Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 8
Assessing the obese diabetic patient for bariatric surgery: which candidate do I choose?
Authors Raffaelli M, Sessa L, Mingrone G, Bellantone R
Received 15 August 2014
Accepted for publication 23 March 2015
Published 8 June 2015 Volume 2015:8 Pages 255—262
DOI https://doi.org/10.2147/DMSO.S50659
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ming-Hui Zou
Marco Raffaelli,1 Luca Sessa,1 Geltrude Mingrone,2 Rocco Bellantone1
1Division of Endocrine and Metabolic Surgery, 2Division of Obesity Diseases, Università Cattolica del Sacro Cuore, Rome, Italy
Abstract: The worldwide prevalence of type 2 diabetes is rising in association with an increasing frequency of overweight and obesity. Bariatric-metabolic procedures are considered as additional therapeutic options, allowing improved diabetes control in most patients. Multiple factors play in concert to achieve the improvements in diabetic remission observed after bariatric-metabolic surgery. Several studies have demonstrated that bariatric-metabolic surgery is an effective treatment for type 2 diabetes when compared with conventional nonsurgical medical treatment. Because the best results are achievable in patients with a relatively short history of diabetes and less advanced controlled disease, the surgical option could be considered early, especially in morbid obese subjects (BMI ≥35 kg/m2) after failure of medical treatment. Patients with extensive weight loss are more likely to achieve type 2 diabetes remission after bariatric surgery. At present, Roux-en-Y gastric bypass seems the surgical procedure of choice because it has fewer risks than biliopancreatic diversion, and it is associated with higher weight loss and metabolic improvements compared with adjustable gastric banding. Recent evidences regarding the effectiveness of sleeve gastrectomy in diabetes remission have to be confirmed by controlled trials with longer follow-up.
Keywords: bariatric surgery, metabolic surgery, diabetes, morbid obesity
Introduction
Obesity is one of the greatest public health problems in industrialized countries. The World Health Organization estimates >400 million adults as obese. Currently, 67% of the US population is either overweight or obese, and in most European countries the prevalence ranges between 40% and 50%.1
Obesity is associated with an increased risk for type 2 diabetes, hypertension, dyslipidemia, cardiovascular diseases, obstructive sleep apnea, musculoskeletal disorders, some cancers, and mortality.1
The worldwide prevalence of type 2 diabetes is rising in association with an increasing frequency of overweight and obesity.2 It has been estimated that the risk of developing type 2 diabetes increases 93-fold in women and 42-fold in men who are severely obese compared to those with healthy weight.3,4 Globally, >312 million people suffer from type 2 diabetes;5 more than 60% of patients with type 2 diabetes are obese.6
Prevention and treatment of “diabesity”7 (the combination of obesity and type 2 diabetes) are important public health priorities.
Long-term antidiabetic diet compliance is poor even when supported by pharmacotherapy, and 50%–90% of diabetic patients remain unable to achieve adequate diabetes control.8–10
Bariatric-metabolic surgery defines procedures designed to produce substantial weight loss, and is associated with other health benefits including improvement or normalization of hyperglycemia, hyperlipidemia, blood pressure, obstructive sleep apnea, and improved quality of life.11–13
Because of its effects on glycemic control, the option of bariatric surgery needs to be considered in appropriately selected diabetic individuals.11 Since the estimation that the medical cost for a type 2 diabetes patient is two to four times greater than that for a patient without diabetes,14 some evidence exists regarding the cost effectiveness of bariatric-metabolic surgery in the treatment of type 2 diabetes mellitus.15,16
Despite these findings, surgery is still considered optional, and, as such, in countries with the highest bariatric surgery uptake, less than 2% of the eligible patients are treated annually.11
Some concerns still exist regarding the selection of diabetic candidates for bariatric-metabolic procedure, the etiology of diabetes remission following bariatric surgery, and the best bariatric-metabolic procedure for adequate diabetes control.5,17
This paper reviews bariatric-metabolic surgery for obese diabetic patients.
Indications for bariatric surgery
Obesity is usually classified by body mass index (BMI), calculated as the body weight in kilograms divided by the height in meters squared (kg/m2).
BMI is known to be of limited accuracy (it does not always reflect fat distribution or the proportion of body weight that consists of fat; furthermore, BMI was developed for European ethnicity and often underestimates health risks in other populations). Recent studies have proposed some alternative indicators of body fat, such as the body adiposity index, the waist/hip ratio, and the waist and hip circumferences.18 Nevertheless, at present, BMI is the internationally accepted standard used to allocate individuals to different size categories.11
Eligible criteria for bariatric-metabolic procedures, as defined by most guidelines,11,19–21 include morbid obesity (BMI ≥35 kg/m2 with significant obesity-related comorbidity – type 2 diabetes, hypertension, obstructive sleep apnea – or BMI ≥40 kg/m2) after failure of nonsurgical options for weight loss.
Absolute contraindications for bariatric surgery include current drug or alcohol abuse, uncontrolled psychiatric illness, and the lack of comprehension of the risks/benefits, expected outcomes, alternatives, and lifestyle changes required with bariatric surgery.22
Interest is increasing in the use of bariatric surgery in patients with a BMI <34.9 kg/m2 with poorly controlled diabetes or other associated comorbidities (such as hypertension and dyslipidemia) with encouraging metabolic outcomes, but further clinical trials are required to evaluate the long-term benefit.2,11,23
Bariatric-metabolic procedures
The most widely performed bariatric procedures are Roux-en-Y gastric bypass, adjustable gastric banding, biliopancreatic diversion (with or without duodenal switch), and sleeve gastrectomy.2
The laparoscopic approach is feasible for all these procedures.
In regards to sleeve gastrectomy, there are limited long-term outcome data.11
Roux-en-Y gastric bypass seems at present the surgical procedure of choice because it has fewer risks than biliopancreatic diversion and it is associated with higher weight loss and metabolic improvements compared to adjustable gastric banding.24 Nevertheless, all these procedures are widely performed in the world. Morbidity and mortality associated with conventional bariatric procedures are generally low in experienced hands.25,26 The 30-day mortality associated with bariatric surgery is estimated at 0.1%–0.3%.25,26
The choice of a particular bariatric surgical procedure depends on many factors including patient (risk factors associated with high perioperative morbidity and mortality, patients’ preference, compliance of the patients to the postoperative follow-up protocol) and surgical factors (expertise and experience in the bariatric surgical procedures, the simplicity and reversibility of the procedure).11
In recent years, novel extraluminal (ie, duodenal–jejunal bypass,27 ileal interposition28) and endoluminal procedures (ie, intra-gastric balloons, duodenal–jejunal bypass liner11,29), and novel bariatric metabolic devices (ie, electronic gastric or gastro-duodenal motility stimulator, vagal nerve blocking devices11) have been introduced, but their use remains experimental and their utility has still to be established.11,29
Mechanisms of action in diabetes remission
The control of diabetes is a direct consequence of the rearrangement in gastrointestinal anatomy and not only of the reduction in caloric intake and of the weight loss following bariatric-metabolic surgery. Bariatric surgery induces rapid improvement of hyperglycemia, reduction in hepatic insulin resistance, improvement in insulin secretion, and changes in food preferences.30,31 Different mechanisms of action have been investigated also based on surgical procedure. For example, in Roux-en-Y gastric bypass, there are thought to be at least three main mechanisms: speed of transit of food from the esophagus into the small bowel, gut hormone responses, and delayed mixing of bile in the distant small bowel.24
Some theories could help to explain the mechanism behind diabetes remission after bariatric surgery. “Hindgut” and “foregut” hypotheses are the most frequently discussed.32 The “hindgut hypothesis” suggests that faster arrival of digested foods to the end of the gastrointestinal tract improves the metabolism of carbohydrates through an increase in the secretion of the glucagon-like peptide 1 and peptide YY and other anorexigenic peptides.33 According to the “foregut hypothesis”, exclusion of the foregut from the passage of nutrients may suppress the production of postulated as-yet-unidentified factors, impairing insulin secretion and leading to other metabolic derangements.32
Nevertheless, increased bile acid reabsorption plays a role in the regulation of cellular function by modulating nuclear transcription, which increases cellular metabolism; this produces an increase in basal metabolic rate, which changes the energy homeostasis, resulting in weight loss.24 Again, bile acids also act on the Farnesoid X receptor, stimulating secretion of fibroblast growth factor-19 with subsequent inhibition of hepatic gluconeogenesis.34
Furthermore, in some surgical procedures the resection of a large part of the stomach, where ghrelin is produced, leads to the reduction of circulating ghrelin levels, thereby decreasing its obesitogenic and diabetogenic properties.32
Several studies have investigated the genetic characteristics associated with bariatric-metabolic procedures outcome, the systemic and anatomic changes that may influence the composition of the gut microbiota in patients who underwent bariatric surgery, the taste receptors of the gut, and the changes in circulating concentrations of many metabolites related to obesity and type 2 diabetes.34
Despite these findings, current evidence suggests that multiple factors play in concert to achieve the improvements in diabetic control observed after bariatric-metabolic procedures.34
The main mechanisms of action in diabetes remission after bariatric-metabolic surgery are reported in Table 1.
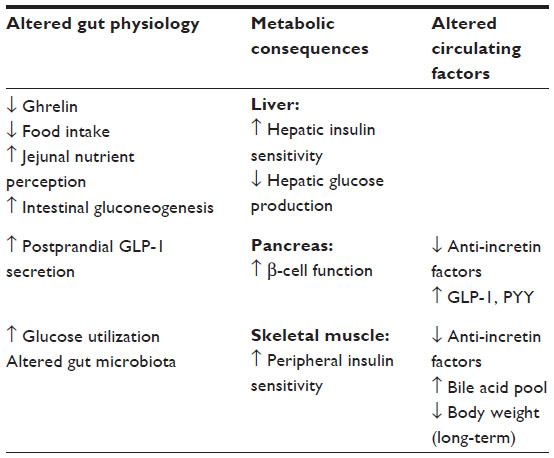 | Table 1 Main mechanisms of action in diabetes remission after bariatric-metabolic surgery |
Further investigations are needed to clearly identify the crucial factors implicated in diabetes remission after bariatric-metabolic procedures.11
Bariatric-metabolic surgery in obese diabetic patients
Type 2 diabetes is a systematic and progressive disease. The usual natural history is the progressive loss of insulin secretory capacity over time and the need for intensification of therapy.11 The subsequent end-organ damage is the major cause of morbidity and mortality.24 Arresting this progression is a formidable therapeutic challenge.
Bariatric-metabolic procedures are considered an additional therapeutic option allowing improved diabetes control in most patients.24
As suggested by the International Diabetes Federation (IDF),11 the achievable goal of bariatric surgery is not cure, but remission, of the diabetic state. After bariatric surgery, a BMI reduction of 5 corresponds to a type 2 diabetes reduction of 33%.35
According to IDF, a substantial improvement in metabolic state may be defined as the lowering of glycosylated hemoglobin (HbA1c) by <20%, LDL <2.3 mmol/L, and blood pressure <135/85 mmHg with reduced medication from the preoperative state.11
Several studies have shown encouraging results regarding the effectiveness of bariatric-metabolic surgery in diabetes remission5 and improvement in other cardiovascular risk factors.12,36
The reported results are limited by the heterogeneity of the populations included (ie, BMI ranging from <30 kg/m2 in some series), by the lack of randomized trials with long follow-up, and by the different criteria used to define remission.
Furthermore, the choice of the best bariatric-metabolic procedure for an effective treatment of type 2 diabetes in obese patients remains an open question.17
Comparison between bariatric surgery and conventional medical treatment for type 2 diabetes
Several studies have demonstrated bariatric-metabolic surgery as an effective treatment for type 2 diabetes when compared with conventional nonsurgical medical treatment.1,37–42
The main findings from the most important international studies are reported in Table 2.
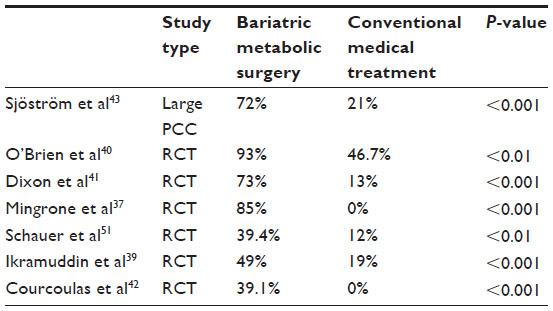 | Table 2 Comparison between bariatric surgery and conventional medical treatment for type 2 diabetes remission rate (%) |
A recent meta-analysis5 confirms these findings, showing an overall type 2 diabetes remission rate of 63.5% for the surgical group versus 15.6% for the conventional nonsurgically treated group (P<0.001) at a mean follow-up of 17.3 months. This meta-analysis was based on the results of 16 studies including 6,131 patients (five randomized controlled trials and eleven observational studies), which compared bariatric surgery with conventional therapy and included type 2 diabetes mellitus endpoints with ≥12-month follow-up.5 The short follow-up time limited these encouraging results, but long-term follow-up studies on this topic are very few.
The best data available are provided by a very long-term follow-up observational study of obese patients with type 2 diabetes: The Swedish Obese Subjects (a prospective matched cohort study).43 Sjöström et al, comparing bariatric surgery and nonsurgical treatment, confirmed that bariatric surgery was associated with more frequent diabetes remission and fewer diabetes-related complications (microvascular and macrovascular) than usual care. On the other hand, in the surgically treated patient group, the reported type 2 diabetes remission of 72% at the 2-year follow-up decreased by 38% and 30% at 10 years and 15 years (although the rates were significantly more favorable than those for the control nonsurgically treated group).43 Nevertheless, even the Swedish Obese Subjects study has certain limitations mainly due to the fact that the randomized design was not approved by the Ethics Review Boards because of high postoperative mortality rates following bariatric surgery in the 1980s and because the matching procedure created surgery and control groups that differed in some respects (age, BMI, blood pressure, and fasting serum insulin at baseline).43
Several studies have shown a more favorable diabetes remission in patients with short diabetes duration at baseline (<4–8 years) and less advanced controlled preoperative diabetes also evaluated by fasting C-peptide (influenced by insulin resistance and residual β-cell function).44–46
The Swedish Obese Subjects43 study confirmed this finding and extended the information by demonstrating that short diabetes duration at baseline is associated with higher remission rates at 10 and 15 years after surgery.43
Given these findings, preoperative metabolic data could be of primary importance to asses which patients may effectively benefit from bariatric-metabolic surgery in diabetes control.45
Patients with extensive weight loss were more likely to achieve type 2 diabetes remission after bariatric surgery. Percent excess weight loss (%EWL) represents an important factor related to the outcome of bariatric surgery and to diabetes remission.47 The risk of diabetes recurrence appeared to be inversely correlated with long-term excess weight loss and directly correlated with the duration of diabetes and severity of diabetes preoperatively.44,48
About one-third of the patients experienced diabetes recurrence within 5 years of initial remission.44
These results can raise some concerns about the use of bariatric-metabolic surgery in diabetic, nonmorbid obese patients2,23 but do not contraindicate bariatric-metabolic procedures in morbidly, obese diabetic patients at higher risk of failure (diabetes duration more than 10 years, preoperative uncontrolled disease) in relation to diabetes remission and recurrence.44 Some studies have demonstrated that a transient period of aggressive glycemic control can induce a beneficial “metabolic memory” effect and reduce incident microvascular events in diabetic patients.44 On the other hand, in these patients, bariatric-metabolic approach can improve other important cardiovascular risk factors.12,36
Given these findings, surgery should not be considered as “the last option” but as an appropriate treatment, especially when diabetes is not controlled or when other obesity-related comorbidities are poorly controlled.2
Comparison between bariatric surgical procedures for remission of type 2 diabetes
Depending on the bariatric-metabolic procedure used, the diabetes remission rate can range from 45% to 97% of patients.17 This observation has raised the question of the surgical procedure of choice for treating type 2 diabetes.
Randomized controlled trials are necessary to assess different bariatric-metabolic procedures for the treatment of type 2 diabetes, by comparing them with each other and with emerging nonsurgical treatments.2
Few high-quality studies have compared the safety and efficacy of the conventional surgical procedures regarding diabetes remission.
Weight loss induced by bariatric surgery is a major factor implicated in diabetes improvement,17 suggesting a “malabsorptive” or “mixed”, associated with higher weight loss, procedure of choice for achieving the best results in diabetes control.
Several studies have shown the superiority of Roux-en-Y gastric bypass over adjustable gastric banding in the treatment of type 2 diabetes.17,49,50
Procedures associated with greater excess weight loss lead to higher remission rates.37,50 A systematic review50 by Buchwald et al comparing adjustable gastric banding, Roux-en-Y gastric bypass, and biliopancreatic diversion reported a %EWL, at 2 years or more, of 49%, 63%, and 73% respectively, associated with diabetes remission in 58%, 71%, and 95% of the patients.
Similar findings were observed in recently published prospective randomized trials.37,38,51
The main findings from the most important international studies are reported in Table 3.
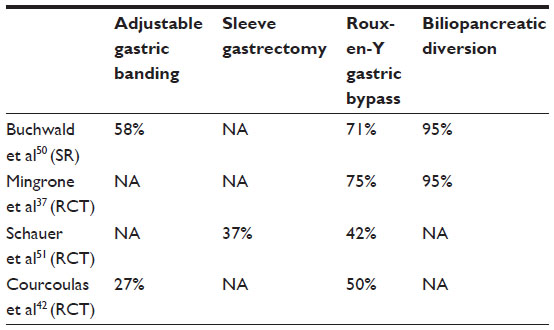 | Table 3 Comparison between bariatric surgical procedures for type 2 diabetes remission rate (%) |
Several studies have shown less weight loss with gastric bypass than with biliopancreatic diversion,50 but these findings seem to apply particularly to markedly obese patients (BMI >50 kg/m2).37 In the study of Mingrone et al,37 comparing medical therapy with gastric bypass and biliopancreatic diversion, at 2 years diabetes remission was observed in no patients in the medical-therapy group versus 75% in the gastric bypass group and 95% in the biliopancreatic diversion group. Of note, preoperative BMI and weight loss did not predict the improvement in hyperglycemia after these procedures. In spite of such important findings, this study also has some limitations, such as the relatively short follow-up period and the lack of cutoffs for dyslipidemia or arterial blood pressure at baseline among the eligibility criteria for randomization.37
On the other hand, intestinal malabsorption after biliopancreatic diversion can increase the incidence of late nutritional complications, such as hypoalbuminemia and deficiencies in vitamin D and calcium, even with vitamin and mineral supplementation.37 Because of these long-term nutritional side effects, the use of biliopancreatic diversion has decreased in the last years (2% of the bariatric procedures).2
At present, laparoscopic Roux-en-Y gastric bypass seems to be the procedure of choice, achieving good %EWL and good diabetes control in morbidly obese patients.
The resolution of diabetes is often observed before a significant weight loss is obtained.17 Indeed, for example, a recent meta-analysis including 9,756 cases (16 studies) of 2-year effect after surgery,52 comparing laparoscopic Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy, showed that laparoscopic Roux-en-Y gastric bypass had a better long-term effect on body weight, while both laparoscopic Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy showed similar effects on type 2 diabetes mellitus.
In recent years, sleeve gastrectomy has been increasing, also based on these findings.2 Sleeve gastrectomy is, theoretically, a technically simpler surgical approach; it is associated with less vitamin deficiency and can be subsequently converted into Roux-en-Y gastric bypass if its effects are considered unsatisfactory. Probably, sleeve gastrectomy will become a valid alternative to Roux-en-Y gastric bypass in the treatment of type 2 diabetes in morbidly obese patients, but longer follow-up (few data with more than 3-year follow-up are available) and controlled studies are needed to establish its effectiveness.17
However, in the trial of Schauer et al,38 comparing the efficacy of intensive medical therapy alone versus medical therapy plus gastric bypass or sleeve gastrectomy in obese patients with uncontrolled type 2 diabetes, medical therapy plus bariatric surgery achieved glycemic control in significantly more patients than medical therapy alone at 12 months, with no difference between the gastric bypass and the sleeve gastrectomy groups. At 3-year follow-up, the results were confirmed, but gastric bypass surgery was found to be more effective than sleeve gastrectomy as regards glycemic control and weight loss.38 Nevertheless, limitations of this study include an inadequate sample size and duration to detect differences in the incidence of diabetes complications (ie, infarction, stroke, or death).38
On the other hand, resolution of diabetes observed before a significant weight loss has been obtained,17 provided the non-weight-loss glycemic control benefits of the bariatric-metabolic procedures, suggesting the developments of new non-surgical procedures and devices mimicking the bariatric-metabolic conventional surgical procedures in order to study their effectiveness on metabolic status independently from weight loss. These novel procedures are still experimental.11
Which candidate do I choose? Which surgical option?
The duration of the benefit of surgery in diabetes remission is still unclear.11
Some studies on middle-aged obese patients provided an association between weight regain and diabetes recurrence.53 The effectiveness of bariatric-metabolic surgery in diabetic patients with BMI less than 35 kg/m2 has not yet been conclusively evaluated.23,42,54 Several studies have shown encouraging results in assessing surgical treatment as a useful tool in diabetic patients with BMI less than 35 kg/m2, as determined by significant changes in body weight, fasting plasma glucose, HbA1c, and lipid levels.39–41,51,54–57
To date, less invasive bariatric-metabolic procedures (ie, adjustable gastric banding, intragastric balloons), novel extraluminal or endoluminal procedures, or new devices could be proposed to diabetic nonobese patients within controlled clinical trials to assess their safety and effectiveness.11
At present, diabetic patients eligible for bariatric-metabolic procedures remain morbid and obese (BMI ≥35 kg/m2 with significant obesity-related comorbidity – type 2 diabetes, hypertension, obstructive sleep apnea – or BMI ≥40 kg/m2) after failure of nonsurgical options for weight loss. On the other hand, the denial of bariatric surgery to a patient with BMI less than 35 kg/m2 suffering from a significant obesity-related comorbidity simply on the basis of the BMI level does not appear to be clinically justified. A clinical decision should be based on a more comprehensive evaluation of the patient and on a more reliable prediction of future morbidity and mortality.23 Nevertheless, ideally a risk stratification (such as detection of early stages of atherosclerotic disease) should be provided to identify pre-diabetes conditions in obese subjects in order to identify high-risk individuals to potentially prevent the occurrence of type 2 diabetes and its related systemic complications.58
In order to assess which patients could benefit from bariatric-metabolic surgery to achieve diabetic control, preoperative metabolic work-up is of primary importance. An accurate evaluation of the glycemic status (including fasting glucose, HbA1c, insulin sensitivity after oral glucose tolerance test, fasting insulin, fasting C-peptide) is needed.44–46
Because the best results are available in patients with a relatively short history of type 2 diabetes, the surgical option could be considered early, especially in morbidly obese subjects after the failure of medical treatment.2
Roux-en-Y gastric bypass seems at present the surgical procedure of choice because it has fewer risks than biliopancreatic diversion and it is associated with higher weight loss and metabolic improvements compared to adjustable gastric banding.24
Recent evidence regarding the effectiveness of sleeve gastrectomy in diabetes remission must be still confirmed with longer follow-up controlled trials,52 but at present sleeve gastrectomy seems a valid surgical option, especially in high-risk patients (ie, elevated comorbidities, previous abdominal surgery). Nonetheless, sleeve gastrectomy can be subsequently converted into Roux-en-Y gastric bypass if its effects are considered unsatisfactory.
Conclusion
Bariatric-metabolic procedures are considered as an additional therapeutic option allowing improved diabetes control in most of patients.24
The achievable goal of bariatric surgery is not cure, but remission, of the diabetes state.11
A more favorable diabetes remission is achievable in patients with a relatively short history of diabetes duration.44–46
In morbidly obese, diabetic patients, surgery should not be considered as “the last option” but as the appropriate treatment, especially when diabetes is not controlled or when other obesity-related comorbidities are poorly controlled.2
Bariatric-metabolic surgery should be proposed after an adequate careful risk–benefit analysis in high-volume centers with multi-disciplinary teams experienced in the management of obesity and diabetes.11 Nevertheless, regular postoperative nutritional monitoring is required, with attention to appropriate diet after the procedure, monitoring of micronutrient status, and individualized nutritional supplementation.11
Further investigations are needed to clarify the duration of the benefit of surgery in diabetes remission, the mechanism of the success of surgery, and the mechanism associated with diabetic recurrence.11
Disclosure
The authors declare no conflicts of interest in this work.
References
Gloy VL, Briel M, Bhatt DL, et al. Bariatric surgery versus non-surgical treatment for obesity: a systematic review and meta-analysis of randomized controlled trials. BMJ. 2013;22(347):f5934. | |
Dixon JB, le Roux CW, Rubino F, Zimmet P. Bariatric surgery for type 2 diabetes. Lancet. 2012;379(9833):2300–2311. | |
Colditz GA, Willet WC, Rotnizky A, Mason JE. Weight gain as a risk factor for clinical diabetes mellitus in women. Ann Intern Med. 1995;122: 481–486. | |
Chan JM, Rimm EB, Colditz GA, Stampfer MJ, Willett WC. Obesity, fat distribution, and weight gain as risk factors for clinical diabetes in men. Diabetes Care. 1994;17:961–969. | |
Ribaric G, Buchwald JN, McGlennon TW. Diabetes and weight in comparative studies of bariatric surgery vs conventional medical therapy: a systematic review and meta-analysis. Obes Surg. 2014;24(3):437–455. | |
Kramer H, Cao G, Dugas L, Luke A, Cooper R, Durazo-Arvizu R. Increasing BMI and waist circumference and prevalence of obesity among adults with type 2 diabetes: the National Health and Nutrition Examination Surveys. J Diabetes Complications. 2010;24:368–374. | |
Sims EA, Danforth E Jr, Horton ES, Bray GA, Glennon JA, Salans LB. Endocrine and metabolic effects of experimental obesity in man. Recent Prog Horm Res. 1973;29:457–496. | |
Resnick HE, Foster GL, Beardsley J, Ratner RE. Achievement of American Diabetes Association clinical practice recommendations among US adults with diabetes, 1999–2002: the National Health and Nutrition Examination Survey. Diabetes Care. 2006;29:531–537. | |
Garber A, Henry R, Ratner R, et al; LEAD-3 (Mono) Study Group. Liraglutide versus glimepiride monotherapy for type2 diabetes (LEAD-3 MONO): randomized, 52-week, phase III, double blind, parallel-treatment trial. Lancet. 2009;373:473–481. | |
Wong K, Glovaci D, Malik S, et al. Comparison of demographic factors and cardiovascular risk factor control among US adults with type 2 diabetes by insulin treatment classification. J Diabetes Complications. 2012;26:169–174. | |
Dixon JB, Zimmet P, Alberti KG, Mbanya JC, Rubino F; International Diabetes Federation Taskforce on Epidemiology and Prevention. Bariatric surgery for diabetes: the International Diabetes Federation takes a position. J Diabetes. 2011;3:261–264. | |
Raffaelli M, Guidone C, Callari C, Iaconelli A, Bellantone R, Mingrone G. Effect of gastric bypass versus diet on cardiovascular risk factors. Ann Surg. 2014;259(4):694–699. | |
Colquitt JL, Picot J, Loveman E, Clegg AJ. Surgery for obesity. Cochrane Database Syst Rev. 2009;2:CD003641. | |
Poirier P, Auclair A. Role of bariatric surgery in diabetes. Curr Cardiol Rep. 2014;16:444. | |
Picot J, Jones J, Colquitt JL, et al. The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: a systematic review and economic evaluation. Health Technol Assess. 2009;13: 1–190, 215–357. | |
Cremieux PY, Buchwald H, Shikora SA, Ghosh A, Yang HE, Buessing M. A study on the economic impact of bariatric surgery. Am J Manag Care. 2008;14:589–596. | |
Pham S, Gancel A, Scotte M, et al. Comparison of the effectiveness of four bariatric surgery procedures in obese patients with type 2 diabetes: a retrospective study. J Obes. 2014;2014:638203. | |
Ricci C, Gaeta M, Rausa E, Macchitella Y, Bonavina L. Early impact of bariatric surgery on type II diabetes, hypertension, and hyperlipidemia: a systematic review, meta-analysis and meta-regression on 6,587 patients. Obes Surg. 2014;24:522–528. | |
NIH. Gastrointestinal surgery for severe obesity: National Institutes of Health Consensus Development Conference Statement. Am J Clin Nutr. 1992;55:615S–619S. | |
Fried M, Hainer V, Basdevant A, et al. Inter-disciplinary European guidelines on surgery of severe obesity. Int J Obes (Lond). 2007;31: 569–577. | |
The Obesity Society and American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Executive summary: guidelines (2013) for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society. Obesity (Silver Spring). 2014;22(Suppl 2):S5–S39. | |
Mechanick JI, Kushner RF, Sugerman HJ, et al. American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic and Bariatric Surgery Medical guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Endocr Pract. 2008;14(Suppl 1):1–83. | |
Busetto L, Dixon J, De Luca M, Shikora S, Pories W, Angrisani L. Bariatric surgery in class I obesity: a position statement from the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO). Obes Surg. 2014;24:487–519. | |
Tham JC, Howes N, le Roux CW. The role of bariatric surgery in the treatment of diabetes. Ther Adv Chronic Dis. 2014;5(3):149–157. | |
Longitudinal Assessment of Bariatric Surgery (LABS) Consortium; Flum DR, Belle SH, et al. Perioperative safety in the longitudinal assessment of bariatric surgery. N Engl J Med. 2009;361: 445–454. | |
Buchwald H, Estok R, Fahrbach K, Banel D, Sledge I. Trends in mortality in bariatric surgery: a systematic review and meta-analysis. Surgery. 2007;142:621–632. | |
Rubino F, Marescaux J. Effect of duodenal-jejunal exclusion in a non-obese animal model of type 2 diabetes: a new perspective for an old disease. Ann Surg. 2004;239:1–11. | |
Strader AD, Vahl TP, Jandacek RJ, Woods SC, D’Alessio DA, Seeley RJ. Weight loss through ileal transposition is accompanied by increased ileal hormone secretion and synthesis in rats. Am J Physiol Endocrinol Metab. 2005;288:E447–E453. | |
Koehestanie P, de Jonge C, Berends FJ, Janssen IM, Bouvy ND, Greve JW. The effect of the endoscopic duodenal-jejunal bypass liner on obesity and type 2 diabetes mellitus, a multicenter randomized controlled trial. Ann Surg. 2014;260(6):984–992. | |
Pournaras DJ, Osborne A, Hawkins SC, et al. Remission of type 2 diabetes after gastric bypass and banding: mechanisms and 2 year outcomes. Ann Surg. 2010;252:966–971. | |
Nannipieri M, Mari A, Anselmino M, et al. The role of beta-cell function and insulin sensitivity in the remission of type 2 diabetes after gastric bypass surgery. J Clin Endocrinol Metab. 2011;96:e1372–e1379. | |
Haluzík M. Bariatric surgery and the mechanism of diabetes remission: are we getting there? J Clin Endocrinol Metab. 2013;98:4336–4338. | |
Cummings DE, Overduin J, Foster-Shubert KE, Carlson MJ. Role of the bypassed proximal intestine in the anti-diabetic effects of bariatric surgery. Surg Obes Relat Dis. 2007;3:109–115. | |
Nguyen KT, Korner J. The sum of many parts: potential mechanisms for improvement in glucose homeostasis after bariatric surgery. Curr Diab Rep. 2014;14:481. | |
Peluso L, Vanek VW. Efficacy of gastric bypass in the treatment of obesity-related comorbidities. Nutr Clin Pract. 2007;22:22–28. | |
Vest AR, Heneghan HM, Agarwal S, Schauer PR, Young JB. Bariatric surgery and cardiovascular outcomes: a systematic review. Heart. 2012;98:1763–1777. | |
Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric surgery versus conventional medical therapy for type 2 diabetes. N Engl J Med. 2012;366:1577–1585. | |
Schauer PR, Bhatt DL, Kirwan JP, et al; STAMPEDE Investigators. Bariatric surgery versus intensive medical therapy for diabetes – 3-year outcomes. N Engl J Med. 2014;370:2002–2013. | |
Ikramuddin S, Korner J, Lee WJ, et al. Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes, hypertension, and hyperlipidemia: The Diabetes Surgery Study Randomized Clinical Trial. JAMA. 2013;309:2240–2249. | |
O’Brien PE, Dixon JB, Laurie C, et al. Treatment of mild to moderate obesity with laparoscopic adjustable gastric banding or an intensive medical program. A randomized trial. Ann Intern Med. 2006;144: 625–633. | |
Dixon JB, O’Brien PE, Playfair J, et al. Adjustable gastric banding and conventional therapy for type 2 diabetes: a randomized controlled trial. JAMA. 2008;299(3):316–323. | |
Courcoulas AP, Goodpaster BH, Eagleton JK, et al. Surgical vs medical treatments for type 2 diabetes mellitus: a randomized clinical trial. JAMA Surg. 2014;149:707–715. | |
Sjöström L, Peltonen M, Jacobson P, et al. Association of bariatric surgery with long-term remission of type 2 diabetes and with microvascular and macrovascular complications. JAMA. 2014;311:2297–2304. | |
Arterburn DE, Bogart A, Sherwood NE, et al. A multisite study of long-term remission and relapse of type 2 diabetes mellitus following gastric bypass. Obes Surg. 2013;23:93–102. | |
Robert M, Ferrand-Gaillard C, Disse E, et al. Predictive factors of type 2 diabetes remission 1 year after bariatric surgery: impact of surgical techniques. Obes Surg. 2013;23:770–775. | |
Dixon JB, Chuang LM, Chong K, et al. Predicting the glycemic response to gastric bypass surgery in patients with type 2 diabetes. Diabetes Care. 2013;36:20–26. | |
Yan YX, Wang GF, Xu N, Wang FL. Correlation between postoperative weight loss and diabetes mellitus remission: a meta-analysis. Obes Surg. 2014;24(11):1862–1869. | |
DiGiorgi M, Rosen DJ, Choi JJ, et al. Re-emergence of diabetes after gastric-bypass in patients with mid- to long-term follow up. Surg Obes Relat Dis. 2010;6:249–253. | |
Campos GM, Rabl C, Roll GR, et al. Better weight loss, resolution of diabetes, and quality of life for laparoscopic gastric bypass versus banding: results of a 2-cohort pair-matched study. Arch Surg. 2011;146: 149–155. | |
Buchwald H, Estok R, Fahrbach K, et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am J Med. 2009;122:248–256.e5. | |
Schauer PR, Kashyap SR, Wolski K, et al. Bariatric surgery versus intensive medical therapy in obese patients with diabetes. N Engl J Med. 2012;366:1567–1576. | |
Zhang C, Yuan Y, Qiu C, Zhang W. A meta-analysis of 2-year effect after surgery: laparoscopic Roux-en-Y gastric bypass versus laparoscopic sleeve gastrectomy for morbid obesity and diabetes mellitus. Obes Surg. 2014;24(9):1528–1535. | |
Campos JM, Lins DC, Silva LB, Araujo-Junior JG, Zeve JL, Ferraz AA. Metabolic surgery, weight regain and diabetes re-emergence. Arq Bras Cir Dig. 2013;26(Suppl 1):57–62. | |
Yin J, Xu L, Mao Z, et al. Laparoscopic Roux-en-Y gastric bypass for type 2 diabetes mellitus in nonobese Chinese patients. Surg Laparosc Endosc Percutan Tech. 2014;24(6):e200–e206. | |
Lee WJ, Chong K, Ser KH, et al. Gastric bypass vs sleeve gastrectomy for type 2 diabetes mellitus: a randomized controlled trial. Arch Surg. 2011;146:143–148. | |
Li Q, Chen L, Yang Z, et al. Metabolic effects of bariatric surgery in type 2 diabetic patients with body mass index of 35 kg/m2. Diabetes Obes Metab. 2012;14:262–270. | |
Reis CE, Alvarez-Leite JI, Bressan J, Alfenas RC. Role of bariatric–metabolic surgery in the treatment of obese type 2 diabetes with body mass index <35 kg/m2: a literature review. Diabetes Technol Ther. 2012;14(4):365–372. | |
Ciccone MM, Scicchitano P, Cameli M, et al. Endothelial function in pre-diabetes, diabetes and diabetic cardiomyopathy: a review. J Diabetes Metab. 2014;5:364. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.