")
Back to Journals » Patient Preference and Adherence » Volume 16
Factors Influencing Treatment Adherence Among Drug-Sensitive Tuberculosis (DS-TB) Patients in Armenia: A Qualitative Study
Authors Grigoryan Z , McPherson R, Harutyunyan T, Truzyan N, Sahakyan S
Received 29 April 2022
Accepted for publication 11 August 2022
Published 1 September 2022 Volume 2022:16 Pages 2399—2408
DOI https://doi.org/10.2147/PPA.S370520
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Zaruhi Grigoryan, Robert McPherson, Tsovinar Harutyunyan, Nune Truzyan, Serine Sahakyan
Turpanjian College of Health Sciences, American University of Armenia, Yerevan, Armenia
Correspondence: Zaruhi Grigoryan, Turpanjian College of Health Sciences, American University of Armenia, 40 Marshal Baghramyan Ave, Yerevan, 0019, Armenia, Tel +37 460612617, Fax +37 460612512, Email [email protected]
Purpose: Despite the availability of effective treatment, tuberculosis (TB) is still one of the leading causes of mortality around the globe. Poor adherence to treatment challenges TB management both globally and locally. Proper adherence to treatment contributes to successful outcomes and prevents the development of drug-resistant forms of TB.
Patients and Methods: We conducted a qualitative study to identify and describe the factors that facilitated treatment adherence among drug-sensitive TB (DS-TB) patients in Armenia. Sixteen in-depth interviews (IDIs) with former DS-TB patients, two IDIs with family members of former DS-TB patients, and a focus group discussion with healthcare providers who manage DS-TB patients were conducted. The educational and ecological assessment component of the PRECEDE-PROCEED model was applied as a conceptual framework to guide the interview content and data analysis.
Results: Former patients’ awareness of TB and its treatment, beliefs about TB, trust in TB healthcare providers, and a sense of responsibility were the most common factors that predisposed them to complete the treatment. Support received from providers, family, and friends, a desire to avoid TB-associated stigma, and good tolerance of TB medications were the main reinforcing factors. Enabling factors included a relatively simple regimen of TB treatment and accessibility and affordability of TB services.
Conclusion: The findings of the study provide new perspectives on factors that facilitate adherence to long-term therapies, such as TB. Interventions that aim to invoke a patient’s sense of responsibility and positive beliefs about TB as well as engage families might promote the successful completion of treatment.
Keywords: treatment completion, PRECEDE-PROCEED, facilitators of TB treatment, people-centered TB care
Introduction
Tuberculosis (TB) is one of the leading causes of mortality around the globe, accounting for 1.5 million deaths worldwide in 2020 alone.1 In Armenia, the estimated TB incidence rate in 2018 was 31 per 100,000 population, of which 20% were drug-resistant, including multidrug- and rifampicin-resistant TB (MDR/RR-TB).2 Furthermore, 44% of previously treated TB cases had MDR/RR-TB. There have also been cases of extensively drug-resistant TB (XDR-TB) in the country with 10 recorded in 2016. The mortality rate from TB in Armenia in 2018 was 1.3 per 100,000 population.2
Despite the availability of effective treatment, poor treatment adherence is still one of the major factors that impedes global efforts in combating the TB epidemic.3,4 The World Health Organization (WHO) defines adherence to TB treatment as “the extent to which patient’s history of therapeutic drug-taking coincides with prescribed treatment”.5 It is estimated that the desired adherence rate to facilitate TB control should exceed 90%.6 Non-adherence to TB treatment threatens TB control by leading to treatment failure and relapse, which in the long run can contribute to increased TB morbidity and mortality, increased duration of TB transmission, and development of drug-resistant TB (DR-TB).7,8
A major response to combat poor TB treatment adherence is the supervised administration of medicine through directly observed treatment short-course (DOT).3 The WHO recommends three types of DOT for drug-sensitive TB (DS-TB) patients based on method of administration: community- or home-based, healthcare facility based, or video-observed.9 It is estimated that, due to DOT, the Stop TB program saved up to 37 million lives between 2000 and 2013.10 Community-level interventions that aim to address social and economic factors of non-adherence have also shown promising results on improving treatment success and decreasing loss to follow-up.11
The introduction and nationwide coverage of TB diagnostic and treatment services utilizing DOT in Armenia, in 1990 and 2002 respectively, was an impactful step in TB management in the country and led to a decline in TB burden between 2004 and 2018.2,12 TB incidence and mortality rates declined by 2.3 and by 3.2 times, respectively, between 2005–2018.2,13 Until 2019, TB treatment in Armenia was organized mainly through healthcare facility-based DOT supervised by nurses or physicians.14 Currently, Armenia is moving towards the institutionalization of people-centered TB care and a shift from facility-based DOT to family-based DOT supervised by supportive family members. The effectiveness of this approach was demonstrated in a cluster randomized trial and is envisioned to support treatment adherence.15
Despite positive trends in TB management, 24.7% of patients were lost to follow-up in Armenia between 2005 and 2011.16 According to a study conducted in 2015 in Armenia, in the cohort of 2013–2014 TB patients, unsuccessful TB treatment outcomes included 2.4% failure to adhere, 6.0% death and 9.5% lost to follow-up.17 Non-adherence to TB treatment, and the emergence and high prevalence of DR-TB are a major concern for TB management in Armenia.18
Patients with DS-TB are susceptible to first-line TB medications and receive the shortest standard 6-month course of four antimicrobial agents.20 Armenia follows the fourth WHO treatment guideline for national TB programs.19 All DS-TB patients receive two months of intensive TB treatment with isoniazid (H), rifampin (R), pyrazinamide (Z), and ethambutol (E) (HRZE) in the TB inpatient care facility, followed by four months of DOT at a TB outpatient center with HR.21
In order to better understand treatment adherence among TB patients in Armenia, we aimed to identify and describe the determinants of adherent behavior that contribute to successful completion of TB treatment among former DS-TB patients. The identified factors, once addressed by TB treatment services, could support TB treatment in Armenia and help to avert treatment interruption and further progression into DR-TB.
Materials and Methods
This explorative qualitative study with deductive content analysis was conducted in outpatient TB facilities in Yerevan (the capital of Armenia), where the largest share of Armenian patients receives TB treatment during the continuation phase.
The educational and ecological assessment component of the PRECEDE-PROCEED model was used to explore participants’ adherence behavior through the trajectory of predisposing, reinforcing, and enabling factors.22 According to the model, predisposing factors (knowledge, attitude, beliefs, and values) rationalize and motivate the behavior. The environmental factors such as availability, accessibility, and affordability of services that facilitate particular behavior are categorized as enabling factors. Reinforcing factors include social support, feedback from health-care providers, and peer influence that reward a particular behavior and result in its repetition.22
The study protocol was approved by the Institutional Review Board (IRB) of the American University of Armenia (AUA-2015-003). The IRB made sure that all procedures of the study met the local and Declaration of Helsinki standards. Informed consent was obtained from all participants prior to the start of the interviews. The participants were notified that any publication based on the findings will include aggregated findings and anonymized quotes.
Study Population and Sampling
The study population included adult (18 years and older) Armenian former pulmonary DS-TB patients who both adhered to and successfully completed anti-tuberculosis treatment in 2012–2014 (hereinafter referred to as “former patients”). Thus, eligible participants either had cured or completed treatment outcomes. We targeted former DS-TB patients to detect the influence of factors that determined treatment adherence with a relatively shorter TB treatment regimen. We also recruited TB physicians from outpatient TB facilities as well as family members of former DS-TB patients to gain additional insights into DS-TB patients’ experiences. To increase variability in responses, we recruited former patients of different genders, ages, occupations, and educational status. Wide geographic coverage was achieved through purposive selection of participants from seven outpatient TB facilities located in different districts of Yerevan. Former patients and family members were first contacted by their nurses or physicians to gain permission for subsequent contact by the research team.
Study Instruments
The semi-structured interview guide for former TB patients (Appendix 1) was developed based on factors suggested by the literature. We categorized all determinants of treatment adherence suggested by the literature into predisposing, reinforcing, and enabling factors and incorporated them into the guide. The final guide included general introductory questions as well as questions to understand participants’ knowledge and beliefs about TB and its medications, their experience with social support, their understanding of the treatment regimen and side effects, and the accessibility and affordability of treatment. After the preliminary analysis of the initial findings from the interviews with former patients, two additional semi-structured guides were developed for TB physicians and family members.
Data Collection
Data collection took place in April 2015. Overall, 21 people participated in 16 in-depth interviews (IDI) with former patients, two IDIs with family members, and a focus group discussion (FGD) with three TB physicians. We concluded data collection upon achieving saturation of responses. The duration of the IDIs varied from 20 to 60 minutes. Interviews were tape-recorded and transcribed verbatim. In cases where participants refused to have the interview be recorded, only notes were taken. The participants’ demographic characteristics are described in Table 1.
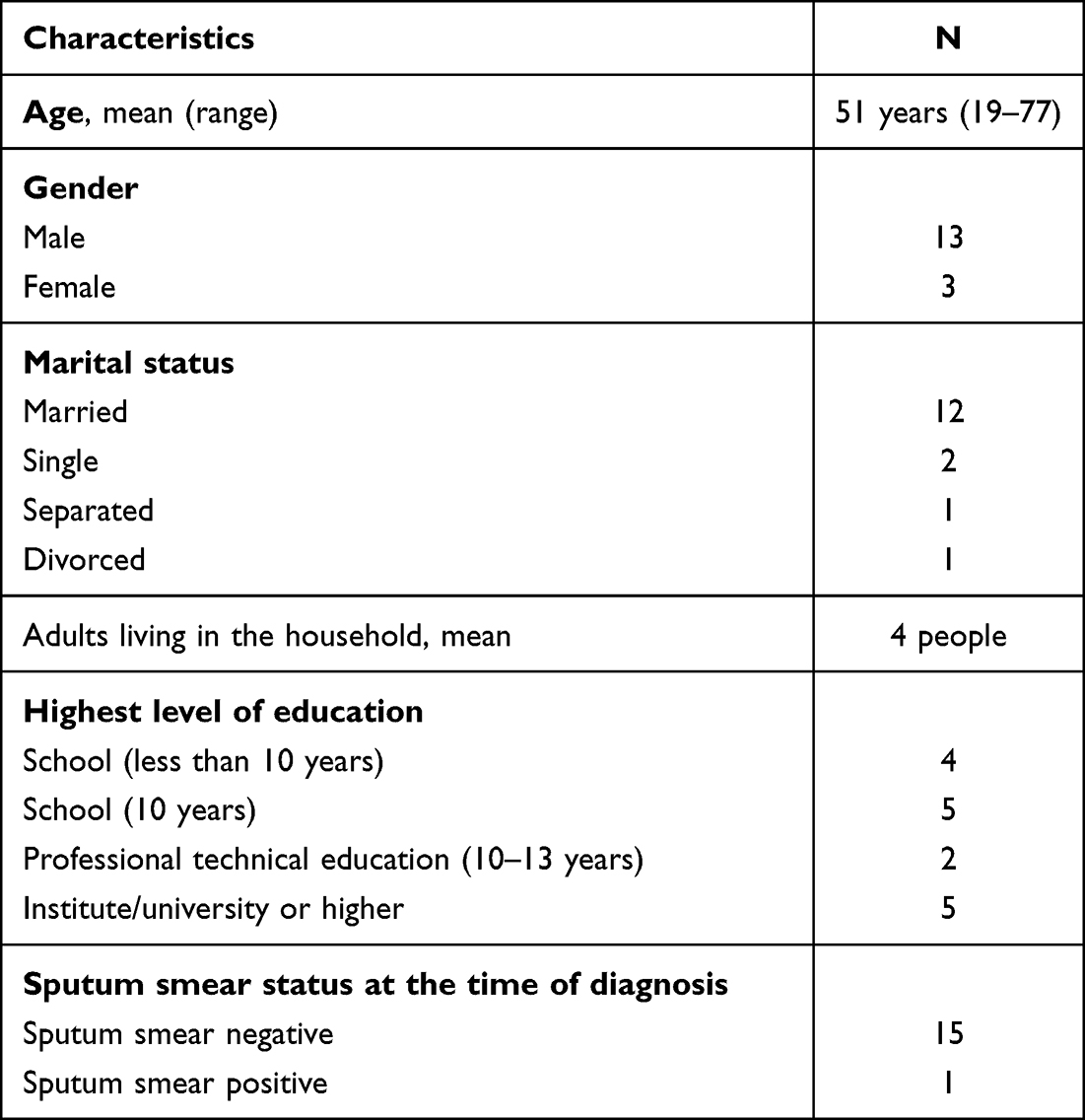 |
Table 1 Demographic Characteristics of Former Pulmonary DS-TB Patients |
Data Analysis
Direct deductive content analysis was used to analyze the textual data.23 Derived facilitators of TB treatment adherence were thematically analyzed and then grouped into categories.
Study Rigor
To achieve increased generalizability and credibility of the results, former patients with different demographic characteristics were selected. To exclude the influence of a single institution and its healthcare providers, patients from almost all outpatient TB facilities in the capital city were recruited into the study. To ensure credibility of the results, factors facilitating treatment adherence explored by this study were reviewed and compared with the international literature. Triangulation between the three groups of respondents increased the reliability of the results.
Results
Predisposing Factors
Awareness of TB and Its Treatment
Although most of the interviewees said that they were satisfied with the level of knowledge they had about TB and its medications, some of their responses indicated poor awareness about TB even at a basic level. In particular, most of them were not aware of the exact route of TB transmission and its risk factors.
Maybe TB can be transmitted through blood. I don’t think that merely communicating with a person with TB can lead to getting infected. P8, 43, y/o male
It is necessary to separate the plate, spoon, towel [of a person with TB] in order not to infect others. I know this much. P5, 68 y/o male
Most of the respondents did not know much about TB medication, including the type of medicine they were taking, the names of drugs, or their specific purpose. However, inadequate knowledge about TB medication did not hinder good adherence. Moreover, some stated that they had no desire to know anything about their medications.
Frankly speaking, I do not remember the names of the drugs; I don’t even want to. I was told to take them [drugs] and I took them as prescribed. P8, 43y/o male
I do not know anything about anti-tuberculosis medication. Anyway, I have taken them and now I am good. P13, 56 y/o male
Despite poor knowledge about medications, the overwhelming majority of former patients agreed that medications have played an important role in their recovery.
If taking medications was meaningless, I would not use them. I mean that medications were helpful. P3, 30 y/o male.
Beliefs About TB
Despite poor knowledge about the disease, the majority of participants stated that untreated TB could lead to irreversible consequences, including death, and admitted they feared the disease. Participants said that TB is a serious disease and they did everything to overcome it. Their belief in the severity of TB and in its treatability was a strong facilitator of treatment adherence.
If untreated, TB means death, slow death. One should receive the treatment in order to be cured. P8 43, y/o male.
If one is not taking medicines, at most after five-six months he will not be able to resist (the disease) P2, 61 y/o male
You will die if you don’t treat TB. Any untreated disease will weaken and ruin your body P5, 68 y/o male
Trust in TB Healthcare Providers
Patients’ trust in their TB physicians’ advice was seen as a strong determinant of their adherence to treatment. Belief in physicians’ professional expertise helped patients to value and follow their recommendations. Physicians likewise stated that patients’ trust has a significant role in successful treatment and further elaborated that they also act as “psychologists” building trust with TB patients and continuously encouraging them to adhere to treatment.
When a person believes in his/her physician, then s/he does whatever the physician tells him or her to do. P6, 57y/o female
We have many roles: psychologists, psychiatrists, physicians, therapists, and friends. Patients need that empathy. Physician 3
Interestingly, a few of the former patients mentioned that they were afraid of not obeying their physicians, as the physicians would not tolerate non-adherence. This factor appeared to facilitate adherence to treatment for certain participants with some physicians explaining that this fear is more typical among younger patients.
I was afraid of the doctor, dear. It was not possible to be non-adherent. I needed to accept doctor’s recommendations like “melted butter”. P5, 68 y/o male
My physician would not like it if a patient did not go and take the medicines for a week. P12, 19 y/o male
Mostly young patients are afraid of physicians- maybe [sometimes] we ask heatedly why he/she did not come for [taking] the medicine. But it passes. We treat them like our relatives. Physician 1
Sense of Responsibility
The most commonly mentioned factor that seemed to stimulate former TB patients to adhere to treatment was their sense of responsibility and willpower. Almost all patients emphasized being cognizant of their health condition and doing every possible thing to overcome TB and ultimately become a “healthy” person.
Generally, I am persistent and consider everything very conscientiously. I never follow my emotions. If it is necessary, then it is necessary. My understanding is that the treatment is necessary and that if you want to become a healthy person and overcome the situation you should pass through all of this. [long treatment]. P6, 57 y/o female
You know what, if one wants to be healed he should be conscientious, if he is foolish then he won’t complete the treatment. Fortunately, I was conscientious and I did what was recommended by physicians. P10, 49 y/o male
This finding was confirmed by TB physicians who mentioned that a sense of responsibility is very important and added that patients’ understanding of the importance of treatment depends on their intellectual level. They further elaborated that an important part of their work is to influence the level of patients’ understanding and awaken their sense of responsibility to promote treatment adherence.
We try to raise everybody [TB patients] to the same level of understanding. Sometimes we succeed and sometimes we fail … We try to change the way they think. Physician 3
Some TB patients mentioned that it was their social responsibility to treat TB, otherwise they would infect surrounding people.
I felt responsible for my big family. I could not let the infection enter my home and harm my children. P6, 57 y/o female
Reinforcing Factors
Support Received from TB Healthcare Providers and Family
Patients shared their experiences of communicating with other people during treatment and stressed social support from family, friends, and healthcare providers as an important facilitator of treatment adherence. According to them, the continuous support from healthcare providers was important throughout the treatment process and they particularly valued the empathy demonstrated by physicians when they informed patients about their TB diagnosis. Healthcare providers were characterized as responsive and caring personalities. Furthermore, physicians’ explanations about the disease and the emphasis they put on the importance of treatment gave the patients the power to fight the disease.
He [the physician] did not tell me the diagnosis right away. I felt that he was trying to say it in a way that would show he was also caring for me and for what has happened to me. That is why I accepted the disease and believed that TB is treatable. P7, 45 y/o male
Healthcare providers were influential with their … words that, if not treated, TB will lead to complications. They [healthcare providers] did not force me, rather they gave valuable recommendations to treat the disease. P12, 19 y/o male
Family members also emphasized the vital role that healthcare providers played in TB patients’ ability to cope with the disease and adhere to treatment.
Medical personnel s support was very important, cheering him up, giving hope. They were careful, supportive. The doctor was very tolerant and diligent. They were giving hope and power. They were so confident when replying to questions. Physicians and nurses are very important for patients not to get disappointed, to be sure that they will be cured. Family member 2
Support provided by family members and others, such as reminders to take medications and provision of moral and financial support, was also noted as an important facilitator of adherence.
I did not lose my hope because there were people next to me. Even if something happens there are people who stand by my family. It gave hope. P7, 45 y/o male
My wife and mother assisted me. They were giving me food on time, paying attention, cheering me up. If there was no such support, then the treatment would not be as good. P10, 49 y/o male
Family members felt responsible for the treatment outcomes of their relatives. They stated that love, respect and a positive attitude were factors that helped them to stand by the patient throughout the course of the disease.
My love for him helped me to cope with the disease. When I was alone, I was feeling very bad, did not know what to do but when we were together, I was pulling myself together, getting serious. And I think he was expecting me to be strong because if I was weak, he would despair. That strong support is important. We did not let anything pass through our fingers. Our power, our love, respect, and positive attitude helped. Family member 2
From the patients’ point of view, the prospect of continuing to receive respect from their family members and appreciation of their role in the family were strong facilitating factors. For example, some patients mentioned that they wanted to be cured in order to keep their leading role in their family.
In my family, my word is a law, my presence is their happiness. My sons and wife do not want my death. They wanted to help me in order for me to continue heading the family. P5, 68 y/o male
TB-Associated Stigma
Some of the former patients stated that they avoided disclosing their condition to other people during treatment because they were afraid it could affect their personal relationships. A number of patients felt so strongly stigmatized by having TB that it pushed them to do everything they could to become cured.
I tried to talk about the disease with those people who would not tell others about it. I did it to avoid drawing negative attention to myself. I tried to speak to those people who would not make the disease a reason for not offering a job or restricting me from entering their homes. P7, 45 y/o male
You know, even contacts with TB physicians are not accepted by people. People know that historically TB has been a very bad disease. We would rather say that we have appendicitis or ulcer but not TB. This disease is shameful; it is better to get rid of it as soon as possible. P5, 68 y/o male
Some of the participants mentioned that being diagnosed with TB was even worse than having cancer.
When I learned about TB I thought I d rather have cancer. P10, 49 y/o male
Tolerance of TB Medications
The majority of respondents stated that they did not have major side effects from their TB treatment. However, some respondents who experienced slight side effects knew how to cope with them by taking medications after a meal as prescribed.
I did not have side effects. I checked my liver because it is the first target of drugs, but it was ok P4, 69 y/o male
In the beginning, I had side effects because I was taking several medicines on an empty stomach. P3, 30 y/o male
If I took drugs when hungry I had some side effects. Knowing preventive measures, I tried not to have such problems. P12, 19 y/o male
Enabling Factors
Treatment Regimen
For the majority of respondents, the treatment regimen did not create any obstacles for adherence. Taking medications over a long period was challenging but understanding that TB treatment could not be delayed helped patients overcome any unpleasant feelings and complete the treatment.
Nothing disturbed me in particular, I just took capsules and received the injections. P4, 69 y/o male
Accessibility and Affordability of TB Treatment Services
All patients praised the accessibility and affordability of TB treatment services stating that healthcare providers, services, and medications both in inpatient and outpatient TB facilities were always accessible.
Thank God it is free of charge and examinations are not associated with any expenditures. P7, 45 y/o male
There were no issues regarding the accessibility of drugs. P2, 61 y/o male
If one wants the treatment, everything is accessible. In the ambulatory treatment I have seen her [the physician] almost every day: she even gave her phone number. A patient can call her any time. In the hospital as well, the physician was always there. P6, 68 y/o female
Discussion
This was the first study that explored factors facilitating treatment adherence among TB patients in Armenia. Most of the factors found to be important for Armenian patients were also highlighted in studies conducted in other countries. However, some of our findings are unique and require further investigation/confirmation by other researchers.
We found that patients’ beliefs regarding the severity of their disease and their trust in the effectiveness of treatment were strong facilitators of treatment adherence. Similarly, Gebremariam et al revealed that beliefs in severity and curability of disease were positive factors for adherence to TB treatment among TB patients co-infected with HIV.24 Other studies concluded that trust in treatment efficacy positively affects adherence.25,26 Former patients interviewed in our study acknowledged that awareness of possible complications from untreated TB helped them adhere to treatment. An interesting facilitator of adherence that emerged in our study was patients’ fear of infecting family members with TB, which, to our knowledge, has not been previously discussed in the literature.
Trust in healthcare providers supported adherence to treatment among our study participants. A belief in the physicians’ competence in performing their professional duties, such as recommendations and prescriptions, strongly motivated participants to follow their guidance. The literature suggests that, in general, trust has a crucial role in building credible patient-physician relationships that, in turn, can influence patient outcomes.27 Previous surveys conducted in Armenia studying the utilization of healthcare services have demonstrated that the lack of trust towards physicians and their professional competencies might be one of the main barriers to seeking care.28,29
Knowledge about TB and TB medications did not seem to facilitate adherence to treatment among our study participants, since many of them did not have even a basic understanding of TB. In contrast to our findings, researchers who studied adherence to DOT among TB patients in Ethiopia and China reported that TB knowledge was found to be a facilitator of adherence.24,30,31 The reason for this discrepancy could be other predisposing factors that seemed to compensate for the lack of knowledge of TB in Armenia. In particular, patients’ strong beliefs in competency of their treating physicians could have been enough to help them adhere to their recommendations and overcome their disease.
Our study showed that feeling personally responsible for their treatment outcomes was one of the most important factors that determined patients’ readiness to complete the treatment. Although all participants acknowledged the important role of healthcare providers in supporting them throughout the treatment, they thought that without their own conscientious attitude physicians would not be able to help them. Other factors revealed as important facilitators of adherence in our study, such as fear of infecting others and desire to become healthy again and continue to lead and support their families, seemed to contribute to this elevated sense of responsibility among our participants.
Our study disclosed two aspects of family support that facilitated adherence to treatment. First, family members provided emotional, moral, and financial assistance for our participants that helped them to overcome the disease. Throughout the treatment, family members consistently encouraged patients to take their medications and eat nutritious meals. This finding is consistent with the literature.32,33 Second, for male participants in particular, their perceived importance and leading role in the family was a strong facilitator of adherence to anti-tuberculosis treatment. These findings are in line with a recent study conducted in Armenia which showed that family-based TB counseling significantly supports treatment adherence through improved interpersonal relationships within families and enhanced family support towards treatment recipients.14 Therefore, the potential of engaging families in the process of TB treatment may have significant implications in terms of addressing non-adherence.
An empathetic patient-provider relationship is an important determinant of adherence to treatment.5 Family members of former patients highly valued the continuous support, encouragement, and empowerment that patients received during the treatment process stating that healthcare providers played an important role in making their patients adhere. Surprisingly, along with appreciating this empathy and support, patients felt that their fear of physicians often made them “obey” and complete the treatment. Patients gave complete authority to the treating physician and acknowledged that their role was to be obedient to physicians’ orders. Similarly, in a study conducted to explore the mechanisms of medication adherence among type 2 diabetic patients, Reach et al reported that some patients remain passive while receiving the treatment, which they described as obedience.34
Perhaps the most interesting revelation in our study was that despite multiple reports in the literature that stigma hinders support and care for patients, the participants in our study who were stigmatized did not perceive it as a barrier to treatment.33,35–37 On the contrary, some of them mentioned that they wanted to adhere to the treatment and be cured as soon as possible because of the associated stigma. This finding is also in contrast with our previous understanding of stigma and its significance in the Armenian culture, where it has been well acknowledged as one of the strongest barriers to treatment for TB and HIV patients.38–40 This finding requires further examination into methods to address this discordance during TB patient counseling sessions and to create an opportunity to support and build resilience among TB patients.
Side effects caused by anti-tuberculosis medication have been shown to be major contributors to poor adherence to treatment.5,16,41 Only a few of our participants had side effects and those who experienced them stated that they did not pay much attention to them. We assume that the absence of serious side effects in this particular group of former TB patients that we interviewed was important for good adherence.
Accessibility and affordability of health care services were perceived to be important facilitators of adherence in our study. Implementation of DOT regimens helps to ensure accessibility and affordability of the intensive continuation phases for all TB patients.42 We found that the DS-TB treatment regimen was delivered appropriately to all study participants. The literature suggests that the complexity of the treatment regimen, its duration, and the variety of drugs are potential barriers to adherence to treatment and that decreasing treatment duration might help with improving treatment adherence.5,43 However, in our study population, only a few participants complained about the treatment course and it appeared that participants’ understanding of the necessity of treatment has had a positive effect on adherence.
Our study has several limitations. First, the sampling strategy, which involved identifying and contacting patients through physicians, could have resulted in the inclusion of those patients who experienced good support from physicians. However, given that our study aimed to study former TB patients with successful treatment experience, we believe that our sampling strategy had only minimal effect on our findings. Second, the study sample ended up including former patients who predominantly had sputum smear-negative TB. Yet, the experience of former patients with sputum smear-positive TB would have brought additional perspectives on facilitators of adherence.
Lastly, the generalizability of our results to other TB patients, including extrapulmonary and DR-TB who experience far more complex TB treatments, is limited. A longer treatment regimen could be facilitated by different factors that we did not explore in the current study.
To our knowledge, this was the first study that focused on factors that promote adherence to the treatment of tuberculosis in Armenia. The validation of findings through IDIs with family members and FGD with physicians strengthened the credibility of study findings.
Conclusion
The paper revealed and discussed valuable factors that may advance TB treatment adherence among other DS-TB patients as well. By invoking patients’ sense of responsibility, positive beliefs about TB as well as engaging families, TB healthcare providers may promote people-centered care and improve patients’ and families’ TB treatment experience and outcomes.
Recommendations
We suggest national TB programs in Armenia and countries with similar TB profiles incorporate the factors we identified into routine counseling of DS-TB patients. Future studies should explore how these factors facilitate treatment adherence among DR-TB patients and also identify additional factors unique to this group. Given that our study successfully applied a conceptual framework for understanding the phenomenon of adherence, we also recommend replication of the described methodology in similar studies of adherent behavior.
Acknowledgment
We are grateful to Dr. Anya Agopian for language editing and improving the writing quality.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Tuberculosis [fact sheet]; 2021. Accessed August 13, 2022. Available at: https://www.who.int/news-room/fact-sheets/detail/tuberculosis. Accessed August 13, 2022.
2. World Health Organization. Global Tuberculosis Report; 2019.
3. Volmink J, Garner P. Directly observed therapy for treating tuberculosis [Systematic Review]. Cochrane Database Syst Rev. 2005;4. doi: 10.1002/14651858
4. Uplekar M, Figueroa-Munoz J, Floyd K. The stop TB strategy: building on and enhancing DOTS to meet the TB-related millennium development goals. WHO Rep. 2006;22. doi:10.2165/00128413-200615310-00002
5. World Health Organization. Adherence to Long-Term Therapies. Evidence for Action; 2003.
6. World Health Organization. Anti-tuberculosis medication side-effects constitute major factor for poor adherence to tuberculosis treatment. Health Policy Plan. 2008;86. doi:10.1093/heapol/czh031
7. Kulkarni P, Akarte S, Mankeshwar R, Bhawalkar J, Banerjee A, Kulkarni A. Non-adherence of new pulmonary tuberculosis patients to anti-tuberculosis treatment. Ann Med Health Sci Res. 2013;3(1):67–74. doi:10.4103/2141-9248.109507
8. Truzyan N, Grigoryan R, Martirosyan H, et al. Operational research on risk factors for MDR TB and MDR TB-HIV/AIDS co-morbidity; 2012.
9. World Health Organization. Treatment of tuberculosis. guidelines for treatment of drug-susceptible tuberculosis and patient care; 2017.
10. United Nations. The Millennium Development Goals Report. Vol. 72. United Nations; 2015.
11. Riccardi N, Alagna R, Motta I, et al. Towards ending TB: civil community engagement in a rural area of Senegal: results, challenges and future proposal. Infect Dis. 2019;51(5):392–394. doi:10.1080/23744235.2019.1572920
12. Vink K, Colombani P, Mosneaga A, et al. Tuberculosis assessment mission to Armenia. World Health Organization; 2005. Available from: https://www.euro.who.int/__data/assets/pdf_file/0019/123166/TubArmAss.pdf. Accessed August 23, 2022.
13. World Health Organization. Global tuberculosis Control: WHO report 2007; 2007.
14. Truzyan N, Crape B, Harutyunyan T, Petrosyan V. Family-based tuberculosis counseling supports directly observed therapy in Armenia: a pilot project. J Tuberc Res. 2018;6:113–124. doi:10.4236/jtr.2018.62011
15. Khachadourian V, Truzyan N, Harutyunyan A, et al. People-centred care versus clinic-based DOT for continuation phase TB treatment in Armenia: a cluster randomized trial. BMC Pulm Med. 2020;20(1):1–10. doi:10.1186/s12890-020-1141-y
16. Sanchez-Padilla E, Marquer C, Kalon S, et al. Reasons for defaulting from drug-resistant tuberculosis treatment in Armenia: a quantitative and qualitative study. Int J Tuberc Lung Dis. 2014;18:160–167. doi:10.5588/ijtld.13.0369
17. Sahakyan S, Petrosyan V, Abrahamyan L. Diabetes mellitus and treatment outcomes of pulmonary tuberculosis: a cohort study. Int J Public Health. 2020;65(1):37–43. doi:10.1007/s00038-019-01277-2
18. World Health Organization. Tuberculosis Country Brief, 2016: Armenia.; 2017.
19. World Health Organization. Implementing the WHO Stop TB Strategy: a handbook for national tuberculosis control programmes; 2008. Available from: http://apps.who.int/iris/bitstream/handle/10665/43792/9789241546676_eng.pdf;jsessionid=287C1F41696423D354F8850510E31E3E?sequence=1. Accessed August 23, 2022.
20. World Health Organization. Tuberculosis: key facts. Available from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis.
21. World Health Organization. Revised Definitions and Reporting Framework for Tuberculosis - 2013 Revision. Vol. 18; 2013.
22. Kreuter M, Green L. Health Program Planning: An Educational and Ecological Approach.
23. Hsieh H, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
24. Gebremariam MK, Bjune G, Frich JC. Barriers and facilitators of adherence to TB treatment in patients on concomitant TB and HIV treatment: a qualitative study. BMC Public Health. 2010;10(1):651. doi:10.1186/1471-2458-10-651
25. Munro S, Lewin S, Smith HJ, Engel ME, Fretheim A, Volmink J. Patient adherence to tuberculosis treatment: a systematic review of qualitative research. PLoS Med. 2007;4(7):e238. doi:10.1371/journal.pmed.0040238
26. Shargie EB, Lindtjørn B. Determinants of treatment adherence among smear-positive pulmonary tuberculosis patients in Southern Ethiopia. PLoS Med. 2007;4(2):e37. doi:10.1371/journal.pmed.0040037
27. Martin LR, Haskard KB, Dimatteo MR, Dimatteo MR. The challenge of patient adherence. Therapeutics and Clinical Risk Management. 2005;1(3):189–199.
28. Tonoyan T, Muradyan L. Health inequalities in Armenia - Analysis of survey results. Int J Equity Health. 2012;11(1):1. doi:10.1186/1475-9276-11-32
29. Andreasyan D, Bazarchyan A, Manukyan S, et al. Health system performance assessment: Armenia; 2016.
30. Wang J, Fei Y, Shen H, Xu B. Gender difference in knowledge of tuberculosis and associated health-care seeking behaviors: a cross-sectional study in a rural area of China. BMC Public Health. 2008;8:354. doi:10.1186/1471-2458-8-354
31. Tekle B, Mariam DH, Ali A. Defaulting from DOTS and its determinants in three districts of Arsi Zone in Ethiopia. Int J Tuberc Lung Dis. 2002;6(7):573-579.
32. Paz-soldán VA, Alban RE, Jones CD, Oberhelman RA. The provision of and need for social support among adult and pediatric patients with tuberculosis in Lima, Peru: a qualitative study. BMC Health Services Research. 2013;13. doi10.1186/1472-6963-13-290
33. Kaulagekar-nagarkar A, Dhake D, Jha P. Perspective of tuberculosis patients on family support and care in rural Maharashtra. Indian J Tuberc. 2012;411007:224–230.
34. Reach G. Obedience and motivation as mechanisms for adherence to medication: a study in obese type 2 diabetic patients. Patient Prefer Adherence. 2011;5:523–531. doi:10.2147/PPA.S24518
35. Courtwright A, Turner AN. Tuberculosis and stigmatization: pathways and interventions. Public Health Rep. 2010;125(SUPPL. 4):34–42. doi:10.1177/00333549101250s407
36. De Schacht C, Mutaquiha C, Faria F, et al. Barriers to access and adherence to tuberculosis services, as perceived by patients: a qualitative study in Mozambique. PLoS One. 2019;14(7):1–11. doi:10.1371/journal.pone.0219470
37. Gebreweld FH, Kifle MM, Gebremicheal FE, et al. Factors influencing adherence to tuberculosis treatment in Asmara, Eritrea: a qualitative study. J Heal Popul Nutr. 2018;37(1):1. doi:10.1186/s41043-017-0132-y
38. International Organization for Migration. Migrant health survey on TB and HIV and health service response for migrants; 2018.
39. Dara M, Krtchyan Z, Ghukasyan G. Extensive review of TB prevention, care and control services in Armenia 21 April – 4 May 2011; 2011.
40. Grigoryan R, Truzyan N, Martirosyan H, Crape B, Petrosyan V, Antonyan M. Analysis of the TB control system in Armenia in both the civilian and penitentiary sectors and recommendations for improvement. Yerevan; 2008.
41. Yee D, Valiquette C, Pelletier M, Parisien I, Rocher I, Menzies D. Incidence of serious side effects from first-line antituberculosis drugs among patients treated for active tuberculosis. Am J Respir Crit Care Med. 2003;167(11):1472–1477. doi:10.1164/rccm.200206-626OC
42. Sharma SK, Mohan A. Directly Observed Treatment, Short-Course (DOTS). J Indian Acad Clin. 2004;5(2):109–113.
43. Riccardi N, Villa S, Alagna R, et al. Advantages and challenges of tailored regimens for drug-resistant tuberculosis: a stoptb Italia look into the future. Infect Drug Resist. 2020;13:2795–2800. doi:10.2147/IDR.S257480
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.