")
Back to Journals » Clinical Ophthalmology » Volume 17
Prevalence of Dry Eye Disease Among Individuals Scheduled for Cataract Surgery in a Norwegian Cataract Clinic
Authors Graae Jensen P , Gundersen M , Nilsen C, Gundersen KG , Potvin R , Gazerani P , Chen X , Utheim TP, Utheim ØA
Received 23 February 2023
Accepted for publication 13 April 2023
Published 27 April 2023 Volume 2023:17 Pages 1233—1243
DOI https://doi.org/10.2147/OPTH.S407805
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Per Graae Jensen,1 Morten Gundersen,1 Christian Nilsen,1 Kjell Gunnar Gundersen,1 Rick Potvin,2 Parisa Gazerani,3 Xiangjun Chen,4– 6 Tor P Utheim,3,4,7,8 Øygunn A Utheim4,7,8
1Ifocus Eye Clinic, Haugesund, Norway; 2Science in Vision, Bend, OR, USA; 3Faculty of Health Sciences, Oslo Metropolitan University, Oslo, Norway; 4Department of Medical Biochemistry, Oslo University Hospital, Oslo, Norway; 5Department of Ophthalmology, Sørlandet Sykehus Arendal, Arendal, Norway; 6Department of Ophthalmology, Vestre Viken Hospital Trust, Drammen, Norway; 7Department of Ophthalmology, Oslo University Hospital, Oslo, Norway; 8The Norwegian Dry Eye Clinic, Oslo, Norway
Correspondence: Per Graae Jensen, Ifocus Eye Clinic, Djupaskarvegen 64 b, Haugesund, 5561, Norway, Tel +47 906 13 685, Email [email protected]
Purpose: To determine the prevalence of dry eye disease (DED) in patients scheduled for cataract surgery in a Norwegian eye clinic.
Patients and Methods: 218 patients scheduled for cataract surgery were examined for DED in one randomly selected eye and questioned regarding symptoms and risk factors. Patients were diagnosed with DED if they fulfilled the DEWS II criteria with symptom score > 12/100 with Ocular Surface Disease Index (OSDI) questionnaire, and the presence of any of the three signs: tear osmolarity > 307 mOsm/L in either eye or a difference in osmolarity between the two eyes of > 8 mOsm/L, corneal fluorescein staining (CSF) ≥ grade 2 and non-invasive tear film breakup time (NIKBUT) of < 10 seconds. Additional tests were the Standard Patient Evaluation of Eye Dryness (SPEED) questionnaire, tear meniscus height (TMH), Schirmer 1, tear film thickness (TFT), corneal sensitivity and meibography (meiboscore). Dry eye test outcomes were correlated with risk factors for DED.
Results: The prevalence of DED was 55.5% according to the DEWS II criteria. The abnormal osmolarity percentage was 66.5, while 29.8% had shortened NIKBUT and 19.7% exhibited CFS ≥ 2. 57% had Schirmer 1 ≤ 10 mm/5 min, and 81.1% had a meiboscore of ≥ 1. 71.2% of subjects scored positive for DED symptoms using the OSDI questionnaire and 69.3% using SPEED. Logistic regression analysis showed that higher age correlated with a lower OSDI symptom score, reduced corneal sensitivity and increased meibomian gland atrophy. Female sex was associated with higher odds of having DED, abnormal NIKBUT and abnormal CFS. Ocular tests for DED did not correlate with OSDI symptom scores when assessed with Spearman`s rank analysis.
Conclusion: The prevalence of DED in an elderly Norwegian population scheduled for cataract surgery is high and associated with female sex. There was a lack of correlation between signs and symptoms of DED.
Keywords: dry eye disease, cataract surgery, corneal fluorescein staining, ocular surface, osmolarity, non-invasive keratograph tear break up time, NIKBUT, meibomian gland dysfunction
Introduction
Dry eye disease (DED) is a common clinical disorder of the anterior ocular surface characterized by an unstable tear film causing discomfort and visual impairment.1 DED occurs as a result of increased evaporation of the tear film and/or reduced tear production.2 Increased evaporation is considered to be the main cause of DED, and is characterized by meibomian gland dysfunction (MGD).3 The most common cause of decreased tear production is age-related hyposecretion.4 Autoimmune conditions like Sjögren’s syndrome can also reduce tear production through the breakdown of the glandular tissue.4
The prevalence of DED varies from 5 to 50% depending on the evaluation criteria.5–8 DED is associated with risk factors like higher age, gender, genetic predisposition, history of arthritis, smoking, diabetes, hypertension and rheumatic disease.8–10 Anti-hypertensive, diabetic medications, anti-depressants, statins and other medications may cause dry eye secondary to decreased tear production, alteration of nerve input including reflex secretion and decreased corneal sensation or a direct inflammatory effect on secretory glands.11,12 In addition, environmental factors like indoor and outdoor climate and the use of visual display unit (VDU) may increase DED prevalence and severity.13
Over the years, various definitions and diagnostic criteria for DED have been proposed. In 2017, the Tear Film & Ocular Surface Society Dry Eye Workshop (TFOS/DEWSII®) Report offered an updated definition based on meta-analyses and reviews of the literature.14 The TFOS DEWSII report proposed the following tests for diagnosing DED: the Ocular Surface Disease Index (OSDI) or Dry Eye Questionnaire (DEQ-5), osmolarity, ocular surface staining (OSS), and non-invasive tear breakup time (NITBUT). In addition, etiological factors can be measured using tear production (Schirmer 1), meibography and corneal sensitivity (CS).14 The Standard Patient Evaluation of Eye Dryness (SPEED) questionnaire is developed for use prior to ocular surgery, and unlike OSDI, does not include questions regarding visual disturbances that may be due to cataract as well as tear film instability.15
DED is an important aspect of cataract surgery both pre- and postoperatively. Numerous studies have shown that an unstable tear film can alter the preoperative biometric measurement, leading to a higher variability and inaccurate IOL power calculation with the potential for an unsatisfactory postoperative result.16–18 Furthermore, cataract surgery is known to either induce or exacerbate preexisting DED, and more than 50% of patients suffer from sore, red eyes, and general ocular discomfort after cataract surgery.19
Previous studies have found a high prevalence of DED in patients scheduled for cataract surgery. Gupta et al found that 80% of their study population, had at least 1 abnormal test result suggestive of DED before cataract surgery.19 Similarly, Trattler et al demonstrated that up to 62% of patients presenting for surgery had a tear film break-up time (TBUT) of < 5 seconds and 77% had positive corneal staining.20 Studies have pointed out that an impaired ocular surface might have an effect on surgical planning with keratometry variability and affect the postoperative outcome, with subsequent patient dissatisfaction. Consequently, preoperative examination to identify and manage any DED is becoming increasingly important.16,21–23
In this prospective, cross-sectional single-center study, we aimed to determine whether the prevalence of signs and symptoms of DED in a cohort of patients scheduled for cataract surgery in an eye clinic located on the west coast of Norway was similar to data in the previous literature.
Materials and Methods
This prospective cross-sectional study was conducted from August 2020 to January 2022. The study population consisted of patients presenting for routine standard phacoemulsification cataract surgery at a single clinical site in Haugesund, Norway. The study followed the tenets of the Declaration of Helsinki and was approved by the Regional Committee for Medical and Health Research Ethics in Norway (Ref. 2020/64847). Informed consent was obtained from all participants. Inclusion criteria included patients who were scheduled for cataract surgery, willing and able to participate in the study, with good mental health, and no systemic disease that would impact the corneal surface. Exclusion criteria were any manifestation of corneal disease or scarring and previously performed corneal refractive procedures. Patients were instructed not to wear contact lenses on the day of examination and not to use any eye drops at least two hours before the examination. The current study is part of a larger project which is investigating the ocular surface before and after surgery.
One eye was randomly selected as the study eye and dry eye examinations were performed only on the study eye, except for osmolarity testing. Osmolarity was measured in both eyes as required by the manufacturer’s instructions. Symptom scores for dry eye disease were assessed with two validated questionnaires, the OSDI and SPEED. The OSDI is expressed in a number from 0 to 100 with higher scores indicating the degree of disability. Summary scores of the questions of the SPEED questionnaire were derived by summing the 0 to 4 scores of each of the 8 questions, and the total is referred as the SPEED score in the range of 0 to 28.1,15 The cutoff score for diagnosing DED was a score ≥13 for OSDI and ≥ 4 for SPEED. In addition, all participants answered a questionnaire regarding medical and medication history, height and weight, use of heat pump at home, smoking, alcohol consumption, breakfast, and activity/training.
An extensive dry eye examination was performed in the following order, with a 3-minute break between each test to standardize the measurements: 1. Tear film osmolarity (Tearlab Osmolarity system, Tearlab Corp, Escondido, California, USA).24 Osmolarity values ≥ 307 mOsm/L in either eye or an inter-eye difference > 8 mOsm/L, were considered as dry or indicating abnormal osmolarity.14 As recommended by the TearLab manufacturer, the measurement from the eye that had the highest osmolarity was used for further analyses. Calibration of the TearLab instrument was performed daily to control for temperature and humidity. 2. Non-invasive keratograph tear break up time (NIKBUT) (OCULUS Keratograph 5M, Medistim, Norway).25 The cut-off criteria for diagnosing dry eyes was <10 seconds for the average measurements.1 3. Bulbar redness (BR), graded 0–4 by the keratograph software (OCULUS Keratograph 5M).26 4. Tear meniscus height (TMH) in mm, with 0.2 mm as the cut-off value for a DED diagnosis (OCULUS Keratograph 5M). 5. Tear film thickness (TFT) (Lipiview II Interferometer, TearScience Inc., Morrisville, NC). A cut-off value of 75 nm was used.27,28 6. Corneal fluorescein staining (CFS). Five µL of fluorescein sodium 2% (without anesthesia) was instilled into the inferior fornix. After 0.5 to 1 minute, the punctate staining of the cornea (CFS) was assessed in a slit lamp biomicroscope at 16 times magnification and cobalt blue light with yellow barrier filter according to the Oxford grading scheme (0–5).29 Subjects with corneal staining of grade 2 and above were categorized as having DED. 7. Tear production was tested with Schirmer strips without anesthesia (Schirmer 1) (TearFlo, MDT, Krakow, Poland). Subjects with a Schirmer test < 10 mm after 5 minutes were considered to have abnormal tear production.30 8. Corneal sensitivity (CS) (Cochet-Bonnet esthesiometer, Luneau SAS, Aesthesiometer 12/100 mm)31 with a grading scale of 0–6 mm, where 6 mm is considered normal, and ≤ 5 considered abnormal. 9. Meibum quality and expressibility were assessed according to DEWSII with some modifications.1 In brief, the 5 central gland orifices of the lower eyelid were examined for meibum in a slit lamp biomicroscope after pressing a cotton swab gently towards the margin of the lower eyelid. Expressibility was graded 0–3; grade 0 when all glands were expressible, grade 1 when 3–4 glands were expressible, grade 2 when 1–2 glands were expressible, and grade 3 where no glands were expressible. The meibum was graded from 0–3: grade 0 showed a clear meibum fluid, grade 1 a cloudy meibum, grade 2 a granular meibum and grade 3 a thick, toothpaste-looking meibum. 10. Meibomian gland dropout (meiboscore) was assessed from infrared images of the lower eye lid (Oculus Keratograph 5M). Grade 0 represented no loss of meibomian glands, grade 1; < 1/3 of glands lost, grade 2; 1/3 – 2/3 glands lost and grade 3; >2/3 glands lost.32
Total prevalence was calculated based on the DEWS II criteria; positive symptom score (OSDI score ≥ 13) plus at least one positive result of the markers of homeostasis (Osmolarity, CFS and/or NIKBUT).
Statistical analysis was performed using the Statistical Package for the Social Sciences (IBM, SPSS Statistics, version 14.0). Testing for normal distribution was performed by using the Kolmogorov–Smirnov test. Continuous data were described as median with interquartile range (IQR), and categorical data in frequencies or percentages. Pearson’s chi-square test was used to compare categorical values and a Mann–Whitney U-test, was used to compare the continuous data. The correlation between ocular DED tests and symptom scores from questionnaires was tested with Spearman’s rank order correlation for nonparametric variables. Logistic regression analyses were computed to address the relationship of independent variables with DED overall, OSDI and objective tests, and the odds ratio was calculated. p < 0.05 was considered to indicate a statistically significant difference.
Results
A total of 222 consecutive patients scheduled to undergo routine cataract surgery met the study criteria. The majority of the patients (95%) were recruited from a small town (Haugesund) along the west coast of Norway, and the rest from the nearby district. Four patients were excluded from the study because they were not able to complete the extensive examination. The inclusion and examination of the patients were distributed throughout four seasons, with average indoor temperatures varying from 22.1°C to 26.7°C, and humidity from 19% to 50%. Patient demographics and characteristics are shown in Table 1. The median patient age at the time of cataract evaluation was 75 years with a range from 47 to 91 years. Fifty-seven percent of the study population were women. Other demographic information included a history of DED with patients using artificial tears minimum twice daily in 28.9% (63 patients); 19.9% (39 patients) had a history of diabetes mellitus, and 63.3% (138 patients) had an installed heat pump at home.
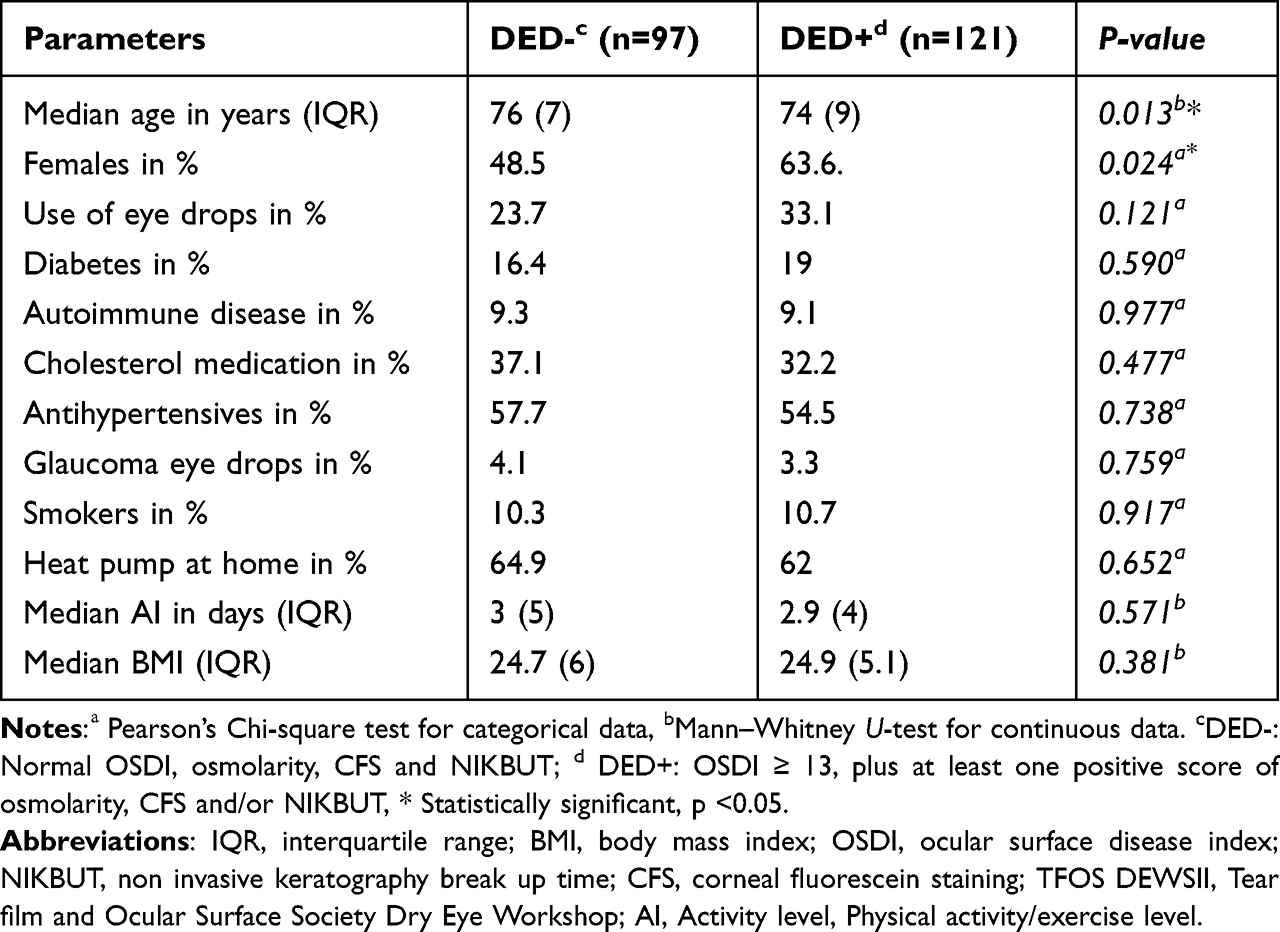 |
Table 1 Demographics and Characteristics of DED Negative (DED-) versus DED Positive (DED+) Subjects According to DEWSII Criteria |
The prevalence of DED according to the DEWSII criteria (with positive OSDI and at least one positive test of Osmolarity, CFS or NIKBUT) was 55.5% (Figure 1). Patients who had symptom scores suggestive of dry eye were 71.2% for OSDI and 69.3% for the SPEED questionnaire. There were no statistically significant differences in percentages of dry eye diagnosis for the two questionnaires (p=0.7). Tear film osmolarity was the most sensitive of the three DEWSII diagnostic tests. 66.5% of patients had abnormal osmolarity, while 29.8% had an unstable tear film (NIKBUT average) and 19.7% exhibited corneal staining. Results from other DED tests indicated that 57% had reduced tear production by Schirmer 1 test, 38.5% had reduced corneal sensitivity and 49.2% had thinning of the tear film (TFT). MGD with a meiboscore ≥ grade 1 was present in 80.1% of patients.
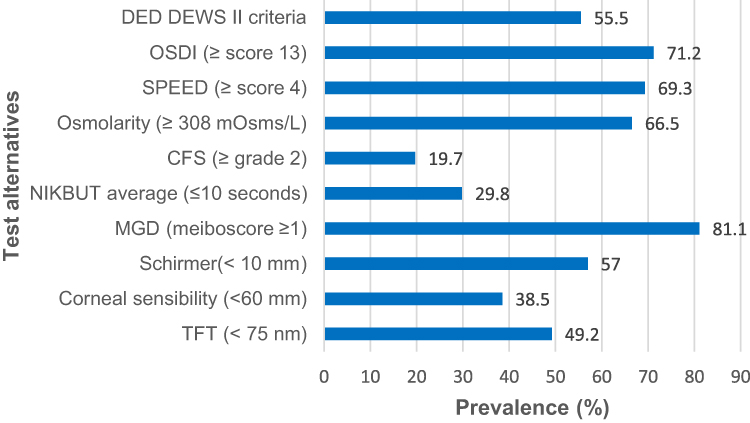 |
Figure 1 The prevalence of DED in % based on DEWS II criteria, subdivided based on dry eye tests. Abbreviations: DED, dry eye disease; DEWS II criteria, According to the Tear Film & Ocular Surface society (TFOS) symptoms and at least one positive result of the markers of homeostasis (Osmolarity, NIKBUT and CFS); OSDI, ocular surface disease Index; SPEED, standard patient evaluation of eye dryness; CFS, corneal fluorescein staining; NIKBUT, non-Invasive keratograph break-up time; MGD, meibomian gland dysfunction; TFT, tear film thickness. |
The association between DED and its signs and symptoms with age and gender were explored in a simple logistic regression model (Table 2). The odds of having DED (based on the DEWS II criteria) were significantly higher in women (male/female OR 1.76, 95% CI 1.10–3.06, p=0.043). The odds of being symptomatic for DED were not significantly higher for women. The odds of having abnormal CFS (OR 1.19, 95% CI 1.05–4.53, p=0.035) and abnormal NIKBUT average (OR 2.00, 95% CI 1.08–3.70, p=0.028) were significantly higher for women. The prevalence of DED (DEWS II criteria) was not significantly associated with age (OR 0.96, 95% CI 0.92–1.00, p=0.09). However, the odds of being symptomatic for DED (OSDI) were associated with younger age (OR 0.92, 95% CI 0.87–0.9, p=0.003). Meibomian gland atrophy was statistically significantly associated with higher age (OR 1.06, 95% CI 1.01–1.12, p=0.01). The risk of having reduced corneal sensitivity was also associated with higher age (OR 1.08, 95% CI 1.02–1.13, p=0.002).
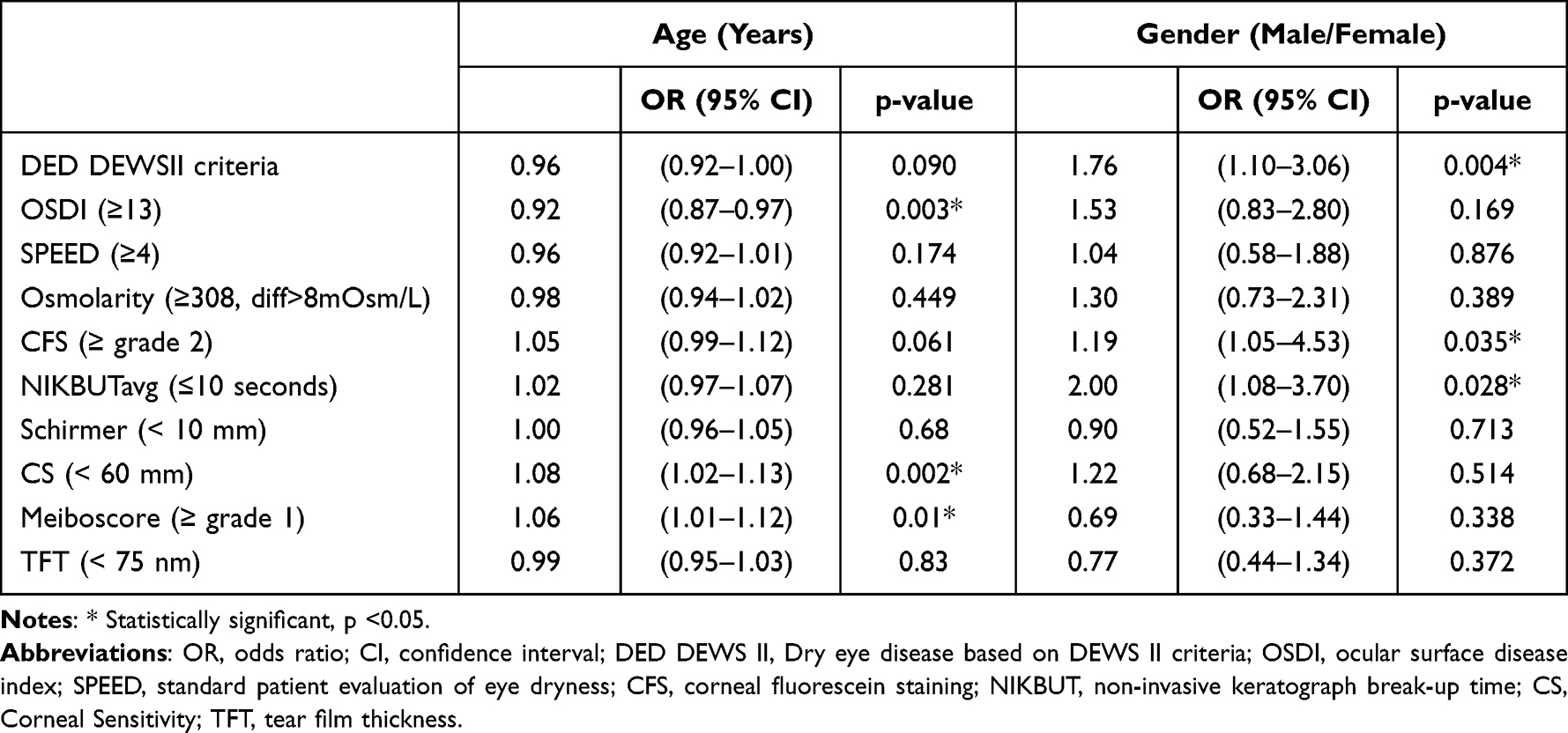 |
Table 2 Association Between DED and Its Signs and Symptoms with Age and Gender in a Simple Logistic Regression Model |
Patients were sub-grouped based on having DED (DED+) or not (DED-) using the DEWSII diagnostic criteria and tested for differences in risk factors for DED. Data for subgroups are presented in Table 1. Patients with DED were statistically significantly younger than non-DED patients (median age 74 years for DED+ versus 76 for DED-, p< 0.013). More DED+ patients were women (63.6% versus 48.5% of DED- patients). For women, the numerically higher distribution in the DED+ group was statistically significant (p= 0.024). The distribution of systemic diseases (diabetes mellitus, autoimmune diseases), use of glaucoma-medication and systemic drugs (anti-hypertensive and cholesterol-lowering) lifestyle (smoking, activity level, BMI) and environmental factors (heat pump) were not statistically significantly different between the sub-groups. With regards to the distribution of abnormal objective tests, there was no statistical significance difference between symptomatic and asymptomatic patients (Table 3).
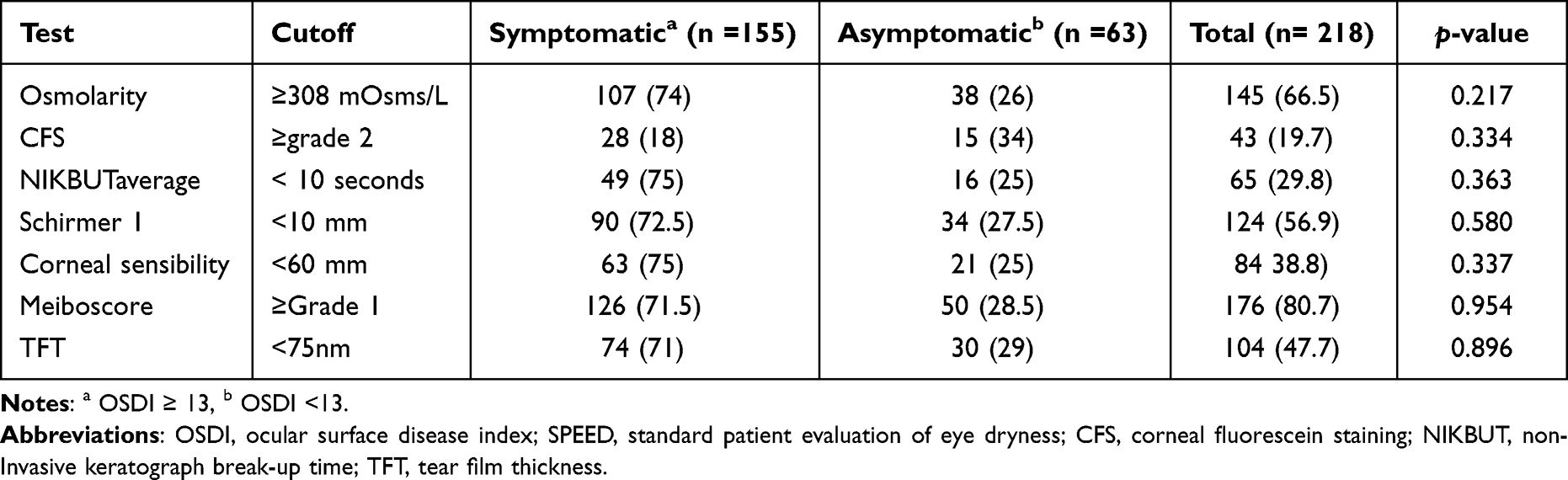 |
Table 3 Distribution of Abnormal Tests in the Study Population (%) |
A Spearman`s rank correlation was computed to assess the relationship between objective DED tests and subjective questionnaire scores (Table 4). We found no correlation between OSDI and any of the objective tests. SPEED showed a weak negative correlation with NIKBUT average (r= 0.17, p=0.009), and a weak positive correlation with tear film thickness (TFT, r=0.18, p=0.009). CFS had a positive correlation with osmolarity, NIKBUT, TFT and Schirmer testing. There was a weak negative correlation between age and OSDI (r=−0.172, p=0.011), age and SPEED (r=−0.143, p=0.035) and CS (r=−0.171, p=0.012). There was no correlation between OSDI and CS (r=0.065, p=0.33).
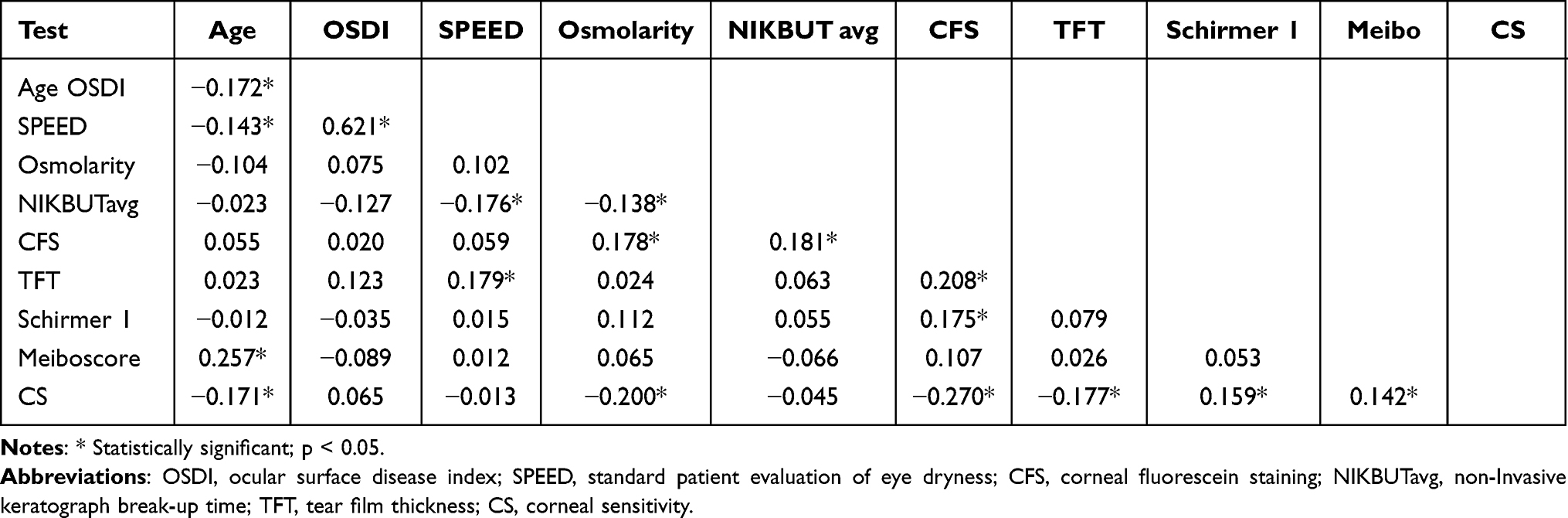 |
Table 4 Correlation Matrix of Objective DED Test and Subjective Questionnaires, Spearman`s Rho Correlation Coefficient |
The population was sub-categorized by severity level (normal, mild, moderate and severe) based on osmolarity scores, CSF, NIKBUT and OSDI. Osmolarity was normal and mildly positive in most patients (33.5% normal and 39.4% mild) (Figure 2A). Similarly, 80.3% of the patients had normal and mild corneal staining on slit lamp evaluation (Figure 2B), and 70.2% of patients were characterized with normal NIKBUT (Figure 2C). As regards to symptom scores with OSDI, 28.9% were normal and 16.1% were mildly affected. In contrast to the objective diagnostic tests where very few of the patients had moderate and severe scores, 19.3% had moderate and 35.8% had severe symptoms when responding to the OSDI (Figure 3A and B). There was no statistically significant difference between the score distribution of the two questionnaires (p = 0.621).
 |
Figure 2 Distribution of: osmolarity grading severity (A), corneal fluorescein staining (CFS) (B), abnormal non-invasive keratography breakup time (NIKBUT) (C) in the study population. |
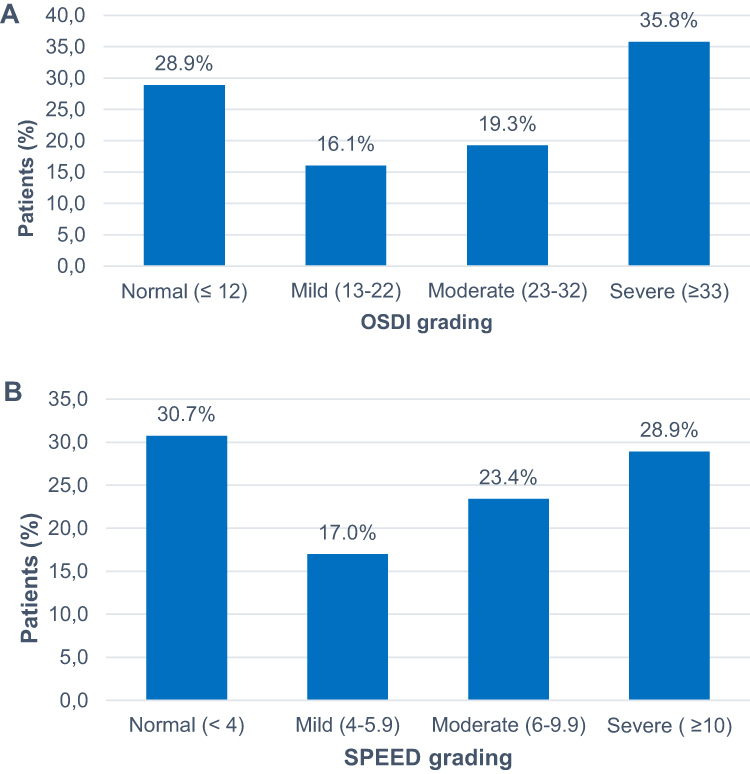 |
Figure 3 Distribution of: the ocular surface disease index (OSDI) questionnaire score (A), the standard patient evaluation of eye dryness questionnaire (SPEED) score in the study population (B). |
The matrix results of the severity of dry eye symptoms based on OSDI questionnaire and the number of positive objective signs (Table 5) further underline the discrepancy between subjective and objective testing in this population. Only 17.1% were asymptomatic with none or one positive objective sign of DED.
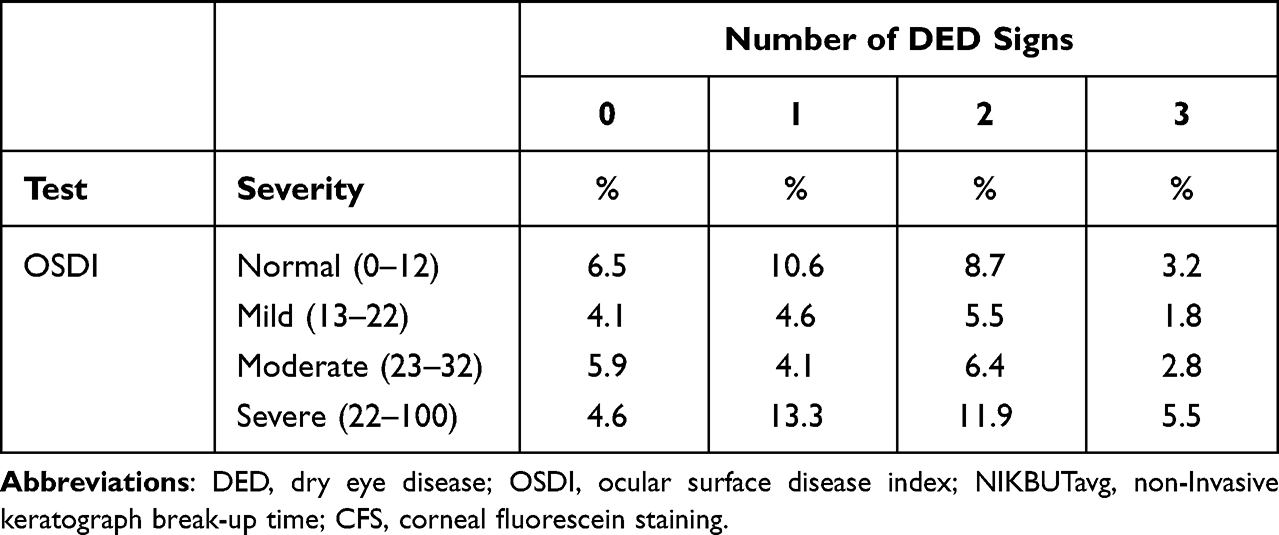 |
Table 5 Matrix Results of the Severity of Dry Eye Symptoms Based on the Ocular Surface Disease Index (OSDI) and the Number of Positive DED Signs (Osmolarity, NIKBUTavg, CSF) |
Discussion
The prevalence of DED in our study population was 55.1% using the DED definition from the DEWS II diagnostic report.1 The percentage is higher than in previous population-based prevalence studies using a combination of symptoms and signs, where the percentages varied from 8.7 to 30.1%.6,33–35 The large variation reported in the literature has been suggested to originate from variations in DED diagnostic criteria, and the use of different questionnaires and dry eye tests.1 In addition, various studies have investigated different age groups (40–96 years). In our study, the median age was 75 years, which is higher than most other previous studies and could be a possible explanation of the reason for the high prevalence of DED since age has been reported to be a risk factor for DED. Noor et al investigated the prevalence of DED in cataract patients in Indonesia (mean age of 75 years) and found that 22.5% were affected.36 The Prospective Health Assessment of Cataract Patients Ocular surface (PHACO) study showed that up to 80% of patients scheduled for cataract surgery had signs of DED in the ocular surface. Seventy-seven percent had corneal staining, and 63% with TBUT < 5 seconds. The mean age of the patients in the PHACO study was 70.7 years.20 Gupta et al found that 80% of patients had at least one abnormal ocular surface test for DED (osmolarity or MMP-9 inflammatory test) prior to cataract surgery, and 40% had two abnormal tests.19 This is consistent with our findings that 77% of patients had at least one, and 46% had two or three positive tests (osmolarity, NIKBUT, CFS).
Multiple studies have identified high age as a major risk factor for DED.35,37–39 We found that the prevalence of DED based on the DEWS II criteria was approaching but not reaching significantly levels of association with age (p=0.09) even though, meibomian gland atrophy increased with age. Moreover, a weak negative correlation was found between age and OSDI, and between age and CS, suggesting that participants with higher age are less likely to experience symptoms due to reduced CS. However, OSDI and CS did not correlate, rendering some uncertainty to reduced CS as an explanatory factor to the finding of fewer DED symptoms among the elderly.
A meta-analysis of DED epidemiology showed that women have a prevalence rate 1.3–1.5 times higher than men, including both signs and symptoms.7 This is in line with our results, where 63% (p=0.023) of our patients with DED were women, and the odds of having DED were significantly higher for females (p=0.004). In our study we found a high level of patients with Schirmer score below 10 mm, which is associated with more severe DED.40 The high percentage of aqueous deficient dry eye disease (ADDE) is in line both with a larger Norwegian cohort of patients that sought help for DED and cohorts of cataract patients.40–42 Even though the prevalence of reduced tear production was 57%, the number of patients that reported using ocular lubricants regularly was only 28%. Therefore, our data suggest that treatment with artificial tears prior to surgery should be considered even in asymptomatic patients.
Despite the rather high prevalence of patients with symptoms of DED in this study population, none of the ocular dry-eye tests correlated with OSDI. However, the SPEED scores showed a weak negative correlation with NIKBUT and a weak positive correlation with TFT. Multiple studies have explored correlations between dry eye symptoms and ocular surface dry eye tests, with mostly conflicting and non-significant findings.43–46 However Lee et al found a correlation between OSDI and NIKBUT for the first breakup time (r= −0.33) and lipid layer thickness (LLT, r= −0.42).47 Also, Blackie et al reported that LLT was significantly correlated with severe symptoms using the SPEED questionnaire.48 Due to the low correlation coefficients in both Lee et al, Blackie et al, and our study, the clinical utility of the correlations is questionable. Nevertheless, our findings that the TFT is linked to symptoms, suggest further research in this area might be beneficial.
Only a few, weak correlations were found between the DED tests used in the study. This could be explained by the multi-factorial nature of DED and that each single dry eye test represents different segments of the DED diagnostic universe. It also underpins the lack of a gold standard for diagnosing DED. Our data suggest that many ocular surface dry eye tests and at least one symptom score questionnaire should be used to screen for DED due to the lack of correlation between tests. In a clinical setting this is time-consuming and uncomfortable for the patient. A simple and evidence-based diagnostic test would be valuable, but evidence supporting a simplified approach is lacking, as is apparent from our findings and those of previous researchers.
There are some limitations to this study. First, the single-center study design may affect the generalizability of the prevalence data. Second, the examinations were complex and time-consuming with many tests and three trained technicians involved, which might have caused a higher variability of the measurements. Third, differences in temperature and humidity during the study period could have affected the dry-eye tests and patient-reported symptoms.
Conclusion
The prevalence of DED in an elderly Norwegian population scheduled for cataract surgery is high and associated with the female sex. Meibomian gland atrophy, but not symptomatic DED increased with age. Both aqueous deficient dry eye and meibomian gland dysfunction are common and should be tested for and treated prior to surgery. Further studies are warranted to identify diagnostic tests that correlate better with symptoms.
Ethical Statement
The research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. The study was approved by the Regional Committee for Medical and Health Research Ethics in Norway (Ref. 2020/64847). All participants have provided written informed consent to participate in this study.
Acknowledgments
The authors wish to thank Bjørn Gjerdrum, PhD, Ifocus Eye Clinic, Haugesund, Norway for help with statistics and writing advice.
Funding
This study was supported by The Research Council of Norway (project nr. 306649).
Disclosure
Dr Per Graae Jensen reports grants from The Research Council of Norway, during the conduct of the study. Dr Morten Gundersen reports grants from Norwegian research council, during the conduct of the study. Dr Rick Potvin reports personal fees from Alcon, personal fees from Carl Zeiss Meditec, outside the submitted work. Dr Øygunn A Utheim reports grants from The Research Council of Norway, during the conduct of the study; received artificial tear fluid from Thea Pharma, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II Diagnostic Methodology report. Ocul Surf. 2017;15(3):539–574. doi:10.1016/j.jtos.2017.05.001
2. Bron AJ, de Paiva CS, Chauhan SK, et al. TFOS DEWS II pathophysiology report. Ocul Surf. 2017;15(3):438–510.
3. Nichols KK, Foulks GN, Bron AJ, et al. The international workshop on meibomian gland dysfunction: executive summary. Invest Ophthalmol Vis Sci. 2011;52(4):1922–1929.
4. Lemp MA. The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007;5(2):75–92.
5. Viso E, Rodriguez-Ares MT, Gude F. Prevalence of and associated factors for dry eye in a Spanish adult population (the Salnes Eye Study). Ophthalmic Epidemiol. 2009;16(1):15–21.
6. Hashemi H, Khabazkhoob M, Kheirkhah A, et al. Prevalence of dry eye syndrome in an adult population. Clin Exp Ophthalmol. 2014;42(3):242–248.
7. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II Epidemiology Report. Ocul Surf. 2017;15(3):334–365.
8. Moss SE, Klein R, Klein BE. Long-term incidence of dry eye in an older population. Optom Vis Sci. 2008;85(8):668–674.
9. Moss SE, Klein R, Klein BE. Prevalence of and risk factors for dry eye syndrome. Arch Ophthalmol. 2000;118(9):1264–1268.
10. Aldaas KM, Ismail OM, Hakim J, et al. Association of Dry Eye Disease With Dyslipidemia and Statin Use. Am J Ophthalmol. 2020;218:54–58.
11. Gomes JAP, Azar DT, Baudouin C, et al. TFOS DEWS II iatrogenic report. Ocul Surf. 2017;15(3):511–538.
12. Frederick T, Fraufelder FWF, Wiley A. Chambers. In: Clinical Ocular Toxicology. Drugs, Chemicals and Herbs. Philadephia: Elsevier Saunders; 2008.
13. Donthineni PR, Shanbhag SS, Basu S. An Evidence-Based Strategic Approach to Prevention and Treatment of Dry Eye Disease, a Modern Global Epidemic. Healthcare. 2021;9(1):653.
14. Craig JP, Nelson JD, Azar DT, et al. TFOS DEWS II Report Executive Summary. Ocul Surf. 2017;15(4):802–812.
15. Asiedu K, Kyei S, Mensah SN, Ocansey S, Abu LS, Kyere EA. Ocular Surface Disease Index (OSDI) Versus the Standard Patient Evaluation of Eye Dryness (SPEED): a Study of a Nonclinical Sample. Cornea. 2016;35(2):175–180.
16. Epitropoulos AT, Matossian C, Berdy GJ, Malhotra RP, Potvin R. Effect of tear osmolarity on repeatability of keratometry for cataract surgery planning. J Cataract Refract Surg. 2015;41(8):1672–1677.
17. Teshigawara T, Meguro A, Mizuki N. The Effect of Rebamipide on Refractive Accuracy of Cataract Surgery in Patients with Dry Eye. Ophthalmol Ther. 2022;11(2):603–611.
18. Hovanesian J, Epitropoulos A, Donnenfeld ED, Holladay JT. The Effect of Lifitegrast on Refractive Accuracy and Symptoms in Dry Eye Patients Undergoing Cataract Surgery. Clin Ophthalmol. 2020;14:2709–2716.
19. Gupta PK, Drinkwater OJ, VanDusen KW, Brissette AR, Starr CE. Prevalence of ocular surface dysfunction in patients presenting for cataract surgery evaluation. J Cataract Refract Surg. 2018;44(9):1090–1096.
20. Trattler WB, Majmudar PA, Donnenfeld ED, McDonald MB, Stonecipher KG, Goldberg DF. The Prospective Health Assessment of Cataract Patients’ Ocular Surface (PHACO) study: the effect of dry eye. Clin Ophthalmol. 2017;11:1423–1430.
21. Chuang J, Shih KC, Chan TC, Wan KH, Jhanji V, Tong L. Preoperative optimization of ocular surface disease before cataract surgery. J Cataract Refract Surg. 2017;43(12):1596–1607.
22. Miyake K, Yokoi N. Influence on ocular surface after cataract surgery and effect of topical diquafosol on postoperative dry eye: a multicenter prospective randomized study. Clin Ophthalmol. 2017;11:529–540.
23. Gibbons A, Ali TK, Waren DP, Donaldson KE. Causes and correction of dissatisfaction after implantation of presbyopia-correcting intraocular lenses. Clin Ophthalmol. 2016;10:1965–1970.
24. Osmolarity test cards, Instructions for use In: TearLab Corporation HSSSD, CA 92121, USA, ed. Molenstraat 15, 2513 BH The Hague, the Netherlands. 2016.
25. OCULUS Optikgeräte GmbH. Oculus Keratograph Instruction Manual. Wetzlar, Germany: OCULUS Optikgeräte GmbH; 2017.
26. Wu S, Hong J, Tian L, Cui X, Sun X, Xu J. Assessment of Bulbar Redness with a Newly Developed Keratograph. Optom Vis Sci. 2015;92(8):892–899.
27. Herbaut A, Liang H, Denoyer A, Baudouin C, Labbé A. Tear film analysis and evaluation of optical quality: a review of the literature. J Fr Ophtalmol. 2019;42(2):e21–e35.
28. Finis D, Pischel N, Schrader S, Geerling G. Evaluation of lipid layer thickness measurement of the tear film as a diagnostic tool for Meibomian gland dysfunction. Cornea. 2013;32(12):1549–1553.
29. Bron AJ, Evans VE, Smith JA. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea. 2003;22(7):640–650.
30. de Monchy I, Gendron G, Miceli C, Pogorzalek N, Mariette X, Labetoulle M. Combination of the Schirmer I and phenol red thread tests as a rescue strategy for diagnosis of ocular dryness associated with Sjogren’s syndrome. Invest Ophthalmol Vis Sci. 2011;52(8):5167–5173.
31. Chao C, Stapleton F, Badarudin E, Golebiowski B. Ocular surface sensitivity repeatability with Cochet-Bonnet esthesiometer. Optom Vis Sci. 2015;92(2):183–189.
32. Arita R, Itoh K, Inoue K, Amano S. Noncontact infrared meibography to document age-related changes of the meibomian glands in a normal population. Ophthalmology. 2008;115(5):911–915.
33. Tian YJ, Liu Y, Zou HD, et al. 上海市江宁街道20岁及以上人群干眼的流行病学调查[Epidemiologic study of dry eye in populations equal or over 20 years old in Jiangning District of Shanghai]. Zhonghua Yan Ke Za Zhi. 2009;45(6):486–491. Chinese.
34. Millán A, Viso E, Gude F, Parafita-Fernández A, Moraña N, Rodríguez-Ares MT. Incidence and Risk Factors of Dry Eye in a Spanish Adult Population: 11-Year Follow-Up From the Salnés Eye Study. Cornea. 2018;37(12):1527–1534.
35. Malet F, Le Goff M, Colin J, et al. Dry eye disease in French elderly subjects: the Alienor Study. Acta Ophthalmol. 2014;92(6):e429–436.
36. Noor NA, Rahayu T, Gondhowiardjo TD. Prevalence of Dry Eye and its Subtypes in an Elderly Population with Cataracts in Indonesia. Clin Ophthalmol. 2020;14:2143–2150.
37. Farrand KF, Fridman M, Stillman I, Schaumberg DA. Prevalence of Diagnosed Dry Eye Disease in the United States Among Adults Aged 18 Years and Older. Am J Ophthalmol. 2017;182:90–98.
38. Schaumberg DA, Sullivan DA, Buring JE, Dana MR. Prevalence of dry eye syndrome among US women. Am J Ophthalmol. 2003;136(2):318–326.
39. Jie Y, Xu L, Wu YY, Jonas JB. Prevalence of dry eye among adult Chinese in the Beijing Eye Study. Eye. 2009;23(3):688–693.
40. Yazdani M, Chen X, Tashbayev B, et al. Tear Production Levels and Dry Eye Disease Severity in a Large Norwegian Cohort. Curr Eye Res. 2018;43(12):1465–1470.
41. Sidaraite A, Mikalauskiene L, Grzybowski A, Zemaitiene R. Evaluation of Ocular Surface after Cataract Surgery-A Prospective Study. J Clin Med. 2022;11:15.
42. Kohli P, Arya SK, Raj A, Handa U. Changes in ocular surface status after phacoemulsification in patients with senile cataract. Int Ophthalmol. 2019;39(6):1345–1353.
43. Begley CG, Chalmers RL, Abetz L, et al. The relationship between habitual patient-reported symptoms and clinical signs among patients with dry eye of varying severity. Invest Ophthalmol Vis Sci. 2003;44(11):4753–4761.
44. Adatia FA, Michaeli-Cohen A, Naor J, Caffery B, Bookman A, Slomovic A. Correlation between corneal sensitivity, subjective dry eye symptoms and corneal staining in Sjögren’s syndrome. Can J Ophthalmol. 2004;39(7):767–771.
45. Mizuno Y, Yamada M, Miyake Y. Association between clinical diagnostic tests and health-related quality of life surveys in patients with dry eye syndrome. Jpn J Ophthalmol. 2010;54(4):259–265.
46. Sullivan BD, Whitmer D, Nichols KK, et al. An objective approach to dry eye disease severity. Invest Ophthalmol Vis Sci. 2010;51(12):6125–6130.
47. Lee JH, Kim CH, Choe CM, Choi TH. Correlation Analysis between Ocular Surface Parameters with Subjective Symptom Severity in Dry Eye Disease. Korean J Ophthalmol. 2020;34(3):203–209.
48. Blackie CA, Solomon JD, Scaffidi RC, Greiner JV, Lemp MA, Korb DR. The relationship between dry eye symptoms and lipid layer thickness. Cornea. 2009;28(7):789–794.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.