")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Assessment and Treatment Strategies for the Aesthetic Improvement of the Lower Face and Neck
Authors Chiu A, Bertucci V, Coimbra DD , Li D
Received 10 March 2023
Accepted for publication 7 June 2023
Published 14 June 2023 Volume 2023:16 Pages 1521—1532
DOI https://doi.org/10.2147/CCID.S405639
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Supplementary video of "Aesthetic improvement of the lower face and neck" [ID 405639].
Views: 124
Annie Chiu,1 Vince Bertucci,2 Daniel Dal’Asta Coimbra,3 Dan Li4
1The Derm Institute, Redondo Beach, CA, USA; 2Private Practice, Woodbridge, Vaughan, ON, Canada; 3Department of Cosmetic Dermatology at Santa Casa de Misericórdia, Rio de Janeiro, RJ, Brazil; 4Department of Plastic and Reconstructive Surgery, Chinese People’s Liberation Army General Hospital, Beijing, People’s Republic of China
Correspondence: Annie Chiu, The Derm Institute, 1636 Aviation Boulevard, #201, Redondo Beach, CA, 90278, USA, Tel +1 (310) 939-9800, Fax +1 (310) 939-9888, Email [email protected]
Background: Interest in aesthetic rejuvenation of the lower face and neck is growing, but published expert guidance is limited.
Objective: Review aesthetic concerns of the lower face and neck and provide expert guidance on evaluation and treatment.
Methods: Twelve international experts participated in an advisory board on lower face and neck aesthetic treatment. They completed a premeeting survey and met twice, reviewing responses and discussing patient evaluation and treatment strategies. They developed decision tree algorithms on patient assessment and treatment planning and sequencing, using clinical cases as a reference.
Results: Treatment concerns include neck and lower face skin laxity, structural bone deficiency, insufficient or excess volume, submental fat, jowls, platysma bands, and masseter muscle prominence. Advisors agreed that the lower face and neck may be the most challenging areas to assess and treat; treatment goals include lower facial contour and overall facial harmony/balance. Advisors recommended first ruling out a surgical approach, then determining whether midface treatment is needed to support the lower face, and lastly evaluating the lower face for significant submental fat, excess or insufficient volume, and structural bone deficiency. To treat the lower face and neck, an anatomical layer approach, moving from deep to superficial layers, beginning with structural support, was recommended. Assessment and treatment decision trees were based on this approach.
Conclusion: The lower face and neck are important but underrecognized areas of aesthetic concern. This article provides expert guidance and a suggested algorithm for assessment and treatment aimed at achieving satisfying and harmonious facial aesthetic results.
Keywords: Chin, jaw, patient satisfaction, plastic surgery, treatment outcomes, algorithms, decision trees
Introduction
Aesthetic treatment of the cheeks, midface, and upper face for enhancing facial attractiveness, patient satisfaction, and social perceptions has been described extensively.1–8 However, the neck and the lower face (eg, chin, jaw, perioral area) are also important areas of aesthetic concern, and procedures to improve their appearance are increasing. Aesthetic chin augmentation procedures increased 63% from 2000 to 2020 in the United States (US),9 and a total of 260,747 neck lifts were performed worldwide in 2019, a 16% increase since 2018.10 More than 200,000 lower face cosmetic surgical procedures were performed in the US overall in 2019, representing one-sixth of all the cosmetic surgical procedures performed that year.11 Studies have demonstrated that some patients, such as older women, recognize greater benefits from lower facial treatment options than middle or upper facial treatments.12,13
There is growing interest in less-invasive approaches for improving the appearance of the lower face, such as injectable treatments for reducing submental and jowl fat, tightening neck and jawline skin laxity, minimizing platysma bands, reducing masseter muscle hypertrophy, adding support to areas to address bone loss, and filling lower facial lines.14–17The hyaluronic acid (HA) fillers VYC-20L (Juvéderm® Voluma® XC; Allergan Aesthetics, an AbbVie Company, Irvine, CA) and VYC-25L (Juvéderm® Volux™; Allergan Aesthetics) are marketed worldwide for use in restoring volume and definition to the chin and jawline in adults older than 21 years of age, including approvals in countries in North America, South America, Europe, and Asia.18,19 Deoxycholic acid injections for reducing the appearance of submental fat have been approved in multiple countries (Kybella® [Allergan Sales, an AbbVie Company; Madison, NJ] in the United States; Belkyra® [Allergan Sales] in Canada, Australia, Europe, and South Korea),20 and 135,586 fat-reducing injection procedures were performed in 2020.9 Botulinum toxin type A (BoNTA) injections have been shown to be an effective nonsurgical treatment for a heavy jawline associated with masseter muscle prominence,21–26 for increased prominence of the platysma muscle (one of the hallmark features of an aging neck),27,28 and for recontouring the jawline and relaxing dynamic wrinkles in the lower face and neck.29
Although aesthetic improvement and rejuvenation techniques for the lower face and neck have become increasingly popular, there is a lack of detailed published guidance to assist clinicians with assessment and treatment of these areas,2,14,30 especially in comparison to the breadth of literature devoted to the midface.31 The objectives of this publication were to review aesthetic concerns of the lower face and neck and their importance in achieving a harmonious facial aesthetic outcome, and to provide expert guidance on evaluation and treatment approaches, with decision trees outlining the different noninvasive/nonsurgical treatment options.
Methods
The sponsor invited 12 international physician expert advisors (dermatologists and plastic surgeons who are experts in full-face aesthetic procedures combining different treatment modalities) to participate in a 2-part virtual advisory board meeting. The objectives of the advisory board were 1) to gather feedback on lower face and neck aesthetic assessment and consultation, available treatment modalities, and treatment evaluation and sequencing, and 2) to develop a consistent algorithm for consulting with aesthetic patients about nonsurgical strategies for improving the appearance of the lower face and neck. The advisors completed a premeeting survey on lower face and neck treatment considerations, then met on November 11 and 21, 2020. At the first meeting, the advisors reviewed survey responses and ranked their objectives in treating the lower face and neck. The anatomy of the lower face and neck and age-related changes were reviewed, and advisors discussed how to address changes related to aging; whether there was an optimal approach to address components such as the skin, subcutaneous tissue, the superficial musculoaponeurotic system (SMAS), ligaments, deep fascia, and bone; and whether there is a best-practice sequencing of treatment, such as an anatomical layer approach, moving from deep layers to superficial layers, beginning with adding structural support. The advisors discussed the layer approach to treatment of the lower face and neck, and their specific challenges of treating each region. The advisors also reviewed available treatment options for the lower face and neck and considered 3 patient cases related to assessing and treating the lower face and 3 neck-related cases.
The purpose of the second meeting was to develop decision tree algorithms for the lower face and neck, providing treatment planning and sequencing. The advisors further discussed the 6 cases to aid in development of the assessment and treatment algorithms.
Results
Expert Clinical Opinion on Aesthetic Concerns in the Lower Face and Neck
Figure 1 lists the major aesthetic concerns of the lower face and neck in clinical practice as identified by the expert advisors. The neck and the lower third of the face are often a driving force behind a patient’s initial visit to an aesthetic clinician, with clearly visible treatment priorities being the area around the mouth, the neck, and the chin/jawline. There may be noticeable fat descent in the jowls, neck and facial skin laxity, muscle changes, lower face fat and volume loss, and overall loss of elasticity.32,33 Treatment that considers the lower face and neck in concert with other regions results in high patient satisfaction, as demonstrated by analyses of the positive impact of panfacial aesthetic treatment on patient-reported outcomes from both the US and Canada HARMONY clinical trials.13,34,35
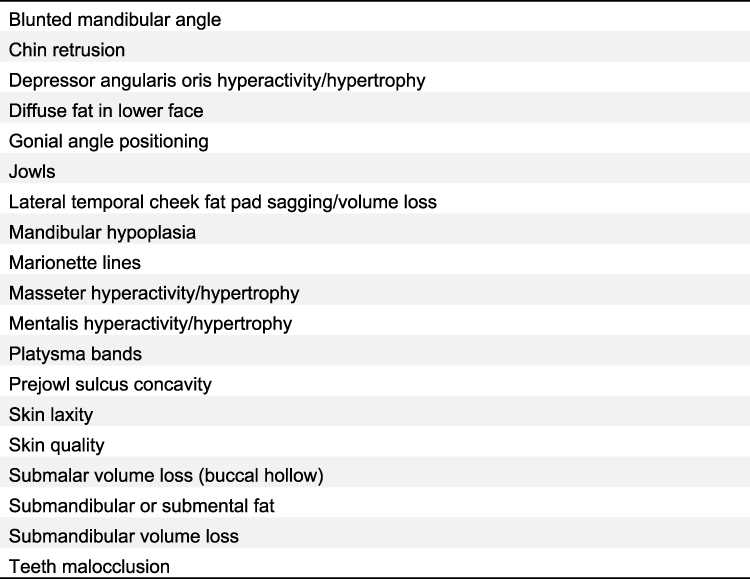 |
Figure 1 An alphabetical listing of the aesthetic concerns of the lower face and neck in clinical practice. |
The advisors agreed that the lower face and neck may be among the most challenging sites of the body to assess and treat because of their complex anatomy;33 the constant mobility of the mandible;36 neck skin laxity that develops with aging, generally after 50 years of age, based on the advisors’ experience;37 and the difficulty of injecting fillers in the thin skin of the neck.37,38 The delicate skin of the neck is also associated with challenges when treatment involves laser and energy-based devices.39 However, neck rejuvenation treatments that may be used successfully include mesotherapy, radiofrequency devices, and injections of dilute HA, biostimulatory agents such as calcium hydroxylapatite and poly-
As sufficient guidance about treatment of the lips exists in the aesthetic literature,40,41 the advisors opted not to include the lips in their discussion and guidance; lower facial contour was the primary concern of the advisory board discussions and this publication. However, lip size and projection contribute to the appearance of a proportionate lower face and are important to consider when treating the nose, chin, and jawline, and the authors recommend measurements such as the Ricketts line to assess the contribution of the lips to a patient’s lower facial contour.42
Expert Clinical Opinion and Recommendations for the Aesthetic Treatment of the Lower Face and Neck
Questions to Ask Before Developing a Treatment Strategy
Based on their clinical practice expertise, the advisors identified 4 main areas of clinical review and assessment to explore when a patient presents with aesthetic concerns of the lower face/neck (Figure 2), in order of importance: 1) ruling out the appropriateness of, necessity of, and patient willingness to undergo a surgical approach; 2) determining whether treatment of the midface is needed first; 3) evaluating the patient’s face for structural bone deficiency; 4) assessing whether there is significant submental fat, excess volume, masseter muscle prominence, or other lower face muscle hypertrophy/hyperactivity; and 5) identifying skin laxity, excess skin, and skin quality issues. The first question is critical for determining how to proceed with the patient; it is important for clinicians to understand whether the patient is more appropriate for surgery and/or a willing surgical candidate before reviewing and selecting nonsurgical treatment options.
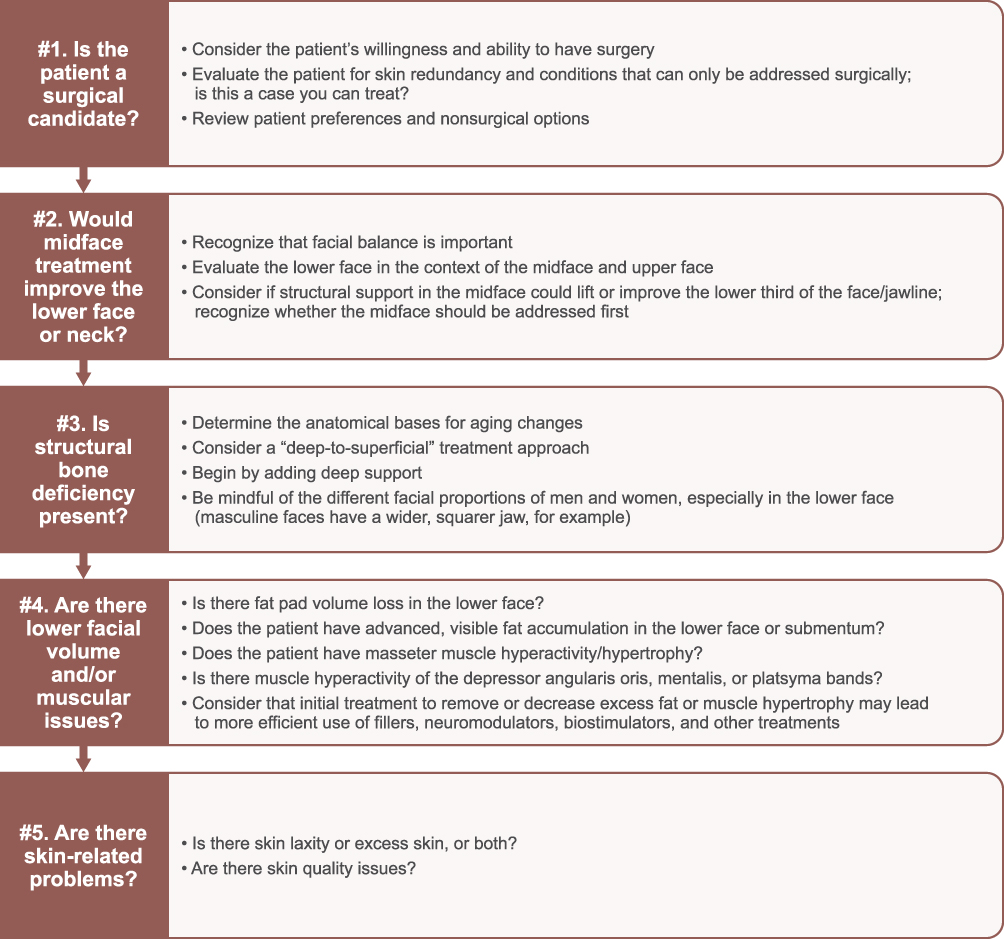 |
Figure 2 Considerations for initial clinical evaluation of patients for aesthetic treatment of the lower face and neck. |
Based on the advisors’ expert experience with favorable outcomes, clinicians are encouraged to evaluate and treat by following a deep-to-superficial anatomical layer approach (from periosteum and deep fascia to ligaments/deep spaces to SMAS to subcutaneous tissue and skin) and to start with treatments that add structural support to the lower face, a technique reinforced by the literature.33,38
The authors suggest that practitioners also keep in mind the variables provided at the bottom of the figure in tandem with the deep to superficial approach. Clinicians are encouraged to assess the patient with all questions in mind while recognizing that a patient often decides feasibility for surgery, treatment preferences, budget, expectations, and other factors that will influence the clinician’s course of action.
Figure 3 outlines the various possible nonsurgical options identified by the advisors. The advisors noted that different layers require different treatment modalities, and patients do not necessarily know which modalities they need. Using the anatomical layer approach will help guide the treatment strategy and can help to explain to patients why a certain modality is or is not appropriate. For example, an energy-based device (ie, laser) rather than a filler is the right modality for a layer 1 (skin) problem.
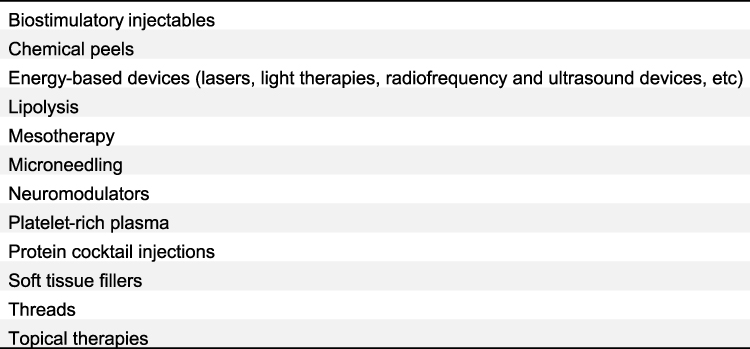 |
Figure 3 Nonsurgical treatment options for the lower face and neck. |
Figures 4–6 describe the initial considerations and questions for the clinician to ask when considering a patient for aesthetic treatment of the lower face/neck, with a decision tree algorithm for each aesthetic treatment consideration. Foremost is evaluating patient candidacy for cosmetic surgery (Figure 4A). The clinician, in concert with the patient, will decide which treatment(s) will make the most difference. For example, if a patient has gross submental fat or skin laxity with excess skin, certain surgical or nonsurgical options may become priorities for treatment (as demonstrated in the decision tree). Figure 4B provides an example of a patient with specific lower face and neck aesthetic concerns that may be best addressed with a combination of nonsurgical and surgical interventions.
 |
Figure 4 (A) Decision tree illustrating considerations for initial clinical evaluation of patient candidacy for surgical correction of lower face/neck; (B) case example of a Hispanic female, 59 years of age, with neck and lower facial aesthetic concerns, which may be most effectively addressed by a combination of nonsurgical (eg, chin retrusion and poorly defined gonial angle) and surgical treatment (eg, skin laxity, mandibular bone loss, blunted mandibular angle, and prominent melomental folds, jowls, and submental fat). Photos courtesy of V. Bertucci, MD. |
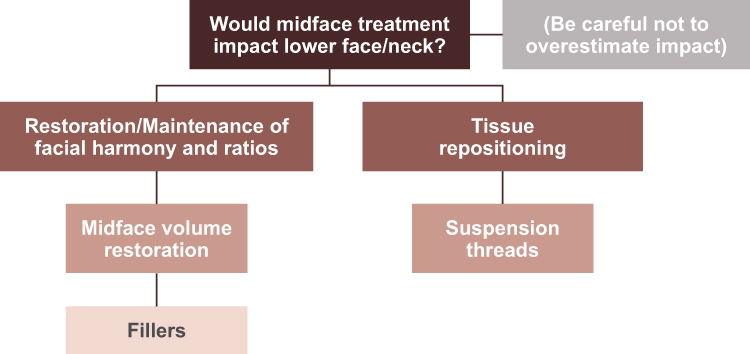 |
Figure 5 Decision tree illustrating considerations for clinical evaluation of patient candidacy for initial midface treatment. |
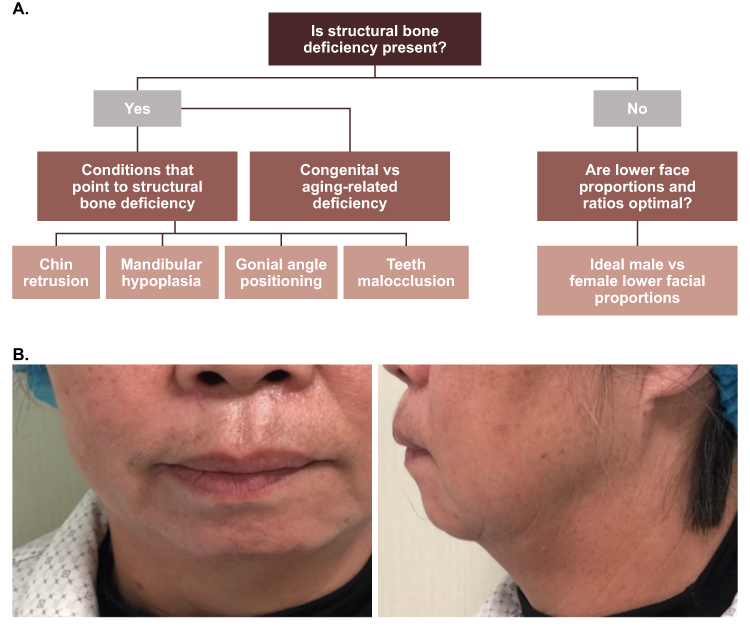 |
Figure 6 (A) Decision tree illustrating considerations for clinical evaluation of structural bone deficiency in the lower face of patients; (B) case example of a female patient 53 years of age with structural bone deficiency in the lower face. Photos courtesy of D. Li, MD. |
The next recommended consideration involves patient candidacy for midface treatment (Figure 5). The lower face should not be evaluated in isolation, as the midface may have a significant impact on the lower face, and midface treatment may improve some of the signs of aging in the lower face.3 Midface assessment is important because facial harmony and balance may be disrupted if the lower face is treated in isolation.14,33
The experts also recommended evaluating the patient for structural bone deficiency (Figure 6A) because it may be a primary contributor to excess skin or perceived laxity. Skin laxity or excess skin (more fully described within Figure 7) may be related to a structural bone deficiency.33 Bone resorption is one of the mechanisms of aging that can affect the contour of the lower face.14,33 If significant bone deficiency is contributing to the appearance of aging in the lower face, treatment requires volume restoration, such as with fillers or biostimulatory agents.14,43 Figure 6B shows a representative patient case example.
Figure 7 Continued. Figure 7 (A) Decision tree illustrating additional considerations for clinical evaluation of aesthetic concerns and potential treatments in the lower face/neck; (B) case example of female patient 44 years of age with masseter muscle hypertrophy, parotid hypertrophy, skin quality issues, chin retrusion, and excess fat. Photos courtesy of D. Li, MD.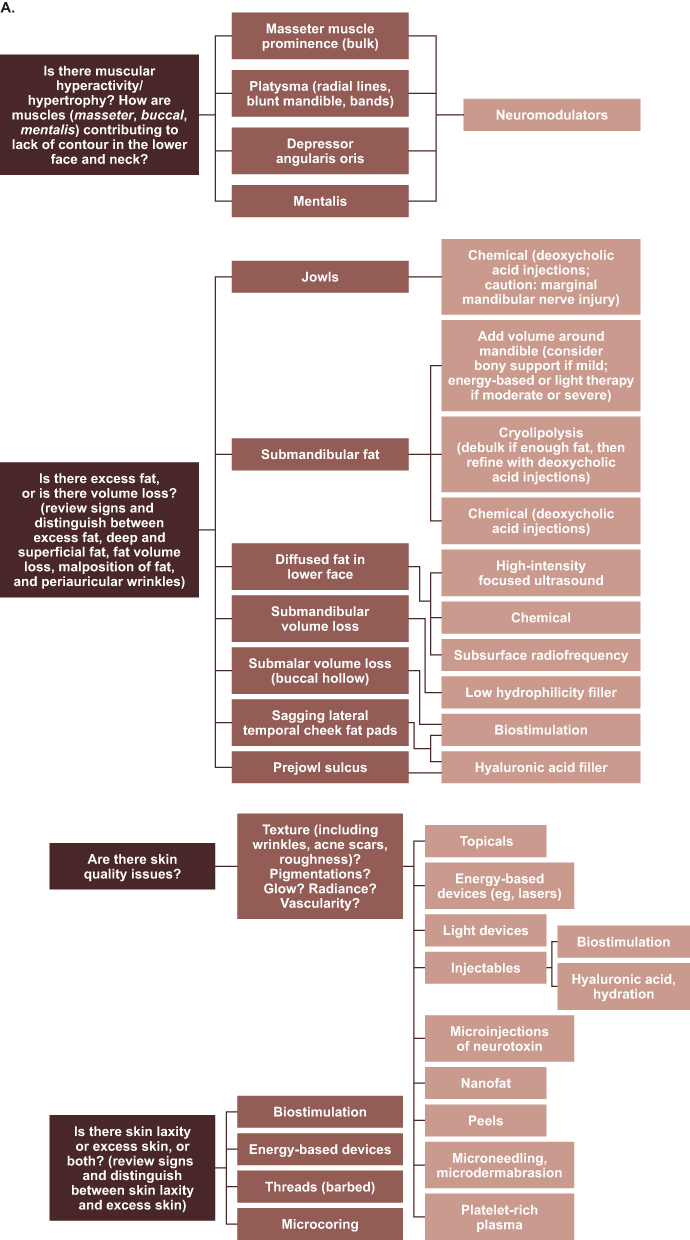

Figure 7A outlines and describes the other considerations of importance in assessing the patient with aesthetic concerns in the lower face and neck, providing a decision tree algorithm for the treatment of each concern. The photos in Figure 7B show a representative example of a patient with some of the concerns described, eg, muscular hypertrophy, skin laxity, chin retrusion, and excess fat.
The treatments that may be applied to the face and neck, and the potential outcomes of treatment, are exemplified by the patient case presented in Figure 8. An example video showing neuromodulator treatment of the lower face and neck appears in Supplementary Video 1.
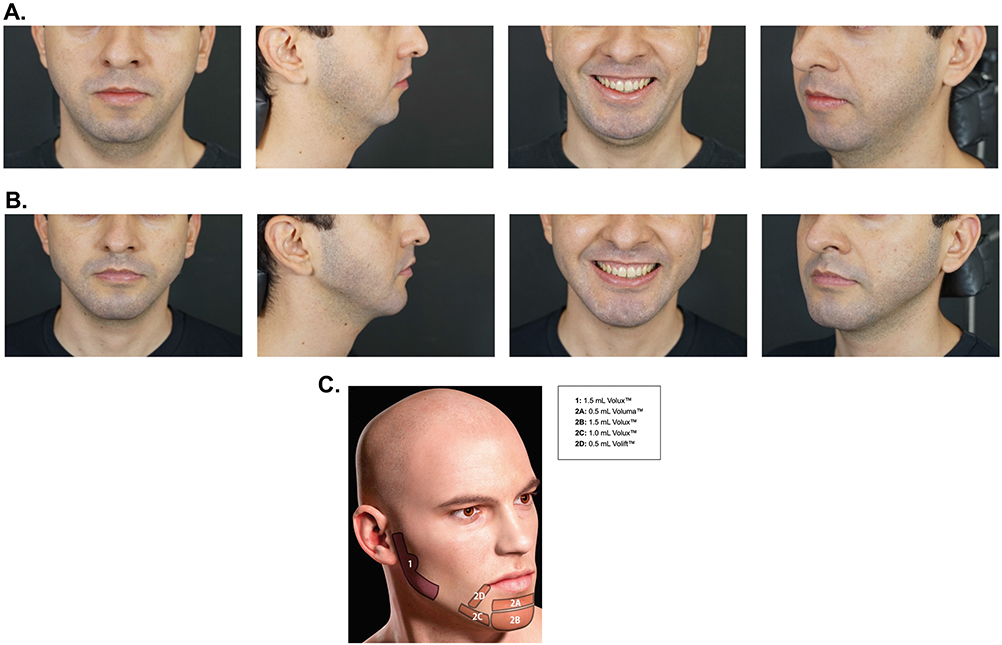 |
Figure 8 Case example of Caucasian male patient 32 years of age treated for aesthetic concerns in the lower face and neck (A) before treatment and (B) 60 days after filler treatment to address structural bone deficiency. The patient received hyaluronic acid injections (Juvederm® Volux™, Voluma™, and Volift™; Allergan Aesthetics, an AbbVie Company, Irvine, CA) in the lower face according to the schematic shown in (C). Photos courtesy of D. Coimbra, MD. |
Discussion
Correcting deficits or flaws in the appearance of the lower face and neck is becoming a high priority among those who seek surgical and nonsurgical aesthetic procedures.9–13 Especially with the heightened influence in recent years of social media upon individuals’ desire to seek aesthetic procedures to enhance their appearance,44 there is increasing awareness of and interest in lower face and neck aesthetic concerns and treatments. Treatment of the lower face and neck is important to maintaining facial balance/harmony and anatomical proportions.13 However, these areas of the face, particularly as they may be addressed by nonsurgical options, are relatively underexplored in the literature.2,14,30
Several clinical studies have demonstrated that a whole-face assessment and treatment approach, which includes consideration of the lower face, results in optimal outcomes, a more balanced facial appearance, and improved patient satisfaction.3,14,17 To address the most significant aesthetic concerns of the lower face and neck, as detailed in Figure 1, clinicians need a strategic evaluation and treatment roadmap for noninvasive/nonsurgical treatment options, with a flexible sequencing of treatments that accounts for patient factors that arise in real-world practice. In this paper, we have aimed to provide such guidance for the practitioner, offering detailed decision trees, with a goal of achieving satisfying and harmonious facial aesthetic results. These are the first expert recommendations on evaluation and treatment approaches for patients presenting with aesthetic concerns of the lower face and neck.
The questions and considerations presented are based on expert best practices, but clinicians should bear in mind that these questions and considerations are not always approached in a linear fashion, and individual patient factors, such as treatment expectations, preferences, budget, gender, age, other conditions, ethnic/cultural preferences, and skin type, may greatly influence the approach. Treatment goals are often different for young versus older patients; preventative strategies for signs of aging may be important for younger patients, whereas changing/repositioning facial attributes and addressing skin laxity may be priorities for older patients. Evidence suggests that older women prioritize the treatment of the lower face with respect to oral commissures and marionette lines, whereas younger women prioritize treatment of the upper face first, then oral commissures.12
Several factors underscore the need for expert guidance when considering the appearance of the lower face and neck. For example, treatment options, particularly injectables, for the lower face and neck are continuing to expand,14 and clinicians need to have an organized approach in evaluating this complex area through education and guidance on best practices. Treatment of the neck, as previously described, can be challenging; it is not always clear which modality should be used. Further, in the authors’ estimation, nonsurgical interventions to address this area are still limited and evolving.
Conclusions
Aesthetic treatment of the lower face and neck is an area of increasing interest, but there is limited published guidance on the topic. The assessment and treatment strategies discussed herein provide valuable information that may serve as a reference, guideline, and decision tree for the broad range of aesthetic clinicians who treat the lower face and neck. Future expert guidance may explore how patient factors impact safety profiles and treatment outcomes.
Abbreviations
BoNTA, botulinum toxin type A; HA, hyaluronic acid; SMAS superficial musculoaponeurotic system; US, United States.
Ethics Statement
The patients in this manuscript have given written informed consent to publication of their case details, including images. Ethical approval was not required as this was a non-interventional study.
Acknowledgments
In addition to the authors, the following advisors also participated in the advisory board and contributed their insights: Charles Boyd, MD, MBA, FACS (Boyd Cosmetic Surgical Institute, Birmingham, MI, USA), Sabrina Fabi, MD (FabskinMD Medical Corporation, San Diego, CA, USA), Lisa Grunebaum, MD (Lisa Danielle Grunebaum, MD, LLC, Miami Beach, FL, USA), Christophe Leys, MD (BVBA Dokter Christophe Leys Dermatologie, Sint-Truiden, Belgium), Rory McGoldrick, MD (Rory Boyd McGoldrick, Dubai, United Arab Emirates), Amir Moradi, MD, MBA (Moradi MD Face Beautiful Inc., Vista, CA, USA), Alexander Rivkin, MD (Westside Aesthetics, Los Angeles, CA, USA), and Reha Yavuzer, MD (Cahit Reha Yavuzer, Istanbul, Turkey). The authors thank Regina Kelly, MA of Peloton Advantage, LLC, an OPEN Health company, for medical writing and editorial support, which was funded by Allergan Aesthetics, an AbbVie Company.
The advisory board on lower face and neck aesthetic treatment that led to this independent publication was organized and funded by Allergan Aesthetics, an AbbVie Company. Editorial support for this article was provided by Regina Kelly, MA of Peloton Advantage, LLC, an OPEN Health company, and was funded by Allergan, an AbbVie Company.
Employees of Allergan Aesthetics, an AbbVie Company, participated in the organization and moderation of the advisory board as well as conducted a courtesy-only review of the manuscript, and supported the decision of the authors to submit for publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Vince Bertucci: advisory board member, paid consultant, clinical trial investigator, and/or speaker for Allergan Aesthetics, an AbbVie Company, Cutera, Evolus, Merz, Galderma, Prollenium, Revance, and Teoxane.
Annie Chiu: advisory board member, paid consultant, speaker, and clinical trial investigator for Allergan Aesthetics, an AbbVie Company, Galderma, Revance, Merz, Cynosure, BTL Aesthetics, and Solta Medical.
Daniel Dal’Asta Coimbra: advisory board member and speaker for Allergan Aesthetics, an AbbVie Company, and Galderma.
Dan Li: advisory board member for Allergan Aesthetics, an AbbVie Company.
The opinions expressed in this article are those of the authors. The authors received an honorarium for their participation in the advisory board but received no honorarium or other form of financial support related to the development of this article.
References
1. Levesque AY, de la Torre JI. Midface anatomy, aging, and aesthetic analysis. Facial Plast Surg Clin North Am. 2015;23(2):129–136.
2. Wang W, Xie Y, Huang RL, et al. Facial contouring by targeted restoration of facial fat compartment volume: the midface. Plast Reconstr Surg. 2017;139(3):563–572.
3. Narurkar VA, Cohen JL, Dayan S, et al. A comprehensive approach to multimodal facial aesthetic treatment: injection techniques and treatment characteristics from the HARMONY study. Dermatol Surg. 2016;42(suppl 2):S177–S191.
4. Callan P, Goodman GJ, Carlisle I, et al. Efficacy and safety of a hyaluronic acid filler in subjects treated for correction of midface volume deficiency: a 24 month study. Clin Cosmet Investig Dermatol. 2013;6:81–89.
5. Dong J, Gantz M, Goldenberg G. Efficacy and safety of new dermal fillers. Cutis. 2016;98(5):309–313.
6. Taub AF. Cheek augmentation improves feelings of facial attractiveness. J Drugs Dermatol. 2012;11(9):1077–1080.
7. Ogilvie P, Fink B, Leys C, et al. Improvement of radial cheek lines with hyaluronic acid-based dermal filler VYC-17.5L: results of the BEAM study. Dermatol Surg. 2020;46(3):376–385.
8. Ogilvie P, Safa M, Chantrey J, et al. Improvements in satisfaction with skin after treatment of facial fine lines with VYC-12 injectable gel: patient-reported outcomes from a prospective study. J Cosmet Dermatol. 2020;19(5):1065–1070.
9. American Society of Plastic Surgeons. 2020 national plastic surgery statistics; 2020. Available from: https://www.plasticsurgery.org/documents/News/Statistics/2020/plastic-surgery-statistics-report-2020.pdf.
10. International Society of Aesthetic Plastic Surgery. ISAPS international survey on aesthetic/cosmetic procedures performed in 2019; 2020. Available from: https://www.isaps.org/wp-content/uploads/2020/12/Global-Survey-2019.pdf.
11. American Society of Plastic Surgeons. 2019 plastic surgery statistics report; 2020. Available from: https://www.plasticsurgery.org/documents/News/Statistics/2019/plastic-surgery-statistics-full-report-2019.pdf.
12. Narurkar V, Shamban A, Sissins P, Stonehouse A, Gallagher C. Facial treatment preferences in aesthetically aware women. Dermatol Surg. 2015;41(suppl 1):S153–S160.
13. Kaminer MS, Cohen JL, Shamban A, et al. Maximizing panfacial aesthetic outcomes: findings and recommendations from the HARMONY study. Dermatol Surg. 2020;46(6):810–817.
14. Lipko-Godlewska S, Bolanča Ž, Kalinová L, et al. Whole-face approach with hyaluronic acid fillers. Clin Cosmet Investig Dermatol. 2021;14(169):653.
15. Patel S, Kridel R. Current trends in management of submental liposis: a pooled analysis and survey. JAMA Facial Plast Surg. 2018;20(3):202–206.
16. Montes JR, Santos E, Chillar A. Jowl reduction with deoxycholic acid. Dermatol Surg. 2020;46(1):78–85.
17. Rzany B, Cartier H, Kestemont P, et al. Full-face rejuvenation using a range of hyaluronic acid fillers: efficacy, safety, and patient satisfaction over 6 months. Dermatol Surg. 2012;38(7 Pt 2):1153–1161.
18. Allergan. Juvéderm Voluma XC [Directions for Use]. Irvine, CA: Allergan; 2020.
19. Allergan. Juvéderm Volux XC [Directions for Use]. Gordon, Australia: Allergan; 2019.
20. Allergan. Kybella [Package Insert]. Irvine, CA: Allergan USA, Inc.; 2020.
21. Moore AP, Wood GD. The medical management of masseteric hypertrophy with botulinum toxin type A. Br J Oral Maxillofac Surg. 1994;32(1):26–28.
22. Rijsdijk BA, van ER, Zonneveld FW, Steenks MH, Koole R. Botulinum toxin type A treatment of cosmetically disturbing masseteric hypertrophy. Ned Tijdschr Geneeskd. 1998;142(10):529–532.
23. von Lindern JJ, Niederhagen B, Appel T, Berge S, Reich RH. Type A botulinum toxin for the treatment of hypertrophy of the masseter and temporal muscles: an alternative treatment. Plast Reconstr Surg. 2001;107(2):327–332.
24. Ahn J, Horn C, Blitzer A. Botulinum toxin for masseter reduction in Asian patients. Arch Facial Plast Surg. 2004;6(3):188–191.
25. Andrade NN, Deshpande GS. Use of botulinum toxin (botox) in the management of masseter muscle hypertrophy: a simplified technique. Plast Reconstr Surg. 2011;128(1):24e–26e.
26. Xie Y, Zhou J, Li H, Cheng C, Herrler T, Li Q. Classification of masseter hypertrophy for tailored botulinum toxin type A treatment. Plast Reconstr Surg. 2014;134(2):209e–218e.
27. Chen DL, Cohen JL. Botulinum toxin-A chemical denervation for platysmal bands: maximal dosing considerations. J Drugs Dermatol. 2015;14(9):931.
28. Sugrue CM, Kelly JL, McInerney N. Botulinum toxin treatment for mild to moderate platysma bands: a systematic review of efficacy, safety, and injection technique. Aesthet Surg J. 2019;39(2):201–206.
29. de Almeida ART, Romiti A, Carruthers JDA. The facial platysma and its underappreciated role in lower face dynamics and contour. Dermatol Surg. 2017;43(8):1042–1049.
30. Sundaram H, Signorini M, Liew S, et al. Global Aesthetics Consensus Group: botulinum toxin type 1—evidence-based review, emerging concepts, and consensus recommendations for aesthetic use, including updates on complications. Plast Reconstr Surg. 2016;137(3):518e–529e.
31. Trinh LN, Gupta A. Hyaluronic acid fillers for midface augmentation: a systematic review. Facial Plast Surg. 2021;37(5):576–584.
32. Agarwal A, Dejoseph L, Silver W. Anatomy of the jawline, neck, and perioral area with clinical correlations. Facial Plast Surg. 2005;21(1):3–10.
33. Braz A, Humphrey S, Weinkle S, et al. Lower face: clinical anatomy and regional approaches with injectable fillers. Plast Reconstr Surg. 2015;136(5 suppl):235s–257s.
34. Weinkle SH, Werschler WP, Teller CF, et al. Impact of comprehensive, minimally invasive, multimodal aesthetic treatment on satisfaction with facial appearance: the HARMONY study. Aesthet Surg J. 2018;38(5):540–556.
35. Bertucci V, Rivers JK, Humphrey S, et al. Canada HARMONY study: comprehensive panfacial approach to aesthetic treatment, including submental fullness, results in improved patient-reported outcomes [poster].
36. Giordano CN, Matarasso SL, Ozog DM. Injectable and topical neurotoxins in dermatology: basic science, anatomy, and therapeutic agents. J Am Acad Dermatol. 2017;76(6):1013–1024.
37. Awaida CJ, Jabbour SF, Rayess YA, El Khoury JS, Kechichian EG, Nasr MW. Evaluation of the microbotox technique: an algorithmic approach for lower face and neck rejuvenation and a crossover clinical trial. Plast Reconstr Surg. 2018;142(3):640–649.
38. Goldie K, Peeters W, Alghoul M, et al. Global consensus guidelines for the injection of diluted and hyperdiluted calcium hydroxylapatite for skin tightening. Dermatol Surg. 2018;44(suppl 1):S32–S41.
39. Mulholland RS. Nonexcisional, minimally invasive rejuvenation of the neck. Clin Plast Surg. 2014;41(1):11–31.
40. Luthra A. Shaping lips with fillers. J Cutan Aesthet Surg. 2015;8(3):139–142.
41. Al-Hoqail RA, Abdel Meguid EM. The lip: a histologic and analytical approach of relevance to esthetic plastic surgery. J Craniofac Surg. 2009;20(3):726–732.
42. Kim H-J, Seo KK, Lee H-K, Kim J. Clinical Anatomy of the Face for Filler and Botulinum Toxin Injection. Singapore: Springer; 2015.
43. Fitzgerald R, Vleggaar D. Facial volume restoration of the aging face with poly-l-lactic acid. Dermatol Ther. 2011;24(1):2–27.
44. Sorice SC, Li AY, Gilstrap J, Canales FL, Furnas HJ. Social media and the plastic surgery patient. Plast Reconstr Surg. 2017;140(5):1047–1056.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.