Back to Journals » Patient Preference and Adherence » Volume 17
Assessing the Pharmacist’s Role in Counseling Asthmatic Adults Using the Correct Inhaler Technique and Its Effect on Asthma Control, Adherence, and Quality of Life
Authors AL-awaisheh RI ![]() , Alsayed AR
, Alsayed AR ![]() , Basheti IA
, Basheti IA ![]()
Received 29 October 2022
Accepted for publication 28 March 2023
Published 6 April 2023 Volume 2023:17 Pages 961—972
DOI https://doi.org/10.2147/PPA.S395258
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Rawa’a Ibrahim AL-awaisheh,1 Ahmad R Alsayed,1 Iman A Basheti1,2
1Department of Clinical Pharmacy and Therapeutics, Faculty of Pharmacy, Applied Science Private University, Amman, 11937, Jordan; 2School of Pharmacy, Faculty of Medicine and Health, University of Sydney, Sydney, Australia
Correspondence: Iman A Basheti, Department of Clinical Pharmacy and Therapeutics, Faculty of Pharmacy, Applied Science Private University, P. O. Box 166, Amman, 11931, Jordan, +962 797708060, Email [email protected]
Purpose: This study was designed to assess inhaler technique skills, asthma control level, adherence, and quality of life scores amongst asthmatic patients living in Amman, Jordan, investigating the role of pharmacist’s educational intervention.
Patients and Methods: This single-blinded randomized parallel-group active-controlled study was conducted at the Jordan University Hospital (JUH) clinic in 2019. Patients were assessed at baseline and follow-up (after three months) on their inhaler technique (based on validated published checklists), asthma control based on the asthma control test (ACT) questionnaire, adherence to treatment, and quality of life (QoL). Patients in the active group were counseled on correct inhaler technique and administration skills, orally and using inhaler adhesive labels delivered by the clinical pharmacist.
Results: Asthma patients (n = 157; active, n = 79, and control, n = 78) were recruited into the study and grouped based on the controller inhaler they were using (Turbohaler (TH) and Accuhaler (ACC). There was no statistically significant difference between both groups at baseline for inhaler technique, adherence, ACT, and QoL. At follow-up, 93.7% of the active group patients used their inhalers correctly, while only 16.7% of the control group used them correctly (P-value < 0.001). Also, the ACT mean score was significantly higher for the active group (21.21± 5.27) versus the control group (15.92± 7.31; P-value < 0.001). The QoL mean score was significantly improved for the active group compared with the control group (active = 63.85± 24.78, Control = 38.746± 3.23, P-value < 0.001). Improvement in adherence for the active group was noticed compared with the control group but did not reach a significant level (P-value=0.691).
Conclusion: Through a practical educational intervention, pharmacists were found to significantly improve patients’ asthma inhaler technique, ACT scores, and QoL scores for patients with asthma.
Keywords: inhaler techniques, ACT, adherence, QoL
Introduction
Asthma is a common and potentially serious chronic disease that burdens patients, their families, and the community.1,2 It causes respiratory symptoms, activity limitation, and flare-ups (exacerbations, mainly due to viruses and other factors) that sometimes require urgent health care and may be fatal.1,3 Asthma level of control is affected by adherence, environment, and mainly by incorrect inhaler technique administration; it leads to treatment failure or inadequate control.1,4,5
The correct inhaler technique administration skills are explained in the device’s product information and printed on the leaflet. Earlier studies reported high rates of inappropriate Turbuhaler (TH) administration techniques,6 where up to 54% of patients using TH did not complete all steps correctly.6 Using the Accuhaler (ACC, also called the Diskus) inhaler due to inadequate inhalation at the beginning of the inhalation process, improper dose loading of the device, and patient exhalation into the device at the end of the process were the main errors reported.7 While TH administration errors were initially due to slow or inadequate inhalation, loading the dose at a degree of more than 45 degrees, unloading or inadequately loading the dose, and exhalation into the inhaler.7
Many health-care providers do not provide counsel to patients on using their inhalers correctly, although that impacts their asthma control.8,9 The impact of the pharmacist’s role on asthma control levels was reported in a community pharmacy-based program which reported a significant improvement in asthma outcomes.10,11 Pharmacist counseling services using inhaler technique education and labels with the technique steps placed on patients’ controller inhalers showed improved asthma control outcomes, including inhaler technique and asthma control.11,12 Patients can benefit from the pharmacist considering the barriers to attending primary health-care facilities.13–15 The counseling between dispensing visits for asthmatic patients led to improved patients’ inhaler technique using the TH and ACC.12
Adherence is also vital for the excellent management of asthmatic patients using inhalers. Using controller medications according to therapeutic plans improves asthma control outcomes. There is a special relationship between adherence and treatment outcomes.16
A recent study in Jordan reported poor knowledge and readiness to deal with asthmatic children.17 This study was conducted to assess the ability of asthma adult patients living in Jordan to demonstrate the correct use of their inhaler controller devices and to assess their asthma control, adherence to their treatment, and QoL scores. The association between inhaler technique improvement following education and asthma control, adherence, and QoL was assessed.
Materials and Methods
Study Design and Subjects
This single-blinded randomized active-controlled study was carried out in 2019 at the University of Jordan Hospital (JUH) and approved by the JUH ethics committee (IRB No. 2019/192) and complied with the Declaration of Helsinki. Adult asthma patients attending the outpatient respiratory clinic were invited to participate in the study by the clinical pharmacist (a researcher with two years of experience) at the respiratory clinic.
Study inclusion criteria included patients between the ages of 18 and 75 with an asthma diagnosis confirmed by a respiratory consultant and intermittent or persistent asthma as defined by the Global Initiative for Asthma (GINA).2 The included participants also were on a controller inhaler with no change in medication or dose for the previous month. They were able to visit the involved clinic during the three-month study period. All eligible patients included in the study provided a signed consent form before study entry. Patients who did not speak or understand Arabic or could not commit to the study period were excluded.
Asthmatic patients were interviewed at the respiratory clinic by an experienced clinical pharmacist working with asthmatic patients. The patients were recruited and randomly allocated to either the interventional (active) group or the non-interventional (control) group. Active group patients were assessed on their inhaler technique. They then received counseling on correct inhaler technique administration skills orally and by using inhaler adhesive labels. In contrast, the control group patients were assessed on their inhaler technique but did not receive counseling on correct inhaler technique administration skills. The predetermined randomization number list was designed using a computer-generated randomization program (www.randomization.com).
The clinical pharmacist conducted a face-to-face interview at the baseline visit and follow-up, which was a visit three months later from the baseline conducted at the clinic. The clinical pharmacist explained the study to the patients using simple, short sentences and a clear voice. Figure 1 represents the study protocol explaining the study process and data collected at the baseline and follow-up, while Figure 2 represents the inhaler technique education protocol.
 |
Figure 1 The study protocol explains the process of the study and data collected at baseline and follow-up. |
 |
Figure 2 Inhaler technique education protocol. |
Outcome Measures
The Outcome Measured at the Baseline
At baseline, the patient’s asthma inhaler administration technique was assessed using placebo inhalers provided by AstraZeneca Pharmaceuticals and GlaxoSmithKline and validated inhaler technique checklists translated into Arabic.18 The inhaler technique checklist contained nine steps, with each correct step counting for one point; hence, each patient was awarded a score out of 9. A score of 9/9 was considered the Correct Technique for TH and ACC. For the TH, four steps were categorized as “essential” (little or no medication would reach the airway), and three steps were classified as essential for the ACC.18 A score of 4/4 for TH and 3/3 for ACC indicates Correct Essential Technique.
Asthma Level of Control
ACT questionnaires assessed asthma control. ACT is a validated self-administered questionnaire to determine the level of asthma control, composed of five questions.19 ACT is one of the numerical assessment tools, “scores from 20–25 are classified as well-controlled asthma; 16–19 as not well-controlled; and 5–15 as very poor controlled asthma”. The Arabic version of ACT was used and validated by Lababidi et al.19 A score of less than 20 in ACT refers to uncontrolled or poorly controlled asthma, and the asthma status should be reassessed.19
Asthma Medication Adherence
All the patients were assessed on their adherence to asthma medications at baseline and follow-up. Twenty asthma adherence validated questionnaire questions were answered with a 6-point scale.20
Quality of Life (QoL)
Asthma-related QoL of patients was evaluated using a validated questionnaire.21 The questionnaire consists of 23 questions exploring many aspects of asthmatic patients’ lives, such as patients’ satisfaction related to their treatment and their exercises.
Clinical Pharmacist Intervention
All patients in both groups underwent face-to-face interviews with a clinical pharmacist on their first visit to the clinic. The clinical pharmacist explained the study to patients using simple, short sentences and a clear voice. At the end of the interview, patients were praised for their cooperation and their contact details were provided for the follow-up visit arrangements.
The active group patients were educated on the correct inhaler technique for TH and ACC with verbal and written instructions (photo label) in the respiratory clinic of the hospital. Inhaler Technique counseling service based on previously published methods,18 going through each step on the checklist to describe and demonstrate correct use. This cycle of assessment and counselling was repeated up to three times, if necessary, until the patient had the correct technique on all steps (Figure 2). At the completion of counselling, the pharmacist used a highlighter pen to identify any incorrect steps from that day’s initial assessment on an “Inhaler Technique Label” which was pre-printed with the relevant checklist. The pharmacist attached the highlighted label to the patient’s controller medication inhaler (not the box), without covering any essential information. Pharmacists recorded the time taken for inhaler technique assessment/education.
At follow-up, active pharmacists repeated inhaler technique assessment/education, and a new label was placed on the patient’s replacement inhaler (or on the old one if still in use). If no steps were incorrect on the initial assessment at any visit, the label was attached to the patient’s inhaler without highlighting. The time required for patients’ counseling on the correct inhaler technique was assessed using a timer since the pharmacist started to demonstrate the proper inhaler technique using a placebo till the patient achieved a 9/9 score on their inhaler. All the required information was collected, and the patients answered the questionnaires (study tools).
The control group patients were assessed on their inhaler technique in the same way as the active group patients but did not receive educational counseling. For ethical purposes, after the study was ended, all control group patients received education on their inhaler technique, the same as that delivered to the active group patients.
Follow-Up Assessment
At follow-up (3 months post-baseline), all patients, both in the active and control groups, were re-assessed for the inhaler technique administration, ACT, adherence, and QoL method.
Patient satisfaction with the pharmaceutical counseling on inhaler technique services they received was assessed at the end of the study. Satisfaction was evaluated through four questions:
Sample Size
The primary outcome determined in this study was the level of asthma control measured by ACT. A sample of 79 and 78 adult asthma patients for each group (active and control) was required to detect a 10% difference in ACT scores between the active and control groups at 80% statistical power and a 5% significance level. The recruitment of patients was carried out over six months, from March 2019 to August 2019.
Statistical Analysis
Following data collection, patients’ responses were coded and entered into a customized database using the Statistical Package for the Social Sciences (SPSS), Version 24.0 (IBM Corp., Armonk, New York, USA). Continuous variables were presented as means and standard deviations, while qualitative variables were presented as frequencies and percentages. The Chi-Square test was used to compare the active and control groups for the categorical data using SPSS. McNemar’s test was used on paired nominal data at baseline and follow-up and was applied to 2×2 contingency tables with a dichotomous trait with matched pairs of subjects. A paired sample t-test was used to compare the continuous data, such as the mean within the group at the baseline and follow-up. In contrast, an independent sample t-test was used to compare the continuous data such as mean between both groups, either at the baseline or follow-up.
Results
Demographics of Study Participants
According to the study’s inclusion criteria, 157 asthmatic adult patients were recruited. The total sample was randomized into two groups: active (n = 79) and control (n = 78). At follow-up, 151 patients were returned for the follow-up study and were re-interviewed at the respiratory clinic of JUH (Figure 3). Three patients from the active group could not come back to the follow-up visit and were too sick to return; two patients from the control group could not return for personal reasons. Three patients out of the total sample could not complete the questionnaires due to another clinic appointment or time pressure (Table 1).
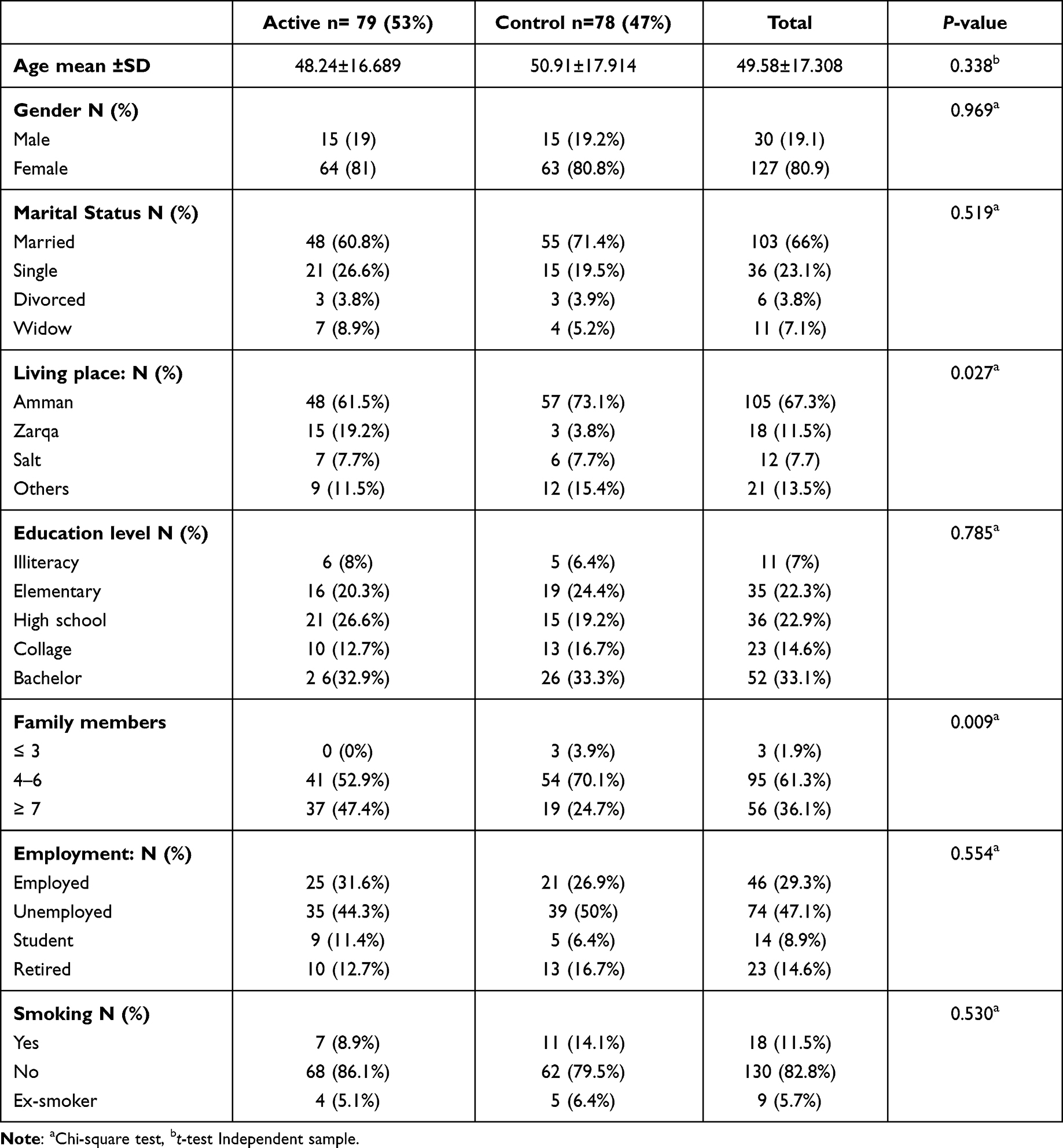 |
Table 1 Demographic Characteristics of the Study Sample (n = 157) for the Active (n = 79) and Control Groups (n = 78) |
 |
Figure 3 Study flow for the study sample (n = 157). |
Measured Outcomes
Asthma Inhaler Technique
For both active and control patients, 157 assessments of the inhaler technique were recorded. These results included the two inhalers, TH (n = 91) and ACC (n = 66) patients. No statistically significant difference in inhaler technique scores between the two active and control groups for TH (P = 0.91) and ACC (P = 0.093) scores were out of 9 for both inhalers.
At follow-up, a significant improvement in inhaler technique was noticed for the active group compared to the control group (P < 0.001 for both TH and ACC). The average time for counselling spent by the pharmacist on correct inhaler technique administration skills was about 1.82 minutes. The difference in correct inhaler technique score at baseline and follow-up for both groups was statistically significant (Active group = 1.33±1.49 and control group = 0.0139±0.313; P < 0.001; independent sample t-test; Table 2).
 |
Table 2 Inhaler Technique Scores and Asthma Control Test (ACT) Scores Comparing Patients in the Active (n = 79) and Control Groups (n = 78) at Baseline and Active (n = 76) and Control (n = 75) at the Follow-Up |
Figure 4 shows the effect of the pharmacist’s counselling for the active group on the correct inhaler administration technique on patients using ACC and TH. Inhaler technique scores were increased, and a statistically significant difference from baseline was found at the three-month follow-up (P < 0.001, Paired Sample t-test). Inhaler technique scores for patients in the control group are represented in Figure 5.
 |
Figure 4 Active group (n = 79) inhaler technique score at baseline before training, baseline after training, and at follow-up (n = 76). |
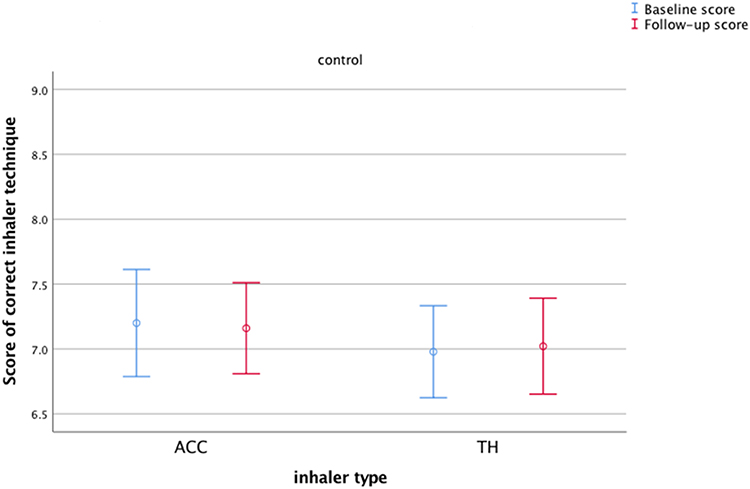 |
Figure 5 Inhaler technique scores for the control group (n = 78) at baseline before training, baseline after training, and at follow-up (n = 75). |
Asthma Level of Control
ACT mean score results for the study population (assessing patients’ symptoms over the past four weeks) were evaluated. There were no statistically significant differences between the mean scores of the active (15.39±6.136) and control groups (14.22±5.892) at baseline (p-value 0.223, independent sample t-test) (Table 2).
At follow-up, the mean scores of asthma control were significantly increased for the active group (21.21±5.27) compared to the control group (15.92±7.30, P-value <0.001).
Among the active group patients at baseline and follow-up, the mean score for the ACT was statistically significant (P-value <0.001, paired sample t-test). The control group also showed a significant improvement in the mean score (p-value 0.012, paired sample t-test), but not as much as the active group (Table 2).
The differences in ACT scores at the baseline and follow-up for both the active and control groups were statistically significant (active, 5.81±5.47 and control, 1.6±5.38; P < 0.001; independent sample t-test).
Patient Adherence Scores
Regarding asthma adherence scores, some active group patients (n = 13, 17.1%) and control group patients (n = 12, 15.4%) were not adherent and did not follow their treatment plan. However, no statistically significant difference (p-value = 0.322) between the groups at baseline was found. Patients reported reasons for non-adherence. For both groups, one of the main reasons that led patients to not follow their treatment plan in the active (n = 48, 60.8%) and control groups (n = 47, 60.3%) was patients’ inability to afford their treatment. Improvement in adherence for the active group was noticed at follow-up compared to the control group, but with no statistically significant difference between the two groups (p = 0.691) (Table 3).
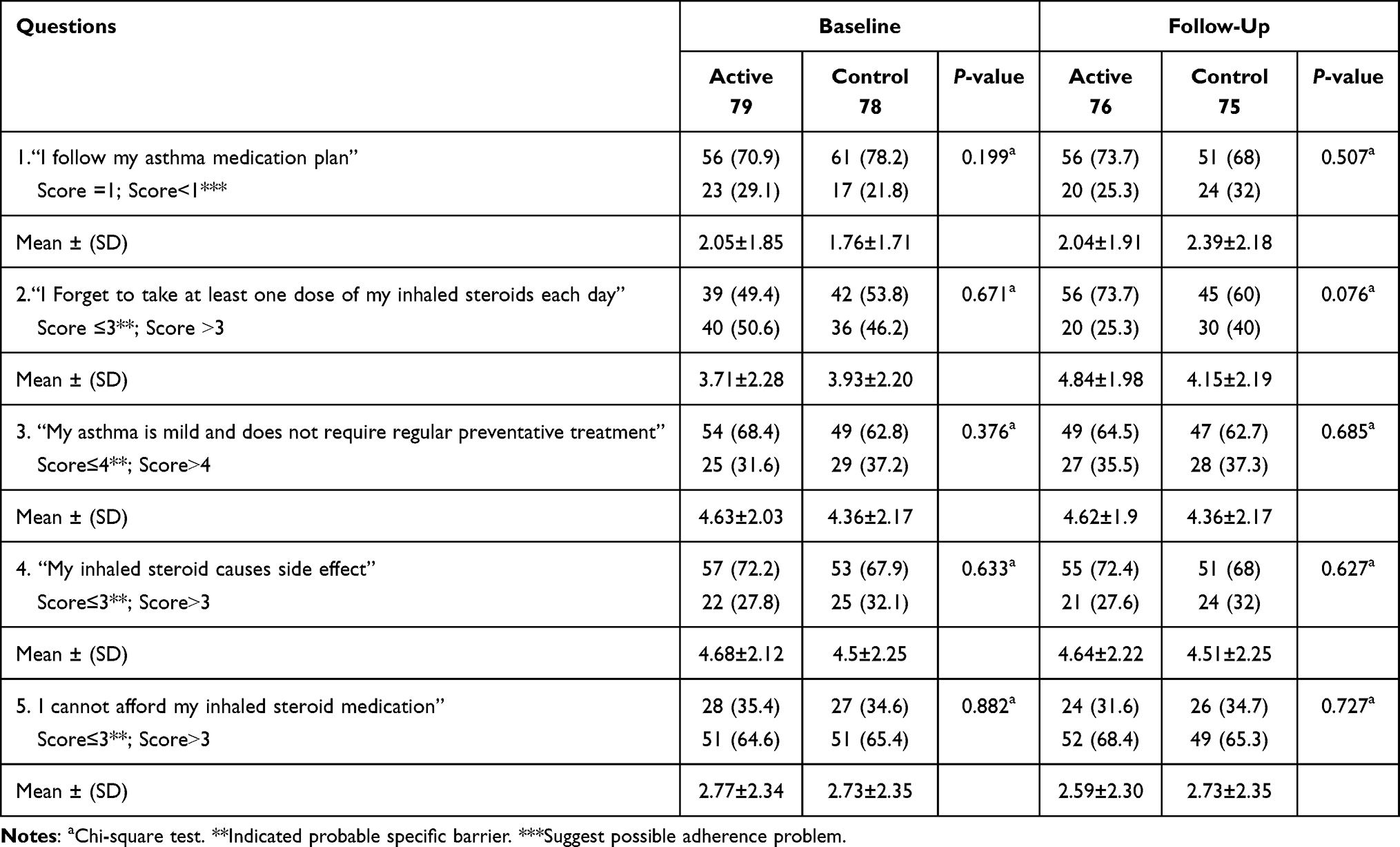 |
Table 3 Clinical Outputs for Adherence, Comparing Patients in the Active (n = 79) and Control Groups (n = 78) at Baseline, and Active (n = 76) and Control (n = 75) at the Follow-Up |
Asthma Related-Quality of Life (QoL)
A strong correlation between ACT scores and AQLQ value was found at baseline (Pearson R = 0.719) and follow-up (Pearson R = 0.820), respectively, with a significant statistical difference between baseline and follow-up (P < 0.001).
At follow-up, active group patients showed a significant improvement in patients’ QoL mean scores (p < 0.001, paired sample t-test). While in the control group, no significant difference in the QoL mean score was found (p = 0.229).
The difference in QoL score at baseline and follow-up for both active and control groups was statistically significant (active = 25.618±23.67 and control = 3.21±20.55; P < 0.001; independent sample t-test) (Table 4).
 |
Table 4 Clinical Outputs for AQLQ, Comparing Participants in the Active Group at the Baseline (n = 79) and Follow-Up (n = 76) at Baseline, and Control Group at the Baseline (n = 78) and at the Follow-Up (n = 75) |
Patients’ Satisfaction with the Service Received
Almost all patients who participated in the active group showed great satisfaction with the role of the clinical pharmacist in what was delivered to them during the inhaler technique education service. Patients’ choice of satisfaction ranged from 1 to 10, and most of the patients chose 10 for any one of the questions, showing great satisfaction with the provided pharmaceutical care service (98.4% of patients reported absolute (score of 10) satisfaction).
Discussion
Worldwide, the correct administration technique is a challenging topic concerning asthma patients.22 Many patients with uncontrolled asthma are referred to hospital clinics in Jordan for urgent treatment and follow-up management. Considering these important facts, this randomized controlled study is the first to target asthma patients attending asthma clinics in hospitals in Amman, Jordan. The study aimed to determine the effect of correcting patients’ inhaler technique on ACT, adherence, and QoL. The results of this study are auspicious as they show that a simple intervention delivered by a clinical pharmacist that did not exceed two minutes led to significant improvements in clinical and humanistic outcomes three months following the intervention. The importance of this study is further highlighted as it sheds light on the roles of pharmacists and their ability to deliver a feasible and effective counseling service to their asthma patients. Also, it added value to the few studies performed in Jordan regarding the novel counseling method on correct inhaler administration technique using an asthma label reminder for the steps of proper inhaler administration technique attached to the patient’s inhaler device.
Results of this study showed that at baseline, outcomes of asthma control for patients indicated very poorly controlled asthma (ACT score ≤15; 56.7%) or not well-controlled asthma (15.3%). A similar study conducted in Jordan in 2016, using the ACT score to assess asthma control, also showed that 71% of patients were classified as having very poorly controlled asthma.23 In this study, 75.8% of patients using the ACC and 81.1% using the TH showed incorrect inhaler administration techniques. No patients were found to be using the Pressurized metered dose inhaler (pMDI) as a controller treatment. As for inhaler technique demonstration skills, similar to what has been reported before, among 31 surveys distributed between two community pharmacies for asthma patients using DPI, only 9.6% reported using their inhaler correctly.24 Additionally, a study performed in France in 2008 at a respiratory clinic assessing the inhaler technique used in patients using DPI showed that around half had at least one administration technique error.25 Differences in inhaler types and use were reported to have different predicted outcomes in practice.26 Although it was found that a different percent of the patients using the ACC reported very poorly controlled asthma compared to TH users, no statistically significant difference was found concerning ACT mean score results comparing both devices. A previous study also showed no significant differences in ACT results comparing the ACC and TH devices.23
In this study, pharmacist counseling was provided in the outpatient hospital clinic, and all the study recruited patients approved for receiving counseling regarding the correct inhaler administration technique. At follow-up, most active group patients showed correct inhaler administration technique, contrary to control group patients. This result demonstrated the significant importance of the pharmacist’s role in counseling the patients on their inhalers correct technique administration. The ACT mean score also improved significantly for patients in the active group. A previous study by Momani et al assessed the impact of inhaler technique counseling among Jordanian asthmatic adolescents. It showed a significant improvement among interventional group patients on asthma control, as the median score of ACT increased.27
Asthma label reminder intervention on the steps of correct inhaler administration technique attached to the patient’s inhaler device was successful among asthmatic patients as three-quarters had correct inhaler administration technique post three months. This was prevalent and noticed among illiterate and elderly patients living without caregivers. Another study performed in 2007 on asthmatic patients in a Sydney hospital to evaluate the effect of pharmacist counseling on correct inhaler administration using the asthma label found similar results to our study. This indicates the effect of pharmacist’s counseling, as 67% of the patients showed correct inhaler technique at follow-up post three months.28 Recent researchers found the effect of the level of asthma control (poorly controlled and not well-controlled asthma) and its related symptoms on the QoL low score.29 Results of this study showed that patients with low ACT scores also had low QoL scores. According to the study findings, improvements in the active group’s inhaler technique were reflected in the observed improvement in ACT scores, consistent with the patient-centered outcomes of asthma-related QoL.
Similar findings were reported in a study performed to assess ACT correlation with asthma QoL score in outpatient clinics on the four domains: symptoms, activity, emotional, and environmental.29 The patients’ ACT score was significantly correlated with QoL’s emotional, activity, symptom, and environmental domains.29 Total QoL score was also significantly affected by ACT scores; patients with low ACT scores at baseline had low QoL scores, while at the second and third visits, the patients’ ACT scores improved.29 Similarly, in this study, the improvement in inhaler technique administration for the active group was reflected in the QoL scores. At baseline, the mean QoL score for the active group was increased at follow-up, with a statistically significant difference. However, patients in the control group’s QoL mean score did not improve at follow-up.
As for treatment adherence, the SmartTrack electronic inhaler reminder was used previously in asthmatic patients to evaluate their inhaler adherence. Results showed that asthma control tests were significantly improved for all patients enrolled in the study.30 In this study, similar results were found to improve patient adherence for the active group at the follow-up compared with the control group, but they did not reach the significance level (p-value=0.691). A more extended assessment period could reveal significant changes between the groups due to the inhaler technique education service delivered in this study. Furthermore, future studies with novel methods31 are recommended to highlight the most critical medical problems practiced and find the appropriate plan to solve them.
Regarding the limitations, the study sample was recruited from one hospital clinic in the capital of Jordan, Amman, which could affect the generalizability of the results to patients living in other areas of the country. Adding on, the study sample was recruited during the winter and spring seasons, which are commonly known for asthma symptoms’ flare-ups. Moreover, at follow-up, patients were interviewed in the summer, which could have affected the differences seen in the ACT scores, explaining the possibility behind the significant improvement in patients’ ACT scores at follow-up for both active and control patients. Nevertheless, the significant difference between patients in the active group and patients in the control group was still apparent, highlighting the effect of the interventional service delivered to the patients.
Conclusion
This randomized controlled study aimed to determine the effect of correcting patients’ inhaler technique on ACT, adherence, and QoL. This result demonstrated the significant importance of the pharmacist’s role in counseling the patients on their inhalers correct technique administration.
The results of this study have demonstrated that a simple intervention delivered by a pharmacist at the respiratory clinics to asthma patients, focusing on the fundamental concept of correct inhaler administration technique, was feasible for incorporation into routine practice. The intervention led to considerable improvements in inhaler technique, asthma control, and asthma-related QoL compared to patients who did not receive the service.
Future studies need to include more clinics in Jordan, distributed in different geographical areas around the country, with more extended assessment periods incorporated into the study’s methodology.
Acknowledgments
The authors would like to thank the participants and JUH members.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work”.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Reddel HK, Bacharier LB, Bateman ED, et al. Global initiative for asthma strategy 2021: executive summary and rationale for key changes. Eur Respir J. 2022;59(1):2102730. doi:10.1183/13993003.02730-2021
2. GINA. Global initiative for asthma (GINA): strategy for asthma management and prevention; 2022.
3. Al-Dulaimi A, Alsayed AR, Maqbali MA, Zihlif M. Investigating the human rhinovirus co-infection in patients with asthma exacerbations and COVID-19. Pharm Pract. 2022;20(2):2665. doi:10.18549/PharmPract.2022.2.2665
4. Price D, Bosnic-Anticevich S, Briggs A, et al. Inhaler competence in asthma: common errors, barriers to use and recommended solutions. Respir Med. 2013;107(1):37–46. doi:10.1016/j.rmed.2012.09.017
5. Volerman A, Toups MM, Hull A, Press VG. A feasibility study of a patient-centered educational strategy for rampant inhaler misuse among minority children with asthma. J Allergy Clin Immunol Pract. 2019;7(6):2028–2030. doi:10.1016/j.jaip.2019.01.044
6. Kamps AW, van Ewijk B, Roorda RJ, Brand PL. Poor inhalation technique, even after inhalation instructions, in children with asthma. Pediatr Pulmonol. 2000;29(1):39–42. doi:10.1002/(SICI)1099-0496(200001)29:1<39::AID-PPUL7>3.0.CO;2-G
7. Crompton G, Dewar M, Allbutt H, Innes J. Inhaler preference and technique in inhaler naïve subjects; a comparison of HFA and conventional devices. Thorax. 2000;55:97–101. doi:10.1136/thorax.55.2.97
8. Fink JB, Rubin BK. Problems with inhaler use: a call for improved clinician and patient education. Respir Care. 2005;50(10):1360–1375.
9. Amin S, Soliman M, McIvor A, Cave A, Cabrera C. Understanding patient perspectives on medication adherence in asthma: a targeted review of qualitative studies. Patient Prefer Adherence. 2020;Volume 14:541–551. doi:10.2147/PPA.S234651
10. Mehuys E, Van Bortel L, De Bolle L, et al. Effectiveness of pharmacist intervention for asthma control improvement. Eur Respir J. 2008;31(4):790–799. doi:10.1183/09031936.00112007
11. Basheti IA, Salhi YB, Basheti MM, Hamadi SA, Al-Qerem W. Role of the pharmacist in improving inhaler technique and asthma management in rural areas in Jordan. Clin Pharmacol. 2019;11:103–116. doi:10.2147/cpaa.S213271
12. Basheti IA, Armour CL, Bosnic-Anticevich SZ, Reddel HK. Evaluation of a novel educational strategy, including inhaler-based reminder labels, to improve asthma inhaler technique. Patient Educ Couns. 2008;72(1):26–33. doi:10.1016/j.pec.2008.01.014
13. Qunaibi E, Basheti IA, Hamadi SA, Bulatova NR, Shanah A, Abu-Gharbieh E. Effect of divergence in patients’ socioeconomic background on their perspective of the role of the community pharmacist in Amman, Jordan. Trop J Pharm Res. 2013;12(2):247–253.
14. Khader H, Alsayed A, Hasoun LZ, et al. Pharmaceutical care and telemedicine during COVID-19: a cross-sectional study based on pharmacy students, pharmacists, and physicians in Jordan. Pharmacia. 2022;69(3):891–901. doi:10.3897/pharmacia.69.e90748
15. Alsayed AR, Halloush S, Hasoun L, et al. Perspectives of the community in the developing countries toward telemedicine and pharmaceutical care during the COVID-19 pandemic. Pharm Pract. 2022;20(1):2618. doi:10.18549/PharmPract.2022.1.2618
16. van Boven JF, Ryan D, Eakin MN, et al. Enhancing respiratory medication adherence: the role of health care professionals and cost-effectiveness considerations. J Allergy Clin Immunol Pract. 2016;4(5):835–846. doi:10.1016/j.jaip.2016.03.007
17. Nour A, Alsayed AR, Basheti I. Prevalence of asthma amongst schoolchildren in Jordan and staff readiness to help. Healthcare. 2023;11(2):183. doi:10.3390/healthcare11020183
18. Basheti IA, Bosnic-Anticevich SZ, Armour CL, Reddel HK. Checklists for powder inhaler technique: a review and recommendations. Respir Care. 2014;59(7):1140–1154. doi:10.4187/respcare.02342
19. Lababidi H, Hijaoui A, Zarzour M. Validation of the Arabic version of the asthma control test. Ann Thorac Med. 2008;3(2):44. doi:10.4103/1817-1737.39635
20. Schatz M, Zeiger RS, Yang S-J, et al. Development and preliminary validation of the adult asthma adherence questionnaireTM. J Allergy Clin Immunol. 2013;1(3):280–288. doi:10.1016/j.jaip.2013.03.001
21. Juniper E, O’byrne P, Guyatt G, Ferrie P, King D. Development and validation of a questionnaire to measure asthma control. Eur Respir J. 1999;14(4):902–907. doi:10.1034/j.1399-3003.1999.14d29.x
22. Hamdan A-J, Ahmed A, Abdullah A-H, et al. Improper inhaler technique is associated with poor asthma control and frequent emergency department visits. Allergy Asthma Clin Immunol. 2013;9(1):8. doi:10.1186/1710-1492-9-8
23. Basheti I, Obeidat N, Ammari W, Reddel H. Associations between inhaler technique and asthma control among asthma patients using pressurised MDIs and DPIs. Int J Tuberc Lung Dis. 2016;20(5):689–695. doi:10.5588/ijtld.15.0557
24. Farabaugh N, McMillan A, Garofoli G. Assessment of asthma inhaler technique in two community pharmacies; 2014.
25. Giraud V, Allaert F-A, Roche N. Inhaler technique and asthma: feasability and acceptability of training by pharmacists. Respir Med. 2011;105(12):1815–1822. doi:10.1016/j.rmed.2011.07.004
26. Lavorini F, Magnan A, Dubus JC, et al. Effect of incorrect use of dry powder inhalers on management of patients with asthma and COPD. Respir Med. 2008;102(4):593–604. doi:10.1016/j.rmed.2007.11.003
27. Almomani BA, Mayyas RK, Ekteish FA, Ayoub AM, Ababneh MA, Alzoubi SA. The effectiveness of clinical pharmacist’s intervention in improving asthma care in children and adolescents: randomized controlled study in Jordan. Patient Educ Couns. 2017;100(4):728–735. doi:10.1016/j.pec.2016.11.002
28. Basheti IA, Obeidat NM, Reddel HK. Effect of novel inhaler technique reminder labels on the retention of inhaler technique skills in asthma: a single-blind randomized controlled trial. NPJ Prim Care Respir Med. 2017;27(1):1–7. doi:10.1038/s41533-017-0011-4
29. Kwon H-S, Lee S-H, Yang M-S, et al. Correlation between the Korean version of asthma control test and health-related quality of life in adult asthmatics. J Korean Med Sci. 2008;23(4):621–627.
30. Scott KM, Von Korff M, Ormel J, et al. Mental disorders among adults with asthma: results from the world mental health survey. Gen Hosp Psychiatry. 2007;29(2):123–133. doi:10.1016/j.genhosppsych.2006.12.006
31. Alsayed AR, Al-Dulaimi A, Alnatour D, Awajan D, Alshammari B. Validation of an assessment, medical problem-oriented plan, and care plan tools for demonstrating the clinical pharmacist’s activities. Saudi Pharm J. 2022;30(10):1464–1472. doi:10.1016/j.jsps.2022.07.007
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.