Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Assessing Risk Factors for Visceral Leishmaniasis Outbreak in South Omo Zone, Southern Ethiopia: Implications for Tailored Intervention Strategies
Authors Churko C ![]() , Kassahun AB
, Kassahun AB ![]() , Yohanes T, Zerdo Z, Degaga TS
, Yohanes T, Zerdo Z, Degaga TS ![]() , Zewdie TH, Bokicho B, Tamiru A, Seife F
, Zewdie TH, Bokicho B, Tamiru A, Seife F ![]() , Kebede Z, Manaye N, Beshah AM, Massebo F, Keto HB, Gebremickael A
, Kebede Z, Manaye N, Beshah AM, Massebo F, Keto HB, Gebremickael A ![]()
Received 21 June 2025
Accepted for publication 17 October 2025
Published 6 November 2025 Volume 2025:18 Pages 7299—7309
DOI https://doi.org/10.2147/JMDH.S548586
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Chuchu Churko,1 Alemayehu Bekele Kassahun,1 Tsegaye Yohanes,2 Zerihun Zerdo,2 Tamiru Shibiru Degaga,3 Tadiwos Hailu Zewdie,3 Belachew Bokicho,4 Adugna Tamiru,5 Fikre Seife,5 Zeyede Kebede,6 Nigus Manaye,6 Abate Mulugeta Beshah,7 Fekadu Massebo,8 Henock Bekele Keto,6 Abinet Gebremickael1
1Collaborative Research and Training Center for Neglected Tropical Diseases, Arba Minch University, Arba Minch, South Ethiopia Region, Ethiopia; 2Department of Medical Laboratory, Arba Minch University, Arba Minch, South Ethiopia Region, Ethiopia; 3Department of Internal Medicine, Arba Minch University, Arba Minch, South Ethiopia Region, Ethiopia; 4Regional Health Bureau, Jinka, South Ethiopia Region, Ethiopia; 5Neglected Tropical Diseases Team, Ministry of Health, Addis Ababa, Ethiopia; 6WHO Country Office, Addis Ababa, Ethiopia; 7WHO African Regional Office, Brazzaville, Republic of the Congo; 8Department of Biology, Arba Minch University, Arba Minch, South Ethiopia Region, Ethiopia
Correspondence: Chuchu Churko, Email [email protected]
Background: Visceral leishmaniasis (VL) is a severe, life-threatening public health concern in Ethiopia. Since early 2022, the outbreak of VL in the South Omo Zone, particularly among pastoralist communities, has resulted in multiple deaths.
Objective: To assess the risk factors contributing to the VL outbreak in South Omo Zone, southern Ethiopia.
Methods: A mixed-method study was conducted in Hammer, Nyangatom, and Selamago districts (areas with the highest case load). The study included a stakeholder consultative workshop and qualitative interviews with health workers, community leaders, and caregivers. A matched case-control study was also performed, and conditional logistic regression was used to analyze quantitative data.
Findings: The stakeholder consultation revealed 64 challenges linked to the outbreak. The top-ranked challenge was the high non-medical cost of VL diagnosis and treatment, followed by limited government and stakeholder commitment. Notably, the absence of governmental structure in the Mursi area (Selamago district) was identified as a significant barrier despite being ranked 11th. Qualitative data highlighted additional challenges: poor transportation, distant treatment services, low awareness, cultural treatment practices, and lengthy therapy duration. Quantitatively, family history of VL was a significant risk factor (AOR = 2.91, 95% CI: 1.73– 4.87), while VL cases were more likely to have good knowledge of the disease than controls (AOR = 6.6, 95% CI: 2.34– 18.42).
Conclusion: The findings highlight significant challenges in the control and management of visceral leishmaniasis (VL) in South Omo Zone, including high non-medical costs of care, limited government commitment, inadequate outbreak preparedness, and shortages of trained providers. Prioritized strategies emphasized strengthening health systems, mobilizing resources, and engaging political and community leaders. Addressing systemic gaps and strengthening community-based interventions are essential for effective VL outbreak control and timely treatment.
Keywords: visceral leishmaniasis, risk factors, outbreaks, South Omo zone, Ethiopia
Introduction
Visceral leishmaniasis (VL) is among the deadly neglected tropical diseases caused by Leishmania parasites and spreads through bites from infected phlebotomine sandflies. It mainly affects impoverished communities in tropical and subtropical regions. Approximately 350 million people in 79 countries are at risk of contracting the disease, with an annual global incidence ranging from 50,000 to 90,000 cases (only 25–45%) and 20,000 to 40,000 deaths annually.1
Ethiopia is a country with a high burden of VL cases, with an estimated annual burden of 2000–4500 cases and an at-risk population of 3.2 million people. The spread of the disease in Ethiopia began in the 1940s along the Kenyan border, and currently, VL has become endemic in various regions of the country, including the southern, southwestern, northern, northwestern, eastern, and southeastern areas.2
Currently, it is endemic in several regions of Ethiopia, including Amhara, Tigray, the Southern Nation, the Nationality of People Region (SNNP), Oromia, and Afar.2 The Humera-Metema lowlands that border Sudan are the most affected regions in the country, with approximately 60% of the reported cases of VL recorded in these areas. The remaining 40% of the VL cases in Ethiopia are spread across different southern foci, such as the Omo Plains, the Aba Roba Focus in the Segen Valley, the Woito River Valley adjacent to South Omo, and the Moyale area.3 A recent systematic review and meta-analysis revealed that the pooled prevalence of VL in Ethiopia was 16%.4
The control and prevention of leishmaniasis are complex and require many tools. According to the World Health Organization (WHO) recommendation, VL prevention measures include early diagnosis and prompt treatment, effective disease surveillance, control of animal reservoir hosts, social mobilization, strengthening partnerships and vector control.1
In 2022, the South Omo Zone of Southern Ethiopia experienced an outbreak of VL, resulting in a loss of life and significant consequences for local communities. These communities, which are primarily pastoralists, face challenges accessing life-saving treatment and are highly vulnerable to the disease. Ongoing drought exacerbates this problem by causing malnutrition and increasing the severity of VL. The movement of individuals in and out of endemic regions may also play a role in the potential for VL outbreaks. Furthermore, the conflicts among the study population and their neighbors, coupled with their nomadic way of life, have led to both internal and international migration. Apart from speculation, no specific factors have been identified as contributing to this outbreak, leaving the causes of the outbreak unclear. This underscores the importance of conducting an assessment to determine the underlying reasons for the outbreak. The primary objective of the present research was to identify the risk factors, challenges and possible solutions for the visceral leishmaniasis outbreak as a starting point for the development of successful prevention and control strategies.
Methods
Study Area Description
This survey was conducted in three districts of the South Omo Zone, southern Ethiopia, affected by an outbreak of visceral leishmaniasis, namely, Selamago, Nyangatom and Hammer. The South Omo zone has a total population of 834,545. The zone bordered Kenya in the south and South Sudan in the southwest.
The Selamago district has 8 health centers (including 3 health centers in the sugarcane factory) and 17 health posts (of which 2 health posts are functional only when there is no security problem). No health posts were made at any of the two health centers (Haylhuha and Maki) in the Selamago district, where there are many reports of VL cases and there are frequent internal conflicts in the community.5 The Nyangatom district has 2 health centers and 15 health posts. There are 4 health centers and 27 health posts in Hammer.
Visceral leishmaniasis cases that came from either side of the border were found at Jinka Hospital in the South Omo Zone of Ethiopia, where the first confirmed case of VL was detected on June 28, 2022. With successive passive screening and laboratory testing of patients fulfilling the clinical criteria, the hospital diagnosed more patients with visceral leishmaniasis, reaching 274 cases by February 2024 (WHO country office unpublished report, 2024). The diagnosis of cases was made using parasitological assessment by trained and skilled laboratory experts at Jinka general hospital.
Study Design and Period
A mixed method study design (both qualitative and matched case control) was employed to identify risk factors, challenges and possible solutions for visceral leishmaniasis outbreak from November 1 to December 30, 2023.
Populations and Sampling
For the quantitative survey, cases were retrieved from the record of patients treated at Jinka Zonal hospital during the outbreak. Controls were close neighbors of cases with no history of VL and no sign and symptoms of VL (splenomegaly, hepatomegaly, fever lasting at least 2 weeks and headache). For one case identified, two controls from neighbors of the case with similar age range (<5 years, 5–14 years, 15–39 years and 40 years and older), sex and location were included in the study. Health extension workers, community leaders, religious leaders and VL cases were involved to explore facilitators of visceral leishmaniasis outbreak. In addition, stakeholder’s workshop was held for two days to explore challenges and possible solutions for the outbreak control.
Eligibility Criteria
For case control study: All cases confirmed as having VL by laboratory were included in the study. Critically ill patients other than VL and those patients who are mentally ill were excluded from the study. Controls that were living in the same area (preferably neighbors) for the VL cases were eligible for interview. Those controls that were lived less than 6 months in the study area were excluded. For in-depth interview study: all health extension workers, community and religious leaders, and VL cases in the study area were eligible for the in-depth interview. But those who were on annual leave, severely ill during data collection were excluded from the study.
Sample Size
For stakeholders meeting, 4 regional health bureau officials, 5 zonal health department personnel, 7 district health office heads and professionals, 6 health facility professionals and heads and 1 partner were involved to identify challenges and solutions for the outbreak. For case control study, The sample size was determined by using the double population proportion approach using Epi Info version 7 statistical software package with the assumption of 95% confidence level (Zα/2 = 1.96), 80% power, case to control ratio of 1:2 and by taking different factors from two different studies conducted in Amhara and Western Tigray regions, Ethiopia by adding 10% non-response rate, final estimated sample size of 504, 168 cases and 336 controls. For in-depth interview, we did not use any statistical formulas to determine sample size, but rather we based on conceptual depth and data saturation (when the complete range of constructs that made up the theory was fully represented by the data/informational redundancy a point when no new insights would be obtained from expanding the sample further). We used 28 participants for in-depth interviews. Purposive sampling technique was used to select the qualitative interviewee.
Operational Definitions
Cases and Controls
Cases were those VL confirmed patients at Jinka hospital where outbreak occurred using parasitological test by trained and skilled laboratory experts and controls were individuals who diagnosed clinically as VL free.
Data Collection
A structured questionnaire was used to assess the risk factors of VL in the outbreak area. The questionnaire has different sections: socio-demographic factors, knowledge, attitude and practices (KAP) on VL, housing condition, living with domestic animals, sleeping nearby termite hills or acacia trees, cracked wall of houses, use of bed nets, travel history, living with dogs, other activities, poverty, travel history, and other factors based on the literature review.
Semi-structured in-depth interview topics were developed and pretested to increase reliability of the tool. All in-depth interview information was recorded by audio ODK software. The audio was recorded in Amharic and other local languages of South Omo (Hammer, Nyangatom and Selamago). The local languages were translated to Amharic during interview by person who could speak both Amharic and the local languages. Then translation of the record to English and transcription was performed using on-line ODK software.
For the stakeholder workshop, a tool was developed which included system, inputs, service delivery, outputs and outcome domains with various questions. Group discussion was held after familiarizing the participants with the data collection tool. Discussion was made in three groups, region-zonal, district and health facility levels. Then, the investigators facilitated the discussion based on the priory organized data collection tool.
Data Processing and Analysis
For qualitative survey, data were organized using manual coding techniques to categorize and produce themes. The method for generating codes involved using an integrated approach to developing code structure. This process involves both inductive development of codes as well as a deductive organizing framework for code types. For stakeholder data, ranking of challenges raised by the participants was made based on its importance, implementation feasibility, health system willingness, financial feasibility, logistic feasibility, efficiency and accessibility. Score was given from 1 to 10 for each above criteria. All participants gave score for the identified challenges out of 10 independently and the result was average for each challenge for all study participants. Finally, priority was given for the highest rank of the challenge. For the case control study, a conditional logistic regression model was fitted to identify determinants of visceral leishmaniasis outbreak.
Ethical Consideration
This study was conducted in accordance with the Declaration of Helsinki, and all participants’ data were strictly confidential throughout the study. Verbal informed consent was acceptable and approved by the Arba Minch University Institutional Ethics Review Board and permission was obtained from South Omo Zone Health Department. Verbal informed consent was also obtained from all study participants. Participants informed consent included publication of anonymized responses/direct quotes. Verbal informed consent was obtained from parents or guardians of participants under age 18 years old.
Results
Background of the Workshop Participants
One consultative stakeholders meeting was conducted for two consecutive days at Jinka town, South Omo zone, South Ethiopia region, Ethiopia from December 30–31, 2023. A total of 23 experts participated in the meeting from regional, zonal, districts and health facilities which were endemic for VL. Majority of these were from districts health office 7 (30.4%) followed by health facilities 6 (26.1%) and zonal health department 5 (21.7%) (Table 1).
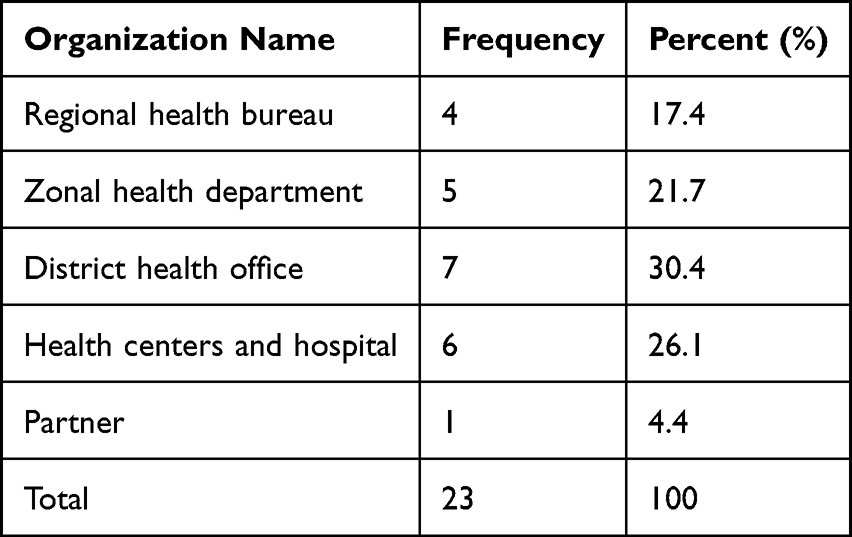 |
Table 1 Stakeholders Consultative Workshop Participants’ Background |
The Top Ranked Challenges of VL Outbreak Control in South Omo Zone
A total of 64 challenges were identified and ranked in this study (Supplementary Table 1.docx). Of the top ten ranked challenges presented in Table 2, three and two challenges were related with health financing and governance/leadership key functional areas, respectively. The top ranked challenge identified by the respondents was expensiveness of the non-medical cost for investigation and management of visceral leishmaniasis. Low commitment of government and stakeholders was recorded as the second most common challenge for the outbreak management. The other top five ranked challenges were no outbreak investigation, no Emergency preparedness and readiness plan (EPRP), mis-management of drugs and insufficient health care provider for VL management (Table 2).
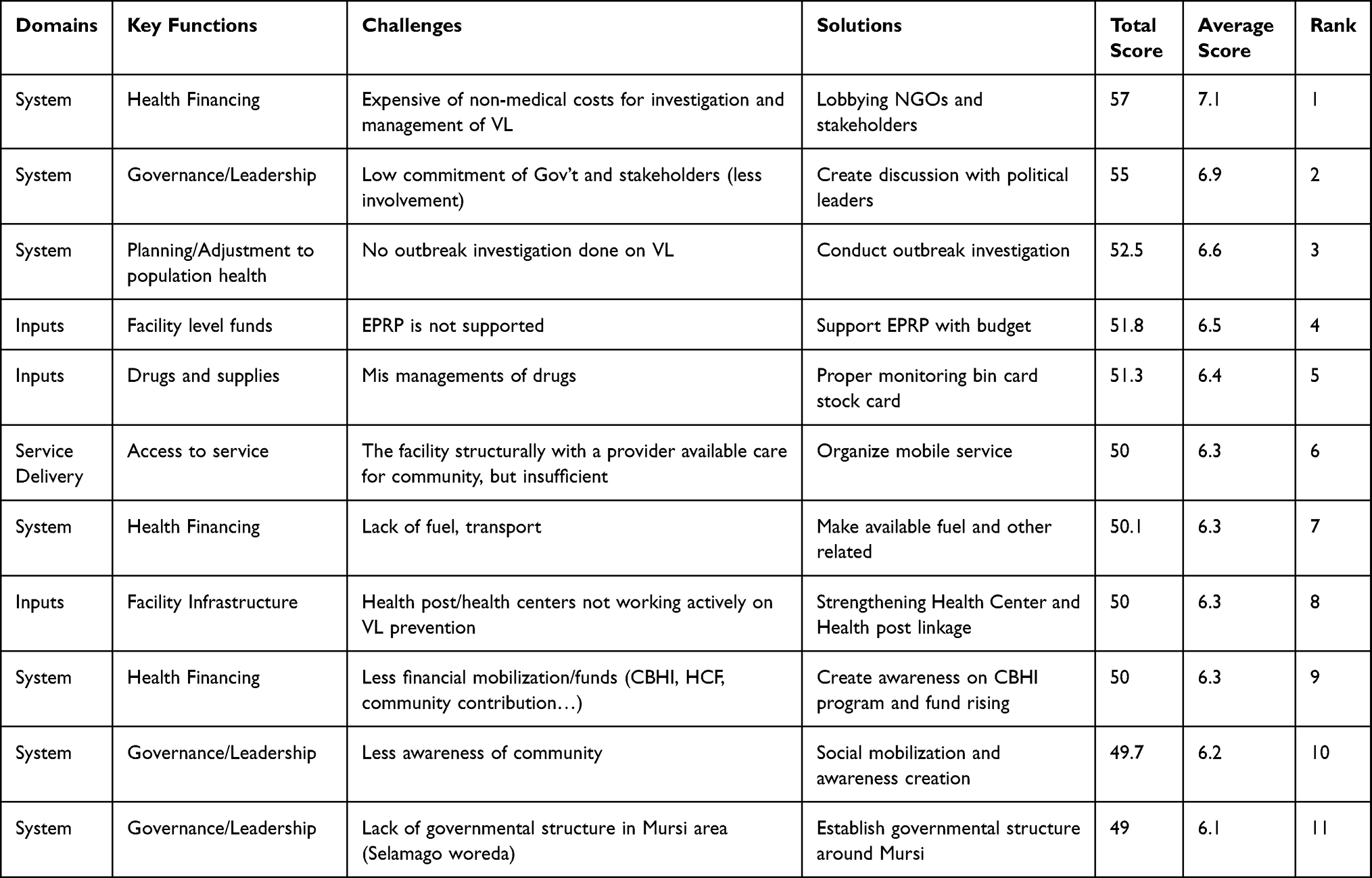 |
Table 2 Top Ten Ranks Strategies for Identified Challenges for VL Control |
Prioritized Strategies/Solutions for the Identified Challenges for VL Control
Table 2 shows the top ten ranked solutions for challenges identified for controlling visceral leishmaniasis outbreak at South Omo zone. Of these strategies, 6 were related with system, 3 input and 1 service delivery domain. The top three strategies were lobbying NGOs and stakeholders for funding to reduce non-medical costs of VL. Creating discussion forum with political leaders and conducting outbreak investigation were considered as the possible solutions for health financing and leadership key functional areas (Table 2).
Socio-Demographic Characteristics of the Case Control Study Participants
One hundred thirty two cases and 258 controls were included in the final analysis of the conditional logistic regression model. The majority of the study subjects were in the age groups of 5–14 years and 15–39 years, with 186 (47.7%) and 165 (42.3%) participants, respectively. More than half, 236 (60.5%), were male participants. Regarding occupation, most of the study subjects were pastoralists, 337 (86.4%). More than one third, 107 (27.4%), of the participants had a family history of visceral leishmaniasis (Table 3).
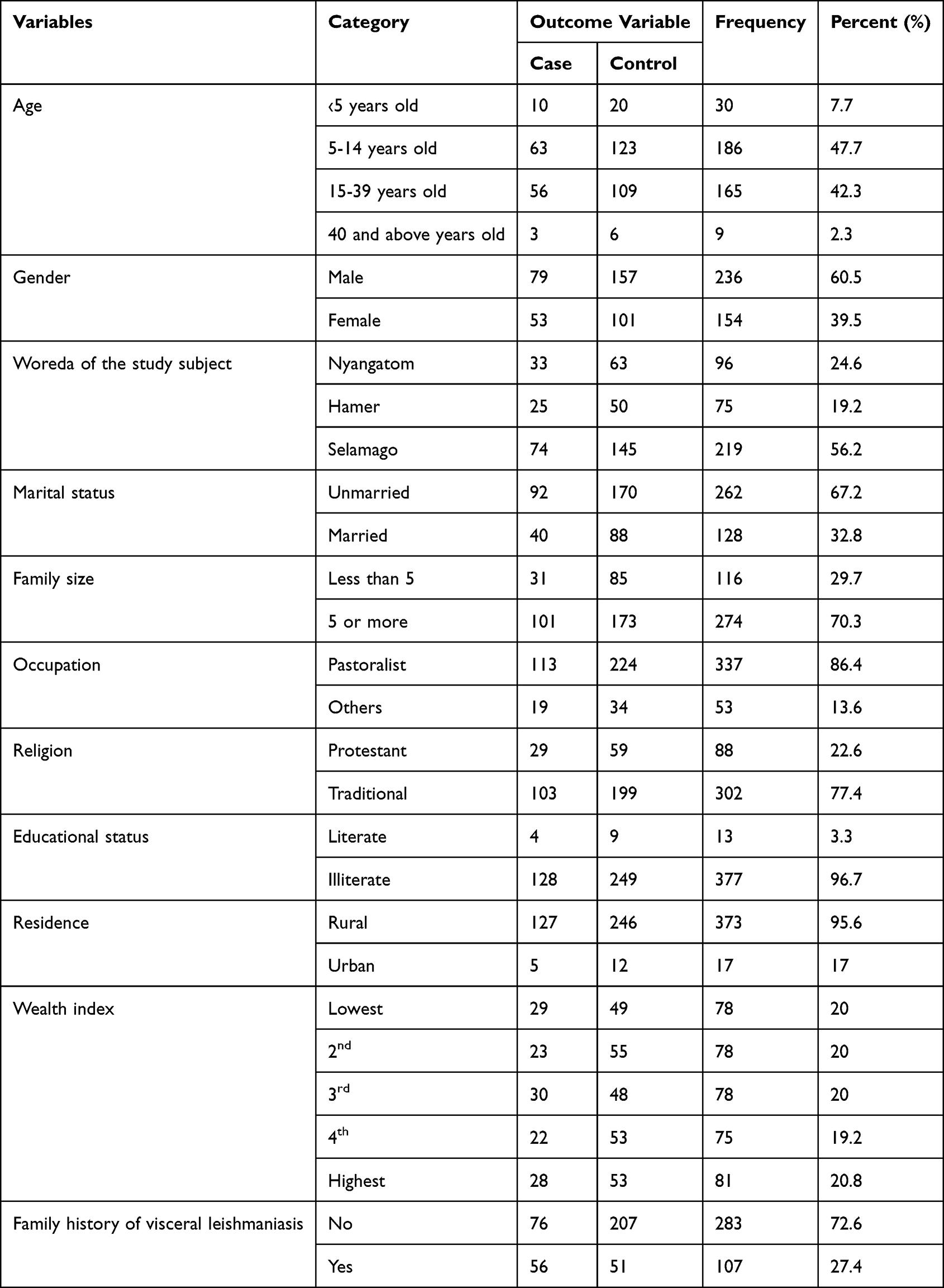 |
Table 3 Socio-Demographic Characteristics of the Study Subjects (N=390) |
Risk Factors of Visceral Leishmaniasis in South Omo Zone
In the univariate analysis, nine variables (marital status, family size, alcohol use, having insect bed nets, family history of VL, presence of termite mounds near the house, cattle ownership, knowledge status, and sleeping under acacia trees) were found to have a p-value of less than 0.25 and were considered candidates for the multivariate conditional logistic regression model. In the final model analysis, two variables (family history of visceral leishmaniasis and knowledge status) were statistically significantly associated with the outcome variable. A family history of visceral leishmaniasis was found to be a risk factor for the VL outbreak (AOR = 2.91, 95% CI: 1.73, 4.87). Regarding participants’ knowledge, those with cases had significantly 6.6 times good knowledge than controls (AOR=6.6, 95% CI: 2.34, 18.42) (Table 4).
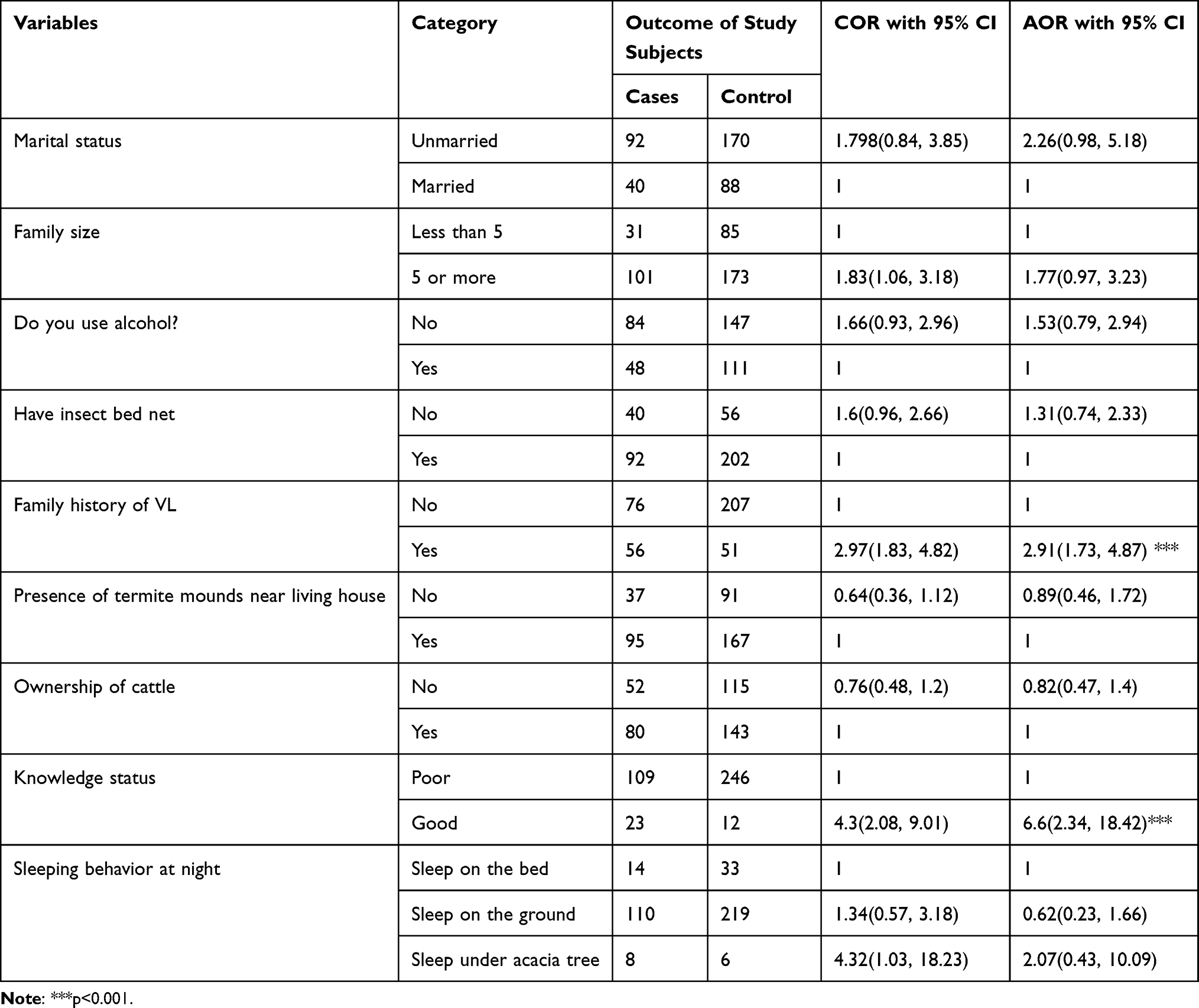 |
Table 4 Multivariate Conditional Logistic Regression Model for Risk Factors of Visceral Leishmaniasis Outbreak in South Omo Zone, South Ethiopia Region, Ethiopia |
Socio-Demographic Characteristics of the in-Depth Interview Study Participants
Majority, 18 (64.3%) of the study subjects were age range between 21 and 40 years old. Nearly three quarter 20 (71.4%) of the respondents were male. In the in-depth interview, health extension and public health workers, religious leaders, community leaders and VL case/caregivers were involved (Table 5).
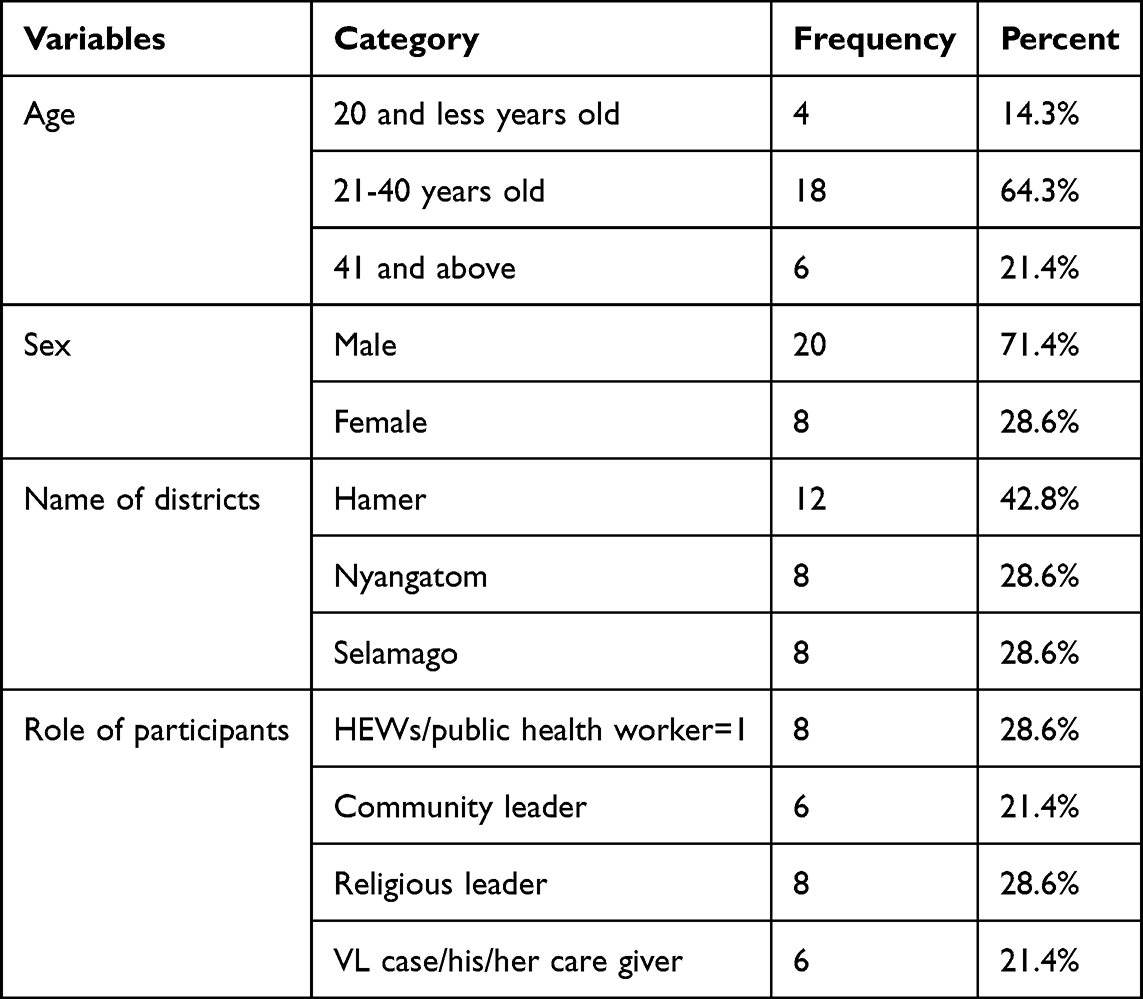 |
Table 5 Socio-Demographic Characteristics of the in-Depth Interview Study Participants, N=28 |
Barriers and Facilitators for Early Treatment of VL
Barriers to Early Treatment
A health extension worker in the Hamer district stated that
lack of money for transportation and the absence of a treatment center near the community were the main challenge for not getting early treatment for visceral leishmaniasis. Another significant barrier was the community’s belief that the disease would heal on its own over time. (32-year-old health extension worker).
A health extension worker from Salamago said that
Firstly, they did not know the consequence of the disease if left untreated. Secondly, transportation problem is a big challenge to access the treatment and third, during travel to hospital for treatment, they fear treatment and other related cost they waste in the stay at hospital. (age=26, Female, HEW)
The other health extension worker mentioned that
the believe of the community towards effectiveness of modern treatment. Rather they prefer to use cultural and religious medications for treatment of visceral leishmaniasis. Even though, they want to take modern treatment, the center is far from the community. (Nyangatom district, HEW, age=27 yrs old, female)
Visceral leishmaniasis patients and their caregivers reported the same barriers to early treatment as those identified by health extension workers. For example, a 25-year-old individual who was treated for and cured of VL said that
when I was sick my big challenge was transportation problem because the treatment center is too far from the community.
Facilitators to Early Treatment
Most participants reported that improving access to transportation, providing diagnosis and treatment centers close to the community preferably at the health center level and raising awareness through community mobilization and sensitization about the importance of early treatment and the complications of delayed care were possible solutions to facilitate early VL treatment. For example, a health extension worker from Selamago district reported that:
providing treatment in health facilities nearby the community will facilitate early treatment. For those who screened as suspected case transportation should be provided. (Age 26, Salamago, female HEW)
A community leader from Hamer said that
we are creating awareness about the importance of treatment and it is given free of cost at hospital. Some them are not aware that it is free from any cost. (Female, age=38 years old)
Similar solution was forwarded by the religious leader
The patients and their families will not go in trouble if the treatment center is nearby the community, at least health center level. (Male, age=70, Kolakeja kebele, Hammer district).
Discussion
To contribute to the goal of universal health coverage, it is essential to ensure early detection and timely reporting, efficient diagnosis and treatment of cases, and the expansion of services to the most vulnerable groups. Everyone should have access to the full range of quality health services they need, when and where they need them, without financial hardship.6 In this study, we identified the challenges and potential solutions related to the visceral leishmaniasis outbreak in the South Omo Zone. Parallel to this, we also tried to identify possible determinants of the disease outbreak and explored barriers and facilitators of early treatments of VL in the study area.
In the current study, the top-ranked challenge in controlling the VL outbreak was the high cost of investigation and treatment. This was followed by limited commitment from the government and stakeholders in the prevention and control of the outbreak. Our qualitative findings support this, revealing that poor community awareness about the fact that treatment is free of charge, as well as a lack of transportation for patients, were key barriers to early treatment. A proposed solution to this challenge is to advocate for greater involvement of stakeholders and the government in the prevention and control of this deadly disease.
The third and fourth challenges identified were the absence of outbreak investigations and the lack of government-supported Emergency Preparedness and Response Plans (EPRP). Participants proposed the following strategies to address these issues: given the fatal nature of the disease, the government should allocate sufficient budget and human resources to support EPRP and conduct rapid outbreak investigations in affected areas. These challenges were not reported in other countries such as Nepal, India, and Bangladesh.7,8 A possible reason for this difference could be the poor economic status of our country, which limits the ability to prioritize and address community concerns.
The study found that the lack of government structure in the Murse/Salamago area and ongoing insecurity were ranked as the 11th major challenge during the stakeholder meeting. There were not functional health posts, health centers or any modern health facilities there. Participants emphasized that establishing a functional government structure is essential for effective outbreak control. Although it was ranked 11th, participants stressed that this issue must be addressed by the Ethiopian government. It cannot be managed solely at the zonal or regional level; national-level involvement is crucial.
According to our case-control study, a family history of visceral leishmaniasis was identified as a risk factor for the occurrence of the outbreak. This finding is consistent with studies conducted in the Americas and other countries, which showed that the odds of VL infection were higher among individuals who had a family member infected with VL compared to those who did not.9–12 This may be due to shared environmental and behavioral factors within households such as living conditions and exposure to sandflies, the vector for VL which contributes to an increased risk of the disease.
Limitations of the Study
This study employed a combination of different research designs to identify the challenges and potential solutions related to outbreak control. However, several limitations should be acknowledged. In the case-control component of the study, the control group consisted of treated cases who had already been informed about the disease and its management during their hospital stay. This prior exposure to information and care may have influenced their responses, potentially affecting the identification of true determinants of the visceral leishmaniasis (VL) outbreak.
Furthermore, in the qualitative component of the study, we relied solely on individual interviews and did not incorporate focus group discussions (FGDs). The absence of FGDs may have limited the depth and diversity of perspectives, particularly regarding community-level barriers and facilitators to early treatment-seeking behavior. FGDs could have provided richer insights into shared beliefs, social dynamics, and cultural practices influencing health-seeking behavior in the affected population.
These limitations should be considered when interpreting the findings, and future research should aim to address them by including a more representative control group and incorporating a broader range of qualitative data collection methods.
Conclusion and Recommendation
The findings highlight significant challenges in the control and management of visceral leishmaniasis (VL) in South Omo Zone, including high costs of care, limited government commitment, inadequate outbreak preparedness, and shortages of trained providers. Prioritized strategies emphasized strengthening health systems, mobilizing resources, and engaging political and community leaders. Quantitative analysis identified family history of VL and knowledge status as key risk factors, while qualitative insights revealed barriers such as lack of awareness, transportation difficulties, cultural beliefs, and limited access to nearby treatment centers. Facilitators included improved access to diagnosis and treatment at local health facilities, community mobilization, and enhanced awareness. Overall, addressing systemic gaps and strengthening community-based interventions are essential for effective VL outbreak control and timely treatment in South Omo Zone.
Data Sharing Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki (as was revised in 2013). Ethical approval was obtained from Arba Minch University Institutional Ethics Review Board and permission was obtained from South Omo Zone Health Department. Oral Informed consent was also obtained from all study participants, and measures were taken to ensure data confidentiality and privacy.
Acknowledgments
This research was conducted with the support of the World Health Organization (WHO) HQ/TDR, the WHO AFRO and the WHO–Ethiopia Country Office. We are particularly grateful to Dr. Abraham ASEFFA for his active facilitation during the transfer of funding from the WHO TDR to Arba Minch University. We also thank the head of the South Omo Zone Health Department, Mr. Tamirat Assefa, and the NTD focal, Mr. Mulusew Alemayehu, for their invaluable support in guiding the data collectors and supervisors throughout the data collection period. We would like to thank the data collectors for their unwavering commitment in collecting data, even in most hardship areas of Selamago and other districts. Finally, we are thankful to the study subjects for their voluntary participation in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work, Project ID P23- 01135, received financial support from TDR, the Special Programme for Research and Training in Tropical Diseases, co-sponsored by UNICEF, UNDP, the World Bank and WHO.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. World Health Organization. Leishmaniasis fact sheet 2023.
2. Tadese D, Hailu A, Bekele F, et al. An epidemiological study of visceral leishmaniasis in North East Ethiopia using serological and leishmanin skin tests. PLoS One. 2019;14(12):e0225083. doi:10.1371/journal.pone.0225083
3. Gadisa E, Tsegaw T, Abera A, et al. Eco-epidemiology of visceral leishmaniasis in Ethiopia. Parasites Vectors. 2015;8:1–10. doi:10.1186/s13071-015-0987-y
4. Assefa A. Leishmaniasis in Ethiopia: a systematic review and meta-analysis of prevalence in animals and humans. Heliyon. 2018;4(8).
5. USAID, Ethiopia south omo zone conflict assessment: final report. 2021.
6. World Health Organization. Developing a strategic plan for the elimination of visceral leishmaniasis in Eastern Africa: report of a stakeholder meeting, Nairobi, Kenya, 24–27 January 2023. World Health Organization; 2024.
7. Mo AX, Pesce J, Hall BF. Visceral leishmaniasis control and elimination: is there a role for vaccines in achieving regional and global goals? Am JTrop Med Hyg. 2016;95(3):514. doi:10.4269/ajtmh.16-0184
8. World Health Organization. Kala-Azar elimination programme: report of a WHO consultation of partners, Geneva, Switzerland, 10-11 February 2015, in Kala-Azar elimination programme: report of a WHO consultation of partners, Geneva, Switzerland, 10-11 February 2015. 2015.
9. Uranw S, Hasker E, Roy L, et al. An outbreak investigation of visceral leishmaniasis among residents of Dharan town, eastern Nepal, evidence for urban transmission of Leishmania donovani. BMC Infect Dis. 2013;13(1):1–9. doi:10.1186/1471-2334-13-21
10. Valero NNH, Uriarte M. Environmental and socioeconomic risk factors associated with visceral and cutaneous leishmaniasis: a systematic review. Parasitol Res. 2020;119(2):365–384. doi:10.1007/s00436-019-06575-5
11. Barnett PG, Singh SP, Bern C, et al. Virgin soil: the spread of visceral leishmaniasis into Uttar Pradesh, India. American JTrop Med Hyg. 2005;73(4):720–725. doi:10.4269/ajtmh.2005.73.720
12. Belo VS, Werneck GL, Barbosa DS, et al. Factors associated with visceral leishmaniasis in the Americas: a systematic review and meta-analysis. PLoS Negl Trop Dis. 2013;7(4):e2182. doi:10.1371/journal.pntd.0002182
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.