")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 19
Assessment of Drug-Related Problems and Health-Related Quality of Life Domains in Elderly Patients with Type 2 Diabetes Mellitus
Authors Al-Azayzih A , Kanaan RJ, Altawalbeh SM
Received 7 August 2023
Accepted for publication 4 November 2023
Published 13 November 2023 Volume 2023:19 Pages 913—928
DOI https://doi.org/10.2147/TCRM.S434235
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Deyun Wang
Ahmad Al-Azayzih, Roaa J Kanaan, Shoroq M Altawalbeh
Department of Clinical Pharmacy, Faculty of Pharmacy, Jordan University of Science and Technology, Irbid, Jordan
Correspondence: Ahmad Al-Azayzih, Clinical Pharmacy Department, Faculty of Pharmacy-Jordan University of Science and Technology, Irbid, 22110, Jordan, Email [email protected]
Aims of the Study: This study aimed to investigate the prevalence and predictors of Drug-related problems (DRPs), as well as to evaluate the impact of DRPs on the health-related quality of life in geriatric patients with type 2 diabetes mellitus.
Methodology: A cross-sectional study was conducted over a three-month period. Patients aged 60 years and older visited diabetes clinics from October 1, 2022, to December 31, 2022, were included in the study. Data were collected through structured questionnaires, whereas lab results, medication records, comorbidities, and the consequences of DRPs were collected from electronic medical records. DRPs were identified and classified using the PCNE V501 classification system. Health-related quality of life (HRQoL) was evaluated using the validated EuroQol criteria.
Results: A total of 491 patients participated in the study, and the mean age of the patients was 67.51 years (SD = 5.84 years). Female patients represented 52.34% of total subjects. A total of 461 (around 94%) experienced at least one drug-related problem (DRP), ranging from one to nine DRPs per patient, with a total number of DRPs equal to 1625 identified. The most common DRP was the drug choice problem, affecting 52.98% of patients. Factors such as high drug frequency, living conditions, the number of diabetes medications, comorbidities, and smoking were significantly associated with higher numbers of DRPs. Higher numbers of DRPs were found to significantly worsen health-related quality of life (HRQoL) among patients.
Conclusion: Geriatric individuals with type 2 diabetes mellitus encounter a significant prevalence of DRPs, with drug choice problems being the most common followed by dosing problems. Risk factors contributing to these DRPs include high drug frequency, living conditions, high number of diabetes medications, multimorbidity, and smoking. Also, the study concluded that the increased number of DRPs was associated with negative impact on HRQoL domains in geriatric patients with type 2 diabetes.
Keywords: drug related problems, PCNE, geriatric, diabetes, multimorbidity, polypharmacy, health-related quality of life, HRQoL
Introduction
Elderly patients encounter a higher incidence of drug-related problems (DRPs) due to age-linked changes in their pharmacodynamic and pharmacokinetic parameters, higher prevalence of chronic diseases associated, and their lifetime exposure to multiple and complex medications to control their conditions.1 Multimorbidity, the coexistence of multiple chronic conditions including diabetes, poses significant clinical burden such as frequent visits to healthcare facilities and hospital admissions and significant increase in mortality and morbidities.2,3 Adding to that DRPs could impose financial challenges for both healthcare systems and patients.4
DRPs, according to the Pharmaceutical Care Network Europe (PCNE) definition, refer to events or circumstances related to drug therapy that result in negative health outcomes.5 DRPs do include non-needed drug treatment, insufficient drug management, adverse drug problems, improper drug dose and frequency, futile drug management and inferior medication adherence.
Various prevalence reports from all over the world showed that DRPs were highly prevalent among their geriatric population ranging from 63.3% to 95.9%.3,6,7 Furthermore, a systematic review analysis indicated that drug-related problems (DRPs) account for more than 15.4% of hospital admissions and 2.7% death rate, with individuals on multiple medications (polypharmacy) and older adults being at an elevated risk of hospitalization caused by DRPs.8
Diabetes Mellitus (DM) is a chronic condition characterized by high blood sugar levels due to insulin secretion or resistance issues, causing long-term organ damage, and thus requires proper use of various hypoglycemic medications to control the disease state and slow down the progression towards microvascular and macrovascular complications.9,10
According to statistics, approximately 15% of people (age 50–69 years) and 22% of people (age 70 years or more) suffered from type 2 diabetes in 2017 and prevalence will continue to rise all over the world as expected to equal around 7% of the whole world population by 2030.11 Elderly individuals with type 2 diabetes may face multiple DRPs, resulting in a poor Health-Related Quality of Life (HRQoL).12 Health-related Quality of Life (HRQoL) refers to a comprehensive concept that includes a patient’s physical, mental, and spiritual functioning, as well as their overall sense of well-being in various aspects of life.13
The EQ-5D is a widely used universal tool for assessing Health-Related Quality of Life (HRQoL). It measures five health dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Patients rate their current health condition within each dimension using a single-digit number, indicating “no issues”, “moderate issues”, or “severe issues”. These ratings are then combined into a 5-digit number, providing an overall representation of the patient’s health state.14
In Jordan, diabetes is a very common condition and according to national surveys from 1994 to 2017, the diabetes prevalence in males aged ≥25 years old increased from 14.2% to reach 32.4% in 2017. The same trend of increased prevalence was noticed among females but with relatively lower prevalence compared to males.15 Reports from the higher population council in Jordan projected that the number of old people (≥60 years) will grow up at a rate of 13.5% of the total population in 2050.16
Previous studies from Jordan have evaluated the DRPs in patients with chronic diseases in both hospital and community pharmacy settings.17,18 However, there is a lack of specific study assessing and evaluating the DRPs among geriatric diabetic patients. So, this study aims to explore the prevalence and factors associated with DRPs as well as their potential impact on health-related quality of life among geriatric patients with type 2 diabetes mellitus.
Methodology
Study Design
Observational cross-sectional study was conducted over three month’s period at King Abdullah University Hospital, Ar-Ramtha, Jordan (KAUH).
Study Sample
Patients with diabetes who met the inclusion criteria and had attended diabetes clinics between October 1, 2022, and December 31, 2022, were invited to participate in this study by signing an informed consent form. Patients eligible to participate in the current study were those aged 60 years of age or older, had type 2 diabetes mellitus, were taking at least two medications, and had the necessary laboratory results available for further analysis.
Sample Size
A minimum sample size of 384 subjects was required to obtain a 95% confidence level with a 5% margin of error, considering standard normal variate at p < 0.05 equal to 1.96 and population proportion of 50% to obtain largest sample size.19
Data Collection
Demographic data and clinical characteristics (age, gender, chronic medications, chronic diseases, medical history) were extracted from the electronic records for patients. Medication adverse reactions were collected through interviews with patients or their caregivers using a structured questionnaire. Open-ended questions were also used to explore any additional concerns or experiences related to drug-related problems (DRPs).
Adverse reactions were identified by directly interviewing the patients, specifically inquiring about any side effects they experienced, as well as any other general reactions.
To obtain patient DRPs, electronic medical records were retrospectively reviewed, including chronic medications, full medical history, and relevant lab results related to their specific conditions. Health-Related Quality of Life (HRQoL) was evaluated using the validated EuroQol instrument.20 EQ-5D was scored to calculate the index value using the crosswalk approach to the currently available three-level version of the EQ-5D (EQ-5D-3L) value sets.21
Identification of DRPs
As per Pharmaceutical Care Network Europe Version 5 (PCNE V501) guidelines, Drug-Related Problems (DRPs) among participants were categorized as follows:
Adverse Reactions
This domain encompasses allergic or non-allergic side effects associated with diabetic medications, such as hypoglycemia, weight gain, and gastrointestinal issues. Patients were asked about any bothersome effects from their medications, and we also found cases where patients needed prophylaxis but did not receive it. For instance, we identified patients on dual anticoagulant/antiplatelet (DAPT) therapy with ulcers who should have received prophylaxis but did not.
Drug Choice Problem
This domain includes the improper choice of medication, its formulation, the duplication of medications from the same therapeutic group or with the same active ingredient, contraindications for drug use, unclear reasons for prescribing a drug, and situations where a drug was necessary but not prescribed. Evaluation involved comparing patient care with recent evidence-based clinical practice guidelines from UpToDate22 to ensure treatment adherence to latest recommendations and avoidance of therapeutic group duplications. Contraindications were assessed based on patient clinical status (kidney function, liver function, past medical history) using information from Lexicomp’s Drug Information Handbook 31st edition.23
Dosing Problem
This domain includes drug dose too low or too high. The appropriateness of drug dosing and adjustments based on kidney and liver function was assessed using Lexicomp’s Drug Information source.23 Only lifelong chronic medications were considered. Kidney function was estimated using the Cockcroft-Gault equation with Ideal Body Weight (IBW) and the latest measured serum creatinine levels, with rounding of serum creatinine to one for those aged 65 years and older to prevent overestimation of creatinine clearance. Liver function evaluation included liver enzyme levels and Child Pugh score for patients with liver cirrhosis.24
Drug Use Problem
This domain includes instances where the drug was not taken/administered at all or not prescribed, and was identified by direct interviews with the patients.
Drug–Drug Interactions (DDIs)
This domain involves manifest or potential drug–drug or drug–food interactions. Identification was done using information from UpToDate, specifying the DDI category along with justification.
Others
This primary domain is identified through direct interviews with the patients, asking for their perceptions of their medications which includes four problems: The patient is not satisfied with the treatment, even though they have been taking the medication(s) correctly. There is not enough awareness about health and diseases, which may lead to potential issues in the future. The patient’s complaints are unclear, and additional clarification is needed. The therapy has not been successful, and the reason for this failure is unknown.
Statistical Analysis
Data analysis was performed using Stata Corp statistical software, Stata: Release 17 (Stata Corp LLC, College Station, TX, USA, 2021). Continuous variables such as age, and number of comorbidities were analyzed in terms of their mean and standard deviation. Categorical variables like gender, BMI, and marital status were presented using frequencies and percentages.
The normality of the data for DRPs and HRQoL was assessed using the Shapiro–Wilk test, revealing that both variables were not normally distributed.
To compare the median number of DRPs between categorical variables, a two-sample Wilcoxon rank-sum test (Mann–Whitney U-test) was conducted. Spearman’s rank correlation was used to examine the association between the number of DRPs and continuous variables, including age, biomedical variables, number of diabetes medications, number of chronic medications, estimated 10-year survival, and Charlson comorbidity index. Furthermore, the Kruskal–Wallis’s test was used to assess differences in the number of DRPs across different levels of drug usage frequency. Statistical significance was set at a 2-sided P-value <0.05. Median regression (Quantile regression) was applied to identify predictors and factors associated with DRPs HRQoL (the utility index value). In both quantile regression models, variables were selected using a backward stepwise process with P < 0.2 to stay.
Ethical Approval
The study proposal was submitted and subsequently approved by the Institutional Review Board of King Abdullah University Hospital (KAUH) at Jordan University of Science and Technology (JUST) (Ref. #53/151/2022). This study complies with the Declaration of Helsinki.
Results
Socio-Demographic Characteristic of the Study Subjects
This study involved 491 elderly patients (age ≥60 years) diagnosed with type 2 diabetes. The average age of the participants was 67.51 years (SD = 5.84 years). Female patients represented 52.34% (n = 257) of the study sample, obese (51.53%), married (81.47%), living with family (93.48%), residing in urban areas (59.67%), had college or university degree (35.85%), were either unemployed or retired (93.69%), and had a low monthly income, less than 500 JD (67.21%). Most of the patients were non-smokers (80.65%) and physically inactive (77.39%). Additionally, more than half of the patients (55.80%) had a family history of diabetes mellitus. The total number of DRPs found in the current study was 1625 DRPs. Patients who did not complete their education had a higher number of DRPs compared to those who had a college/university education (P = 0.002). Similarly, patients with a low monthly income were associated with a higher number of DRPs compared to those with a monthly income higher than 500 JD (p < 0.001). Furthermore, patients with family history of diabetes mellitus had a higher number of DRPs compared to patients without family history, and this difference was statistically significant (p = 0.029). Detailed results on the sample characteristics and DRPs distribution are presented in Table 1.
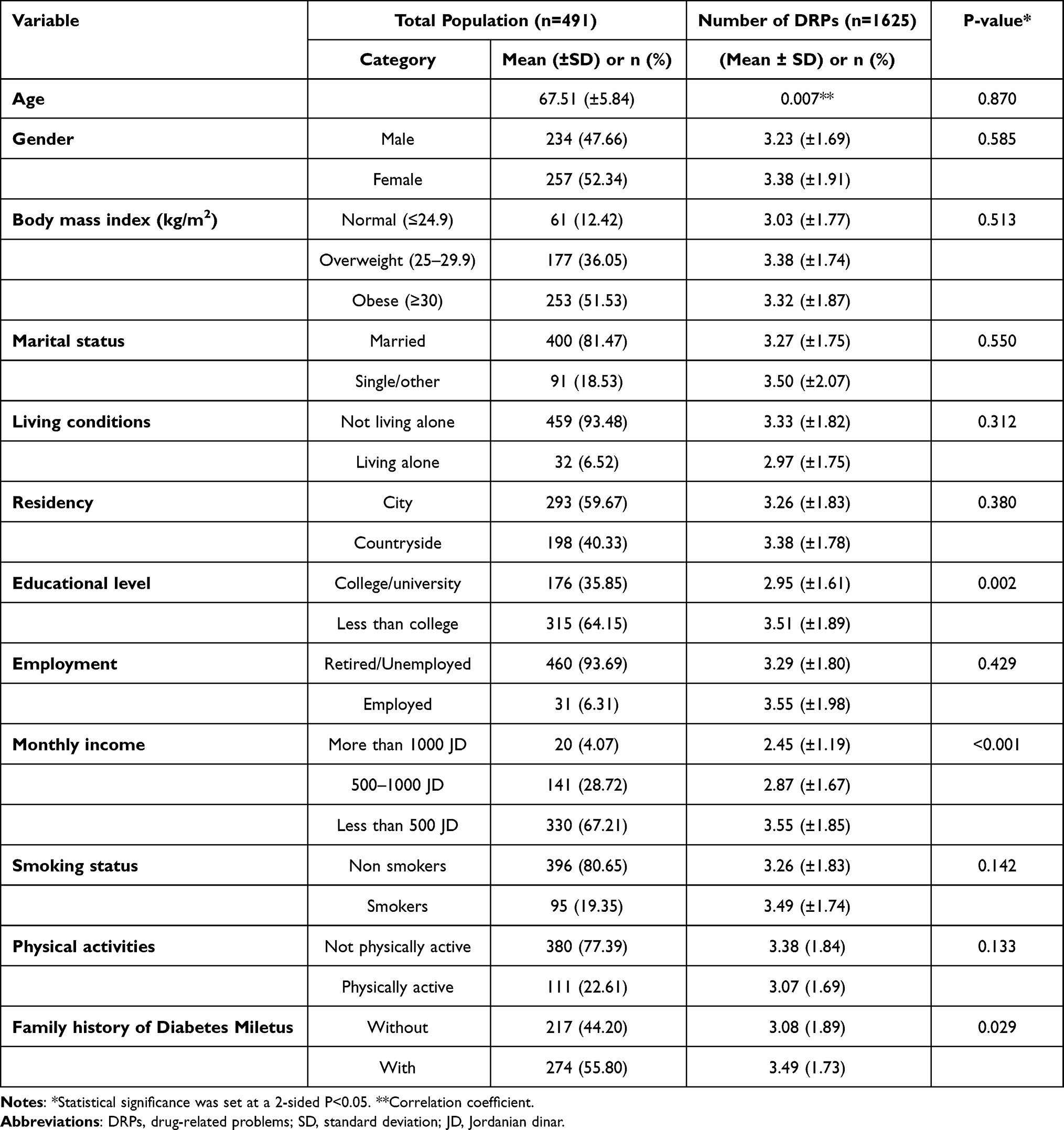 |
Table 1 Socio-Demographic Characteristic of the Study Subjects |
DRPs Distribution by Comorbidities Among Study Subjects
Table 2 presents DRPs distribution by comorbid conditions. Participants with hypertension had a significantly higher mean number of DRPs (3.41) compared to those without hypertension (2.66) (p = 0.005). Similarly, participants with a history of myocardial infarction had a higher mean number of DRPs (3.88) compared to those without myocardial infarction (3.19) (p < 0.001). Participants with heart failure had a notably higher mean number of DRPs (4.46) compared to those without heart failure (3.21) (p < 0.001). Charlson comorbidity index was significantly positively correlated with the number of DRPs (correlation coefficient was 0.130; p = 0.004), suggesting that participants with higher Charlson comorbidity index scores had a higher number of DRPs. The estimated 10-year survival showed a significant negative weak correlation (correlation coefficient was −0.130; p-value = 0.004) with the number of DRPs, indicating that participants with higher number of DRPs had lower estimated 10-year survival.
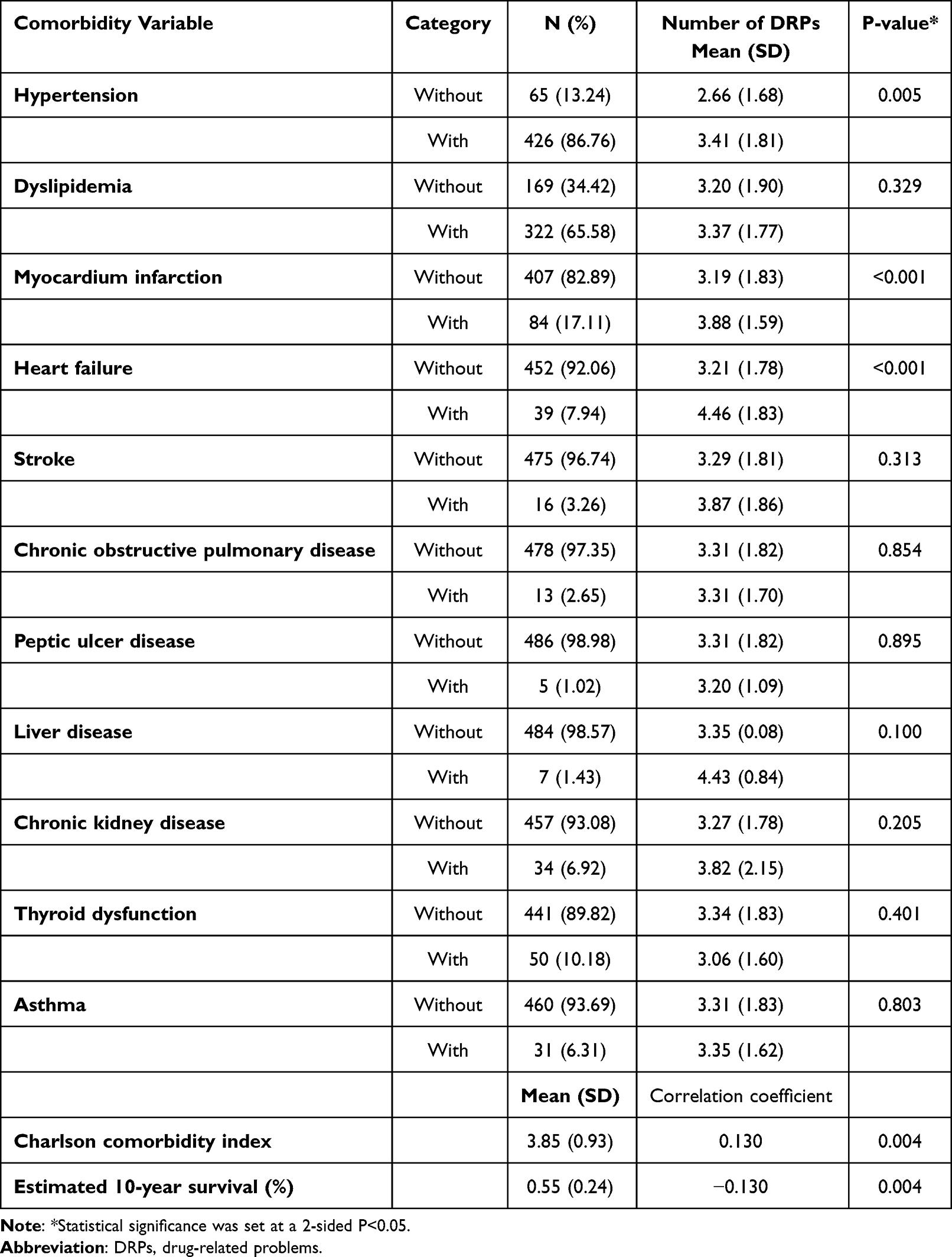 |
Table 2 Disease Characteristics of the Study Subjects |
Medication Characteristics of Study Subjects
Medication frequency was significantly associated with the number of DRPs (p = 0.040). Specifically, participants who took medications three times or more daily had the highest mean number of DRPs (3.54), followed by those taking medication twice daily with a mean of 3.22 DRPs. More details about DRPs distribution by medication characteristics are presented in Table 3.
 |
Table 3 Medication Characteristics of the Study Subjects |
EQ-5D-3L Health Dimensions as Reported by the Study Subjects
Regarding HRQoL analysis, negative correlation was found between the number of DRPs and the estimated utility values (correlation coefficient = −0.237; P value <0.001). Among the five health domains, the activity domain was the most severely affected domain with 25.46% participants expressing an inability to carry out their regular activities, followed by the pain domain (19.35% reported experiencing severe pain) and anxiety domain (18.53% of patients reported experiencing extreme levels of anxiety). EQ-5D-3L health dimensions as reported by the study participants are described in Table 4.
 |
Table 4 EQ-5D-3L Health Dimensions as Reported by the Study Subjects |
Number and Classification of Drug-Related Problems (DRPs) Among Study Subjects
As described in Table 5, out of a total of 491 patients, 461 patients experienced drug-related problems (DRPs), with an average of 3.31 DRPs per patient (SD = 1.81), ranging from (1–9) DRPs per patient. The most common drug-related problem category was the drug choice problem, affecting 52.98% (861 out of 1625) of the patients. Within this category, inappropriate drug selection (not the most appropriate for the indication) accounted for 2.58% (42 out of 1625) of the cases. Additionally, inappropriate duplication of therapeutic group or active ingredient accounted for 0.98% of the cases, contra-indication for drug use constituted 1.78%, drug use without clear indication amounted to 7.02%, and the absence of a prescribed drug despite a clear indication represented a significant portion at 40.62%. Dosing problems accounted for 26.40% of the identified drug-related problems. Among these, cases where the drug dose was too low or the dosage regime was not frequent enough accounted for 25.91%, while cases with drug doses being too high or the dosage regime being excessive made up 0.49% of the cases. A smaller proportion of patients, 0.12%, experienced drug use problems such as not taking or administering the drug at all. Interactions between medications were observed in 1.11% (18 out of 1625) of the cases, encompassing both potential and manifest interactions. Other drug-related problems reported included patient dissatisfaction with therapy despite taking medications correctly (1.11%) and insufficient awareness of health and disease, which potentially leads to future problems, at a rate of 10.09%.
 |
Table 5 Number and Classification of Drug-Related Problems (DRPs) Among Study Subjects |
Drug–Drug Interactions Encountered Among Study Subjects
The most frequent drug–drug interactions were interactions between (candesartan and spironolactone) as well as (bisoprolol and verapamil) with 3 cases for each interaction. Category × Interaction was encountered in 2 patients (interaction between gemfibrozil and atorvastatin). The rest of the drug–drug interactions were classified under category C with the exception of one case which was classified under category D of drug–drug interactions. Table 6
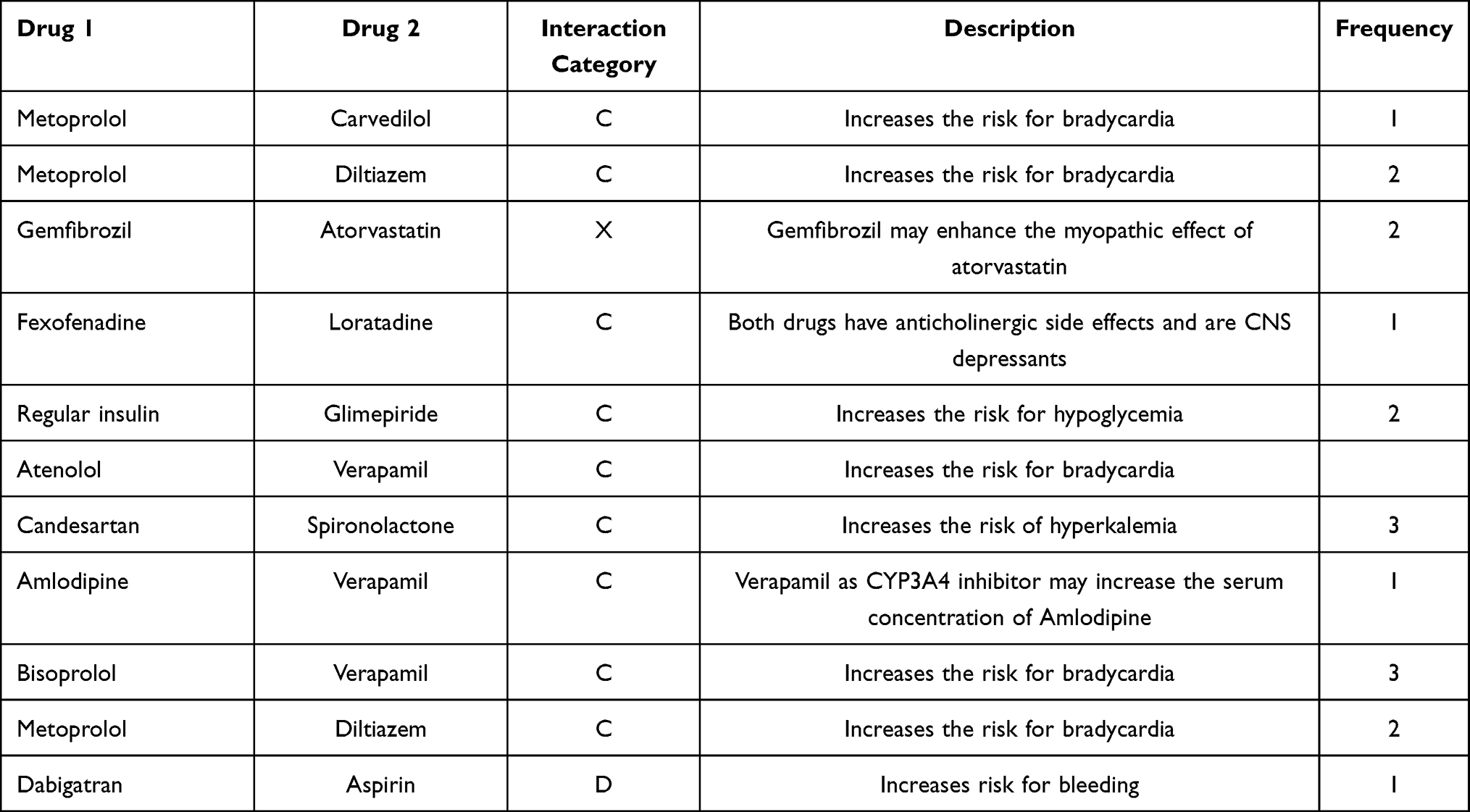 |
Table 6 Drug–Drug Interactions Among Study Subjects |
Adverse Drug Reactions Among Study Participants
The total number of adverse drug reactions reported was 133 adverse events. The most common adverse drug reactions reported by patients were nausea (n = 44, 33.1%), hypoglycemia (n = 17, 12.8%), constipation (n = 15, 11.3%), abdominal pain (n = 11, 8.3%), weight gain (n = 9, 6.8%), headache (n = 8, 6.0%), dizziness (n = 7, 5.3%), and insomnia (n = 4, 3.0%). Other adverse effects such as allergic reactions, skin rash muscle pain, dry cough, dry mouth, fatigue, blurred vision, weight loss, mood changes, and elevated liver enzymes represented 13.4% of the total adverse effects encountered in the study patients. Table 7
 |
Table 7 Adverse Reactions Among Study Subjects (n = 133) |
Variables Associated with the Number of Drug-Related Problems Among Study Subjects
The results demonstrate a significant association between various factors and the number of DRPs. Compared to once per day frequency of drug intake, three times and more drug frequency was associated with higher number of DRPs adjusting for potential confounders (coefficient = 0.483, 95% CI [0.09–0.86], p = 0.015). Also, the number of diabetes medications taken by a patient was positively and significantly associated with the number of DRPs (coefficient = 0.266, 95% CI [0.03–0.50], p = 0.025), and a higher number of comorbidities were significantly associated with a higher number of DRPs (coefficient = 0.323, 95% CI [0.19–0.46], p-value < 0.001). Moreover, patients who are not living alone and those with a monthly income between 500 and 1000 JD (compared to less than 500 JOD) had lower predicted number of DRPs (p-values < 0.05). Being smoker and having a family history of DM were both significantly and positively associated with the number of DRPs (p-values < 0.05). Table 8
 |
Table 8 Variables Associated with the Number of Drug-Related Problems |
Variables Associated with Health-Related Quality of Life (HRQoL) Among Study Subjects
Each additional DRP was associated with a decrease in HRQoL (as indicated by the estimated utility value) by 0.02 units (Coefficient = −0.02, 95% CI [−0.03 to −0.004], p = 0.010). Additionally, female gender was associated with lower utility values compared to males (Coefficient = −0.11, 95% CI [−0.16 to −0.05], p < 0.001). Charlson comorbidity index increases by one point was associated with 0.04 decrease in median utility value (Coefficient = −0.04, 95% CI [−0.07 to −0.01], p-value = 0.006), and similarly higher number of chronic medications were associated with a decrease in median utility value (Coefficient = −0.02, 95% CI [−0.03 to −0.007], p-value = 0.001). On the other hand, having a family history of diabetes, physical activities, and higher educational levels were significantly associated with higher utility values adjusting for potential confounders (P values < 0.05) (Table 9).
 |
Table 9 Variables Associated with Health-Related Quality of Life (HRQoL) |
Discussion
This study is the first to identify both prevalence and associated factors related to the development of DRPs and their effects on health-related quality of life domains in elderly patients with type 2 diabetes mellitus in Jordan.
Our study’s findings showed that DRPs are highly prevalent among older patients, estimated at 94% with average DRPs per patient equal to 3.31. A Previous study evaluated the DRPs among outpatients with chronic conditions has reported an average DRPs equal to 11.2 per outpatient. Same previous study has attributed the elevated instances of DRPs to be associated with older age (>57 years).17 Another study from Jordan, which was conducted on patients diagnosed with chronic diseases and visited community pharmacies, showed that mean DRPs of 4.1 per patients.18 Such disagreement and variations in DRPs prevalence between these studies and our study regarding the mean DRPs reported might be attributed to differences in study populations, study design and methodologies, the nature of chronic comorbidities and healthcare facilities settings evaluated in each study.
The most prevalent drug-related problem found in this study was the drug choice problem, accounting for 52.98%. This finding is inconsistent with the previous work where adverse reactions were found to be the most prevalent in a systematic review analysis study that includes 27 studies.25 A study from Thailand reported that lack of medication adherence category was the most prevalent DRP followed by necessity for adding more drug therapy and adverse drug reactions categories.6
The high prevalence of DRP in the study population was attributed to a set of factors, including the higher utilization of anti-diabetic medications, which is consistent with earlier research findings showing that administering multiple antidiabetic medications increases the risk of medication-related side effects such as hypoglycemia.26 Patients who use many medications to manage their diabetes may be more likely to develop DRPs due to the complexity of their prescription regimens and doses. Also, the possibility of drug–drug and drug–food interactions.
Likewise, a noteworthy correlation was observed between increased frequency of medication intake and a greater occurrence of drug-related problems (DRPs). This result indicates that individuals with more frequent dosing schedules may encounter difficulties in adhering to their prescribed treatment plan, potentially leading to omissions, or skipped doses, which could contribute to the development of DRPs.27
Additionally, there was a strong correlation between multimorbidity and a higher DRPs number. The difficulty of managing numerous chronic illnesses at once can support this link. This could lead to more drug interactions and the need for additional medications, which would raise the number of DRPs.28 This is also in line with the finding of a strong correlation between the number of DRPs and the Charlson Comorbidity Index.
Investigating the association between DRPs occurrence and present comorbidities among geriatric patients. Our results indicated that patients with myocardial infarction (MI), heart failure (HF), and localized solid tumors exhibited a higher number of DRPs compared to other comorbidities which might be attributed to the polypharmacy and use of numerous medications to control their conditions. The use of multiple medications to manage their disease problems could be associated with more medications errors incidences (missing dose, wrong dose, wrong medication schedule), also polypharmacy prescribing cascade of adding more medications to treat other medications side effects as a new medical problem will enhance the risk of drug interactions, adverse reactions, and adherence issues, leading to a higher number of Drug-Related Problems (DRPs) in these patient populations, especially geriatric patients.29
Our study also identified a significant correlation between patients who do not live alone and a lower median number of DRPs. This result implies that having carers or other people nearby to help may improve drug adherence to treatment regimens. Patients who are supported by others may get reminders or help taking their prescriptions as directed, which lowers the risk of DRPs.30
When compared to patients with monthly incomes of less than 500 JD, patients with incomes between 500 and 1000 JD were correlated with lower median number of DRPs. Higher income enables the patient to have better access to medications, healthcare providers, and education, reducing the likelihood of DRPs. Financial stability and the capacity to pay for medications and healthcare services also play a significant role in medication adherence and thus, minimize the risk of DRPs developments.31
Additionally, a greater median number of DRPs was strongly correlated with smoking and having a family history of diabetes. Smoking has a negative impact on general health and medication management and has been linked to several health-related problems. Smoking may alter how some medications are metabolized, resulting in decreased therapeutic levels and an increase in DRPs, particularly if doctors neglected to take smoking into account when treating smoker patients.32 In addition to that, the age-number of DRPs relationship that was shown to be positive is in line with earlier research.3 Patients are more likely to develop DRPs as they age since they frequently have several chronic illnesses and are prescribed many prescription medications.
From other perspectives, the study evaluated the impact of DRPs on HRQoL as well. The median utility value of HRQoL was shown to be negatively correlated with the number of DRPs. To achieve the best results for HRQoL, healthcare providers should consider the holistic management of patients, including psychological and social factors. Patients’ quality of life can be considerably enhanced by identifying and treating DRPs through interdisciplinary collaboration and patient-centered treatment.33
Gender is one of many characteristics that have been linked to HRQoL, with females scoring 0.11 units lower than males. This is consistent with a study from USA that attributed the low HRQoL scores in women compared to men due the impact of both sociodemographic and socioeconomic characteristics on both genders.34 According to previous studies, females suffering from type 2 diabetes are generally experiencing a higher psychological impact such as the feeling of anger, anxiety, and depression associated with their diabetes management concerns and being always under social pressure to carry out their roles in family care, thus affecting their overall HRQOL negatively.35,36 The Charlson comorbidity index negative correlation with HRQoL is another interesting finding from our study. This finding is consistent with a systematic review describing how HRQoL for patients with chronic conditions like diabetes is negatively affected by the load burden of comorbidities.37
In our study, an increase in the number of medications was likewise linked to a decline in HRQoL. (This result is in line with earlier studies that showed polypharmacy has a detrimental effect on HRQoL). Higher pharmaceutical burden was linked to worse HRQoL scores among older persons with chronic conditions such as diabetes.38,39 Increased medication burden is mainly associated with increased patient exposure to health complications and medication adverse events leading to recurrent hospital admissions. Thus, greater need for healthcare support and lack of self-support which could impact their mental health as well as their functional capacity and social well-being status.40,41 In parallel, an Australian cohort study found that polypharmacy consistently had a negative connection with HRQoL in a variety of patient demographics.42 These results underline how crucial it is to tailor prescription regimens and weigh the advantages and disadvantages of polypharmacy to lessen the negative effects on HRQoL.
This study revealed that patients with a family history of diabetes had significantly higher HRQoL scores compared to those without family history of DM. This favorable correlation shows that family support, shared experiences, and genetic predispositions may help people with a family history of diabetes manage their disease and maintain overall wellbeing. Furthermore, the potential social and psychological support received by diabetic patients with family history of DM from their family could positively improve their HRQoL domains. Providing socio-psychological support to elderly diabetic patients would help in DM-associated emotional stress and depression relief, improving patients’ eating habits, and enhancing patients' adherence to their medication regimens.43
Physical activity would provide patients with better control of their blood glucose level and help further in controlling other comorbidities symptoms such as elevated blood pressure and dyslipidemia which will improve patients’ overall quality of life and reduce risk of DM-associated complication and mortality rate.44 Diabetic patients with higher education level can understand their disease status and medication prescribed much better compared to their counterparts which will allow them to comply more effectively with recommended treatments options and lifestyle modifications necessary to control their disease condition.45 This study found a strong relationship between improved HRQoL and both physical activity and higher education levels. These results are in line with a large body of research that shows how physical activity and education can improve HRQoL in people with chronic conditions like diabetes. Numerous studies have shown that regular physical activity, greater levels of education and disease management are all related to health-related quality of life.46
Study Limitations
The sample size was relatively small, comprising only 491 patients, which may not be sufficient to draw definitive conclusions, despite using sample size calculations for patient selection. Furthermore, due to its extensive use in research, compatibility, and user-friendliness, the study used an older version (PCNE v.5) of the classification algorithm rather than the more recent version (v.9). Also, the study is unicentered. However, it is important to note that KAUH is a tertiary hospital that caters to a large and varied population, including various medical cases.
Conclusion
DRPs prevalence among geriatric patients with type 2 diabetes was high (94%). Drug choice and dosing problems were the most common DRPs encountered in this study. DRPs were associated significantly with polypharmacy, smoking, living alone, low monthly income, and presence of numerous comorbidities. Health-related quality of life (HRQoL) was correlated negatively with increased number of DRPs. Future directions to reduce the modifiable risk factors such as polypharmacy prescribing should be followed by healthcare providers to minimize the occurrence of DRPs among geriatrics patients with diabetes, improve their HRQoL and overall patients’ health care. Also, this study results showed the urgent need to conduct more diabetes educational programs to ensure that elderly diabetic patients have the essential knowledge and skills to reach the optimum health outcomes and to reduce both disease and drug-related complications.
Funding
This research was approved by the Deanship of Research at Jordan University of Science and Technology, Irbid, Jordan (Approval #: 559-2022). This study did not receive any financial support or funding.
Disclosure
The authors declare no competing interests in this work.
References
1. Mangoni AA, Jackson SH. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol. 2004;57(1):6–14. doi:10.1046/j.1365-2125.2003.02007.x
2. Chan DC, Chen JH, Kuo HK, et al. Drug-related problems (DRPs) identified from geriatric medication safety review clinics. Arch Gerontol Geriatr. 2012;54(1):168–174. doi:10.1016/j.archger.2011.02.005
3. Hailu BY, Berhe DF, Gudina EK, Gidey K, Getachew M. Drug related problems in admitted geriatric patients: the impact of clinical pharmacist interventions. BMC Geriatr. 2020;20(1):13. doi:10.1186/s12877-020-1413-7
4. Unutmaz GD, Soysal P, Tuven B, Isik AT. Costs of medication in older patients: before and after comprehensive geriatric assessment. Clin Interv Aging. 2018;13:607–613. doi:10.2147/CIA.S159966
5. Pharmaceutical Care Network Europe Association Classification for drug related problems V 5.01. https://www.pcne.org/upload/files/16_PCNE_classification_V5.01.pdf.
6. Paisansirikul A, Ketprayoon A, Ittiwattanakul W, Petchlorlian A. Prevalence and Associated Factors of Drug-Related Problems Among Older People: a Cross-Sectional Study at King Chulalongkorn Memorial Hospital in Bangkok. Drugs Real World Outcomes. 2021;8(1):73–84. doi:10.1007/s40801-020-00219-2
7. Ahmad A, Mast MR, Nijpels G, Elders PJ, Dekker JM, Hugtenburg JG. Identification of drug-related problems of elderly patients discharged from hospital. Patient Prefer Adherence. 2014;8:155–165. doi:10.2147/PPA.S48357
8. Ayalew MB, Tegegn HG, Abdela OA. Drug Related Hospital Admissions; A Systematic Review of the Recent Literatures. Bull Emerg Trauma. 2019;7(4):339–346. doi:10.29252/beat-070401
9. Genuth SM, Palmer JP, Nathan DM, Classification and Diagnosis of Diabetes. Cowie CC, Casagrande SS, Menke A, et al. editors. Diabetes in America.
10. Hoogwerf BJ. Type of diabetes mellitus: does it matter to the clinician? Cleve Clin J Med. 2020;87(2):100–108. doi:10.3949/ccjm.87a.19020
11. Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al Kaabi J. Epidemiology of Type 2 Diabetes - Global Burden of Disease and Forecasted Trends. J Epidemiol Glob Health. 2020;10(1):107–111. doi:10.2991/jegh.k.191028.001
12. Abedini MR, Bijari B, Miri Z, Shakhs Emampour F, Abbasi A. The quality of life of the patients with diabetes type 2 using EQ-5D-5 L in Birjand. Health Qual Life Outcomes. 2020;18(1):18. doi:10.1186/s12955-020-1277-8
13. Haraldstad K, Wahl A, Andenaes R, et al. A systematic review of quality of life research in medicine and health sciences. Qual Life Res. 2019;28(10):2641–2650. doi:10.1007/s11136-019-02214-9
14. Balestroni G, Bertolotti G. EuroQol-5D (EQ-5D): an instrument for measuring quality of life. Monaldi Arch Chest Dis. 2012;78(3):155–159. doi:10.4081/monaldi.2012.121
15. Ajlouni K, Batieha A, Jaddou H, et al. Time trends in diabetes mellitus in Jordan between 1994 and 2017. Diabet Med. 2019;36(9):1176–1182. doi:10.1111/dme.13894
16. Higher Population Council in Jordan. https://www.hpc.org.jo/en.
17. Al-Azzam SI, Alzoubi KH, AbuRuz S, Alefan Q. Drug-related problems in a sample of outpatients with chronic diseases: a cross-sectional study from Jordan. Ther Clin Risk Manag. 2016;12:233–239. doi:10.2147/TCRM.S98165
18. Basheti IA, Qunaibi EA, Bulatova NR, Samara S, AbuRuz S. Treatment related problems for outpatients with chronic diseases in Jordan: the value of home medication reviews. Int J Clin Pharm. 2013;35(1):92–100. doi:10.1007/s11096-012-9713-4
19. Charan J, Biswas T. How to calculate sample size for different study designs in medical research? Indian J Psychol Med. 2013;35(2):121–126. doi:10.4103/0253-7176.116232
20. EuroQol G. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy (New York). 1990;16(3):199–208. doi:10.1016/0168-8510(90)90421-9
21. van Hout B, Janssen MF, Feng YS, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 2012;15(5):708–715. doi:10.1016/j.jval.2012.02.008
22. UpToDate. Available from: www.uptodate.com.
23. Lexi- Comp, Inc. Adult Drug Information Handbook: A Clinically Relevant Resource for All Healthcare Professions.
24. Tsoris A, Marlar CA. Use of the Child Pugh Score in Liver Disease. Treasure Island (FL): StatPearls; 2023.
25. Ni XF, Yang CS, Bai YM, Hu ZX, Zhang LL. Drug-Related Problems of Patients in Primary Health Care Institutions: a Systematic Review. Front Pharmacol. 2021;12:698907. doi:10.3389/fphar.2021.698907
26. Naser AY, Wong ICK, Whittlesea C, et al. Use of multiple antidiabetic medications in patients with diabetes and its association with hypoglycaemic events: a case-crossover study in Jordan. BMJ Open. 2018;8(11):e024909. doi:10.1136/bmjopen-2018-024909
27. Jimmy B, Jose J. Patient medication adherence: measures in daily practice. Oman Med J. 2011;26(3):155–159. doi:10.5001/omj.2011.38
28. Sanchez-Fidalgo S, Guzman-Ramos MI, Galvan-Banqueri M, Bernabeu-Wittel M, Santos-Ramos B. Prevalence of drug interactions in elderly patients with multimorbidity in primary care. Int J Clin Pharm. 2017;39(2):343–353. doi:10.1007/s11096-017-0439-1
29. Troncoso-Marino A, Roso-Llorach A, Lopez-Jimenez T, et al. Medication-Related Problems in Older People with Multimorbidity in Catalonia: a Real-World Data Study with 5 Years’ Follow-Up. J Clin Med. 2021;10(4). doi:10.3390/jcm10040709
30. Kusaslan Avci D. Evaluation of the relationship between loneliness and medication adherence in patients with diabetes mellitus: a cross-sectional study. J Int Med Res. 2018;46(8):3149–3161. doi:10.1177/0300060518773223
31. Ramanath K, Nedumballi S. Assessment of medication-related problems in geriatric patients of a rural tertiary care hospital. J Young Pharm. 2012;4(4):273–278. doi:10.4103/0975-1483.104372
32. Kratz T, Diefenbacher A. Psychopharmacological Treatment in Older People: avoiding Drug Interactions and Polypharmacy. Dtsch Arztebl Int. 2019;116(29–30):508–518. doi:10.3238/arztebl.2019.0508
33. Farha RA, Saleh A, Aburuz S. The impact of drug related problems on health-related quality of life among hypertensive patients in Jordan. Pharm Pract (Granada). 2017;15(3):995. doi:10.18549/PharmPract.2017.03.995
34. Cherepanov D, Palta M, Fryback DG, Robert SA. Gender differences in health-related quality-of-life are partly explained by sociodemographic and socioeconomic variation between adult men and women in the US: evidence from four US nationally representative data sets. Qual Life Res. 2010;19(8):1115–1124. doi:10.1007/s11136-010-9673-x
35. Moeineslam M, Amiri P, Karimi M, Jalali-Farahani S, Shiva N, Azizi F. Diabetes in women and health-related quality of life in the whole family: a structural equation modeling. Health Qual Life Outcomes. 2019;17(1):178. doi:10.1186/s12955-019-1252-4
36. Penckofer S, Ferrans CE, Velsor-Friedrich B, Savoy S. The psychological impact of living with diabetes: women’s day-to-day experiences. Diabetes Educ. 2007;33(4):680–690. doi:10.1177/0145721707304079
37. Makovski TT, Schmitz S, Zeegers MP, Stranges S, van den Akker M. Multimorbidity and quality of life: systematic literature review and meta-analysis. Ageing Res Rev. 2019;53:100903. doi:10.1016/j.arr.2019.04.005
38. Alqallaf SM, Matar L, Ghuloom K, Alabbad K, Alshaikh F, Alhaddad M. Medication-related burden from the perspective of the elderly. Med Pharm Rep. 2022;95(3):320–331. doi:10.15386/mpr-2133
39. Van Wilder L, Devleesschauwer B, Clays E, Pype P, Vandepitte S, De Smedt D. Polypharmacy and Health-Related Quality of Life/Psychological Distress Among Patients With Chronic Disease. Prev Chronic Dis. 2022. doi:10.5888/pcd19.220062
40. Remelli F, Ceresini MG, Trevisan C, Noale M, Volpato S. Prevalence and impact of polypharmacy in older patients with type 2 diabetes. Aging Clin Exp Res. 2022;34(9):1969–1983. doi:10.1007/s40520-022-02165-1
41. Montiel-Luque A, Nunez-Montenegro AJ, Martin-Aurioles E, et al. Medication-related factors associated with health-related quality of life in patients older than 65 years with polypharmacy. PLoS One. 2017;12(2):e0171320. doi:10.1371/journal.pone.0171320
42. Aljeaidi MS, Haaksma ML, Tan ECK. Polypharmacy and trajectories of health-related quality of life in older adults: an Australian cohort study. Qual Life Res. 2022;31(9):2663–2671. doi:10.1007/s11136-022-03136-9
43. Kalra S, Jena BN, Yeravdekar R. Emotional and Psychological Needs of People with Diabetes. Indian J Endocrinol Metab. 2018;22(5):696–704. doi:10.4103/ijem.IJEM_579_17
44. Asfaw MS, Dagne WK. Physical activity can improve diabetes patients’ glucose control; A systematic review and meta-analysis. Heliyon. 2022;8(12):e12267. doi:10.1016/j.heliyon.2022.e12267
45. Aschalew AY, Yitayal M, Minyihun A. Health-related quality of life and associated factors among patients with diabetes mellitus at the University of Gondar referral hospital. Health Qual Life Outcomes. 2020;18(1):62. doi:10.1186/s12955-020-01311-5
46. Marquez DX, Aguinaga S, Vasquez PM, et al. A systematic review of physical activity and quality of life and well-being. Transl Behav Med. 2020;10(5):1098–1109. doi:10.1093/tbm/ibz198
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.