Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
Assessment of COPD-Related Knowledge Among Internal Medicine Nurses: A Cross-Sectional Study
Authors Ma Y, Peng Y ![]() , Chen P, Nie N, Chen Y
, Chen P, Nie N, Chen Y ![]()
Received 22 September 2019
Accepted for publication 2 December 2019
Published 17 December 2019 Volume 2019:14 Pages 2917—2925
DOI https://doi.org/10.2147/COPD.S232055
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chunxue Bai
Yiming Ma,* Yating Peng,* Ping Chen, Na Nie, Yan Chen
Department of Respiratory and Critical Care Medicine, The Second Xiangya Hospital, Central South University, Changsha, Hunan 410011, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Chen
Department of Respiratory and Critical Care Medicine, The Second Xiangya Hospital, Central South University, No. 139 Renmin Road, Changsha, Hunan 410011, People’s Republic of China
Email [email protected]
Background: Since most internal medicine nurses work with chronic obstructive pulmonary disease (COPD) patients daily, their ability to meet the needs of COPD patients is an important issue. Our study aimed to assess COPD-related knowledge in internal medicine nurses.
Methods: A descriptive cross-sectional study including 175 participants was conducted to investigate COPD-related knowledge levels among internal medicine nurses in a large top-ranked tertiary hospital in China. The Bristol COPD Knowledge Questionnaire (BCKQ) was used to test COPD-related knowledge levels in the participants.
Results: Overall BCKQ score for all nurses in this study was 35.76 ± 5.49. In comparison with non-respiratory nurses, the overall score among respiratory nurses was significantly higher (39.01 ± 3.95 vs 33.32 ± 5.23, p < 0.001). The mean scores for four topics (epidemiology, breathlessness, oral steroids, and inhaled steroids) were less than 3 among both respiratory and non-respiratory nurses. Subgroup analysis of specialist respiratory wards showed that nurses in the chronic airway disease ward had the highest overall knowledge score (40.47 ± 4.03). Linear regression analysis demonstrated that the overall BCKQ score was significantly related to the population of nurses (β coefficient = 3.016, 95% confidence interval [CI]: 0.953–5.079, p < 0.01), education (β coefficient = 4.710, 95% CI: 1.979-7.440, p < 0.01) and previous rotation in respiratory wards (β coefficient = 3.871, 95% CI: 1.776-5.967, p < 0.001).
Conclusion: Internal medicine nurses at this tertiary hospital showed deficits in COPD-related knowledge. Appropriate and systematic education about COPD knowledge and strengthening rotation among different wards are necessary for improving COPD-related knowledge levels among internal medicine nurses.
Keywords: COPD, knowledge, nurse, internal medicine, BCKQ
Introduction
Chronic obstructive pulmonary disease (COPD) is a common, preventable and treatable disease that is characterized by persistent respiratory symptoms and airflow limitation that is due to airway and/or alveolar abnormalities usually caused by significant exposure to noxious particles or gases and influenced by host factors including abnormal lung development.1 COPD has become the third leading cause of death all over the world, and around 3 million people die each year from COPD.2 In China, there are nearly 100 million COPD patients, and the prevalence of this disease in the population over 40 years of age is 13.7%.3 In order to reduce the heavy disease burden associated with COPD, joint efforts are required from all sides, including patients, relatives, and health care workers.
The knowledge level of patients regarding COPD is an important factor affecting disease progression.4–6 However, the overall disease knowledge level in COPD patients is poor.7,8 Most subjects claimed to understand their disease and available treatments, but less than half actually understood the symptoms and causes of COPD.7 Another study showed that patients’ knowledge of COPD was poor in several domains including the causes of COPD, the consequences of inadequate therapy and the management of exacerbations.8 Patient education is known to improve the levels of disease knowledge and quality of life.4,5 Furthermore, it could also reduce respiratory-related hospital admissions and emergency department visits among COPD patients.6 However, the lack of knowledge among patients with COPD emphasizes the general lack of patient education.9
Healthcare workers including physicians and nurses are the primary agents involved in patient education, and they play an important role in helping patients improve their self-management skills.10–12 In particular, nurses form the largest group of healthcare workers and they substantially contribute to patient education.13 Since most internal medicine nurses work with COPD patients daily, their ability to meet the needs of COPD patients is a critical factor and it requires them to possess sufficient knowledge of COPD. Therefore, understanding the levels of COPD-related knowledge among internal medicine nurses is important. However, only a few studies have attempted to investigate the COPD-related knowledge levels among internal medicine nurses. Our study aimed to thoroughly investigate COPD-related knowledge levels among internal medicine nurses from multiple perspectives, identify specific aspects of possible knowledge deficits, and explore the relationships between potential factors and knowledge levels.
Methods
Study Design, Setting and Participants
A descriptive cross-sectional study to investigate the COPD-related knowledge levels among internal medicine nurses was conducted in a large top-ranked tertiary hospital in China from August 2019 to September 2019. There were two target populations: (1) Respiratory nurses (nurses working in respiratory wards); 2) Non-respiratory nurses (nurses working in internal medicine wards other than respiratory wards, including cardiology, gastroenterology, nephrology, hematology, and rheumatology wards). Inclusion criteria included: (1) Obtain a full nurse’s license; (2) Working in internal medicine wards including specialized intensive care units. Exclusion criteria included: Unwilling to participate in this study or unable to cooperate. Ethical approval was obtained from the Ethics Committee for the Second Xiangya Hospital, Central South University. All participants signed an informed consent before enrollment.
Data Sources, Bias and Study Size
Self-administrated structured questionnaires were distributed to participants during their work hours. Information regarding basic socio demographic characteristics, including age, gender, education background, years of nursing experience, professional titles, previous rotation experience in respiratory wards, and working wards, was collected. The Bristol COPD Knowledge Questionnaire (BCKQ) was used to test COPD-related knowledge levels in participants. BCKQ is a useful COPD knowledge assessment instrument for broad cross-sectional surveys that was designed by White et al14 and published in 2006. It is composed of 13 topics (epidemiology, etiology, symptoms, breathlessness, phlegm, infections, exercise, smoking, vaccination, inhaled bronchodilators, antibiotics, oral steroids, and inhaled steroids), and each topic contains five items. There are three response options for each item, namely, “True”, “False”, and “Don’t know”. One point is scored if the answer is correct for each item, otherwise, zero point is scored. The overall BCKQ score ranges from 0 to 65, and the knowledge level is positively correlated to the overall score. BCKQ shows good internal consistency for 65 items (Cronbach’s alpha = 0.73) and good test-retest reliability (r = 0.71). The Chinese version of BCKQ was compiled by Wong and Yu et al15 in 2016, and we obtained permission for use from the authors. In order to control potential bias, the eligible criteria were followed strictly, the data were checked independently, and divergences were discussed until coming to a consensus; In addition, the response rate was guaranteed, and no missing data existed in this study. With 80% power and α level at 0.05, the minimum sample size required to yield significant results was achieved with the hypothetical mean overall BCKQ score.16
Statistical Methods
Continuous variables are expressed as mean ± standard deviation (SD) with 95% confidence interval (CI) and categorical variables as number (n) or percentage (%). Independent sample t test and Chi-squared test were performed to investigate intergroup differences. Linear regression analysis was conducted to explore relations between factors and knowledge levels. SPSS Windows Version 23.0 (IBM Corporation, Armonk, NY, USA) and GraphPad Prism Version 7.04 (GraphPad, San Diego, CA) were used to perform statistical analysis. The significance level was set at 0.05.
Results
Participants
Questionnaires were initially distributed to 180 nurses who met the inclusion criteria. Five nurses were excluded because of going on vacation (n=3) or going out for training (n=2). Finally, 175 nurses were included in this study and the response rate was 97.2%, including 75 respiratory nurses and 100 non-respiratory nurses. All questionnaires were completed integrally and there were no missing data. A flowchart diagram of the study is shown in Figure 1.
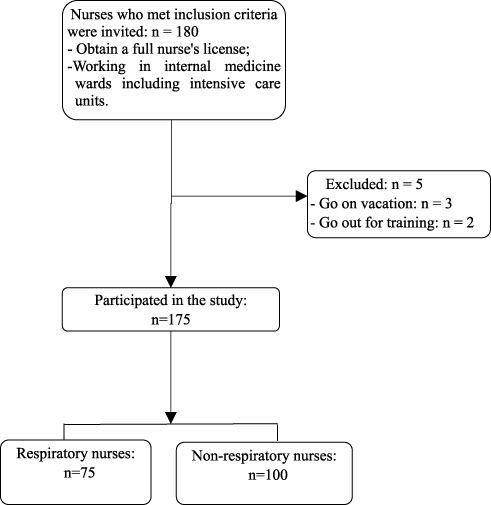 |
Figure 1 Flowchart diagram of this study. |
Descriptive Data
Basic socio-demographic characteristics of the included nurses are listed in Table 1. The respiratory and non-respiratory nurses showed a significant difference only in their previous rotation experience in respiratory wards (p < 0.001). There were no significant differences in other characteristics between the two populations (p > 0.05).
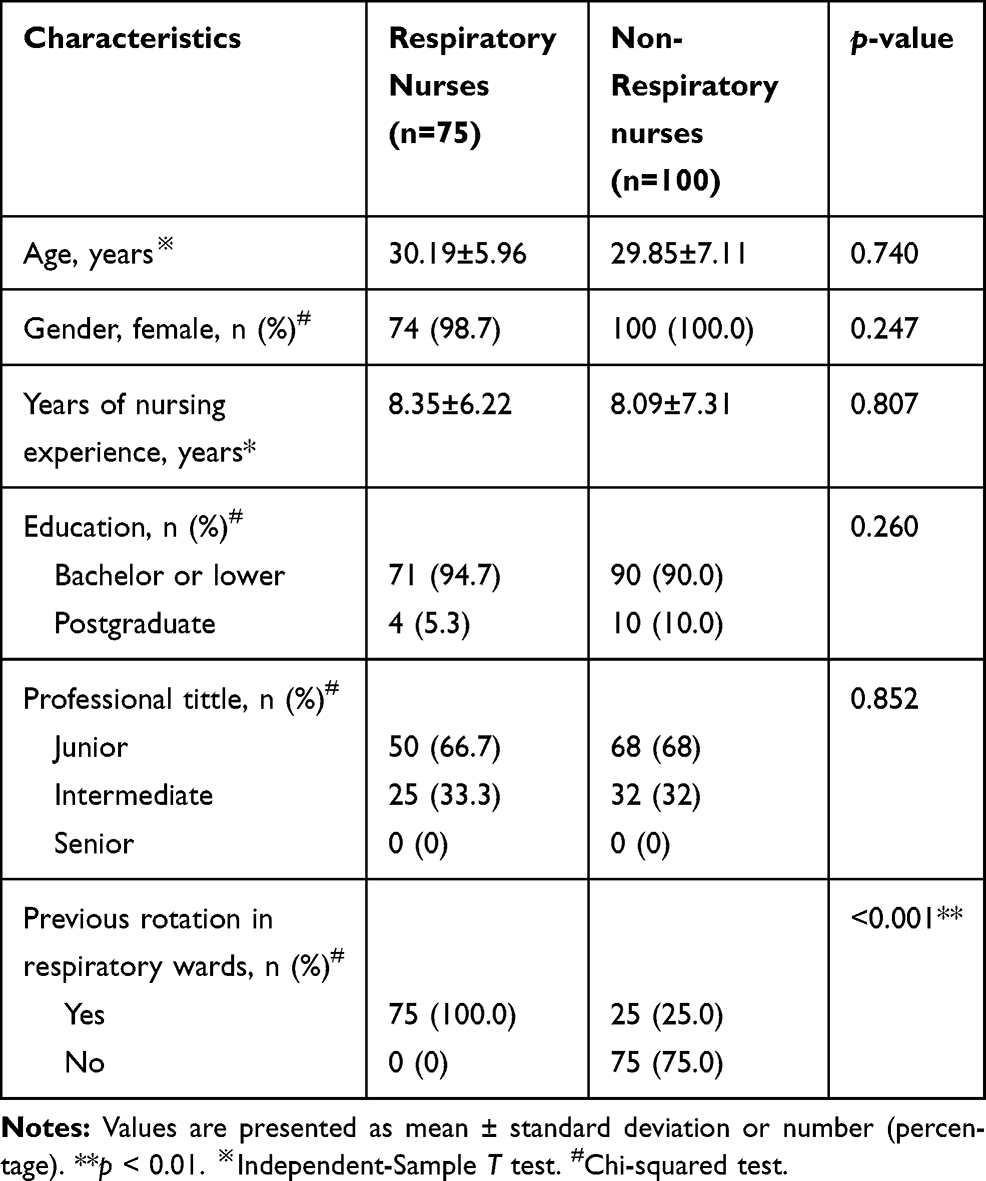 |
Table 1 Basic Socio Demographic Characteristics for Two Populations (n=175) |
Outcome Data
Overall BCKQ scores and scores for each topic in both populations are shown in Table 2. Overall BCKQ score for all participants in this study was 35.76 ± 5.49, and the score for respiratory nurses was significantly higher than that for non-respiratory nurses (39.01 ± 3.95 vs 33.32 ± 5.23, p < 0.001). Knowledge levels regarding epidemiology, symptoms, phlegm, infections, exercise, vaccination, inhaled bronchodilators, antibiotics, oral steroids, and inhaled steroids in respiratory nurses were significantly higher than those in non-respiratory nurses. Among respiratory nurses, mean scores in four topics (epidemiology, breathlessness, oral steroids, and inhaled steroids) were less than 3. Among non-respiratory nurses, mean scores in ten topics (epidemiology, symptoms, breathlessness, infections, exercise, smoking, vaccination, inhaled bronchodilators, oral steroids, and inhaled steroids) were less than 3. The distribution of overall BCKQ scores in the two populations is demonstrated in Figure 2. Based on the median overall BCKQ score (37) among all participants, we considered BCKQ scores no less than 37 (37–65) as indicating better COPD-related knowledge and BCKQ scores less than 37 (0–36) as indicating poorer knowledge. The percentage of subjects with better knowledge among non-respiratory nurses was much smaller (33% vs 76%, p < 0.001).
 |
Table 2 Overall BCKQ Scores and Scores for Each Topic in Two Populations (n=175) |
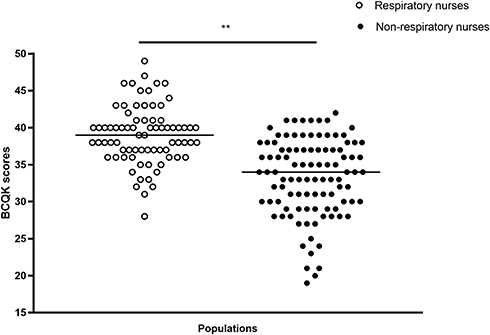 |
Figure 2 Distribution of overall BCKQ scores in two populations (n=175). **p < 0.01. Abbreviation: BCKQ, Bristol COPD Knowledge Questionnaire. |
Table 3 demonstrates the percentages of nurses in both populations giving a correct response for all 65 items indexed by 13 topics and their five items (a, b, c, d, e). Among respiratory nurses, items 8b “Stopping smoking will slow down further lung damage” and 8c “Stopping smoking is pointless as the damage is done” showed the highest percentage of nurses giving a correct response (100%). However, item 4a “Severe breathlessness prevents travel by air” had the lowest correct-response percentage (0%). Among non-respiratory nurses, the highest percentage of nurses giving a correct response appeared for the items 1a “In COPD the word ‘chronic’ means it is severe”, 8b “Stopping smoking will slow down further lung damage”, and 11b “Excessive use of antibiotics can cause resistant bacteria (germs)” (95%). In contrast, the lowest correct-response percentage was found for the items 4a “Severe breathlessness prevents travel by air” and “Steroid inhalers can be used for rapid relief of breathlessness” (4%).
 |
Table 3 Percentages of Participants in Respiratory Nurses (Non-Respiratory Nurses) Giving a Correct Response for All 65 Items Indexed by 13 Topics and Their Five Items (a, b, c, d, e) (n=175) |
The respiratory ward is divided into four specialist wards, namely, the rare disease ward (W1), chronic airway disease ward (W2), tumor ward (W3), and respiratory intensive care ward (W4). Figure 3 shows overall BCKQ scores among nurses in each specialist respiratory ward and the total hospitalization days of all COPD patients in 2018 for each specialist respiratory ward. Nurses in W2 had the highest overall BCKQ score (40.47 ± 4.03), followed by those in W3 (39.15 ± 4.22), W1 (38.83 ± 3.61), and W4 (38.27 ± 3.88), and the total hospitalization length (days) of all COPD patients for each specialist respiratory ward in 2018 from high to low was W2 (4239), W1 (1347), W3 (1160), and W4 (474).
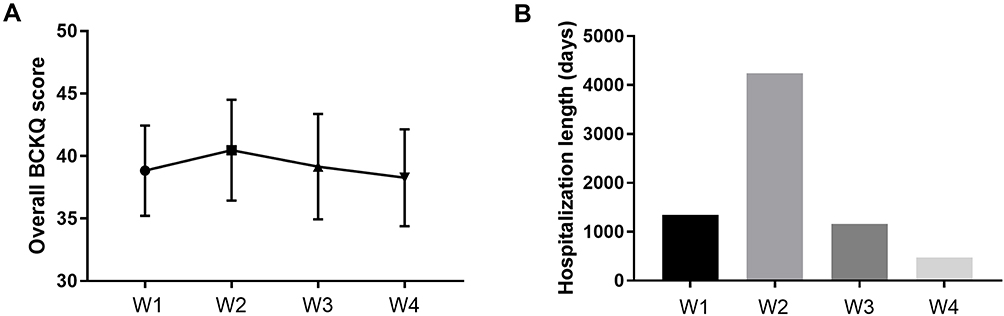 |
Figure 3 Overall BCKQ scores and the total hospitalization length (days) of all COPD patients in 2018 for each specialist respiratory ward. (A) Overall BCKQ scores of nurses for each specialist respiratory ward (n = 75). (B) Total hospitalization length (days) of all COPD patients in 2018 for each specialist respiratory ward. Abbreviations: BCKQ, Bristol COPD Knowledge Questionnaire; W1, rare disease ward; W2, chronic airway disease ward; W3, tumor ward; W4, respiratory intensive care ward. |
Table 4 summarizes the linear regression coefficients (β) of potential factors related to knowledge levels in all internal medicine nurses. Linear regression analysis demonstrated that the overall BCKQ score was significantly related to the population of nurses (β coefficient = 3.016, 95% CI: 0.953–5.079, p < 0.01) and subjects with postgraduate degrees had an excess of 4.710 for overall BCKQ score compared with subjects who had bachelor or lower degrees (95% CI: 1.979–7.440, p < 0.01). Previous rotation experience in respiratory wards showed a significant relation to overall BCKQ score (β coefficient = 3.871, 95% CI: 1.776–5.967, p < 0.001). No relations were found between overall BCKQ score and other factors, including age, years of nursing experience, and professional title.
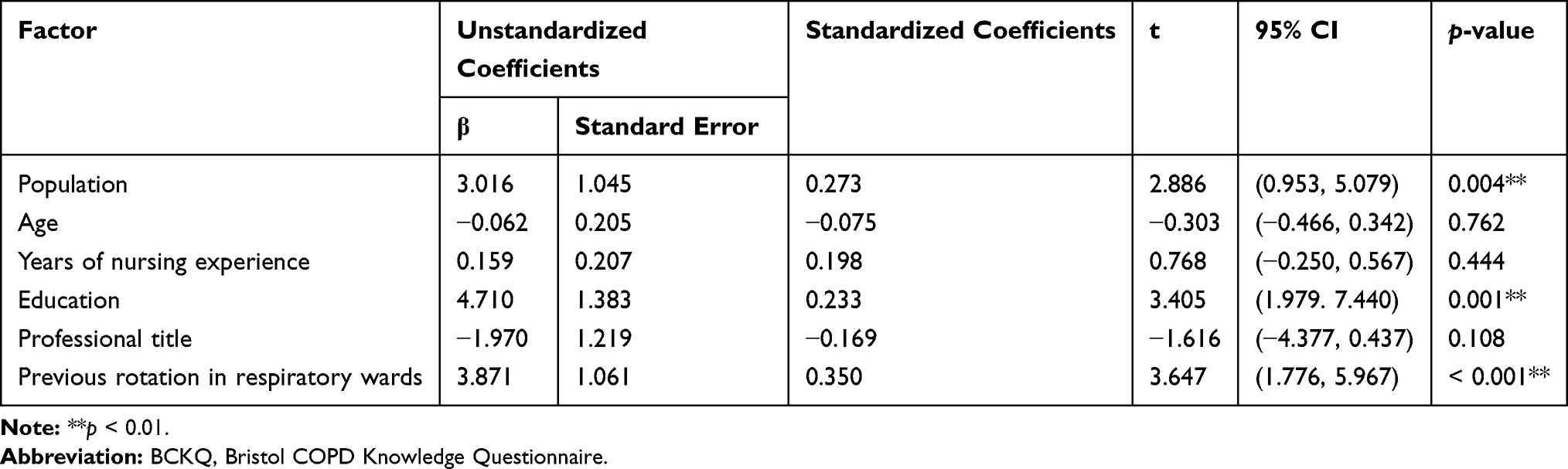 |
Table 4 Linear Regression Coefficients (β) of Potential Factors Related to BCKQ Score in Internal Medicine Nurses |
Considering the median overall BCKQ scores of respiratory nurses (39) and non-respiratory nurses (34) as the respective threshold values, we divided the nurses in each population into two subgroups. Basic sociodemographic characteristics of the subgroups were further compared in Tables 5 and 6. Subgroup analysis of non-respiratory nurses demonstrated that the percentage of nurses who had rotated in respiratory wards was higher among nurses with better knowledge (BCKQ score ≥34) than those with poorer knowledge (36.5% vs 12.5%, p < 0.01).
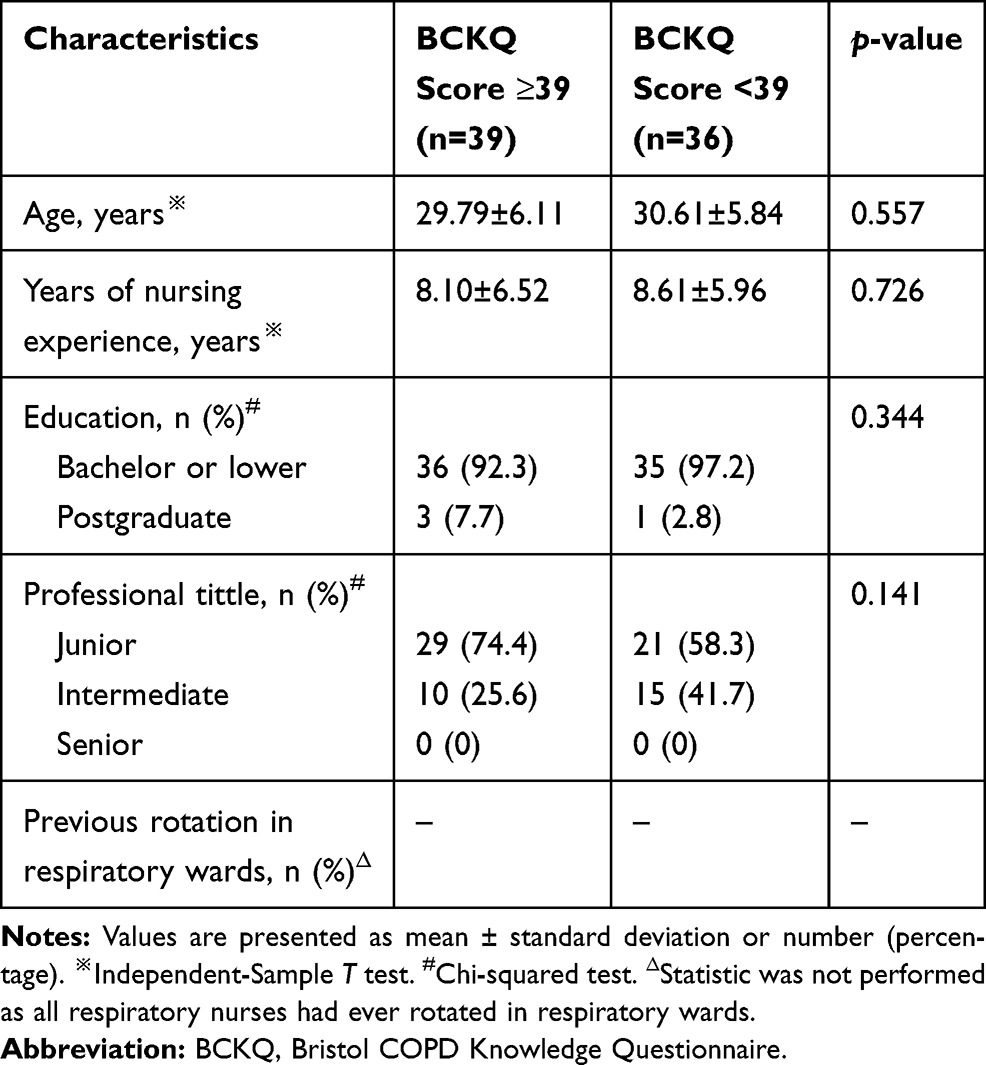 |
Table 5 Comparison of Basic Socio Demographic Characteristics Between Subgroups in Respiratory Nurses (n=75) |
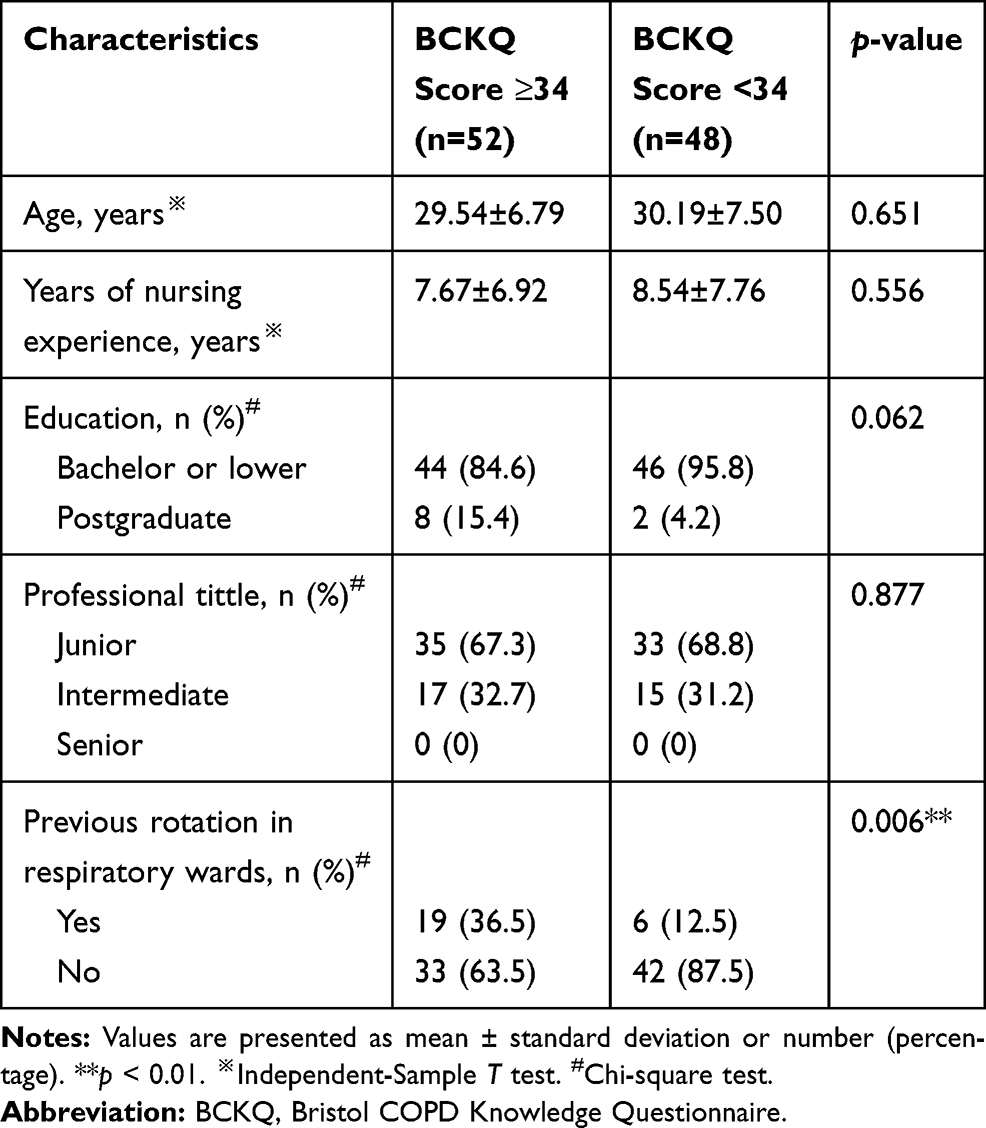 |
Table 6 Comparison of Basic Socio Demographic Characteristics Between Subgroups in Non-Respiratory Nurses (n=100) |
Discussion
This cross-sectional study involved 175 internal medicine nurses, including 75 respiratory nurses and 100 non-respiratory nurses. In comparison with the full score of 65, the overall BCKQ score for all nurses in this study was 35.76 ± 5.49. Surprisingly, when we compared this overall BCKQ score for nurses in our study with the overall score for patients, who had received no education previously, as reported by White et al14 (36.1 ± 5.9) and Wong and Yu et al15 (40.28 ± 10.76), the knowledge level in nurses was lower than that in patients, which indicated poor levels of COPD-related knowledge among nurses.
Respiratory nurses showed significant knowledge deficits in the topics of epidemiology, breathlessness, oral steroids, and inhaled steroids, while non-respiratory nurses showed obvious knowledge deficits in the topics of epidemiology, symptoms, breathlessness, infections, exercise, smoking, vaccination, inhaled bronchodilators, oral steroids, and inhaled steroids. This suggests that internal medicine nurses generally lack COPD-related knowledge for the above-mentioned topics and education about COPD knowledge aiming to nurses can be primarily based on these aspects. Deep analysis for each item showed generally incorrect knowledge about items 1b “COPD can only be confirmed by breathing tests”, 4a “Severe breathlessness prevents travel by air”, 4c “Breathlessness means that your oxygen levels are low”, 7e “Exercise should be stopped”, 8d “Stopping smoking usually results in improved lung function”, 8e “Nicotine replacement therapy is only available on prescription”, 9e “You can have a pneumonia jab and a flu jab on the same day”, 13a “Inhaled steroids should be stopped if you are given steroid tablets”, and 13b “Steroid inhalers can be used for rapid relief of breathlessness” in both populations. Besides, among nurses in respiratory wards, incorrect knowledge about item 2e “Women are less vulnerable to the effects of cigarette smoking than men.” and 12e “Steroid tablets can increase your appetite” was also obvious. There is an urgent need to correct these misconceptions.
In China, nurses are the main source of health-related information. The high rates of wrong responses related to symptoms and treatments indicate a high possibility of wrong information delivery to the public. As expected, the levels of COPD-related knowledge in respiratory nurses were significantly higher than those in non-respiratory nurses. In addition, subgroup analysis of specialist wards showed that COPD-related knowledge level was higher in nurses working in the chronic airway disease ward than in those working in the other three specialist respiratory wards. Moreover, linear regression analysis demonstrated that the knowledge levels of nurses who had rotated in respiratory wards were much higher, indicating an association between previous rotation experience and overall BCKQ score. Besides, subgroup analysis of non-respiratory nurses showed that the percentage of nurses who had rotated in respiratory wards was higher among nurses with better knowledge levels than in those with poorer knowledge levels. These results all further indicate that strengthening rotation among different wards is quite necessary for improving COPD-related knowledge levels among internal medicine nurses, as they are more likely to acquire COPD-related knowledge both actively and passively in this process of rotation.
To improve disease knowledge level and long-term outcomes of COPD patients, effective patient education is of vital importance. The COPD-related knowledge level in patients has been shown to correlate with their self-management behavior.17 In a longitudinal national register study comparing those not participating in education programs to those who did, the health-related quality of life (HRQoL) of non-participants deteriorated significantly.18 Collinsworth et al19 reported that the time to first all-cause and COPD-related readmission appeared shorter for patients receiving education. Dogan and Ovayolu et al20 found that the health education provided by nurses to COPD patients can significantly improve PaO2, PaCO2, FEV1 and SaO2 of patients in the education group. Nurses and physicians are primarily responsible for education and this has also been proved in patients’ perspective.7 Global initiative for chronic obstructive lung disease (GOLD) 2020 indicated that topics of patient education for COPD should cover smoking cessation, correct use of inhaler devices, and early recognition of exacerbation, etc.1 This requires education providers, including nurses and physicians, to have a good knowledge of COPD, so that the quality of education they provide for patients can be guaranteed.
However, the COPD-related knowledge levels among education providers were not as good as expected. A cross-sectional study in Saudi Arabia showed that 61.4% of physicians appeared to be unaware of any COPD guidelines, and 63.6% reported not adhering to guidelines.21 Heikkila et al22 reported that almost half (46%) of the pharmacists did not know that COPD is a national public health issue, and around 50% of the pharmacists were not familiar with the current care guideline on COPD. Perez, et al23 reported poor familiarity with recommendations for COPD among clinicians. Guo et al24 reported that nurses lacked sufficient pulmonary rehabilitation knowledge and skills for COPD and the accuracy rate of PR knowledge was only around 12%. All these results highlight the necessity to carry out appropriate and systematic education about COPD-related knowledge among nurses and physicians.
Since most internal medicine nurses work with COPD patients daily, their ability to meet the needs of COPD patients is critical. Thus, there is a great need for nurses from different wards to master COPD-related knowledge, so that they can provide better health guidance for patients. Strengthening the rotation of internal medicine nurses among different wards may be a useful approach in this regard. A previous study showed that a significant increase in mean knowledge score about the surgical patient population was observed in nurses who underwent rotation.25 Furthermore, Adejumo et al26 reported that nurses with nephrology rotation experience during their training had significantly higher mean knowledge score of chronic kidney disease than others. For respiratory nurses, strengthening professional theoretical knowledge regularly and accelerating the research on a certification system for specialist nurses in the respiratory department are also recommended.
There are some limitations for this study. First, this is a single-center study with participants coming from a large tertiary hospital, so its generalizability is limited, and the results may not represent the COPD-related knowledge levels in nurses from hospitals of different degrees. However, our results could provide powerful evidence to speculate that the state of COPD-related knowledge in lower-degree hospitals might be much worse than expected, and more large-scale studies involving nurses from hospitals of different degrees ought to be performed to prove it. Second, this was an observational study rather than a cause-effect study. Interventional studies that provide a training intervention for nurses can be designed. Finally, there is no specific standard based on the overall BCKQ score range to evaluate the knowledge level, so the scores cannot be used to categorize the participants' knowledge levels (good, fair, or poor) and are only useful for estimating the knowledge level by score. Although these limitations exist, this study serves as a reference for the assessment of each detailed aspect of COPD-related knowledge in internal medicine nurses.
In all, our study thoroughly investigated the current status of COPD-related knowledge among internal medicine nurses from multiple perspectives and gave a further confirm that knowledge level about COPD among healthcare workers was poor. Besides, we also explored the potential factors that may be related to COPD knowledge levels in nurses, which have not been reported previously. A high-quality and widely used questionnaire assessing COPD knowledge, BCKQ, was used, and the results obtained with it added credibility to the study’s findings. This study may provide important reference for the need to improve COPD-related knowledge level among internal medicine nurses.
Conclusion
Internal medicine nurses at this tertiary hospital showed deficits in COPD-related knowledge. Appropriate and systematic education about COPD knowledge and strengthening rotation among different wards are necessary for improving COPD-related knowledge levels among internal medicine nurses.
Ethics Approval and Consent to Participate
The study was reviewed by the chair of the Institutional Review Board in the Second Xiangya Hospital. Written informed consent was obtained from each participant. None of the authors has a financial relationship with a commercial entity that has interest in the subject of this manuscript. The authors declare that they have no competing interests in this work.
Acknowledgments
This project carried out with the support of the National Key Clinical Specialist Construction Projects ((2012) No. 650) and National Natural Science Foundation of China (No. 81400032, No. 81600031, and No. 81873410). We want to thank Dr. YU Wai-cho in Princess Margaret Hospital for providing us the traditional Chinese version of the BCKQ. We are grateful that the statistics expert, Pro. Jingcheng Shi, in Central South University provides us support of statistics methods.
Disclosure
The authors report no conflicts of interest.
References
1. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease 2020 report. Available from: http://goldcopd.org/wp-content/uploads/2019/11/GOLD-2020-REPORT-ver1.1wms.pdf. Accessed Dec 6, 2019.
2. Naghavi M, Wang H, Lozano R, et al. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385(9963):117–171.
3. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health CPH study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
4. Folch-Ayora A, Orts-Cortes MI, Macia-Soler L, Andreu-Guillamon MV, Moncho J. Patient education during hospital admission due to exacerbation of chronic obstructive pulmonary disease: effects on quality of life-controlled and randomized experimental study. Patient Educ Couns. 2019;102(3):511–519. doi:10.1016/j.pec.2018.09.013
5. Chang Y-Y, Dai Y-T. The efficacy of a flipping education program on improving self-management in patients with chronic obstructive pulmonary disease: a randomized controlled trial. Int J Chron Obstruct Pulmon Dis. 2019;14:1239–1250. doi:10.2147/COPD.S196592
6. Wang T, Tan JY, Xiao LDX, Deng RL. Effectiveness of disease-specific self-management education on health outcomes in patients with chronic obstructive pulmonary disease: an updated systematic review and meta-analysis. Patient Educ Couns. 2017;100(8):1432–1446. doi:10.1016/j.pec.2017.02.026
7. Dhand R, Mahler DA, Carlin BW, et al. Results of a patient survey regarding COPD knowledge, treatment experiences, and practices with inhalation devices. Respir Care. 2018;63(7):833–839. doi:10.4187/respcare.05715
8. Hernandez P, Balter M, Bourbeau J, Hodder R. Living with chronic obstructive pulmonary disease: a survey of patients’ knowledge and attitudes. Respir Med. 2009;103(7):1004–1012. doi:10.1016/j.rmed.2009.01.018
9. Uzel FI, Karadag P, Onur ST, Turan D, Yenturk E, Tuncay E. A basic question: are patients with chronic obstructive pulmonary disease aware of their disease? Turk Thorac J. 2017;18(4):114–118. doi:10.5152/TurkThoracJ.2017.16048
10. Yawn BP, Thomashow B. Management of patients during and after exacerbations of chronic obstructive pulmonary disease: the role of primary care physicians. Int J Gen Med. 2011;4:665–676.
11. Benzo R, McEvoy C. Effect of health coaching delivered by a respiratory therapist or nurse on self-management abilities in severe COPD: analysis of a large randomized study. Respir Care. 2019;64(9):1065–1072. doi:10.4187/respcare.05927
12. Baker E, Fatoye F. Patient perceived impact of nurse-led self-management interventions for COPD: a systematic review of qualitative research. Int J Nurs Stud. 2019;91:22–34. doi:10.1016/j.ijnurstu.2018.12.004
13. Alleyne G, Hancock C, Hughes P. Chronic and non-communicable diseases: a critical challenge for nurses globally. Int Nurs Rev. 2011;58(3):328–331. doi:10.1111/j.1466-7657.2011.00912.x
14. White R, Walker P, Roberts S, Kalisky S, White P. Bristol COPD Knowledge Questionnaire (BCKQ): testing what we teach patients about COPD. Chron Respir Dis. 2006;3(3):123–131. doi:10.1191/1479972306cd117oa
15. Wong CK, Yu WC. Correlates of disease-specific knowledge in Chinese patients with COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:2221–2227. doi:10.2147/COPD.S112176
16. Chow SJ, Shao J, Wang H, Lokhnygina Y Sample Size Calculations in Clinical Research. Chapman and Hall/CRC; 2017.
17. Yang H, Wang H, Du L, Wang Y, Wang X, Zhang R. Disease knowledge and self-management behavior of COPD patients in China. Medicine. 2019;98(8):e14460. doi:10.1097/MD.0000000000014460
18. Henoch I, Lofdahl CG, Ekberg-Jansson A. Influences of patient education on exacerbations and hospital admissions in patients with COPD – a longitudinal national register study. Eur Clin Respir J. 2018;5(1):13. doi:10.1080/20018525.2018.1500073
19. Collinsworth AW, Brown RM, James CS, Stanford RH, Alemayehu D, Priest EL. The impact of patient education and shared decision making on hospital readmissions for COPD. Int J Chron Obstruct Pulmon Dis. 2018;13:1325–1332. doi:10.2147/COPD.S154414
20. Dogan U, Ovayolu N. The effects of health education given by nurses to COPD patients on the daily oxygen concentrator usage time. Adv Respir Med. 2017;85(1):15–21. doi:10.5603/ARM.2017.0004
21. Alsubaiei ME, Frith PA, Cafarella PA, et al. COPD care in Saudi Arabia: physicians’ awareness and knowledge of guidelines and barriers to implementation. Int J Tuberc Lung Dis. 2017;21(5):592–595. doi:10.5588/ijtld.16.0656
22. Heikkila JM, Parkkamaki S, Salimaki J, Westermarck S, Pohjanoksa-Mantyla M. Community pharmacists’ knowledge of COPD, and practices and perceptions of medication counseling of COPD patients. Int J Chron Obstruct Pulmon Dis. 2018;13:2065–2074. doi:10.2147/COPD.S159726
23. Perez X, Wisnivesky JP, Lurslurchachai L, Kleinman LC, Kronish IM. Barriers to adherence to COPD guidelines among primary care providers. Respir Med. 2012;106(3):374–381. doi:10.1016/j.rmed.2011.09.010
24. Guo SE, Shen HC, Okoli C, et al. Generalist versus specialist nurses’ knowledge, attitudes, and behavioral intentions toward promoting pulmonary rehabilitation for patients with chronic obstructive pulmonary disease: a cross-sectional correlational study. Medicine. 2018;97(43):e12975. doi:10.1097/MD.0000000000012975
25. Sigsby LM, Yarandi HN. A knowledge comparison of nursing students in perioperative versus other rotations. AORN J. 2004;80(4):699–707. doi:10.1016/S0001-2092(06)61324-0
26. Adejumo OA, Akinbodewa AA, Iyawe IO, Emmanuel A, Ogungbemi O. Assessment of knowledge of chronic kidney disease among non-nephrology nurses in Akure, South-West Nigeria. Saudi J Kidney Dis Transpl. 2018;29(6):1417–1423. doi:10.4103/1319-2442.248288
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.