Back to Journals » Journal of Inflammation Research » Volume 19
Artificial Intelligence for Predicting Immunotherapy Efficacy in Non-Small Cell Lung Cancer
Authors Cao P, Jia X, Yang Y, Wang X, Zhu J, Li X, Yang Z, Wen Q
Received 30 November 2025
Accepted for publication 24 February 2026
Published 17 March 2026 Volume 2026:19 581764
DOI https://doi.org/10.2147/JIR.S581764
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Junhao Wang
Pingdong Cao,1 Xiao Jia,2 Yuqi Yang,1 Xi Wang,3 Jian Zhu,4 Xiaomei Li,1 Zhe Yang,1 Qiang Wen1
1Department of Radiation Oncology, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Shandong First Medical University, Jinan, People’s Republic of China; 2School of Control Science and Engineering, Shandong University, Jinan, People’s Republic of China; 3Department of Radiation Oncology, Stanford University School of Medicine, Palo Alto, CA, USA; 4Department of Radiation Physics, Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, Shandong, 250021, People’s Republic of China
Correspondence: Qiang Wen, Department of Radiation Oncology, Shandong Provincial Hospital Affiliated to Shandong First Medical University, 324 Jingwu Road, Jinan, Shandong, 250021, People’s Republic of China, Tel +86 18560222576, Email [email protected]
Abstract: Immune checkpoint inhibitors (ICIs) have significantly improved the clinical outcomes for patients with non-small cell lung cancer (NSCLC). However, patient heterogeneity and the limitations of current biomarkers contribute to variations in therapeutic responses. Identifying potential beneficiaries of immunotherapy and predicting efficacy remain critical challenges. In recent years, artificial intelligence (AI) has become increasingly applied in cancer treatment, particularly for modeling clinical data and predicting patient prognosis. By integrating multi-omics data such as radiomics, pathomics, genomics, transcriptomics, proteomics, and microbiomics, AI enables comprehensive biomarker discovery and facilitates prediction of immunotherapy responses and potential toxicities in NSCLC patients. Despite these advancements, challenges such as data standardization, limited interpretability, and technical barriers persist. This review summarizes the application of AI in predicting immunotherapy efficacy for NSCLC patients and discusses the challenges and future directions in the context of precision medicine.
Keywords: immunotherapy, immune checkpoint inhibitors, artificial intelligence, deep learning, machine learning, non-small cell lung cancer
Introduction
Lung cancer remains the leading cause of cancer-related mortality worldwide, with non-small cell lung cancer (NSCLC) as the most common histological subtype.1 As biotechnology advances and fully understanding of tumor immune escape mechanisms, immunotherapy has emerged as an important treatment option for NSCLC, alongside surgery, chemotherapy, targeted therapy, and radiotherapy.2,3
Immunotherapy achieves durable tumor control and complete responses by reactivating the cancer–immunity cycle and restoring effective innate and adaptive antitumor immunity.4 The principal modalities include immune checkpoint inhibitors (ICIs), chimeric antigen receptor (CAR) T-cell therapy, therapeutic cancer vaccines, and other forms of adoptive cell therapy (ACT).5 ICIs work therapeutically by targeting key regulatory pathways in immune modulation, primarily by blocking inhibitory signals mediated by programmed cell death protein 1 (PD-1), programmed death-ligand 1 (PD-L1), and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4).6 Current evidence supports PD-L1 expression, tumor mutational burden (TMB), and microsatellite instability–high/deficient mismatch repair (MSI-H/dMMR) as among the most informative and cost-effective biomarkers to guide clinical enrichment of patients who are more likely to benefit from immunotherapy.7,8 However, reliance on single or two-marker biomarkers yields suboptimal accuracy in predicting immunotherapy response. Some PD-L1-high/TMB-high tumors fail to respond, while a proportion of PD-L1-low/TMB-low tumors respond to ICIs, reflecting biological heterogeneity and the dynamic nature of the tumor–immune microenvironment.9,10 These discrepancies underscore the need for more robust strategies to monitor treatment effectiveness and to better identify patients most likely to benefit from ICIs, with the goal of improving clinical outcomes. Components of the tumor microenvironment (TME), including the abundance, phenotype, and spatial organization of immune-infiltrating cells, have shown potential for predicting immunotherapy efficacy.11 However, the predictive value of TME-based measures remains uncertain in clinical practice because of intratumoral heterogeneity, the lack of standardized assays, and the dynamic complexity of antitumor immunity, highlighting the need for prospective validation. Consequently, exploring ways to monitor the effectiveness of immunotherapy and to identify for patients who might potentially benefit from ICIs is crucial for improving the prognosis of immunotherapy.
In recent decades, research in cancer immunotherapy has progressively advanced toward the integration of diverse large-scale datasets, including radiomics, pathomics, genomics, and laboratory findings.12 Such multimodal data have been extensively utilized to enhance cancer diagnosis, evaluate therapeutic efficacy, predict prognosis, and elucidate tumor biology, thereby reshaping clinical management paradigms.13,14 Artificial intelligence (AI) harnesses these curated datasets to model and predict clinically relevant outcomes with high accuracy.15,16 This process involves data preprocessing, model development, and the application of pretrained algorithms that incorporate prior knowledge. Machine learning (ML), as a subset of AI, enables the resolution of complex problems without explicit programming.17 Among ML approaches, deep learning (DL) demonstrates superior efficiency and precision in high-dimensional data processing and holds great promise for improving immunotherapeutic strategies in NSCLC.18,19 Collectively, AI-driven applications offer substantial potential to enhance therapeutic response monitoring and prognostic prediction in NSCLC immunotherapy.
In this review, we systematically discuss the critical roles of AI in NSCLC immunotherapy, emphasizing its applications in evaluating treatment efficacy and prognosis prediction. Furthermore, we address current research limitations and outline future perspectives for potential developments.
AI in Oncology and Immunotherapy
Tumor heterogeneity is a key factor contributing to phenotypic diversity and variability in treatment response, and it exhibits multidimensional characteristics. Tumor heterogeneity manifests across multiple biological dimensions. At the genomic level, it is reflected in diverse mutational landscapes; at the proteomic level, in differential protein expression profiles; and at the tissue level, in variations in cellular organization and tumor microenvironmental composition. Consequently, this multidimensional heterogeneity can be characterized not only through genomic and proteomic analyses but also by imaging-based and other multimodal approaches that capture structural and functional diversity within tumors.
AI has considerable promise in cancer immunotherapy because it can process complex, high-dimensional data and extract informative features.20,21 When integrated into clinical oncology workflows, AI enhances the assessment of tumor heterogeneity and provides critical support for personalized treatment planning.22 In digital pathology, supervised ML can automatically identify tissues and cells on whole-slide images (WSIs) and generate reliable visual diagnostic outputs.23 DL, which employs multilayer neural networks to learn high-level representations from large datasets, offers superior representational capacity,24 and enables the discovery and quantification of immune biomarkers, the delineation of immune subtypes, and comprehensive profiling of immune-related features.25,26 In medical imaging, AI-based radiomics extracts high-dimensional features that capture tumor macroscopic architecture, surrogates of molecular profiles, and microenvironmental characteristics.27 As noninvasive approaches, these methods complement and mitigate the limitations of biopsy and help address spatial and temporal heterogeneity, thereby enabling dynamic monitoring of immunotherapy response and improving prognostic prediction.28,29 Tumor responses to immunotherapy are inherently complex and involve numerous biological pathways and regulatory networks.30,31 By harnessing multi-omics and multidimensional data, AI can develop predictive models that enable comprehensive characterization of the tumor immune microenvironment and its dynamic evolution, thereby supporting the optimization of therapeutic strategies and improving the accuracy of outcome prediction32,33 (Figure 1).
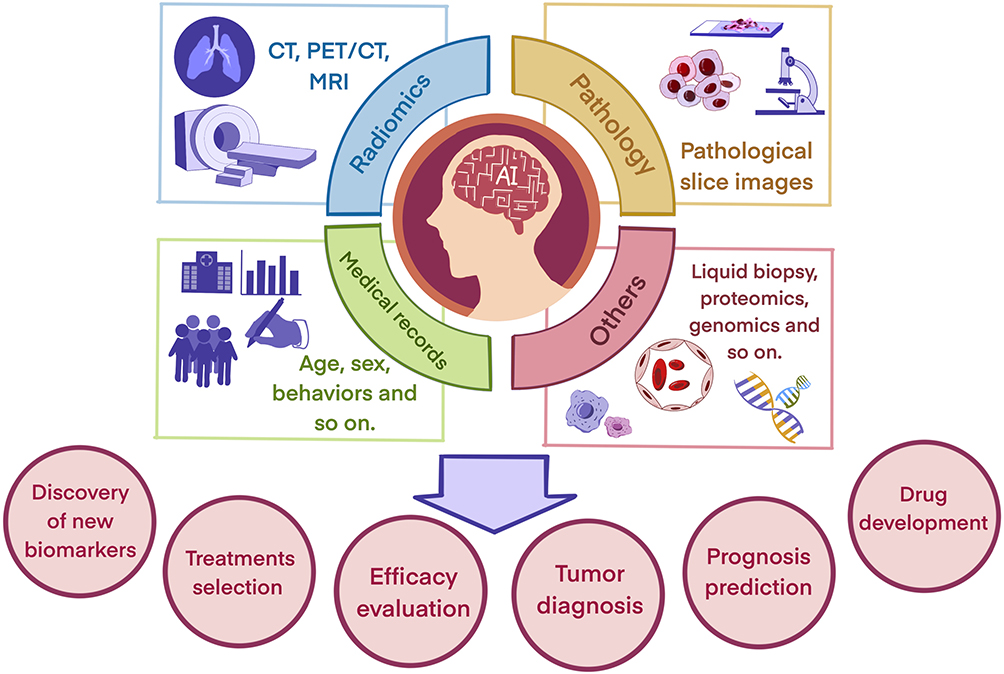 |
Figure 1 Applications of AI in oncology. |
Application of AI in NSCLC Immunotherapy
AI-assisted strategies for predicting immunotherapy efficacy can be broadly divided into indirect and direct approaches (Figure 2). Indirect approaches utilize AI models to infer the expression of biomarkers associated with treatment response, providing an indirect estimate of therapeutic benefit. In contrast, direct approaches employ end-to-end training on patients’ multimodal raw data to predict clinical endpoints without relying on predefined features or hand-crafted biomarkers. In NSCLC, AI has been applied to estimate PD-L1 expression, TMB, and tumor microenvironmental features. By fusing multimodal data streams, researchers have developed composite predictive models that support response prediction, patient stratification, and personalized immunotherapy design (Table 1). These models not only predict treatment responses but also facilitate patient stratification and the development of personalized immunotherapy strategies. Beyond efficacy prediction, AI is increasingly being explored for its potential to support clinical decision-making, particularly in the identification and prediction of immune-related adverse events (irAEs). Frameworks that incorporate longitudinal monitoring, multi-timepoint data fusion, and interpretable model design are likely to further enhance clinical applicability.
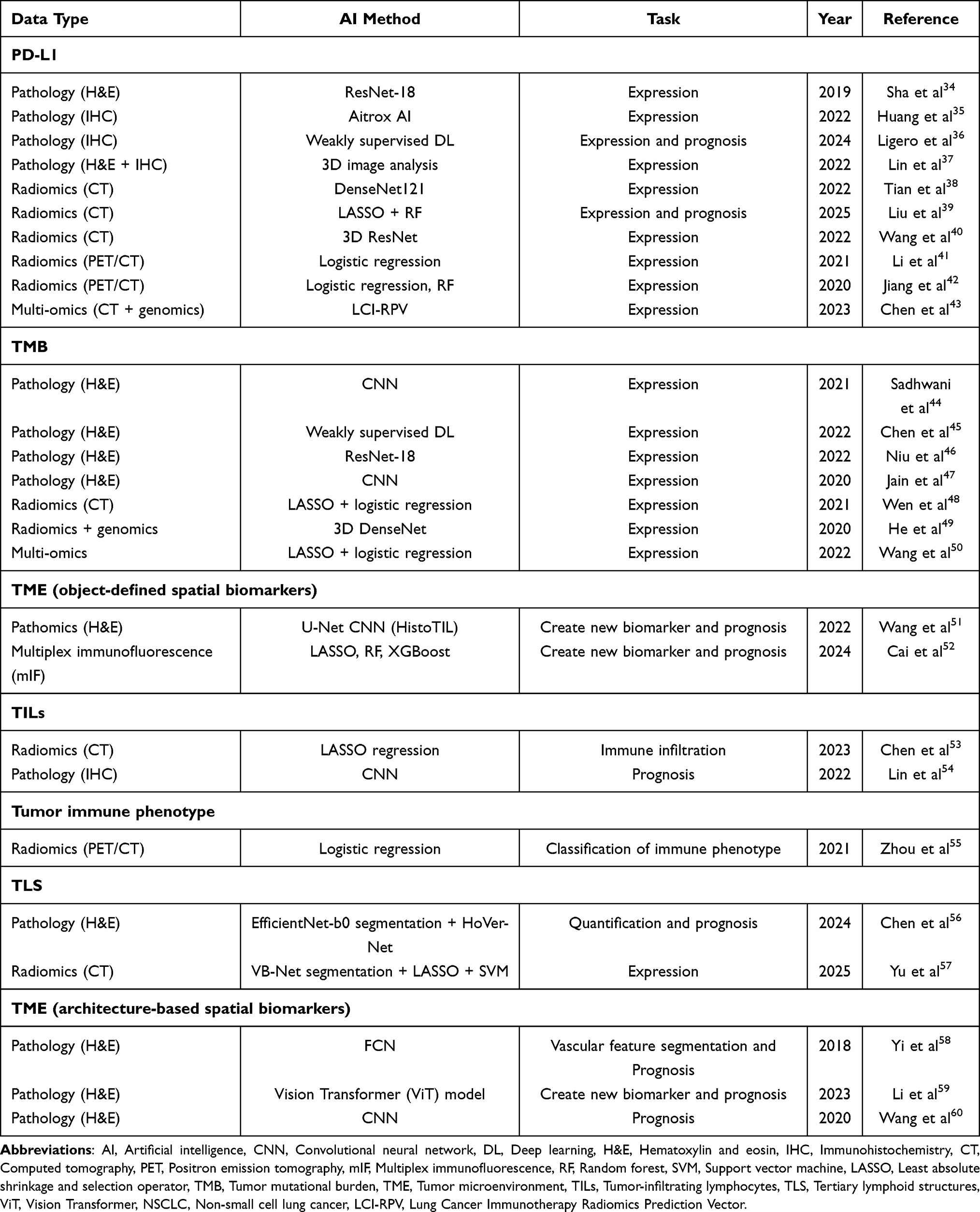 |
Table 1 AI-Based Models for Biomarker Prediction in NSCLC Immunotherapy |
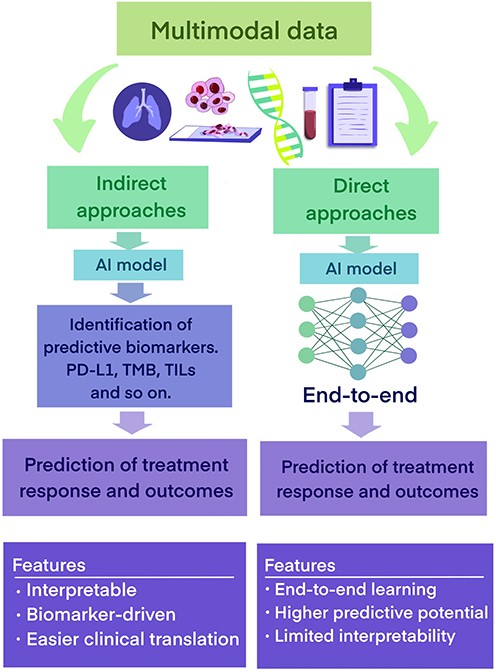 |
Figure 2 Workflow of indirect and direct AI-based approaches for predicting immunotherapy efficacy. |
Predicting Biomarkers
Pd-L1
PD-L1 is a key biomarker for identifying appropriate patients for immunotherapy, and numerous studies have shown that higher PD-L1 expression is associated with improved responses to ICIs and better clinical outcomes.61,62 In routine practice, PD-L1 is quantified by immunohistochemistry on tissue sections, most commonly using the tumor proportion score (TPS) or the combined positive score (CPS).63 However, its predictive performance is constrained by assay and platform heterogeneity (including antibody clones), intra- and intertumoral heterogeneity, variable immunohistochemical cutoff criteria and scoring algorithms, preanalytical factors, and inter-observer variability.64,65 These limitations yield only modest accuracy for PD-L1 as a standalone predictor of treatment efficacy and underscore the need for complementary biomarkers or composite models.
Advances in digital pathology and the widespread deployment of slide scanners have enabled the clinical adoption of AI for high-resolution whole-slide image processing and quantitative analysis. This progress has facilitated the automated assessment of PD-L1 expression in NSCLC. The Aitrox AI Model, an AI-assisted scoring system, reported superior classification performance compared with experienced pathologists for distinguishing PD-L1–positive from PD-L1–negative tumor cells, achieving 79.13% accuracy.35 Such tools support more standardized and reproducible quantification and can streamline pathology workflows. To avoid interobserver variability, Ligero et al developed a weakly supervised method that can predict PD-L1 status in NSCLC patients, with AUC values of 0.88 for the training set. This research proposed an end-to-end approach that predicts PD-L1 status directly from WSIs, without traditional steps such as cell detection and pigment quantification.36
In addition, the correlation between PD-L1 levels and the response to anti-PD-L1/PD-1 therapy can be unstable, likely due to the limited representativeness of biopsy samples and the spatial and temporal heterogeneity of tumors. Lin et al addressed this challenge by combining tissue-clearing technology with a convolutional neural network (CNN) model, enabling precise three-dimensional (3D) quantification of PD-L1 expression in NSCLC specimens.37 This 3D imaging approach allows for comprehensive evaluation of PD-L1 expression across different tumor regions, uncovering substantial intratumoral variability that is often missed in conventional two-dimensional (2D) sections. As a result, it enhances the understanding of the heterogeneity of PD-L1 expression within the TME and provides insights into the spatial relationships between tumor and immune cells. This offers critical perspectives on the immune–tumor interface and its potential impact on therapeutic response. Furthermore, the study demonstrated that 3D quantitative assessment of PD-L1 expression correlated more strongly with clinical outcomes of immunotherapy than traditional two-dimensional analyses.
PD-L1 protein expression is governed by genetic and regulatory mechanisms, and its imaging correlates often manifest as subtle morphological and textural differences in tumor tissue that are not easily visible to the naked eye. Radiomic features derived from high-throughput image analysis provide a quantitative foundation for assessing PD-L1–related heterogeneity on imaging. Compared with tissue sampling, medical imaging offers a noninvasive, longitudinal, and more comprehensive means of PD-L1 assessment. Tian et al developed a CT-based convolutional neural network to identify patients with high PD-L1 expression, reporting AUCs of approximately 0.78 in both the training and validation sets.38 Their model placed greater emphasis on peritumoral regions, suggesting that deep learning–derived representations can complement conventional quantitative radiomic features for classifying high versus low PD-L1 expression. In a separate study, Liu et al extracted radiomic features from baseline arterial-phase contrast-enhanced CT scans of 204 patients and trained multiple classifiers (naive Bayes, decision tree, XGBoost, and random forest (RF)) to predict PD-L1 status and immunotherapy outcomes in NSCLC.39 The RF model achieved the highest performance, with AUCs of 0.98 in both the training and validation cohorts. While these findings highlight the potential of radiomics and DL for noninvasive PD-L1 evaluation, rigorous external validation across multiple centers will be essential to confirm generalizability and mitigate overfitting.
Models based on single-omics data provide limited predictive power and cannot fully capture the biological complexity of tumors. To enhance PD-L1 prediction, investigators have adopted multi-omics strategies. Li et al employed fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) to combine radiomic features with clinicopathologic variables, resulting in a model that achieved superior diagnostic performance compared with either feature set alone (AUC = 0.81).41 In a retrospective analysis, the lung cancer immunotherapy radiomics prediction vector (LCI-RPV) combined CT-derived imaging features with CD274 counts and PD-L1 mRNA expression, yielding an AUC of 0.70 for PD-L1 positivity in two independent cohorts and effectively distinguishing patients with expression levels above clinically relevant thresholds.43 In conclusion, the multi-omics paradigm holds significant potential for discovering biomarkers, refining patient stratification, and enabling more precise, personalized therapeutic interventions in precision oncology.
TMB
TMB, defined as the total number of somatic mutations per megabase of tumor DNA after exclusion of germline variants, has been investigated as a predictive biomarker for PD-1/PD-L1 blockade efficacy in NSCLC.66 As the number of somatic mutations increases, the probability of producing immunogenic neoantigens rises, which can be processed and presented via MHC molecules and recognized by tumor-specific T cells. Recently, multiple clinical trials have reported an association between higher TMB and improved benefit from ICIs, although the strength and consistency of this relationship vary across assays, thresholds, and patient populations.67–69 Despite these observations, the clinical application of TMB remains challenging, as whole-exome sequencing (WES), the current reference approach for TMB assessment, is costly and technically demanding.
AI provides a promising approach for rapid and economical TMB estimation in lung cancer. Using lung adenocarcinoma (LUAD) images from The Cancer Genome Atlas (TCGA) and an independent set of 50 hematoxylin and eosin (H&E) WSIs, researchers built a two-part DL pipeline: a histologic-subtype classifier (LungCNN-Histo) to label histologic patterns across WSIs of resection specimens, and a weakly supervised model that used case-level TMB status as training labels to predict TMB directly from WSIs.44 In external validation, this system achieved AUCs ranging from 0.78 to 0.98 and outperformed models based solely on clinical variables. In a separate analysis, multi-omics data from TCGA-LUAD (somatic mutations, gene expression, miRNA, and DNA methylation) were used to train a machine-learning classifier that distinguished high- versus low-TMB groups with 91.1% sensitivity and 75.0% specificity, with quantitative real-time polymerase chain reaction (qRT-PCR) providing orthogonal validation.50 Collectively, these strategies reduce the dependence on WES while maintaining diagnostic performance.
Radiomics parameters derived from medical imaging offer a non-invasive alternative. Wen et al developed combined models that integrated radiomic features with clinical and morphologic factors to predict PD-L1 expression and TMB status, achieving AUCs of 0.839 and 0.818, respectively.48 Multivariate analysis further indicated that histologic differentiation grade was associated with TMB. These results suggest that combined radiomics-clinical models can improve predictive accuracy and inform treatment decision-making in practice. Despite the rapid advancements in AI algorithms, the predictive value of TMB in forecasting the efficacy of immune therapies remains unsettled. Early studies have reported a lack of positive correlation between TMB and clinical outcomes in NSCLC patients undergoing immunotherapy.70 Future work should prioritize harmonization of assay platforms, establishment of clinically actionable TMB thresholds, and integration of TMB with complementary biomarkers, such as PD-L1 expression and tumor-infiltrating lymphocytes, to enhance predictive performance and generalizability.
TME
TME is a key determinant of ICI efficacy because antitumor immunity depends not only on tumor intrinsic features but also on the composition, functional state, and spatial arrangement of immune and stromal cells. In routine practice, traditional biomarkers such as PD-L1 and TMB show only modest predictive performance, and even patients with high values may not benefit, which has led to increased attention on the tumor immune microenvironment. Immune-inflamed tumors, characterized by abundant intratumoral tumor-infiltrating lymphocytes (TILs), generally respond better to checkpoint blockade, whereas immune-excluded tumors, with immune cells confined to the stromal or peripheral regions, and immune-desert tumors, with scarce infiltration, are often less sensitive.71,72 This reflects the fact that effective immunity is shaped by complex interactions among immune cells, stromal components, and the vasculature, and by whether effector cells can access tumor epithelial nests. Accordingly, quantitative profiling of TME phenotypes and related features, including TIL spatial patterns, tertiary lymphoid structures, and vascular characteristics, provides clinically meaningful context for patient stratification and drives AI-based approaches that can standardize and scale TME characterization.
As a central component of tumor–immune interactions, the density and spatial architecture of TILs provide the structural basis for defining immune phenotypes such as immune-desert, inflamed, and excluded tumors, each exhibiting distinct sensitivities to ICIs. However, traditional manual assessment is limited by variability and modest reproducibility. Wang et al developed HistoTIL, which was validated across multiple NSCLC cohorts and, in some settings, complemented—and in some cases, exceeded—the predictive capacity of PD-L1 status alone for survival.51 Cai et al employed multiplex immunofluorescence to construct spatial interaction networks of regulatory T cells (Tregs) and their neighboring cells in resectable NSCLC.52 They identified a spatial immune signature that independently predicted recurrence and further demonstrated that enrichment of FOXP3⁺ Tregs was associated with increased PD-1/PD-L1 cell clustering, highlighting the contribution of an immunosuppressive microenvironment to prognosis. Building on these tissue-based spatial insights, radiomics has been used to estimate immune cell infiltration noninvasively and at the whole-tumor scale. Chen et al derived a CT-based radiomics signature of CD8⁺ TIL density that achieved an AUC of 0.83, suggesting that imaging-derived features can serve as surrogates for effector T-cell abundance.53 Zhou et al applied FDG-PET/CT radiomics to classify tumor immune types and successfully identified immunologically “hot” tumors that are more likely to benefit from checkpoint blockade.55
The dynamic changes in the immune microenvironment and the distribution of immune cells can interfere with treatment response evaluation and affect prognosis. Pseudoprogression may occur during immunotherapy when checkpoint inhibition activates the host immune response. Effector T cells and other immune cells infiltrate the TME, potentially leading to a transient increase in lesion size or the appearance of new lesions on imaging. This phenomenon reflects immune cell influx and inflammation rather than true tumor progression. However, with continued therapy, some patients subsequently show lesion shrinkage or stabilization, indicating a potential clinical benefit. A recent radiomics-based AI study developed a baseline CT model using combined intratumoral and peritumoral features to identify pseudoprogression in NSCLC patients treated with ICIs, achieving high discrimination (AUC = 0.95).73
In contrast, hyperprogressive disease (HPD) represents a distinct pattern of rapid tumor acceleration under immunotherapy, which is associated with poor outcomes, making early recognition critical.74 Proposed mechanisms for HPD include the activation of oncogenic pathways in tumor cells and the abnormal recruitment of regulatory Tregs following ICI therapy. These changes can enhance an immunosuppressive microenvironment, driving accelerated tumor growth.75–77 Other potential contributors to HPD may involve tumor immune evasion, dysregulated activation of suppressive immune cells, and remodeling of the tumor microenvironment. However, the precise molecular basis remains to be fully elucidated. Investigating the mechanisms underlying HPD and identifying predictive biomarkers is critical for guiding patient stratification and preventing unnecessary immunotherapy. Vaidya et al extracted intratumoral and peritumoral texture features alongside quantitative vessel tortuosity and trained a random forest classifier that successfully differentiated HPD from other response patterns with strong performance.78
Tumor-associated tertiary lymphoid structures (TLSs) represent higher-order lymphoid aggregates within the TME that support antigen presentation and lymphocyte activation. Larger TLS areas and a higher B-cell content have been associated with improved survival in resected NSCLC. Chen et al developed a deep learning model for automated TLS segmentation from H&E slides, achieving a dice coefficient of 0.91, and linked TLS density with immune-related signatures such as CXCL13.56 Yu et al demonstrated that CT-based radiomics can noninvasively predict TLS status, with performance exceeding both clinical models and expert radiologist assessments.57
The tumor vasculature plays a critical role in modulating antitumor immune activity. Abnormal angiogenesis promotes hypoxia, restricts cytotoxic T-cell trafficking, and drives immunosuppression via VEGF signaling. This understanding provides a rationale for combining VEGF blockade with checkpoint inhibitors. To enable systematic vascular assessment, Yi et al developed a fully convolutional neural network that accurately identifies microvessels in H&E images of lung adenocarcinoma, demonstrating robust generalization across independent cohorts.58 Li et al proposed an outcome-supervised survival model based on a Vision Transformer (ViT) backbone, which leverages self-attention to capture global spatial dependencies within the TME.59 This framework demonstrated superior generalization for predicting immunotherapy outcomes compared with CNNs.
Beyond spatially quantifiable TME features, emerging evidence suggests that functional and metabolic reprogramming of immune cells also critically shapes the tumor immune microenvironment and may underlie imaging- or AI-derived biomarkers. Zhang et al reported that in elderly patients with lung squamous cell carcinoma (LSCC), Tregs overexpress SOAT2, an endoplasmic reticulum enzyme that promotes cholesterol esterification.79 This metabolic reprogramming, mediated through the SREBP2–HMGCR–GGPP pathway, enhances Treg suppressive function while reducing CD8⁺ T-cell proliferation, migration, and antitumor activity. Analysis of patient cohorts further demonstrated that increased SOAT2 expression was associated with reduced immune infiltration and poorer prognosis in elderly LSCC patients. These findings suggest that metabolic alterations within Tregs represent an additional layer of immune regulation within the TME, complementing spatial immune features and potentially influencing responses to immunotherapy. Computational pathology and imaging enhance our understanding of the TME by quantifying TILs, TLSs, and vascular features, and by integrating their spatial interactions, thereby generating reproducible biomarkers beyond PD-L1 and TMB.
Response and Outcome
The monitoring of immunotherapy response and outcome largely depends on experienced oncologists who need to synthesize heterogeneous information, including patient symptoms, medical imaging, and laboratory test results. This data integration workflow is complex and may compromise the accuracy of response assessment, potentially delaying necessary treatment adjustments. The immune-related Response Evaluation Criteria in Solid Tumors (iRECIST) provide a standardized framework for evaluating immunotherapy outcomes. However, reliance on delayed radiographic signals and susceptibility to pseudoprogression limit the ability of iRECIST to capture atypical response patterns, which can have downstream implications for clinical decision-making.
Radiomics
Radiomics enables the quantitative extraction of high-dimensional features from routine imaging, offering a noninvasive means to characterize tumor heterogeneity beyond visual inspection. Recent AI-driven radiomics applications for predicting immunotherapy response are summarized in Table 2. To enhance clarity and readability, the table is organized by key study characteristics, including imaging modality, sample size, clinical endpoints, model type, validation strategy, and main performance metrics.
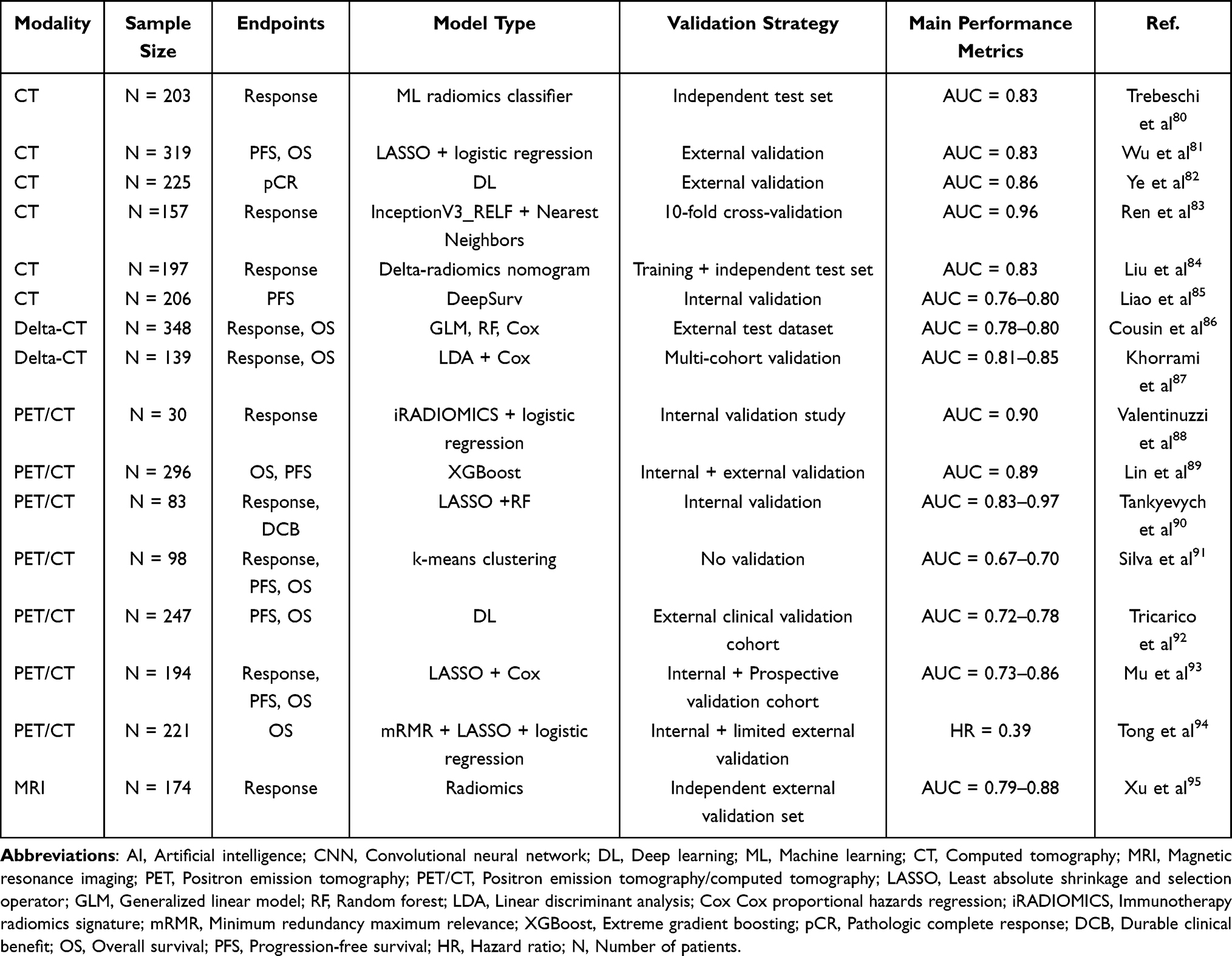 |
Table 2 Studies Using AI-Based Radiomics to Predict Response and Outcomes to Immunotherapy in Lung Cancer |
CT imaging provides valuable information on the primary tumor, nodal disease, and distant metastases. Early studies demonstrated that morphological heterogeneity and texture patterns in baseline CT images correlated with ICIs response. Trebeschi et al reported that lesions with compact borders, nonuniform density, and higher heterogeneity were more likely to respond to treatment (AUC = 0.83).80 Wu et al incorporated intratumoral and peritumoral features selected by least absolute shrinkage and selection operator (LASSO), which successfully distinguished responders, stratified survival, and emphasized the prognostic value of peritumoral characteristics. These results suggest that static CT-derived signatures can serve as useful baseline predictors.81 Ye et al constructed models named LUNAI-uCT (noncontrast CT), LUNAI-eCT (contrast-enhanced CT), and LUNAI-fCT (fusion of both phases) to predict pathological complete response after neoadjuvant immunochemotherapy.82 The fusion model achieved the highest performance (AUC = 0.86), indicating that multiphase CT information improves prognostic accuracy in resectable NSCLC.
While baseline CT-derived signatures have shown promise, they provide only a static snapshot of a disease that evolves dynamically. Delta radiomics, which analyzes serial scans to quantify temporal changes in imaging features, offers a more dynamic approach. Cousin et al extracted features from sequential CT scans and demonstrated that a delta-radiomics RF model (AUC = 0.80) outperformed RECIST (AUC = 0.66) in predicting durable benefit.86 Khorrami et al extended this concept with DelRadX, which integrates intra- and perinodular texture changes to predict survival.87 These findings suggest that longitudinal image dynamics may better reflect the underlying biology of immunotherapy response than size-based criteria. Additionally, Barabino et al retrospectively analyzed radiomic features from baseline and post-treatment CT scans of 43 NSCLC lesions treated with ICIs.96 They identified 27 delta features that were significantly associated with treatment response, of which 9 were specifically linked to pseudoprogression.
The combination of 18F FDG PET metabolic data with CT anatomy further enriches radiomic analysis by capturing both metabolic activity and structural heterogeneity. Valentinuzzi et al developed a PET radiomics score for predicting pembrolizumab response in metastatic NSCLC, demonstrating better performance than clinical criteria for overall survival (OS) (AUC = 0.90).88 Lin et al integrated intratumoral and peritumoral PET/CT radiomics to assess metabolic heterogeneity and found significant associations with immunotherapy outcomes and survival, further supporting the prognostic relevance of metabolic features.89 Building on these findings, Tankyevych et al incorporated baseline and follow-up PET/CT scans with delta-radiomics features, achieving AUCs up to 1.00 for disease progression and above 0.80 for durable benefit prediction.90 These studies suggest that PET/CT radiomics, particularly when incorporating temporal dynamics, provides functional insights that frequently surpass CT alone in predictive performance. Although still limited in NSCLC, magnetic resonance imaging (MRI) radiomics holds specific promise in the context of brain metastases, where outcomes to ICIs are notably heterogeneous. Xu et al developed a contrast-enhanced MRI nomogram for patients with brain metastases, achieving AUCs above 0.80 for predicting intracranial progression-free survival (PFS).95 This highlights the potential of advanced MRI techniques to guide immunotherapy management in this challenging setting. AI-based radiomics offers a noninvasive complement to tissue biopsy and addresses both intertumoral and intratumoral heterogeneity by leveraging quantitative imaging signatures. By coupling medical imaging with machine learning, these approaches provide actionable insights into immunotherapy efficacy and hold significant promise for more precise and personalized treatment strategies.
Pathomics
H&E-stained tissue slides remain the benchmark for histopathological assessment of solid tumors. However, the rising number of cases and interobserver variability limit the effectiveness of conventional methods in predicting immunotherapy outcomes. AI has emerged as a transformative approach in histopathology. Sirinukunwattana et al used a Spatially Constrained Convolutional Neural Network (SC-CNN) to achieve precise segmentation and classification of nuclei in whole-slide images, enabling quantitative analysis of tissue compartments and demonstrating how AI can enhance diagnostic practices.97 Recent advances in AI-driven pathomics for predicting immunotherapy outcomes in NSCLC are summarized in Table 3.
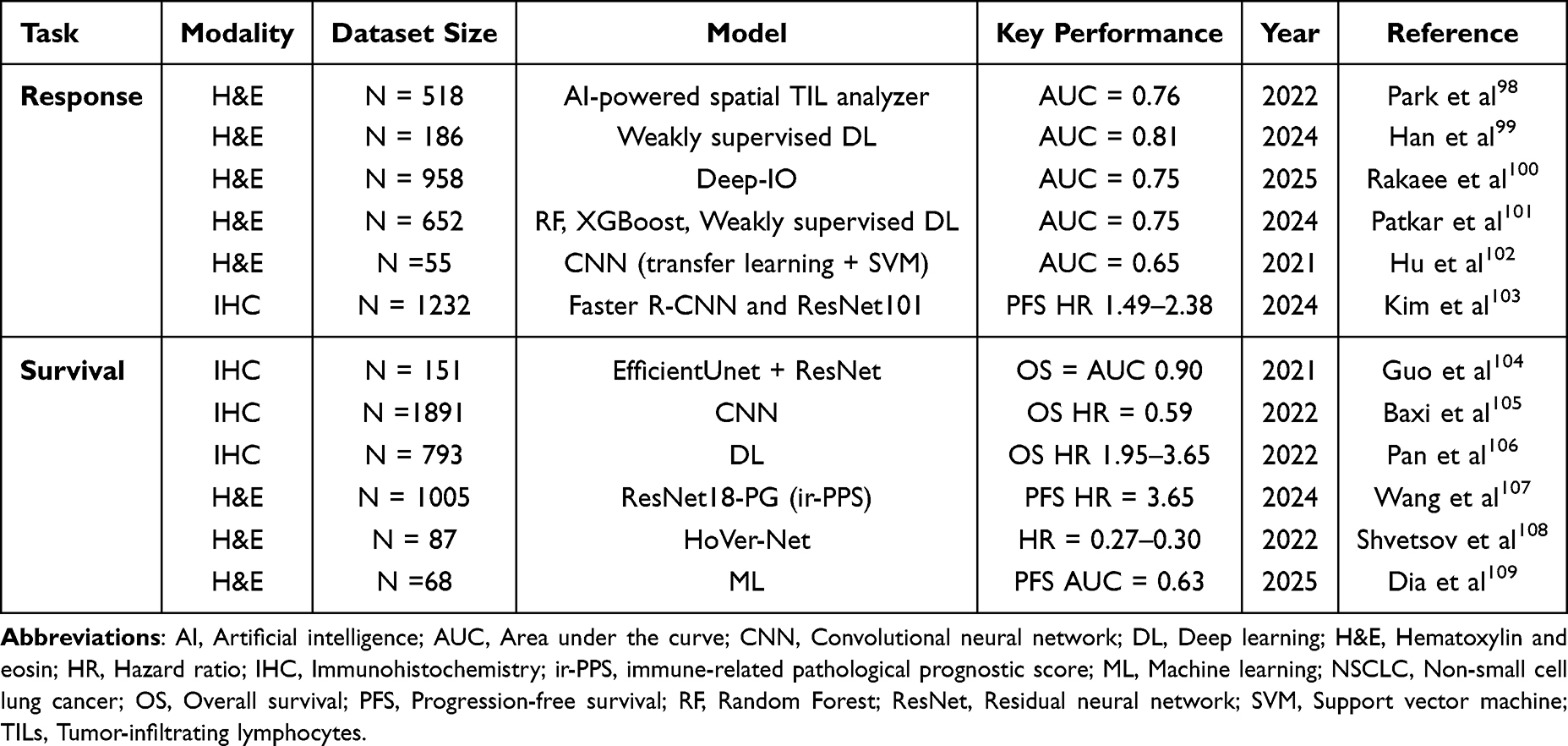 |
Table 3 AI Applications in Pathomics for Predicting Immunotherapy Response and Prognosis in NSCLC |
Using H&E slides, Han et al first demonstrated that weakly supervised learning applied to H&E slides could predict major pathological response to neoadjuvant chemoimmunotherapy in a multicenter cohort of 186 patients, achieving AUCs above 0.80.99 Building on this, Rakaee et al developed Deep-IO, a supervised model trained on 958 advanced NSCLC cases, which predicted objective response with an AUC of 0.75 in internal validation and 0.66 in external cohorts.100 The features learned by Deep-IO were independent of PD-L1 expression and TMB, and the model retained prognostic value, with a significant association with survival (Hazard Ratio (HR) = 0.56 for PFS; HR = 0.53 for OS). Patkar et al further showed that AI could capture TME characteristics directly from H&E slides to predict treatment outcomes.101 The HistoTME model was trained on more than 1,800 NSCLC cases, reconstructed 30 immune signatures, achieved an AUC of 0.75 for first-line response, and stratified overall survival with hazard ratios as low as 0.39 in patients with low PD-L1 expression. Furthermore, Hu et al conducted a proof-of-concept study applying the same convolutional model to NSCLC and melanoma.102 Although performance was higher in melanoma (AUC = 0.78) than in NSCLC (AUC = 0.65), these results support cross-cancer generalization and motivate further work on model transferability.
Beyond H&E-based assessments, AI models applied to IHC slides have shown strong potential because IHC provides molecularly specific information that complements the morphology visible on H&E. Kim et al evaluated AI-based PD-L1 scoring in NSCLC treated with immune checkpoint inhibitors and reported that patients with AI-defined TPS less than 1% had very low response rates of approximately 2% and shorter survival.103 Compared with patients with TPS ≥ 50%, the hazard ratios were 2.38 for PFS and 1.90 for OS. Notably, nearly half of the patients classified as negative by pathologists but reclassified as positive by AI experienced improved responses and longer survival, suggesting that AI can recover signals missed by manual scoring. Moving beyond a single marker, Guo et al applied DL to IHC images stained for ten immune checkpoint molecules and incorporated spatial features of tumor cells and lymphocytes.104 Their models achieved AUC values above 0.80 for overall and relapse-free survival in independent cohorts, demonstrating that multi-biomarker and spatial analysis yield richer prognostic information. Baxi et al conducted a large multi-cohort validation across several tumor types, including NSCLC. Using CNNs to analyze 1,746 PD-L1 IHC slides from pivotal CheckMate trials, they evaluated associations with response and survival. In NSCLC, AI and manual scoring showed similar predictive performance for treatment response with a summary AUC of about 0.60, but AI-defined PD-L1 positivity exhibited stronger and more consistent associations with overall survival. For example, in CheckMate 057, the HR for OS was 0.59 with AI scoring versus 0.70 with manual assessment.105 These findings suggest that AI-driven pathology, leveraging both H&E and IHC slides, can generate reproducible and biologically meaningful biomarkers. By quantifying TME features and capturing spatial relationships, AI models can improve risk stratification and enhance the prediction of immunotherapy outcomes in NSCLC.
Liquid Biopsy
Traditional biomarkers face challenges in dynamically monitoring tumor-immune interactions and identifying responders. Liquid biopsy has emerged as a promising technique for capturing tumor heterogeneity and improving the accuracy of immunotherapy predictions.110 Circulating tumor DNA (ctDNA) is a tumor-specific biomarker that enables highly sensitive detection of recurrence by identifying trace amounts of tumor-derived DNA in the blood. This is particularly useful for early surveillance in cases with low tumor burden, as it facilitates timely therapeutic adjustments. In parallel, minimal residual disease (MRD) monitoring assesses the presence of residual tumor after treatment and serves as a key predictor of recurrence risk.111 Guided by DL, Widman et al developed a plasma whole-genome sequencing ctDNA signal enrichment platform, named MRD-EDGE, which monitors tumor burden with high sensitivity and detects postoperative MRD in NSCLC. The platform achieved a detection sensitivity of 0.70 at a tumor fraction of 5×10−5 and enabled dynamic tracking of plasma tumor fraction following neoadjuvant ICI treatment.112 In addition, Guibert et al observed marked reductions in ctDNA among patients with pseudoprogression, whereas ctDNA increased in those with true progression.113
Using routinely available blood indices, Benzekry et al applied multiple machine learning algorithms, including support vector machines (SVM), RF, logistic regression (LR), naive Bayes, and single-layer neural networks, to evaluate the predictive value of the neutrophil-to-lymphocyte ratio (NLR) in metastatic NSCLC patients treated with ICIs.114 NLR correlated with disease control and six-month survival, with the RF model achieving the best performance for disease control (AUC = 0.74 ± 0.03). AI has also been leveraged to derive molecular signatures from peripheral blood. Zhou et al employed multicolor flow cytometry to automatically classify immune-cell subsets and generated a liquid immune profile–based signature associated with survival in lung cancer patients receiving anti-PD-1/PD-L1 therapy.115 As technology advances, combining ctDNA and MRD monitoring with immunotherapy biomarkers such as PD-L1, TMB, and MSI provides a robust strategy for assessing treatment efficacy and refining individualized management.
Proteomics
Proteomics provides a powerful method for profiling protein expression and post-translational modifications in cancer, thereby capturing the functional state of immune responses by directly reflecting cellular processes. Proteomic measurements can delineate real-time interactions between proteins and the TME, serving as dynamic biomarkers for immune activation and therapeutic efficacy in lung cancer. Mass spectrometry (MS)-based proteomics remains the cornerstone for high-throughput protein identification and quantification116 and has been widely applied to discover protein biomarkers predictive of immunotherapy outcomes, aiding in patient stratification and precision treatment. Recent work, using unsupervised ML on a panel of more than 1,600 serum autoantibodies, identified 13 signature features that correlated strongly with five-year survival in lung cancer.117 This demonstrates the value of computational analysis in biomarker discovery. These findings underscore the potential of proteomics, combined with advanced computational methods, to enhance biomarker discovery and support the development of personalized immunotherapy strategies. A serum protein classifier was also developed using ML techniques that integrated MS features with clinical data from 116 NSCLC patients treated with nivolumab.118 The model successfully stratified patients into resistant, intermediate, and sensitive groups and demonstrated strong discrimination for clinical benefit. Furthermore, ML-based approaches have identified multiple serum-derived proteins with prognostic relevance in patients receiving immune checkpoint blockade, facilitating outcome stratification.119 The incorporation of AI into proteomics represents a promising direction for improving assessment and guiding therapeutic strategies post-immunotherapy.
Microbiota
The microbiota, particularly the gut microbiome, plays pivotal roles in multiple stages of immune regulation. The underlying mechanisms involve enhancing antigen presentation, promoting effector T cell function, suppressing the activity of immunosuppressive cells and cytokines, augmenting antibody responses, and upregulating chemokine expression.120,121 As a result, the microbiome significantly modulates the TME and can influence the efficacy of ICIs. Bifidobacterium has been shown to induce dendritic cell activation, promoting the proliferation of tumor-specific CD8+ T cells and exerting antitumor immune effects.122 AI models based on the microbiome have demonstrated clinical value by identifying microbial signatures that predict response to ICIs,123 forecast clinical outcomes,124 and predict drug resistance125 and irAEs.126 Furthermore, factors such as diet, sleep cycles, physical activity, and medications that directly or indirectly affect gut microbiota composition and metabolic functions may influence the characteristics and efficacy of gut microbiota and ICIs.
Genomics
Recent studies underscore the pivotal role of genomic alterations in shaping both tumor behavior and patient responses to ICIs in NSCLC. DL-based analyses have provided valuable insights into key biomarkers that influence treatment outcomes, particularly identifying epidermal growth factor receptor (EGFR) mutations, which are linked to a higher incidence of HPD in NSCLC patients undergoing immunotherapy.127 However, the role of genetic alterations extends beyond individual mutations. Pathway-level analyses have uncovered resistance-associated signaling cascades, including PDGF, ESR1, YAP/TAZ, EGFR, IGF, and AGTR1, which facilitate immune evasion and compromise the effectiveness of immunotherapy.128 Notably, mutations in STK11 and CDKN2B have been shown to correlate with reduced therapeutic benefit from ICIs, highlighting how specific genomic alterations directly impact immunotherapy outcomes.
In addition to somatic mutations, immunoregulation-related genes (IRGs) have emerged as significant determinants of both patient prognosis and ICI response. Wang et al developed a novel IRG-based prognostic index (IRGI) by integrating RNA-seq data from lung adenocarcinoma (LUAD) cohorts with XGBoost machine learning models.129 This model effectively stratified patients into high- and low-risk groups, revealing significant differences in survival outcomes and TME immune infiltration. To enhance the interpretability of the model, SHapley Additive exPlanations (SHAP) analysis was employed, which identified GREM1 as the key factor contributing most to the model’s predictive power. This finding underscores the importance of immune-related genetic features in regulating antitumor immunity. By combining genomic information with AI-driven models, the IRGI framework not only improves the precision of patient stratification but also helps guide personalized immunotherapy strategies. Together, these studies highlight the value of genomic profiling, which spans from identifying driver mutations and resistance pathways to understanding immunoregulatory gene expression, in offering critical insights into tumor biology and treatment responsiveness. The integration of such genomic data with AI approaches enhances the accuracy of predicting ICIs efficacy and provides a solid foundation for precision immuno-oncology in NSCLC. By leveraging this integrated approach, AI models can not only predict treatment responses more accurately but also identify novel biomarkers that can guide more effective, personalized therapeutic strategies. This convergence of genomics and artificial intelligence promises to improve patient outcomes and refine treatment paradigms in the era of precision oncology.
Multi-Modality Data
Single-omics approaches have demonstrated utility in predicting immunotherapy outcomes; however, they capture only a limited portion of the complex biological processes driving antitumor immune responses. In contrast, multi-omics strategies provide complementary layers of information, offering a more comprehensive view of tumor–immune interactions. By integrating diverse biological data, AI can uncover latent patterns and generate robust, generalizable models. As such, AI-driven multi-omics methods hold great promise for enhancing the prediction of immunotherapy benefit, particularly in NSCLC.
Several recent studies have explored the potential of combining multiple omics layers with AI to predict immunotherapy responses more accurately. Sun et al integrated CT radiomics with RNA-based CD8⁺ T-cell signatures to predict immunotherapy benefit in NSCLC. Their radiogenomic score demonstrated moderate discrimination (AUC = 0.67) and was significantly associated with both response and survival (HR = 0.52).130 This study provided an early, noninvasive connection between imaging features and immune phenotypes, illustrating the power of combining imaging and molecular data. To improve predictive accuracy, Yang et al developed the SimTA framework in a cohort of 200 patients with advanced NSCLC.131 By combining serial CT radiomics, longitudinal blood biomarkers, and clinical data, SimTA overcame the static nature of previous methods by modeling asynchronous time-series inputs. This approach stratified patients with stable disease beyond RECIST, achieving an AUC of 0.80, with low-risk patients showing significantly longer PFS (HR = 3.14) and OS (HR = 2.46). In another study, Farina et al analyzed data from 264 stage IV NSCLC patients across two centers using ensemble models that incorporated baseline and follow-up CT imaging, clinical, and blood features.132 Their model predicted durable clinical benefit with AUCs of 0.82 at six months and 0.75 at nine months, with an overall survival C-index of approximately 0.74. These results demonstrated the model’s generalizability and ability to capture sustained outcomes over time.
Expanding on these findings, Vanguri et al developed DyAM, a deep learning model that combines baseline CT radiomics, digitized PD-L1 immunohistochemistry, and genomic profiles from the MSK-IMPACT panel in 247 NSCLC patients receiving PD-L1 therapy.133 This multimodal approach significantly improved response prediction compared to individual modalities (AUC = 0.80) and demonstrated a strong association with OS (C-index = 0.74). Notably, DyAM incorporated an attention mechanism, which quantified the contribution of each modality, enhancing model interpretability and providing biological context for the predictions. Finally, to address scalability and clinical robustness, Captier et al incorporated a combination of PET/CT, digitized pathology, bulk RNA sequencing, and clinical variables in one of the largest multimodal NSCLC cohorts to date.134 Their model achieved a C-index of approximately 0.75 for survival, indicating stable and clinically meaningful performance at scale.
Recent studies show that AI-driven multimodal co-analysis enhances prediction of immunotherapy outcomes in NSCLC. By linking imaging, pathology, molecular, and clinical features, these approaches consistently outperform unimodal analyses in both short-term response assessment and long-term survival prediction. Beyond improved accuracy, models that use longitudinal data and multi-institutional cohorts exhibit greater robustness, generalizability, and interpretability. Fatima et al further reviewed the translational value of multimodal AI in NSCLC, emphasizing that radiomics, digital pathology, and ctDNA-integrated models can play a critical role in predicting actionable biomarkers, such as mesenchymal–epithelial transition (MET) status, optimizing patient selection, and dynamically guiding treatment strategies.135 Giulia et al differentiated between locally acquired resistance and systemically acquired resistance in NSCLC patients through longitudinal monitoring of radiomic features and immune signatures.136 The model, which incorporated multi-omics features, exhibited strong predictive performance, achieving ROC-AUC values ranging from 0.88 to 0.99. This strategy facilitates a more comprehensive assessment of patient status and supports the development of personalized therapeutic approaches. These advances highlight the potential of multimodal AI as a promising strategy to refine patient stratification, capture dynamic tumor–immune interactions, and accelerate the clinical translation of precision immuno-oncology.
irAEs
Approximately one-third of patients receiving immunotherapy develop irAEs, which can affect multiple organs, including the skin, respiratory tract, gastrointestinal tract, and cardiovascular system.137,138 The underlying mechanism involves ICI-induced immune dysregulation, which disrupts immune homeostasis while targeting tumor cells. Key hallmarks of irAEs include imbalanced T-cell responses, increased autoantibody production, and aberrant cytokine activity.139 These adverse events represent a major cause of treatment discontinuation and can profoundly affect patient outcomes.
Immune checkpoint inhibitor-related pneumonitis (iCIP) is the most common respiratory complication.140,141 DL models have shown promise in predicting iCIP in lung cancer patients. Cheng et al developed a multi-model nomogram that incorporated clinical variables with deep radiomics features extracted using a ResNet-50-V2 backbone enhanced by a feature pyramid network.142 The model achieved AUCs of 0.91 in the training set and 0.90 in the test set, outperforming clinical-only or radiomics-only models. The risk of pneumonitis increases when immunotherapy is combined with radiotherapy.143,144 In a cohort of 243 patients treated with combined therapy, Yang et al used 3D U-Net to analyze tumor and lung volumes on CT and employed graph attention networks for feature selection and fusion.145 The model reached an AUC of 0.82, exceeding conventional approaches. iCIP and radiation pneumonitis (RP) exhibit considerable overlap in clinical presentation and radiological characteristics. Timely differentiation between these two conditions is essential to avoid unnecessary treatment interruption or inappropriate management adjustments. However, most existing studies have been limited by small sample sizes and modest predictive performance.146,147 Recently, a radiomics model developed by Qiu et al utilized quantitative radiomic features to distinguish the etiology of pneumonia. Using LASSO for feature selection and logistic regression for model construction, they established a radiomics nomogram.148 Incorporating features such as bilateral changes and sharp lesion borders, the model achieved notable improvements in classification performance, with AUC values of 0.891 and 0.896. This approach provides a more accurate diagnostic tool for clinical decision-making.
Cardiotoxicity is another clinically relevant irAE. Using 356 medical history variables as candidate predictors, an XGBoost decision tree was trained to estimate the probability of cardiac adverse events in patients receiving PD-1 or PD-L1 therapy. The model achieved an AUC of 0.65 (95% CI 0.58 to 0.75).149 Lower neutrophil-to-lymphocyte ratio (NLR) was associated with a reduced risk, consistent with a protective effect in patients with more favorable systemic inflammatory profiles. In contrast, abnormal body temperature and elevated heart rate emerged as significant risk factors. These findings support the feasibility of machine learning-based risk stratification for cardiotoxicity during ICI therapy and highlight readily obtainable clinical features that can inform monitoring strategies.
Limitations and Future Directions
Although AI algorithms have shown promise in evaluating immunotherapy responses and predicting clinical outcomes in NSCLC, significant barriers persist in translating these technological advancements into routine clinical practice. Overcoming these challenges is essential to develop a clinically feasible framework that enables the reliable integration of AI-driven solutions into real-world oncology care.
Data Availability and Standardization
The principal barrier to broader radiomics deployment is the lack of high-quality, standardized imaging across institutions. Variability in imaging acquisition protocols, scanner hardware, reconstruction algorithms, and post-processing can alter radiomic features, undermining consistency and reproducibility, and leading to unreliable results. A further limitation is the scarcity of large, publicly available datasets. Since data-hungry AI models require extensive, diverse training cohorts to achieve robust performance,150 the availability of such datasets remains a key challenge. To establish an optimal AI-based predictive model for immunotherapy, it is crucial to integrate multiple layers of patient data, including genomics, imaging, proteomics, and pathological information. Increasingly, pan-cancer studies are being conducted to evaluate the efficacy of PD-1 and PD-L1 therapies, underscoring the importance of complete and standardized datasets that facilitate data sharing across multiple centers.151 Initiatives such as The Cancer Imaging Archive and the Quantitative Imaging Network play a crucial role in addressing these challenges by fostering cross-institutional collaboration and providing access to large and diverse datasets. These collective efforts are essential for improving the precision and generalizability of AI-based predictive models and accelerating their incorporation into clinical practice.
Reliability of Prediction
The reliability and interpretability of AI predictions in immunotherapy remain major challenges. While AI shows promise for forecasting treatment response, model performance often varies due to the complexity of development pipelines and the instability of high-dimensional data. Common issues include overfitting, selection bias, and data leakage, which can compromise clinical reliability even when internal metrics appear favorable. Robust external validation, careful cohort design, and rigorous calibration are therefore essential prerequisites for clinical deployment. Interpretability is equally important for clinical acceptance by patients and healthcare professionals. Recent work has focused on improving transparency through concept learning models, case-based reasoning, counterfactual explanations, concept attribution, and linguistically grounded explanations. Additional strategies include latent-space interpretation, attribution maps, incorporation of anatomical priors, and visualization of internal network representations.152 These advancements are crucial for strengthening trust in AI-based predictions and ensuring their effective integration into clinical practice with a clear understanding of the decision-making process.
Technical Barriers
The incorporation of artificial intelligence into radiomics and pathology holds transformative potential for oncology; however, multiple technical barriers continue to limit widespread adoption. These challenges fall into four broad domains: workforce and tooling, data standardization and infrastructure, model interpretability, and regulatory and systems issues.
DL has reduced several limitations of manual feature selection in radiomics, including time burden and interobserver variability. However, successful deployment still requires advanced computational knowledge. Many radiologists and clinicians lack the programming skills, algorithmic literacy, and workflow familiarity needed to implement these tools independently. Public datasets such as RIDER and The Cancer Imaging Archive support external validation of radiomic signatures, and open-source toolkits such as PyRadiomics, RaCaT, and ImaGene lower the technical threshold by enabling feature extraction without building pipelines from the ground up. These resources, however, are not substitutes for systematic training. Without broader education and sustained cross-disciplinary collaboration, the gap between data scientists and medical professionals will continue to hinder clinical integration.
A major obstacle is the absence of standardized protocols for AI-based pathology and radiomics. Robust model development requires large, high-quality, and consistently labeled datasets. Image annotation is labor-intensive and depends on expert pathologists, whose subjective interpretations can introduce variability, particularly for subtle or qualitatively difficult alterations. The transition from conventional to digital pathology is further slowed by the cost of scanners, specialized software, secure storage, and the expertise required to manage large image files. Without harmonized acquisition, annotation, and storage standards, reproducibility and cross-institutional collaboration remain limited, weakening the reliability of AI-assisted diagnostics.
The “black-box” nature of many deep learning systems remains a significant barrier to clinical adoption. While AI models can achieve high predictive accuracy, their internal decision-making processes are often opaque, making it difficult for clinicians to understand or explain results. This lack of interpretability undermines trust among healthcare providers and patients, who may be reluctant to rely on recommendations that cannot be clearly justified. Involving AI specialists in routine workflows offers only a temporary workaround and is not sustainable at scale. To improve transparency, investigators have developed methods such as attribution maps, counterfactual explanations, concept learning, and visualization of network activations. However, these techniques are still evolving, and acceptance in routine practice remains limited. Progress will depend on intuitive, user-friendly interfaces that translate model reasoning into clinically meaningful narratives, together with uncertainty quantification, standardized reporting, and prospective validation, so that “black box” predictions can be interpreted, communicated, and trusted at the point of care.
Broader systemic and regulatory challenges also affect the clinical deployment of AI. Multi-center studies frequently encounter data heterogeneity, including differences in imaging protocols, annotation standards, and quality-control procedures that undermine reproducibility. Legal and ethical constraints related to patient privacy and data security further limit data sharing across institutions and national borders, restricting the size and diversity of datasets available for model development and validation. Regulatory frameworks for medical AI remain fragmented, with uneven requirements for analytical validation, clinical trial design, post-market surveillance, and approval pathways. To overcome these barriers, the field requires harmonized international guidelines, common data elements and reporting standards, and secure, interoperable platforms that support cross-institutional data exchange while protecting privacy. Without coordinated global efforts, AI systems risk remaining confined to experimental use, unable to achieve the robustness, generalizability, and trustworthiness required for routine oncology practice. Addressing these technical, systemic, and interpretability challenges will be pivotal for clinical translation. Investment in education, infrastructure, and standardization, coupled with transparent model design, uncertainty quantification, and rigorous external validation, can accelerate progress. Through coordinated collaboration among clinicians, data scientists, engineers, and policymakers, AI systems can evolve from experimental tools into integral components of precision oncology, improving diagnostic accuracy, therapeutic decision-making, and patient outcomes.
Conclusion
In summary, AI-based algorithms have great potential in identifying tumor biomarkers and evaluating immunotherapy efficacy, providing a noninvasive avenue for individualized assessment and prediction in NSCLC. These tools are expected to augment, rather than replace, clinical judgment and therefore require appropriate oversight and governance. Rigorous external and prospective validation remains essential before full integration into clinical routine practice. Despite current challenges, the long-term outlook for precision oncology is favorable: as methods mature and standards are established, AI should enable more objective and precise disease characterization and ultimately improve patient care and outcomes.
Abbreviations
ICIs, Immune checkpoint inhibitors; NSCLC, Non-small cell lung cancer; AI, Artificial intelligence; CAR, Chimeric antigen receptor; ACT, Adoptive cell therapy; PD-1, Programmed cell death protein 1; PD-L1, Programmed death-ligand 1; CTLA-4, Cytotoxic T-lymphocyte-associated protein 4; TMB, Tumor mutational burden; MSI-H/dMMR, Microsatellite instability–high/deficient mismatch repair; TME, Tumor microenvironment; ML, Machine learning; DL, Deep learning; WSI, Whole-slide image; H&E, Hematoxylin and eosin; CNN, Convolutional neural network; CT, Computed tomography; PET, Positron emission tomography; MRI, Magnetic resonance imaging; AUC, Area under the curve; LUAD, Lung adenocarcinoma; MHC, Major histocompatibility complex; WES, Whole-exome sequencing; qRT-PCR, Quantitative real-time polymerase chain reaction; TILs, Tumor-infiltrating lymphocytes; TLSs, Tertiary lymphoid structures; VEGF, Vascular endothelial growth factor; ViT, Vision Transformer; TPS, Tumor proportion score; CPS, Combined positive score; RF, Random forest; XGBoost, Extreme Gradient Boosting; LASSO, Least absolute shrinkage and selection operator; LCI-RPV, Lung Cancer Immunotherapy Radiomics Prediction Vector; HPD, Hyperprogressive disease; LSCC, Lung squamous cell carcinoma; HR, Hazard ratio; PFS, Progression-free survival; OS, Overall survival; C-index, Concordance index; iRECIST, Immune-related Response Evaluation Criteria in Solid Tumors; ctDNA, Circulating tumor DNA; MRD, Minimal residual disease; NLR, Neutrophil-to-lymphocyte ratio; LIPS, Liquid immune profile–based signature; MS, Mass spectrometry; SVM, Support vector machine; SC-CNN, Spatially Constrained Convolutional Neural Network; IRGs, Immunoregulation-related genes; IRGI, Immunoregulation-related gene index; SHAP, SHapley Additive exPlanations; MET, mesenchymal–epithelial transition; irAEs, Immune-related adverse events; CIP/iCIP, (Immune) checkpoint inhibitor-related pneumonitis; RP, Radiation pneumonitis; U-Net, U-shaped convolutional neural network.
Data Sharing Statement
Data sharing is not applicable to this article as no data were created or analysed in this study.
Ethics Statement
This review article does not involve any original studies with human participants or animals. Therefore, ethical approval and informed consent were not required.
Author Contributions
Conceptualization and clinical orientation of the review topic, Qiang Wen and Zhe Yang; Methodology and formal analytical framework, Pingdong Cao; Investigation and systematic literature screening, Yuqi Yang; Data curation and data interpretation, Jian Zhu and Xi Wang; Data visualization and results interpretation, Xiao Jia and Xiaomei Li; Writing – original draft preparation, Qiang Wen and Pingdong Cao; Writing – critical review and substantive revision, Pingdong Cao, Xiao Jia, Yuqi Yang, Xi Wang, Jian Zhu, Xiaomei Li, Zhe Yang and Qiang Wen; Supervision, Qiang Wen and Zhe Yang; Funding acquisition, Qiang Wen. All authors contributed to manuscript revision and approved the submitted version. All authors have read and agreed to the published version of the manuscript. All authors have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Natural Science Foundation of Shandong Province (grant number ZR2024MH268), Shandong Provincial Medical System Staff Science and Technology Innovation Program (grant number SDYWZGKCJH2022018) and Jinan Science and Technology Clinical Medicine Innovation Plan (grant number 20238073). The funding sources had no role in the study design, data collection, analysis of interpretation, or writing of this manuscript.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Hendriks LE, Remon J, Faivre-Finn C, et al. Non-small-cell lung cancer. Nat Rev Dis Primers. 2024;10(1):71. doi:10.1038/s41572-024-00551-9
2. Liu B, Zhou H, Tan L, Siu KTH, Guan X-Y. Exploring treatment options in cancer: tumor treatment strategies. Signal Transduct Target Ther. 2024;9(1):175.
3. Li CL, Yuan X, Yi P. The role of immunotherapy in lung cancer treatment: current strategies, future directions, and insights into metastasis and immune microenvironment. Current Gene Ther. 2025;25(4):453–22. doi:10.2174/0115665232340926241105064739
4. Wu Z, Li S, Zhu X. The mechanism of stimulating and mobilizing the immune system enhancing the anti-tumor immunity. Front Immunol. 2021;12:682435. doi:10.3389/fimmu.2021.682435
5. Sahu M, Suryawanshi H. Immunotherapy: the future of cancer treatment. J Oral Maxillofacial Pathol. 2021;25(2):371. doi:10.4103/0973-029X.325257
6. Shiravand Y, Khodadadi F, Kashani SMA, et al. Immune checkpoint inhibitors in cancer therapy. Current Oncol. 2022;29(5):3044–3060. doi:10.3390/curroncol29050247
7. Doroshow DB, Bhalla S, Beasley MB, et al. PD-L1 as a biomarker of response to immune-checkpoint inhibitors. Nat Rev Clin Oncol. 2021;18(6):345–362. doi:10.1038/s41571-021-00473-5
8. Aggarwal C, Ben-Shachar R, Gao Y, et al. Assessment of tumor mutational burden and outcomes in patients with diverse advanced cancers treated with immunotherapy. JAMA Network Open. 2023;6(5):e2311181–e. doi:10.1001/jamanetworkopen.2023.11181
9. Addeo A, Friedlaender A, Banna GL, Weiss GJ. TMB or not TMB as a biomarker: that is the question. Crit Rev Oncol. 2021;163:103374. doi:10.1016/j.critrevonc.2021.103374
10. Shen X, Zhao B. Efficacy of PD-1 or PD-L1 inhibitors and PD-L1 expression status in cancer: meta-analysis. BMJ. 2018;362. doi:10.1136/bmj.k3529
11. Lu C, Liu Y, Ali NM, Zhang B, Cui X. The role of innate immune cells in the tumor microenvironment and research progress in anti-tumor therapy. Front Immunol. 2023;13:1039260. doi:10.3389/fimmu.2022.1039260
12. Jiang P, Sinha S, Aldape K, Hannenhalli S, Sahinalp C, Ruppin E. Big data in basic and translational cancer research. Nat Rev Cancer. 2022;22(11):625–639. doi:10.1038/s41568-022-00502-0
13. Zhou H, Zhou F, Zhao C, Xu Y, Luo L, Chen H. Multimodal data integration for precision oncology: challenges and future directions. arXiv preprint arXiv:240619611. 2024.
14. Boehm KM, Khosravi P, Vanguri R, Gao J, Shah SP. Harnessing multimodal data integration to advance precision oncology. Nat Rev Cancer. 2022;22(2):114–126. doi:10.1038/s41568-021-00408-3
15. Waqas A, Tripathi A, Ramachandran RP, Stewart PA, Rasool G. Multimodal data integration for oncology in the era of deep neural networks: a review. Front Artificial Intell. 2024;7:1408843. doi:10.3389/frai.2024.1408843
16. Cammarota G, Ianiro G, Ahern A, et al. Gut microbiome, big data and machine learning to promote precision medicine for cancer. Nat Rev Gastroenterol Hepatol. 2020;17(10):635–648. doi:10.1038/s41575-020-0327-3
17. Sarker IH. Machine learning: algorithms, real-world applications and research directions. SN Comp Sci. 2021;2(3):160. doi:10.1007/s42979-021-00592-x
18. Sarker IH. Deep learning: a comprehensive overview on techniques, taxonomy, applications and research directions. SN Comp Sci. 2021;2(6):1–20. doi:10.1007/s42979-021-00815-1
19. Rane NL, Paramesha M, Choudhary SP, Rane J. Machine learning and deep learning for big data analytics: a review of methods and applications. Partners Universal Int Innovation J. 2024;2(3):172–197.
20. Xie J, Luo X, Deng X, et al. Advances in artificial intelligence to predict cancer immunotherapy efficacy. Front Immunol. 2023;13:1076883. doi:10.3389/fimmu.2022.1076883
21. Wen Q, Qiu L, Qiu C, et al. Artificial intelligence in predicting efficacy and toxicity of immunotherapy: applications, challenges, and future directions. Cancer Lett. 2025;630:217881. doi:10.1016/j.canlet.2025.217881
22. Kann BH, Hosny A, Aerts HJ. Artificial intelligence for clinical oncology. Cancer Cell. 2021;39(7):916–927. doi:10.1016/j.ccell.2021.04.002
23. Wu B, Moeckel G. Application of digital pathology and machine learning in the liver, kidney and lung diseases. J Pathol Inform. 2023;14:100184. doi:10.1016/j.jpi.2022.100184
24. Mienye ID, Swart TG. A comprehensive review of deep learning: architectures, recent advances, and applications. Information. 2024;15(12):755. doi:10.3390/info15120755
25. El Nahhas OS, Van Treeck M, Wölflein G, et al. From whole-slide image to biomarker prediction: end-to-end weakly supervised deep learning in computational pathology. Nat Protocols. 2025;20(1):293–316. doi:10.1038/s41596-024-01047-2
26. Kang Y, Vijay S, Gujral TS. Deep neural network modeling identifies biomarkers of response to immune-checkpoint therapy. iScience. 2022;25(5):104228. doi:10.1016/j.isci.2022.104228
27. Hussain D, Al-Masni MA, Aslam M, et al. Revolutionizing tumor detection and classification in multimodality imaging based on deep learning approaches: methods, applications and limitations. J X-Ray Sci Technol. 2024;32(4):857–911. doi:10.3233/XST-230429
28. Feretzakis G, Juliebø-Jones P, Tsaturyan A, et al. Emerging trends in AI and radiomics for bladder, kidney, and prostate cancer: a critical review. Cancers. 2024;16(4):810. doi:10.3390/cancers16040810
29. Bera K, Braman N, Gupta A, Velcheti V, Madabhushi A. Predicting cancer outcomes with radiomics and artificial intelligence in radiology. Nat Rev Clin Oncol. 2022;19(2):132–146. doi:10.1038/s41571-021-00560-7
30. Hu A, Sun L, Lin H, Liao Y, Yang H, Mao Y. Harnessing innate immune pathways for therapeutic advancement in cancer. Signal Transd Targeted Ther. 2024;9(1):68.
31. Maffuid K, Cao Y. Decoding the complexity of immune–cancer cell interactions: empowering the future of cancer immunotherapy. Cancers. 2023;15(16):4188. doi:10.3390/cancers15164188
32. Camps J, Jiménez-Franco A, García-Pablo R, Joven J, Arenas M. Artificial intelligence-driven integration of multi-omics and radiomics: a new hope for precision cancer diagnosis and prognosis. BBA. 2025;1871(6):167841. doi:10.1016/j.bbadis.2025.167841
33. Xu Z, Li W, Dong X, et al. Precision medicine in colorectal cancer: leveraging multi-omics, spatial omics, and artificial intelligence. Clin Chim Acta. 2024;559:119686. doi:10.1016/j.cca.2024.119686
34. Sha L, Osinski BL, Ho IY, et al. Multi-field-of-view deep learning model predicts nonsmall cell lung cancer programmed death-ligand 1 status from whole-slide hematoxylin and eosin images. J Pathol Inform. 2019;10(1):24. doi:10.4103/jpi.jpi_24_19
35. Huang Z, Chen L, Lv L, et al. A new AI-assisted scoring system for PD-L1 expression in NSCLC. Comput Methods Programs Biomed. 2022;221:106829. doi:10.1016/j.cmpb.2022.106829
36. Ligero M, Serna G, El Nahhas OS, et al. Weakly supervised deep learning predicts immunotherapy response in solid tumors based on PD-L1 expression. Canc Res Commun. 2024;4(1):92–102. doi:10.1158/2767-9764.CRC-23-0287
37. Lin -Y-Y, Wang L-C, Hsieh Y-H, et al. Computer-assisted three-dimensional quantitation of programmed death-ligand 1 in non-small cell lung cancer using tissue clearing technology. J Transl Med. 2022;20(1):131. doi:10.1186/s12967-022-03335-5
38. Tian P, He B, Mu W, et al. Assessing PD-L1 expression in non-small cell lung cancer and predicting responses to immune checkpoint inhibitors using deep learning on computed tomography images. Theranostics. 2021;11(5):2098. doi:10.7150/thno.48027
39. Liu Z, Yao Y, Zhao M, et al. Radiomics models derived from arterial-phase-enhanced CT reliably predict both PD-L1 expression and immunotherapy prognosis in non-small cell lung cancer: a retrospective, multicenter cohort study. Acad Radiol. 2025;32(1):493–505. doi:10.1016/j.acra.2024.07.028
40. Wang C, Ma J, Shao J, et al. Non-invasive measurement using deep learning algorithm based on multi-source features fusion to predict PD-L1 expression and survival in NSCLC. Front Immunol. 2022;13:828560. doi:10.3389/fimmu.2022.828560
41. Li J, Ge S, Sang S, Hu C, Deng S. Evaluation of PD-L1 expression level in patients with non-small cell lung cancer by 18F-FDG PET/CT radiomics and clinicopathological characteristics. Front Oncol. 2021;11:789014. doi:10.3389/fonc.2021.789014
42. Jiang M, Sun D, Guo Y, et al. Assessing PD-L1 expression level by radiomic features from PET/CT in nonsmall cell lung cancer patients: an initial result. Acad Radiol. 2020;27(2):171–179. doi:10.1016/j.acra.2019.04.016
43. Chen M, Lu H, Copley SJ, et al. A novel radiogenomics biomarker for predicting treatment response and pneumotoxicity from programmed cell death protein or ligand-1 inhibition immunotherapy in NSCLC. J Thorac Oncol. 2023;18(6):718–730. doi:10.1016/j.jtho.2023.01.089
44. Sadhwani A, Chang H-W, Behrooz A, et al. Comparative analysis of machine learning approaches to classify tumor mutation burden in lung adenocarcinoma using histopathology images. Sci Rep. 2021;11(1):16605. doi:10.1038/s41598-021-95747-4
45. Chen S, Xiang J, Wang X, et al. Deep learning-based approach to reveal tumor mutational burden status from whole slide images across multiple cancer types. arXiv preprint arXiv:220403257. 2022.
46. Niu Y, Wang L, Zhang X, et al. Predicting tumor mutational burden from lung adenocarcinoma histopathological images using deep learning. Front Oncol. 2022;12:927426. doi:10.3389/fonc.2022.927426
47. Jain MS, Massoud TF. Predicting tumour mutational burden from histopathological images using multiscale deep learning. Nature Mach Intell. 2020;2(6):356–362. doi:10.1038/s42256-020-0190-5
48. Wen Q, Yang Z, Dai H, Feng A, Li Q. Radiomics study for predicting the expression of PD-L1 and tumor mutation burden in non-small cell lung cancer based on CT images and clinicopathological features. Front Oncol. 2021;11:620246. doi:10.3389/fonc.2021.620246
49. He B, Dong D, She Y, et al. Predicting response to immunotherapy in advanced non-small-cell lung cancer using tumor mutational burden radiomic biomarker. J Immuno Ther Cancer. 2020;8(2):e000550. doi:10.1136/jitc-2020-000550
50. Wang J, Chen P, Su M, Zhong G, Zhang S, Gou D. Integrative modeling of multiomics data for predicting tumor mutation burden in patients with lung cancer. Biomed Res Int. 2022;2022(1):2698190. doi:10.1155/2022/2698190
51. Wang X, Barrera C, Bera K, et al. Spatial interplay patterns of cancer nuclei and tumor-infiltrating lymphocytes (TILs) predict clinical benefit for immune checkpoint inhibitors. Sci Adv. 2022;8(22):eabn3966. doi:10.1126/sciadv.abn3966
52. Cai S, Yang G, Hu M, et al. Spatial cell interplay networks of regulatory T cells predict recurrence in patients with operable non-small cell lung cancer. Cancer Immunol Immunother. 2024;73(10):189. doi:10.1007/s00262-024-03762-x
53. Chen Y, Xu T, Jiang C, You S, Cheng Z, Gong J. CT-based radiomics signature to predict CD8+ tumor infiltrating lymphocytes in non-small-cell lung cancer. Acta Radiol. 2023;64(4):1390–1399. doi:10.1177/02841851221126596
54. Lin H, Pan X, Feng Z, et al. Automated whole-slide images assessment of immune infiltration in resected non-small-cell lung cancer: towards better risk-stratification. J Transl Med. 2022;20(1):261. doi:10.1186/s12967-022-03458-9
55. Zhou J, Zou S, Kuang D, Yan J, Zhao J, Zhu X. A novel approach using FDG-PET/CT-based radiomics to assess tumor immune phenotypes in patients with non-small cell lung cancer. Front Oncol. 2021;11:769272. doi:10.3389/fonc.2021.769272
56. Chen Z, Wang X, Jin Z, et al. Deep learning on tertiary lymphoid structures in hematoxylin-eosin predicts cancer prognosis and immunotherapy response. NPJ Precision Oncol. 2024;8(1):73. doi:10.1038/s41698-024-00579-w
57. Yu Y, Yang T, Ma P, et al. Determining the status of tertiary lymphoid structures in invasive pulmonary adenocarcinoma based on chest CT radiomic features. Insights Into Imaging. 2025;16(1):28. doi:10.1186/s13244-025-01906-w
58. Yi F, Yang L, Wang S, et al. Microvessel prediction in H&E Stained Pathology Images using fully convolutional neural networks. BMC Bioinf. 2018;19(1):64. doi:10.1186/s12859-018-2055-z
59. Li B, Yang L, Zhang H, et al. Outcome-supervised deep learning on pathologic whole slide images for survival prediction of immunotherapy in patients with non–small cell lung cancer. Mod Pathol. 2023;36(8):100208. doi:10.1016/j.modpat.2023.100208
60. Wang S, Rong R, Yang DM, et al. Computational staining of pathology images to study the tumor microenvironment in lung cancer. Cancer Res. 2020;80(10):2056–2066. doi:10.1158/0008-5472.CAN-19-1629
61. Fehrenbacher L, Spira A, Ballinger M, et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, open-label, Phase 2 randomised controlled trial. Lancet. 2016;387(10030):1837–1846. doi:10.1016/S0140-6736(16)00587-0
62. Mok TS, Wu Y-L, Kudaba I, et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, Phase 3 trial. Lancet. 2019;393(10183):1819–1830. doi:10.1016/S0140-6736(18)32409-7
63. Lantuejoul S, Sound-Tsao M, Cooper WA, et al. PD-L1 testing for lung cancer in 2019: perspective from the IASLC pathology committee. J Thorac Oncol. 2020;15(4):499–519. doi:10.1016/j.jtho.2019.12.107
64. Udall M, Rizzo M, Kenny J, et al. PD-L1 diagnostic tests: a systematic literature review of scoring algorithms and test-validation metrics. Diagn Pathol. 2018;13(1):12. doi:10.1186/s13000-018-0689-9
65. Keppens C, Dequeker EM, Pauwels P, Ryska A, ‘t Hart N, von der Thüsen JH. PD-L1 immunohistochemistry in non-small-cell lung cancer: unraveling differences in staining concordance and interpretation. Virchows Archiv. 2021;478(5):827–839. doi:10.1007/s00428-020-02976-5
66. Meléndez B, Van Campenhout C, Rorive S, Remmelink M, Salmon I, D’Haene N. Methods of measurement for tumor mutational burden in tumor tissue. Transl Lung Cancer Res. 2018;7(6):661. doi:10.21037/tlcr.2018.08.02
67. Gandara DR, Agarwal N, Gupta S, et al. Tumor mutational burden and survival on immune checkpoint inhibition in> 8000 patients across 24 cancer types. J Immuno Ther Cancer. 2025;13(2):e010311. doi:10.1136/jitc-2024-010311
68. Sorich MJ, Manning-Bennett AT, Li LX, et al. Tumour mutational burden and immune checkpoint inhibitor response in non-small cell lung cancer: a continuous modelling approach. Targeted Oncol. 2025;20(2):361–369. doi:10.1007/s11523-024-01124-2
69. Palmeri M, Mehnert J, Silk A, et al. Real-world application of tumor mutational burden-high (TMB-high) and microsatellite instability (MSI) confirms their utility as immunotherapy biomarkers. ESMO Open. 2022;7(1):100336. doi:10.1016/j.esmoop.2021.100336
70. Carbone DP, Reck M, Paz-Ares L, et al. First-line nivolumab in stage IV or recurrent non–small-cell lung cancer. N Engl J Med. 2017;376(25):2415–2426. doi:10.1056/NEJMoa1613493
71. Zheng S, Wang W, Shen L, Yao Y, Xia W, Ni C. Tumor battlefield within inflamed, excluded or desert immune phenotypes: the mechanisms and strategies. Exp Hematol Oncol. 2024;13(1):80.
72. Shen J, Choi Y-L, Lee T, et al. Inflamed immune phenotype predicts favorable clinical outcomes of immune checkpoint inhibitor therapy across multiple cancer types. J Immuno Ther Cancer. 2024;12(2):e008339. doi:10.1136/jitc-2023-008339
73. Li Y, Wang P, Xu J, Shi X, Yin T, Teng F. Noninvasive radiomic biomarkers for predicting pseudoprogression and hyperprogression in patients with non-small cell lung cancer treated with immune checkpoint inhibition. Oncoimmunology. 2024;13(1):2312628. doi:10.1080/2162402X.2024.2312628
74. Park HJ, Kim KW, Won SE, et al. Definition, incidence, and challenges for assessment of hyperprogressive disease during cancer treatment with immune checkpoint inhibitors: a systematic review and meta-analysis. JAMA network open. JAMA Network Open. 2021;4(3):e211136–e. doi:10.1001/jamanetworkopen.2021.1136
75. Tay C, Qian Y, Sakaguchi S. Hyper-progressive disease: the potential role and consequences of T-regulatory cells foiling anti-PD-1 cancer immunotherapy. Cancers. 2020;13(1):48. doi:10.3390/cancers13010048
76. Marcucci F, Rumio C. The tumor-promoting effects of the adaptive immune system: a cause of hyperprogressive disease in cancer? Cell Mol Life Sci. 2021;78(3):853–865. doi:10.1007/s00018-020-03606-8
77. Shen P, Han L, Ba X, Qin K, Tu S. Hyperprogressive disease in cancers treated with immune checkpoint inhibitors. Front Pharmacol. 2021;12:678409. doi:10.3389/fphar.2021.678409
78. Vaidya P, Bera K, Patil PD, et al. Novel, non-invasive imaging approach to identify patients with advanced non-small cell lung cancer at risk of hyperprogressive disease with immune checkpoint blockade. J Immuno Ther Cancer. 2020;8(2):e001343. doi:10.1136/jitc-2020-001343
79. Zhang M, Cui J, Chen H, et al. Increased SOAT2 expression in aged regulatory T cells is associated with altered cholesterol metabolism and reduced anti-tumor immunity. Nat Commun. 2025;16(1):630. doi:10.1038/s41467-025-56002-w
80. Trebeschi S, Drago S, Birkbak N, et al. Predicting response to cancer immunotherapy using noninvasive radiomic biomarkers. Ann Oncol. 2019;30(6):998–1004. doi:10.1093/annonc/mdz108
81. Wu S, Zhan W, Liu L, et al. Pretreatment radiomic biomarker for immunotherapy responder prediction in stage IB–IV NSCLC (LCDigital-IO Study): a multicenter retrospective study. J Immuno Ther Cancer. 2023;11(10):e007369. doi:10.1136/jitc-2023-007369
82. Ye G, Wu G, Qi Y, et al. Non-invasive multimodal CT deep learning biomarker to predict pathological complete response of non-small cell lung cancer following neoadjuvant immunochemotherapy: a multicenter study. J Immuno Ther Cancer. 2024;12(9):e009348. doi:10.1136/jitc-2024-009348
83. Ren Q, Xiong F, Zhu P, et al. Assessing the robustness of radiomics/deep learning approach in the identification of efficacy of anti–PD-1 treatment in advanced or metastatic non-small cell lung carcinoma patients. Front Oncol. 2022;12:952749. doi:10.3389/fonc.2022.952749
84. Liu Y, Wu M, Zhang Y, et al. Imaging biomarkers to predict and evaluate the effectiveness of immunotherapy in advanced non-small-cell lung cancer. Front Oncol. 2021;11:657615. doi:10.3389/fonc.2021.657615
85. Liao C-Y, Chen Y-M, Wu Y-T, et al. Personalized prediction of immunotherapy response in lung cancer patients using advanced radiomics and deep learning. Cancer Imaging. 2024;24(1):129. doi:10.1186/s40644-024-00779-4
86. Cousin F, Louis T, Dheur S, et al. Radiomics and delta-radiomics signatures to predict response and survival in patients with non-small-cell lung cancer treated with immune checkpoint inhibitors. Cancers. 2023;15(7):1968. doi:10.3390/cancers15071968
87. Khorrami M, Prasanna P, Gupta A, et al. Changes in CT radiomic features associated with lymphocyte distribution predict overall survival and response to immunotherapy in non–small cell lung cancer. Cancer Immunol Res. 2020;8(1):108–119. doi:10.1158/2326-6066.CIR-19-0476
88. Valentinuzzi D, Vrankar M, Boc N, et al. [18F] FDG PET immunotherapy radiomics signature (iRADIOMICS) predicts response of non-small-cell lung cancer patients treated with pembrolizumab. Radiol Oncol. 2020;54(3):285. doi:10.2478/raon-2020-0042
89. Lin X, Liu Z, Zhou K, et al. Intratumoral and peritumoral PET/CT-based radiomics for non-invasively and dynamically predicting immunotherapy response in NSCLC. Br J Cancer. 2025;132(6):558–568. doi:10.1038/s41416-025-02948-z
90. Tankyevych O, Trousset F, Latappy C, et al. Development of radiomic-based model to predict clinical outcomes in non-small cell lung cancer patients treated with immunotherapy. Cancers. 2022;14(23):5931. doi:10.3390/cancers14235931
91. Silva SB, Wanderley CWS, Gomes Marin JF, et al. Tumor glycolytic profiling through 18F-FDG PET/CT predicts immune checkpoint inhibitor efficacy in advanced NSCLC. Therapeut Adv Med Oncol. 2022;14:17588359221138386. doi:10.1177/17588359221138386
92. Tricarico P, Humbert O, Chardin D. Clinical evaluation of AI-generated total metabolic tumor volume on 18F-FDG PET/CT for patients with metastatic lung cancer treated with immunotherapy. Médecine Nucléaire. 2024;48(2):46–47. doi:10.1016/j.mednuc.2024.01.005
93. Mu W, Tunali I, Gray JE, Qi J, Schabath MB, Gillies RJ. Radiomics of 18F-FDG PET/CT images predicts clinical benefit of advanced NSCLC patients to checkpoint blockade immunotherapy. Eur J Nucl Med Mol Imaging. 2020;47(5):1168–1182. doi:10.1007/s00259-019-04625-9
94. Tong H, Sun J, Fang J, et al. A machine learning model based on PET/CT radiomics and clinical characteristics predicts tumor immune profiles in non-small cell lung cancer: a retrospective multicohort study. Front Immunol. 2022;13:859323. doi:10.3389/fimmu.2022.859323
95. Xu J, Wang P, Li Y, et al. Development and validation of an MRI-Based nomogram to predict the effectiveness of immunotherapy for brain metastasis in patients with non-small cell lung cancer. Front Immunol. 2024;15:1373330. doi:10.3389/fimmu.2024.1373330
96. Barabino E, Rossi G, Pamparino S, et al. Exploring response to immunotherapy in non-small cell lung cancer using delta-radiomics. Cancers. 2022;14(2):350. doi:10.3390/cancers14020350
97. Sirinukunwattana K, Raza SEA, Tsang Y-W, Snead DR, Cree IA, Rajpoot NM. Locality sensitive deep learning for detection and classification of nuclei in routine colon cancer histology images. IEEE Transactions Med Imag. 2016;35(5):1196–1206. doi:10.1109/TMI.2016.2525803
98. Park S, Ock C-Y, Kim H, et al. Artificial intelligence–powered spatial analysis of tumor-infiltrating lymphocytes as complementary biomarker for immune checkpoint inhibition in non–small-cell lung cancer. J Clin Oncol. 2022;40(17):1916–1928. doi:10.1200/JCO.21.02010
99. Han D, Li H, Zheng X, et al. Whole slide image-based weakly supervised deep learning for predicting major pathological response in non-small cell lung cancer following neoadjuvant chemoimmunotherapy: a multicenter, retrospective, cohort study. Front Immunol. 2024;15:1453232. doi:10.3389/fimmu.2024.1453232
100. Rakaee M, Tafavvoghi M, Ricciuti B, et al. Deep learning model for predicting immunotherapy response in advanced Non− Small cell lung cancer. JAMA Oncol. 2025;11(2):109–118. doi:10.1001/jamaoncol.2024.5356
101. Patkar S, Chen A, Basnet A, et al. Predicting the tumor microenvironment composition and immunotherapy response in non-small cell lung cancer from digital histopathology images. NPJ Precision Oncol. 2024;8(1):280. doi:10.1038/s41698-024-00765-w
102. Hu J, Cui C, Yang W, et al. Using deep learning to predict anti-PD-1 response in melanoma and lung cancer patients from histopathology images. Transl Oncol. 2021;14(1):100921. doi:10.1016/j.tranon.2020.100921
103. Kim H, Kim S, Choi S, et al. Clinical Validation of artificial intelligence–powered PD-L1 tumor proportion score interpretation for immune checkpoint inhibitor response prediction in non–small cell lung cancer. JCO Precis Oncol. 2024;8:e2300556.
104. Guo H, Diao L, Zhou X, et al. Artificial intelligence-based analysis for immunohistochemistry staining of immune checkpoints to predict resected non-small cell lung cancer survival and relapse. Transl Lung Cancer Res. 2021;10(6):2452. doi:10.21037/tlcr-21-96
105. Baxi V, Lee G, Duan C, et al. Association of artificial intelligence-powered and manual quantification of programmed death-ligand 1 (PD-L1) expression with outcomes in patients treated with nivolumab±ipilimumab. Mod Pathol. 2022;35(11):1529–1539. doi:10.1038/s41379-022-01119-2
106. Pan X, Lin H, Han C, et al. Computerized tumor-infiltrating lymphocytes density score predicts survival of patients with resectable lung adenocarcinoma. iScience. 2022;25(12):105605. doi:10.1016/j.isci.2022.105605
107. Wang Y, Ju X, Hua R, et al. Deep learning analysis of histopathological images predicts immunotherapy prognosis and reveals tumour microenvironment features in non-small cell lung cancer. Br J Cancer. 2024;131(11):1833–1845. doi:10.1038/s41416-024-02856-8
108. Shvetsov N, Grønnesby M, Pedersen E, et al. A pragmatic machine learning approach to quantify tumor-infiltrating lymphocytes in whole slide images. Cancers. 2022;14(12):2974. doi:10.3390/cancers14122974
109. Dia AK, Kolnohuz A, Yolchuyeva S, et al. Computational analysis of whole slide images predicts PD-L1 expression and progression-free survival in immunotherapy-treated non-small cell lung cancer patients. J Transl Med. 2025;23(1):510. doi:10.1186/s12967-025-06487-2
110. Ko J, Baldassano SN, Loh P-L, Kording K, Litt B, Issadore D. Machine learning to detect signatures of disease in liquid biopsies–a user’s guide. Lab Chip. 2018;18(3):395–405. doi:10.1039/C7LC00955K
111. Peng Y, Mei W, Ma K, Zeng C. Circulating tumor DNA and minimal residual disease (MRD) in solid tumors: current horizons and future perspectives. Front Oncol. 2021;11:763790. doi:10.3389/fonc.2021.763790
112. Widman AJ, Shah M, Frydendahl A, et al. Ultrasensitive plasma-based monitoring of tumor burden using machine-learning-guided signal enrichment. Nature Med. 2024;30(6):1655–1666. doi:10.1038/s41591-024-03040-4
113. Guibert N, Mazieres J, Delaunay M, et al. Monitoring of KRAS-mutated ctDNA to discriminate pseudo-progression from true progression during anti-PD-1 treatment of lung adenocarcinoma. Oncotarget. 2017;8(23):38056. doi:10.18632/oncotarget.16935
114. Benzekry S, Grangeon M, Karlsen M, et al. Machine learning for prediction of immunotherapy efficacy in non-small cell lung cancer from simple clinical and biological data. Cancers. 2021;13(24):6210. doi:10.3390/cancers13246210
115. Zhou J-G, Donaubauer A-J, Frey B, et al. Prospective development and validation of a liquid immune profile-based signature (LIPS) to predict response of patients with recurrent/metastatic cancer to immune checkpoint inhibitors. J Immuno Ther Cancer. 2021;9(2):e001845. doi:10.1136/jitc-2020-001845
116. Park Y, Kim MJ, Choi Y, et al. Role of mass spectrometry-based serum proteomics signatures in predicting clinical outcomes and toxicity in patients with cancer treated with immunotherapy. J Immuno Ther Cancer. 2022;10(3):e003566. doi:10.1136/jitc-2021-003566
117. Patel AJ, Tan T-M, Richter AG, Naidu B, Blackburn JM, Middleton GW. A highly predictive autoantibody-based biomarker panel for prognosis in early-stage NSCLC with potential therapeutic implications. Br J Cancer. 2022;126(2):238–246. doi:10.1038/s41416-021-01572-x
118. Chae YK, Kim WB, Davis AA, et al. Mass spectrometry-based serum proteomic signature as a potential biomarker for survival in patients with non-small cell lung cancer receiving immunotherapy. Transl Lung Cancer Res. 2020;9(4):1015. doi:10.21037/tlcr-20-148
119. Muller M, Hummelink K, Hurkmans DP, et al. A serum protein classifier identifying patients with advanced non–small cell lung cancer who derive clinical benefit from treatment with immune checkpoint inhibitors. Clin Cancer Res. 2020;26(19):5188–5197. doi:10.1158/1078-0432.CCR-20-0538
120. Peña-Romero AC, Orenes-Piñero E. Dual effect of immune cells within tumour microenvironment: pro-and anti-tumour effects and their triggers. Cancers. 2022;14(7):1681. doi:10.3390/cancers14071681
121. Abdul-Rahman T, Ghosh S, Badar SM, et al. The paradoxical role of cytokines and chemokines at the tumor microenvironment: a comprehensive review. Eur J Med Res. 2024;29(1):124. doi:10.1186/s40001-024-01711-z
122. Pei B, Peng S, Huang C, Zhou F. Bifidobacterium modulation of tumor immunotherapy and its mechanism. Cancer Immunol Immunother. 2024;73(5):94. doi:10.1007/s00262-024-03665-x
123. Shoji F, Yamashita T, Kinoshita F, et al. Artificial intelligence-derived gut microbiome as a predictive biomarker for therapeutic response to immunotherapy in lung cancer: protocol for a multicentre, prospective, observational study. BMJ Open. 2022;12(6):e061674. doi:10.1136/bmjopen-2022-061674
124. Liu B, Chau J, Dai Q, Zhong C, Zhang J. Exploring gut microbiome in predicting the efficacy of immunotherapy in non-small cell lung cancer. Cancers. 2022;14(21):5401. doi:10.3390/cancers14215401
125. Gong -T-T, He X-H, Gao S, Wu Q-J. Application of machine learning in prediction of chemotherapy resistant of ovarian cancer based on gut microbiota. J Cancer. 2021;12(10):2877. doi:10.7150/jca.46621
126. McCulloch JA, Davar D, Rodrigues RR, et al. Intestinal microbiota signatures of clinical response and immune-related adverse events in melanoma patients treated with anti-PD-1. Nature Med. 2022;28(3):545–556. doi:10.1038/s41591-022-01698-2
127. Mu W, Jiang L, Zhang J, et al. Non-invasive decision support for NSCLC treatment using PET/CT radiomics. Nat Commun. 2020;11(1):5228. doi:10.1038/s41467-020-19116-x
128. Fomin V, So WV, Barbieri RA, et al. Machine learning identifies clinical tumor mutation landscape pathways of resistance to checkpoint inhibitor therapy in NSCLC. J Immuno Ther Cancer. 2025;13(3):e009092. doi:10.1136/jitc-2024-009092
129. Wang M, Wang Y, Li Y, Zhang C, Li C, Bi N. Interpretable artificial intelligence based on immunoregulation-related genes predicts prognosis and immunotherapy response in lung adenocarcinoma. Front Bioinform. 2025;5:1613761. doi:10.3389/fbinf.2025.1613761
130. Sun R, Limkin EJ, Vakalopoulou M, et al. A radiomics approach to assess tumour-infiltrating CD8 cells and response to anti-PD-1 or anti-PD-L1 immunotherapy: an imaging biomarker, retrospective multicohort study. Lancet Oncol. 2018;19(9):1180–1191. doi:10.1016/S1470-2045(18)30413-3
131. Yang Y, Yang J, Shen L, et al. A multi-omics-based serial deep learning approach to predict clinical outcomes of single-agent anti-PD-1/PD-L1 immunotherapy in advanced stage non-small-cell lung cancer. Am J Transl Res. 2021;13(2):743.
132. Farina B, Guerra ADR, Bermejo-Peláez D, et al. Integration of longitudinal deep-radiomics and clinical data improves the prediction of durable benefits to anti-PD-1/PD-L1 immunotherapy in advanced NSCLC patients. J Transl Med. 2023;21(1):174. doi:10.1186/s12967-023-04004-x
133. Vanguri RS, Luo J, Aukerman AT, et al. Multimodal integration of radiology, pathology and genomics for prediction of response to PD-(L) 1 blockade in patients with non-small cell lung cancer. Nat Cancer. 2022;3(10):1151–1164. doi:10.1038/s43018-022-00416-8
134. Captier N, Lerousseau M, Orlhac F, et al. Integration of clinical, pathological, radiological, and transcriptomic data improves prediction for first-line immunotherapy outcome in metastatic non-small cell lung cancer. Nat Commun. 2025;16(1):614. doi:10.1038/s41467-025-55847-5
135. Fatima SH, Faisal SJ, Batool SV, et al. Evaluating the combined efficacy of Telisotuzumab Vedotin and artificial intelligence in the treatment of non-squamous non-small cell lung cancer: a narrative review focusing on pharmaceutical and technical insights. Front Oncol. 2025;15:1673586. doi:10.3389/fonc.2025.1673586
136. Mazzaschi G, Marrocchio C, Moron Dalla Tor L, et al. Longitudinal blood immune-inflammatory and radiomic profiling to decode different patterns of acquired resistance to immunotherapy in patients with NSCLC. Clin Cancer Res. 2025;31(8):1533–1545. doi:10.1158/1078-0432.CCR-24-1926
137. Belum V, Benhuri B, Postow M, et al. Characterisation and management of dermatologic adverse events to agents targeting the PD-1 receptor. Eur J Cancer. 2016;60:12–25. doi:10.1016/j.ejca.2016.02.010
138. De Camargo Correia G S, Pai T, Li S, et al. Immune-related adverse events in patients with lung cancer. Current Oncol Rep. 2023;25(11):1259–1275. doi:10.1007/s11912-023-01462-w
139. Gomatou G, Tzilas V, Kotteas E, Syrigos K, Bouros D. Immune checkpoint inhibitor-related pneumonitis. Respiration. 2021;99(11):932–942. doi:10.1159/000509941
140. Cho JY, Kim J, Lee JS, et al. Characteristics, incidence, and risk factors of immune checkpoint inhibitor-related pneumonitis in patients with non-small cell lung cancer. Lung Cancer. 2018;125:150–156. doi:10.1016/j.lungcan.2018.09.015
141. Suresh K, Voong KR, Shankar B, et al. Pneumonitis in non–small cell lung cancer patients receiving immune checkpoint immunotherapy: incidence and risk factors. J Thorac Oncol. 2018;13(12):1930–1939. doi:10.1016/j.jtho.2018.08.2035
142. Cheng M, Lin R, Bai N, et al. Deep learning for predicting the risk of immune checkpoint inhibitor-related pneumonitis in lung cancer. Clin Radiol. 2023;78(5):e377–e85. doi:10.1016/j.crad.2022.12.013
143. Chen F, Niu J, Wang M, Zhu H, Guo Z. Re-evaluating the risk factors for radiation pneumonitis in the era of immunotherapy. J Transl Med. 2023;21(1):368. doi:10.1186/s12967-023-04212-5
144. Shaverdian N, Lisberg AE, Bornazyan K, et al. Previous radiotherapy and the clinical activity and toxicity of pembrolizumab in the treatment of non-small-cell lung cancer: a secondary analysis of the KEYNOTE-001 Phase 1 trial. Lancet Oncol. 2017;18(7):895–903. doi:10.1016/S1470-2045(17)30380-7
145. Yang L, Cui H, Duan Y, Yao Y, Zou B, Wang L. Radiotherapy-immunotherapy related pneumonitis prediction from pre-treatment CT using a deep graph-based integrative model. Am Soc Clin Oncol. 2022.
146. Chen X, Sheikh K, Lin C, et al. CT radiomics and machine learning for distinguishing radiotherapy vs. immune checkpoint inhibitor-induced pneumonitis in non-small cell lung cancer patients. Int J Radiat Oncol Biol Phys. 2020;108(3):S163.
147. Cheng J, Pan Y, Huang W, et al. Differentiation between immune checkpoint inhibitor‐related and radiation pneumonitis in lung cancer by CT radiomics and machine learning. Med Phys. 2022;49(3):1547–1558. doi:10.1002/mp.15451
148. Qiu Q, Xing L, Wang Y, Feng A, Wen Q. Development and validation of a radiomics nomogram using computed tomography for differentiating immune checkpoint inhibitor-related pneumonitis from radiation pneumonitis for patients with non-small cell lung cancer. Front Immunol. 2022;13:870842. doi:10.3389/fimmu.2022.870842
149. Heilbroner SP, Few R, Neilan TG, et al. Predicting cardiac adverse events in patients receiving immune checkpoint inhibitors: a machine learning approach. J ImmunoTher Cancer. 2021;9(10):e002545. doi:10.1136/jitc-2021-002545
150. Deo RC. Machine learning in medicine. Circulation. 2015;132(20):1920–1930. doi:10.1161/CIRCULATIONAHA.115.001593
151. Shameer K, Johnson KW, Glicksberg BS, Dudley JT, Sengupta PP. The whole is greater than the sum of its parts: combining classical statistical and machine intelligence methods in medicine. Heart. 2018;104(14):1228. doi:10.1136/heartjnl-2018-313377
152. Salahuddin Z, Woodruff HC, Chatterjee A, Lambin P. Transparency of deep neural networks for medical image analysis: a review of interpretability methods. Comput Biol Med. 2022;140:105111. doi:10.1016/j.compbiomed.2021.105111
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.