Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Assessing Breastfeeding and Family-Centered Care: A Delphi-Based Scale and Its Prediction of Child Psychological Status
Authors Yang Y, Sun N, Wang M, Liu M, Chen S, Liu Y, Jiang W
Received 12 June 2025
Accepted for publication 23 November 2025
Published 3 December 2025 Volume 2025:18 Pages 7847—7864
DOI https://doi.org/10.2147/JMDH.S546721
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Yafei Yang,* Na Sun,* Mengke Wang, Mengying Liu, Shiyan Chen, Ye Liu, Wei Jiang
Department of Pediatrics, South China Hospital, Medical School, Shenzhen University, Shenzhen, 518116, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Jiang, Department of Pediatrics, South China Hospital, Medical School, Shenzhen University, No. 1 Fuxin Road, Pinghu Street, Longgang District, Shenzhen, Guangdong Province, 518116, People’s Republic of China, Email [email protected]
Purpose: This study aims to develop and validate the Breastfeeding and Family-Centered Care Assessment Scale (ScaleSc) utilizing the Delphi method and to examine its association with child psychological status.
Methods: Children aged 6– 14 years were enrolled as study participants. Through multiple rounds of structured expert consultation, a comprehensive scale encompassing core elements of breastfeeding practices and family-centered care was systematically developed. Concurrently, support vector machine (SVM) and decision tree models were constructed utilizing ScaleSc scores alongside other relevant clinical characteristics of the participants.
Results: Multivariate modeling identified higher ScaleSc scores as a significant protective factor against poor psychological status, with the scale demonstrating substantial predictive importance within both computational models. Furthermore, exposure to school bullying (SchBull) emerged as a potent risk factor, exhibiting a markedly elevated odds ratio (OR) of 43.982 within the logistic regression analysis, highlighting its profound detrimental impact on child psychological well-being. The study robustly confirmed the significant influence of breastfeeding practices and family-centered care on child psychological development, demonstrating the ScaleSc’s efficacy in quantitatively linking these critical early-life factors to psychological outcomes.
Conclusion: This research successfully developed and clinically validated the ScaleSc, establishing its significant utility for assessing child psychological status.
Keywords: Delphi method, scale development, model construction, child psychology, breastfeeding, family-centered care
Introduction
Childhood constitutes a critical period for lifelong physical and psychological development, wherein mental health exerts a profound influence on a child’s growth trajectory and future outcomes.1 In recent years, concomitant with socioeconomic advancement and lifestyle transformations, mental health concerns among children have emerged as an increasingly prominent public health challenge.2 Substantial evidence indicates that childhood psychological issues not only detrimentally impact immediate learning, social functioning, and quality of life but may also persist into adulthood if left unaddressed, thereby conferring long-term adverse consequences on individual well-being, psychosocial adaptation, and vocational development.3
Given this significant burden, research has sought to identify key modifiable determinants of child mental health. Early nurturing caregiving is a cornerstone of healthy development; however, the specific, quantifiable contributions of breastfeeding and family-centered care—two foundational yet interconnected practices—remain inadequately explored due to the absence of a standardized assessment tool.
Breastfeeding, as the earliest nutritional modality experienced by infants, provides not only optimal nourishment but also facilitates maternal-infant bonding that fulfills emotional needs and fosters psychological security.4 Concurrently, family-centered care establishes a consistent, stable, and nurturing developmental environment that subtly yet significantly shapes multiple dimensions of psychological development, including emotion regulation, cognitive maturation, and social competence acquisition.5
Nevertheless, contemporary research examining the psychological impact of breastfeeding and family-centered care predominantly focuses on simplistic univariate associations, lacking systematic and integrative assessment frameworks.6 The development and validation of a breastfeeding and family-centered care assessment scale via the Delphi method7 will enable comprehensive and precise quantification of the relative contributions of these factors to childhood psychological development. Furthermore, in-depth investigation into the predictive validity of scale scores regarding child psychological outcomes will facilitate early identification of developmental vulnerabilities, thereby providing a robust foundation for implementing evidence-based early interventions and personalized mental health promotion strategies.
This study aims to develop the aforementioned scale utilizing the Delphi method and elucidate the relationship between scale-derived metrics and childhood psychological functioning. The anticipated outcomes will address critical knowledge gaps while contributing novel theoretical perspectives and methodological approaches to advance both scholarship and practical applications within the field of child mental health.
Methods
Scale Development
Expert Panel Composition and Selection Criteria
A chief physician specializing in pediatrics was recruited based on demonstrated expertise in child growth assessment, management of common pediatric conditions, and documented research contributions to breastfeeding-child health associations. This individual provided medical theoretical frameworks and clinical guidance throughout scale development.
Concurrently, a chief nursing officer with distinguished achievements in nursing management and clinical practice was engaged, requiring many years’ specialized experience in pediatric nursing and family-centered care. This individual possessed comprehensive proficiency in clinical protocols and workflow standardization, coupled with an extensive research background in nursing science. Primary responsibilities encompassed coordinating all nursing-related scale development activities to ensure instrument content alignment with evidence-based clinical practice requirements.
Three registered nurses fulfilling the following criteria were recruited: 1) ≥ 5 years of dedicated pediatric clinical experience, 2) documented diligence and accountability, and 3) demonstrated interpersonal communication competencies. These nurses participated in preliminary scale testing, data collection, and recruitment logistics while providing frontline clinical perspectives during item refinement.
Two associate professors or full professors specializing in developmental child psychology were invited based on their expertise in psychological assessment instrumentation and child mental health evaluation. Their responsibilities encompassed both guiding the selection of psychological indicators during scale design and advising on statistical methodologies for subsequent psychometric analyses.
Five pediatric graduate candidates (master’s or doctoral researchers) were selected according to the following qualifications: 1) comprehensive pediatric knowledge base, 2) proficiency in fundamental research methodologies, and 3) capacity to conduct literature reviews, data organization, and preliminary questionnaire development under faculty supervision, thereby facilitating research implementation.
Item Pool Development
A multidisciplinary expert panel comprising medical, nursing, and psychological specialists collaboratively established comprehensive search strategies utilizing both controlled descriptors and free-text terms. Key search parameters included English terminology such as “breastfeeding”, “family-centered nursing”, “child mental state”, “breastfeeding practice”, “family nursing intervention”, and “pediatric psychological assessment”. Literature published within the preceding decade (2014–2024) was systematically retrieved to ensure contemporary relevance, encompassing comprehensive searches of international databases (PubMed, Web of Science, Embase) and Chinese repositories [China National Knowledge Infrastructure (CNKI), Wanfang Data Knowledge Service Platform, VIP Chinese Science and Technology Journal Database). Supplementary searches extended to conference proceedings and dissertation databases including the CNKI Thesis Database and ProQuest Dissertations & Theses Global to maximize literature coverage.
Two pediatric graduate researchers independently executed the search protocol and conducted preliminary screening, eliminating duplicate records and publications failing to meet predefined inclusion criteria (eg, irrelevant themes, non-conforming study populations). Subsequently, two psychology professors performed blinded verification of screening decisions, with discordant selections resolved through panel consensus. All retained literature underwent systematic organization using reference management software (NoteExpress, EndNote), categorized by thematic focus, methodological approach, and key findings.
The research team conducted critical appraisals of included studies to extract data pertaining to: 1) breastfeeding behavior assessment metrics, 2) implementation and evaluation frameworks for family-centered care, and 3) determinants and measurement indicators of child psychological status. Extracted content was synthesized into a preliminary item repository. Conceptual redundancies were harmonized through terminological standardization, while contradictory findings were reconciled through critical appraisal to establish an evidence-based foundation for scale development.
Parallel to literature analysis, semi-structured patient interviews were conducted using a predefined protocol exploring: (1) challenges encountered during breastfeeding experiences, and (2) desired support mechanisms within family-centered care contexts. Interview transcripts underwent thematic analysis and were integrated with literature-derived evidence, ultimately yielding 33 initial items categorized into five conceptual dimensions for subsequent scale refinement.
Expert Consultation
A rigorously constituted panel of 15 multidisciplinary experts participated in two iterative rounds of consultation to refine the preliminary instrument, comprising 3 pediatricians, 6 clinical psychologists, and 6 nursing administration specialists, with a mean professional experience of 23.16 ± 7.26 years. During the initial consultation phase, evaluators assessed each item’s necessity, relevance, operational feasibility, and comprehensibility using a standardized 5-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree). Concurrently, participants provided qualitative recommendations for modifying specific elements or proposing structural revisions to the questionnaire architecture. Items achieving mean scores ≥ 3.5 were retained without modification, whereas those scoring below this threshold underwent either substantive revision or elimination based on consolidated expert feedback.
Pilot Testing
A feasibility assessment of scale items was conducted through convenience sampling of 30 pediatric patient-caregiver dyads admitted to our hospital between January and February 2024. The preliminary instrument was administered in hardcopy format with face-to-face guidance from research team members, who provided standardized operational definitions and contextual clarifications to enhance participant comprehension.
Reliability and Validity Validation
Study Population
Four distinct cohorts were consecutively enrolled via convenience sampling for sequential validation phases: Cohort 1 comprised 30 established pediatric patient-caregiver dyads participating in qualitative interviews (March 2024); Cohort 2 included 81 dyads undergoing exploratory factor analysis (April-May 2024); Cohort 3 consisted of 298 dyads completing formal reliability and validity testing (June-November 2024); and Cohort 4 involved 40 dyads assessed for test-retest reliability (December 2024).
Inclusion criteria encompassed: (1) children aged 6–14 years meeting predefined developmental parameters; (2) clinically stable children without major congenital anomalies, genetic disorders, psychiatric conditions, or chronic illnesses impacting neurodevelopment (eg, congenital heart disease, inborn errors of metabolism, autism spectrum disorder), thereby minimizing confounding health influences on psychological status; (3) documented history of breastfeeding during infancy; (4) presence of a consistent primary caregiver (parent/grandparent) capable of comprehending and conscientiously completing assessment instruments while exhibiting voluntary commitment to research participation; and (5) provision of informed consent by legal guardians.
Exclusion criteria eliminated: (1) households with non-traditional family structures and (2) families experiencing major physical trauma (eg, severe vehicular accidents, burns) or psychologically distressing events (eg, familial dissolution, bereavement) within the preceding 3 months, as such acute stressors could significantly compromise psychological assessment validity. General characteristics of the cohorts are delineated in Table 1.
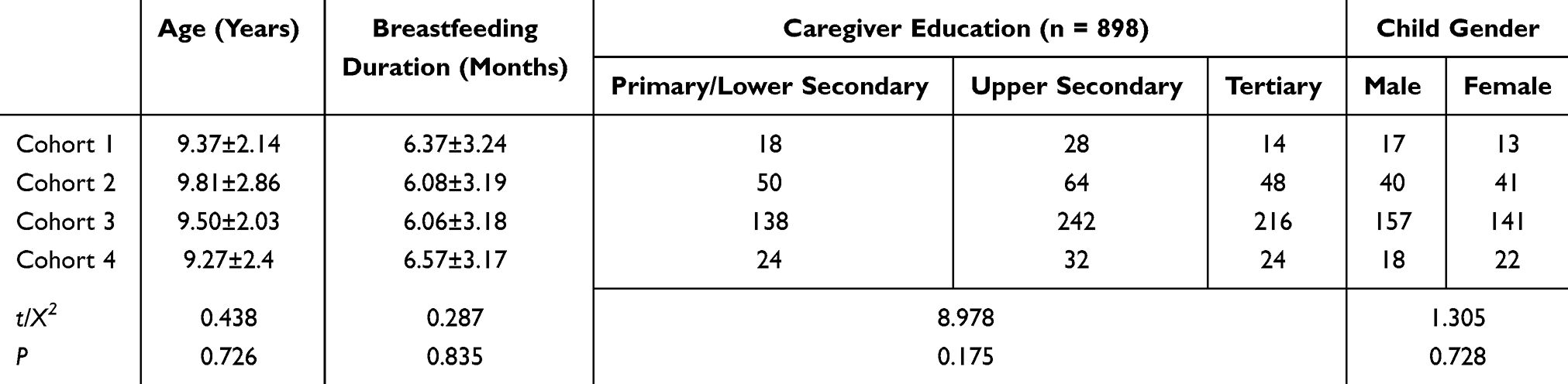 |
Table 1 General Characteristics Across Validation Cohorts |
Data Collection and Quality Control
The 12 research team members underwent domain-specific training and were organized into three specialized units. Prior to survey administration, comprehensive disclosure regarding study objectives and procedures was provided to all participants. Following acquisition of informed consent, researchers administered questionnaires individually, permitting participants to either self-complete instruments or provide verbal responses with investigator transcription. All completed documents were collected immediately post-administration, with same-day data entry into the research database utilizing Microsoft Excel software. To ensure data integrity, the research team implemented rigorous same-day verification protocols involving systematic inspection of all responses to identify and eliminate invalid or incomplete submissions prior to formal analysis.
Item Analysis
Three complementary analytical approaches were employed for psychometric refinement. First, critical ratio (CR) analysis assessed discriminatory power by ranking all scale scores in ascending order, designating the lowest 27% as the low-performance group and the highest 27% as the high-performance group. Inter-group differences were compared using t-tests, with items demonstrating non-significant differentiation (P > 0.05) or inadequate discrimination (CR < 3) considered for removal. Second, Pearson correlation coefficients evaluated item representativeness and dimensionality, whereby items exhibiting weak associations with total scale scores (r < 0.4) were flagged for potential elimination due to poor conceptual coherence. Finally, homogeneity testing examined internal consistency through item-total statistics. Any item whose deletion substantially increased the overall Cronbach’s α coefficient was designated for exclusion to optimize scale reliability.8
Validity Analysis
Exploratory factor analysis (EFA) was performed on Cohort 2 following methodological recommendations by Lloret-Segura et al (2014),9 utilizing a 5-point Likert scale (1 = complete disagreement, 2 = disagreement, 3 = neutral, 4 = agreement, 5 = strong agreement). Post-data collection, principal axis factoring with promax rotation identified latent constructs. Items demonstrating factor loadings below 0.50 were systematically eliminated, with sampling adequacy confirmed by a Kaiser-Meyer-Olkin (KMO) statistic exceeding 0.80, indicating optimal suitability for factor extraction.
Content validity was quantified through the content validity index (CVI) derived from two iterative evaluation rounds by 15 domain experts using the identical Likert framework. Both item-level (I-CVI) and scale-level (S-CVI) indices were computed, establishing acceptable content validity at thresholds of I-CVI ≥ 0.75 and S-CVI/universal agreement ≥ 0.80.
Structural validity was assessed via confirmatory factor analysis (CFA) within a structural equation modeling (SEM) framework, evaluating model fit through multiple indices: chi-square/degree of freedom ratio (X2/DF), comparative fit index (CFI), root mean square error of approximation (RMSEA), goodness-of-fit index (GFI), Tucker-Lewis index (TLI), and incremental fit index (IFI).10
Convergent validity was determined by calculating average variance extracted (AVE) and composite reliability (CR), with values exceeding 0.50 and 0.70 respectively indicating adequate construct representation. Discriminant validity was established when the square root of AVE for each factor exceeded its correlation coefficients with all other latent constructs,11 thereby confirming measurement distinctiveness across theoretical domains.
Reliability Analysis
Internal consistency was quantified through Cronbach’s α coefficient and split-half reliability, while temporal stability was assessed via test-retest reliability. A minimum of 10% of participants from the primary validation cohort were systematically re-evaluated using identical instrumentation at a 1-week post-administration interval. Measurement consistency was deemed methodologically acceptable when Cronbach’s α exceeded the conventional threshold of 0.70.8
Predictive Model Development and Participant Characteristics
Following scale validation, 197 pediatric patients presenting to our hospital between January and May 2025 were prospectively enrolled. Participants were stratified into two cohorts based on integrated psychological assessments: a control group exhibiting favorable mental health status (n = 108) and a study group demonstrating suboptimal psychological functioning (n = 89). Classification utilized standardized instruments including the Child Behavior Checklist12 (CBCL; Cronbach’s α = 0.943), the Screen for Child Anxiety Related Emotional Disorders13(SCARED; Cronbach’s α = 0.971), and structured clinical interviews, with detailed diagnostic criteria specified in Model Construction. Comparative analysis confirmed baseline equivalence in demographic characteristics between cohorts (Table 2), permitting subsequent predictive modeling. The study protocol received the approval from the Ethics Committee of our hospital, with written informed consent obtained from all legal guardians.
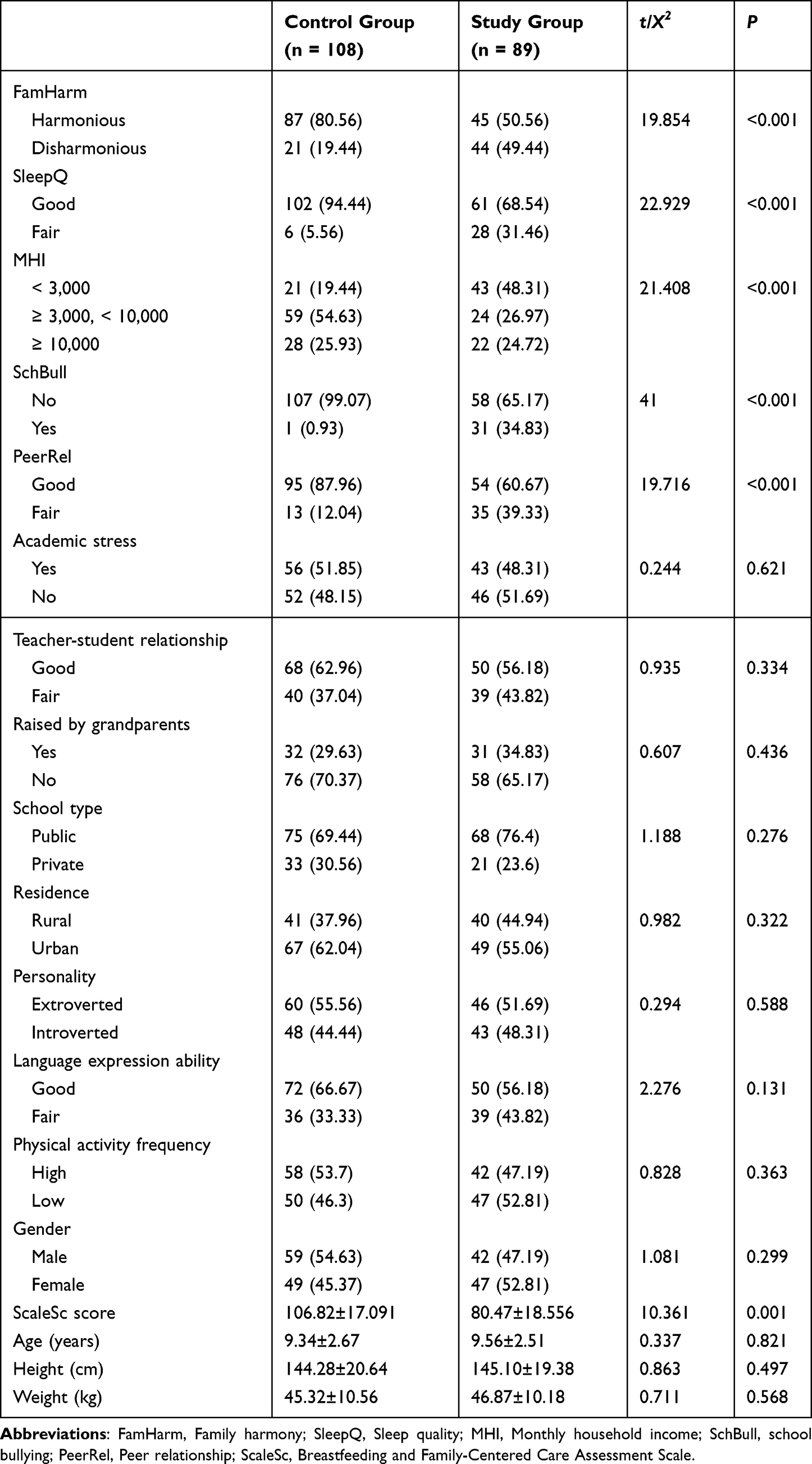 |
Table 2 Analysis of Clinical Characteristics Between Patient Groups |
Inclusion criteria: (1) Children aged 6–12 years meeting WHO growth standards14 and clinical eligibility requirements; (2) Age-appropriate neurodevelopmental trajectories confirmed through pediatric evaluation, encompassing physical growth, linguistic competence, cognitive maturation, and socioemotional functioning without evidence of significant delay; (3) Medically stable status without major congenital disorders (eg, structural heart defects, inborn metabolic errors), chronic conditions requiring acute intervention (eg, uncontrolled diabetes, asthma exacerbations), active systemic infections (eg, severe pneumonia, encephalitis), or psychiatric comorbidities that might confound psychological assessment; (4) Family stability with cognitively competent parents demonstrating comprehension of study protocols and willingness to participate.
Exclusion criteria: (1) History of significant physical trauma (eg, major vehicular accidents, severe burns, complex fractures) or acute psychological trauma (eg, parental bereavement, parental divorce, bullying victimization) within the preceding 3 months, as such events may induce transient psychological disturbances compromising baseline assessment validity; (2) Intellectual disability confirmed by psychometric testing (IQ < 70) given distinct developmental trajectories that limit generalizability to neurotypical populations; (3) Parental refusal to participate or caregiver cognitive impairment precluding reliable data provision.
Model Construction
SPSS software was employed to construct the logistic regression model. Statistical analysis and modeling within the R environment utilized specific package: Support vector machine (SVM) modeling was performed using the e1071 package; model evaluation and parameter tuning were conducted with the caret package; data preprocessing and manipulation were handled by the dplyr package; receiver operating characteristic (ROC) curve analysis was executed via the pROC package; feature importance calculation was implemented using the randomForest package; and decision tree visualization was generated with the rpart package.
Data Collection
Control group (better psychological status) criteria:15 Children were classified into the control group based on the following multi-method assessment. A CBCL social competence T-score ≥ 60 and all syndrome scale T-scores (eg, anxious/depressed) < 60, indicating no significant abnormalities in social competence or emotional/behavioral problems and overall stable functioning. Furthermore, total scores and all subscale scores (separation anxiety, social phobia, panic disorder, generalized anxiety, school phobia) on the SCARED were below established clinical cut-offs, signifying absence of significant anxiety symptoms, generally relaxed affect in daily life and learning, and calm responses to various situations. Clinical interviews revealed children exhibiting good mental status: clear and fluent speech, active and enthusiastic sharing of daily experiences and interests, stable mood, natural expressions, relaxed posture, and good eye contact and interaction with the interviewer. Positive descriptions of harmonious relationships with family and peers were provided. Parental reports confirmed regular daily routines, normal sleep and appetite patterns, absence of significant emotional volatility or behavioral problems, smooth developmental progression, and no major stressful life events.
Study group (poorer psychological status) criteria:16 Children were assigned to the study group if they met either of the following CBCL criteria: a social competence T-score < 40, reflecting significant deficits in activity participation, social interaction, or academic performance, or at least one syndrome scale T-score ≥ 60 (eg, elevated anxious/depressed scores indicating negative emotions like anxiety/depression, or elevated aggressive behavior scores suggesting problems like aggression or destruction). Additionally, a total SCARED score or any subscale score exceeding the clinical cut-off was required. For instance, a high separation anxiety score indicated excessive distress (crying, nervousness, somatic symptoms like vomiting/diarrhea) upon parental separation, while a high social phobia score reflected extreme tension/shyness in social settings, avoidance of interaction, and fear of negative evaluation. Clinical interviews in this group consistently showed negative and low mood, lethargy, weak and slow verbal responses, frequent use of brief/negative phrases (eg, “don’t know”, “whatever”), disinterest in interview content, and active avoidance of certain topics. Marked emotional lability was observed, including sudden crying without apparent cause or intense anger over minor issues. Nonverbal cues included rigid/uncomfortable posture (eg, hunching), avoidance of eye contact, and minimal interaction with the interviewer. Parental reports documented recent poor sleep quality (difficulty initiating sleep, frequent night waking), significantly reduced appetite with weight loss, difficulty concentrating, low learning efficiency, frequent conflicts/arguments with peers at school, increasing social withdrawal and sensitivity, and reluctance to communicate with family. If recent stressful events occurred (eg, changing schools, family disruption), children exhibited significant adjustment difficulties and maladaptation.
Concurrently, comprehensive clinical data were collected based on parental reports and hospital records. This encompassed height, weight, academic stress levels, quality of teacher-student relationships, whether raised by grandparents, school type, residence location, personality traits (extroverted/introverted), language expression ability, attention test results, motor skills, family harmony status (FamHarm), sleep quality (SleepQ), monthly household income (MHI), experience of school bullying (SchBull), peer relationship quality (PeerRel), and scores on the Breastfeeding and Family-Centered Care Assessment Scale (ScaleSc).
Statistical Analysis
Data processing was performed using SPSS version 27.0 and R version 4.4.3. The level of agreement among expert opinions was assessed using the coefficient of variation (CV) and Kendall’s coefficient of concordance (KCC). The expert authority coefficient (Cr) was calculated as the average of the judgment foundation coefficient (Ca) and the familiarity coefficient (Cs). SEM, implemented via the lavaan package in R, was employed to assess scale validity. Scale psychometric properties were rigorously evaluated using item-total correlation analysis, CR values, EFA, CFA, and Cronbach’s α coefficient to evaluate content validity, internal consistency, and test reliability, respectively. Categorical data are presented as frequency and percentage, while quantitative data are expressed as mean ± standard deviation (SD). Data visualization was generated using the ggplot2 package. Statistical significance was defined as a P-value < 0.05.
Results
Expert Consultation Results
Fifteen questionnaires were distributed for each of the two rounds of expert consultation, achieving a 100% response rate in both instances. During the first consultation round, experts raised concerns regarding item 11 (“Family members are always busy and have no time to accompany the child”), questioning its relevance as it appeared negatively correlated with the overall scale score. Consequently, this item was removed based on expert consensus, resulting in a refined scale comprising 32 items. The second consultation round elicited positive engagement and high levels of active participation from the experts. The Cr for the first round was 0.82; following the deletion of item 11, the Cr increased significantly to 0.9375, with both values exceeding the acceptable threshold of 0.700. Furthermore, KCC values for the two consultation rounds were 0.625 and 0.564, respectively, both reaching statistical significance (P < 0.001). These results indicate a good level of expert consensus and high reliability of the consultation process.
Interview Results
A total of 20 questionnaires were distributed, with all 20 returned questionnaires deemed valid, yielding a 100% valid response rate. Concurrently, patient feedback received during the interview process highlighted the need for enhanced clarity regarding specific terminology. Consequently, supplementary explanations were incorporated for certain terms; for instance, the descriptor “common trauma” was elaborated to include specific examples such as “abrasions, minor burns, etc.”.
Item Analysis Results
A preliminary survey distributed 30 questionnaires, yielding 30 valid responses with an effective response rate of 98.86%, indicating high patient engagement. Results from the CR analysis, performed on the subsequently analyzed dataset comprising 87 questionnaires, demonstrated strong discriminatory power for all scale items. The t-values comparing the low-scoring group to the high-scoring group ranged from −10.781 to −25.954 for individual items (all P < 0.001), while the CR values fell between 11.65 and 13.26. These statistically robust findings confirm that all items possess excellent discriminatory ability, warranting no item deletion. Furthermore, the correlation coefficients between each individual item and the total scale score ranged from 0.549 to 0.842 (all P < 0.001), signifying a high level of internal consistency for every item within the scale. This strong internal consistency further supports the retention of all items.
Psychometric Validation
EFA Results
EFA yielded a 5-factor solution for the scale. The KMO measure of sampling adequacy was 0.768, and Bartlett’s test of sphericity was significant (χ2 = 2,476.322), supporting the factorability of the data. Following factor extraction and rotation, the analysis confirmed 5 distinct factors: Factor 1 pertained to breastfeeding practices, Factor 2 encompassed family-centered care operations, Factor 3 reflected family environmental support, Factor 4 represented health education knowledge, and Factor 5 captured psychological care and emotional support. Communalities ranged from 0.579 to 0.956, and the cumulative variance explained by these five factors reached 75.454%, indicating that the solution effectively accounted for a substantial proportion of the variance within the scale. Consistent with standard criteria for factor loading retention (loading ≥ 0.5), items 25, 32, 10, 24, and 26 were removed due to loadings below this threshold. The retained items demonstrated high loading values onto their respective primary factors, aligning well with the scale’s original conceptual framework and demonstrating good structural validity (Table 3).
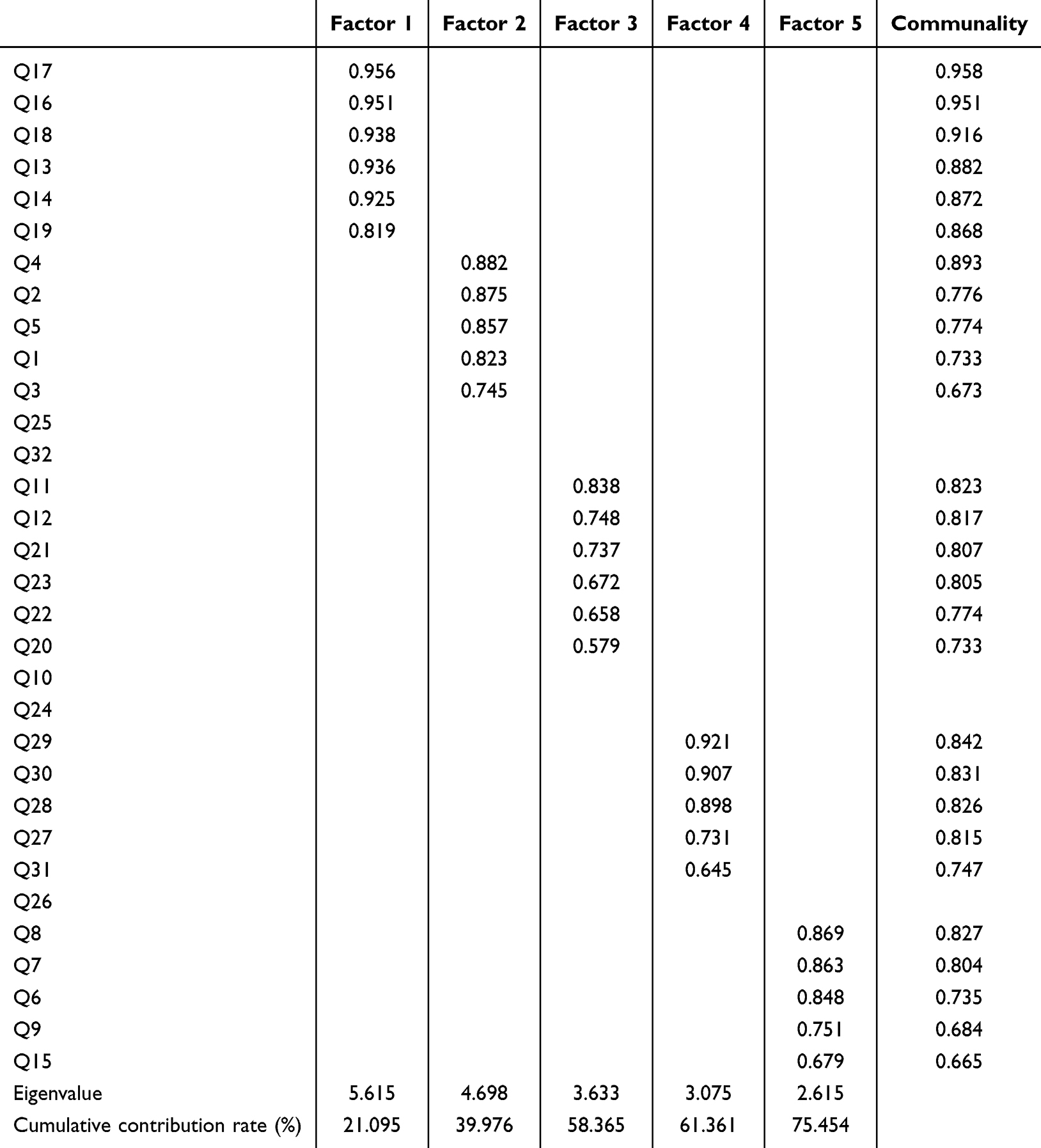 |
Table 3 Exploratory Factor Analysis Results |
Model Fit Indices
The CFA demonstrated excellent fit for the questionnaire’s factor structure, meeting established criteria for good model fit (Table 4). The standardized parameter estimates for the final model are presented in Figure 1.
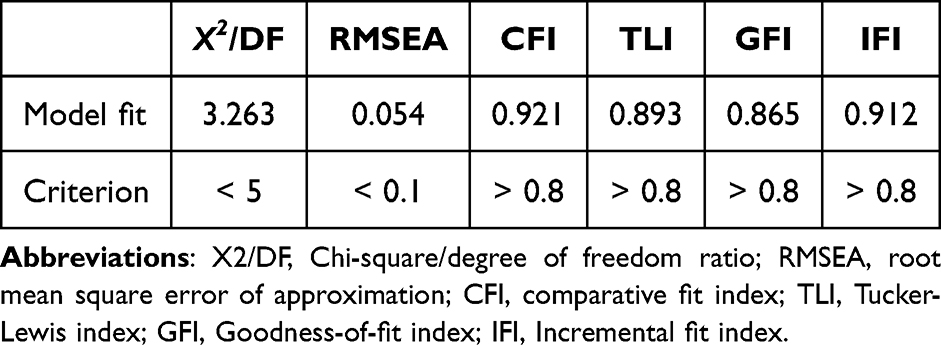 |
Table 4 Global Fit Indices for the Confirmatory Factor Analysis Model |
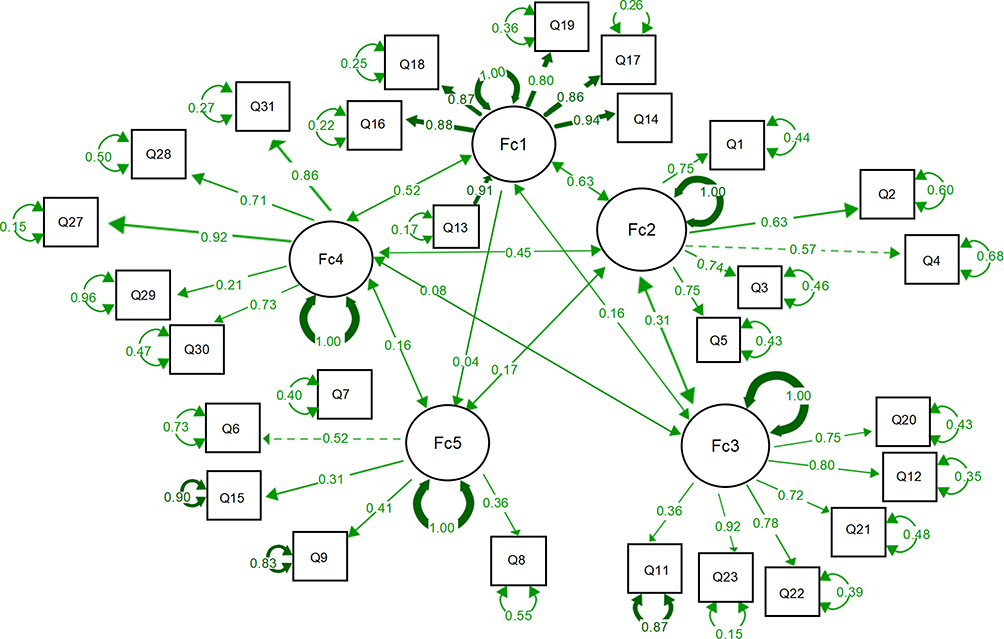 |
Figure 1 Standardized model fit paths. |
Convergent Validity
Convergent validity analysis revealed robust psychometric properties for the scale. The standardized factor loadings for all retained items ranged from 0.692 to 0.975. Furthermore, the CR values for all five dimensions exceeded the recommended threshold of 0.70, and the AVE values for each dimension were all greater than the established benchmark of 0.50. These results collectively demonstrate strong convergent validity for the scale, confirming that items within each dimension effectively measure their intended underlying construct (Table 5).
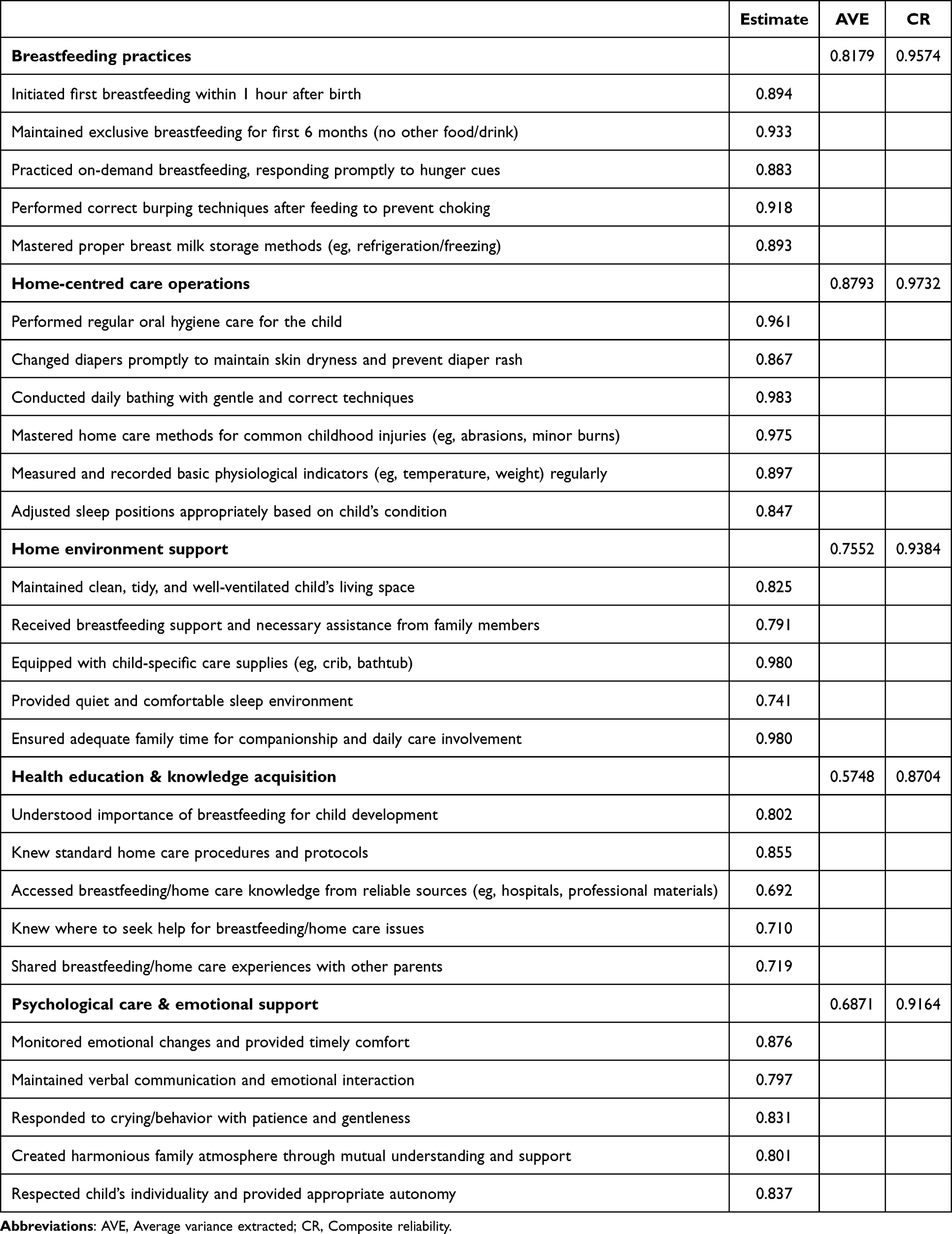 |
Table 5 Convergent Validity Analysis Results |
Discriminant Validity
Assessment of discriminant validity demonstrated that the square roots of the AVE for all five dimensions exceeded the inter-construct correlation coefficients presented in the matrix (Table 6). This finding indicates that each dimension shares more variance with its own indicators than with the other constructs within the scale. Consequently, the five dimensions are empirically distinct, and the scale demonstrates robust discriminant validity, confirming that the constructs measure conceptually different aspects of breastfeeding and family nursing care.
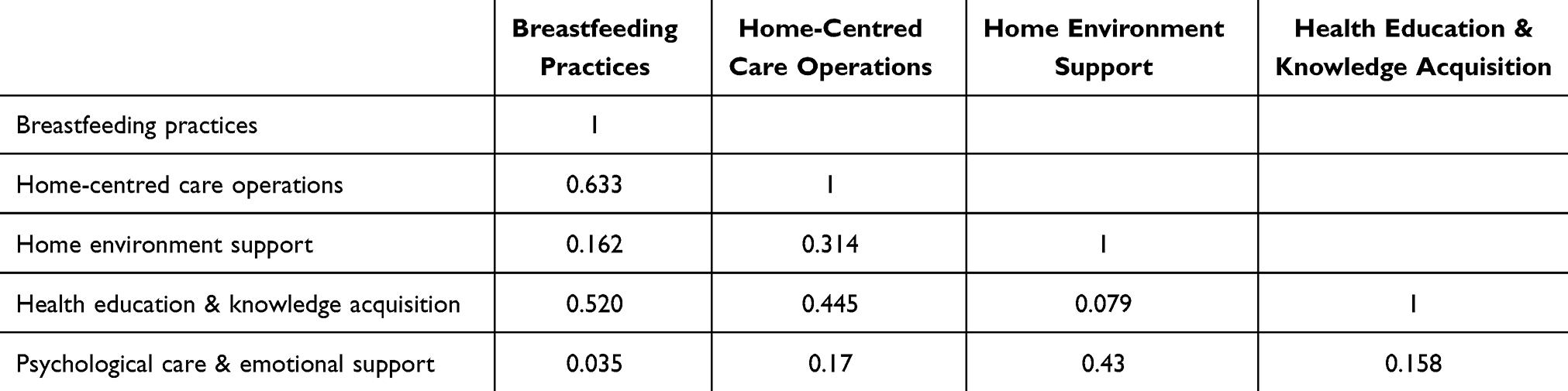 |
Table 6 Discriminant Validity Analysis Results |
Content Validity
The assessment of content validity, based on ratings of item importance provided by the panel of 15 domain experts, yielded excellent results. The I-CVI values ranged from 0.875 to 1.00 across all scale items, while the S-CVI reached 0.9687, demonstrating strong content validity for the scale.
Reliability Analysis
The scale demonstrated robust reliability across all assessment metrics. Cronbach’s α coefficients for the four individual dimensions and the overall scale all exceeded 0.70, indicating high internal consistency. Similarly, the test-retest reliability coefficients for the dimensions and total scale were also consistently greater than 0.70, confirming excellent temporal stability. Additionally, the Guttman split-half coefficient was 0.875. All reported reliability coefficients achieved statistical significance (P < 0.001), solidifying the scale’s measurement stability (Table 7).
 |
Table 7 Reliability Analysis Results |
Modeling of Patient Clinical Characteristics
Significant differences emerged between the two patient groups across key clinical characteristics following statistical modeling. Specifically, variables demonstrating statistically significant differences (P < 0.05) included FamHarm, SleepQ, MHI, SchBull, PeerRel, and ScaleSc scores. These findings indicate distinct clinical profiles between the groups for these parameters (Table 2).
Development of Logistic Regression Model
Variables demonstrating significant differences between groups were incorporated into a multivariate binary logistic regression analysis. Categorical predictors were coded as follows: Harmonious FamHarm, good SleepQ, absence of SchBull, and good PeerRel were assigned a value of 0, with all other states coded as 1. MHI was categorized ordinally: < 3,000 (coded 0), ≥ 3,000 but < 10,000 (coded 1), and ≥ 10,000 (coded 2). The regression analysis identified several significant independent predictors of poor child psychological status. Specifically, FamHarm, SleepQ, SchBull, and PeerRel emerged as significant risk factors. Conversely, higher ScaleSc scores acted as a significant protective factor against poor psychological status. Notably, the odds ratio (OR) for SchBull was 43.982, indicating that exposure to bullying was associated with a substantially increased risk, corresponding to a 43.982-fold higher adjusted odds of poor psychological status compared to non-exposed children. Complete results for all variables in the final model are detailed in Table 8.
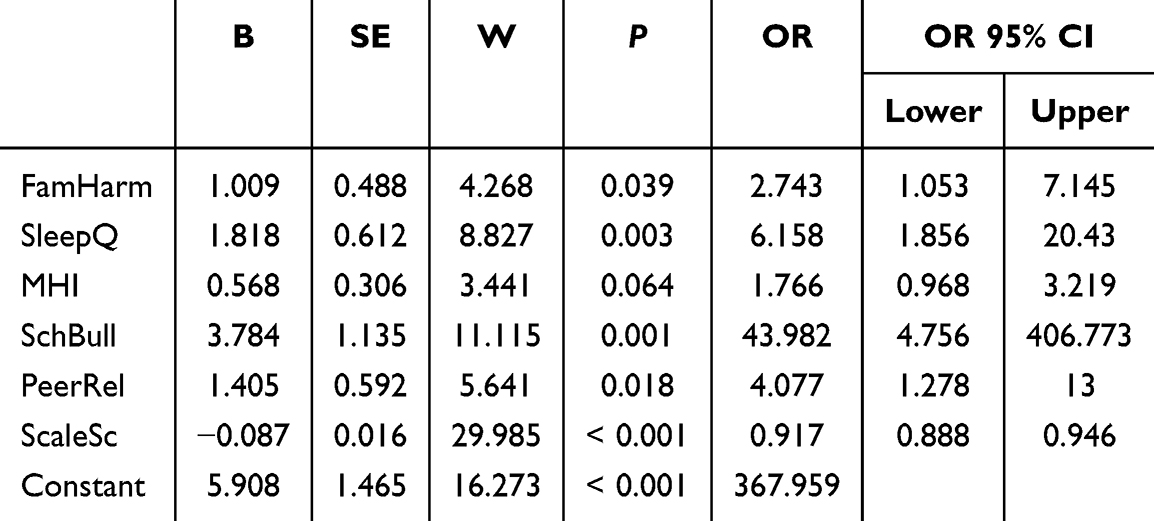 |
Table 8 Results of Multivariate Binary Logistic Regression Analysis |
Development of SVM Model
To validate the impact of clinical characteristics on child psychological status, the dataset was analyzed using a SVM algorithm. Visual representation of feature distributions across the two groups is provided in Figure 2A, facilitating intuitive comparison of central tendencies and dispersion patterns for each variable. Feature importance was rigorously evaluated through multiple methods. Figure 2B illustrates the results of permutation feature importance (PFI) analysis, identifying the ScaleSc score as the most influential predictor within the SVM model. Complementing this, Figure 2C presents random forest (RF)-based importance assessments, utilizing both mean decrease in accuracy (MDA; left panel) to quantify the average reduction in out-of-bag (OOB) accuracy when a feature is randomly permuted, and mean decrease in Gini impurity (MDG; right panel) to reflect the feature’s contribution to node purity. Consistent with the PFI results, both RF-based metrics (MDA and MDG) confirmed ScaleSc as the paramount predictive feature. Model hyperparameter tuning (HPO) outcomes are depicted in Figure 2D, demonstrating optimal SVM performance (ROC = 0.927) achieved at sigma = 0.01 and cost = 0.1. The learning curve in Figure 2E shows converging and stabilized performance metrics on both training and test sets with increasing sample size, indicating absence of overfitting or underfitting. Decision boundary visualizations (Figures 2F and G) further illustrate the model’s effective classification capability. Finally, the ROC curve analysis (Figure 2H) yielded an area under the curve (AUC) of 0.951, collectively demonstrating robust overall performance of the optimized SVM model, as seen in Figure 2.
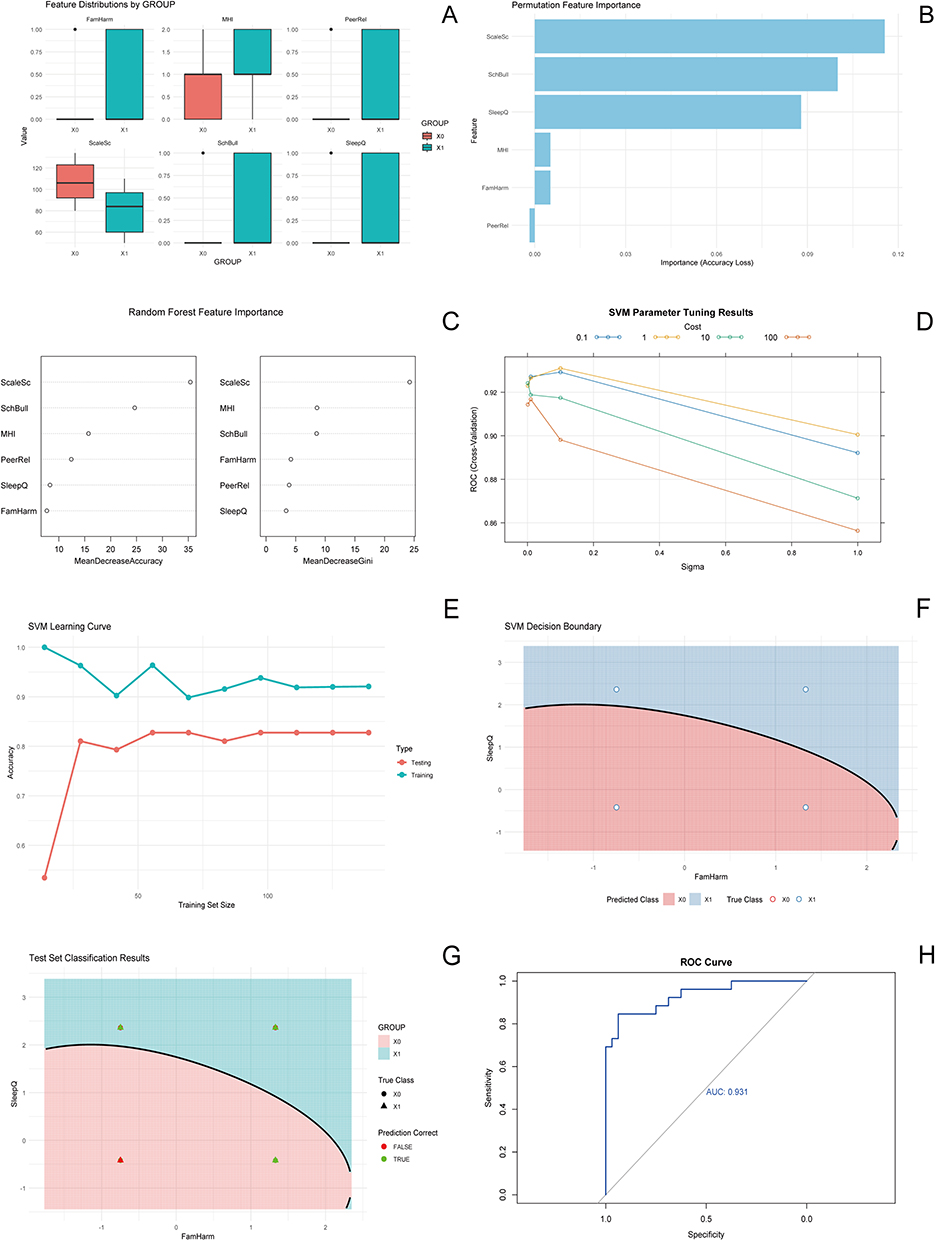 |
Figure 2 SVM model analysis. Notes: (A) Feature distributions by GROUP; (B) Permutation feature importance; (C) Random forest feature importance; (D) SVM parameter tuning results; (E) SVM learning curve; (F) SVM decision boundary; (G) Test set classification results, (H) ROC Curve. X0, Control group; X1, Study group. |
Decision Tree Model
The decision tree algorithm employed the ScaleSc score as its primary split, partitioning cases based on whether the value was ≥ 79 or < 79. For instances where ScaleSc ≥ 79, subsequent branching occurred based on the following hierarchical criteria: absence or presence of SchBull (0 or 1), MHI (given the established ordinal coding: 0, 1, 2), and further stratification using ScaleSc thresholds (eg, ≥ 107). Cases entering the ScaleSc < 79 branch proceeded directly to a terminal node for classification. Each terminal node assigns the final class prediction based on the majority class prevalence within that node, thereby determining the predicted psychological status category for the sample (Figure 3).
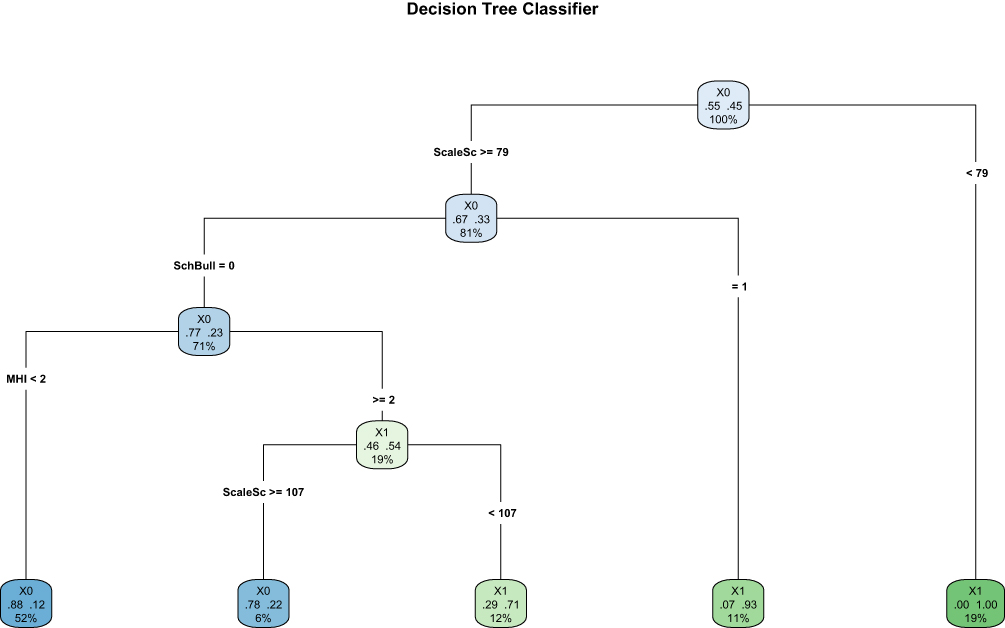 |
Figure 3 Decision tree classifier. |
Discussion
Childhood represents a critical period for psychological development, and suboptimal psychological status during this phase carries significant multifaceted risks. At the individual level, compromised mental well-being can manifest as diminished learning capacity, impaired concentration, and reduced memory function, thereby hindering knowledge acquisition and skill mastery, ultimately impeding academic progression.17 Within social contexts, children experiencing psychological difficulties frequently encounter substantial challenges in establishing and maintaining healthy interpersonal relationships. This may present as social withdrawal, aggression, or avoidant behaviors, significantly impairing the development of essential social skills and the formation of robust emotional support networks.18 From a long-term perspective, persistent adverse psychological states substantially elevate the risk of developing psychiatric disorders in adulthood, including anxiety and depressive disorders.17 Despite the recognized importance of early influences, research systematically quantifying the impact of specific modifiable factors on child psychological outcomes remains limited. Crucially, the substantial contributions of breastfeeding, a cornerstone of early nutrition and emotional bonding19 and the nurturing environment fostered by family-centered care on psychological development have not been systematically quantified through validated instruments. Consequently, the development of the ScaleSc utilizing the Delphi method, and the subsequent rigorous investigation of its predictive utility for child psychological status, constitutes a necessary and valuable endeavor. This facilitates the precise identification of key modifiable determinants, provides a robust scientific foundation for targeted early intervention and prevention strategies, and significantly contributes to the promotion of child mental health, thereby holding considerable theoretical and practical significance.
The present study employed a meticulous development process for the ScaleSc, commencing with an extensive literature review to establish a comprehensive preliminary item pool ensuring broad content coverage. This initial pool underwent iterative refinement and revision through structured expert consultation rounds and targeted patient interviews. The Cr for the initial consultation round was 0.82; subsequent deletion of items demonstrating poor correlation with the overall scale significantly elevated the Cr to 0.9375. The panel comprised 15 highly qualified experts recruited from four distinct provinces/municipalities across China, representing diverse yet critical fields including medicine, nursing, and psychology. Their recognized expertise and authoritative standing within their respective disciplines provided robust professional validation, ensuring the ScaleSc’s content validity and clinical relevance. Following initial scale formulation, cognitive interviews were conducted with 35 patients to rigorously assess readability, comprehensibility, and face validity, confirming that respondents could interpret items clearly and provide accurate responses. During the psychometric validation phase, sample size determination adhered strictly to established scientific principles, ensuring adequate statistical power for robust evaluation of the scale’s properties. Collectively, this rigorous multi-stage methodology underpins the ScaleSc’s capacity for precise assessment of breastfeeding practices and family-centered care effectiveness.
Psychometric evaluation confirmed the ScaleSc’s robust validity and reliability. Validity, encompassing CVI, structural validity, discriminant validity, and convergent validity, was comprehensively established. All CR values significantly exceeded the threshold of 3.0, and all Pearson correlation coefficients surpassed 0.4, providing strong evidence for the sound distribution and relevance of all retained scale items. The integrated methodological approach, incorporating literature synthesis, Delphi consultation, pilot testing, and comprehensive psychometric analysis, affirmed the scale’s internal homogeneity. EFA was employed to elucidate the optimal factor structure, supplemented by an “item deletion procedure” to enhance parsimony, ultimately yielding a refined scale comprising 27 items distributed across five coherent dimensions. The EFA solution demonstrated excellent concordance with the scale’s original conceptual framework, confirming its robust structural validity. Standardized factor loadings ranged from 0.692 to 0.983, indicating appropriate item grouping within each dimension. CFA further validated the structure, with the RMSEA < 0.08, satisfying established criteria for excellent model fit. Regarding reliability, Cronbach’s α coefficients for all five dimensions exceeded 0.80, indicating strong internal consistency.
Following its rigorous validation, the ScaleSc was integrated into multivariate analyses examining predictors of poor child psychological status. Multivariate binary logistic regression identified higher ScaleSc scores as a significant protective factor against adverse psychological outcomes, confirming its positive orientation (ie, higher scores indicate more favorable breastfeeding/family-centered care practices, associated with better psychological status). Notably, exposure to SchBull emerged as a potent risk factor, exhibiting a substantial OR of 43.982. This profound impact of bullying stems from multifaceted detrimental pathways. Psychologically, bullying inflicts enduring trauma, fostering chronic fear, pervasive insecurity, and profound helplessness or hopelessness, thereby eroding resilience and significantly increasing vulnerability to depression and anxiety disorders.20 At the level of self-perception, denigrating and humiliating bullying severely damages self-esteem, diminishes self-efficacy, fosters negative self-schemata, and undermines confidence and identity formation.21 Concurrently, the pervasive fear of bullying often compels social avoidance, precipitating social skill deficits and impairing the child’s capacity to engage in and learn from normative social interactions, ultimately hindering societal integration. Environmental factors compound these effects: unstable family environments or inadequate parental emotional support and guidance deprive children of crucial coping resources.22 Schools lacking effective anti-bullying policies and supportive climates leave victims isolated and unprotected, allowing bullying behaviors to proliferate. These interconnected mechanisms collectively inflict profound psychological harm from multiple angles, underscoring the critical urgency and paramount importance of implementing comprehensive strategies to prevent and intervene against school bullying to safeguard child mental health.23
The preeminent predictive strength of the ScaleSc, as evidenced by its dominance in the SVM and decision tree models, can be interpreted through a bio-psycho-social lens that elucidates the profound mechanisms linking breastfeeding and family-centered care to psychological development. From a biological standpoint, breastfeeding is not merely a source of nutrition but a potent regulator of the infant’s stress response system.24 The act of breastfeeding facilitates skin-to-skin contact, mutual gaze, and nurturing touch, which have been shown to reduce infant cortisol levels and promote the release of oxytocin.25 This neurobiological calibration in early life provides a stable foundation for emotional security and is hypothesized to foster long-term resilience to stress, a core component of psychological health. Psychologically, both breastfeeding and family-centered care co-create a secure attachment base. The consistent, responsive caregiving quantified by the ScaleSc—whether through feeding on demand or through sensitive responses to a child’s distress—teaches the child that the world is predictable and that they are worthy of care. This internal working model is fundamental to the development of healthy self-concept, emotion regulation skills, and the capacity to form trusting relationships later in life26 The ScaleSc effectively captures these dyadic and familial interaction patterns that are crucial for forging a resilient psyche. Socially, a family-centered environment rich in positive communication and engagement provides the primary “training ground” for social competence. Children learn to interpret social cues, manage conflicts, and express emotions within the safety of the family unit. The ScaleSc items pertaining to family interactions likely tap into this critical social-learning process. Therefore, the ScaleSc operates as a unifying metric that quantifies these interconnected biological, psychological, and social pathways, thereby explaining its superior utility in predicting a child’s psychological status.
The robust psychometric properties of the ScaleSc suggest its potential utility beyond the Chinese context in which it was developed, given the universal importance of its core care constructs. However, cultural specificity in certain items (eg, those on family roles) must be examined. Cross-cultural validation is needed to establish linguistic and conceptual equivalence, transforming the ScaleSc into a tool for global comparative research.
In summary, this research successfully developed and rigorously validated the ScaleSc, demonstrating its significant clinical utility and predictive accuracy for assessing child psychological status. However, several methodological limitations warrant careful consideration. Firstly, the geographical and cultural diversity of the participant sample may be insufficient, introducing potential selection bias and limiting the generalizability of the findings across diverse regions and cultural contexts, thereby potentially restricting extrapolation to broader populations. Secondly, while the ScaleSc was meticulously constructed using the Delphi method, it is conceivable that certain critical facets of breastfeeding and family-centered care influencing child psychology may not be fully encapsulated by the current item set, potentially introducing measurement error and impacting the comprehensiveness and precision of assessments. Thirdly, the study primarily focused on the associations between breastfeeding/family-centered care and psychological status, without comprehensively accounting for other potentially significant confounding variables (eg, socioeconomic status, neighborhood environment, genetic predispositions), which may lead to overestimation or underestimation of the core relationships examined. Finally, the cross-sectional or retrospective design inherently precludes definitive conclusions regarding causality between the measured variables. Furthermore, the absence of longitudinal follow-up data impedes a comprehensive understanding of the dynamic trajectory and long-term effects of breastfeeding and family-centered care on psychological development throughout childhood and adolescence. Future research addressing these limitations will be essential to further refine the scale and elucidate the complex interplay of factors influencing child mental health.
Conclusion
This study successfully developed and validated the ScaleSc as a reliable and robust tool. We demonstrated that a higher ScaleSc score is a significant protective factor for child psychological health, establishing its value in quantifying the positive impact of breastfeeding and family-centered care. Its role as a key predictor in computational models underscores the clinical utility of the ScaleSc. These findings support the application of the ScaleSc as a practical tool for early identification of children at risk for psychological difficulties, thereby facilitating timely and targeted interventions. While the ScaleSc shows great promise, the cross-sectional design and regional sample of this study limit causal inference and generalizability. Future longitudinal studies across diverse populations are essential to confirm these findings, establish causality, and validate the universal predictive power of the ScaleSc.
Data Sharing Statement
The data used and/or analyzed during the current study are available from the corresponding author.
Ethics Approval and Consent to Participate Declarations
The study protocol was approved by the Ethics Committee of South China Hospital, Medical School, Shenzhen University (approval number: HNLS20250725001-A), with written informed consent obtained from all legal guardians.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Winston R, Chicot R. The importance of early bonding on the long-term mental health and resilience of children. London J Prim Care. 2016;8(1):12–14. doi:10.1080/17571472.2015.1133012
2. Jiao WY, Wang LN, Liu J, et al. Behavioral and emotional disorders in children during the COVID-19 epidemic. J Pediatr. 2020;221(264–266):e261. doi:10.1016/j.jpeds.2020.03.013
3. Remschmidt H, Belfer M. Mental health care for children and adolescents worldwide: a review. World Psychiatry. 2005;4(3):147–153.
4. Prentice AM. Breastfeeding in the modern world. Ann Nutr Metab. 2022;78(Suppl 2):29–38. doi:10.1159/000524354
5. Behere AP, Basnet P, Campbell P. Effects of family structure on mental health of children: a preliminary study. Indian J Psychol Med. 2017;39(4):457–463. doi:10.4103/0253-7176.211767
6. Brockway ML. Effect of Alberta family integrated care (FICare) on breastfeeding self-efficacy and breastmilk feeding in moderate and late preterm infants. Univ Calgary. 2019.
7. Shang Z. Use of Delphi in health sciences research: a narrative review. Medicine. 2023;102(7):e32829. doi:10.1097/MD.0000000000032829
8. Amirrudin M, Nasution K, Supahar S. Effect of variability on Cronbach alpha reliability in research practice. Jurnal Matematika Statistika dan Komputasi. 2021;17(2):223–230. doi:10.20956/jmsk.v17i2.11655
9. Sun HJ, Wu MT, Qu J, et al. Development and validation of the out-of-hospital adherence questionnaire for stroke patients (OHAQ-SP). BMC Neurol. 2024;24(1):460. doi:10.1186/s12883-024-03962-z
10. Tobón S, Luna Nemecio J. Complex thinking and sustainable social development: validity and reliability of the COMPLEX-21 scale. Sustainability. 2021;13(12):6591. doi:10.3390/su13126591
11. Mata-López WA, Juárez-Hernández LG, Tobón S, Montesinos-López OA. Analysis of construct validity and reliability of two instruments to evaluate professional oriented activities. Revista Española de Orientación y Psicopedagogía. 2021;32(2):47–68. doi:10.5944/reop.vol.32.num.2.2021.31278
12. Jiang Z, Wang D, Xu H, et al. Diagnostic efficiency and psychometric properties of CBCL DSM-oriented scales in a large sample of Chinese school-attending students aged 5-16. Asian J Psychiatr. 2023;88(103724):103724. doi:10.1016/j.ajp.2023.103724
13. Uspst F, Mangione CM, Barry MJ, et al. Screening for anxiety in children and adolescents: US preventive services task force recommendation statement. JAMA. 2022;328(14):1438–1444. doi:10.1001/jama.2022.16936
14. Yu W, Zhang ZZ. Age-based grouping criteria in medicine. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2023;45(2):285–289. doi:10.3881/j.issn.1000-503X.15133
15. Panda PK, Gupta J, Chowdhury SR, et al. Psychological and behavioral impact of lockdown and quarantine measures for COVID-19 pandemic on children, adolescents and caregivers: a systematic review and meta-analysis. J Trop Pediatr. 2021;67(1). doi:10.1093/tropej/fmaa122
16. Okuyama J, Seto S, Fukuda Y, et al. Mental health and physical activity among children and adolescents during the COVID-19 pandemic. Tohoku J Exp Med. 2021;253(3):203–215. doi:10.1620/tjem.253.203
17. Hampton-Anderson JN, Carter S, Fani N, et al. Adverse childhood experiences in African Americans: framework, practice, and policy. Am Psychol. 2021;76(2):314–325. doi:10.1037/amp0000767
18. Saracho ON. Theories of child development and their impact on early childhood education and care. Early Childhood Educ J. 2023;51(1):15–30. doi:10.1007/s10643-021-01271-5
19. Modak A, Ronghe V, Gomase KP. The psychological benefits of breastfeeding: fostering maternal well-being and child development. Cureus. 2023;15(10):e46730. doi:10.7759/cureus.46730
20. Luo X, Zheng R, Xiao P, et al. Relationship between school bullying and mental health status of adolescent students in China: A nationwide cross-sectional study. Asian J Psychiatr. 2022;70(103043):103043. doi:10.1016/j.ajp.2022.103043
21. Eyuboglu M, Eyuboglu D, Pala SC, et al. Traditional school bullying and cyberbullying: prevalence, the effect on mental health problems and self-harm behavior. Psychiatry Res. 2021;297(113730):113730. doi:10.1016/j.psychres.2021.113730
22. Ahmed GK, Metwaly NA, Elbeh K, et al. Risk factors of school bullying and its relationship with psychiatric comorbidities: a literature review. Egyptian J Neurol Psychiatry Neurosurg. 2022;58(1):16. doi:10.1186/s41983-022-00449-x
23. Norman JO, Berger C, Yoneyama S, et al. School bullying: moving beyond a single school response to a whole education approach. Pastoral Care Educ. 2022;40(3):328–341. doi:10.1080/02643944.2022.2095419
24. Vilar-Compte M, Hernandez-Cordero S, Ancira-Moreno M, et al. Breastfeeding at the workplace: a systematic review of interventions to improve workplace environments to facilitate breastfeeding among working women. Int J Equity Health. 2021;20(1):110. doi:10.1186/s12939-021-01432-3
25. Tucker Z, O’Malley C. Mental health benefits of breastfeeding: a literature review. Cureus. 2022;14(9):e29199. doi:10.7759/cureus.29199
26. Kadir NA, Razman MA, Marhaban SM. Family-based care in child protection: a literature review. Al-Kashaf. 2024;4(03):78–90.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.