–1D and 1F–1H; consequently)
For asthmatic children who have allergic rhinitis, ratio of esRAGE/sRAGE, was significantly lower compared to children who have not; (0.92 ± 2.08 vs. 1.57 ± 8.59, Asymptotic significance (Asymp. Sig.) (2-tailed) = 0.026) (Figure 2A), and close to significancy the sRAGE level was lower for children with allergic rhinitis, whereases FeNO levels were not different if allergic rhinitis was present or not (Figure 2A). Asthmatic children who have atopic dermatitis have significantly higher FeNO levels when compared to children without (22.58 ± 16.49 vs. 16.80 ± 15.86, Asymp. Sig. (2-tailed) = 0 0.014) (Figure 2B). In addition, asthmatic children with food allergies had higher sRAGE levels; (982.23 ± 480.79 vs. 742.96 ± 563.93, Asymp. Sig. (2-tailed) = 0.017) (Figure 2C).
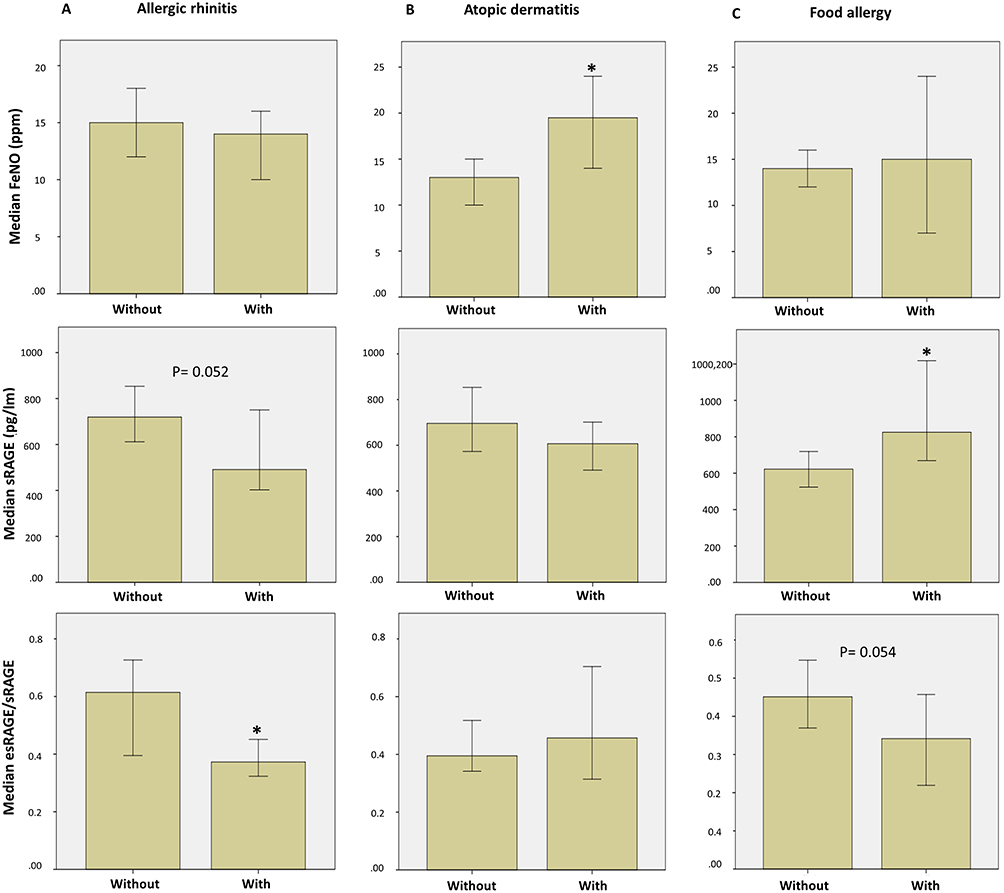 |
Figure 2 Comparisons between asthmatic children who have concomitant allergic disease and who have not in levels of FeNO, sRAGE and esRAGE/RAGE ratio. (A) asthmatic children without and with allergic rhinitis; ratio of esRAGE/sRAGE, was significantly lower compared to children who have not; (0.92 ± 2.08 vs. 1.57 ± 8.59, Asymp. Sig. (2-tailed) =0.026) and a trend for the sRAGE level to be lower, while FeNO levels were not different; (B) asthmatic children without and with atopic dermatitis; atopic dermatitis was associated with higher FeNO levels (22.58 ± 16.49 vs. 16.80 ± 15.86, Asymp. Sig. (2-tailed) =0 0.014); (C) asthmatic children without and with food allergy; food allergy was associated with higher sRAGE levels; (982.23 ± 480.79 vs. 742.96± 563.93, Asymp. Sig. (2-tailed) = 0.017) and a trend to reduced esRAGE/RAGE ratio. *P value of ≤.05 is considered significant. Abbreviations: FeNO, Fraction of exhaled nitric oxide; sRAGE, soluble receptor for advanced glycation end products; esRAGE; endogenously soluble isoform of receptor for advanced glycation end products; ACT, asthma control test. |
Factors Affecting FeNO Levels and esRAGE/sRAGE
We conducted logistic regression to identify variables that affect FeNO level (Table 5) and esRAGE/sRAGE (Table 6) among all study participants, control, and asthmatic groups. Age significantly affected FeNO level among all participants (Table 5). For esRAGE/sRAGE, exposure to smoking among all participants and use of inhaled corticosteroids among asthmatic children significantly affected the ratio (Table 6).
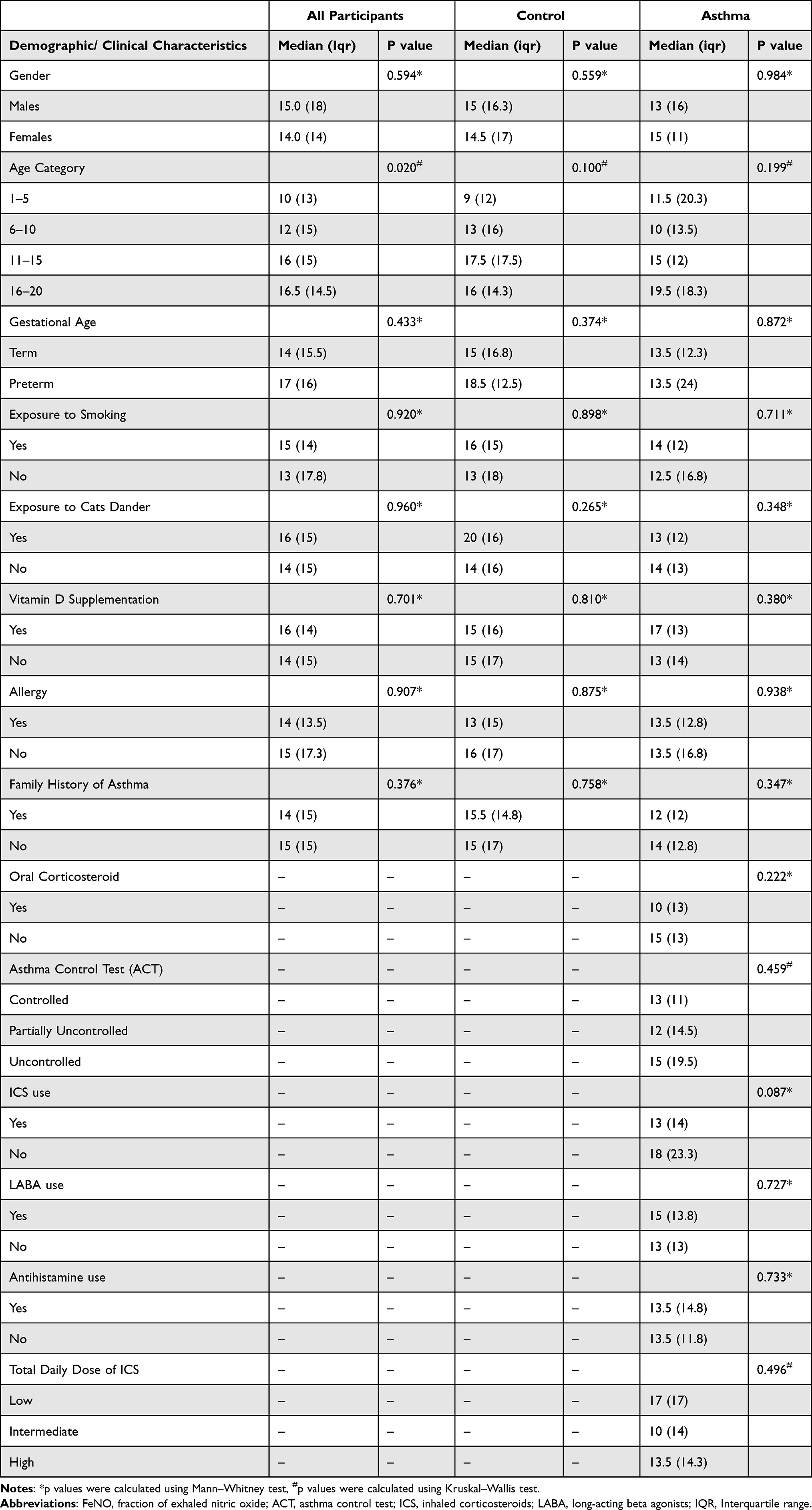 |
Table 5 Factors Affecting FENO Level Among All Participants, Control Group and Asthmatic Patients’ |
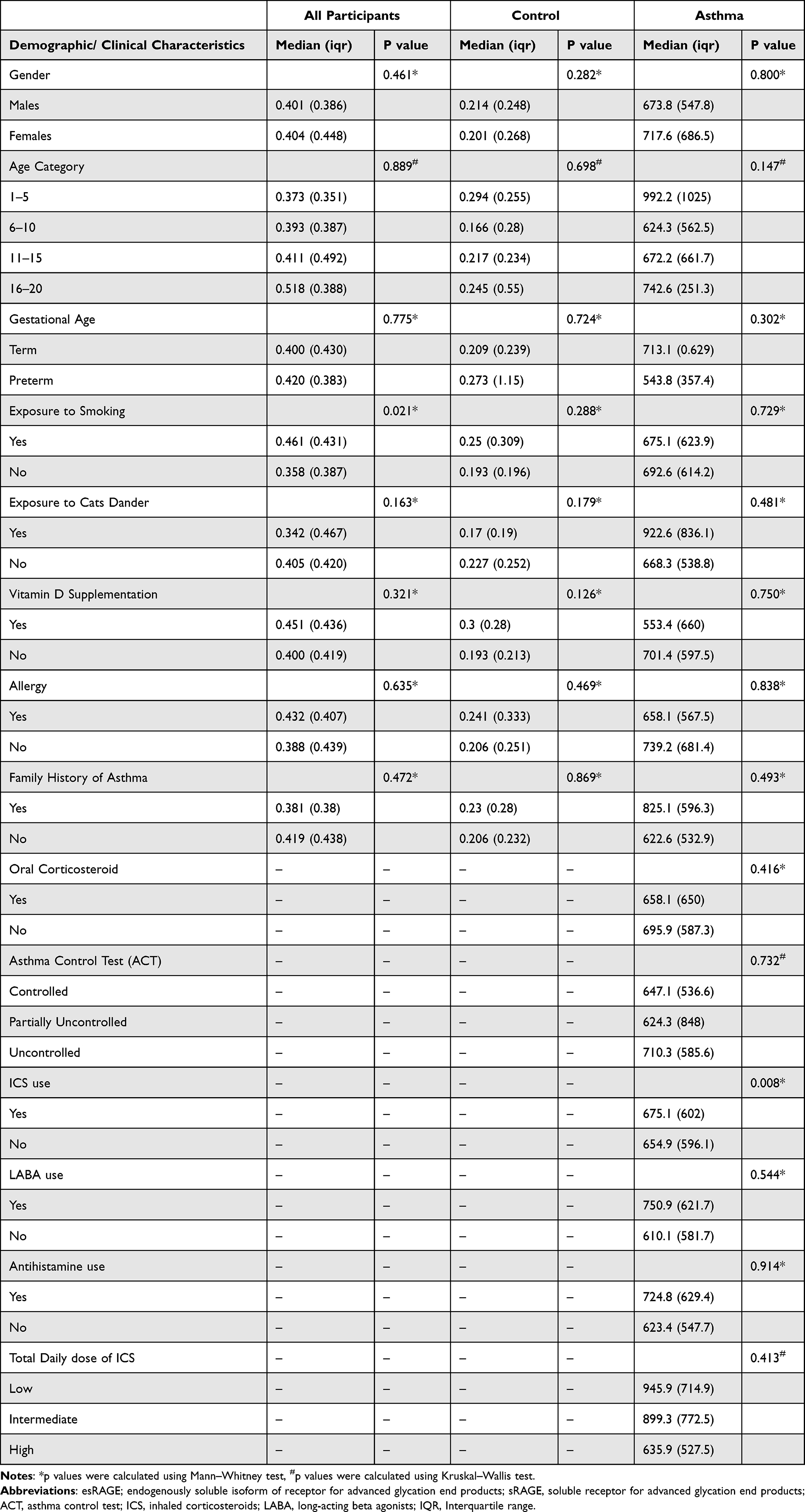 |
Table 6 Factors Affecting ESRAGE/SRAGE Among All Participants, Control Group and Asthmatic Patients |
Correlation Analyses
There was a significant positive correlation between age and FeNO measurement in both asthmatic and control children (0.178 p = 0.035) (Figure S1A). Indeed, there was a significant positive correlation for all participants (r = 0.186, p = 0.003) (Figure S1B). A trend for a negative but weak correlation was observed between ACT score and FeNO for all participants (r = −0.161, p = 0.057) (Figure S2A). When corrected for age and BMI, FeNO was significantly but weakly correlated with ACT score, (r = −0.180, p = 0.034. spearman) (Figure S2B).
Correlation analyses did not reveal significant correlations between FeNO and any of RAGE markers (sRAGE, esRAGE, or esRAGE/sRAGE) in all participants or in asthmatic children. Regarding sRAGE levels, there was a significant slight negative correlation with body mass index (BMI) (r = −0.225, p = 0.008) (Figure S3). There was no significant correlation between ACT score and sRAGE or esRAGE/sRAGE ratio observed in asthmatic children or all participants, however, in uncontrolled asthma group, esRAGE/sRAGE negatively correlated with ACT (r = −0.329, p = 0.038) (Figure S4).
Taken together, these data indicate that the studied biomarkers do not exhibit strong correlations with the level of asthma control assessed by ACT.
Receiver Operating Curve (ROC) for FeNO and RAGE
ROC analysis was utilized to illustrate validity of FeNO, and RAGE markers (sRAGE, esRAGE, or esRAGE/sRAGE) for use in predicting asthma among all study children (GINA guidelines as gold-standard criteria) (Figure 3A) and lack of asthma control among asthma children (ACT as gold-standard criteria) (Figure 3B).
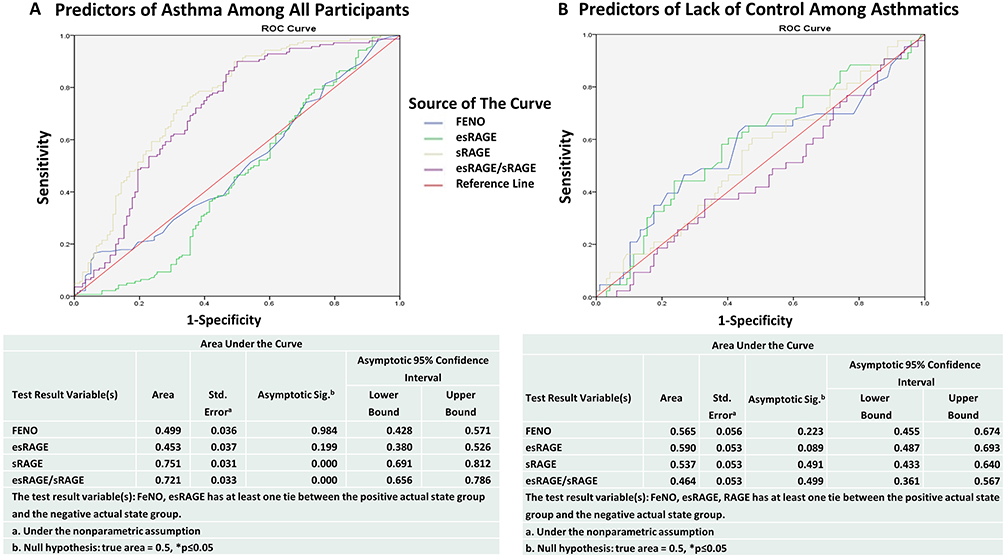 |
Figure 3 ROC curve of FeNO, sRAGE, esRAGE, esRAGE/RAGE, among different study groups. (A) ROC curve of FeNO, sRAGE, esRAGE, esRAGE/RAGE among all participants (n = 258). AUC of test variables in identifying asthma (GINA standards) are depicted in the tables under the corresponding curve; number of actual positive results(asthmatics) = 140 (B) ROC curve of FeNO, sRAGE, esRAGE, esRAGE/RAGE in asthmatic patients (n = 140). AUC of test variables in identifying lack of control (ACT as gold standard) are depicted in the tables under the corresponding curve; number of actual positive results (uncontrolled asthma) = 43. a, Under the nonparametric assumption; b, Null hypothesis: true area = 0.5; *P value of ≤.05 is considered significant. Abbreviations: ROC curve, receiver-operating characteristic curve; FeNO, fraction of exhaled nitric oxide; sRAGE, soluble receptor for advanced glycation end products; esRAGE; endogenously soluble isoform of receptor for advanced glycation end products; AUC, Area under the curve; ACT, asthma control test. |
Interestingly, sRAGE and esRAGE/sRAGE provided a significant predictive value for asthma among all participants as revealed by ROC analysis (Figure 3A). In which, sRAGE, had an area under the curve (AUC) of 0.751 ± 0.031, asymptotic significance (asymp. Sig.) = 0.000, 95% CI (0.691–0.812). For sRAGE, a cut off value of 683.59 (pg/mL) had a sensitivity of 51.4% and a specificity of 80%, while a cut off value of 403.39 (pg/mL) had a sensitivity of 23.6% and a specificity of 90%. The positive and negative predictive values for sRAGE were (71.4, 49.1), respectively. The ratio of esRAGE/sRAGE had an AUC of, 0.711 ± 0.033, Asymp. sig. = 0.000, CI (0.646–0.777). A cut off value of 0.4279 had sensitivity of 48.6% and specificity of 80%, and a cut off value of (0.9226) had sensitivity of 12.9% and specificity of 90%. The positive and negative predictive values for esRAGE/sRAGE were (62.1%, 46.7%), respectively. On the other hand, neither FeNO, nor soluble RAGE biomarkers had a significant diagnostic value regarding detection of lack of control of asthma among asthmatic patients (Figure 3B).
Discussion
The current study evaluates use of FeNO and sRAGE as markers for asthma in children who were previously diagnosed with asthma and being evaluated by respiratory pediatricians in Jordanian population. As summarized in Figure 4 demonstrating the mechanisms underlying allergic airway inflammation in asthma that involves RAGE signaling and biosynthesis of NO, there is compelling evidence in literature for a potential use of serum RAGE as a minimally invasive asthma biomarker and exhaled NO as a non-invasive asthma biomarker in children. Our findings in this study show that FeNO levels were not different between asthmatic patients who were followed up and control patients or between asthmatic children grouped according to ACT score. Furthermore, FeNO level did not demonstrate usefulness as a marker of asthma control level as assessed by ROC analysis using ACT as gold standard. Correlation analysis in this study revealed that FeNO was significantly correlated to age as previously reported but weakly correlated with ACT score. Similar to our findings, a study on Iranian asthmatic children, reported higher FeNO than what we found (28.5 ppb), and a comparable ACT mean score (19.8), found no significant correlation with ACT score. Additionally, there was no significant correlation between FeNO and changes in respiratory function measures before and after the administration of bronchodilator.30 In the literature there is inconsistency about the correlations between FeNO and ACT scores in children.31 Furthermore, there is no consensus that the measurement of FeNO has a predictive value of asthma control compared to lung function tests or that regular measurement of FeNO is beneficial in dose adjustment of steroids.9 It was noted before that among different control measures, the worst agreement was for FeNO and ICS.32 FeNO levels, whether expressed as a continuous variable or dichotomized, were not associated with future risk for exacerbations in either unadjusted or adjusted models.33
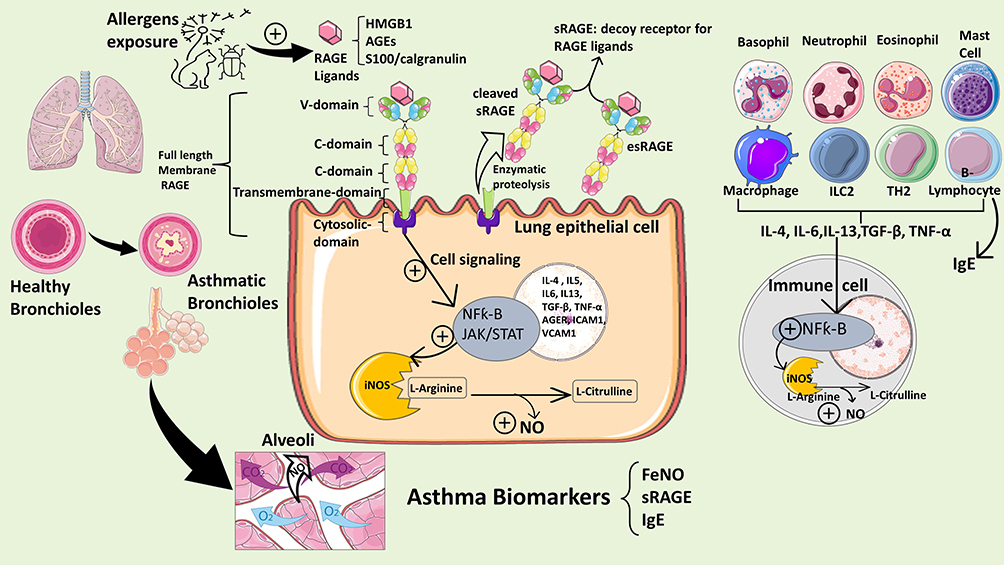 |
Figure 4 This schematic summarizes the mechanisms underlying allergic airway inflammation in asthma involving RAGE signaling and biosynthesis of nitric oxide (NO). Allergens trigger release of RAGE ligands such as HMGB1, S100/calgranulins which bind to and activate RAGE on lung epithelial cells. RAGE structure is depicted showing its variable domain (V-domain), two constant domains(C-domain), and cytosolic domain. The RAGE protein exists as full-length membrane-bound RAGE (mRAGE), as well as a soluble form (sRAGE), which lacks the transmembrane and signaling domains, and functions as a decoy receptor. sRAGE can be produced endogenously by alternative splicing (esRAGE) or through proteolytic cleavage of the full-length mRAGE. Upon ligand binding, intracellular signaling cascades are initiated which leads to transcriptional activation of NF-κB- and STAT-dependent gene transcription. RAGE-dependent activation of NF-κB induces a positive feedback loop by inducing RAGE (AGER gene) and NF-kB gene transcription and is suspected to stimulate release of cytokines that activate resident immune cells in the lung and is also released into the circulation to activate TH2 cells and ILC2s producing large amounts of IL-4, IL-5 and IL-13 and other cytokines activating B cells to produce allergy-specific globulins (IgE). The IgE specific to allergens will then bind to eosinophils to exacerbate allergic airway inflammation and airway hyperresponsiveness. The biosynthesis of NO in the airways is induced by inducible NO Synthase (iNOS) expressed in lung epithelial cells and inflammatory cells (basophils, eosinophils, neutrophils, mast cells, B or T lymphocytes). NO produced intracellularly will diffuse to the lumen of the airways. Upregulation of iNOS induced by NF-kB during allergic inflammation generates elevated level of exhaled NO in the bronchial airways which can be detected as “FeNO” indicating degree of inflammation. Abbreviations: RAGE, receptor for advanced glycation end products; sRAGE, soluble receptor for advanced glycation end products; esRAGE, endogenously soluble receptor for advanced glycation end products; HMGB1, high mobility group box-1; FENO, fraction of exhaled nitric oxide; NO, nitric oxide; iNOS, inducible nitric oxide synthase; NF-kB, nuclear factor-kappa B; TGF-β, transforming growth factor- β; TNF-α, tumor necrosis factor- α; JAK/STAT, Janus kinase/ The signal transduction and activator of transcription; AGER, RAGE gene; ICAM1, Intercellular adhesion molecule 1; VCAM1, vascular cell adhesion molecule 1; ILC2, type 2 innate lymphoid cells; TH2, T-helper 2-high; IL, interleukins; IgE, Immunoglobulin type E. The figure was constructed by using pictures from Servier Medical Art. Servier Medical Art by Servier is licensed under a Creative Commons Attribution 3.0 Unported License (https://creativecommons.org/licenses/by/3.0/). |
As allergic asthma is the most prevalent phenotype among asthmatic children, reduced FeNO levels to a level comparable to control group may be explained by ICS use in the majority of asthmatic children of the current study. In this regard, a previous study demonstrated that FeNO was a poor indicator of asthma control in children on asthma medication as it exhibited low accuracy to discriminate well-controlled from not well-controlled asthma.34 In essence, it is more likely that patients with poor disease control are more frequently treated with high doses of ICS resulting in lower FeNO levels as compared to less severe forms of the disease due to their immune-suppressive effects.35 However, logistic regression analysis for factors affecting FeNO levels in this study revealed significancy for age and only a trend for ICS use which might be due to the size limitation of our study.
In accordance, a previous study reported that for asthmatic patients regardless of treatment, FeNO levels were not related to asthma control or other clinical variables. In the former study, among untreated patients, higher FeNO values were associated with the occurrence of cough or wheeze, while in patients on ICS, adherence to therapy was the only determinant to degree of inflammation.36 Furthermore, recent studies found that even using asthma medications in doses that lowers FeNO levels cannot improve clinical markers of asthma control, therefore improvement in asthma control measures did not seem to be detected.37 FeNO measurement was suggested previously to aid in diagnosing asthma or predicting asthma development in wheezing children.38 FeNO has been suggested by several reports as useful screening tool for asthma, although several factors were shown to confound the interpretation of an elevated FeNO level such as atopy and smoking.39 Several reports indicated that FeNO can be used as a marker to evaluate patient’s adherence to treatment plan and predict response to different medications as reviewed recently.38 Although, FeNO-guided asthma management was shown previously to have promising benefits, most clinical trials had variable effectiveness.40,41 In a Meta‐analysis study, FeNO‐guided asthma management strategy was shown to partially improve the outcomes of pediatric asthma by reducing asthma exacerbations and improving the forced expiratory volume in a second (FEV1), at the expense of increased ICS dose without any beneficial effects on symptom control, quality of life.39 In the setting of chronic inflammatory airway disease including asthma, conventional tests such as FEV1, reversibility or provocation tests are indirectly associated with airway inflammation. However, FeNO is suggested to be advantageous for asthma patients’ clinical management including direct detection of eosinophilic airway inflammation, anticipation of corticosteroid responsiveness, assessment of airway inflammation to evaluate need of corticosteroids and adjust dosing and revealing otherwise unsuspected lack of adherence to corticosteroid therapy.9
In contrary to our findings in Jordan, a cross sectional study on asthmatic patients in Vietnam, revealed an inverse correlation between FeNO and ACT score and spirometry indicators of airway obstruction.41 Moreover, significant differences in FeNO were seen between different asthma control groups.41 Additionally, other studies indicated that FeNO values were related to several markers of asthma control, such as nighttime symptoms, beta-agonist use, and bronchodilator reversibility,42 as well as to the use of oral or inhaled steroid treatment.43 In addition, previous studies showed that FeNO was raised in asthmatic children, especially when asthma is uncontrolled and during exacerbations.44 FeNO was associated with eosinophilic inflammation in endobronchial biopsies of children with difficult asthma after systemic steroids treatment, and FeNO measurement was suggested to help with identifying patients with persistent symptoms associated with airway eosinophilia.45
Reviewing literature thoroughly, it’s quite legitimate that the disparity between FeNO and lung function or clinical manifestations might be due to the heterogeneity of studied populations of children including genetic backgrounds and environmental factors, variable inclusion criteria regarding severity of asthma, use of inhaled corticosteroid therapy and dosage, presence of atopy, different techniques used to measure FeNO, as well as different measures for asthma control assessment used. Hence, FeNO is still suggested as a complementary tool rather than a solely diagnostic tool to be used along with lung function tests to assess airway inflammation, and to enhance control of asthma symptoms with better use of asthma medications.46
On the other hand, we show that serum soluble RAGE level and ratio of esRAGE/RAGE have potential usefulness as markers of asthma, but not as asthma control indicator as they were only significantly different between asthmatic and control patients. This was supported by ROC analysis which revealed that both sRAGE or esRAGE/sRAGE ratio have significant validity as a screening or diagnostic tool for asthma. Similarly, a previous study on Egyptian population found that serum sRAGE levels were decreased in asthmatic subjects compared to healthy controls and were lowest in subjects with neutrophilic phenotype.47 Additionally, reduced plasma sRAGE levels in Chinese children with recurrent wheezing were inversely correlated with increased fraction of exhaled nitric oxide and increased risk of asthma.48 However, our study did not find significant correlations between FeNO and any of RAGE markers in all study participants or in asthmatic children. Association analysis in another study revealed that increase in sRAGE concentration was associated with lower odds of asthma.49 Moreover, sRAGE was identified as putatively causal for and protective against asthma.49
Experimental studies support our findings as they demonstrate compelling evidence on the role of reduced levels of sRAGE predisposing to asthma development or aggravating inflammation. Experimental models for allergens -induced sensitization revealed that allergens exposure induces T2 inflammation in mRAGE-dependent pathway.17,50 Similarly, another study showed that allergen-dependent activation of a toll-like receptor-4 (TLR4) induces secretion of High mobility group box-1 (HMGB1) which in turn binds RAGE to induce allergic sensitization and amplify inflammation.51
Therefore, sRAGE may present a putative therapeutic target in asthma treatment or prevention. Previous experimental studies demonstrated that sRAGE works as a decoy receptor and administration of sRAGE diminishes lipopolysaccharides-induced T-helper 1 and T-helper 17 cytokines.20 In neutrophilic asthma, sRAGE prevents T-helper17-mediated airway inflammation in neutrophilic asthma at least partly by blocking HMGB1/RAGE signaling.20 Furthermore, a previous work indicated that plasma sRAGE may be a biomarker of severe asthma and may be associated with genetic polymorphism of RAGE G82S gene variants in neutrophilic asthmatics.18
Whereas in a well-treated and controlled population in another study, there were no differences in plasma sRAGE levels compared to control children.52
Regarding esRAGE levels, we utilized an ELISA kit that only detects the soluble splice variant of RAGE (esRAGE) and does not cross react with cleaved mRAGE to investigate whether it has a potential usefulness as marker for asthma. Indeed, we did not find any differences in esRAGE levels between asthmatic and control children, or among all participants. Although esRAGE was extensively studied as a biomarker in many chronic diseases, previous findings about esRAGE in asthma were limited and contradicting. In induced sputum, esRAGE levels were significantly higher in asthmatic patients than in normal controls.53,54 However, there was no significant increase in esRAGE level associated with severity of asthma.54 In another study, systemic sRAGE that was significantly correlated to esRAGE was decreased in subjects with neutrophilic asthma or COPD compared to those without airway neutrophilia who had similar to control levels.19 As our study did not either measure sputum esRAGE or identify the endotype of asthma, comparison with latter findings is not valid. It is intriguing that the total sRAGE was lower in asthmatic than control in the present study while no differences in esRAGE levels were detected which can be either due to reduced levels of mRAGE or shedding of mRAGE due to changes in the regulation of enzymes responsible for cleaving the mRAGE.22
ROC analysis in this study revealed that neither sRAGE markers nor FeNO were useful to assess control level of asthma using ACT as gold standard. This might be related to limitations due to the number of subjects included in this study, to the disparity between ACT measure and the studied markers, or probably ACT control measure could be inferior to these markers in differentiating between asthmatic children in term of control level.
Conclusion
The current study supports utilizing sRAGE as a marker for asthma and emphasizes its role in asthma as a potential therapeutic target. However, our results indicate that both FeNO and sRAGE have a limited role in the management of asthmatic children or assessment of asthma control.
Abbreviations
FeNO, Fraction of exhaled nitric oxide; RAGE, advanced glycation end-product receptor; sRAGE, soluble RAGE; esRAGE, endogenously soluble isoform of RAGE; mRAGE, plasma membrane bound RAGE; ACT, asthma control test; TH2-high, T-helper 2-high; TH2-low, T-helper 2-low; AUC, area under the curve; df, degree of freedom; asymp. Sig, asymptotic significance; ACT, Asthma control test; cACT, children ACT; ICS, inhaled corticosteroids; FEV1, forced expiratory volume in 1 minute; TLR4, toll-like receptor-4; HMGB1, High mobility group box-1.
Funding
This study was funded by The Scientific Research Board of The University of Jordan, Amman, Jordan, Grant #448-2019/2020.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bhakta NR, Woodruff PG. Human asthma phenotypes: from the clinic, to cytokines, and back again. Immunol Rev. 2011;242(1):220–232. doi:10.1111/j.1600-065X.2011.01032.x
2. Al-Sheyab NA, Alomari MA. Prevalence, associated factors, and control level of asthma symptoms among adolescents in Northern Jordan. Int J Adolesc Med Health. 2018;32(3). doi:10.1515/IJAMH-2017-0159
3. The Hashemite Kingdom of Jordan The Higher Health Council. The national strategy for health sector in Jordan; 2015.
4. Abu-Ekteish F, Otoom S, Shehabi I. Prevalence of asthma in Jordan: comparison between bedouins and urban schoolchildren using the international study of Asthma and allergies in childhood Phase III protocol. Allergy Asthma Proc. 2009;30(2):181–185. doi:10.2500/AAP.2009.30.3208
5. Mulholland A, Ainsworth A, Pillarisetti N. Tools in Asthma evaluation and management: when and how to use them? Indian J Pediatr. 2018;85(8):651–657. doi:10.1007/s12098-017-2462-6
6. Wan XC, Woodruff PG. Biomarkers in Severe Asthma. Immunol Allergy Clin North Am. 2016;36(3):547. doi:10.1016/J.IAC.2016.03.004
7. Darbà J, Ascanio M, Syk J, Alving K. Economic evaluation of the use of FeNO for the diagnosis and management of Asthma patients in primary care in Sweden. Clin Outcomes Res. 2021;13:289–297. doi:10.2147/CEOR.S306389
8. Mehta S, Lilly CM, Rollenhagen JE, Haley KJ, Asano K, Drazen JM. Acute and chronic effects of allergic airway inflammation on pulmonary nitric oxide production. Am J Physiol Lung Cell Mol Physiol. 1997;272(1):16. doi:10.1152/AJPLUNG.1997.272.1.L124
9. Dweik RA, Boggs PB, Erzurum SC, et al. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011;184(5):602–615. doi:10.1164/RCCM.9120-11ST
10. Global Burden of Disease: GBD cause and risk summaries. Available from: https://www.thelancet.com/gbd/summaries.
11. World Health Organization. Asthma. Available from: https://www.who.int/news-room/fact-sheets/detail/asthma.
12. Albataineh E, Al-Zayadneh E, Al-Shagahin H, Soloman A, Altarawneh A, Aldmour I. Asthma control and its predictive factors in adult Asthma Patients. Orig Artic J Clin Med Res. 2019;11(12):807–817. doi:10.14740/jocmr4021
13. Sachs-Olsen C, Lødrup Carlsen KC, Mowinckel P, et al. Diagnostic value of exhaled nitric oxide in childhood asthma and allergy. Pediatr Allergy Immunol. 2010;21(1–Part–II):e213–e221. doi:10.1111/J.1399-3038.2009.00965.X
14. Karrasch S, Linde K, Rücker G, et al. Accuracy of FENO; for diagnosing asthma: a systematic review. Thorax. 2017;72(2):109 LP–116 . doi:10.1136/thoraxjnl-2016-208704
15. Milutinovic PS, Alcorn JF, Englert JM, Crum LT, Oury TD. The receptor for advanced glycation end products is a central mediator of Asthma pathogenesis. Am J Pathol. 2012;181(4):1215–1225. doi:10.1016/J.AJPATH.2012.06.031
16. Sukkar MB, Ullah MA, Gan WJ, et al. RAGE: a new frontier in chronic airways disease. Br J Pharmacol. 2012;167(6):1161–1176. doi:10.1111/J.1476-5381.2012.01984.X
17. Perkins TN, Donnell ML, Oury TD. The axis of the receptor for advanced glycation endproducts in asthma and allergic airway disease. Allergy. 2021;76(5):1350–1366. doi:10.1111/ALL.14600
18. Lyu Y, Zhao H, Ye Y, et al. Decreased soluble RAGE in neutrophilic asthma is correlated with disease severity and RAGE G82S variants. Mol Med Rep. 2018;17(3):4131–4137. doi:10.3892/MMR.2017.8302/HTML
19. Sukkar MB, Wood LG, Tooze M, et al. Soluble RAGE is deficient in neutrophilic asthma and COPD. Eur Respir J. 2012;39(3):721–729. doi:10.1183/09031936.00022011
20. Zhang F, Su X, Huang G, et al. sRAGE alleviates neutrophilic asthma by blocking HMGB1/RAGE signalling in airway dendritic cells. Sci Rep. 2017;7(1):1–12. doi:10.1038/s41598-017-14667-4
21. Zhou Y, Jiang Y, Wang W, et al. HMGB1 and RAGE levels in induced sputum correlate with asthma severity and neutrophil percentage. Hum Immunol. 2012;73(11):1171–1174. doi:10.1016/j.humimm.2012.08.016
22. Raucci A, Cugusi S, Antonelli A, et al. A soluble form of the receptor for advanced glycation endproducts (RAGE) is produced by proteolytic cleavage of the membrane-bound form by the sheddase a disintegrin and metalloprotease 10 (ADAM10). FASEB J. 2008;22(10):3716–3727. doi:10.1096/FJ.08-109033
23. Hudson BI, Carter AM, Harja E, et al. Identification, classification, and expression of RAGE gene splice variants. FASEB J. 2008;22(5):1572–1580. doi:10.1096/FJ.07-9909COM
24. Li Y, Wu R, Tian Y, Bao T, Tian Z; Allergy ZTAPJ of, 2017 undefined. Fraction of exhaled nitric oxide and soluble receptors for advanced glycation end products are negatively correlated in children with recurrent wheezing. Asian Pac J Allergy Immunol. 2017;35(1):33–37. doi:10.12932/AP0746
25. Patregnani JT, Fujiogi M, Camargo CA, et al. Serum soluble receptor for advanced glycation end products in infants with bronchiolitis: associations with acute severity and recurrent wheeze. Clin Infect Dis an off Publ Infect Dis Soc Am. 2021;73(9):e2665–e2672. doi:10.1093/cid/ciaa1700
26. Liang Y, Hou C, Kong J, et al. HMGB1 binding to receptor for advanced glycation end products enhances inflammatory responses of human bronchial epithelial cells by activating p38 MAPK and ERK1/2. Mol Cell Biochem. 2015;405(1–2):63–71. doi:10.1007/s11010-015-2396-0
27. Exhaled NO. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am J Respir Crit Care Med. 2005;171(8):912–930. doi:10.1164/RCCM.200406-710ST
28. Nathan RA, Sorkness CA, Kosinski M, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004;113(1):59–65. doi:10.1016/j.jaci.2003.09.008
29. Liu AH, Zeiger RS, Sorkness CA, et al. The Childhood Asthma Control Test: retrospective determination and clinical validation of a cut point to identify children with very poorly controlled asthma. J Allergy Clin Immunol. 2010;126(2):267–273, 273.e1. doi:10.1016/j.jaci.2010.05.031
30. Dabbaghzadeh A, Tavakol M, Gharagozlou M. The Role of FENO in comparison to spirometry and ACT in control of children Asthma symptoms. Iran J Allergy Asthma Immunol. 2019;18(5):479–486. doi:10.18502/IJAAI.V18I5.1898
31. Waibel V, Ulmer H, Horak E. Assessing asthma control: symptom scores, GINA levels of asthma control, lung function, and exhaled nitric oxide. Pediatr Pulmonol. 2012;47(2):113–118. doi:10.1002/PPUL.21529
32. Green RJ, Klein M, Becker P, et al. Disagreement among common measures of asthma control in children. Chest. 2013;143(1):117–122. doi:10.1378/chest.12-1070
33. Cabral ALB, Vollmer WM, Barbirotto RM, Martins MA. Exhaled nitric oxide as a predictor of exacerbation in children with moderate-to-severe asthma: a prospective, 5-month study. Ann Allergy Asthma Immunol. 2009;103(3):206–211. doi:10.1016/S1081-1206(10)60183-4
34. Vijverberg SJH, Koster ES, Koenderman L, et al. Exhaled NO is a poor marker of asthma control in children with a reported use of asthma medication: a pharmacy-based study. Pediatr Allergy Immunol. 2012;23(6):529–536. doi:10.1111/J.1399-3038.2012.01279.X
35. Knuffman J, Sorkness C, Lemanske RF; RLJJ of allergy and, 2009 undefined. Phenotypic predictors of long-term response to inhaled corticosteroid and leukotriene modifier therapies in pediatric asthma. J Allergy Clin Immunol. 2009;123(2):411–416. doi:10.1016/j.jaci.2008.11.016
36. Cano-Garcinuño A, Carvajal-Urueña I, Díaz-Vázquez CA, et al. 5 Clinical correlates and determinants of airway inflammation in pediatric Asthma. Jiaci.org. 2010;20(4):303–310.
37. Fritsch M, Uxa S, Horak F, et al. Exhaled nitric oxide in the management of childhood asthma: a prospective 6-months study. Pediatr Pulmonol. 2006;41(9):855–862. doi:10.1002/PPUL.20455
38. Di Cicco M, Peroni DG, Ragazzo V, Comberiati P. Application of exhaled nitric oxide (FeNO) in pediatric asthma. Curr Opin Allergy Clin Immunol. 2021;21(2):151–158. doi:10.1097/ACI.0000000000000726
39. Wang X, Tan X, Li Q. Effectiveness of fractional exhaled nitric oxide for asthma management in children: a systematic review and meta-analysis. Pediatr Pulmonol. 2020;55(8):1936–1945. doi:10.1002/PPUL.24898
40. Majid H, Kao C. Utility of exhaled nitric oxide in the diagnosis and management of asthma. Curr Opin Pulm Med. 2010;16(1):42–47. doi:10.1097/MCP.0b013e328332ca46
41. Nguyen VN, Chavannes NH. Correlation between fractional exhaled nitric oxide and Asthma Control Test score and spirometry parameters in on-treatment- asthmatics in Ho Chi Minh City. J Thorac Dis. 2020;12(5):2197–2209. doi:10.21037/JTD.2020.04.01
42. Covar RA, Szefler SJ, Martin RJ, et al. Relations between exhaled nitric oxide and measures of disease activity among children with mild-to-moderate asthma. J Pediatr. 2003;142(5):469–475. doi:10.1067/mpd.2003.187
43. Taylor DR, Pijnenburg MW, Smith AD, Jongste JCD. Exhaled nitric oxide measurements: clinical application and interpretation. Thorax. 2006;61(9):817 LP–827 . doi:10.1136/thx.2005.056093
44. Pijnenburg MWH, De Jongste JC. Exhaled nitric oxide in childhood asthma: a review. Clin Exp Allergy. 2008;38(2):246–259. doi:10.1111/J.1365-2222.2007.02897.X
45. Payne DNR, Adcock IM, Wilson NM, Oates T, Scallan M, Bush A. Relationship between exhaled nitric oxide and mucosal eosinophilic inflammation in children with difficult asthma, after treatment with oral prednisolone. Am J Respir Crit Care Med. 2012;164(8 I):1376–1381. doi:10.1164/AJRCCM.164.8.2101145
46. Ferrante G, Malizia V, Antona R, Corsello G, La Grutta S. The value of FeNO measurement in childhood asthma: uncertainties and perspectives. Multidiscip Respir Med. 2013;8(1):50. doi:10.1186/2049-6958-8-50
47. El-Seify MYH, Fouda EM, Nabih ES. Serum level of soluble receptor for advanced glycation end products in asthmatic children and its correlation to severity and pulmonary functions. Clin Lab. 2014;60(6):957–962. doi:10.7754/CLIN.LAB.2013.130418
48. Tereshchenko S, Smolnikova M, Belenjuk V, Novitsky I. Soluble receptor for advanced glycation end products (sRAGE) in asthmatic children as a new marker of the disease control. Eur Respir J. 2021;58(suppl 65):A3076. doi:10.1183/13993003.CONGRESS-2021.PA3076
49. Bui H, Keshawarz A, Hwang SJ, et al. A genomic approach identifies sRAGE as a putatively causal protein for asthma. J Allergy Clin Immunol. 2022;149(6):1992–1997.e12. doi:10.1016/j.jaci.2021.11.027
50. Perkins TN, Oczypok EA, Milutinovic PS, Dutz RE, Oury TD. RAGE-dependent VCAM-1 expression in the lung endothelium mediates IL-33-induced allergic airway inflammation. Allergy Eur J Allergy Clin Immunol. 2019;74(1):89–99. doi:10.1111/ALL.13500
51. Ullah MA, Loh Z, Gan WJ, et al. Receptor for advanced glycation end products and its ligand high-mobility group box-1 mediate allergic airway sensitization and airway inflammation. J Allergy Clin Immunol. 2014;134(2):440–450. doi:10.1016/j.jaci.2013.12.1035
52. Magnier J, Julian V, Sapin V, et al. Soluble Receptor of Advanced Glycation End-Products (sRAGE) in pediatric asthma: a prospective study in 68 children aged 7 years. Appl Sci. 2022;12(12):5926. doi:10.3390/APP12125926
53. Koyama H, Shoji T, Yokoyama H, et al. Plasma level of endogenous secretory RAGE is associated with components of the metabolic syndrome and atherosclerosis. Arterioscler Thromb Vasc Biol. 2005;25(12):2587–2593. doi:10.1161/01.ATV.0000190660.32863.CD
54. Watanabe T, Asai K, Fujimoto H, Tanaka H, Kanazawa H, Hirata K. Increased levels of HMGB-1 and endogenous secretory RAGE in induced sputum from asthmatic patients. Respir Med. 2011;105(4):519–525. doi:10.1016/j.rmed.2010.10.016
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.