Back to Journals » Risk Management and Healthcare Policy » Volume 19
Artificial Intelligence and Enhanced Recovery After Surgery as Patient Safety Strategies for Perioperative Care in Resource-Limited Settings
Authors Mohamed IA ![]() , Hassan AM
, Hassan AM
Received 14 April 2026
Accepted for publication 1 June 2026
Published 3 June 2026 Volume 2026:19 616788
DOI https://doi.org/10.2147/RMHP.S616788
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Keon-Hyung Lee
Ibrahim Abdullahi Mohamed, Abdirahman Mohamed Hassan
Department of Anaesthesiology and Critical Care, Dr. Sumait Hospital, SIMAD University, Mogadishu, Somalia
Correspondence: Ibrahim Abdullahi Mohamed, Email [email protected]
Abstract: Artificial intelligence (AI) and Enhanced Recovery After Surgery (ERAS) are increasingly discussed as strategies for improving perioperative quality, efficiency, and recovery, but their implementation in resource limited settings requires a clear patient safety framework. In this commentary, resource limited settings refer to perioperative systems constrained by shortages of trained workforce, essential equipment, monitoring capacity, reliable data infrastructure, financing, or governance support. This commentary argues that AI and ERAS should be viewed as complementary rather than competing approaches. ERAS provides a structured pathway for standardizing perioperative care, while AI may support risk stratification, clinical decision support, monitoring, adherence tracking, and operational efficiency. Perioperative care is a suitable field for AI integration because it is time-sensitive, multidisciplinary, data-rich, and highly dependent on coordinated decisions across the preoperative, intraoperative, and postoperative continuum. However, digital tools cannot compensate for absent safety infrastructure, weak governance, or poor-quality data. A pragmatic strategy for low-resource settings is therefore to first establish essential perioperative safety standards, implement context-adapted ERAS elements, and then selectively deploy ethically governed AI applications with human oversight and local validation. Framed in this way, AI-supported ERAS pathways may strengthen patient safety, recovery, and risk management while supporting broader health system resilience.
Keywords: digital health, clinical decision support, low resource health systems, perioperative pathways, patient safety, implementation science
Introduction
Healthcare systems in resource limited settings face simultaneous access and quality gaps in surgical and anaesthesia care. In this commentary, resource-limited settings refer to health systems or hospitals where perioperative care is constrained by shortages of trained personnel, essential equipment, monitoring capacity, oxygen and medicines, reliable digital infrastructure, financing, or governance support. Universal access to safe, affordable surgical and anaesthesia care remains central to health system performance, yet perioperative services in many low- and middle-income countries continue to be constrained by workforce shortages, infrastructure gaps, inconsistent monitoring, and weak data systems.1,2 Enhanced Recovery After Surgery (ERAS) offers structured, multidisciplinary, evidence-based pathways intended to reduce unwarranted variation in perioperative practice, shorten hospital stay, and reduce postoperative complications, and LMIC specific ERAS guidance is now available for primary and secondary hospitals.3,4
Recent literature has increasingly examined the future of ERAS through artificial intelligence (AI), personalized care, digital health technologies, implementation barriers, and resource-related challenges.5 At the same time, AI is entering perioperative medicine through risk prediction, decision support, physiologic monitoring, workflow optimization, and recovery forecasting, which refers to prediction of postoperative recovery trajectory, complication risk, functional readiness, and discharge preparedness.6,7 Perioperative care is a suitable area for AI integration because it is time-sensitive, multidisciplinary, data-rich, and dependent on repeated decisions across the preoperative, intraoperative, postoperative, and discharge phases.
This commentary examines how AI and ERAS can be understood not as competing innovations but as complementary strategies for strengthening perioperative care in resource-limited settings. It reflects a narrative literature-informed and policy oriented interpretation of published guidelines, systematic reviews, related Risk Management and Healthcare Policy literature, and contextual implementation considerations rather than primary experimental or observational research. The manuscript’s added value is its explicit focus on patient safety, risk management, staged implementation, local validation, and governance in low-resource perioperative systems, rather than on technology adoption alone.
This focus is aligned with recent Risk Management and Healthcare Policy literature emphasizing AI governance, just culture, systems thinking, clinical decision support, medical device risk management, clinical pathway monitoring, and surgical safety improvement in resource-limited settings.8–12 The purpose is therefore not technological enthusiasm for its own sake, but a pragmatic framework for safer, more equitable, and more efficient perioperative care.
Why AI and ERAS Matter Together
ERAS is fundamentally a care redesign strategy. It links preoperative optimization, standardized anaesthetic and analgesic practices, early nutrition, early mobilization, nausea prevention, structured fluid management, and coordinated postoperative recovery into a single pathway. In randomized evidence syntheses, ERAS implementation has been associated with shorter length of stay and fewer general postoperative complications, although measured outcomes vary across surgical specialties and study designs.4 In low resource settings, its value is particularly compelling because many ERAS elements are organizational rather than technology-intensive: teamwork, protocolization, communication, and consistent perioperative processes.3
AI, by contrast, is not a pathway but a set of tools. Contemporary perioperative AI applications include automated risk stratification, physiologic trend recognition, early warning support, imaging assistance, operating room logistics, and postoperative outcome prediction.6,7 These functions may help clinicians identify which patients need optimization, which intraoperative events warrant earlier intervention, and which postoperative patients require closer observation or discharge planning support. In principle, AI may support ERAS implementation by making pathway delivery more personalized, timely, and auditable. In this context, auditable means that pathway steps, alerts, decisions, adherence, outcomes, overrides, and feedback can be documented and reviewed for quality improvement and accountability.
The relationship is especially important because ERAS can provide the clinical structure within which AI outputs become useful. Predictive models have limited value if care pathways are fragmented or if no agreed response follows an alert or risk estimate. Conversely, ERAS programs generate standardized perioperative processes and measurable outcomes that are more suitable for feedback loops, adherence dashboards, and continuous quality improvement. When paired thoughtfully, ERAS offers the operational backbone and AI offers targeted augmentation.
Implementation in Resource-Limited Settings
The strongest perioperative gains in resource limited environments are likely to come from adapting proven practices rather than importing high complexity systems unchanged from digitally mature hospitals. Digitally mature hospitals are institutions with reliable electricity and connectivity, interoperable electronic records, routine data capture, technical support, cybersecurity processes, and formal digital governance. Many resource-limited hospitals do not yet have these conditions, and this makes staged implementation essential.
This principle is crucial for both ERAS and AI. Local hospitals may not initially be able to support comprehensive digital perioperative platforms, but they may be able to implement selected ERAS elements, simplified data capture, structured postoperative monitoring, and limited decision support tools. Workforce digital literacy is a key determinant because clinicians, nurses, anaesthesia providers, data officers, and managers must understand what digital tools can and cannot do, how alerts should be interpreted, how data quality affects outputs, and when human escalation is required.
Recent experience from Rwanda illustrates stepwise ERAS adoption through knowledge assessment, protocol development, multidisciplinary engagement, and preliminary implementation rather than one-time policy declaration alone.13 Recent surgical safety work from Somalia similarly shows that context-sensitive, low-cost interventions, including focused education, leadership support, and visual prompts, can improve adherence to safety processes in a fragile health system.12 These examples are relevant beyond their individual settings because they show that perioperative innovation becomes more credible when it is locally owned, adapted, supported by training, and connected to routine quality improvement.
The same logic should guide AI adoption. Early AI use cases in these settings should be bounded and supportive rather than autonomous. Examples include preoperative risk screening, early warning systems based on routinely collected observations, operating theatre scheduling support, stock and bed use forecasting, and simple dashboards that track ERAS pathway adherence. These tools may strengthen efficiency and situational awareness, but they should not be mistaken for substitutes for clinical judgment or for the foundational requirements of safe perioperative care.
Risk, Governance, and Patient Safety
AI in health care raises well described concerns regarding bias, transparency, accountability, privacy, cybersecurity, and clinician overreliance.3,14–16 In this commentary, clinician overreliance refers to automation bias, alert fatigue, and possible reduction in independent clinical judgment when digital recommendations are accepted without sufficient assessment. These concerns are especially important in perioperative medicine because decisions are time sensitive, multidisciplinary, and often made under conditions of uncertainty. In resource limited settings, governance risks may be amplified by sparse digital infrastructure, weak procurement oversight, limited incident reporting, and datasets that are incomplete or poorly representative of the patients who will actually be managed.
The World Health Organization has emphasized that AI for health must be governed in ways that protect autonomy, promote transparency, assign accountability, and ensure that technology serves public benefit rather than worsening existing inequities.14,16 A systematic review of AI guidance also shows that formal standards and consensus statements are expanding, underscoring that responsible implementation depends on more than technical accuracy alone.17 This expectation is consistent with a recent SWOT analysis of artificial intelligence in clinical medicine, which highlights that responsible AI integration requires attention to data quality, algorithmic bias, interpretability, privacy, and consistent evaluation frameworks.15
For perioperative services, this means that AI tools should be introduced with clearly defined clinical scope, human oversight, documentation of performance, processes for override and escalation, attention to data stewardship, and mechanisms for post-implementation review. Local validation before deployment is essential because models developed in better resourced or different populations may perform poorly when case mix, documentation practices, monitoring frequency, laboratory access, or postoperative follow-up differ. In hospitals with limited data infrastructure, local validation may begin pragmatically through small-scale silent testing, clinician review of outputs, comparison with observed outcomes, documentation of false alerts and missed events, and staged use before full clinical integration.
Equally important, digital innovation should not distract from the minimum conditions required for safe surgery and anaesthesia. Global surgery and anaesthesia frameworks, together with WHO WFSA international standards, make clear that safe perioperative care depends on trained personnel, oxygen, monitoring, equipment, medicines, recovery capacity, and systems of quality assurance.1,2 No AI tool can compensate for absent pulse oximetry, unreliable electricity, lack of postoperative observation, or severe workforce shortages. In such environments, introducing sophisticated algorithms without fixing the safety floor risks widening rather than narrowing quality gaps.
Practical Priorities for Implementation
As summarized in Table 1, a realistic implementation strategy should begin with a safety floor and proceed through staged, context sensitive implementation. Context sensitive implementation means adapting the intervention to local workforce, infrastructure, supply chains, digital maturity, financing, patient needs, and governance capacity while preserving essential safety principles. Hospitals need reliable monitoring, oxygen, standard operating processes, recovery observation, essential analgesics and fluids, and consistent use of the surgical safety checklist before more advanced digital tools are expected to deliver value2,18 (Table 1).
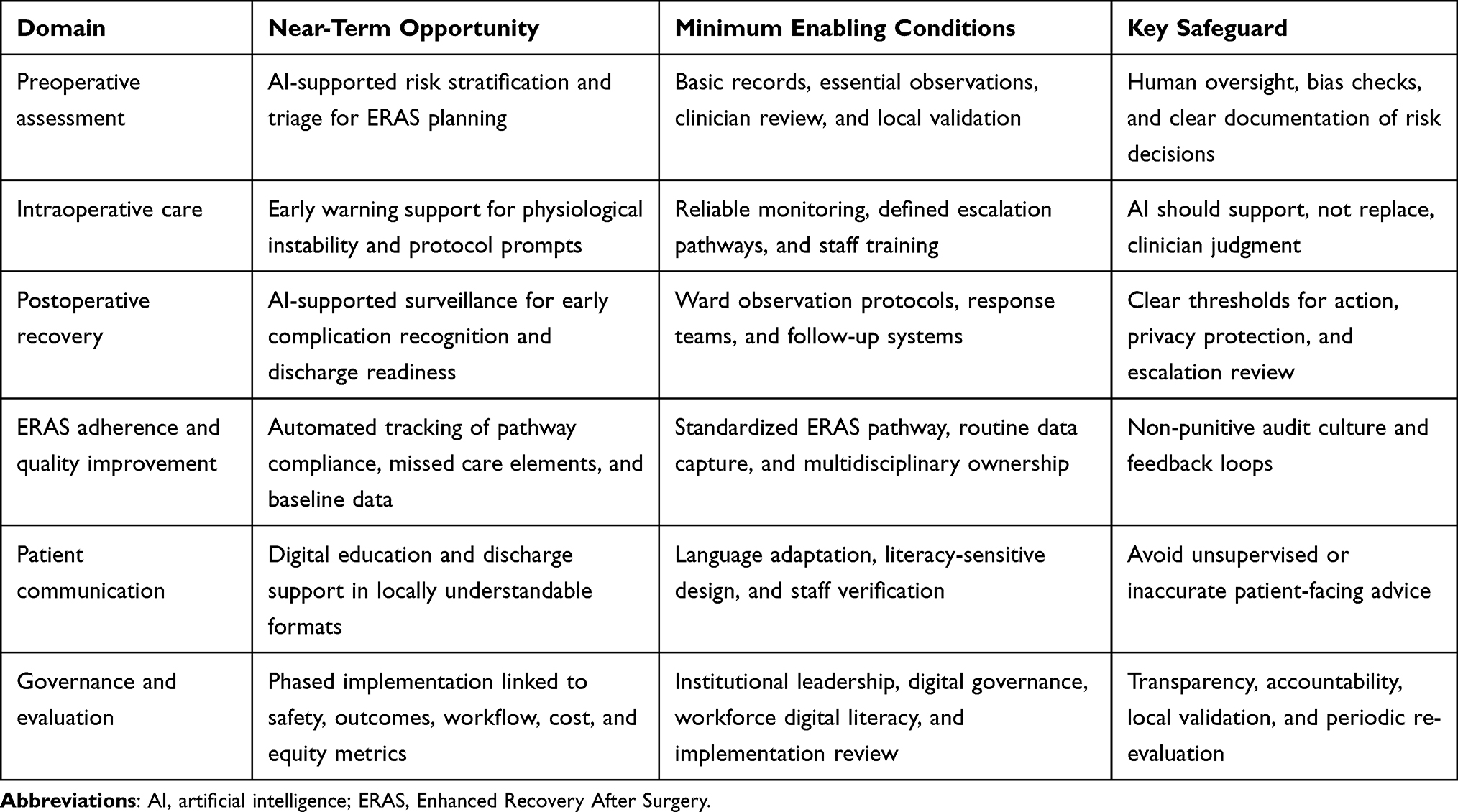 |
Table 1 Conceptual Staged Priorities for Integrating Artificial Intelligence and ERAS in Resource-Limited Perioperative Care |
The next step is to implement context adapted ERAS bundles. In hospitals with severe staffing or supply limitations, this should not mean abandoning ERAS, but prioritizing feasible, high value elements such as patient education, reduced fasting where appropriate, multimodal analgesia using available medicines, nausea prevention, early mobilization, early feeding when clinically feasible, clear discharge criteria, and routine audit of protocol adherence.3,4,13 Standardization at this stage is important because it creates the pathway logic and baseline data needed for later digital augmentation. Baseline data are intended primarily for quality improvement monitoring, while future AI model development should only be considered when data quality, governance, representativeness, and validation capacity are adequate.
Only then should AI be added selectively to support clearly defined problems. Priority applications should be those that reduce cognitive burden, improve early recognition of deterioration, assist pathway adherence, or improve use of limited perioperative resources. Tools should be locally validated, clinically supervised, and judged not only by algorithmic performance but also by their effect on postoperative complications, recovery, cost, workflow, staff trust, and equity. Feedback loops should operate through regular multidisciplinary review of ERAS adherence, patient outcomes, alert performance, staff concerns, and unintended consequences, followed by protocol refinement and renewed measurement.
Implementation should be governed as a quality improvement and implementation research agenda rather than a technology purchase. Implementation research helps identify barriers and facilitators, choose strategies, understand context, and evaluate outcomes such as adoption, fidelity, acceptability, feasibility, sustainability, and equity.19 In resource limited settings, the success of AI and ERAS will depend less on novelty than on disciplined implementation, local adaptability, workforce training, governance capacity, and sustained clinical ownership.
Policy and Risk-Management Implications
For policy makers and health system leaders, the central implication is that AI enabled perioperative innovation should be regulated and evaluated as a sociotechnical risk management process. Procurement decisions should require evidence of clinical scope, data requirements, human oversight, cybersecurity safeguards, bias assessment, local validation plans, and post deployment monitoring. Hospitals should avoid purchasing isolated digital tools that are not connected to ERAS pathways, escalation protocols, staff training, patient safety metrics, and accountability structures.
For perioperative leaders, the priority is to build reliable care processes before expecting AI to improve outcomes. This includes checklist adherence, recovery room observation, pain and nausea protocols, discharge criteria, basic outcome measurement, and multidisciplinary review. For researchers, the evidence gap is not only whether AI can predict risk, but whether AI-supported ERAS pathways improve patient safety, workflow, equity, and cost effectiveness in real world resource limited settings. For journals and policy audiences focused on risk management, this shifts the conversation from whether AI is innovative to whether it is safe, governed, locally valid, and embedded in systems that can act on its outputs.
Conclusion
Artificial intelligence and ERAS have important but different roles in perioperative strengthening. ERAS offers an evidence based framework for standardizing recovery oriented care, while AI offers tools that may improve prediction, coordination, monitoring, adherence tracking, and operational efficiency. In resource limited settings, their combined value lies in careful sequencing: establish essential perioperative safety, implement feasible ERAS pathways, and then adopt narrowly scoped AI applications under clear governance and human oversight. Successful implementation depends on infrastructure readiness, governance capacity, workforce training, local validation, and contextual adaptation. Framed in this way, innovation and recovery are not separate agendas. Together, they may support safer perioperative care, better use of scarce resources, and more resilient health systems.
Abbreviations
AI, artificial intelligence; ERAS, Enhanced Recovery After Surgery; LMICs, low- and middle-income countries; WHO, World Health Organization; WFSA, World Federation of Societies of Anaesthesiologists.
Ethics Approval and Consent
Not applicable. This article is a commentary and did not involve human participants, patient data, or identifiable personal information.
Acknowledgments
This research was supported by SIMAD University, Somalia. The authors extend sincere appreciation to perioperative clinicians working in low-resource settings whose practical realities continue to inform efforts to strengthen safe surgery, anaesthesia, and recovery-oriented care.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Meara JG, Leather AJM, Hagander L, et al. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015;386(9993):569–6. doi:10.1016/S0140-6736(15)60160-X
2. Gelb AW, Morriss WW, Johnson W, et al. World Health Organization-World Federation of Societies of Anaesthesiologists (WHO-WFSA) international standards for a safe practice of anesthesia. Anesth Analg. 2018;126(6):2047–2055. doi:10.1213/ANE.0000000000002927
3. Oodit R, Biccard BM, Panieri E, et al. Guidelines for perioperative care in elective abdominal and pelvic surgery at primary and secondary hospitals in low-middle-income countries (LMICs): enhanced Recovery After Surgery (ERAS) Society recommendation. World J Surg. 2022;46(8):1826–1843. doi:10.1007/s00268-022-06587-w
4. Sauro KM, Smith C, Ibadin S, et al. Enhanced recovery after surgery guidelines and hospital length of stay, readmission, complications, and mortality: a meta-analysis of randomized clinical trials. JAMA Network Open. 2024;7(6):e2417310. doi:10.1001/jamanetworkopen.2024.17310
5. Abosheisha M, Nasr E, Abdellatif M, et al. The future of Enhanced Recovery After Surgery in general surgery: integrating artificial intelligence, personalized care, and technological advances. Cureus. 2025;17(9):e91528. doi:10.7759/cureus.91528
6. Han L, Char DS, Aghaeepour N, et al. Artificial intelligence in perioperative care: opportunities and challenges. Anesthesiology. 2024;141(2):379–387. doi:10.1097/ALN.0000000000005013
7. Fei Q, Zhang Y, Liu C, et al. Artificial intelligence in anesthesia and perioperative medicine. Anesthesiol Perioper Sci. 2025;3(2):24. doi:10.1007/s44254-025-00107-4
8. Glarcher M, Vaismoradi M. Healthcare systems at the intersection of just culture and artificial intelligence: emerging challenges for nursing management. Risk Manag Healthc Policy. 2026;19:1–6. doi:10.2147/RMHP.S572893
9. Ouda E, Chaabi I, Abualola H, et al. The role of artificial intelligence in reducing dispensing errors for patient safety and quality: a systems approach. Risk Manag Healthc Policy. 2026;19:1–12. doi:10.2147/RMHP.S573762
10. Zhu W, Zhang P, Xia W, et al. AI-driven medical device risk management: a new paradigm integrating large language models and prompt engineering for standard-risk knowledge graph construction and application. Risk Manag Healthc Policy. 2026;19:1–17. doi:10.2147/RMHP.S571156
11. Li KC, Zeng W, Su K, Li G. Six Sigma and statistical process control in clinical pathway management: an evaluation using coefficient of variation, control charts, and process performance index. Risk Manag Healthc Policy. 2026;19:1–10. doi:10.2147/RMHP.S564118
12. Yusuf FY, Hussein AM, Elmi AH, Mohamed DA, Abdi AO. Improving surgical safety in Somalia: a closed-loop audit study of WHO surgical safety checklist adherence. Risk Manag Healthc Policy. 2025;18:4003–4010. doi:10.2147/RMHP.S572567
13. Nyundo M, Gasakure M, Muhawenayo E, et al. Introducing enhanced recovery after surgery (ERAS) program in Rwanda: a step-by-step approach from KAP study to protocol development and preliminary implementation. BMC Surg. 2025;25(1):173. doi:10.1186/s12893-025-02909-6
14. World Health Organization. Ethics and governance of artificial intelligence for health. World Health Organization; 2021. Available from: https://www.who.int/publications/i/item/9789240029200.
15. Sallam M, Snygg J, Allam D, Kassem R, Damani M. Artificial intelligence in clinical medicine: a SWOT analysis of AI progress in diagnostics, therapeutics, and safety. J Innov Med Res. 2025;4(3):1–20. doi:10.63593/JIMR.2788-7022.2025.06.001
16. World Health Organization. Ethics and governance of artificial intelligence for health: guidance on large multi-modal models. World Health Organization; 2025. Available from: https://www.who.int/publications/i/item/9789240084759.
17. Wang Y, Li N, Chen L, et al. Guidelines, consensus statements, and standards for the use of artificial intelligence in medicine: systematic review. J Med Internet Res. 2023;25:e46089. doi:10.2196/46089
18. Haynes AB, Weiser TG, Berry WR, et al. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med. 2009;360(5):491–499. doi:10.1056/NEJMsa0810119
19. Proctor E, Silmere H, Raghavan R, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health. 2011;38(2):65–76. doi:10.1007/s10488-010-0319-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Criteria For Agreement When Conducting Local Consensus Discussions: A Qualitative Study
Pagano L, Long JC, Francis-Auton E, Hirschhorn A, Braithwaite J, Arnolda G, Sarkies MN
Journal of Healthcare Leadership 2025, 17:159-172
Published Date: 5 May 2025