Back to Journals » International Journal of Women's Health » Volume 15
Prevalence, Impact, and Diagnostic Challenges of Benign Breast Disease: A Narrative Review
Authors Fraker JL, Clune CG, Sahni SK, Yaganti A, Vegunta S
Received 19 October 2022
Accepted for publication 5 May 2023
Published 18 May 2023 Volume 2023:15 Pages 765—778
DOI https://doi.org/10.2147/IJWH.S351095
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Jessica L Fraker,1 Caroline G Clune,2,3,* Sabrina K Sahni,4,* Avani Yaganti,5,* Suneela Vegunta1
1Division of Women’s Health Internal Medicine, Mayo Clinic, Scottsdale, AZ, USA; 2Center for Breast Care, Mayo Clinic Health System — Southwest Wisconsin Region, La Crosse, WI, USA; 3Division of General Internal Medicine, Mayo Clinic, Rochester, MN, USA; 4Jacoby Center for Breast Health, Mayo Clinic, Jacksonville, FL, USA; 5Southern Illinois University School of Medicine, Springfield, IL, USA
*These authors contributed equally to this work
Correspondence: Jessica L Fraker, Division of Women’s Health Internal Medicine, Mayo Clinic, 13400 E Shea Blvd, Scottsdale, AZ, 85259, USA, Email [email protected]
Abstract: Benign breast diseases, which are commonly seen in clinical practice, have various clinical presentations and implications, as well as management strategies. This article describes common benign breast lesions, presentations of these lesions, and typical radiographic and histologic findings. Also included in this review are the most recent data and guideline-based recommendations for the management of benign breast diseases at diagnosis, including surgical referral, medical management, and ongoing surveillance.
Keywords: breast biopsy, imaging, management, surveillance
Introduction
Breast-related concerns are common reasons patients seek care from health care professionals. Common concerns include a self-detected palpable lump, skin changes, breast pain, or nipple discharge. Patients may also seek care because of abnormalities detected on routine screening mammograms. Many of these breast concerns and findings have benign causes and are referred to as benign breast diseases or benign breast lesions. Some benign lesions can be more easily distinguished on standard imaging, whereas others may require more advanced imaging techniques or biopsy for a definitive diagnosis.
A key consideration with benign breast lesions is whether the biopsy findings on pathology align with findings from the examination and imaging, known as clinical- or radiologic-pathologic concordance.1 Lesions that are not concordant should generally be surgically excised.1 Two other factors that influence management are risk of upgrade to malignancy (risk of finding concurrent breast cancer) and future risk of breast cancer associated with a specific lesion type.
Benign breast lesions can be broadly grouped into nonproliferative lesions, proliferative lesions without atypia, and proliferative lesions with atypia.1,2 These groups are separated by histologic appearance of the lesions and the associated risk that future breast cancer will develop in patients with these types of lesions. Nonproliferative lesions have minimal to no associated increased risk of breast cancer as well as minimal risk of upgrade, so routine observation is generally recommended.1 Simple cysts and nonproliferative fibrocystic change are common examples of nonproliferative lesions.1,2 Individuals with proliferative lesions without atypia (including some fibroepithelial lesions, papillary lesions, radial scars) may have a slightly increased risk (relative risk of approximately 2.0) of future breast cancer.1 Proliferative lesions with atypia have a higher associated risk of future breast cancer, so these lesions are considered clinically to be high risk. For proliferative lesions with and without atypia, rates of upgrade to malignancy vary by lesion, as do management recommendations.
Clinical management depends on patient-specific factors and individual risk factors associated with the lesion. Some lesions require no additional management, and routine screening can be resumed. Other clinical management strategies include more frequent surveillance imaging for a select time to ensure lesion stability, referral for surgical excision, or consideration of endocrine therapies to reduce the future risk of breast cancer. Types of lesions, management strategies, and risks for future cancer are discussed in further detail in this article; risks are also summarized in Table 1.
 |
Table 1 Associated Risks of Benign Breast Disease |
Lesions and Management Strategies
Fibroepithelial Lesions
Fibroepithelial lesions, which include fibroadenomas and phyllodes tumors, are a unique group of breast disorders that have similar histologic features but vary clinically. Fibroadenomas are the most common of the benign breast masses, whereas phyllodes tumors are uncommon and can range from benign neoplasms to malignant tumors capable of distant metastasis.18
Fibroadenoma
A fibroadenoma is a common breast lesion that most often affects women of reproductive age and commonly presents as a painless mass, generally ranging in size from 2 to 3 cm. Although the exact cause is unknown, fibroadenomas develop from stromal and epithelial tissue and are thought to be estrogen-sensitive lesions.19,20 As a result, they have a propensity to increase in size during the menstrual cycle, during pregnancy, and with menopausal hormone therapy. They usually regress at menopause.19 There are various types of fibroadenomas—from simple fibroadenomas, which comprise about 70% to 90% of all fibroadenomas, to cellular fibroadenomas, which have similar histologic features to a phyllodes tumor.21,22 Juvenile fibroadenomas are rare and are more commonly seen in adolescents aged 10 to 18 years as well as in premenopausal women.22 These lesions enlarge rapidly, often causing substantial breast growth or asymmetry. Lesions larger than 5 cm are referred to as giant fibroadenomas.22
Complex fibroadenomas contain specific histologic features including cysts >3 mm, calcifications, sclerosing adenosis, and papillary metaplasia.22,23 These characteristics are considered pathologic and may influence future risk for breast cancer. A study by Nassar et al23 showed that the overall risk of breast cancer for a woman with fibroadenoma was slightly elevated (relative risk, 1.60). However, for women with a complex fibroadenoma, an even higher relative risk of 2.27 has been reported, with the risk largely dependent on the degree of proliferation.23 Cellular fibroadenomas have high stromal cellularity and can often resemble a benign phyllodes tumor histologically. Because of this similarity, surgical excision is often recommended to confirm the diagnosis.24
Many fibroadenomas are first identified on screening mammography. Diagnosis can often be made largely from imaging findings of diagnostic mammography and focused ultrasonography; however, for a definitive diagnosis, biopsy may be indicated. If women have a high likelihood of fibroadenoma based on imaging findings but have not had a biopsy, surveillance with imaging is recommended at 6, 12, and 24 months to document lesion stability. Surgical excision of the lesion can be considered for women with large, rapidly growing, or painful fibroadenomas.25
Phyllodes Tumors
Phyllodes tumors comprise about 0.3% to 1.0% of all breast tumors.26 They commonly present in premenopausal women and have a similar clinical presentation to fibroadenomas, averaging 4 to 5 cm in size.27,28 Phyllodes tumors often have a round, lobulated appearance with partially indistinct or circumscribed margins on mammography and ultrasonography. Cystic features are commonly seen in malignant variants.27 Phyllodes tumors arise from the breast stroma and are stimulated by various growth factors. Other factors such as pregnancy, trauma, lactation, or increased estrogen production may also cause these tumors to grow.28
Like fibroadenomas, phyllodes tumors can be classified and differentiated on the basis of histologic features and are graded as benign, borderline, or malignant.28 Benign phyllodes tumors are likely to recur, and malignant phyllodes tumors can metastasize.27 A large meta-analysis that included 54 retrospective studies reported an 8% local recurrence rate for benign types, 13% for borderline, and 18% for malignant phyllodes tumors.27,29
The mainstay treatment for phyllodes tumors is surgical excision.30 The need for re-excision in patients with residual positive margins remains controversial. However, women with a borderline or malignant phyllodes tumor with positive margins should undergo re-excision.28 Long-term surveillance of benign phyllodes tumors includes clinical breast examination and ultrasonography every 6 months for 2 years to monitor for recurrence in addition to age-appropriate screening.31,32 Figure 1 shows sonographic images of a fibroepithelial lesion, which was revealed to be a phyllodes tumor on biopsy.
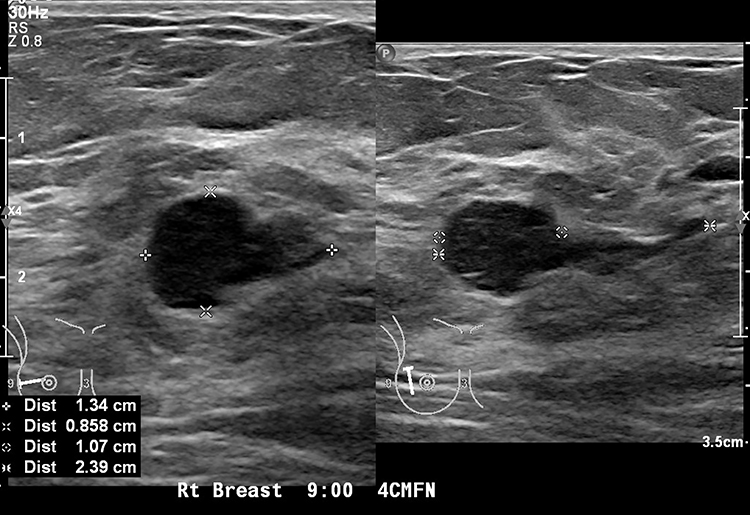 |
Figure 1 Sonographic image showing a fibroepithelial lesion with borderline findings. Biopsy revealed phyllodes tumor. Abbreviations: 4 CMFN, 4 centimeters from nipple; Dist, distance; Rt, right. |
Papillary Lesions
Intraductal papilloma is the most common heterogeneous group of papillary lesions of the breast.4 They comprise 10% of benign breast lesions,33 and their incidence has been estimated at 2% to 3% among cisgender women.34 Pathologically, papillomas are discrete intraductal polypoid lesions. They can harbor atypia, which may affect management.35,36 Clinically, papillomas can present in various ways including nipple discharge and a palpable mass, or they can be first seen on screening breast imaging.37 Papillary lesions present more commonly in the central breast and in the subareolar region, but they can also be found peripherally.4 Papillomas have been reported to comprise 40% to 70% of cases of pathologic nipple discharge.34 On mammography, papillomas appear as well-defined round or oval soft-tissue opacities, with or without microcalcifications.4,33 Ultrasonography may reveal an intraductal mass, an intracystic mass, or a solid mass.35 The incidence of asymptomatic papilloma has increased with the rising availability of advanced imaging and core needle biopsy for breast lesions.34
Management strategies for papilloma are still being debated. For management, papillomas are often divided into 3 subgroups: papilloma with atypia, multiple papillomas and/or peripheral papilloma, and solitary papilloma without atypia (or solitary benign papilloma). There is consensus regarding management of papillomas with atypia on biopsy. These papillary lesions have been shown to be associated with a high rate (at least 25–30%) of upgrade to carcinoma on excision, and practice recommendations include proceeding with surgical excision.8 The presence of a papilloma with atypia was reported with an associated relative risk of 5.11 for future malignancy,35 a risk that is comparable or slightly greater than that of other atypias.
Multiple papillomas are discrete entities with varied definitions in the literature and include recurrent papilloma, papillomas diagnosed on biopsy of different sites, or multiple papillomas (>5) seen on surgical excisional pathology.5,35 For multiple and peripheral papillomas, surgical excision is recommended.33 Multiple papillomas without atypia are associated with a relative future cancer risk of 3.01, which falls between the risks for proliferative lesions and atypia. Multiple papillomas with atypia have a reported relative risk of 7.01, which is greater than the relative risk for atypical hyperplasia without papilloma.35 For patients with papillomas and associated atypia, follow-up should include surveillance and future risk-reduction strategies according to recommendations for high-risk lesions, discussed in detail later in this article.
The management of solitary papilloma without atypia has been updated because of variable rates of upstaging at excision. More recent studies have consistently shown low upgrade rates for lesions sized <1 cm (0–3%).4–6 One of the few prospective studies reported the risk of upgrade at 1.7%.37 These data have challenged the need for surgical excision, and while no consensus exists, data support radiologic surveillance over surgical excision. However, patients with symptomatic papilloma can be referred for surgical excision of the tumor. Patients with solitary papilloma have a relative risk of 2.04 of developing future breast cancer, similar to the risk associated with other proliferative lesions without atypia.35 Figures 2 and 3 show sonographic images of papillomas: Figure 2, multiple papillomas, and Figure 3, a single papilloma with cystic spaces.
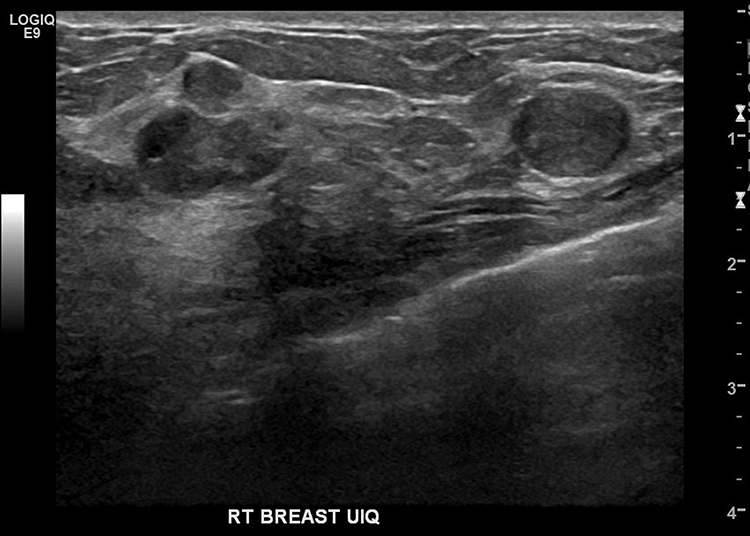 |
Figure 2 Sonographic image showing multiple papillomas. Abbreviations: Rt indicates right; UIQ, upper inner quadrant. |
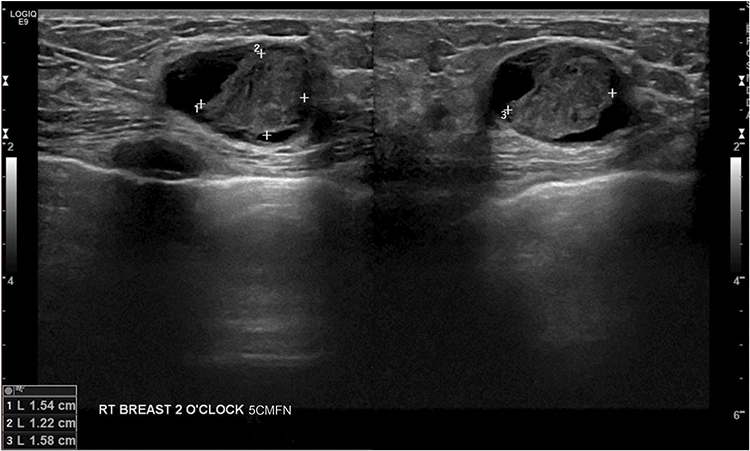 |
Figure 3 Sonographic image showing a single papilloma with cystic spaces. Abbreviations: 5CMFN, 5 centimeters from nipple; RT, right. |
Pseudoangiomatous Stromal Hyperplasia
Pseudoangiomatous stromal hyperplasia (PASH) is a rare benign proliferative disease of the breast characterized by activation and increase in myofibroblastic activity.38 Although commonly seen in premenopausal women, PASH also occurs in men with underlying gynecomastia and postmenopausal women on hormone therapy. As a result, it has been widely accepted that PASH is in part hormonally mediated.39 In a study by Jones et al40 that included 57 women with biopsy-proven PASH, 44% of lesions presented as a palpable mass, and 53% were found incidentally on screening mammography. The remaining 3% were found during evaluation of an unrelated abnormality.40 On a mammogram, PASH is most commonly seen as a noncalcified oval mass with circumscribed or partially circumscribed margins,38 focal asymmetry, or less commonly, an area of architectural distortion. On ultrasonography, these lesions appear nonspecific.38 For biopsy-confirmed PASH lesions, no long-term surveillance is required. Surgical excision should be considered if biopsy results are discordant or if symptomatic relief is needed.41 Alternatively, selective estrogen receptor modulators, such as tamoxifen or raloxifene, can be considered for management of PASH.41 Figure 4 shows an example on magnetic resonance imaging of pseudoangiomatous stromal hyperplasia.
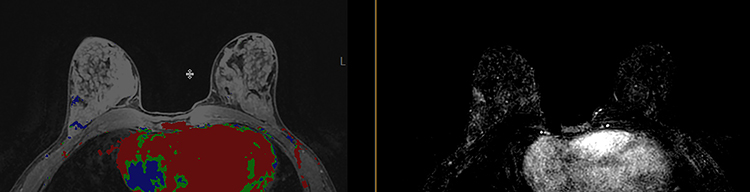 |
Figure 4 Magnetic resonance image showing enhancement in the area of pseudoangiomatous stromal hyperplasia. |
Flat Epithelial Atypia
Flat epithelial atypia (FEA) is an uncommon breast proliferative lesion described histologically as a columnar cell change of the epithelial layer, with or without hyperplasia of the terminal duct lobular unit.42 The affected cells have low-grade cytologic atypia without complex architectural patterns; essentially, the epithelial cell layer change is flat.42,43 Patients with FEA are generally asymptomatic and without palpable findings on breast examination; the FEA is often discovered incidentally on a biopsy performed because of abnormal findings on breast imaging,43,44 most commonly microcalcifications.45 Less commonly, FEA can be seen on ultrasonography as an irregular or complex mass.43 FEA may be found with other higher risk lesions or carcinoma, with atypical ductal hyperplasia (ADH) being most common.8 A biopsy finding of isolated FEA is associated with a future risk for breast cancer similar to that of other proliferative lesions without atypia.8 For this reason, an isolated finding of FEA on biopsy does not warrant the use of risk-reducing medications or high-risk screening imaging strategies for long-term surveillance.9
Clinical management of FEA with surgical excision is an ongoing topic of research and debate and is related to how often FEA is upgraded at the time of surgical excision to higher risk forms of atypia such as ADH, atypical lobular hyperplasia (ALH), lobular carcinoma in situ (LCIS), or carcinoma. The rate of upgrade to cancer varies across studies, with previous studies showing upgrade rates up to 42%, although there has generally been a trend toward lower rates in more recent and higher quality studies.9 This change is thought to be due, at least in part, to improving imaging techniques and ability to determine radiologic-pathologic concordance, as well as to improved biopsy sampling techniques with larger gauge needles and vacuum-assisted biopsy.8,9 More recent studies have shown upgrade rates to malignancy of less than 10%, even some below 3%, particularly when accounting for focal FEA in isolation, radiologic-pathologic concordance, and biopsy sampling in which all microcalcifications have been removed.8,9,46
Previously, patients often underwent surgical excision of FEA; however, several studies as well as guidelines from both the American Society of Breast Surgeons (ASBrS) and the National Comprehensive Cancer Network (NCCN) suggest that surveillance alone may be appropriate in some cases.47,48 The recommended surveillance regimen is a clinical breast examination and mammography (with or without ultrasonography) every 6 months for at least 1 to 2 years.47,48 Surveillance should be considered in cases of isolated focal FEA without other associated high-risk lesions, biopsy and imaging with radiologic-pathologic concordance, removal of all microcalcifications on biopsy, and no associated mass on imaging.8 FEA associated with other high-risk atypia such as ADH or discordant findings with imaging should be excised,47,48 and management should be directed according to recommendations for a high-risk lesion.8,49,50 Coexistence of additional patient-specific risk factors that may warrant lesion excision rather than observation include patient history of a high-risk genetic mutation or a personal history of breast cancer.51,52
Radial Scar/Complex Sclerosing Lesion
The terms radial scar and complex sclerosing lesion are sometimes used interchangeably, but in this review, the lesions will be referred to collectively as radial scar. Radial scars are rare and histologically composed of a fibroelastic center with entrapped glandular elements, ducts, and lobules that radiate outward from the center and have associated proliferative changes.8,10 Historically, radial scars have been distinguished by size and defined as lesions ≤1 cm, and complex sclerosing lesions were considered as those >1 cm.9 The appearance of these lesions histologically and radiographically may mimic an invasive carcinoma; on histology this can be distinguished, but it can be difficult to distinguish the appearance of radial scar from carcinoma on imaging alone, leading to the need for core needle biopsy to confirm the diagnosis.8
Radial scars are generally asymptomatic and not associated with palpable masses on examination.10 They can be found on biopsy done for a mammographic abnormality most commonly as a spiculated mass, or they can be found incidentally on biopsies completed for other reasons.10 They are not a precursor to malignancy, and studies show an increased future risk similar to that for other proliferative breast lesions.8,10 Radial scars can also be associated with other proliferative lesions, concurrent atypia, or carcinoma on biopsy.8
Management of radial scars has been controversial, particularly regarding the decision for surgical excision of the lesion vs observation. This results partly from varying reported rates of upgrade to malignancy at surgical excision. Previous studies showed upgrade rates from 0% to 40%, but more recent studies showed upgrade rates of 10% or less when radial scar was evaluated without associated atypia.8,10,11 The lower rates of upgrade to malignancy are most likely due to advanced imaging and procedural technologies mentioned for FEA, including better biopsy sampling with larger gauge needles, vacuum-assisted biopsy techniques, and the ability to determine radiologic-pathologic concordance.8,11 Concurrent nonmalignant high-risk lesions can also be found on surgical excision with upgrade rates of 12% to 26% reported in recent studies.10
Some radial scars can be observed when specific criteria are met, such as when a lesion is ≤1 cm, is found incidentally on biopsy, was adequately sampled on biopsy, and has radiologic-pathologic concordance.50,53 Excision is generally recommended if a radial scar is associated with a high-risk lesion, is large (>1 cm), is associated with a mass on imaging, or has radiologic-pathologic discordance.10,54 This management strategy is supported by guidelines from the ASBrS and NCCN.47,48 When radial scar lesions are not excised, it is recommended that patients be followed up with physical examinations and mammography and/or ultrasonography every 6 months for 1 to 2 years.47,48 Despite lower rates of upgrade to malignancy with surgical excision of radial scars on more recent studies, as with FEA, the rates of upgrade to other concurrent high-risk lesions remain elevated. It is therefore recommended to consider surgical excision for individual patients if finding of a high-risk lesion would influence clinical management.8,10 Figure 5 shows distortion in an area of radial scar on mammographic imaging.
 |
Figure 5 Mammographic image showing distortion in an area of radial scar. Yellow circle on figure outlines area of architectural distortion on mammography, biopsy revealed radial scar on pathology. |
Proliferative Breast Lesions with Atypia: ADH, ALH, and LCIS
In this section, ADH, ALH, and LCIS are discussed as high-risk breast lesions. Identifying these lesions on breast biopsy carries an increased lifetime risk of breast cancer. The 25-year risk for ADH and ALH is approximately 30%;1,55 for LCIS, the risk is 2% per year.56,57
Atypical Ductal Hyperplasia
ADH is an epithelial proliferation of atypical cells with monomorphic round nuclei, partially involving the breast ducts.50 The involvement of fewer than 2 separate ducts or an overall size less than 2 to 3 mm is also needed for a diagnosis of ADH.50,58 ADH is most often diagnosed by core needle biopsy of abnormal microcalcifications identified on routine screening mammography.50,59,60 ADH has features similar to low-grade ductal carcinoma in situ (DCIS) but can be differentiated from DCIS by both qualitative and quantitative measures.58,60 Unlike DCIS, ADH cells lack nuclear atypia and cell necrosis.59 Occurrence of ADH in the general population varies widely (1–20% of benign breast biopsies).59,61–63 Various factors may increase an individual’s risk of developing ADH, including personal history of prior ADH or breast cancer or a family history of breast cancer.62,64,65 Upgrade rates from ADH to DCIS have been studied extensively and vary. Recent studies estimate upgrade rates from 7.5% to 56%.12,66–68 A metaanalysis of 93 studies12 showed an upgrade risk of ADH to invasive cancer of 9% (95% CI, 7–11%) for surgically excised lesions compared with 3.4% for lesions that were managed by follow-up (95% CI, 1.8–6.4%). The authors identified the risk factors associated with upgrade as age, overall breast cancer risk, lesion size, multiple lesions, needle gauge, and number of previous biopsies.69
Surgical excision remains the most highly recommended management option for ADH because of high upgrade rates to malignancy.47 A systematic review and meta-analysis showed that ADH was significantly more likely to be upgraded than other non-ADH lesions.12 Overall upgrade rates were 10% to 20%, with upgrades mostly to DCIS but in some cases to invasive breast cancer.12 Lower upgrade rates were generally associated with radiologic-pathologic concordance, small lesion size, near removal (more than 50%) of lesions by core needle biopsy, fewer foci of ADH, age less than 50 years, no necrosis, and no papillary architecture.61,70 Whereas the NCCN supports surgical excision after an initial ADH diagnosis,48 other guidelines favor active surveillance.33,71 On the basis of recent data, the ASBrS has stated that some cases of ADH can be observed with patient follow-up, but given the variability of recent studies, most patients with ADH should have the lesion surgically excised.47 This is an area of ongoing research, and recommendations for management continue to evolve. Figure 6 shows mammographic calcifications that on biopsy were revealed to be flat epithelial atypia and atypical ductal hyperplasia.
Atypical Lobular Hyperplasia
ALH is an epithelial proliferation of atypical monomorphic cells that distend the acini of terminal duct lobular units.50 The most common mammographic abnormalities are abnormal microcalcifications (86%), but mass lesions, architectural distortion, or focal asymmetry are also seen.50,68 To qualify as ALH, at least 1 acinus within a lobular unit must be distended with more cells typical of ALH than normal.72 A quantitative distinction can be made between ALH and LCIS; in ALH, the percentage of acini distended by neoplastic cells is less than 50%, whereas it is greater than 50% in LCIS.50,73,74 The estimated rate of ALH diagnosis on core needle biopsy is about 0.9%.68 The upgrade rates of ALH vary greatly because many studies include both ALH and LCIS; however, studies of isolated ALH show much lower rates of upgrade than rates for ADH and LCIS—less than 5% on average.13
Radiologic-pathologic concordance of a small, well-sampled lesion can predict those patients who are low risk and who could reasonably be followed up by close clinical surveillance.13,14 Some patients will need to have the ALH lesion surgically excised. Indications for consideration of surgical excision are a discordant lesion, an associated mass or other benign breast lesion such as papilloma or radial scar, or in some cases a personal or strong family history of breast cancer.47,68,75 The NCCN and ASBrS endorse surgical excision of ALH lesions if core needle biopsy results are discordant with imaging.47,48 However, if the biopsy results are concordant with imaging, clinical and radiologic surveillance can be considered.47,48
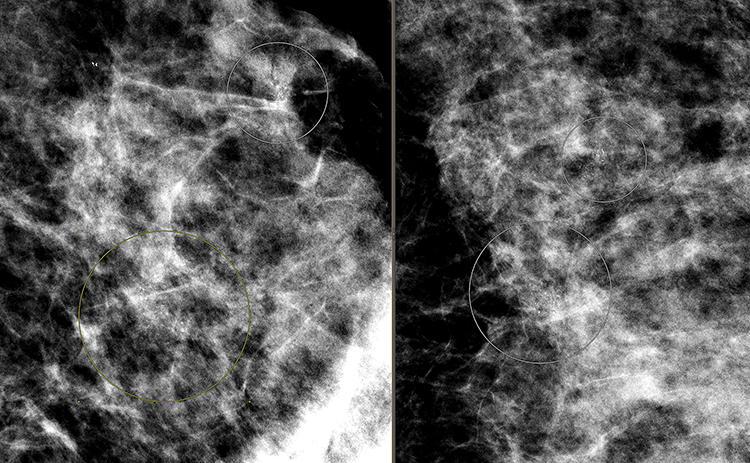 |
Figure 6 Mammographic image showing calcifications. Biopsy revealed flat epithelial atypia and atypical ductal hyperplasia. Yellow and white circles on figure outline areas of calcifications on mammography, biopsies revealed flat epithelial atypia and atypical ductal hyperplasia. |
Lobular Carcinoma in situ
First described in 1941,76 LCIS is a lobular neoplasia of the terminal duct lobular units, and its clinical significance and management remain controversial.77 Data for the incidence of LCIS are limited, given its lack of classic clinical presentation and radiologic features. It is often found incidentally on biopsy for other lesions. Reports suggest that LCIS is found in 0.5% to 3.8% of benign breast biopsies.71 LCIS, especially the pleomorphic and florid subtypes, can be seen as calcifications on a mammogram. Studies show that the incidence of LCIS has increased over time, partly because of improved screening methods and an aging population.78
LCIS is further subtyped into classic, pleomorphic, or florid LCIS.79 Classic LCIS is diagnosed microscopically when more than 50% of the acinar spaces in the lobule are distorted and distended by a dyshesive proliferation of cells with small, uniform nuclei. The pleomorphic subtype is characterized by cells that exhibit marked nuclear pleomorphism, often with a central area of necrosis in the involved acinar spaces.80 Florid LCIS, also known as LCIS with necrosis, is characterized by massive expansions of the acini along with central necrosis. The necrotic foci often harbor calcifications.81
Surgical excision is favored to manage LCIS; however, risk varies by subtype. For pleomorphic and florid LCIS, available studies show a high rate of upgrade to invasive carcinoma and DCIS on surgical excision (40% and 15%, respectively).57,82 Therefore, surgical resection is recommended for nonclassical types of LCIS. The range of upgrade rates in classic LCIS is wide, although recent, well-powered studies have suggested that the upgrade rate at surgical excision is lower than once believed when pure classic LCIS is identified on core needle biopsy, radiologic and pathologic diagnoses are concordant, and no other lesions requiring excision are present.14–16 A recent meta-analysis showed a rate of 5.8% for upgrade to malignancy.17
Management of Proliferative Breast Lesions with Atypia
Management of ADH, ALH, and LCIS can be complex, and historically surgical excision was standard of care. Newer data suggest that observation alone without surgery may be appropriate in many circumstances, particularly when there is radiologic-pathologic concordance, but this remains a topic of ongoing research and some controversy. For this reason, consulting a breast specialist for management decisions regarding these lesions is recommended when possible. For lesions that are not surgically excised, there should be close short-term surveillance with clinical breast examination and focused imaging (mammography, with ultrasound added as appropriate) every 6 months for 1 to 2 years to ensure lesion stability.47,48
Another complex management consideration with these high-risk lesions regards longer-term surveillance and risk-reduction strategies. Patients should be actively involved in shared decision-making because surveillance requires patient adherence with close follow-up. Use of enhanced screening for patients with a high lifetime risk should be made based on standard clinical risk factors and quantitative risk assessment. However, surveillance recommendations based only on diagnosis of these high-risk lesions vary without clear consensus. Although practitioners agree that patients should be followed up clinically and undergo annual mammography, recommendations for annual magnetic resonance imaging (MRI) are more controversial. Patient-specific risk factors, such as genetic mutations that increase the risk of breast cancer, breast density, and a family history of breast cancer, should all be considered when clinical management decisions are made. Clinical management should be based on individual risk, which can be estimated with the use of risk-assessment calculators that incorporate patient factors, such as IBIS ([International Breast Cancer Intervention Study] based on the Tyrer-Cuzick algorithm)83 and BCRAT ([Breast Cancer Risk Assessment Tool] based on the Gail model).84 These calculators can be used to estimate 5-year, 10-year, and lifetime risks. Patients with a 5-year risk of invasive breast cancer of 1.7% or greater by the BCRAT or a lifetime risk of breast cancer of 20% or greater by models that are largely dependent on family history, such as IBIS, are generally considered to be high risk, and lesion management is recommended according to high-risk guidelines.48
For patients with proliferative breast lesions with atypia and a lifetime risk of 20% or greater, the NCCN recommends enhanced surveillance including a clinical encounter every 6 to 12 months, annual screening mammography with tomosynthesis where available, and consideration of annual supplemental imaging with breast MRI to begin 10 years before the youngest age of diagnosis of an affected family member (not before age 25 for MRI and 30 for mammography) or age 40, whichever comes first.48 Alternatives such as contrast-enhanced mammography, whole breast ultrasonography, or molecular breast imaging can be considered for those patients who qualify but are unable to complete MRI.48,85,86 The American College of Radiology recommends a contrast-enhanced breast MRI in addition to screening mammography annually for high-risk persons.87 The risks and benefits of contrast-enhanced MRI, such as possible gadolinium toxicity, cost, and false-positive findings, can lead to unnecessary tests and anxiety for patients and should be discussed thoroughly with patients before scheduling.88–90
The NCCN recommends appropriate risk-reduction strategies including lifestyle modifications and risk-reducing pharmacologic agents.91 High-risk patients may also benefit from use of endocrine therapies including the selective estrogen receptor modulators tamoxifen and raloxifene and the aromatase inhibitors anastrozole and exemestane as preventive medications to reduce the risk of breast cancer. The aromatase inhibitors are currently used off-label for this purpose. These therapies have been shown to have a risk-reduction benefit that outweighs risk, most notably for patients 35 years or older with a 5-year risk of 3% or greater by the BCRAT or a 10-year risk of 5% or greater by the IBIS model.92–97 For patients who meet these criteria, use of these medications should be considered and discussed in shared decision-making, including risks and benefits based on individual patient comorbidities.92,93 A meta-analysis of several large trials evaluating use of these medications for risk reduction in atypical hyperplasia narrowed the focus to 4 placebo-controlled trials, with results showing reduced relative risk of 41% to 79% with use of an active agent vs placebo (National Surgical Adjuvant Breast and Bowel Project P-1 [NSABP P-1], Mammary Prevention 3 [MAP.3], International Breast Cancer Intervention Studies, I and II [IBIS-I and IBIS-II]).55 Findings from the NSABP P-1 trial showed that 5 years of tamoxifen compared with placebo reduced the risk of invasive breast cancer by 56% in women with LCIS, compared with 49% for all women with increased risk in the study.56,93
In clinical practice, however, patients’ use of these medications can be poor for various reasons,98 including hesitancy by practitioners to prescribe endocrine therapy.99 Other concerns of patients are cost, insurance coverage, and risk of adverse effects.100,101 Therefore, the possible benefits, adverse effects, and risks associated with these medications should be discussed and medication choice individualized for patient-specific preferences and comorbidities. Shared decision-making with patients and detailed education regarding these medications should guide their use.
Conclusion
Benign breast lesions, which are commonly found in clinical practice, have varied clinical and radiologic presentations and clinical management strategies. Better diagnostic technologies, both imaging and procedural, have allowed for improved radiologic-pathologic concordance. More recent studies have shown a trend toward lower upgrade rates of these lesions, which has led to more conservative management, such as observation with examinations and imaging surveillance rather than surgical excision.
Management strategies for some of these lesions are still being debated, and consensus on recommendations is lacking. Lesions such as most fibroadenomas, solitary benign papillary lesions, FEA, radial scar, and PASH, when isolated without atypia, are not associated with significantly increased risk enough to warrant high-risk screening strategies or risk-reducing endocrine therapies. However, these lesions can influence lifetime risk for breast cancer, and therefore individualized risk assessment using risk-calculation models should be completed for these patients. The outcomes of risk stratification based on 5-year, 10-year, and lifetime risk estimates should be used to identify patients who could benefit from high-risk management strategies. Atypical hyperplasia, including ADH, ALH, LCIS, and papilloma with atypia, carry an increased risk, and high-risk surveillance and risk-reducing medications should be considered in shared decision-making with patients. For discussion of management options, patients should be referred to health care professionals with expertise in treating patients with high-risk lesions.
Abbreviations
ADH, atypical ductal hyperplasia; ALH, atypical lobular hyperplasia; ASBrS, American Society of Breast Surgeons; BCRAT, Breast Cancer Risk Assessment Tool; DCIS, ductal carcinoma in situ; FEA, flat epithelial atypia; IBIS, International Breast Cancer Intervention Study; LCIS, lobular carcinoma in situ; MAP.3, Mammary Prevention 3, Exemestane for Prevention of Breast Cancer; MRI, magnetic resonance imaging; NCCN, National Comprehensive Cancer Network; NSABP P-1, National Surgical Adjuvant Breast and Bowel Project P-1, Tamoxifen for the Prevention of Breast Cancer; PASH, pseudoangiomatous stromal hyperplasia.
Ethics Approval and Informed Consent
Approval by the Mayo Clinic Institutional Review Board was not required for this review article.
Acknowledgments
Sandhya Pruthi, MD, Division of General Internal Medicine, Mayo Clinic, provided suggestions/revisions of the article at one time during the writing process. Richard E. Sharpe Jr, MD, MBA, Department of Radiology, Mayo Clinic, provided breast imaging case examples from a clinical radiologic database for the lesions described in the article. Marianne Mallia, ELS, MWC, senior scientific/medical editor, Mayo Clinic, substantively edited the manuscript. The Scientific Publications staff at Mayo Clinic provided proofreading, administrative, and clerical support.
Funding
No funding was received for this review article.
Disclosure
The authors declare that they have no competing interests.
References
1. Klassen CL, Hines SL, Ghosh K. Common benign breast concerns for the primary care physician. Cleve Clin J Med. 2019;86(1):57–65. doi:10.3949/ccjm.86a.17100
2. Hartmann LC, Sellers TA, Frost MH, et al. Benign breast disease and the risk of breast cancer. N Engl J Med. 2005;353(3):229–237. doi:10.1056/NEJMoa044383
3. Wu Y-T, Chen S-T, Chen C-J, et al. Breast cancer arising within fibroadenoma: collective analysis of case reports in the literature and hints on treatment policy. World J Surg Oncol. 2014;12(1):335. doi:10.1186/1477-7819-12-335
4. Kulka J, Madaras L, Floris G, Lax SF. Papillary lesions of the breast. Virchows Arch. 2022;480(1):65–84. doi:10.1007/s00428-021-03182-7
5. Jatana S, Zahra S, Miron AD, et al. A retrospective study evaluating outcomes of surgical excision versus radiologic follow-up of benign breast papillomas without atypia. Am J Surg. 2022;224(3):932–937. doi:10.1016/j.amjsurg.2022.04.029
6. Symbol B, Ricci A. Management of intraductal papilloma without atypia of the breast diagnosed on core biopsy: size and sampling matter. Breast J. 2018;24(5):738–742. doi:10.1111/tbj.13052
7. Degnim AC, Frost MH, Radisky DC, et al. Pseudoangiomatous stromal hyperplasia and breast cancer risk. Ann Surg Oncol. 2010;17(12):3269–3277. doi:10.1245/s10434-010-1170-5
8. Racz JM, Carter JM, Degnim AC. Challenging atypical breast lesions including flat epithelial atypia, radial scar, and intraductal papilloma. Ann Surg Oncol. 2017;24(10):2842–2847. doi:10.1245/s10434-017-5980-6
9. Amin AL, Wagner JL. Contemporary management of atypical breast lesions identified on percutaneous biopsy: a narrative review. Ann Breast Surg. 2021;5:9. doi:10.21037/abs-20-117
10. Bao JJ, Jaskowiak NT. Clinical management of radial scar without atypia diagnosed on core needle biopsy. Ann Breast Surg. 2021;5. doi:10.21037/abs-20-85
11. Farshid G, Buckley E. Meta-analysis of upgrade rates in 3163 radial scars excised after needle core biopsy diagnosis. Breast Cancer Res Treat. 2019;174(1):165–177. doi:10.1007/s10549-018-5040-3
12. Schiaffino S, Calabrese M, Melani EF, et al. Upgrade rate of percutaneously diagnosed pure atypical ductal hyperplasia: systematic review and meta-analysis of 6458 lesions. Radiology. 2020;294(1):76–86. doi:10.1148/radiol.2019190748
13. Sen LQ, Berg WA, Hooley RJ, Carter GJ, Desouki MM, Sumkin JH. Core breast biopsies showing lobular carcinoma in situ should be excised and surveillance is reasonable for atypical lobular hyperplasia. AJR Am J Roentgenol. 2016;207(5):1132–1145. doi:10.2214/AJR.15.15425
14. Middleton LP, Sneige N, Coyne R, et al. Most lobular carcinoma in situ and atypical lobular hyperplasia diagnosed on core needle biopsy can be managed clinically with radiologic follow-up in a multidisciplinary setting. Cancer Med. 2014;3(3):492–499. doi:10.1002/cam4.223
15. Bowman K, Munoz A, Mahvi DM, Breslin TM. Lobular neoplasia diagnosed at core biopsy does not mandate surgical excision. J Surg Res. 2007;142(2):275–280. doi:10.1016/j.jss.2007.03.052
16. Murray MP, Luedtke C, Liberman L, Nehhozina T, Akram M, Brogi E. Classic lobular carcinoma in situ and atypical lobular hyperplasia at percutaneous breast core biopsy: outcomes of prospective excision. Cancer. 2013;119(5):1073–1079. doi:10.1002/cncr.27841
17. Shehata MN, Rahbar H, Flanagan MR, et al. Risk for upgrade to malignancy after breast core needle biopsy diagnosis of lobular neoplasia: a systematic review and meta-analysis. J Am Coll Radiol. 2020;17(10):1207–1219. doi:10.1016/j.jacr.2020.07.036
18. Tummidi S, Kothari K, Agnihotri M, Naik L, Sood P. Fibroadenoma versus phyllodes tumor: a vexing problem revisited! BMC Cancer. 2020;20(1):648. doi:10.1186/s12885-020-07129-0
19. Salati SA. Breast fibroadenomas: a review in the light of current literature. Pol Przegl Chir. 2020;93(1):40–48. doi:10.5604/01.3001.0014.5676
20. Ajmal M, Khan M, Van Fossen K. Breast fibroadenoma. StatPearls [Internet]. StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535345/.
21. Lee M, Soltanian HT. Breast fibroadenomas in adolescents: current perspectives. Adolesc Health Med Ther. 2015;6:159–163. doi:10.2147/AHMT.S55833
22. Basara Akin I, Balci P. Fibroadenomas: a multidisciplinary review of the variants. Clin Imaging. 2021;71:83–100. doi:10.1016/j.clinimag.2020.10.058
23. Nassar A, Visscher DW, Degnim AC, et al. Complex fibroadenoma and breast cancer risk: a Mayo Clinic Benign Breast Disease Cohort Study. Breast Cancer Res Treat. 2015;153(2):397–405. doi:10.1007/s10549-015-3535-8
24. Tan PH. Fibroepithelial lesions revisited: implications for diagnosis and management. Mod Pathol. 2021;34(Suppl 1):15–37. doi:10.1038/s41379-020-0583-3
25. Greenberg R, Skornick Y, Kaplan O. Management of breast fibroadenomas. J Gen Intern Med. 1998;13(9):640–645. doi:10.1046/j.1525-1497.1998.cr188.x
26. Limaiem F, Kashyap S. Phyllodes tumor of the breast. StatPearls [Internet]. StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK541138/.
27. Weaver M, Stuckey A. Benign breast disorders. Obstet Gynecol Clin North Am. 2022;49(1):57–72. doi:10.1016/j.ogc.2021.11.003
28. Parker SJ, Harries SA. Phyllodes tumours. Postgrad Med J. 2001;77(909):428–435. doi:10.1136/pmj.77.909.428
29. Lu Y, Chen Y, Zhu L, et al. Local recurrence of benign, borderline, and malignant phyllodes tumors of the breast: a systematic review and meta-analysis. Ann Surg Oncol. 2019;26(5):1263–1275. doi:10.1245/s10434-018-07134-5
30. Tan BY, Acs G, Apple SK, et al. Phyllodes tumours of the breast: a consensus review. Histopathology. 2016;68(1):5–21. doi:10.1111/his.12876
31. National Comprehensive Cancer Network. Breast cancer. Available from: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1419.
32. Telli ML, Horst KC, Guardino AE, Dirbas FM, Carlson RW. Phyllodes tumors of the breast: natural history, diagnosis, and treatment. J Natl Compr Canc Netw. 2007;5(3):324–330. doi:10.6004/jnccn.2007.0027
33. Neal L, Sandhu NP, Hieken TJ, et al. Diagnosis and management of benign, atypical, and indeterminate breast lesions detected on core needle biopsy. Mayo Clin Proc. 2014;89(4):536–547. doi:10.1016/j.mayocp.2014.02.004
34. Hodorowicz-Zaniewska D, Szpor J, Basta P. Intraductal papilloma of the breast - management. Ginekol Pol. 2019;90(2):100–103. doi:10.5603/GP.2019.0017
35. Lewis JT, Hartmann LC, Vierkant RA, et al. An analysis of breast cancer risk in women with single, multiple, and atypical papilloma. Am J Surg Pathol. 2006;30(6):665–672. doi:10.1097/00000478-200606000-00001
36. MacGrogan G, Tavassoli FA. Central atypical papillomas of the breast: a clinicopathological study of 119 cases. Virchows Arch. 2003;443(5):609–617. doi:10.1007/s00428-003-0888-x
37. Nakhlis F, Baker GM, Pilewskie M, et al. The incidence of adjacent synchronous invasive carcinoma and/or ductal carcinoma in situ in patients with intraductal papilloma without atypia on core biopsy: results from a prospective multi-institutional registry (TBCRC 034). Ann Surg Oncol. 2021;28(5):2573–2578. doi:10.1245/s10434-020-09215-w
38. Raj SD, Sahani VG, Adrada BE, et al. Pseudoangiomatous stromal hyperplasia of the breast: multimodality review with pathologic correlation. Curr Probl Diagn Radiol. 2017;46(2):130–135. doi:10.1067/j.cpradiol.2016.01.005
39. Yoon KH, Koo B, Lee KB, et al. Optimal treatment of pseudoangiomatous stromal hyperplasia of the breast. Asian J Surg. 2020;43(7):735–741. doi:10.1016/j.asjsur.2019.09.008
40. Jones KN, Glazebrook KN, Reynolds C. Pseudoangiomatous stromal hyperplasia: imaging findings with pathologic and clinical correlation. AJR Am J Roentgenol. 2010;195(4):1036–1042. doi:10.2214/AJR.09.3284
41. Pruthi S, Reynolds C, Johnson RE, Gisvold JJ. Tamoxifen in the management of pseudoangiomatous stromal hyperplasia. Breast J. 2001;7(6):434–439. doi:10.1046/j.1524-4741.2001.07611.x
42. Schnitt SJ. The diagnosis and management of pre-invasive breast disease: flat epithelial atypia--classification, pathologic features and clinical significance. Breast Cancer Res. 2003;5(5):263–268. doi:10.1186/bcr625
43. Solorzano S, Mesurolle B, Omeroglu A, et al. Flat epithelial atypia of the breast: pathological-radiological correlation. AJR Am J Roentgenol. 2011;197(3):740–746. doi:10.2214/AJR.10.5265
44. DiPasquale A, Silverman S, Farag E, Peiris L. Flat epithelial atypia: are we being too aggressive? Breast Cancer Res Treat. 2020;179(2):511–517. doi:10.1007/s10549-019-05481-9
45. Prowler VL, Joh JE, Acs G, et al. Surgical excision of pure flat epithelial atypia identified on core needle breast biopsy. Breast. 2014;23(4):352–356. doi:10.1016/j.breast.2014.01.013
46. Wahab RA, Lee SJ, Mulligan ME, Zhang B, Mahoney MC. Upgrade rate of pure flat epithelial atypia diagnosed at core needle biopsy: a systematic review and meta-analysis. Radiol Imaging Cancer. 2021;3(1):e200116. doi:10.1148/rycan.2021200116
47. The American Society of Breast Surgeons. Consensus guideline on concordance assessment of image-guided breast biopsies and management of borderline or high-risk lesions; 2018. Available from: https://www.breastsurgeons.org/docs/statements/Consensus-Guideline-on-Concordance-Assessment-of-Image-Guided-Breast-Biopsies.pdf.
48. National Comprehensive Cancer Network. Breast cancer screening and diagnosis. Available from: https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1421.
49. Liu C, Dingee CK, Warburton R, et al. Pure flat epithelial atypia identified on core needle biopsy does not require excision. Eur J Surg Oncol. 2020;46(2):235–239. doi:10.1016/j.ejso.2019.10.029
50. Bahl M. Management of high-risk breast lesions. Radiol Clin North Am. 2021;59(1):29–40. doi:10.1016/j.rcl.2020.08.005
51. Grabenstetter A, Brennan S, Salagean ED, Morrow M, Brogi E. Flat epithelial atypia in breast core needle biopsies with radiologic-pathologic concordance: is excision necessary? Am J Surg Pathol 2020;44(2):182–190. doi:10.1097/PAS.0000000000001385
52. Lamb LR, Bahl M, Gadd MA, Lehman CD. Flat epithelial atypia: upgrade rates and risk-stratification approach to support informed decision making. J Am Coll Surg. 2017;225(6):696–701. doi:10.1016/j.jamcollsurg.2017.08.022
53. Cohen MA, Newell MS. Radial scars of the breast encountered at core biopsy: review of histologic, imaging, and management considerations. AJR Am J Roentgenol. 2017;209(5):1168–1177. doi:10.2214/AJR.17.18156
54. Liu RQ, Chen L, Padilla-Thornton A, et al. Upstage rate of radial scar/complex sclerosing lesion identified on core needle biopsy. Am J Surg. 2021;221(6):1177–1181. doi:10.1016/j.amjsurg.2021.03.029
55. Hartmann LC, Degnim AC, Santen RJ, Dupont WD, Ghosh K. Atypical hyperplasia of the breast--risk assessment and management options. N Engl J Med. 2015;372(1):78–89. doi:10.1056/NEJMsr1407164
56. King TA, Pilewskie M, Muhsen S. Lobular carcinoma in situ: a 29-year longitudinal experience evaluating clinicopathologic features and breast cancer risk. J Clin Oncol. 2015;33(33):3945–3952. doi:10.1200/JCO.2015.61.4743
57. Racz JM, Carter JM, Degnim AC. Lobular neoplasia and atypical ductal hyperplasia on core biopsy: current surgical management recommendations. Ann Surg Oncol. 2017;24(10):2848–2854. doi:10.1245/s10434-017-5978-0
58. Walia S, Ma Y, Lu J, Lang JE, Press MF. Pathology and current management of borderline breast epithelial lesions. AJHO. 2017;13(8):24–31.
59. Myers DJ, Walls AL. Atypical breast hyperplasia. StatPearls [Internet]. StatPearls Publishing; 2022. Available from: http://www.ncbi.nlm.nih.gov/books/NBK470258/.
60. Page DL, Rogers LW. Combined histologic and cytologic criteria for the diagnosis of mammary atypical ductal hyperplasia. Hum Pathol. 1992;23(10):1095–1097. doi:10.1016/0046-8177(92)90026-y
61. Pena A, Shah SS, Fazzio RT, et al. Multivariate model to identify women at low risk of cancer upgrade after a core needle biopsy diagnosis of atypical ductal hyperplasia. Breast Cancer Res Treat. 2017;164(2):295–304. doi:10.1007/s10549-017-4253-1
62. Menes TS, Rosenberg R, Balch S, Jaffer S, Kerlikowske K, Miglioretti DL. Upgrade of high-risk breast lesions detected on mammography in the Breast Cancer Surveillance Consortium. Am J Surg. 2014;207(1):24–31. doi:10.1016/j.amjsurg.2013.05.014
63. Deslauriers N, Sideris L, Dufresne M-P, et al. Breast lesions of uncertain malignant potential: a challenge for surgeons. Cancer Clin Oncol. 2012;1(1):77–87. doi:10.5539/cco.v1n1p77
64. Hoogerbrugge N, Bult P, de Widt-Levert LM, et al. High prevalence of premalignant lesions in prophylactically removed breasts from women at hereditary risk for breast cancer. J Clin Oncol. 2003;21(1):41–45. doi:10.1200/JCO.2003.02.137
65. Brem RF. Management of breast atypical ductal hyperplasia: now and the future. Radiology. 2020;294(1):87–88. doi:10.1148/radiol.2019192192
66. Mooney KL, Bassett LW, Apple SK. Upgrade rates of high-risk breast lesions diagnosed on core needle biopsy: a single-institution experience and literature review. Mod Pathol. 2016;29(12):1471–1484. doi:10.1038/modpathol.2016.127
67. Gagnon N, Martel E, Cadrin-Chenevert A, Ledoux E, Racicot C, Villiard R. Upgrade rate of atypical ductal hyperplasia: ten years experience and predictive factors. J Surg Res. 2021;266:311–318. doi:10.1016/j.jss.2021.03.063
68. Lewin AA, Mercado CL. Atypical ductal hyperplasia and lobular neoplasia: update and easing of guidelines. AJR Am J Roentgenol. 2020;214(2):265–275. doi:10.2214/AJR.19.21991
69. Harrington L, diFlorio-Alexander R, Trinh K, MacKenzie T, Suriawinata A, Hassanpour S. Prediction of atypical ductal hyperplasia upgrades through a machine learning approach to reduce unnecessary surgical excisions. JCO Clin Cancer Inform. 2018;2:1–11. doi:10.1200/CCI.18.00083
70. Racz JM, Degnim AC. When does atypical ductal hyperplasia require surgical excision? Surg Oncol Clin N Am. 2018;27(1):23–32. doi:10.1016/j.soc.2017.07.011
71. Morrow M, Schnitt SJ, Norton L. Current management of lesions associated with an increased risk of breast cancer. Nat Rev Clin Oncol. 2015;12(4):227–238. doi:10.1038/nrclinonc.2015.8
72. Page DL, Dupont WD, Rogers LW. Ductal involvement by cells of atypical lobular hyperplasia in the breast: a long-term follow-up study of cancer risk. Hum Pathol. 1988;19(2):201–207. doi:10.1016/s0046-8177(88)80350-2
73. Gulla S, Lancaster R, De Los Santos J. High-risk breast lesions and current management. Semin Roentgenol. 2018;53(4):252–260. doi:10.1053/j.ro.2018.08.001
74. Page DL, Dupont WD, Rogers LW, Rados MS. Atypical hyperplastic lesions of the female breast. A long-term follow-up study. Cancer. 1985;55(11):2698–2708. doi:10.1002/1097-0142(19850601)55:11<2698::aid-cncr2820551127>3.0.co;2-a
75. Holbrook AI, Hanley K, Jeffers C, Kang J, Cohen MA. Triaging atypical lobular hyperplasia and lobular carcinoma in situ on percutaneous core biopsy to surgery or observation: assiduous radiologic-pathologic correlation works, quantitating extent of disease does not. Arch Pathol Lab Med. 2019;143(5):621–627. doi:10.5858/arpa.2018-0232-OA
76. Foote FW, Stewart FW. Lobular carcinoma in situ: a rare form of mammary cancer. Am J Pathol. 1941;17(4):491–4963. doi:10.3322/canjclin.32.4.234
77. Georgian-Smith D, Lawton TJ. Calcifications of lobular carcinoma in situ of the breast: radiologic-pathologic correlation. AJR Am J Roentgenol. 2001;176(5):1255–1259. doi:10.2214/ajr.176.5.1761255
78. van Maaren MC, Avila AO, van Manen JG, et al. Trends in incidence, treatment, survival and subsequent breast cancer in lobular carcinoma in situ in the Netherlands: a population-based analysis. Breast. 2021;59:376–382. doi:10.1016/j.breast.2021.07.020
79. Rendi MH, Dintzis SM, Lehman CD, Calhoun KE, Allison KH. Lobular in-situ neoplasia on breast core needle biopsy: imaging indication and pathologic extent can identify which patients require excisional biopsy. Ann Surg Oncol. 2012;19(3):914–921. doi:10.1245/s10434-011-2034-3
80. Pleasant V. Management of breast complaints and high-risk lesions. Best Pract Res Clin Obstet Gynaecol. 2022;83:46–59. doi:10.1016/j.bpobgyn.2022.03.017
81. Wen HY, Brogi E. Lobular carcinoma in situ. Surg Pathol Clin. 2018;11(1):123–145. doi:10.1016/j.path.2017.09.009
82. D’Alfonso TM, Wang K, Chiu YL, Shin SJ. Pathologic upgrade rates on subsequent excision when lobular carcinoma in situ is the primary diagnosis in the needle core biopsy with special attention to the radiographic target. Arch Pathol Lab Med. 2013;137(7):927–935. doi:10.5858/arpa.2012-0297-OA
83. IBIS breast cancer risk evaluation tool. Available from: https://ems-trials.org/riskevaluator/.
84. National Cancer Institute. Breast cancer risk assessment tool. Available from: https://bcrisktool.cancer.gov/calculator.html.
85. Sun Y, Wei W, Yang HW, Liu JL. Clinical usefulness of breast-specific gamma imaging as an adjunct modality to mammography for diagnosis of breast cancer: a systemic review and meta-analysis. Eur J Nucl Med Mol Imaging. 2013;40(3):450–463. doi:10.1007/s00259-012-2279-5
86. Georgian-Smith D, Lawton TJ. Controversies on the management of high-risk lesions at core biopsy from a radiology/pathology perspective. Radiol Clin North Am. 2010;48(5):999–1012. doi:10.1016/j.rcl.2010.06.004
87. Monticciolo DL, Newell MS, Moy L, Niell B, Monsees B, Sickles EA. Breast cancer screening in women at higher-than-average risk: recommendations from the ACR. J Am Coll Radiol. 2018;15(3Pt A):408–414. doi:10.1016/j.jacr.2017.11.034
88. Lord SJ, Lei W, Craft P, et al. A systematic review of the effectiveness of magnetic resonance imaging (MRI) as an addition to mammography and ultrasound in screening young women at high risk of breast cancer. Eur J Cancer. 2007;43(13):1905–1917. doi:10.1016/j.ejca.2007.06.007
89. Leach MO, Boggis CR, Dixon AK, et al. Screening with magnetic resonance imaging and mammography of a UK population at high familial risk of breast cancer: a prospective multicentre cohort study (MARIBS). Lancet. 2005;365(9473):1769–1778. doi:10.1016/S0140-6736(05)66481-1
90. Port ER, Park A, Borgen PI, Morris E, Montgomery LL. Results of MRI screening for breast cancer in high-risk patients with LCIS and atypical hyperplasia. Ann Surg Oncol. 2007;14(3):1051–1057. doi:10.1245/s10434-006-9195-5
91. National Comprehensive Cancer Network. Breast cancer risk reduction. Available from: https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1420.
92. US Preventive Services Task Force. Breast cancer: medication use to reduce risk. Available from: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/breast-cancer-medications-for-risk-reduction.
93. Visvanathan K, Fabian CJ, Bantug E, et al. Use of endocrine therapy for breast cancer risk reduction: ASCO clinical practice guideline update. J Clin Oncol. 2019;37(33):3152–3165. doi:10.1200/JCO.19.01472
94. Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the national surgical adjuvant breast and bowel project P-1 study. J Natl Cancer Inst. 1998;90(18):1371–1388. doi:10.1093/jnci/90.18.1371
95. Cummings SR, Eckert S, Krueger KA, et al. The effect of raloxifene on risk of breast cancer in postmenopausal women: results from the MORE randomized trial. Multiple outcomes of raloxifene evaluation. JAMA. 1999;281(23):2189–2197. doi:10.1001/jama.281.23.2189
96. Vogel VG, Costantino JP, Wickerham DL, et al. Update of the national surgical adjuvant breast and bowel project study of tamoxifen and raloxifene (STAR) P-2 trial: preventing breast cancer. Cancer Prev Res. 2010;3(6):696–706. doi:10.1158/1940-6207.CAPR-10-0076
97. Goss PE, Ingle JN, Ales-Martinez JE, et al. Exemestane for breast-cancer prevention in postmenopausal women. N Engl J Med. 2011;364(25):2381–2391. doi:10.1056/NEJMoa1103507
98. Trivedi MS, Coe AM, Vanegas A, Kukafka R, Crew KD. Chemoprevention uptake among women with atypical hyperplasia and lobular and ductal carcinoma in situ. Cancer Prev Res. 2017;10(8):434–441. doi:10.1158/1940-6207.CAPR-17-0100
99. Ravdin PM. The lack, need, and opportunities for decision-making and informational tools to educate primary-care physicians and women about breast cancer chemoprevention. Cancer Prev Res. 2010;3(6):686–688. doi:10.1158/1940-6207.CAPR-10-0100
100. Heisey R, Pimlott N, Clemons M, Cummings S, Drummond N. Women’s views on chemoprevention of breast cancer: qualitative study. Can Fam Physician. 2006;52:624–625.
101. Cyrus-David MS, Strom SS. Chemoprevention of breast cancer with selective estrogen receptor modulators: views from broadly diverse focus groups of women with elevated risk for breast cancer. Psychooncology. 2001;10(6):521–533. doi:10.1002/pon.547
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cerebrovascular Fibromuscular Dysplasia – A Practical Review
Kesav P, Manesh Raj D, John S
Vascular Health and Risk Management 2023, 19:543-556
Published Date: 28 August 2023