Back to Journals » Eye and Brain » Volume 13
Artifactual Visual Field Defects Identified on Technically “Reliable” Visual Field Studies in a Neuro-Ophthalmology Practice
Authors Galarza P, Parnasa E, Guttmann N ![]() , Kruger JM
, Kruger JM ![]()
Received 29 July 2020
Accepted for publication 25 December 2020
Published 14 April 2021 Volume 2021:13 Pages 79—88
DOI https://doi.org/10.2147/EB.S274523
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Margaret Wong-Riley
Pablo Galarza,1,* Elhanan Parnasa,2,* Noah Guttmann,3 Joshua M Kruger1
1Neuro-Ophthalmology Service, Department of Ophthalmology, Hadassah Medical Center, Jerusalem, Israel; 2Hebrew University-Hadassah School of Medicine, Jerusalem, Israel; 3Independent Researcher, Toronto, Ontario, Canada
*These authors contributed equally to this work
Correspondence: Joshua M Kruger
Neuro-Ophthalmology Service, Department of Ophthalmology, Hadassah Medical Center, Jerusalem, Israel
Tel +972508946493
Email [email protected]
Purpose: To assess the reliability of automated visual field studies with neurological abnormalities and normal reliability indices that were inconsistent with the remainder of the neuro-ophthalmic assessment.
Methods: Retrospective observational study from the clinical practice of a neuro-ophthalmologist at a tertiary referral center.
Results: From 2230 patient charts, ten cases were identified that met the inclusion criteria. In eight of the cases repeat visual field testing had no reproducible abnormality. Four of these cases were concerning for a bitemporal or homonymous hemianopia. None of the patients, including the two cases with a reproducible defect, developed any convincing manifestations of an organic disease related to the visual field defect.
Conclusion: Our findings suggest that even marked neurological abnormalities on reliable automated visual field tests can be false. When the remainder of the neuro-ophthalmic evaluation is inconsistent with the test result, we recommend that clinicians attempt to immediately repeat the visual field study.
Keywords: automated perimetry, visual field, Humphrey, reliability
Background
Standard automated perimetry is the most common method used for accurately assessing peripheral vision. Unfortunately, the test can be challenging for patients to perform, and inaccurate results often occur.1 The machinery is programmed to assess reliability by providing various indices including fixation losses, false positives, false negatives, and gaze tracking. When the reliability indices are poor, the clinician is reassured that any abnormal results are likely artifact. When the reliability indices are acceptable, clinicians may infer that an abnormality represents true pathology. We conducted a retrospective analysis to assess the clinical outcome of cases where automated visual field testing with reliable indices revealed an abnormality that was not otherwise apparent from the neuro-ophthalmic assessment.
Methods
This retrospective observational study was conducted in accordance with the Declaration of Helsinki and with the approval of the local ethics review board at Hadassah Medical Center. A chart review was conducted of all patients seen in the neuro-ophthalmology clinic of the senior author (JMK), during his work at the institution between 2014 and 2019.
The inclusion criteria were the following:
1) Patients that underwent a full neuro-ophthalmology assessment.
2) Automated visual field testing had a specific abnormality for at least one eye with reliable indices. The mean deviation had to be at least −3 dB. Fixation losses had to be under 20%, false positives under 15%,2 and false negatives under 25%.3 A visual field abnormality was considered specific if it conformed to one of the non-artifactual abnormalities described in the publications of the Optic Neuritis Treatment Trial, the Ocular Hypertension Treatment Study, or the Idiopathic Intracranial Hypertension Treatment Trial.4–6
3) The automated visual field tests were available in the hospital electronic medical record for direct review.
4) The remainder of the neuro-ophthalmic assessment was inconsistent with the visual field abnormality.
5) The senior author expressed skepticism in his note regarding the validity of the visual field test and recommended performing it again.
The clinical practice of the senior author is to describe any visual field that does not convincingly represent true pathology as being possible “artifact”. Therefore, the first step of the search strategy was to identify all patient charts in which the word “artifact” had occurred (all of the senior author’s patient records are electronic). These charts were then reviewed to determine whether the case met the inclusion criteria. Some cases were also identified with the personal recall of the senior author.
If the visual field of only one eye met the inclusion criteria, then the features of the contralateral visual field study were still considered in classifying the overall pattern of the abnormality even if the reliability indices of the contralateral eye did not meet the inclusion criteria (eg homonymous or bitemporal hemianopia).
Patients were contacted when the authors wished to use their specific visual field as a figure in this publication. In all cases, the patients provided informed written consent to publish their visual field tests in this study (name, date, and personal identification number were removed).
Results
The clinic data base included the records of 2230 patients. A search for the word “artifact” identified 159 patient charts. The content of these charts was then reviewed. Seven cases were identified that met the inclusion criteria. The senior author personally recalled another three cases that also met the inclusion criteria.
Table 1 summarizes the details of the 10 patients that met the inclusion criteria.
 |
Table 1 |
The ages of the patients ranged from 25 to 72 years. There were 4 males and 6 females. The clinical background and presenting symptoms varied widely. In all cases, patients had been tested with a central 24–2 threshold test. The test strategy was SITA-standard in 5 patients and SITA-fast in the remaining 5 patients. There was a range of 1 day to 3 months between the initial and repeat visual field testing with an average of 4.23 weeks (SD ± 3.9 weeks).
For eight of the patients, repeat visual field testing had no reproducible or concerning abnormalities. From these cases, the initial visual field abnormality was concerning for a hemianopia in four cases, a nerve fiber bundle defect in 3 cases, and bilateral maculopathy in one case. Regarding the four cases that were concerning for a hemianopia, in three of the cases the patient was urgently referred by either a neurologist or a general ophthalmologist who had ordered a visual field test and were alarmed by an unexpected pattern of a hemianopia. The two patients being referred by neurologists had already been referred for an urgent MRI scan. In one case it had already been performed and showed no evidence of a relevant lesion. In the other case, the MRI had not yet been performed and was deferred after a repeat visual field had no concerning findings.
In 3 cases deemed by the senior author as being less concerning, where follow-up only occurred after a span of months, the patient was referred for a retinal nerve fiber layer OCT scan, in addition to a repeat visual field study. In all three cases there were no findings on the OCT that correlated with the initial visual field defect.
Figures 1–8 demonstrate the visual field abnormalities that were not reproducible.
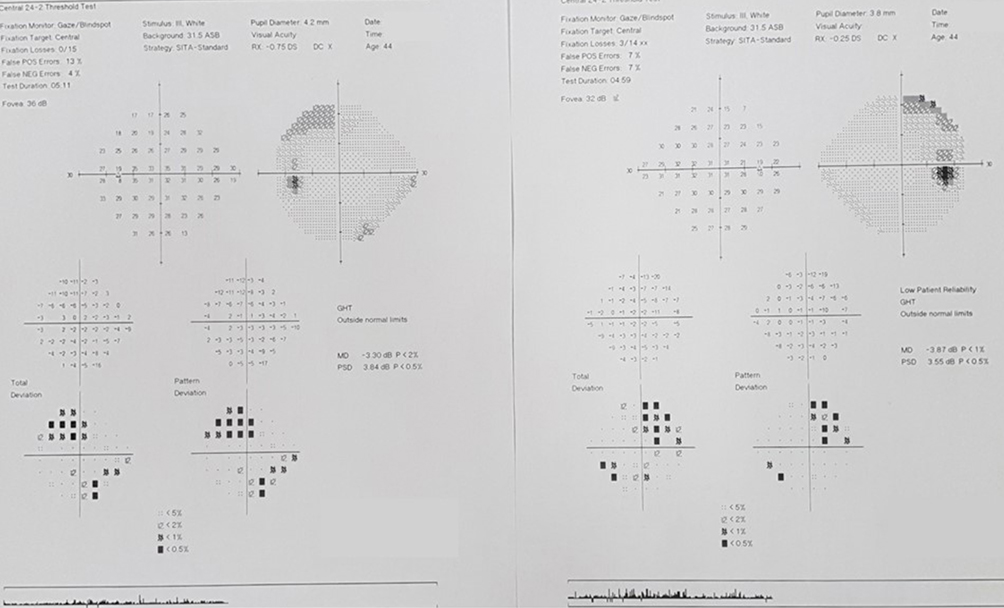 |
Figure 1 (Patient 1) A 44-year old man with a history of recent bilateral optic disc edema presented for routine follow-up at the neuro-ophthalmology clinic. The disc edema had subsided but an automated visual field study, performed with fair reliability, was suggestive of a superior bitemporal hemianopia and a left inferior nasal step. Recent magnetic resonance imaging (MRI) was reviewed to confirm that there was no evidence of a chiasmopathy. The visual field study was repeated the following day and was essentially normal for both eyes. |
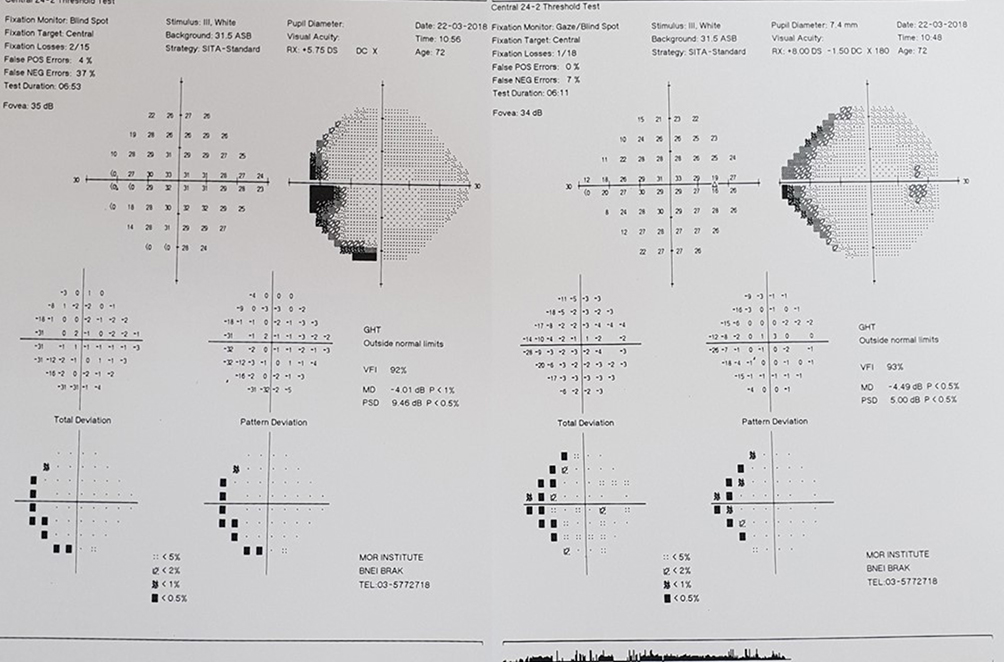 |
Figure 2 (Patient 2) A 72-year old man was referred for automated perimetry after his ocular pressure was noted to be elevated. The visual field study demonstrated a left homonymous defect and prompted an urgent referral from his general ophthalmologist. On neuro-ophthalmology assessment, it was noted that the study was performed with a large hyperopic correction, which can produce a rim-like artifact anomaly. The visual field study was repeated, ensuring that the trial lens was closely opposed to the eyes, and the result was normal. |
 |
Figure 3 (Patient 3) A 35-year old woman, generally healthy, presented to the hospital emergency complaining of blurred vision. On exam, the visual acuity of each eye was slightly limited and an automated visual field test, performed reliably, demonstrated bilateral central scotomas. Color vision, pupil reactivity, slit-lamp exam, and OCT of the maculae and retinal nerve fiber layer were all normal for both eyes. The visual field test was repeated the following day without any concerning findings. The patient was referred to an optometrist, who detected an uncorrected refractive error. |
 |
Figure 4 (Patient 4) A 64-year woman with suspected Parkinson’s disease was referred for a visual field test after she noted a black spot in her visual field. Her neurologist noted a dense left temporal hemianopia. He referred her for a neuro-ophthalmology exam and MRI due to a concern of a mass asymmetrically injuring the chiasm (junctional scotoma). The spot in her visual field was determined to be a vitreous floater related to her high myopia. The MRI was unremarkable, and a repeat visual field showed no reproducibility of the abnormality. |
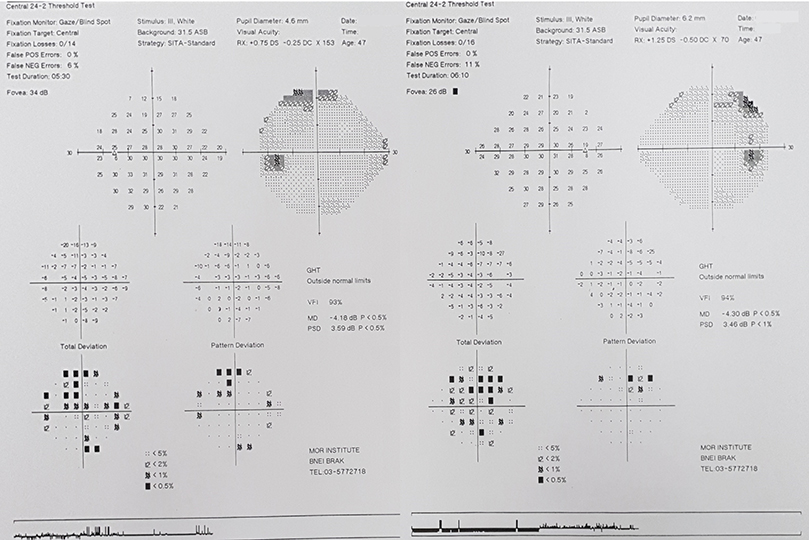 |
Figure 5 (Patient 5) A 47-year woman with a history of transient vision loss, suspected to be migrainous, was referred by her family doctor for a visual field study in order to renew her driver’s license. The result was reviewed by her neurologist, who was concerned about a bitemporal hemianopia. All other aspects of the neuro-ophthalmology exam were normal. A repeat visual field had no reproducible findings. |
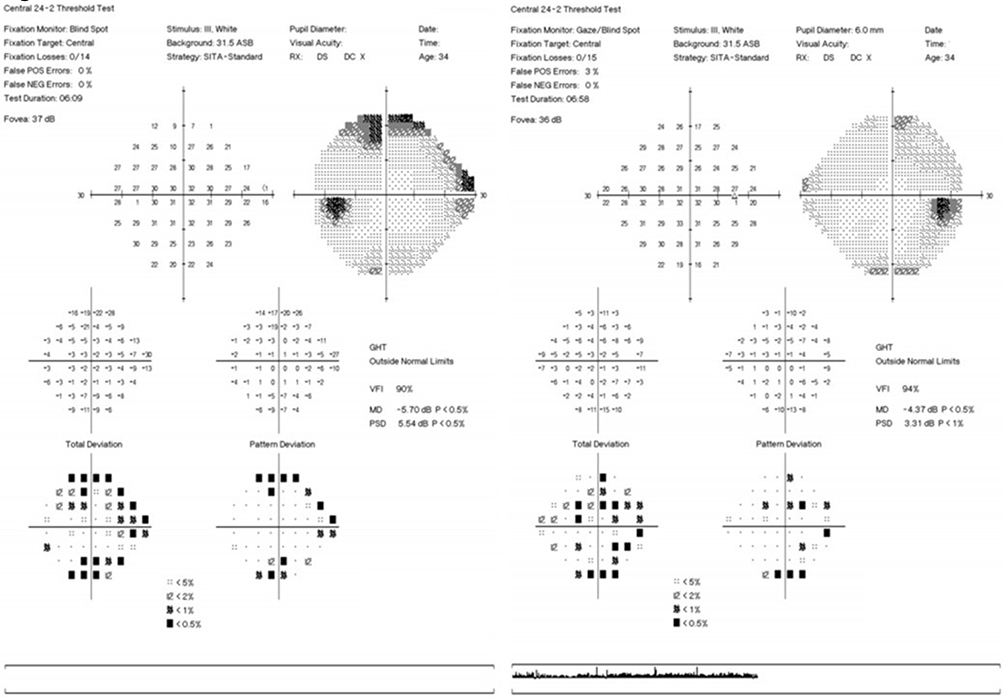 |
Figure 6 (Patient 6) A 34-year woman with multiple sclerosis was referred for evaluation due to a transient vision disturbance. Automated perimetry was performed reliably and demonstrated a right eye inferior depression and blind spot enlargement. The left eye had superior and inferior partial arcuate defects. There were no other findings. A repeat test was essentially normal for each eye. |
 |
Figure 7 (Patient 7) A 49-year woman with a history of Grave’s disease was referred by her endocrinologist to rule out a compressive optic neuropathy after she began to experience eye discomfort and a sensation that the eyes were protruding. Automated visual fields for the right eye were performed with a relatively high false negative rate (33%) and showed a generalized reduction in sensitivity with a dense superior altitudinal defect, inferior nasal step and blind spot enlargement. The left eye study was performed reliably and showed a generalized reduction in sensitivity with moderate superimposed nasal defects. The neuro-ophthalmology exam was otherwise unremarkable. The patient was referred for another automated visual field test that was normal for both eyes. |
 |
Figure 8 (Patient 8) A 65-year woman with diabetes was referred for evaluation due to blurred vision. On exam she was found to have a decompensating esophoria. A technically reliable visual field was suspicious for a left homonymous hemianopia. A repeat test had no reproducible findings. |
There were two cases that met the inclusion criteria where the visual field abnormality was reproducible. In both cases the visual field abnormality localized to the nerve fiber bundle. The first patient had extreme bilateral visual field constriction. Investigations including MRI, electrophysiology, and repeat OCT, including RNFL analysis, were essentially normal. After 6 months, the patient reported that his vision had spontaneously recovered. Automated perimetry at this point was normal. A non-organic etiology was suspected. The second patient, referred from a neurologist, also underwent brain MRI and OCT with no explanatory findings. He was lost to ophthalmology follow-up after one month. In records from a neurology clinic visit 8 months later the patient was no longer complaining of blurred vision.
Discussion
The results of this retrospective analysis suggest that marked neurological abnormalities on reliable automated visual field tests can merely be testing artifact. None of the patients, including those with a reproducible defect, demonstrated any subsequent manifestations of an organic disease related to the visual field defect. To the best of our knowledge, this is the first publication to emphasize that visual field studies concerning for neurologic abnormalities can be false positives even though they have normal reliability. These cases suggest that clinicians should have a low threshold for immediately repeating an automated visual field test in situations where the history and exam findings are inconsistent with the visual field abnormality.
There are several possibilities of how specific artifactual abnormalities can occur:
- Several studies have demonstrated that neurologic visual field defects can be non-organic.7,8 In our study we believe that this occurred in two patients where we suspected a non-organic etiology for the visual field defects.
- Lens rim artifact occurs when peripheral test stimuli are obscured from the patient’s eye by the rim of the trial lens or the lens holder.2 It can occur if the trial lens is not sufficiently close to the tested eye. It is also associated with high hyperopic corrections.2 Three of our cases (Figures 2, 5 and 8) were suspected to be associated with lens rim artifact.
- Uncorrected refractive error is expected to cause a generalized depression of the whole visual field,2 yet the case presented in Figure 3 suggests that it can cause focal abnormalities. Perhaps this can occur in cases of significant astigmatism where various zones of the visual field stimuli will be variously affected. This hypothesis would need to be formally tested.
- Eyelid ptosis or dermatochalasis can obstruct the peripheral visual field.9 In one dramatic case report, a pattern of a bitemporal hemianopia was produced due to lateral ptosis in both eyes.10 We do not believe that the visual field abnormalities in our patients were produced by a ptosis since none of them had appropriate eyelid findings. Furthermore, unless the eyelids were taped, the visual field defect would be expected to be reproduced.
- The phenomenon of false-negatives is well established in automated perimetry and involves the development of artifactual depressions in areas of a normal visual field.2 It is particularly associated with inexperienced patients.11 We suspect that these artifactual depressions can rarely occur, completely by chance, in clusters that mimic specific neurological defects. We believe that this is the explanation for some of our cases.
It should be emphasized that true visual field loss is commonly asymptomatic12 and all other findings on a neuro-ophthalmic examination can be normal including testing by confrontation.13 Therefore, any abnormality on a reliable test should be considered real even if there are no associated symptoms or exam findings. By no means do we mean to suggest that clinicians should, for example, defer referring for neuroimaging. We do recommend in parallel, that the automated perimetry be repeated as quickly as possible to confirm that the abnormality is reproducible.
There are a number of limitations in our study:
- Gaze tracking is considered to be a good indicator of reliability14 but there are no absolute metrics for classifying a field as reliable versus unreliable. Therefore, we could not incorporate gaze tracking in our inclusion criteria.
- Our inclusion criteria required a false negative rate of less than 25%. High false negative rates can occur when there are true visual field defects.2 Thus, our inclusion criteria may have excluded visual field studies that many experts would have still considered reliable. We believed that a strict approach was preferable in order to establish the specificity of our findings.
- In some cases, there was a significant time interval between the initial and follow-up visual field test (up to 3 months). Therefore, we must consider the possibility that the initial visual field represented true pathology and that there was a visual recovery by the time of the follow-up exam. The fact that neither MRI nor follow-up OCT showed any abnormalities related to the visual field defect suggests that this possibility is unlikely. Future directions should include a prospective study in which patients undergo visual field retesting on the same day.
- Cases were identified by searching for the word “artifact” in patient charts. Several cases that the senior author recalled did not have the word “artifact” in the patient chart. Therefore, it is possible that our cases underrepresent the true occurrence of the described phenomena. A multicentre, prospective study would be helpful to address this issue.
In summary, our retrospective study suggests that even the results of technically reliable automated perimetry can be false, prompting unnecessary anxiety, investigations, and costs. While the urgency for workup should not change, we do recommend that the perimetry be repeated as quickly as possible to confirm the reproducibility of the abnormality.
Abbreviations
MRI, magnetic resonance imaging; OCT, optical coherence tomography; SITA, Swedish Interactive Thresholding Algorithm.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Birt CM, Shin DH, Samudrala V, Hughes BA, Kim C, Lee D. Analysis of reliability indices from Humphrey visual field tests in an urban glaucoma population. Ophthalmology. 1997;104(7):1126–1130. doi:10.1016/s0161-6420(97)30173-0
2. Heijl A, Patella V, Bengtsson B. The Field Analyzer Primer: Effective Perimetry.
3. American Academy of Ophthalmology. 2020-2021 BCSC; Basic and Clinical Science Course. Brar VS, editor. American Academy of Ophthalmology; 2020.
4. Keltner JL, Johnson CA, Cello KE, Dontchev M, Gal RL, Beck RW. Visual field profile of optic neuritis. Arch Ophthalmol. 2010;128(3):330–337. doi:10.1001/archophthalmol.2010.16
5. Keltner JL, Johnson CA, Cello KE, et al. Classification of visual field abnormalities in the ocular hypertension treatment study. Arch Ophthalmol. 2003;121(5):643–650. doi:10.1001/archopht.121.5.643
6. Wall M, Johnson CA, Cello KE, et al. Visual field outcomes for the idiopathic intracranial hypertension treatment trial (IIHTT). Invest Ophthalmol Vis Sci. 2016;57(3):805–812. doi:10.1167/iovs.15-18626
7. Thompson JC, Kosmorsky GS, Ellis BD. Field of dreamers and dreamed-up fields: functional and fake perimetry. Ophthalmology. 1996;103(1):117–125. doi:10.1016/s0161-6420(96)30751-3
8. Stewart JF. Automated perimetry and malingerers. Can the Humphrey be outwitted? Ophthalmology. 1995;102(1):27–32. doi:10.1016/s0161-6420(95)31059-7
9. Alniemi ST, Pang NK, Woog JJ, Bradley EA. Comparison of automated and manual perimetry in patients with blepharoptosis. Ophthalmic Plast Reconstr Surg. 2013;29(5):361–363. doi:10.1097/IOP.0b013e31829a7288
10. Levine BM, Lelli GJ. Bitemporal hemianopia caused by bilateral blepharoptosis. Orbit. 2010;29(6):351–353. doi:10.3109/01676830.2010.516467
11. Heijl A, Lindgren G, Olsson J. The effect of perimetric experience in normal subjects. Arch Ophthalmol. 1989;107(1):81–86. doi:10.1001/archopht.1989.01070010083032
12. Liu GT, Vope NJ, Galetta SL. Neuro-Ophthalmology: Diagnosis and Management.
13. Kerr NM, Chew SSL, Eady EK, Gamble GD, Danesh-Meyer HV. Diagnostic accuracy of confrontation visual field tests. Neurology. 2010;74(15):1184–1190. doi:10.1212/WNL.0b013e3181d90017
14. Ishiyama Y, Murata H, Asaoka R. The usefulness of gaze tracking as an index of visual field reliability in glaucoma patients. Invest Ophthalmol Vis Sci. 2015;56(11):6233–6236. doi:10.1167/iovs.15-17661
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.