Back to Journals » Journal of Asthma and Allergy » Volume 15
Changes in Cough Reflex Sensitivity in Children After Removal of Hypertrophied Adenoid Tissue
Authors Sojak J, Durdik P, Omar Mohamedova E, Grendar M, Lucanska M, Pec MJ, Tatar M, Pecova R ![]()
Received 30 December 2021
Accepted for publication 16 March 2022
Published 19 April 2022 Volume 2022:15 Pages 517—524
DOI https://doi.org/10.2147/JAA.S347355
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Jan Sojak,1 Peter Durdik,2 Eva Omar Mohamedova,3 Marian Grendar,4 Miroslava Lucanska,5 Martin Jozef Pec,6 Milos Tatar,7 Renata Pecova7
1Clinic of Otorhinolaryngology and Head and Neck Surgery, Faculty of Medicine, Slovak Medical University in Bratislava, Central Military Hospital in Ruzomberok, Ruzomberok, Slovak Republic; 2Clinic of Children and Adolescent, Jessenius Faculty of Medicine in Martin, Comenius University in Bratislava, University Hospital Martin, Martin, Slovak Republic; 3Outpatient Department of Clinical Immunology and Allergology in Ruzomberok, Ruzomberok, Slovak Republic; 4Biomedical Center, Jessenius Faculty of Medicine in Martin, Comenius University in Bratislava, Martin, Slovak Republic; 5Clinic of Otorhinolaryngology and Head and Neck Surgery, Jessenius Faculty of Medicine in Martin, Comenius University in Bratislava, University Hospital Martin, Martin, Slovak Republic; 6Clinic of Internal Medicine I, Jessenius Faculty of Medicine in Martin, Comenius University in Bratislava, University Hospital Martin, Martin, Slovak Republic; 7Department of Pathological Physiology, Jessenius Faculty of Medicine in Martin, Comenius University in Bratislava, Martin, Slovak Republic
Correspondence: Renata Pecova, Department of Pathological Physiology, Jessenius Faculty of Medicine in Martin, Comenius University in Bratislava, Malá Hora 4C, Martin, 036 01, Slovak Republic, Tel +421 43 2633 622, Email [email protected]
Purpose: The co-occurrence of adenoids and chronic cough is common in children. The goal of this research was to specify changes in cough reflex sensitivity as a result of adenoid tissue removal.
Patients and Methods: The sample group consisted of 17 children (six boys and 11 girls, aged 4– 12 years, mean age 6.24 years), all of them possessing symptoms of chronic cough and adenoids, confirmed by nasal fiberoptic endoscopy. This sample group underwent cough reflex sensitivity assessment, which took place both prior to and after endoscopic adenoidectomy. The definition of the cough reflex sensitivity is the lowest capsaicin concentration that caused two (C2) or five (C5) coughs. Capsaicin aerosol in ascending concentrations (from 0.61 to 1250 μmol/L) was inhaled by a single-breath method (KoKo DigiDoser), with the addition of an inspiratory flow regulator valve (RIFR).
Results: Concentrations of capsaicin causing two (C2) and five coughs (C5) were reported. Cough sensitivity (geometric mean with 95% CI) for C2 was 31.86 (12.98– 78.18) μmol/L preoperatively and 11.97 (6.16– 23.26) μmol/L postoperatively (P=0.064). Cough sensitivity for C5 was 234.91 (97.19– 567.77) μmol/L preoperatively and 69.13 (29.08– 164.35) μmol/L postoperatively (P=0.022). The children’s pulmonary function was within the normal range.
Conclusion: In our study, adenoidectomy significantly increased cough reflex sensitivity in non-atopic children suffering from chronic cough.
Keywords: adenoids, adenoidectomy, cough, cough reflex sensitivity, chronic cough, children
Introduction
Adenoid Hypertrophy
Children are born with the physiological presence of the nasopharyngeal tonsil, which develops until the age of 5–7 years. Naturally occurring enlargement is most intense and noticeable in the age range from 3 to 5 years. It starts to deteriorate around the age of 8 and may exist until the age of 15 years. Pathogenic bacteria may colonize the nasopharyngeal tonsil over time, chronic inflammation occurs, and the lymphatic tissue fails to maintain its protective role, therefore losing immunity, becomes hypertrophic, and loses the ability to self-purify, and the adenoid tissue fails to meet its purpose. Excessive hypertrophy of nasopharyngeal tonsil is termed adenoid hypertrophy (AH).1 While the presence of AH is not clearly understood, the involvement of inflammatory and allergic components has been suggested. The prevalence of AH in children is between 42% and 70%.2
Chronic Cough
The definition of chronic cough in children is a cough lasting for more than 4 weeks, which has been methodically assessed, with treatment aimed at the root cause irrespective of the severity of the cough.3 Common etiologies of chronic cough in children are not the same as those in adults. Two aspects are taken into consideration: age and setting. Common etiologies of chronic cough in adults are not assumed to be the prevalent causes in children aged ≤14 years, and their age and the clinical environment (eg, country and region) should be taken into account when assessing and handling their chronic cough.4
Cough Reflex Sensitivity
The measurement of cough reflex sensitivity (CRS) is used to determine the reactivity/sensitivity threshold of afferent nerve endings of the airways responsible for coughing. It can be used to monitor patients with chronic cough and also to monitor cough therapy. This method is suitable for investigating the pathogenesis of a chronic cough.5,6 Capsaicin can be used, as it is effective at low pH even in isoosmotic concentrations, and has a low rate of nerve-end tachyphylaxis for repeated aerosol stimulation at the same concentration. The assumed mechanism of coughing is the release of tachykinins as a result of capsaicin-induced provocation. CRS is defined as the lowest aerosol concentration of the tussive substance which, upon inhalation, results in a cough response. CRS modifications directly indicate changes in the reactivity of the afferent nerve endings of the airways. CRS changes in various pathological processes. For individual respiratory diseases, significant differences may be found in CRS values.7,8 It has been clearly proven that the cough response threshold is affected by age, gender, and stage of puberty. The cough reflex is subject to certain maturation, which tends to decrease the cough response threshold in girls and increase it in boys.9 So far, there is no clear explanation as to which factors accurately influence the sex differences in cough reflex and CRS. Cough sensitivity is also affected by constitutional, immunological, and hormonal factors, as well as by environmental and socioeconomic factors.
Materials and Methods
Study Subjects
The sample group of children consisted of 17 Caucasian children (six boys and 11 girls, aged 4–12 years, mean age 6.24 years).
There were several inclusion criteria: 1) age from 3 to 15 years; 2) chronic cough; 3) symptoms of AH; 4) objectified presence of AH, complete ENT examination, including anterior rhinomanometry, with exclusion of other potential causes of nasal obstruction, and nasopharyngeal swab; 5) no adenoidectomy in the past; 6) medical history negative for any respiratory or systemic diseases and exclusion of obstructive ventilatory defect, verified by pediatric examination and spirometry (ZAN500 Body; nSpire Health GmbH, Germany); 7) no upper or lower respiratory tract infections for at least 21 days before the test; 8) medical history negative for allergic diseases and atopy-negative status based on outpatient examination by an immunoallergologist: total immunoglobulin E (IgE), specific IgE, pediatric panel for chosen inhalation and food allergens, skin-prick tests for year-round and seasonal allergens; 9) no topical or systemic corticosteroids, antileukotrienes, antihistamines, or decongestants taken by the children during the examination or for a period of at least 2 weeks prior to the examination; 10) no contraindication to endoscopic adenoidectomy under general anesthesia; and 11) a good level of cooperation during the examinations.
Atopy-positive children were excluded; as atopy positive we consider a personal or familial trend to make IgE antibodies in response to low doses of allergens that normally exist in the surroundings, commonly proteins to which everybody is exposed. A propensity to develop typical symptoms such as asthma, rhinoconjunctivitis, or eczema/dermatitis was a second exclusion criterion. The term atopy was adopted if IgE sensitization was evidenced by IgE antibodies in serum or by a positive skin-prick test.10
The same methods of outpatient examinations and measurements were realized 1 day before adenoidectomy, and, for control, postoperative measurements were taken 3 months after the surgery. The main aims of the postoperative ENT examination were to assess the condition of the nasal and nasopharyngeal cavity and to exclude the AH residues.
The Ethics Committee of Jessenius Faculty of Medicine in Martin, Comenius University in Bratislava (EK 11732012) agreed to this study, and it was conducted in accordance with the Declaration of Helsinki. All the parents of the observed group of children were appropriately advised with regard to all aspects of the study, including the options for possible treatment, and provided written consent to such.
Cough Reflex Sensitivity Testing
The CRS measurement was realized as a single-breath capsaicin test. The solution was prepared from microcrystalline purified capsaicin (99.98%) in 98.6% ethanol with a mixture of high alcohols (Tween 80, Sigma-Aldrich) and sterile stabilized buffered physiological saline (pH=7). The examination was performed by inhalation of an aerosol of sterile buffered saline and subsequent inhalation of the aerosol at increasing concentrations of capsaicin (0.61, 1.221, 2.441, 4.883, 9.766, 19.531, 39.063, 78.125, 156.25, 312.5, 625, and 1250 μmol/L). The child was asked to perform quiet, slightly deep breathing through the mouthpiece of the nebulizer, with a limited, defined flow of the device. The aerosol was applied in a bolus-inspired method by computer-controlled nebulization for 400 ms (digital nebulizer KoKo DigiDoser; nSpire Health Inc, Louisville, CO), with the addition of an inspiratory flow regulator valve (RIFR; nSpire Health Inc, Louisville, CO).
A coughing response was recorded during inhalation of the tussive aerosol and for the next 15 seconds. The dose of each tussive substance concentration was applied by a single application using the single-breath method (assuming correct full-dose administration).11,12
During a positive cough reaction a full response was recorded, according to the examination protocol, along with the location of the irritant stimulus and subjective symptoms. The appropriate concentration was inhaled only once because of a cumulative effect on nerve endings in the airway. Parameters C2 and C5 were determined only by the number of clearly defined coughs. The C2 rating corresponds to the child coughing at a given concentration on average two to four times. The C5 rating corresponds to the child coughing at a given concentration five or more times. Hyporeactors were excluded. During the examination with tussive capsaicin concentrations, we carried out a “blind” control by random administration of physiological saline (twice during the entire course).11,12
Questionnaires
The subjective cough score was recorded. Before and after adenoidectomy, we asked the parents (considering the age of the children) to fill out the Hull Cough Sensitivity Questionnaire (HCSQ) and a questionnaire (score 0–70) on the most frequent AH symptoms based on anamnestic data: 1) nasal obstruction, mouth breathing, dry mouth; 2) rhinolalia clausa; 3) rhinorrhea, chronic runny nose; 4) postnasal drip, throat clearing; 5) chronic cough, upper airway cough syndrome; 6) chronic and recurrent infections of upper and 7) lower airways, wheezing; 8) swallowing difficulty, halitosis, nausea, feeding aversion; 9) obturation of the Eustachian tube, hearing loss; 10) chronic and recurrent persistent otitis media with effusion; 11) snoring; 12) obstructive sleep apnea, restless sleep; 13) enuresis; and 14) inattention, daytime sleepiness, morning headache.
Endoscopic Adenoidectomy
The adenoidectomy was performed under general anesthesia with endoscopic supervision (Karl Storz rigid endoscope, 4 mm, 70°) using a Beckman adenoid curette and St. Clair-Thompson and Jurasz adenoid forceps. Apart from this surgery, there were no other forms of treatment that could potentially influence the observed criteria.
Statistical Analysis
We compared preoperative and postoperative parameters of CRS and investigated the association between CRS and adenoidectomy. The process of analysis of the results was performed on two levels: we first individually assessed each individual and then proceeded to group analysis. The results were presented as the geometric mean and 95% confidence interval; the level of statistical significance was determined as P<0.05 and P<0.01. We used the Wilcoxon paired two-sample test. Software used for analysis was R version 3.2.3, 2015-12-10 (R Core Team, 2015, R: A language and environment for statistical computing, R Foundation for Statistical Computing, Vienna, Austria, https://www.R-project.org/).13
Results
CRS (geometric mean with the 95% CI) for the C2 parameter was 31.86 (12.98–78.18) µmol/L preoperatively and 11.97 (6.16–23.26) µmol/L postoperatively (P=0.064) (Figure 1 and Table 1). CRS for the C5 parameter was 234.91 (97.19–567.77) µmol/L preoperatively and 69.13 (29.08–164.35) µmol/L postoperatively (P=0.022) (Figure 2 and Table 1). The children’s pulmonary function was within regular limits.
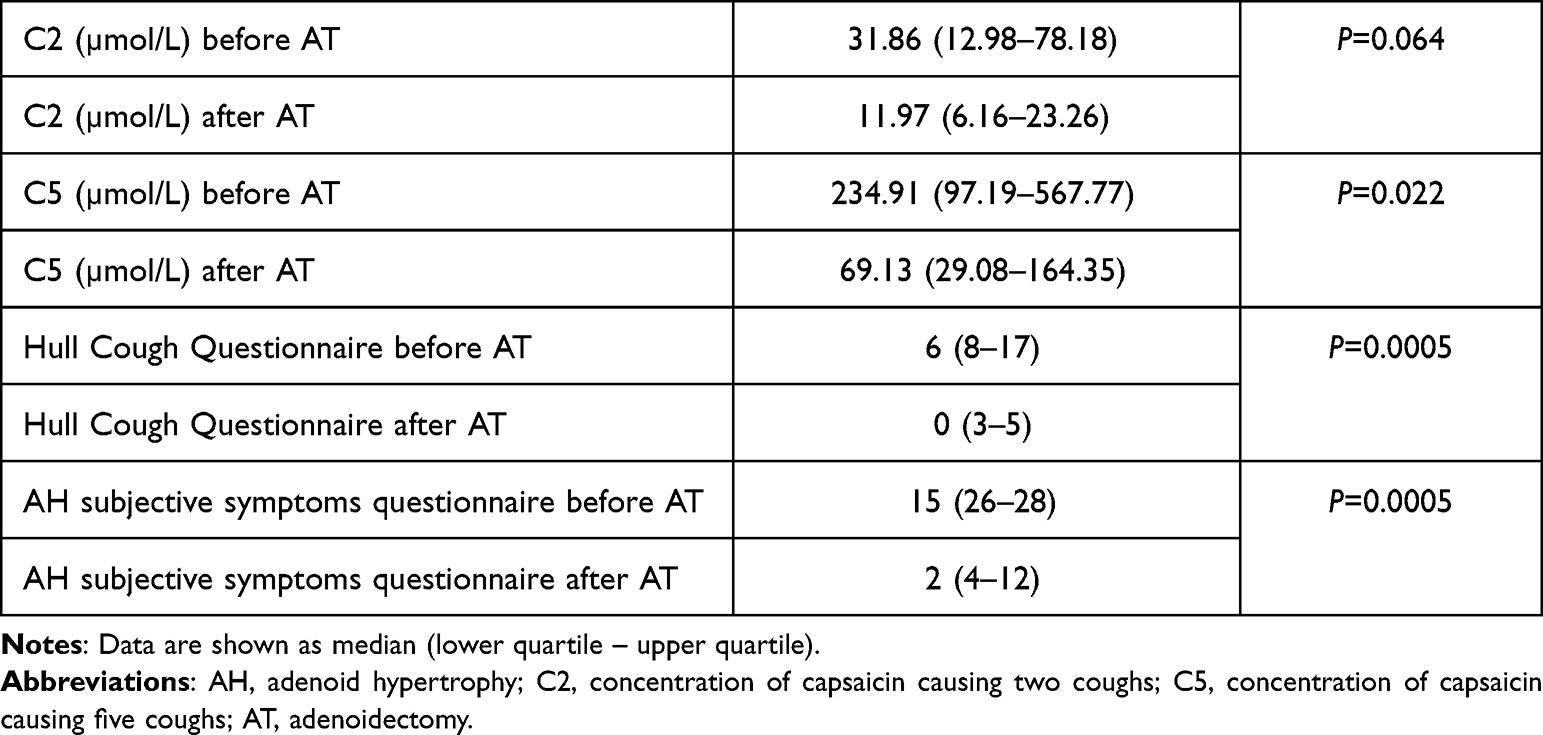 |
Table 1 Cough reflex sensitivity (CRS) - C2 and C5 values, Hull Cough Questionnaire and AH subjective symptoms questionnaire before and after AT |
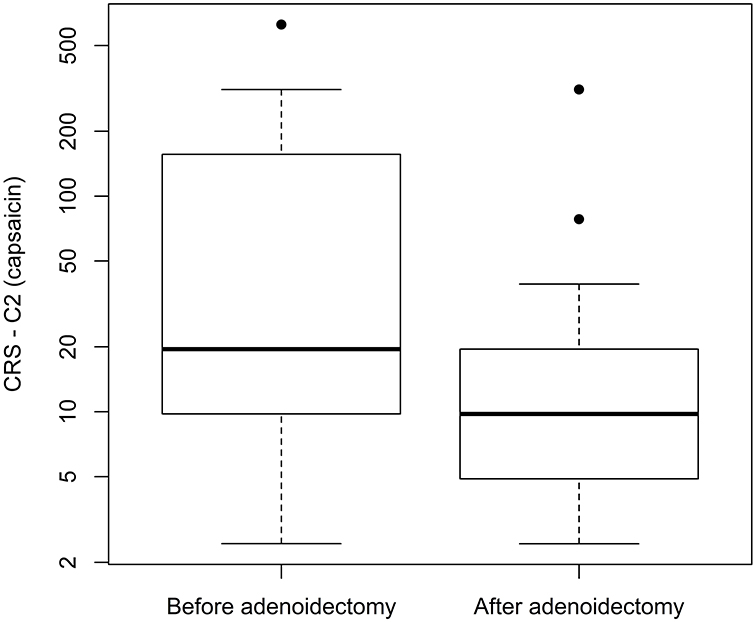 |
Figure 1 Cough reflex sensitivity (CRS) – C2 values before and after endoscopic adenoidectomy in children with chronic cough. C2, concentration of capsaicin causing at least two coughs (P=0.064). |
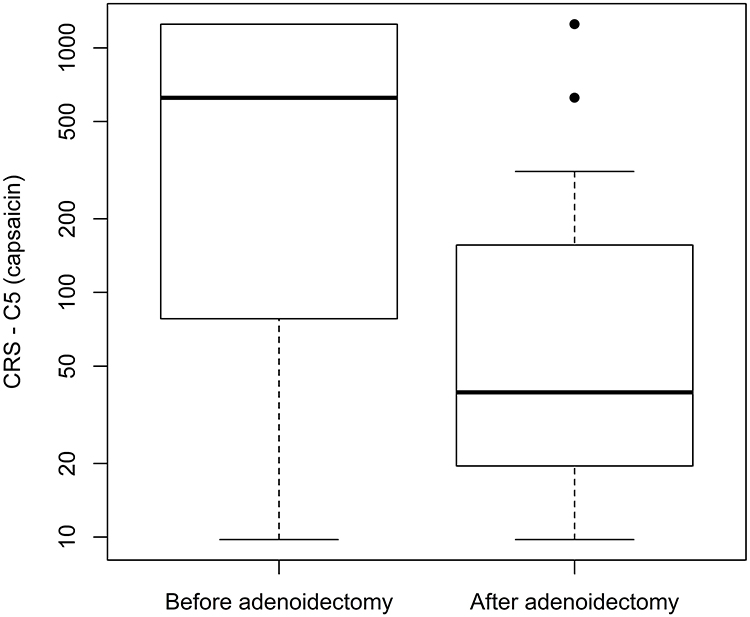 |
Figure 2 Cough reflex sensitivity (CRS) – C5 values before and after endoscopic adenoidectomy in children with chronic cough. C5, concentration of capsaicin causing at least five coughs (P=0.022). |
We found a significant change in subjective cough assessment and a significant improvement in subjective AH symptoms after adenoidectomy (Table 1).
Discussion
The main goal of this research was to classify characteristics of the modification of CRS after adenoidectomy in non-atopic children with chronic cough. We hypothesized that CRS would eventually decrease owing to: 1) reduced postnasal drip of mucus; 2) the regression of chronic inflammation of the nasopharynx and the subsequent decrease in production of proinflammatory mediators; and 3) the removal of pathogens and local infection from the nasopharynx.
The occurrence of AH in the nasopharyngeal cavity is a fairly routine issue in childhood. It presents a physical obstruction in the area of posterior choanae and in the posterior section of the nasal cavity, causing declining nasal cavity patency and the symptoms mentioned in the AH subjective symptoms questionnaire (see ”Questionnaires“ in Materials and Methods) that may all be recurrent concomitant symptoms associated with AH and the results of its severity.14,15 Dysmorphic, allergic, or phlogistic pathologies can be considered as a cause of nasal obstruction in the group of children lacking AH obstruction.16 There are two groups of manifestations that can overlap: nasal airway obstruction and nasal mucosa inflammation. As a result, a physical barrier can result in the build-up of secretions, and blockage of the nasal cavity and paranasal sinuses.1,17 Both nasal obstruction and/or phlogistic issues such as adenoiditis may cause the symptoms mentioned above.16
There is no information in the literature about the prevalence of chronic cough in children with AH. Upper airway cough syndrome (UACS) is an important cause of childhood chronic coughing and was found to be the second most common cause of chronic cough. The population prevalence is as high as 24.71% and is just behind that of cough variant asthma.18 UACS is not a specific disease but a chronic cough syndrome that is caused by a variety of upper airway diseases.19 CRS could be modulated by AH within UACS.
There are many studies regarding the pathogenesis of chronic cough. Chronic inflammation and increased airway reactivity are hot points in these studies. Some authors have suggested that upregulation of airway sensitivity, which can be caused by a variety of factors, is one of the causes of UACS.20 In children with chronic cough, the increase in airway epithelial nerves expressing transient receptor potential vanilloid 1 (TRPV1) was synchronous with the increase in transforming growth factor-β2 (TGF-β2). This preliminary finding proved the authors’ hypothesis that there is a link between chronic cough and UACS in children. There are two mechanisms: chronic inflammation, which is represented by an increase in TGF-β2, and increased airway reactivity, which is represented by an increase in TRPV1, act together to facilitate UACS in children. Airway remodeling resulting from chronic airway inflammation may be one explanation for the relevance of the two mechanisms.18 Based on the analysis of clinical factors,18 found that coughing children often had higher levels of TRPV1 and TGF-β2 compared to non-coughing children.
Normally, AH and the symptoms associated with it are dealt with through adenoidectomy. Adenoidectomy is recognized as one of the most common and efficient surgical treatments in children. Studies have also shown the positive effects of adenoidectomy in enhancing nasal patency and lowering nasal obstruction symptoms.21,22 A period of 3 months after surgery is recommended before postoperative measurements are taken owing to the fact that if they are performed sooner (eg, within 1 month after surgery), the changes in parameters are not that noticeable, which may be a direct consequence of the healing process and the existence of edema.
In spite of adenoidectomy, the CRS for C2 and C5 increased, and our hypothesis was not confirmed. There are several probable explanations for this. 1) There is altered deposition of the inhaled capsaicin in the airways after adenoidectomy. The removal of adenoid tissue may allow the capsaicin to deposit more in the larynx and the lower airways. This finding provides an explanation for capsaicin cough sensitivity changes among subjects with altered anatomy of the upper airway. 2) The cough is not associated with the pathological increased drip of mucus from the nasopharynx due to AH, but mucus production is caused mainly by the chronic inflammation in the nasal cavity and/or paranasal sinuses. 3) The cough is not associated predominantly with the chronic inflammation of the nasopharynx, but is mainly due to the chronic inflammation in the nasal cavity and/or paranasal sinuses with continued production of proinflammatory mediators. 4) Adenoid extraction does not necessarily eliminate the occurrence of remaining pathogens in the nasopharynx: the local infection prevails, as well as increased production of mucus and potential production of proinflammatory mediators. Postoperative swabs confirmed persistent bacterial colonization; our group of children was part of a larger study consisting of a group of 100 children with AH, and in only 49% of those children did the preoperative pathological finding change to physiological owing to adenoidectomy.23 5) The etiology of the cough is probably not associated with the processes in the upper respiratory tract. A potential etiological factor is non-acid reflux; however, it would be hard to find evidence for this.24 One explanation for this finding may be a single etiology producing two separate pathological processes, one AH and the other increased CRS.
On the other hand, we found a significant change in subjective symptoms, with an improvement in the assessment of both cough and AH symptoms after adenoidectomy (Table 1).
In this study, there are several limitations that should be mentioned, such as sampling. AH was a common diagnosis in all cases, except for in the control group. The sampling group was not large enough, and the number of boys and girls was unequal. Statistical results collected on a small sample may not be as objective as with a larger group, and this should be dealt with in future studies.
However, this study was not focused on determining the entire range of factors impacting CRS measures, but aimed to describe and outline the impact of adenoidectomy on cough outcome measures.
Conclusion
To conclude, CRS for C2 and C5 increased (decrease in C2 and C5 values) after adenoidectomy in non-atopic children with chronic cough. This research attributed the disputed impact of adenoidectomy to lower objectively measured CRS in children with chronic cough. Subjective cough severity was improved.
When indicating adenoidectomy, it is necessary to consider, as well as chronic cough, the presence of other frequent concomitant symptoms related to AH, which may not be improved by surgery, as unindicated surgical interventions should be avoided.
Acknowledgments
This work was supported by the project of Ministry of Health of the Slovak Republic [2018/12-UKMT-8]. This publication has been produced with the support of Interreg V-A Slovenská republika–Česká republika 2014–2020, co-financed by the European Regional Development Fund; strengthening the research and development capacity of the Slovak–Czech cross-border region in the field of plasma technologies for medical use [ITMS: 304031S579].
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Papaioannou G, Kambas I, Tsaoussoglou M, Panaghiotopoulou-Gartagani P, Chrousos G, Kaditis AG. Age-dependent changes in the size of adenotonsillar tissue in childhood: implications for sleep-disordered breathing. J Pediatr. 2013;162(2):269–274.e4. doi:10.1016/j.jpeds.2012.07.041
2. Pereira L, Monyror J, Almeida FT, et al. Prevalence of adenoid hypertrophy: a systematic review and meta-analysis. Sleep Med Rev. 2018;38:101–112. doi:10.1016/j.smrv.2017.06.001
3. Chang AB, Oppenheimer JJ, Weinberger M, Weir K, Rubin BK, Irwin RS. Use of management pathways or algorithms in children with chronic cough: systematic reviews. Chest. 2016;149(1):106–119. doi:10.1378/chest.15-1403
4. Chang AB, Oppenheimer JJ, Weinberger MM, et al.; CHEST Expert Cough Panel. Use of management pathways or algorithms in children with chronic cough: CHEST guideline and expert panel report. Chest. 2017;151(4):875–883. doi:10.1016/j.chest.2016.12.025
5. Fuller RW. Cough provocation tests: their clinical value. Pulm Pharmacol Ther. 2002;15(3):273–276. doi:10.1006/pupt.2002.0355
6. Morice AH, Millqvist E, Bieksiene K, et al. ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. Eur Respir J. 2020;55(1):1901136. doi:10.1183/13993003.01136-2019
7. Choudry NB, Fuller RW. Sensitivity of the cough reflex in patients with chronic cough. Eur Respir J. 1992;5(3):296–300.
8. Pecova R, Frlickova Z, Pec J, Tatar M. Cough sensitivity in atopic dermatitis. Pulm Pharmacol Ther. 2003;16(4):203–206. doi:10.1016/S1094-5539(02)00214-6
9. Varechova S, Plevkova J, Hanacek J, Tatar M. Role of gender and pubertal stage on cough sensitivity in childhood and adolescence. J Physiol Pharmacol. 2008;59(Suppl6):719–726. PMID: 19218699.
10. Johansson SG, Bieber T, Dahl R, et al. Revised nomenclature for allergy for global use: report of the nomenclature review committee of the World Allergy Organization, October 2003. J Allergy Clin Immunol. 2004;113(5):832–836. doi:10.1016/j.jaci.2003.12.591
11. Morice AH, Kastelik JA, Thompson R. Cough challenge in the assessment of cough reflex. Br J Clin Pharmacol. 2001;52(4):365–375. doi:10.1046/j.0306-5251.2001.01475.x
12. Morice AH, Fontana GA, Belvisi MG, et al.; European Respiratory Society (ERS). ERS guidelines on the assessment of cough. Eur Respir J. 2007;29(6):1256–1276. doi:10.1183/09031936.00101006
13. Maechler M, Rousseeuw P, Struyf A, Hubert M, Hornik K. Cluster: cluster analysis basics and extensions. R package version 2.0.5.; 2016.
14. Chohan A, Lal A, Chohan K, Chakravarti A, Gomber S. Systematic review and meta-analysis of randomized controlled trials on the role of mometasone in adenoid hypertrophy in children. Int J Pediatr Otorhinolaryngol. 2015;79(10):1599–1608. doi:10.1016/j.ijporl.2015.07.009
15. Sardón Prado O, González Pérez-Yarza E, Aldasoro Ruiz A, Oñate Bergara E, Mintegui Aranburu J, Emparanza Knörr JI. Síndrome de apneas-hipopneas obstructivas del sueño [Obstructive sleep apnea-hypopnea syndrome]. An Pediatr. 2006;64(2):120–125. doi:10.1157/13084170
16. Cassano P, Gelardi M, Cassano M, Fiorella ML, Fiorella R. Adenoid tissue rhinopharyngeal obstruction grading based on fiberendoscopic findings: a novel approach to therapeutic management. Int J Pediatr Otorhinolaryngol. 2003;67(12):1303–1309. doi:10.1016/j.ijporl.2003.07.018
17. Lucanska M, Hajtman A, Calkovsky V, Kunc P, Pecova R. Upper airway cough syndrome in pathogenesis of chronic cough. Physiol Res. 2020;69(Suppl 1):S35–S42. doi:10.33549/physiolres.934400
18. Lu YX, Gu QL, Du J, et al. Upper airway cough syndrome in children and two inflammmatory factors: TRPV1 and TGF-β2. Int J Pediatr Otorhinolaryngol. 2014;78(3):445–450. doi:10.1016/j.ijporl.2013.12.010
19. Yu L, Xu X, Lv H, et al. Advances in upper airway cough syndrome. Kaohsiung J Med Sci. 2015;31(5):223-8. doi:10.1016/j.kjms.2015.01.005
20. Chung KF. Chronic ´cough hypersensitivity syndrome´: a more precise label for chronic cough. Pulm Pharmacol Ther. 2011;24(3):267–271. doi:10.1016/j.pupt.2011.01.012
21. Feres MF, Hermann JS, Sallum AC, Pignatari SS. Endoscopic evaluation of adenoids: reproducibility analysis of current methods. Clin Exp Otorhinolaryngol. 2013;6(1):36–40. doi:10.3342/ceo.2013.6.1.36
22. Sojak J, Durdik P, Pecova R. The effect of adenoidectomy on transnasal airflow in children with hypertrophy of adenoid tissue. Afr J Paediatr Surg. 2018;15(3):126–130. doi:10.4103/ajps.AJPS_135_15
23. Dikaszová A, Sojak J, Sičák M, Grendár M. Vplyv endoskopickej adenoidektómie na mikrobiologické nálezy u detí s hypertrofiou adenoidných vegetácií. Pediatria. 2020;15(6):341–344.
24. Xu X, Yu L, Chen Q, Lv H, Qiu Z. Diagnosis and treatment of patients with nonacid gastroesophageal reflux-induced chronic cough. J Res Med Sci. 2015;20(9):885–892. doi:10.4103/1735-1995.170625
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.