Back to Journals » Risk Management and Healthcare Policy » Volume 14
Who are the “Real” Experts? The Debate Surrounding COVID-19 Health Risk Management: An Israeli Case Study
Authors Gesser-Edelsburg A ![]() , Zemach M, Hijazi R
, Zemach M, Hijazi R ![]()
Received 16 March 2021
Accepted for publication 2 June 2021
Published 21 June 2021 Volume 2021:14 Pages 2553—2569
DOI https://doi.org/10.2147/RMHP.S311334
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Anat Gesser-Edelsburg,1 Mina Zemach,2 Rana Hijazi1
1School of Public Health and the Health and Risk Communication Research Center, University of Haifa, Haifa, 3498838, Israel; 2Midgam Research & Consulting Ltd, Bnei Brak, 5126112, Israel
Correspondence: Anat Gesser-Edelsburg
School of Public Health and the Health and Risk Communication Research Center, University of Haifa, Mount Carmel, Haifa, 3498838, Israel
Tel +972 544 243530
Fax +973 3 6322143
Email [email protected]
Background: The uncertainty surrounding the COVID-19 crisis and the different approaches taken to manage it have triggered scientific controversies among experts. This study seeks to examine how the fragile nature of Israeli democracy accommodated differences of opinion between experts during the COVID-19 crisis.
Objective: To map and analyze the discourse between experts surrounding issues that were the topic of scientific controversy. To examine the viewpoints of the public regarding the positions of the different experts.
Methods and Sample: A sequential mixed study design. The qualitative research was a discourse analysis of 435 items that entailed mapping the voices of different experts regarding controversial topics. In the quantitative study, a total of 924 participants answered a questionnaire examining topics that engendered differences of opinion between the experts.
Results: The results showed that there was no dialogue between opposition and coalition experts. Moreover, the coalition experts labeled the experts who criticized them as “coronavirus deniers” and “anti-vaxxers.” The coalition changed its opinion on one issue only—the issue of lockdowns. When we asked the public how they see the scientific controversy between the coalition and the opposition experts, they expressed support for opposition policies on matters related to the implications of the lockdowns and to transparency, while supporting government policy mainly on topics related to vaccinations. The research findings also indicate that personal and socio-demographic variables can influence how the public responds to the debate between experts. The main differentiating variables were the personal attribute of conservatism, locus of control, age, and nationality.
Conclusion: Controversy must be encouraged to prevent misconceptions. The internal discourse in the committees that advise the government must be transparent, and coalition experts must be consistently exposed to the views of opposition experts, who must be free to voice their views without fear.
Keywords: COVID-19, health risk management, Israeli public, sequential mixed study design, discourse between experts, viewpoints of the public
Introduction
The COVID-19 crisis has affected governance systems such that decision-makers at all levels “have to make decisive calls about courses of actions during difficult conditions of value complexity, short response time, threat, and uncertainty.”1 Unlike other types of crises, pandemics are distinguished by tremendous uncertainty when making decisions about the characteristics, extent and gravity of the illness and the methods that will be effective in eradicating it.2–4
Under the uncertain conditions of a pandemic, people need to trust experts to help them understand and respond to the problem, governments to coordinate policy guidelines and make choices about levels of coercion, and citizens as they collaborate to minimize infection.5 The reciprocal relations between politics and science during a crisis find expression in the famous statement made by English politicians during the COVID-19 crisis to justify their policies: “We are following the science.”6
Yet this statement is inaccurate for two main reasons. One is that the pandemic has proven that expert judgments do not exist in a vacuum. They arise from specific social and political contexts. Guy Benveniste7 claimed that “technical” decisions are basically made on political or economic grounds. Expertise is required as a resource to support particular policy programs, such that the selection and interpretation of data are related to policy goals. Likewise, King and Melanson8 claimed that when knowledge is engaged in the resolution of public problems, it is shaped, manipulated, and repeatedly biased by the dynamics of the policy arena.
Considerations that are “non-scientific” influence the advice given by experts as well as the politicians who set policy. According to Alfred Moore and Michael K. MacKenzie,9 whenever scientists provide advice to political leaders, they place their expert authority at risk of being used in ways they cannot control in order to serve political ends. According to one scenario, when scientists give unwelcome advice they risk being dismissed on the grounds that they must be taking sides. According to another scenario, expert authority can be used to release political leaders from responsibility.
In considering the issue of the politicization of science, Alex Stevens10 declared:
From my own research and experience of the processes by which scientific evidence gets into policy, I know that things are rarely as simple as ministers directly ‘following the science’. There is always a risk that bias enters this process, especially when it is hidden from view.
Another reason there is no such thing as “pure science” derives from that fact that experts can be given the same information yet relate to it differently depending upon their opinions, desires, background and professional experience.11,12 Hence, Lavazza and Farina 13 claimed that when values come into play it is no longer just a matter of finding the “best technical solution” but also of making discretionary choices that affect citizens and that cannot be imposed solely on the basis of epistemic authority.
Proof of this can be found in the various and sundry ways that science has described COVID-19 and that different countries have responded. Singapore, Hong Kong, South Korea, Germany,14 Italy15 and New Zealand provide different examples of how to limit the initial spread of the virus, with different policy mixes. Hong Kong, for example, never declared a rigid lockdown. New Zealand ordered social distancing early and hard, while Sweden16 pursued a much more relaxed approach. These different approaches were informed by scientific findings, but, as Alex Stevens10 asserted, they were the result of political decisions, not science.
During the COVID-19 crisis, not only were there differences in opinion between experts from different countries, but also within the countries themselves. For example, at first the UK adopted a strategy guided heavily by disease modelling, using social distancing to slow the spread of the virus and preventing the health service from being overwhelmed, while waiting for a vaccine or natural herd immunity to develop.17 Yet the UK government was also severely criticized by public health experts who wanted much more testing to identify and isolate patients in the hope of eradicating the virus.18
These conditions marked by uncertainty and by different approaches have triggered scientific controversies during the COVID-19 period, mainly between groups working with governments, which for the most part supported conservative enforcement measures such as lockdowns, and experts representing the voice of the opposition. For example, more than 50,000 scientists and medical personnel across the globe signed an anti-lockdown petition called the Barrington Declaration,19 calling on governments to take a more targeted approach rather than blanket policy interventions.20 This raises several questions: Do experts engage in scientific discourse when they themselves have differences of opinion, and if so, how? Furthermore, within the group of experts who set government policy, is there room for the minority opinion?
In answer to these questions, philosopher Michel Foucault points to the misconception of many of these experts regarding the existence of one scientific truth. According to Foucault,21 scientific discourse is no different from other forms of discourse, and is context-, time- and place-dependent. Misconception leads people, including experts, to think about the world and identify processes in certain terms, but at the same time prevents them from noticing details or scientific theories that are inconsistent with the prevailing concepts. Foucault cites the example of the scientific theory of Gregor Mendel (1822–1884), who is now known as the father of genetics but was rejected by the scientists of his time. What Mendel asserted was correct, but his scientific discovery did not fit “within the truth of the biological discourse” of his time.
Doubt exists at the core of all scientific discourse, making scientific controversies inevitable As Gideon Rosen22 asserts,
It should be obvious that reasonable people can disagree, even when confronted with the same body of evidence … it would appear to be a fact of epistemic life that a careful review of the evidence does not guarantee consensus, even among thoughtful and otherwise rational investigators.
Yet despite the understanding that science generates doubt and controversy, the literature indicates that experts have trouble listening to the opinions of other experts and engaging in democratic discourse23 marked by many opinions and disagreements. The main reason for this is the paternalism of the experts who chart government policy. Indeed, they perceive disagreement in how they chart government policy as a threat to their professional status. Moreover, they fear that as soon as such a controversy is exposed, the public will not comply with their decisions.13,24
Studies on decision-making25–28 and management strategy29 as well as cognitive studies30,31 and advice process research32 indicate that groups make more educated decisions than individuals and diverse groups reach better decisions than smaller groups. Yet to achieve good performance, groups must overcome “groupthink”. According to social psychologist Janis (1972), groupthink describes how in-group pressures make group members strive for unanimity, causing decision-making to deteriorate and fail to appraise alternative courses of action.33 Leaders who take a centralist approach to management tend to avoid dissenting information or opinions and to lead the organization toward ignoring such opinions when making decisions,34,35 resulting in erroneous conclusions. When leaders provide only partial information in the form of “hidden profiles”,36 the organization may make erroneous decisions.29
In view of the failures deriving from striving for consensus, a large body of literature points to the importance of dissent and disagreement in decision-making. According to Scott E. Page,
when we meet people who think differently than we do …, we should see opportunity and possibility. We should recognize that a talented ‘I’ and a talented ‘they’ can become an even more talented ‘we’. That happy vision rests not on blind optimism, or catchy mantras. It rests on logic. A logic of diversity.37
Cognitive diversity37 is achieved when a core group that is diverse in terms of race, gender, and national makeup of its members reflects cognitive diversity. Such groups tend to be more capable and more responsive than homogeneous groups that convey the notion that only people like us count. When such core groups exhibit independence, creativity, and power, the other members of the organization tend to express independent and creative opinions as well.38,39 Benefits in accuracy are gained by integrating advice that comes from multiple independent points of view.40,41 Alfred Moore and Michael K. MacKenzie9 contend that experts need to have their arguments challenged if they are to avoid the cognitive pitfalls associated with overconfidence. Disagreements among experts (and others) can help expose implicit value commitments, disciplinary assumptions, and blind spots. Experts exposed to dissent actually search for more information,42 consider more strategies to facilitate performance, and exhibit more original thought.43 Oppositional argument helps diverse groups do a better work of evaluating claims both for and against given propositions.44
Research indicates that nations with a history of suppressing scientific controversies also will tend to suppress controversies regarding COVID-19 and will adopt less democratic methods, such as curfews and lockdown policies, to cope with the virus.45 Israel constitutes a special test case of how a democratic nation is coping with the virus. When the pandemic broke out, Israel was in the midst of a profound constitutional crisis that affected how it managed the pandemic. Indeed, when the COVID-19 pandemic began, Israel was being governed by an interim prime minister operating under three criminal indictments, after three election cycles.46,47 The pandemic generated a multidimensional crisis in Israel that undermined economic and social resilience, challenged effective governance and even provided a cover for processes that had the potential to harm democratic values.
This study seeks to examine how the fragile nature of Israeli democracy accommodated differences of opinion between experts during the pandemic crisis. Moreover, beyond a number of opinion papers discussing experts and COVID-19,10,13 we found no empirical studies that examined the issue of experts during the COVID-19 crisis. This empirical study seeks to add information to the research literature by mapping the many voices of the experts, analyzing their discourse during the pandemic and examining public opinions regarding the controversies.
Research Objectives
The objectives of this research are as follows:
To map the voices of the various experts who support the government (hereinafter, “the coalition”) versus those who oppose the government (hereinafter, “the opposition”) regarding the policy Israel adopted during the COVID-19 pandemic.
To analyze the discourse between these experts surrounding issues that were the topic of scientific controversy.
To identify and characterize the attitudes of coalition experts that worked with the government compared to those in the opposition who criticized the government.
To examine the viewpoints of the public at large regarding the positions of the different experts and to attempt to answer the question of how and whether Israeli democracy was able to accommodate disagreements between experts during the pandemic crisis.
Materials and Methods
Research Framework
This research is a mixed-methods study and is divided into two parts. The first part uses a sequential mixed study design,48 such that data collection for the qualitative study preceded collection of the quantitative data. The triangulation design49 entails simultaneous collection of qualitative and quantitative data. Hence the two parts of the research were of equal value at this stage, and the analysis, which included data integration and interpretation, was conducted simultaneously for the qualitative and the quantitative data.
The qualitative research is a communication study based on discourse analysis50–52 that included mapping the different voices of the coalition and the opposition regarding controversial topics during the COVID-19 crisis in Israel. The quantitative study entailed administering a questionnaire to a representative sample of the public examining topics that engendered differences of opinion between the experts. The study was approved by the Ethics Committee of the Faculty of Social Welfare and Health Sciences, University of Haifa, Approval Number 088/20.
In the following sections, we first describe the methods used in the qualitative research and then the methods used in the quantitative research.
Qualitative Research Methods
Research Sample
The research sample included 435 items representative of the dominant coalition and opposition voices. These materials included press conferences, media interviews, official letters, radio interviews, posts on social networks (Facebook and Twitter), opinion articles and official government guidelines. Directed sampling was used to locate the dominant expert voices in the discourse.53
The materials were sampled during the period from November 1, 2020 through February 18, 2021. The expert groups were mapped by means of searching Google for the names of those whose voices and opinions were dominant during the COVID-19 outbreak in Israel. After that, we searched the traditional media and the social networks for the names of each member of the opposition and coalition groups emerging from the initial search. The search results were classified according to exclusion and inclusion criteria, such that the dominant voices in the coalition included only members of official committees that advised the Ministry of Health and the government. The dominant voices in the opposition included only professionals with academic education currently or formerly serving in key positions in the health system and academia. The opposition did not included ordinary citizens who expressed critical and skeptical opinions regarding government policy.
The dominant coalition voices include senior officials in the Ministry of Health, among them the Director General, the Deputy Director General, the Director of Public Health Services and more. In addition, the group of experts in the coalition included two advisory bodies. The first is the so-called Professional Coronavirus Cabinet of the Magen Israel program,54 a professional team whose task is to advise and assist the Coronavirus Project Coordinator. The team includes 14 experts from medical and public health fields, including hospital directors, experts in epidemiology and psychology and more. Some team members hold senior positions in the Health Ministry, such as the Director and the Deputy Director of Public Health Services. A number of experts from within the Magen Israel Professional Coronavirus Cabinet sounded opposing opinions: Prof. Hagai Levine, Chair of the Israeli Association of Public Health Physicians; Prof. Nadav Davidovitch, Director, School of Public Health, Ben Gurion University; Prof. Idit Matot, Director of the Division of Surgery and Chair of the Department of Anesthesiology, Intensive Care and Pain at the Tel Aviv Medical Center; and Prof. Zeev Rotstein, Director, Hadassah Medical Center. Prof. Matot and Prof. Levine resigned from the Coronavirus Cabinet during the crisis.
The second advisory body is the National Security Council (NSC) Advisory Team for Coping with the Coronavirus Crisis55 made up of 20 experts who are not from the fields of medicine and public health and are mostly physicists.
The dominant opposition voices are from a variety of fields related to health, society and medicine:
The Model Common Sense group56 represents an independent organization of ten experts from the field of medicine, among them academics, researchers, hospital directors, epidemiologists and immunologists. In addition to the group members, several other prominent doctors and professionals worked on their behalf, including Dr. Raya Leibowitz, Dr. Rotem Inbar and Dr. Shelli Segal.
The Coronavirus Public Emergency Council57 is an independent organization of leading doctors, researchers and people from the welfare field who decided they could no longer remain silent in view of how the COVID-19 crisis was being managed. The PECC includes 21 members, some of whom are also part of the Model Common Sense group.
Prof. Yoram Lass, former Director-General of the Ministry of Health, was the first person in Israel to criticize the government’s policy.58,59 Prof. Lass is not affiliated with any group.
Dr. Michal Haran,60 an expert in hematology and internal medicine and a senior lecturer at the Hebrew University School of Medicine, spoke out about the issue of vaccinations and the emergency approval granted by the FDA.
Validity and Reliability
Throughout the qualitative research, all information relevant to the research was collected, from the stage of gathering the raw data through the analysis stage to the final findings and conclusions.61 In addition, the researchers consulted by portraying the data so as to be able to confirm or refute the research reliability.62 Hence, the information was accessible to the researchers and all steps in the research process were open, as were the analytic methods and the interpretations of the findings.63 The two researchers collaborated in analyzing the sample. The analysis included reading and transcribing all the materials and constructing the research questions. The researchers then searched the materials for answers to the research questions (see section on research instruments), and each researcher coded the answers separately. After that, the findings were integrated and the research reliability was examined by applying inter-rater reliability in analyzing the materials based on the previously determined research questions.64
Research Instruments
A protocol questionnaire was constructed for analyzing the materials, as specified below. The goal of the questionnaire was to map the interested parties, detect controversial issues, identify opposition and coalition positions for each of these issues, and find statements by members of the coalition regarding opposition criticism.
- Who are the interested parties in the coalition?
- Who are the interested parties in the opposition?
- What are the positions and fields of the interested parties in the coalition and the opposition?
- What are the issues generating differences of opinion between the coalition and the opposition?
- Did any coalition members criticize from the inside, and how did their colleagues relate to them and their criticism?
- How did the coalition react to opposition criticism and what words did they use in their response? Was their critical response pertinent or personal?
Analysis
The data from the qualitative study were analyzed using the language-dominant view of language discourse analysis method.50–52 Discourse analysis recognizes speech not as a direct representation of human experience, but rather as an explicit linguistic tool constructed and shaped by numerous social or ideological influences. In analyzing the materials, we sought answers to the questions posed in the research protocol. At first, we gave separate consideration to the materials of each member of the groups. After that, we integrated all the joint responses from the coalition and the opposition and identified the controversial issues. A total of ten controversial issues were identified: lockdown policies, testing policies, older people as an at-risk population group, children as an at-risk population group, morbidity data, wearing masks and infection in closed places versus open places, hospital collapse, intimidation, transparency, and COVID-19 vaccinations.
Next, the materials in the study sample were analyzed according to the groups and their members, while characterizing the various viewpoints in each group regarding the controversial topics. The results of the analysis were also depicted graphically and in three tables (see Findings section).
Quantitative Research Methods
Research Population and Sample
The survey entailed interviewing representative samples of each of the following subgroups in the adult population (age 18+): Arabs (N=314), ultra-Orthodox Jews (N=305), and Jews who are not ultra-Orthodox (N=305). A total of 924 participants were interviewed.
Data Collection
The interviews were conducted during the second week of January 2021 via telephone or the internet. The internet interviewees were sampled from iPanel, the largest Israeli internet panel. Among the Arabs and ultra-Orthodox participants, most of those over the age of 55 were interviewed by telephone, while among those under age 55, half were interviewed by telephone and half via the internet. Among the Jews who are not ultra-Orthodox, most over the age of 65 were interviewed by telephone, while most under age 65 were interviewed via the internet. Up to five attempts were made to reach each sampled participant, and the response rate was 62%.
Research Instruments
As noted above, the research questionnaire was constructed based on the findings of the qualitative research. The questionnaire included seven of the ten issues identified in the qualitative research as eliciting differences of opinion between the coalition and the opposition:
Viewpoints regarding the lockdowns and the guidelines and prohibitions imposed between the lockdowns, and perceived reasons for the lockdowns.
Perceptions regarding government transparency in managing the crisis and the implications of these perceptions on trust in the government.
The education system and children.
Restrictions imposed on the older population.
Viewpoints and perceptions on various vaccination-related issues.
Attitude toward experts within and outside the government system who were critical of the various steps adopted by the government (personal price paid by opposition experts for criticizing the system).
Strategies adopted by the system for conveying information to the public as perceived by the interviewees (intimidation, solidarity, and the like).
The questionnaire also examined socio-demographic and personal attributes relevant to the issue of critical thinking. Because we sought to examine the interviewees’ viewpoints regarding controversial issues, we examined personal attributes such as conservatism, locus of control and tendency to be critical.
Some of the questions were formulated as statements, such that interviewees were asked to indicate the degree to which they agree or disagree with the statement. Other questions were formulated as two contradictory claims, such that interviewees had to indicate which claim they agreed with and to what extent. Both types of questions were answered on a 4-point ordinal scale. A few questions required answering on a nominal scale. Participants answered the personal attribute questions on a 7-point scale. The complete questionnaire is provided in Supplementary Table S1.
Validity and Reliability
The questions, including those on personal attributes, were validated by face validity. An operational description was given for each personal attribute. Reliability was examined using the split half method, such that each of the samples was randomly divided into two sub-samples. The congruence between the two sub-samples was examined using Chi-square testing for goodness of fit. The research only included questions for which the analysis rejected the null hypothesis (p≤0.05).
Analysis
The data were analyzed in two stages: data processing and data analysis.
The data processing stage entailed the following:
- Examining the representativeness of each of the samples based on the following variables: sex, age, residential area. In the Arab population sample, the data was weighted to avoid sampling bias.
- Combining the files of the participants from the different population groups into an integrated file that represents the entire adult population of Israel by assigning appropriate weight to each of the samples. All the analyses were conducted in an integrated file that included the three samples.
- Combining several questions into one joint index. The joint index for all the questions enabled us to examine how the socio-demographic and personal attributes were connected to the overall position of the interviewees: Did they tend to support the government or the opposition? The condition for combining questions was a Cronbach’s alpha value ≥0.70 or a Cronbach’s alpha value ≥ 0.60 and a factor analysis showing that the combined questions were loaded on the same dimension. According to the Cronbach’s alpha data, we were able to construct the following indexes:
- Viewpoints regarding guidelines and prohibitions typifying the lockdown periods. This index included Questions 3, 4.1, 4.2, 5 and 7 (Cronbach’s alpha =0.810).
- Extent of support for experts who criticized Ministry of Health policies. This index included Questions 9.1 and 9.2 (Cronbach’s alpha =0.617). Factor analysis showed that all the questions converged around the same dimension.
- Viewpoints regarding vaccinations. The index included Questions 6, 15.1, 15.2, 15.3, 15.4, 15.5, 17 (Cronbach’s alpha =0.715).
- Restrictions imposed on older adults. Questions 11 and 18 (Cronbach’s alpha =0.711).
- Joint index for all the above questions, with the addition of questions on transparency of information conveyed by the government (Questions 10, 12, 13). While constructing a joint index for these questions was not possible, they could be included in the joint index of all the questions (Cronbach’s alpha = 0.862). A few questions entailed a nominal scale and therefore could not be integrated into any index (Questions 8, 14, 16).
The data analysis stage entailed the following:
- Mapping the interviewees’ positions along an axis ranging from support for the opposition’s positions (ie, experts who criticized government policies) to support for the coalition’s positions (ie, support for government policies). Two criteria were used in the mapping: dichotomic marginal frequencies and average marginal frequencies. Questions whose scale was nominal were categorized only according to marginal frequencies. These two criteria coincide at the following intersection points:
- Topics on which at least 55% of the interviewees expressed agreement with the government and the average was under 2.3 on a 4-point scale were classified as topics on which the public supported the coalition positions.
- Topics on which 46% to 54% supported the coalition positions or alternatively supported anti-system (ie, opposition) positions and the average ranged from 2.3 to 2.7 on a 4-point scale were classified as topics marked by a tie between the two sides.
- Topics on which at least 55% expressed opinions critical of the system or its actions and whose average was greater than 2.7 on a 4-point scale were classified as topics on which the public opposed the government (opposition positions).
- Examining how socio-demographic and personal attributes are linked to viewpoints on controversial topics.
The data were analyzed using Chi-square Automatic Interaction Detection (CHAID, also referred to as “Answer Tree”), a method used to study relationships between a dependent variable and a series of predictor variables.65 This method is similar to a step-wise regression, but it chooses the predictor with the highest significance for each level of the model. By testing the differences between groups defined by a certain independent variable, it considers the interrelations between this variable and other independent variables.66 It also allows for the use of categorical variables. When the dependent variable is an interval, the CHAID uses F-testing; otherwise, it uses Chi-square. If the dependent variable is continuous, it divides the scale into categories based on the distribution of the answers.65,67 Due to the large number of cases in the sample, a difference between groups was deemed significant if P≤.001. The answer tree identifies the best predictors of a dependent variable out of a list of independent variables. It does so by identifying the independent variable that best distinguishes groups that are significantly different from each other regarding the dependent variable and accordingly dividing the sample of participants into subgroups. Other than the decision about which independent variables to introduce into the analysis, no preliminary assumptions are made concerning the best distinguishing variables or the cutoff points for these variables. Both are determined by the analysis.
The analysis is conducted in steps. The first step identifies the independent variable distinguishing the groups that differ from each other regarding the dependent variables and divides the participants into these subgroups. The following steps identify the second and third best distinguishing variables, and so on. However, unlike, step-wise regression, the subsequent steps do not refer to the sample as a whole but rather treat each subgroup separately. For this reason, the second best predictor is not necessarily the same for all the subgroups, but rather can differ from one subgroup to another. The analysis continues until it cannot find an additional variable to add to the distinction among groups with the dependent variables.
Results
First, we discuss the results of the qualitative research and after that of the quantitative research.
Qualitative Research Findings
The findings of the qualitative research are as follows:
- Graphical mapping of the groups comprising the coalition and the opposition (Figure 1).
- Outlining the coalition positions versus the opposition positions regarding each controversial topic separately (Supplementary Table S2), except for the issue of COVID-19 vaccinations, which due to the extent of interest is depicted in a separate table (Supplementary Table S3).
- Outlining issues related to COVID-19 vaccinations, including vaccination extent, vaccinations for at-risk population groups, compulsory vaccination and sanctions imposed on those who choose not to be vaccinated, green passport, vaccinating teachers (Supplementary Table S3).
- Focusing on some of the personal attacks by coalition members on opposition members who criticized government policy (Supplementary Table S4).
 |
Figure 1 Infographic depicting mapping of the groups comprising the coalition and the opposition. |
Quantitative Research Findings
The findings of the quantitative research are as follows:
Topics for which the public tends to support government policy (the coalition) are clearly divided from those for which the public tends to support the opposition’s positions. More specifically, support for the government emerged on topics related to vaccinations, while support for the opposition emerged on topics related to the consequences of the lockdowns and to transparency. In contrast, positions reflecting equality or near equality between those supporting government policy and those opposing it are spread across a variety of topics (eg, protecting the older population versus providing them autonomy in their social lives).
When the interviewees were asked who they believe more—the doctors advising the government ministries or the experts that criticize them—the groups were almost equal: 21.8% believed the advising doctors more, while 16.1% placed more trust in the doctors from the opposition. Forty-one percent believe both groups equally, eleven percent do not believe any of them and ten percent stated they do not know. Forty-seven percent think that critics are putting their careers in jeopardy, 37.8% think they are not, and 14.8% had no opinion.
 |
Table 1 Indexes |
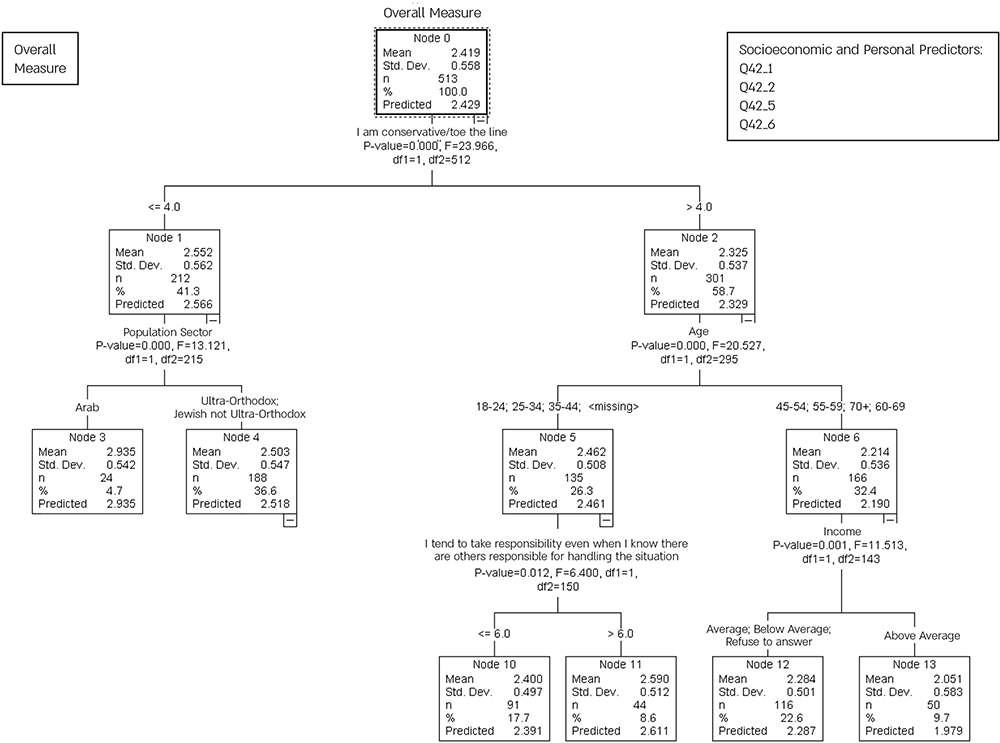 |
Figure 2 Correlations between interviewees’ attributes (socio-demographic and personal) and their viewpoints. |
CHAID of Overall Index
The main discriminatory variable was the personal attribute of conservatism. Interviewees with a tendency toward conservatism are more likely to agree with the coalition’s viewpoints (support for government policies) (M= 2.325) than interviewees who are less conservative, who tend to support the opposition’s views (M=2.552).
Each of the two groups also has an additional explanatory variable. Among those who are conservative, the additional explanatory variable is age, such that those age 45 and above show more support for the government (M=2.214), while those age 44 and younger support the opposition’s positions more (M=2.462). Among those who are less conservative, the additional explanatory variable is nationality, such that Jews tend more to support government policy (M=2.503) while Arabs show more support for the opposition (M=2.935).
Among older conservatives, income level serves as an additional variable, such that people with above average incomes support the government (M=2.051) more than those whose incomes are average or below average (M=2.284). Among younger conservatives, locus of control serves as an additional variable, such that those with a higher internal locus of control support the opposition (M=2.590) more than those with a lower internal locus of control (M=2.400). For those who are less conservative, whether Jews or Arabs, there is no additional explanatory variable.
In summary, the group that exhibits the highest support for government policies tends to be conservative, older than 45 and with an above-average income (M=2.051), while the group that shows the most support for the opposition consists of Arabs who are not conservative (M=2.935).
Discussion
The discussion of the research findings is divided into three parts: 1) scientific controversies and whether they underwent any changes; 2) public opinions concerning these scientific controversies; 3) attitude of coalition experts toward the opposition.
Scientific Controversies
The research findings show that the various groups of experts had differences of opinion regarding the policies Israel should adopt in coping with COVID-19. These competing views demonstrate how experts can interpret evidence differently due to assumptions about cause and effect that they take for granted. Moreover, dissimilar ethical claims can lead to very different decisions.17 Such controversies find expression in several areas, among them issues related to lockdowns, conducting tests, conveying morbidity information to the public, vaccinations, information communication strategies, transparency, the school system and children, and restrictions imposed on older adults.
The opposition experts contended that after the first three lockdowns Israel’s lockdown policy should be stopped, that commercial operations and the economy should be opened and that children should go back to school after the schools had been closed for an extended period of time. They claimed that the country should return to normal functioning while at the same time budgets and resources should be allocated to the public health system. Moreover, steps should be taken to safeguard the older population while respecting their freedom and autonomy, and those who choose not to be vaccinated should not be coerced either directly or indirectly.
This scientific controversy between different groups of experts in Israel has also emerged in other countries surrounding similar issues, For example, more than 50,000 scientists and medical personnel across the globe signed an anti-lockdown petition known as the Barrington Declaration,19 which calls on governments to take a more targeted approach rather than adopting blanket policy interventions.20 The experts who signed this petition criticized their governments’ lockdown policies, which they claimed dealt a serious blow to citizens’ emotional, physical and economic welfare, wreaked tremendous damage and trampled individual liberty, freedom of movement and autonomy.
During the crisis, the experts who criticized Israeli government policy were not able to influence the experts who supported and advised the government, nor did the coalition experts influence those in the opposition. The research findings indicate that there was no significant professional dialogue between these two groups of experts. Prof. Eyal Shahar, a professor of epidemiology at the University of Arizona and a member of the opposition Model Common Sense group, expressed this quite well:
Another recent worrisome trend in the world of medicine and of science in general is the deviation from the basic values of scientific thought and the deterioration of open professional discussion to the point of silencing and muzzling those with differences of opinion.68
This lack of dialogue between the different groups of experts has many causes. As emerging from the literature, some derive from the fears of experts who espouse government policy. These experts perceive that their lack of agreement would pose a threat to their professional standing and they also worry that the public will not accept their decisions if the controversy is exposed.13,24 Another reason for the lack of dialogue derives from the paternalistic approach that seeks a monopoly on science. Indeed, the experts advising the government may even see themselves as the representatives of science in their field. Regarding this issue, John Beatty claimed that change must derive from the way in which experts who advise the government and sit on the committees represent themselves.
One important factor that contributes to a more candid communication of the state of knowledge, including the extent of disagreement, within an expert committee is that such groups are generally representative of expertise in a particular area rather than constituting the sum of that expertise.24
Along with issue of striving for uniformity,69,70 which is typical of most groups that manage crises and/or policy, the professional literature in many fields of knowledge also points to the numerous advantages of “cognitive” diversity.37 A discourse of disagreement is of major importance, both in the decision-making process71 of the group itself, as expressed in attention and acceptance of minority opinions,43,72 and in the successful influence that the accommodation of professional controversies exerts on the final result.42,73
The findings of the current study indicate that the coalition opinion changed on one issue only—the issue of lockdowns. The expert committee that advised the government determined that the lockdown policy had run its course. “The forecasts were wrong. The lockdown as a magical cure is no longer feasible, it’s dead” (Prof. Ran Balicer, Chief, Professional Coronavirus Cabinet of the Magen Israel program).74 Nevertheless, Prof. Balicer also qualified his conclusion: “If we do not exercise control in loosening the lockdown, there will be many funerals.”75 In other words, contrary to the opinion of the opposition experts calling for an immediate return to normal life, the expert committee still supported restrictions.
It is important to note that announcement of the failure of the lockdown policy indicates that the opposition/minority opinion has the power to influence policy. According to Charlan Nemeth and Joel Wachtler,76 sometimes a minority can sway a majority to accept its conception. The realities in the political arena demonstrate that a strong and vocal minority can sway majority opinion. Moscovici and Faucheux77 and Moscovici and Nemeth claimed that it is possible to influence the majority opinion by means of a consistent behavioral style. When the minority group remains consistent and expresses its criticism over time, it can undermine the confidence of the majority, raise doubts and considerations, and thus challenge the majority opinion.78,79
The announcement in Israel regarding the failure of the lockdown policy can also be interpreted in terms of the influence of the conservative leadership, which the opposition experts opposed during the entire period. Certainly the reality marked by economic and social damages and the absence of a significant drop in morbidity80 had an impact on understanding that the lockdown policy as of now has run its course.
Public Opinions Concerning Scientific Controversies
When the interviewees in this study were asked who they believe more—the experts advising the government or those critical of government policy - their answers were equally divided. People can have difficulty distinguishing between health experts working for the government and those critical of the government.81 Experts tend to look alike, sound alike, and “advise” alike, leaving people to navigate the cacophony.
When we asked people how they see the scientific controversy between the coalition experts and those in the opposition, the results pointed to a clear distinction between the issues on which the public tends to support government policy (coalition) and those on which the public tends to support the opposition. Support for opposition policies was found on matters related to the implications of the lockdowns and to transparency.
The main interpretation of the finding regarding opposition to lockdowns is that during the entire COVID-19 period, which has lasted almost a year, the public personally experienced the consequences of the lockdowns and was able to assess the advantages and disadvantages achieved. In view of the high health price paid by Israel up to the time of writing this paper (more than 5,000 deaths despite the lockdowns)82 and the high economic price (over a million unemployed,83 along with the emotional costs forced upon the Israeli public84), most Israelis were critical of the lockdown policy. That is, this reality and its consequences led the interviewees to oppose and criticize the lockdowns.
Furthermore, the study found that the public believes that the government and its advisory committees lack transparency in their operations. It is reasonable to assume that the 30-year confidentiality ruling regarding the protocols of these committees85,86 caused many interviewees to wonder why this information blackout is necessary. Is concealment one of the reasons? This information blackout and concealment led the interviewees to think that the lack of transparency has a deleterious impact on reliability. Studies point to the major importance of transparency in achieving public trust, while lack of transparency is harmful to trust.87,88 Public trust in government institutions and leaders is considered essential in any country that seeks to impose its sovereignty on the people and maintain order. If citizens do not place trust in the authority of the government, the character of the country as well as its political, economic and social stability are liable to be harmed.89
Support for government policy emerged mainly on topics related to vaccinations, which may be explained by the fact that the study was conducted at the beginning of the vaccination campaign. The public could not yet formulate an independent opinion about the COVID-19 vaccination and its repercussions due to lack of experience as well as the lockdown policy. The public thus tended to accept the government’s position despite its mixed opinions (support or opposition related to framing the vaccination as experimental and to whether young people should be vaccinated).
The public had mixed views regarding a variety of topics, for example the issue of the older population. On the one hand, the public supported the government position that prohibited family members from visiting older relatives. On the other hand, the public had reservations about the issue of older people’s autonomy, that is, their right to decide upon their social contacts as they saw fit. The interviewees may have accepted the government position that the older population needed to be protected and isolated to prevent mortality because they recognized the life-saving narrative that echoed throughout the crisis. On the other hand, some interviewees acknowledged that the older population should have autonomous control over their lives.
The interviewees’ mixed viewpoints testify to a cognitive and dual process that integrates agreement and disagreement with decision-makers and indicates that the interviewees examined each issue on a case-by-case basis rather than a personal basis. That is, as the interviewees noted, they did not perceive the experts who advised the government as more expert than those who voiced the opposition position.
Sophia Rosenfeld’s book Democracy and Truth90 describes this dialectic of disagreement. According to Rosenfeld, ever since the French and American Revolutions, the politics of democracy have mediated between the refined and systemized knowledge of experts and the plain common sense of ordinary people. Indeed, she suggests that democratic politics need both expert knowledge and common sense and that based upon rational disagreement, these two factors can be integrated into a kind of symbiosis.
The research findings also indicate that personal and socio-demographic variables can influence how the public responds to the debate between the different experts. The main differentiating variable is the personal attribute of conservatism. Interviewees who tend to be more conservative agree more with the coalition’s views, as opposed to less conservative interviewees, who agree more with the opposition views. These findings may be explained by the fact that people who tend toward conservatism also tend to support the establishment’s views and to accept its approach and claims, as opposed to those who tend to be less conservative. Each of these groups has an additional explanatory variable. Among those who are conservative, the additional explanatory variable is age, such that those age 45 and above show more support for the government, while those age 44 and younger give more support to the opposition’s positions. These findings are in line with studies showing that young people are less established and tend to be less conservative91,92 than older people and to adopt anti-establishment opinions and approaches in politics, as well as in health policies, as reflected in this study.
Among those who are less conservative, the additional explanatory variable is nationality. Jews support government policy (coalition), while Arabs support the opposition. The coronavirus crisis revealed that as a minority group the Arabs experienced a crisis of trust in the government.93 The research findings are in line with this fact.
Among older conservatives, income level serves as an additional variable. People with above average incomes support the government more than those whose incomes are average or below average. This finding may be explained by the fact that the COVID-19 crisis was more detrimental economically to weakened population groups94 and served to widen social gaps. Hence, those harmed by the economic crisis tended to give less support to government policy.
Among younger conservatives, locus of control serves as an additional variable. Those with a higher internal locus of control support the opposition more than those with a lower internal locus of control. A possible explanation for this variable is that people who place less trust in external forces and more on themselves tend to adopt more independent views and approaches, thus supporting those who are more critical.
Attitude of Coalition Experts Toward the Opposition
In fighting anti-smoking and anti-tobacco legislation and trends, the tobacco industry adopted an effective strategy that entailed personal attacks on scientists and experts whose findings were detrimental to the industry.95 The strategy described these scientists or experts as eccentric and marginal individuals motivated by personal agendas.4 Other industries have also adopted this personal attack strategy. During COVID-19, public health professionals or policymakers depicted their critics as ideologues with research biases who were trying to promote their personal agendas.
The research findings indicate that the coalition experts labeled the experts who criticized them as “coronavirus deniers” and “anti-vaxxers.” The coalition members’ attitudes toward criticism of the government’s policies were not to the point. Moreover, they framed the professional debate as a debate between science and deniers of science, which certainly was not the case. As indicated in the mapping, the experts who criticized government policy were for the most part academics from the field of medicine whose credentials were no less outstanding than those who supported government policy. In addition, those in the establishment and the coalition directed personal attacks against those who criticized them. Instead of attacking the substance of the argument itself, they launched attacks against the character, motives or other attributes of their critics.96 This avoids genuine debate by creating a diversion to some irrelevant but often highly charged issue. Ad hominem attacks divert attention from the primary arguments and thus neutralize the fundamental discussion. Moreover, we also found that experts who criticized government policy from within the system found themselves under personal attack as well. This was the case for experts who sought to give voice to the views of the opposition expert in the television documentary: “And what if the whole world is wrong?” Some of those who tried to change decisions from within were dismissed.
Personal attacks against opposition experts who dared to criticize and ask questions were also translated into practical actions, for example in the form of reprimands or even dismissal. Dr. Michal Haran, who wrote a comprehensive and detailed position paper outlining the uncertainties and challenges in the FDA’s emergency approval of the Pfizer vaccine, received a letter from the council reprimanding her for deceiving the public.97 Moreover, Prof. Eitan Friedman98 was not renewed as director of the oncogenetics department at Sheba Medical Center, a hospital located at the center of the country.
When the interviewees were asked whether criticism of the health system is detrimental to the careers of the critics, 47% indicated that such criticism is indeed detrimental. The notion that criticism can endanger a career testifies to the public atmosphere in Israel and the silencing policy. One of the most important attributes of democracy is tolerance of other people’s opinions. The literature indicates that nations that are less democratic tended to be less tolerant of criticism during the COVID-19 crisis and to adopt more extreme measures, such as lockdowns.99 The research findings show that the fragile situation in Israel brought on by the governmental and legal crisis has exposed difficulties in accommodating a discourse that embraces and adopts disagreements and controversies.
Managing the global discourse rather than engaging in dialogue has generated the aforementioned failures in the decision-making process. Moreover, from a historical perspective, it is precisely those committees that at times of crisis were smart enough to include experts with differing opinions and from different fields that achieved effective results. During the Ebola epidemic, for example, the Scientific Advisory Group for Emergencies (SAGE) convened historians, anthropologists, behavioral scientists, engineers, mathematical modelers and infectious-disease experts from around the world.100
Research Limitations
Because the study was conducted during a particular time period, the findings must be considered within the context of this period and cannot shed light on all the consequences. In addition, while the qualitative research that mapped and analyzed the voices of the experts did include most of the expert groups, there may be other groups. Moreover, the research referred primarily to groups rather than to individuals, with the exception of two lone voices that led the opposition discourse.
Future research should examine the implications of the discourse between the experts and its impact on the greater public as well as on health workers in the health system.
Conclusion
During a health crisis that includes elements of uncertainty, the situation must be examined from several perspectives. The major challenge during a crisis such as COVID-19 is how to translate science into concrete guidelines for the citizens. In the literature it appears that the issue of trust between politicians and experts, between experts and politicians, and between citizens and politicians must be addressed in order to build resilience among the citizens.5,101
But beyond the issue of trust, Andrea and Farina13 claimed that during COVID-19 politicians were required not only to provide technical guidelines but also those that touch upon the lifestyle of citizens and that involve values. In such a case, politicians need to frame science as something that suits the lifestyle of the citizens: “not all expert recommendations need to be automatically implemented, as some recommendations include axiological and regulatory elements that should be justified in the political process“ (p. 10). As noted in the present study, it is precisely the scientific controversy between different experts that can give politicians the tools to understand the complexity of the problem. The policy support from each of these experts also represents a different world of values. Politicians are required to identify and involve citizens in this process. Recognizing that the problem or the solution is not merely “pure science” allows politicians to show mental flexibility and change policy according to reality as well.
It is important to encourage controversy and differences of opinion in order to challenge thinking and prevent misconceptions and dogmatic views. Rethinking the effectiveness of lockdowns among the experts in Israel proves this. We suggest that rethinking can have an impact along two lines. The first entails the inclusion of experts from the behavioral sciences who can show the committees how they are conducting their discourse and recommend dialectic discussion methods. The second involves providing consistent exposure to experts from the opposition, who can make their opinions heard without fear and thus challenge the system to think and draw conclusions.
In addition, the groups advising the government should respect minority opinions and communicate these to the public, which expects full transparency. Thus, minority opinions must be synthesized into the reports communicated to the public in order to reinforce public trust in the decision-making process. Moreover, the discourse between the various experts must be respectful, open and accepting, without deteriorating into an impassioned discourse and into silencing others. A country that wants to preserve its democracy must also pay attention to, accommodate and be challenged by criticism from within.
Abbreviations
COVID-19, coronavirus disease 2019; FDA, Food and Drug Administration; SAGE, Scientific Advisory Group for Emergencies; The PECC, The Coronavirus Public Emergency Council.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of The Faculty of Social Welfare and Health Sciences at the University of Haifa (approval no.088/20). Written informed consent was obtained from study participants. Participant informed consent included the publication of anonymized responses. Privacy and confidentiality of participants were guaranteed before, during, and after data collection. The authors confirm that this study was conducted in accordance with the Declaration of Helsinki.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nohrstedt D. Uncertainty, accountability, and the conduct of post‐crisis inquiries. In: Svedin L, editor. Ethics and Crisis Management. Charlotte, NC: Information Age Publishing; 2011:199–216.
2. de Vries G, Verhoeven I, Boeckhout M. Taming uncertainty: the WRR approach to risk governance. J Risk Res. 2011;14(4):485–499. doi:10.1080/13669877.2011.553728
3. Gesser-Edelsburg A, Stolero N, Mordini E, Billingsley M, James JJ, Green MS. Emerging infectious disease (EID) communication during the 2009 H1N1 influenza outbreak: literature review (2009-2013) of the methodology used for EID communication analysis. Disaster Med Public Health Prep. 2015;9(2):199–206. doi:10.1017/dmp.2014.126
4. Gesser-Edelsburg A, Shir-Raz Y. Risk Communication and Infectious Diseases in an Age of Digital Media. London and New York: Routledge; 2016.
5. Cairney P, Wellstead A. COVID-19: effective policymaking depends on trust in experts, politicians, and the public. Policy Design Pract. 2020;1–14. doi:10.1080/25741292.2020.1837466
6. Horton R. How can any scientists stand by this government now? The Guardian. 2020.
7. Benveniste G. The Politics of Expertise.
8. King LR, Melanson P. Knowledge and politics. Public Policy. 1972;20:82–101.
9. Moore A, MacKenzie MK. Policy making during crises: how diversity and disagreement can help manage the politics of expert advice. BMJ. 2020;371:m4039. doi:10.1136/bmj.m4039
10. Stevens A. Governments cannot just ‘follow the science’ on COVID-19. Nat Hum Behav. 2020;4(6):560. doi:10.1038/s41562-020-0894-x
11. Nelkin D. The political impact of technical expertise. Soc Stud Sci. 1975;5(1):35–54. doi:10.1177/030631277500500103
12. Oreskes N. Why Trust Science? Princeton, NJ: Princeston University Press; 2019.
13. Lavazza A, Farina M. The role of experts in the Covid-19 pandemic and the limits of their epistemic authority in democracy. Front Public Health. 2020;8:356. doi:10.3389/fpubh.2020.00356
14. Rothmund T, Farkhari F, Azevedo F, Ziemer CT. Scientific trust, risk assessment, and conspiracy beliefs about COVID-19 - four patterns of consensus and disagreement between scientific experts and the German public. 2020. doi:10.31234/osf.io/4nzuy
15. Malandrino A, Demichelis E. Conflict in decision making and variation in public administration outcomes in Italy during the COVID-19 crisis. Eur Policy Anal. 2020;6(2):138–146. doi:10.1002/epa2.1093
16. Franks PW, Nilsson PM. Sweden under fire for ‘relaxed’ coronavirus approach – here’s the science behind it. The Conversation. 2020 March 28.
17. Nicholds A. Coronavirus: why experts disagree so strongly over how to tackle the disease. The Conversation. 2020 April 8.
18. Sridhar D. The lockdown only buys us time: to really defeat the virus we need mass testing now. The Guardian. 2020 April 1.
19. Blanchard S, Spencer B. 6,500 scientists and medics sign anti-lockdown petition calling for ‘focused protection’ of vulnerable people from COVID so the young can build herd immunity. Mail Online. 2020 October 6.
20. Sikora K. Twitter. 2020 September 1.
21. Foucault M. The order of things: an archaeology of the human sciences. In: Young RJC, editor. Untying the Text: A Post-Structuralist Reader. London: Routledge & Kegan Paul; 1981:48–78.
22. Rosen G. Nominalism, naturalism, epistemic relativism. Noûs. 2001;35(s15):69–91. doi:10.1111/0029-4624.35.s15.4
23. Moore A, Invernizzi-Accetti C, Markovits E, Pamuk Z, Rosenfeld S. Beyond populism and technocracy: the challenges and limits of democratic epistemology. Contemp Political Theory. 2020;19(4):730–752. doi:10.1057/s41296-020-00398-1
24. Beatty J. Masking disagreement among experts. Episteme. 2006;3(1):52–67. doi:10.1353/epi.0.0001
25. Janis IL. Groupthink: Psychological Studies of Policy Decisions and Fiascos. Boston: Houghton Mifflin; 1982.
26. Kahneman D, Klein G. Conditions for intuitive expertise: a failure to disagree. Am Psychol. 2009;64(6):515–526. doi:10.1037/a0016755
27. Schwenk CR. Strategic decision making. J Manage. 1995;21(3):471–493. doi:10.1177/014920639502100304
28. Nemeth CJ, Connell JB, Rogers JD, Brown KS. Improving decision making by means of dissent1. J Appl Soc Psychol. 2001;31(1):48–58. doi:10.1111/j.1559-1816.2001.tb02481.x
29. Baron R, Kerr N. Group Process, Group Decision, Group Action.
30. Festinger L. Informal social communication. Psychol Rev. 1950;57(5):271–282. doi:10.1037/h0056932
31. Schachter S. Deviation, rejection, and communication. J Abnorm Psychol. 1951;46(2):190–207. doi:10.1037/h0062326
32. Bonaccio S, Dalal RS. Advice taking and decision-making: an integrative literature review, and implications for the organizational sciences. Organ Behav Hum Dec. 2006;101(2):127–151. doi:10.1016/j.obhdp.2006.07.001
33. Larrick RP. The social context of decisions. Annu Rev Organ Psychol Organ Behav. 2016;3(1):441–467. doi:10.1146/annurev-orgpsych-041015-062445
34. Hoever IJ, van Knippenberg D, van Ginkel WP, Barkema HG. Fostering team creativity: perspective taking as key to unlocking diversity’s potential. J Appl Psychol. 2012;97(5):982–996. doi:10.1037/a0029159
35. van Knippenberg D, De Dreu CKW, Homan AC. Work group diversity and group performance: an integrative model and research agenda. J Appl Psychol. 2004;89(6):1008–1022. doi:10.1037/0021-9010.89.6.1008
36. Schulz-Hardt S, Brodbeck FC, Mojzisch A, Kerschreiter R, Frey D. Group decision making in hidden profile situations: dissent as a facilitator for decision quality. J Pers Soc Psychol. 2006;91(6):1080–1093. doi:10.1037/0022-3514.91.6.1080
37. Page SE. Difference: How the Power of Diversity Creates Better Groups, Firms, Schools, and Societies. Princeton, NJ: Princeton University Press; 2007.
38. Kleiner A. Are you in with the in crowd? Harvard Business Review. 2003.
39. Yaniv I. The benefit of additional opinions. Curr Dir Psychol Sci. 2004;13(2):75–78. doi:10.1111/j.0963-7214.2004.00278.x
40. Johnson TR, Budescu DV, Wallsten TS. Averaging probability judgments: Monte Carlo analyses of asymptotic diagnostic value. J Behav Decis Mak. 2001;14(2):123–140. doi:10.1002/bdm.369
41. Soll JB. Intuitive theories of information: beliefs about the value of redundancy. Cogn Psychol. 1999;38(2):317–346. doi:10.1006/cogp.1998.0699
42. Nemeth C, Rogers J. Dissent and the search for information. Br J Soc Psychol. 1996;35(1):67–76. doi:10.1111/j.2044-8309.1996.tb01083.x
43. Nemeth CJ, Kwan JL. Originality of word associations as a function of majority vs. minority influence. Soc Psychol Q. 1985;48(3):277–282. doi:10.2307/3033688
44. Mercier H, Sperber D. Why do humans reason? arguments for an argumentative theory. Behav Brain Sci. 2011;34(2):57–74. doi:10.1017/s0140525x10000968
45. Barceló J, Rahn TH, Cheng C, Kubinec R, Messerschmidt L. Suppression and timing: using COVID-19 policies against political dissidents? SocArXiv. 2020. doi:10.31235/osf.io/yuqw2
46. Gesser-Edelsburg A, Cohen R, Hijazi R, Abed Elhadi Shahbari N. Analysis of public perception of the Israeli Government’s early emergency instructions regarding COVID-19: online survey study. J Med Internet Res. 2020;22(5):e19370. doi:10.2196/19370
47. Gesser-Edelsburg A, Hijazi R. When politics meets pandemic: how Prime Minister Netanyahu and a small team communicated health and risk information to the Israeli public during the early stages of COVID-19. Risk Manag Healthc Policy. 2020;13:2985–3002. doi:10.2147/RMHP.S280952
48. Tashakkori A, Teddlie C. SAGE Handbook of Mixed Methods in Social & Behavioral Research.
49. Creswell JW, Plano Clark VL. Designing and Conducting Mixed Methods Research.
50. Boutain DM. Critical language and discourse study: their transformative relevance for critical nursing inquiry. Adv Nurs Sci. 1999;21(3):1–8. doi:10.1097/00012272-199903000-00004
51. Parker I. Discourse Dynamics: Critical Analysis for Social and Individual Psychology. New York, NY: Routledge; 2014.
52. Thorne S. Data analysis in qualitative research. Evid Based Nurs. 2000;3(3):68–70. doi:10.1136/ebn.3.3.68
53. Morse JM. Sampling in grounded theory. In: Bryant A, Charmaz K, editors. The SAGE Handbook of Grounded Theory. Thousand Oaks, CA: Sage; 2007:229–244.
54. Ministry of Health. The CORONA cabinet. September 10, 2020. Available from: https://govextra.gov.il/ministry-of-health/magen-israel/the-cabinet/.
55. National Security Council (NSC) Advisory Team for Coping with the Coronavirus Crisis. Report No. 6 - Concluding report: a complete view of the day-to-day management of the pandemic. May 10, 2020. Available from: https://www.weizmann.ac.il/physics/waxman/sites/physics.waxman/files/uploads/Corona/%D7%93%D7%95%D7%97%20%D7%9E%D7%A1%D7%9B%D7%9D.pdf.
56. Model Common Sense. 2021. Available from: https://www.facebook.com/ModelCommonSense.
57. Coronavirus Public Emergency Council. 2021. Available from: https://www.pecc.org.il/.
58. Lass Y. Yarom Lass Twitter account. Available from: https://www.facebook.com/%D7%A4%D7%A8%D7%95%D7%A4%D7%A1%D7%95%D7%A8-%D7%99%D7%95%D7%A8%D7%9D-%D7%9C%D7%A1-103537644680361/.
59. Lass Y. Yoram Lass Facebook page. Available from: https://twitter.com/lassyoram?lang=en.
60. Haran M. Michal Haran Facebook page. Available from: https://www.facebook.com/michal.haran.3.
61. Huberman AM, Miles MB. Data management and analysis methods. In: Denzin NK, Lincoln YS, editors. Handbook of Qualitative Research. Thousand Oaks, CA: Sage Publications, Inc; 1994:428–444.
62. Merriam SB. Qualitative Research and Case Study Applications in Education. Revised and Expanded from Case Study Research in Education. San Francisco, CA: Jossey-Bass; 1998.
63. Riessman CK. Narrative Analysis. Thousand Oaks, CA: Sage Publications, Inc; 1993.
64. Lombard M, Snyder-Duch J, Bracken CC. Content analysis in mass communication: assessment and reporting of intercoder reliability. Hum Commun Res. 2002;28(4):587–604. doi:10.1111/j.1468-2958.2002.tb00826.x
65. Kass GV. An exploratory technique for investigating large quantities of categorical data. J R Stat Soc Ser C Appl Stat. 1980;29(2):119–127. doi:10.2307/2986296
66. Gesser-Edelsburg A, Zemach M, Lotan T, Elias W, Grimberg E. Perceptions, intentions and behavioral norms that affect pre-license driving among Arab youth in Israel. Accid Anal Prev. 2018;111:1–11. doi:10.1016/j.aap.2017.11.005
67. McCarty JA, Hastak M. Segmentation approaches in data-mining: a comparison of RFM, CHAID and logistic regression. J Bus Res. 2007;60(6):656–662. doi:10.1016/j.jbusres.2006.06.015
68. Yehezkelli Y. Caution! slippery slope: the pandemic and disturbing trends in the world of medicine. Doctors Only. 2021 February 4.
69. Allen VL. Situational factors in conformity. In: Berkowitz L, editor. Advances in Experimental Social Psychology. Vol. 2. New York, NY: Academic Press; 1965:133–175.
70. Mackie DM. Systematic and nonsystematic processing of majority and minority persuasive communications. J Pers Soc Psychol. 1987;53(1):41–52. doi:10.1037/0022-3514.53.1.41
71. Dean JW, Sharfman MP. Does decision process matter? A study of strategic decision-making effectiveness. Acad Manage J. 1996;39(2):368–396. doi:10.2307/256784
72. Atsumi T, Bumstein E. How is minority influence digerent from majority influence and what does it have to do with awareness of being influenced? University of Michigan; 1992.
73. Herek GM, Janis IL, Huth P. Decision making during international crises: is quality of process related to outcome? J Conflict Resolut. 1987;31(2):203–226. doi:10.1177/0022002787031002001
74. Filut A. The closure is behind us, and the government still does not have an orderly plan. Calcalist. 2021 February 7.
75. Weissberg H, Weinreb G. Prof. Balicer: “If they open the closure in an uncontrolled manner, there will be a lot of funerals”. Globes. 2021 February 4.
76. Nemeth C, Wachtler J. Creating the perceptions of consistency and confidence: a necessary condition for minority influence. Sociometry. 1974;37(4):529–540. doi:10.2307/2786425
77. Moscovici S, Faucheux C. Social influence, conformity bias, and the study of active minorities. In: Berkowitz L, editor. Advances in Experimental Social Psychology. Vol. 6. Academic Press; 1972:149–202.
78. Moscovici S, Nemeth C. Social influence II: minority influence. In: Nemeth C, editor. Social Psychology: Classic and Contemporary Integrations. Chicago, IL: Rand McNally; 1974:217–249.
79. Nemeth C, Swedlund M, Kanki B. Patterning of the minority’s responses and their influence on the majority. Eur J Soc Psychol. 1974;4(1):53–64. doi:10.1002/ejsp.2420040104
80. Drukman Y, Yanko A. Despite the closure: the positive rate is high, there are no signs of a decrease in morbidity. YNET. 2021 January 26.
81. Kearnes M, Cook BR, Kuch D. We should listen to coronavirus experts, but local wisdom counts too. The Conversation. 2020 April 1.
82. Calaclist and YNET. Israel breaks a dismal negative record: more than 5,000 die from the outbreak of the corona crisis. Calcalist. 2021 February 4.
83. Bramli Golan D. More women, more young, more unemployed: the third closure is over, these are its prices. Globes. 2021 February 7.
84. Linder R. Every tenth family in Israel has someone who has developed an addiction, and there is no one to treat it. The Marker. 2021 February 12.
85. The Movment for Freedom of Information. We appealed to the Supreme Court - to disclose the minutes of the cabinet meeting in the Corona crisis. 2021. Available from: https://www.meida.org.il/?p=11037.
86. Shaffir S. These days, transparency is a matter of saving lives. haaretz. 2020 October 18.
87. Bennett P, Calman K, Curtis S, Smith D. Risk Communication and Public Health.
88. Henrich N, Holmes B. Communicating during a pandemic: information the public wants about the disease and new vaccines and drugs. Health Promot Pract. 2011;12(4):610–619. doi:10.1177/1524839910363536
89. Bensman J. The aesthetics and politics of footnoting. Int J Polit Cult Soc. 1988;1(3):443–470. doi:10.1007/BF01385430
90. Rosenfeld S. Democracy and Truth a Short History. Pennsylvania: University of Pennsylvania Press; 2019.
91. Tilley J. Do we really become more conservative with age? The Guardian. 2015 November 3.
92. Chait J. New survey shows young people are staying liberal and conservatives are dying off. Intelligencer. 2018, March 1.
93. Lavie E, Elran M, Sawaed K, Abu Mokh M, Dallashi M. Israel’s Arab society and the Coronavirus challenge. The Institute for National Security Studies; 2020:1288.
94. Weissberg H. The corona may pass, but inequality in the economy has increased. 5 graphs that indicate this. Globes. 2021 January 22.
95. Oreskes N, Conway EM. Merchants of Doubt: How a Handful of Scientists Obscured the Truth on Issues from Tobacco Smoke to Global Warming. New York: Bloomsbury Press; 2010.
96. Hughes W, Lavery J. Critical Thinking: An Introduction to the Basic Skills – Canadian Seventh Edition. Peterborough: Broadview Press; 2015.
97. Leitersdorf I, Hacco E. Dr. Michal Haran - Your publication dated 15. 12.20regarding “position paper” - Corona virus vaccines. 2021. Available from: https://www.health.gov.il/Services/Committee/deceive/Documents/2017204.pdf.
98. Atzuma. To bring back Prof. Friedman. December 30, 2020. Available from: https://www.atzuma.co.il/menaker?fbclid=IwAR0-v9M4VSroINsqiJ2K0GePaEj9eL7VF8E8OF_emD1TV-d3WGiAYsyXhuQ.
99. Barceló J, Høye rahn T, Kubinec R, Messerschmidt L. Suppression and timing: using COVID-19 policies against political dissidents? SocArXiv. 2020.
100. Donnelly CA, Boyd I, Campbell P, et al. Four principles to make evidence synthesis more useful for policy. Nature. 2018;558(7710):361–364. doi:10.1038/d41586-018-05414-4
101. Ruffa C, Eck K. In a pandemic, should the experts or the politicians be in charge? Political Violence at a Glance. 2020. Available from: https://politicalviolenceataglance.org/2020/04/01/in-a-pandemic-should-the-experts-or-the-politicians-be-in-charge/.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.