Back to Journals » Patient Preference and Adherence » Volume 16
Patient-Reported Barriers to Adherence Among ACEI/ARB Users from a Motivational Interviewing Telephonic Intervention
Authors Majd Z, Mohan A, Johnson ML, Essien EJ ![]() , Barner JC
, Barner JC ![]() , Serna O, Gallardo E, Fleming ML, Ordonez N, Holstad MM
, Serna O, Gallardo E, Fleming ML, Ordonez N, Holstad MM ![]() , Abughosh SM
, Abughosh SM
Received 3 February 2022
Accepted for publication 15 July 2022
Published 4 October 2022 Volume 2022:16 Pages 2739—2748
DOI https://doi.org/10.2147/PPA.S360461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Zahra Majd,1 Anjana Mohan,1 Michael L Johnson,1 Ekere J Essien,1 Jamie C Barner,2 Omar Serna,3 Esteban Gallardo,3 Marc L Fleming,4 Nancy Ordonez,5 Marcia M Holstad,6 Susan M Abughosh1
1Department of Pharmaceutical Health Outcomes and Policy, University of Houston College of Pharmacy, Houston, TX, USA; 2Health Outcomes Division, The University of Texas at Austin, Austin, TX, USA; 3CareAllies, Houston, TX, USA; 4Department of Pharmaceutical Economics and Policy, Chapman University School of Pharmacy, Irvine, CA, USA; 5Department of Pharmacy Practice and Translational Research, University of Houston College of Pharmacy, Houston, TX, USA; 6Nell Hodgson Woodruff School of Nursing, Emory University, Atlanta, GA, USA
Correspondence: Susan M Abughosh, Department of Pharmaceutical Health Outcomes and Policy, University of Houston College of Pharmacy, Health 2 Room 4048, 4349 Martin Luther King Boulevard, Houston, TX, 77204-5047, USA, Tel +1 832-842-8395, Fax +1 832-842-8383, Email [email protected]
Purpose: Hypertension is a common comorbidity among type 2 diabetes mellitus (T2DM) patients, which increases the risk of cardiovascular diseases. Despite the proven benefit of angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) in this population, poor medication adherence is prevalent, resulting in higher complications and mortality rate. Motivational interviewing (MoI) has demonstrated effectiveness in improving medication adherence and identifying barriers. This study aimed to assess and identify patient-reported barriers to adherence to ACEI/ARB from an MoI telephonic intervention conducted by student pharmacist interns.
Patients and Methods: This retrospective study was conducted within an MoI intervention customized by past ACEI/ARB adherence trajectories for nonadherent patients with T2DM and hypertension enrolled in a Medicare Advantage Plan. Adherence barriers were extracted from the interviewers’ notes by two independent researchers. Descriptive analysis was performed to summarize the overall frequency of barriers as well as across trajectory groups, identified from the initial and follow-up calls.
Results: In total, 247 patients received the initial MoI call from which 41% did not communicate any barrier for ACEI/ARB use despite having low adherence. About 59% of the patients reported at least one barrier during the initial call. The most common barriers included forgetfulness, discontinuation by physicians, side effects, multiple comorbidities, polypharmacy, lack of knowledge about disease/medication, and cost issues. The follow-up calls helped with uncovering at least one new barrier for 28 patients who previously communicated a different issue with their medication during the first call. Additionally, 18 patients with initial denial for having any barrier to adherence reported at least one barrier throughout the follow-up calls.
Conclusion: This study summarized patient-reported barriers to ACEI/ARB adherence from an MoI telephonic intervention performed among nonadherent patients. Identifying specific barriers for patients may help to further design tailored interventions that address the barriers and improve adherence.
Keywords: angiotensin converting enzyme inhibitors, angiotensin receptor blockers, adherence barriers, group-based trajectory modeling, motivational interviewing, polypharmacy
Introduction
Hypertension (HTN) is a common comorbid condition with type 2 diabetes mellitus (T2DM). According to a recent study on National Health and Nutrition Examination Survey (NHANES) 2017–2018, the prevalence of HTN in T2DM patients was ranged from 67.6% to 80.4%.1 HTN is a major, yet modifiable risk factor for cardiovascular disease (CVD) among diabetic patients.2 Atherosclerotic CVD—the leading cause of morbidity and mortality in T2DM population—includes acute coronary syndrome, myocardial infarction (MI), angina, coronary or other arterial revascularization, stroke, transient ischemic attack, or peripheral arterial disease.2 CVD is the largest contributor to the direct and indirect costs of diabetes in the US healthcare system with an estimated $37.3 billion spending in cardiovascular-related complications associated with T2DM.3
Controlling blood pressure (BP) with antihypertensive pharmacotherapy is crucial in T2DM patients as it helps reduce risks of all-cause mortality, CVD events, heart failure, and microvascular complications.4–8 The American Diabetes Association (ADA) recommends angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) as one of the first-line drug classes for managing HTN in individuals with diabetes due to their beneficial effects in lowering CVD events.3
Medication adherence is defined as “the extent to which a patient’s behavior matches the agreed recommendations from a healthcare provider.”9 The link between BP control and adherence to antihypertensive drugs is well established.10–12 However, poor medication adherence continues to contribute to suboptimal BP control, hence resulting in increased risk for CVD, hospitalization, and cost burden, especially among older adults with multiple comorbid conditions.13–18 Proportion of days covered (PDC) is frequently used to measure medication adherence in the literature.19 It is also utilized by the Centers for Medicare and Medicaid Services (CMS) to measure adherence to ACEI/ARBs as it is one of the Five-Star measures in diabetic population. This Five-Star quality rating system is a program developed by CMS to evaluate beneficiaries’ experience with their health plan performance.20
Group-based trajectory modeling (GBTM) is increasingly applied in adherence studies using health insurance administrative claims data due to its advantages over PDC. Compared to PDC that categorizes patients as adherent versus nonadherent with a single value estimate, GBTM illustrates longitudinal patterns of medication adherence.21–23 Additionally, this method provides clusters of patients with similar medication-taking behavior over time, which could help in designing tailored adherence promotion interventions as these patients may share common characteristics and underlying barriers.21,24–26
Poor medication adherence is a multifactorial issue in HTN management. Medication costs, treatment regimen characteristics, disease conditions, patient–provider relationship, and psychosocial problems have been noted as important predictors of adherence.27 Understanding patients’ specific barriers to adherence to HTN pharmacotherapy is a necessary step in developing tailored interventions to improve adherence. Motivational interviewing (MoI) is an effective patient-centered intervention for improving adherence to chronic medications.26,28–30 This method helps patients with identifying barriers to adherence and exploring possible solutions through a supportive, collaborative, empathic and evocative conversation with a healthcare professional.31
This study aimed to assess and identify barriers to adherence to ACEI/ARB from an MoI telephonic intervention conducted by MoI-trained student pharmacist interns among T2DM patients enrolled in a Texas Medicare Advantage Plan (MAP).
Materials and Methods
Study Design and Participants
This study was conducted within a previous MoI intervention study, which was customized by past ACEI/ARB adherence patterns for nonadherent patients (aged ≥65 years) with comorbid T2DM and HTN enrolled in a MAP. Patients were excluded from this study if they had a diagnosis of dementia or had any contraindication for ACEI/ARB use.
The MoI intervention study was designed in two phases as described below.
Phase I: Identifying Adherence Trajectory Patterns
Through the initial phase, a retrospective claims database analysis from a MAP was performed to identify patients with similar medication filling behavior patterns for ACEI/ARB using GBTM. The four trajectories identified were adherent, rapid decline, gaps in adherence, and gradual decline (Figure 1). Patients were randomly selected for the MoI telephone intervention study if they presented any of the 3 lower adherence trajectories. Details of this study and trajectory modeling have been published elsewhere.32
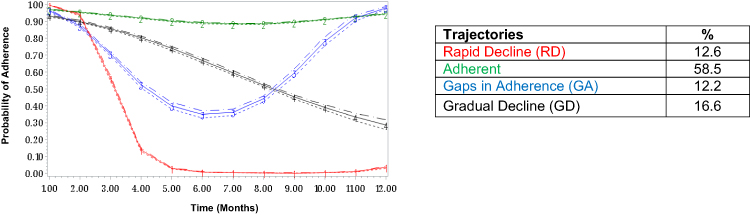 |
Figure 1 Baseline adherence trajectory groups. |
Phase II: MoI Telephone Intervention
This prospective study was designed to contact patients in low adherence trajectory groups with phone-based MoI intervention calls during which barriers to adherence to ACEI/ARB medications faced by the patient and potential solutions were identified and discussed in a collaborative manner. A total of 250 patients were reached out for the intervention group. The intervention consisted of an initial telephone call plus up to five follow-up calls conducted by fourth year pharmacy students participating in 6-week rotations at the health plan, who had training in MoI and data confidentiality. After each call, the interviewers documented notes from the conversation as well as the barriers discussed with the patient in an established Excel sheet. The interviewers could record more than one barrier for each patient within a single call. If patients denied having any barrier to ACEI/ARB adherence in a call, it was recorded as “denial of barrier.” Post-intervention adherence was measured at months 6 and 12 and compared to the control group to assess effectiveness of the MoI intervention. During the initial call, participants were asked for a verbal consent to participate in the study using a script in accordance with all IRB requirements. Patients were allowed to leave the study if they no longer wanted to participate. Patients in the control group received usual care, which includes receiving a telephone call from a pharmacy technician as a refill reminder.
Current Study: Retrospective Assessment of Adherence Barriers
Following the completion of Phase II of the MoI intervention study, the de-identified data and interviewers’ notes from the calls were provided to the authors of the current study. The two authors (Z.M. and A.M.) independently reviewed the notes and documented adherence barriers identified from each call. If a patient reported the same barrier in a subsequent call(s), it was not double counted to avoid inflation of the count of barriers. Evaluations of both reviewers were compared, and any discrepancies were resolved by discussing it with a third reviewer (S.A.). The barriers with similar themes were collapsed to provide fewer meaningful categories.
Statistical Analysis
Demographic and clinical characteristics of the patients including baseline adherence trajectory groups were summarized using mean (SD) or frequency (percentage). Descriptive analysis was performed to summarize the overall frequency of the first call barriers as well as across each trajectory groups. Additionally, barriers reported within the initial calls were compared with those identified throughout the follow-up calls to determine whether the follow-up conversation helped uncover new barriers. All statistical analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC).
Results
Patient Characteristics
A total of 247 patients successfully completed at least one call. Figure 2 describes the number of patients participated in the initial and follow-up calls. The baseline demographic and clinical characteristics of the participants are presented in Table 1. The mean (SD) age of the patients was 72.06 (9.28) years, and about 60% were female. Majority of the patients (89%) were prevalent users of ACEI/ARB medications (were prescribed ACEI/ARB medications prior to the study) and 49% were low-income subsidy beneficiaries.
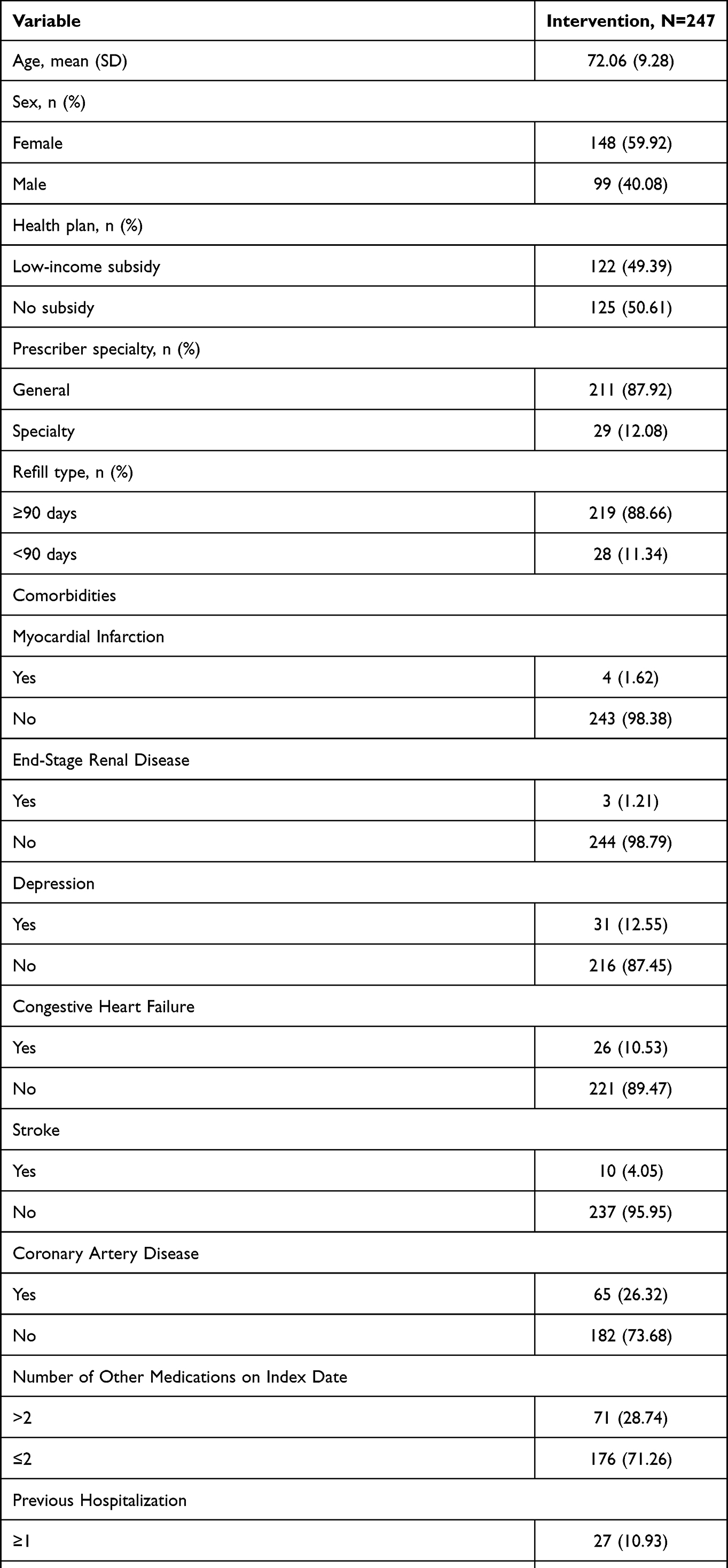 |
Table 1 Baseline Demographic of Patients Who Received the Intervention |
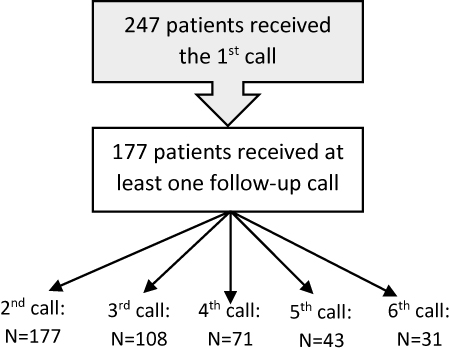 |
Figure 2 Motivational interviewing intervention flowchart. |
Initial Calls
After reviewing the notes from the initial calls made to 247 patients, 41% did not communicate any barrier for ACEI/ARB use despite having poor adherence. About 59% of the patients reported at least one barrier including forgetfulness (42.6%), discontinuation by physicians (12.9%), side effects (10.3%), multiple comorbidities/polypharmacy (8.4%), lack of knowledge about disease/medication (6.5%), cost issues (5.8%), and family issues (4.5%). In the rapid decline trajectory group, forgetfulness was the most frequent barrier (38.3%) followed by denial of barrier (36.2%), lack of knowledge about disease/medication (6.4%), and multiple comorbidities/polypharmacy (6.4%). In the gaps in adherence group, denial of barrier was mostly reported (42.5%), followed by forgetfulness (25.5%) and side effects (8.49%). Among patients with gradual decline in adherence, denial of barrier (38.5%), forgetfulness (20.2%) and discontinuation by physicians (13.5%) were the most prevalent barriers, respectively. The barriers with lower frequencies included multiple comorbidities/polypharmacy, lack of knowledge about disease/medication, cost issues, family issues/affected by a disaster, physician/pharmacy communication issue, transportation barrier, lack of organization or routine, and physician adjusted dose. Table 2 describes the barrier distributions across trajectories.
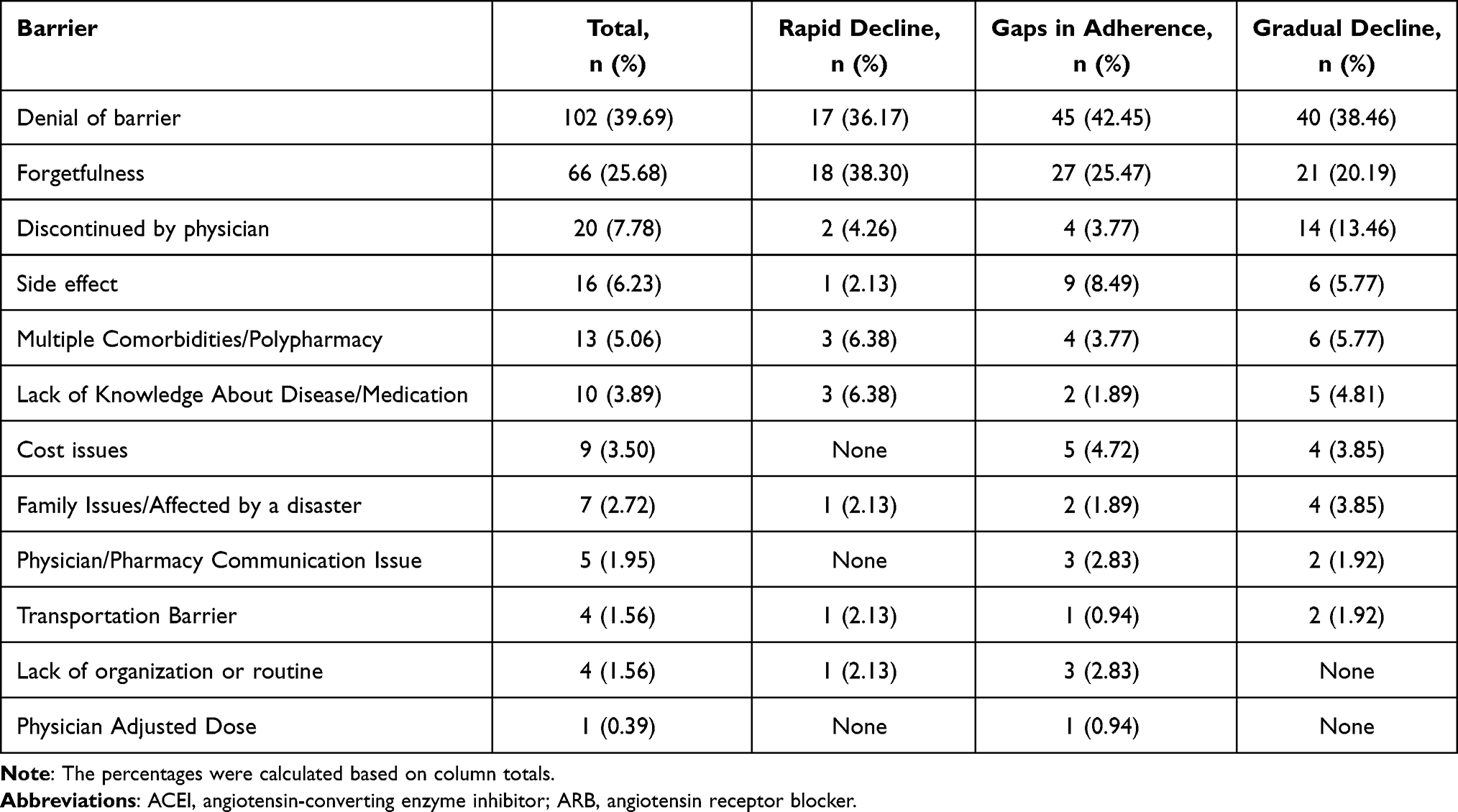 |
Table 2 Barriers to ACEI/ARB Adherence Identified from the Initial Call, in Total and Across Trajectories |
Follow-Up Calls
Throughout the follow-up calls, 28 patients expressed at least one new barrier, different from the barrier identified from the initial call. Moreover, 18 patients who denied having any barrier in the first call communicated at least one barrier from the second call (up to the sixth call). The new barriers identified from the follow-up calls are summarized in Table 3 and mostly included forgetfulness, lack of knowledge about disease/medication, and family issues/affected by a disaster.
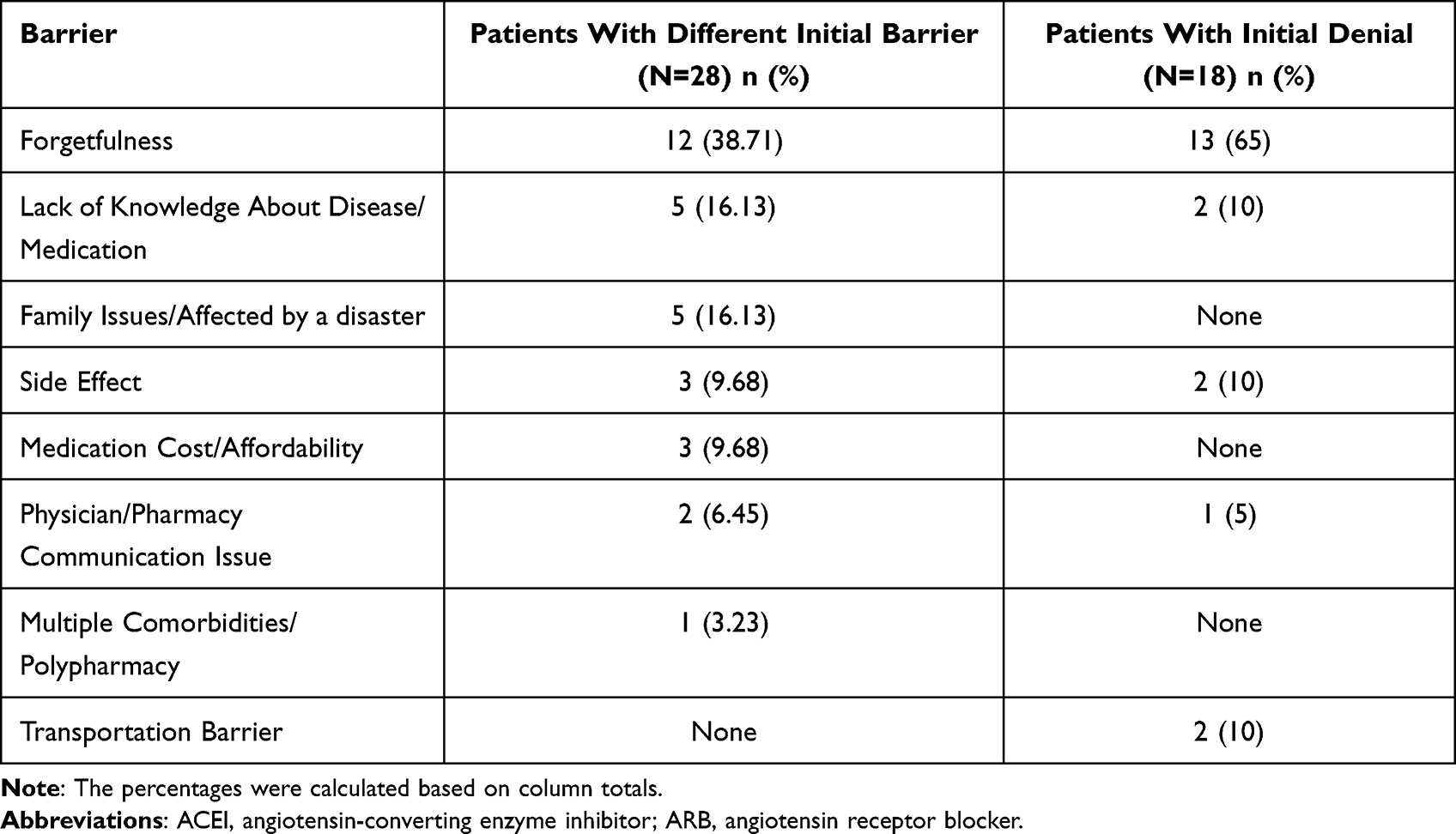 |
Table 3 New Barriers to ACEI/ARB Adherence Identified from the Follow-Up Calls |
Discussion
This retrospective study was nested within a previous MoI intervention project with the aim of identifying patient-specific barriers to ACEI/ARB adherence from the phone calls made by student pharmacist interns. Findings revealed that about 41% of the patients failed to report any barrier despite having low adherence to ACEI/ARBs. Furthermore, forgetfulness was the most frequent barrier in the study population. Studies have shown that HTN patients believe forgetfulness and unintentional skipping of doses are important reasons for their nonadherence, particularly in older adults.33–38 Also, a previously conducted study among Medicare Advantage Plan members taking statins, oral antidiabetics, ACEIs, and ARBs similarly found forgetfulness and denial as the most common patients’ barriers.39 Nonadherence has been classified as “intentional” vs “unintentional” in the literature.40 Although forgetfulness is considered an underlying cause for “unintentional” nonadherence, it may predict future “intentional” nonadherence as research showed forgetfulness could be a proxy for reduced motivation, low belief in the treatment and perceived need for the medication.40–44 Therefore, a patient-centered intervention such as MoI would be an effective method to assess patients’ beliefs about the medications and address potential reasons for both types of nonadherence.41 Potential solutions to help patients with forgetfulness include integration of medication-taking into daily routines, using pill boxes and organizers, and reminder phone calls from family, friends, or pharmacists.33,36
Another important finding from this study was that about 18% of the patients with initial denial for having any issue with their medication communicated at least one barrier and 20% uncovered a different new barrier during the follow-up calls. These results highlight the value of MoI-based interventions in improving adherence compared to traditional informative approaches, which only provide advice and education to patients above 65 years old with a chronic disease.45 In fact, one of the key characteristics of MoI interventions that contribute to unraveling medication adherence barriers is development of empathy and collaboration between patients and providers and creating a supportive conversation in which patients feel more engaged in the process of care and have higher intrinsic motivation towards change instead of feeling externally imposed.45 Furthermore, in line with previous studies, results from the current study support the notion that a greater number of patient encounters (ie, follow-up calls) during MoI could increase the probability of having an impactful intervention.45,46 Although almost all the initial calls were completed before the pandemic, a number of follow-up calls were made after the COVID-19 outbreak, which could have had an impact on the barriers and patients’ responses.
Despite differences in adherence patterns, similar barriers were reported among the different trajectory groups. Given the small sample size, this study was not powered enough to detect significant differences in barriers. However, patients with gaps in adherence trajectory reported side effect as a barrier to ACEI/ARB adherence more frequently than the other groups. Discussing common adverse effects of ACEI/ARBs and providing potential solutions and educating about serious events that need immediate discontinuation may address some of the concerns for such patients. During the intervention, patients were encouraged to discuss side effects with their physician and not stopping them on their own as switching to a different medication could solve the side effect for patients and prevent from treatment nonadherence.
Although we had less than 10% of the study population reporting physician’s discontinuation of therapy as the reason for nonadherence, majority of the cases fell within the gradual decline group. Physician recommended discontinuation should not be considered as nonadherence as the patient is following doctor’s order. However, in this study, we were unable to verify if the medication was actually discontinued by the physician. Future work should examine the link between what patient says and the physician order.
Although about half of the patients had low socioeconomic status in this study, cost issue was not prevalent (less than 5%). In this Medicare Advantage Plan, patients with limited income and resources were eligible for receiving assistance to help them with prescription drug costs, which may have explained why cost issues were not a concern for adherence in this patient population. Other barriers found in this study were in line with previous findings.28,37–39,47–49
Limitations
Findings of the current study should be interpreted in light of several limitations. First, this study used a small sample of patients from a MAP, which limits the generalizability of the barriers to other health insurance plans across different regions. Also, the limited sample size did not allow statistical comparisons for the barriers across trajectory groups or the number of intervention calls. Second, although the student pharmacist interns were trained to record any barrier identified from the calls, they may have been biased towards reporting only barriers from a list created by the investigators before the intervention based on the literature. Third, the role of caregivers in assisting patients with their medications and addressing barriers was not assessed in this study. Future studies can explore and identify adherence barriers from caregivers of older adults and evaluate the effect of interventions solely targeted at caregivers.
Conclusion
This study identified patient-reported barriers to ACEI/ARB adherence among high-risk patients ≥65 years old from an MoI telephonic intervention conducted by student pharmacist interns. Using MoI interventions with multiple patient encounters may help with uncovering patient-specific barriers and developing a more individualized approach, even in nonadherent patients with initial denial for having any issues with their medication. Educating patients on different ways to overcome forgetfulness as the main barrier reported among older adult population is of high importance.
IRB Approval
The study was approved by the institutional review board at the University of Houston and is compliant with the Declaration of Helsinki. Participants receiving the intervention consented to participation using a script in accordance with all NIH human subject ethical guidelines and the University of Houston IRB requirements for recruitment and informed consent.
Funding
This study was funded by the National Heart, Lung, and Blood Institute (NHLBI) (grant numbers: 1R15HL135700-01A1).
Disclosure
Dr. Abughosh reports grants from NIH, during the conduct of the study and grants from CARsgen and Valeant Pharmaceuticals, outside the submitted work. Dr. Barner reports grants from NIH and personal fees from University of Houston, during the conduct of the study and grants from Centers for Disease Control, Texas Health and Human Services, and Pharmaceutical Research Manufacturers of America Foundation, outside the submitted work. Dr. Fleming reports grants from National Heart, Lung, and Blood Institute and National Institute on Minority Health and Health Disparities (U-54). Dr. Fleming also reports contracts from Texas Health and Human Services Commission and CoI funding on a grant from Texas Council for Developmental Disabilities, outside the submitted work. Dr. Gallardo is an employee of CareAllies, a subsidiary of Cigna, outside of the submitted work. The authors report no other potential conflicts of interest for this work.
References
1. Rana J, Oldroyd J, Islam MM, Tarazona-Meza CE, Islam R. Prevalence of hypertension and controlled hypertension among United States adults: evidence from NHANES 2017–18 survey. Int J Cardiol Hypertens. 2020;7:100061. doi:10.1016/j.ijchy.2020.100061
2. De Boer IH, Bangalore S, Benetos A, et al. Diabetes and hypertension: a position statement by the American Diabetes Association. Diabetes Care. 2017;40(9):1273–1284. doi:10.2337/dci17-0026
3. Care ADAJD. 10. Cardiovascular disease and risk management: standards of medical care in diabetes—2021. Diabetes Care. 2021;44:S125–S150.
4. Emdin CA, Rahimi K, Neal B, Callender T, Perkovic V, Patel AJJ. Blood pressure lowering in type 2 diabetes: a systematic review and meta-analysis. JAMA. 2015;313(6):603–615. doi:10.1001/jama.2014.18574
5. Ettehad D, Emdin CA, Kiran A, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387(10022):957–967. doi:10.1016/S0140-6736(15)01225-8
6. Brunström M, Carlberg B. Effect of antihypertensive treatment at different blood pressure levels in patients with diabetes mellitus: systematic review and meta-analyses. BMJ. 2016;352. doi:10.1136/bmj.i717
7. Bangalore S, Kumar S, Lobach I, Messerli FHJC. Blood pressure targets in subjects with type 2 diabetes mellitus/impaired fasting glucose: observations from traditional and Bayesian random-effects meta-analyses of randomized trials. Circulation. 2011;123(24):2799–2810. doi:10.1161/CIRCULATIONAHA.110.016337
8. Thomopoulos C, Parati G, Zanchetti A. Effects of blood-pressure-lowering treatment on outcome incidence in hypertension: 10–should blood pressure management differ in hypertensive patients with and without diabetes mellitus? Overview and meta-analyses of randomized trials. J Hypertens. 2017;35(5):922–944. doi:10.1097/HJH.0000000000001276
9. Sabaté E, Sabaté E. Adherence to Long-Term Therapies: Evidence for Action. World Health Organization; 2003.
10. Ho PM, Magid DJ, Shetterly SM, et al. Importance of therapy intensification and medication nonadherence for blood pressure control in patients with coronary disease. Arch Intern Med. 2008;168(3):271–276. doi:10.1001/archinternmed.2007.72
11. Stewart K, George J, Mc Namara K, et al. A multifaceted pharmacist intervention to improve antihypertensive adherence: a cluster-randomized, controlled trial (HAPPy trial). J Clin Pharm Ther. 2014;39(5):527–534. doi:10.1111/jcpt.12185
12. Moultry AM, Pounds K, Poon IOJTCP. Managing medication adherence in elderly hypertensive patients through pharmacist home visits. Consult Pharm. 2015;30(12):710–719. doi:10.4140/TCP.n.2015.710
13. McLean DL, Simpson SH, McAlister FA, Tsuyuki R. Treatment and blood pressure control in 47,964 people with diabetes and hypertension: a systematic review of observational studies. Can J Cardiol. 2006;22(10):855–860. doi:10.1016/S0828-282X(06)70304-X
14. Natarajan N, Putnam W, Van Aarsen K, Lawson KB, Burge F. Adherence to antihypertensive medications among family practice patients with diabetes mellitus and hypertension. Can Fam Physician. 2013;59(2):e93–e100.
15. Grant RW, Devita NG, Singer DE, Meigs J. Polypharmacy and medication adherence in patients with type 2 diabetes. Can Fam Physician. 2003;26(5):1408–1412.
16. Ho PM, Rumsfeld JS, Masoudi FA, et al. Effect of medication nonadherence on hospitalization and mortality among patients with diabetes mellitus. Arch Intern Med. 2006;166(17):1836–1841. doi:10.1001/archinte.166.17.1836
17. Brown LC, Johnson JA, Majumdar SR, Tsuyuki RT, McAlister FAJC. Evidence of suboptimal management of cardiovascular risk in patients with type 2 diabetes mellitus and symptomatic atherosclerosis. Cmaj. 2004;171(10):1189–1192. doi:10.1503/cmaj.1031965
18. Yang Q, Chang A, Ritchey MD, Loustalot F. Antihypertensive medication adherence and risk of cardiovascular disease among older adults: a population-based cohort study. J Am Heart Assoc. 2017;6(6):e006056. doi:10.1161/JAHA.117.006056
19. Peterson AM, Nau DP, Cramer JA, Benner J, Gwadry-Sridhar F, Nichol M. A checklist for medication compliance and persistence studies using retrospective databases. Value Health. 2007;10(1):3–12. doi:10.1111/j.1524-4733.2006.00139.x
20. Owen J. Medicare star ratings: stakeholder proceedings on community pharmacy and managed care partnerships in quality: American Pharmacists Association and Academy of Managed Care Pharmacy. J Am Pharm Assoc. 2014;54(3):228–240. doi:10.1331/JAPhA.2014.13180
21. Vadhariya A, Fleming ML, Johnson ML, et al. Group-based trajectory models to identify sociodemographic and clinical predictors of adherence patterns to statin therapy among older adults. Am Health Drug Benefits. 2019;12(4):202.
22. Franklin JM, Shrank WH, Pakes J, et al. Group-based trajectory models: a new approach to classifying and predicting long-term medication adherence. Med Care. 2013;51:789–796. doi:10.1097/MLR.0b013e3182984c1f
23. Nagin DS, Odgers CL. Group-based trajectory modeling in clinical research. Annu Rev Clin Psychol. 2010;6:109–138. doi:10.1146/annurev.clinpsy.121208.131413
24. Franklin JM, Krumme AA, Shrank WH, Matlin OS, Brennan TA, Choudhry NK. Predicting adherence trajectory using initial patterns of medication filling. Am J Manag Care. 2015;21(9):e537–e544.
25. Lo-Ciganic W-H, Donohue JM, Jones BL, et al. Trajectories of diabetes medication adherence and hospitalization risk: a retrospective cohort study in a large state Medicaid program. J Gen Intern Med. 2016;31(9):1052–1060. doi:10.1007/s11606-016-3747-6
26. Abughosh SM, Vadhariya A, Johnson ML, et al. Enhancing statin adherence using a motivational interviewing intervention and past adherence trajectories in patients with suboptimal adherence. J Manag Care Spec Pharm. 2019;25(10):1053–1062. doi:10.18553/jmcp.2019.25.10.1053
27. Unni EJ, KBJPe F. Unintentional non-adherence and belief in medicines in older adults. Patient Educ Couns. 2011;83(2):265–268. doi:10.1016/j.pec.2010.05.006
28. Abughosh S, Wang X, Serna O, et al. A motivational interviewing intervention by pharmacy students to improve medication adherence. J Manag Care Spec Pharm. 2017;23(5):549–560. doi:10.18553/jmcp.2017.23.5.549
29. DiIorio C, McCarty F, Resnicow K, et al. Using motivational interviewing to promote adherence to antiretroviral medications: a randomized controlled study. AIDS Care. 2008;20(3):273–283. doi:10.1080/09540120701593489
30. Ogedegbe G, Chaplin W, Schoenthaler A, et al. A practice-based trial of motivational interviewing and adherence in hypertensive African Americans. Am J Hypertens. 2008;21(10):1137–1143. doi:10.1038/ajh.2008.240
31. Turner AP, Sloan AP, Kivlahan DR, Haselkorn J. Telephone counseling and home telehealth monitoring to improve medication adherence: results of a pilot trial among individuals with multiple sclerosis. Rehabil Psychol. 2014;59(2):136. doi:10.1037/a0036322
32. Paranjpe R, Johnson ML, Essien EJ, et al. Group-based trajectory modeling to identify patterns of adherence and its predictors among older adults on Angiotensin-Converting Enzyme Inhibitors (ACEIs)/Angiotensin Receptor Blockers (ARBs). Patient Prefer Adherence. 2020;14:1935. doi:10.2147/PPA.S270809
33. Holt EW, Rung AL, Leon KA, Firestein C, Krousel-Wood M. Medication adherence in older adults: a qualitative study. Educ Gerontol. 2014;40(3):198–211. doi:10.1080/03601277.2013.802186
34. Ogedegbe G, Harrison M, Robbins L, Mancuso CA, Allegrante JPJE. Barriers and facilitators of medication adherence in hypertensive African Americans: a qualitative study. Ethn Dis. 2004;14(1):3–12.
35. Tsiantou V, Pantzou P, Pavi E, Koulierakis G, Kyriopoulos J. Factors affecting adherence to antihypertensive medication in Greece: results from a qualitative study. Patient Prefer Adherence. 2010;4:335. doi:10.2147/PPA.S12326
36. Abughosh SM, Wang X, Serna O, et al. A pharmacist telephone intervention to identify adherence barriers and improve adherence among nonadherent patients with comorbid hypertension and diabetes in a medicare advantage plan. J Manag Care Spec Pharm. 2016;22(1):63–73. doi:10.18553/jmcp.2016.22.1.63
37. Krousel-Wood MA, Muntner P, Islam T, Morisky DE, Webber L. Barriers to and determinants of medication adherence in hypertension management: perspective of the cohort study of medication adherence among older adults. Med Clin N Am. 2009;93(3):753–769. doi:10.1016/j.mcna.2009.02.007
38. Okwuonu CG, Ojimadu NE, Okaka EI, Akemokwe F. Patient-related barriers to hypertension control in a Nigerian population. Int J Gen Med. 2014;7(345):345–353. doi:10.2147/IJGM.S63587
39. Daly CJ, Verrall K, Jacobs D. Impact of community pharmacist interventions with managed care to improve medication adherence. J Pharm Pract. 2019;34:0897190019896505.
40. Clifford S, Barber N, Horne R. Understanding different beliefs held by adherers, unintentional nonadherers, and intentional nonadherers: application of the necessity–concerns framework. J Psychosom Res. 2008;64(1):41–46. doi:10.1016/j.jpsychores.2007.05.004
41. Gadkari AS, McHorney CAJBHSR. Unintentional non-adherence to chronic prescription medications: how unintentional is it really? BMC Health Serv Res. 2012;12(1):1–12. doi:10.1186/1472-6963-12-98
42. Kim E, Gupta S, Bolge S, Chen -C-C, Whitehead R, Bates J. Adherence and outcomes associated with copayment burden in schizophrenia: a cross-sectional survey. J Med Econ. 2010;13(2):185–192. doi:10.3111/13696991003723023
43. Proulx M, Leduc N, Vandelac L, Grégoire J-P, Collin JJPE. Social context, the struggle with uncertainty, and subjective risk as meaning-rich constructs for explaining HBP noncompliance. Patient Educ Couns. 2007;68(1):98–106. doi:10.1016/j.pec.2007.05.014
44. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–567. doi:10.1016/S0022-3999(99)00057-4
45. Moral RR, de Torres LAP, Ortega LP, et al. Effectiveness of motivational interviewing to improve therapeutic adherence in patients over 65 years old with chronic diseases: a cluster randomized clinical trial in primary care. Patient Educ Couns. 2015;98(8):977–983. doi:10.1016/j.pec.2015.03.008
46. Ekong G, Kavookjian J. Motivational interviewing and outcomes in adults with type 2 diabetes: a systematic review. Patient Educ Couns. 2016;99(6):944–952. doi:10.1016/j.pec.2015.11.022
47. Odegard PS, Gray S. Barriers to medication adherence in poorly controlled diabetes mellitus. Diabetes Educ. 2008;34(4):692–697. doi:10.1177/0145721708320558
48. Bailey GR, Barner JC, Weems JK, et al. Assessing barriers to medication adherence in underserved patients with diabetes in Texas. Diabetes Educ. 2012;38(2):271–279. doi:10.1177/0145721711436134
49. Yap AF, Thirumoorthy T, Kwan YHJG. Systematic review of the barriers affecting medication adherence in older adults. Geriatr Gerontol Int. 2016;16(10):1093–1101. doi:10.1111/ggi.12616
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.