Back to Journals » Clinical Ophthalmology » Volume 17
Assessing Agreement and Variability Among Alternative Devices for Intraocular Pressure Measurement: A Comparative Study
Authors Lin CW ![]() , Wang JJ, Lai CH, Chen CY
, Wang JJ, Lai CH, Chen CY ![]() , Lai IC
, Lai IC
Received 2 September 2023
Accepted for publication 1 November 2023
Published 15 November 2023 Volume 2023:17 Pages 3453—3461
DOI https://doi.org/10.2147/OPTH.S438358
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Chen-Wei Lin,1,2,* Jin-Jhe Wang,2,* Chien-Hsiung Lai,2– 5 Chau-Yin Chen,2,3 Ing-Chou Lai2,3,6
1Department of Medical Education, Chang Gung Memorial Hospital, Chiayi, 61363, Taiwan; 2Department of Ophthalmology, Chang Gung Memorial Hospital, Chiayi, 61363, Taiwan; 3Department of Medicine, Chang Gung University, Taoyuan, 33302, Taiwan; 4Department of Nursing, Chang Gung University of Science and Technology, Chiayi, 61363, Taiwan; 5School of Traditional Chinese Medicine, College of Medicine, Chang Gung University, Taoyuan, 33302, Taiwan; 6Department of Ophthalmology, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, 83301, Taiwan
*These authors contributed equally to this work
Correspondence: Jin-Jhe Wang, Department of Ophthalmology, Chiayi Chang Gung Memorial Hospital, No. 8, Sec. W., Jiapu Road, Puzi City, Chiayi County, 613, Taiwan, Tel +886 5 3621000, Fax +886 5 3623002, Email [email protected]
Purpose: Intraocular pressure (IOP) measurement is critical in diagnosing and managing eye conditions. This study aims to assess the comparability of three alternative devices for measuring IOP: Noncontact tonometer, Icare rebound tonometer, and Tono-Pen.
Patients and Methods: A cross-sectional study included 172 adult participants (87 males and 85 females) who underwent IOP and central corneal thickness (CCT) assessments. IOP was measured using Noncontact (Canon TX-20), Icare (Icare TA01i), and Tono-Pen (Tonopen XL). CCT was measured with the built-in pachymetry of the Noncontact tonometer. Correlation coefficients and Bland-Altman analyses were conducted to assess the relationships and agreements between these tonometers. Participants were grouped based on IOP and CCT levels. The mean of the standard deviation of the three tonometer results was calculated to evaluate measurement result variability. One-way analysis of variance was conducted for comparing between the groups.
Results: IOP measurements among the three devices were not significantly different, indicating their comparability. Correlation analysis revealed strong correlations between the tonometers. Bland-Altman analysis showed good agreement, with the Icare rebound tonometer and Tono-Pen exhibiting narrower limits of agreement. Furthermore, IOP levels influenced measurement result variability, with higher IOP levels associated with greater variance.
Conclusion: This study demonstrates that the alternative devices examined can provide reliable IOP measurements. It highlights the potential of these alternative devices for IOP measurement. These findings have implications for clinical practice, offering practitioners additional tools for accurate IOP assessment.
Keywords: intraocular pressure, tonometer, noncontact, icare, Tono-Pen
Introduction
Intraocular pressure (IOP) is regarded as one of the vital signs of the eyes. The measurement of IOP is crucial in everyday ophthalmologic practice.1 In the Ocular Hypertension Treatment Study, primary open-angle glaucoma has been shown to be associated with higher IOP.2,3 In the Early Manifest Glaucoma Trial, the importance of IOP control in the management of glaucoma has also been described.4 Accurate measurement is of utmost importance in managing glaucoma patients, as the treatment is based on maintaining optimal IOP levels because abnormally high or low IOP can have detrimental effects on the eyes.5,6 Factors such as central corneal thickness (CCT), corneal power, corneal astigmatism, and prior corneal surgery, need to be considered while measuring IOP.7,8
Goldmann applanation tonometry, widely considered the universal gold standard for measuring IOP, has several drawbacks associated with its clinical use.9 Firstly, the examination necessitates a skilled and experienced ophthalmologist due to its steep learning curve. Secondly, the diagnostic test cannot be utilized to assess patients in a supine position or those who are uncooperative with slit lamp examinations. Thirdly, the test requires the use of fluorescein dye and topical anesthesia. Fourthly, the contact nature of the procedure poses a risk of corneal infection and discomfort for patients. Lastly, the lack of portability and the need for a slit lamp setup render large-scale population screening impractical.10,11
As a result of the aforementioned limitations, several new alternative tools for measuring IOP have emerged to replace Goldmann applanation tonometry. The most popular diagnostic devices used in clinical settings are Noncontact tonometer, Icare rebound tonometer, and Tono-Pen.12,13 Noncontact tonometer utilizes an air pulse to deform the cornea and calculate the IOP, allowing for measurement without direct contact with the eyes. With compact size and portability, Icare rebound tonometer employs the rebounding force of a light probe when striking the cornea to determine the IOP. Tono-Pen combines both applanation and indentation methods and is particularly suitable for evaluating the IOP of uncooperative patients.14
Even though previous studies have presented the agreement between Noncontact tonometer, Icare rebound tonometer, and Tono-Pen with Goldmann applanation tonometry for measuring IOP, the findings of these studies remain inconclusive at present.13–17 In the clinical setting, the second tonometer would be used if the follow-up IOP is significantly different from the previously measured IOP to enhance the reliability of the measurement; however, the agreement between the three alternative devices has yet to be established.17,18 Additionally, based on our knowledge, there is a lack of discussion on the variance in measurement results obtained from these three methods. Therefore, the purpose of this article is to compare the IOP values obtained using Noncontact tonometer, Icare rebound tonometer, and Tono-Pen across a wide range of IOP levels and different corneal thickness levels, and to assess the agreement among these three IOP measurement tools.
Materials and Methods
Study Participants
This was a cross-sectional study that enrolled adults aged range from 18 to 88 years old. A total of 172 participants (87 males and 85 females) who came for routine ophthalmology inspection at the ophthalmology outpatient department of Chiayi Chang Gung Memorial Hospital, a regional teaching hospital in southern Taiwan, were recruited in 2022. The subjects with corneal edema, central corneal opacities, >3-dimensional corneal astigmatism, nystagmus, ocular infection, ocular trauma, cornea with contact lens, keratoconus, any history of laser or intraocular surgery within the past three months were excluded from the study. This study was approved by the Medical Ethics Committee of Chang Gung Memorial Hospital (institutional review board numbers: 202001816B0), and the study protocol followed the principles outlined in the Declaration of Helsinki. All subjects received comprehensive information regarding the study’s specifics and provided signed informed consent before their inclusion.
Study Design
All participants underwent thorough ophthalmologic examinations on the same day in the following sequence. First, IOP was measured in a sitting position in the sequence of Noncontact (Canon TX-20, Canon, Tokyo, Japan), Icare (Icare TA01i, Icare Finland Oy, Helsinki, Finland), and Tono-Pen (Tonopen XL, Reichert Technologies, Depew, NY). The instruments were all calibrated based on the manufacturers’ instructions before measurement. An interval of 10 minutes was set between each IOP measurement device to decrease the interference of sequential measurements and enhance accuracy.9 Second, the CCT measurement was performed with the built-in pachymetry of the Noncontact tonometer.
During Noncontact measurement, three consecutive measurements on each eye were performed. Each measurement difference should be less than two mmHg. If not, the result would be discarded, and another measurement would continue being conducted. The average of the three results were used for data analysis. The measurement of Icare was conducted using a probe inserted into the device and positioned perpendicularly to the central cornea, with an alignment of 4–8mm. A total of six consecutive measurements were conducted. The software automatically disregarded the highest and lowest values, and the IOP was determined based on the remaining four measurements. For Tono-Pen measurement, the participants were instilled with one drop of Proparacaine 0.5% ophthalmic solution in each eye. Each eye was tapped with the measuring probe on the central cornea repeatedly for six times and the result was automatically shown. To enhance the accuracy of the measurement, we repeated the measurement of Icare and Tono-pen twice. If the results were within two mmHg, the final IOP would be recorded as the average of the two measurement results. If the difference between the two measurement results was larger than two mmHg, the third measurement would be conducted. The average of the closer two results were recorded. The IOP value should be between 7 to 50 mmHg according to the instruction manuals of the devices; otherwise, the results were discarded.
In this study, we measured the IOP and CCT of both eyes of each patient, the right eye first followed by the left eye. The subjects were divided into three groups according to the IOP measured by Noncontact tonometer: low IOP group (7 mmHg ≤ IOP < 10 mmHg), normal IOP group (10 mmHg ≤ IOP <21mmHg), and high IOP group (21 mmHg ≤ IOP ≤50 mmHg). Another grouping was based on CCT, with thin CCT group (CCT ≤ 550 μm), medium CCT group (550 μm < CCT ≤ 573 μm), and thick CCT group (CCT > 573 μm). The groups were divided according to the tertile of CCT levels.
Statistical Analysis
In this study, continuous variables were presented as means with standard deviations, while categorical variables were expressed as numbers and percentages of observations. Pearson correlation and linear regression tests were performed to evaluate the three IOP measurement devices. The interpretation of the Pearson correlation coefficient (r) is as follows: a value of 0–0.2, 0.2–0.4, 0.4–0.6, 0.6–0.8, 0.8–1.0, indicating a very weak (or no correlation), weak, moderate, strong, and very strong correlation, respectively. For comparing groups larger than three, the one-way analysis of variance was conducted. Bland-Altman analysis was used to determine the agreement between the IOP measurements by three instruments. All statistical analyses were two-sided, and the null hypothesis was rejected at a 95% confidence interval. The statistical analysis was performed using the Statistical Program for Social Sciences (SPSS) version 26 (IBM Corporation, Armonk, NY, USA) and Python version 3.10.
Results
In this study, 172 subjects were recruited with a mean age of 58.74±14.25 years old (range: 18–88). Among these participants, 87 were males and 85 were females. The baseline demographics are shown in Table 1. The IOP measured by Noncontact tonometer, Icare rebound tonometer, and Tono-Pen were 15.23±4.37 mmHg (range: 7.1–42.9), 14.53±4.88 mmHg (range: 7–42), and 14.92±3.68 mmHg (range: 7–35), respectively (Table 1). No significant difference was noted between the three IOP measurement methods (p = 0.11). The mean central corneal thickness was 561.69±32.85 μm. The distribution of the IOP measurement of the three tools is presented in Figure 1.
 |
Table 1 Baseline Demographics and Mean IOP of the Study Population |
 |
Figure 1 Distribution plots of intraocular pressure measured by different tonometers. Abbreviation: IOP, intraocular pressure. |
The correlation analysis is illustrated in Figure 2. The correlation coefficients of Noncontact tonometer and Icare rebound tonometer, Noncontact tonometer and Tono-Pen, and Icare rebound tonometer and Tono-Pen, were r = 0.785, r = 0.749, and r = 0.829, respectively. The agreement between the three IOP measurement devices is shown in Figure 3 as Bland-Altman plots. The Bland-Altman plots did not reveal any significant evidence of heteroscedasticity for any index tests, which means the variability is equal across the range of mean errors. Furthermore, the plots displayed narrower 95% limits of agreement for the Icare rebound tonometer and Tono-Pen compared to the other two index tests.
 |
Figure 2 Scatter plots and linear regression lines between two of the three tonometers. |
 |
Figure 3 Bland-Altman plots between two of the three tonometers. |
We further divided the patients into three different IOP subgroups. The mean of the standard deviation of the three results measured by different tonometers at varying levels of intraocular pressure was calculated, showing 1.76±1.03, 1.71±0.93, and 2.81±1.90 in the low, normal, and high IOP groups, respectively. The high IOP group had a significantly higher mean of the standard deviation of the three results by post hoc analysis (p<0.001). The result is manifested in Figure 4.
 |
Figure 4 A bar chart showing the mean of the standard deviation of the three values measured by different tonometers at different levels of intraocular pressure (p<0.001). Low IOP group (7 mmHg ≤ IOP < 10 mmHg), normal IOP group (10 mmHg ≤ IOP <21mmHg), and high IOP group (21 mmHg ≤ IOP ≤50 mmHg). Abbreviation: IOP, intraocular pressure. |
Moreover, to compare the mean of the standard deviation of the three results measured by different tonometers at different levels of corneal thickness, we divided the subjects into three groups according to the tertile of CCT levels. The mean was 1.93±1.07, 1.67±1.10, and 1.76±1.08 in the thin, medium, and thick CCT groups, respectively (p=0.165). The result can be found in Figure 5.
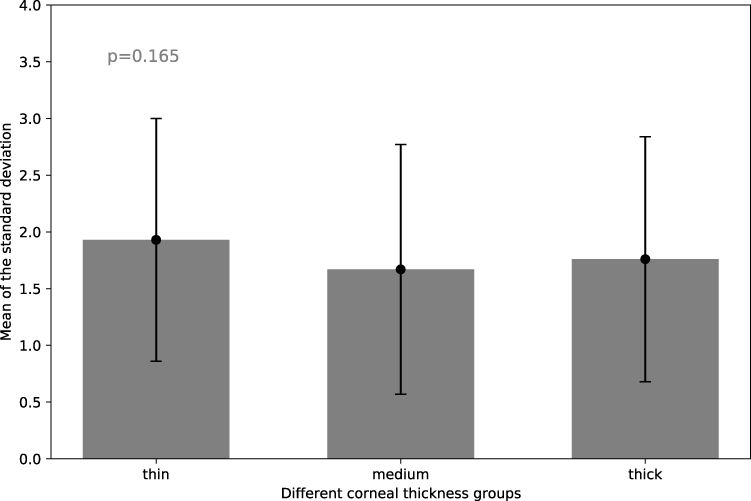 |
Figure 5 A bar chart showing the mean of the standard deviation of the three values measured by different tonometers at different levels of corneal thickness (p=0.165). Thin CCT group (CCT ≤ 550 μm), medium CCT group (550 μm < CCT ≤ 573 μm), and thick CCT group (CCT > 573 μm). Abbreviation: CCT, central corneal thickness. |
Discussion
The presented results indicate that Noncontact tonometer, Icare rebound tonometer, and Tono-Pen can provide reliable measurements of IOP. This suggests that these alternative devices can be valuable tools for IOP measurement in clinical practice, particularly when direct contact or a slit lamp examination may not be feasible or preferred. Although Goldmann applanation tonometry is still recognized as the gold standard for IOP measurement, plenty of situations may occur when the tonometer cannot be used in clinical settings. For example, using Goldmann applanation tonometry takes a longer time to assess the IOP while the Noncontact tonometer can roughly estimate the IOP or screen patients without a past history of glaucoma, making the ophthalmologic visit more efficient and decreasing the chance of eye infection by avoiding direct contact with the cornea. In addition, using Goldmann applanation tonometry is a complex technique to operate by experienced and skilled ophthalmologists compared to Icare rebound tonometer, which can evaluate the IOP in a simple and fast way, avoid the usage of anesthesia, and prevent potentially dangerous microaerosol spreading.15,19 Furthermore, Goldmann applanation tonometry is useless if the patients cannot comfortably sit in front of the slit lamp. By contrast, Tono-Pen can play a vital role in determining the IOP in intensive care units or emergency department.20
The findings revealed strong correlations among the different tonometers, indicating a good agreement in measuring IOP, which supports the interchangeability of these alternative devices, enabling clinicians to select the most appropriate tool based on patient characteristics, examination conditions, and patient comfort. Furthermore, the narrower limits of agreement observed with the Icare rebound tonometer and Tono-Pen suggest that these devices may offer more consistent and reliable measurements compared to the Noncontact tonometer. This finding has potential benefits in monitoring IOP fluctuations over time and evaluating the effectiveness of treatment in patients with glaucoma. By having multiple reliable options for measuring IOP, clinicians can have greater flexibility and adaptability in clinical practice, tailoring the choice of tonometer to individual patient needs and specific clinical situations.
To our knowledge, prior studies have discussed the reproducibility, comparability, and agreement among different kinds of IOP measurement devices; however, neither investigated the variability of the measurement values by different tools.14,15,17 Therefore, we used the concept of standard deviation to analyze the degree of dispersion of the measurement result of the three tonometers. Our finidings revealed that the standard deviation of the three IOP measurements was significantly higher in the high IOP group compared to the low and normal IOP groups. This suggests that patients with higher IOP levels may exhibit greater variability in IOP measurement results across different devices. Clinicians need to take this into account when interpreting and comparing IOP measurements obtained from different tonometers. However, the study found that corneal thickness did not affect the variability of IOP measurement results. These findings have important implications for clinical practice. When selecting an IOP measurement device, clinicians should consider the individual patient’s IOP level instead of corneal thickness. Patients with high IOP levels may benefit from devices that have demonstrated better agreement with Goldmann applanation tonometry to get a more accurate result. On the other hand, patients with normal or low IOP levels may have more flexibility in the choice of IOP measurement device. Moreover, the variability associated with high IOP levels should be considered when interpreting IOP measurements and making treatment decisions. Clinicians should be cautious when relying solely on a single measurement and consider obtaining multiple measurements or using devices with higher agreement in these specific patient populations. Further research is warranted to understand better the underlying reasons for the observed variability based on IOP levels and corneal thickness. Investigating factors such as biomechanical properties of the cornea and variations in ocular physiology may provide insights into the differences in measurement results. Additionally, evaluating the impact of these variations on glaucoma diagnosis, progression monitoring, and treatment outcomes will be valuable in optimizing patient care.
To acknowledge the limitations of this study is essential. First, the study was conducted on a specific population from a single medical center, which may limit the generalizability of the findings. Additionally, we did not explore other factors that may influence IOP measurement accuracy. Factors such as ocular surface conditions, refractive error, and the presence of other eye diseases could potentially impact the agreement and variability among different tonometers. Investigating these factors would contribute to a more comprehensive understanding of the performance and applicability of these devices in clinical practice. Lastly, the study compared the agreement and variability among Noncontact tonometer, Icare rebound tonometer, and Tono-Pen. The results of Goldmann applanation tonometry and other alternative devices for IOP measurement were not included in this study, and their performance and comparison with the mentioned tonometers still need to be explored. Further research is necessary to validate the findings, assess long-term reliability, and investigate additional factors affecting measurement accuracy. Addressing these limitations will enhance our understanding and utilization of these devices in clinical practice, ultimately benefiting the diagnosis and management of patients with glaucoma and other ocular conditions.
Conclusion
In conclusion, this study compared Noncontact tonometer, Icare rebound tonometer, and Tono-Pen as alternative tools for measuring IOP. The results showed no significant difference in IOP measurements among the three devices, indicating their comparability. Correlation analysis demonstrated strong correlations between the tonometers. Bland-Altman plots indicated good agreement, with the Icare rebound tonometer and Tono-Pen exhibiting narrower limits of agreement. The study also found that IOP levels influenced the variability of measurement results. These findings highlight the potential of these alternative devices for IOP measurement, providing valuable insights for ophthalmologists in clinical practice.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shiose Y. Intraocular pressure: new perspectives. Surv Ophthalmol. 1990;34(6):413–435. doi:10.1016/0039-6257(90)90122-C
2. Gordon MO, Beiser JA, Brandt JD, et al. The ocular hypertension treatment study: baseline factors that predict the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120(6):714–720. doi:10.1001/archopht.120.6.714
3. Gordon MO, Kass MA. What we have learned from the ocular hypertension treatment study. Am J Ophthalmol. 2018;189:xxiv–xxvii. doi:10.1016/j.ajo.2018.02.016
4. Heijl A, Leske MC, Bengtsson B, et al. Reduction of intraocular pressure and glaucoma progression: results from the early manifest glaucoma trial. Arch Ophthalmol. 2002;120(10):1268–1279. doi:10.1001/archopht.120.10.1268
5. Yao F, Peng J, Zhang E, et al. Pathologically high intraocular pressure disturbs normal iron homeostasis and leads to retinal ganglion cell ferroptosis in glaucoma. Cell Death Differ. 2023;30(1):69–81. doi:10.1038/s41418-022-01046-4
6. Biswas S, Jhanji V, Leung CK. Prevalence of glaucoma in myopic corneal refractive surgery candidates in Hong Kong China. J Refract Surg. 2016;32(5):298–304. doi:10.3928/1081597X-20160229-01
7. Kim YW, Park KH. Exogenous influences on intraocular pressure. Br J Ophthalmol. 2019;103(9):1209–1216. doi:10.1136/bjophthalmol-2018-313381
8. Biswas S, Biswas P. Relationship between diurnal variation in intraocular pressure and central corneal power. Optom Vis Sci. 2023;100(1):96–104. doi:10.1097/opx.0000000000001974
9. Chen M, Zhang L, Xu J, et al. Comparability of three intraocular pressure measurement: iCare pro rebound, non-contact and Goldmann applanation tonometry in different IOP group. BMC Ophthalmol. 2019;19(1):1–10. doi:10.1186/s12886-019-1236-5
10. Badakere SV, Chary R, Choudhari NS, Rao HL, Garudadri C, Senthil S. Agreement of intraocular pressure measurement of Icare ic200 with Goldmann applanation tonometer in adult eyes with normal cornea. Ophthalmol Glaucoma. 2021;4(3):238–243. doi:10.1016/j.ogla.2021.04.002
11. Nakakura S, Asaoka R, Terao E, et al. Evaluation of rebound tonometer iCare IC200 as compared with IcarePRO and Goldmann applanation tonometer in patients with glaucoma. Eye and Vis. 2021;8(1):1–9. doi:10.1186/s40662-021-00249-z
12. Wu Y, Luttrell I, Feng S, et al. Development and validation of a machine learning, smartphone-based tonometer. Br J Ophthalmol. 2020;104(10):1394–1398. doi:10.1136/bjophthalmol-2019-315446
13. Jose J, Ramesh SV, Pai HV, et al. Agreement and repeatability of Icare ic100 tonometer. Indian J Ophthalmol. 2020;68(10):2122. doi:10.4103/ijo.IJO_546_19
14. Nayak RR, Kandula P, Johri B, Pai SG, Kamath SJ. A comparative study of intraocular pressure measurement using tonopen and Goldmann applanation tonometer. Int J Sci Res. 2017;6(5):665–669.
15. Brusini P, Salvetat ML, Zeppieri M, Tosoni C, Parisi L. Comparison of ICare tonometer with Goldmann applanation tonometer in glaucoma patients. J Glaucoma. 2006;15(3):213–217. doi:10.1097/01.ijg.0000212208.87523.66
16. Jansson U, Brautaset R, Cerviño A, Nilsson M. A comparison of the canon TX-20P™ non-contact tonometer and pachymeter in healthy eyes. Int J Ophthalmic Pract. 2012;3(3):96–102. doi:10.12968/ijop.2012.3.3.96
17. Tamçelik N, Atalay E, Cicik E, Özkök A. Comparability of Icare pro rebound tonometer with Goldmann applanation and noncontact tonometer in a wide range of intraocular pressure and central corneal thickness. Ophthalmic Res. 2015;54(1):18–25. doi:10.1159/000381781
18. Kutzscher AE, Kumar RS, Ramgopal B, et al. Reproducibility of 5 methods of ocular tonometry. Ophthalmol Glaucoma. 2019;2(6):429–434. doi:10.1016/j.ogla.2019.07.006
19. Kim KN, Jeoung JW, Park KH, Yang MK, Kim DM. Comparison of the new rebound tonometer with Goldmann applanation tonometer in a clinical setting. Acta Ophthalmol. 2013;91(5):e392–e396. doi:10.1111/aos.12109
20. Bao B, Diaconita V, Schulz DC, Hutnik C. Tono-pen versus Goldmann applanation tonometry: a comparison of 898 eyes. Ophthalmol Glaucoma. 2019;2(6):435–439. doi:10.1016/j.ogla.2019.07.004
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.