Back to Journals » Patient Preference and Adherence » Volume 15
Patient Preferences for Subcutaneous versus Intravenous Administration of Treatment for Chronic Immune System Disorders: A Systematic Review
Authors Overton PM ![]() , Shalet N
, Shalet N ![]() , Somers F, Allen JA
, Somers F, Allen JA
Received 22 January 2021
Accepted for publication 19 March 2021
Published 19 April 2021 Volume 2021:15 Pages 811—834
DOI https://doi.org/10.2147/PPA.S303279
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Paul M Overton,1 Natalie Shalet,2 Fabian Somers,3 Jeffrey A Allen4
1Beacon Medical Communications, Brighton, UK; 2NAS Healthcare Solutions, London, UK; 3UCB Pharma, Brussels, Belgium; 4Department of Neurology, Section of Neuromuscular Medicine, University of Minnesota, Minneapolis, MN, USA
Correspondence: Jeffrey A Allen
Department of Neurology, Section of Neuromuscular Medicine, University of Minnesota, 420 Delaware Street SE, MMC 295, Minneapolis, MN, 55455, USA
Tel +1 612-625-1969
Fax +1 612-625-7950
Email [email protected]
Background: For many chronic immune system disorders, the available treatments provide several options for route of administration. The objective of this systematic literature review is to inform discussions about therapy choices for individual patients by summarizing the available evidence regarding the preferences of patients with chronic immune system disorders for intravenous (IV) or subcutaneous (SC) administration.
Methods: Searches of the MEDLINE, Embase and Cochrane Library databases were conducted using terms designed to capture studies reporting patient preferences between IV and SC therapy published in English. Relevant studies were limited to those in which mode of administration, including treatment frequency and setting, was the main difference between comparators.
Results: In total, 49 studies were included in the review. Among 18 studies that compared IV and SC immunoglobulin therapy, 16 found patients to prefer the SC administration route. The results of the 31 studies comparing IV infusion and SC injection of non-immunoglobulin therapies were mixed, with patients favoring SC administration in 20, IV infusion in seven, and having no overall preference in four. Patient experience had a strong effect on preferences, with treatment-experienced patients preferring their current administration route in most studies. Patients preferring SC administration tended also to prefer treatment at home, mainly due to the convenience and comfort of home treatment and the avoidance of having to attend hospital. By contrast, patients preferring IV infusion tended to cite the lower treatment frequency and a dislike of self-injecting, and preferred hospital treatment, mainly due to the presence of healthcare professionals and resulting feelings of safety.
Conclusion: In general patients with chronic immune system disorders tend to be more likely to choose SC administration than IV infusion, but preferences may vary according among individuals. These findings may assist discussions around appropriate treatment choices for each patient.
Keywords: systematic literature review, decision making, preference, administration route, immunodeficiency, autoimmune disorders
Plain Language Summary
Patients’ individual preferences are an important factor in deciding which treatment to use. Many chronic immune system disorders – immunodeficiencies and autoimmune conditions – have several available treatments which can be administered by infusion into a vein (intravenously) or under the skin (subcutaneously). The most suitable treatment may vary for each patient, depending on their individual preferences and circumstances.
We conducted this systematic review of the published literature to provide an overview of studies describing patients’ preferences for intravenous or subcutaneous treatment. In total, we included 49 references. Of these, the majority found that patients preferred subcutaneous treatment, a major advantage of which was the possibility of treatment at home, which was seen as more convenient and comfortable than hospital treatment. Among patients who preferred intravenous infusions, the main advantages were the lower treatment frequency, the presence of healthcare professionals and the resulting feelings of safety. Many patients had experience of either intravenous or subcutaneous treatment, and tended to prefer their current treatment option.
By describing what is known about patients’ preferences for treatment administration route, and the reasons for those preferences, this review is intended to inform discussions about available treatments and help decide on the most appropriate choice of therapy for individual patients.
Introduction
For many chronic immune system disorders – immunodeficiencies and autoimmune conditions – treatments with multiple administration routes are available. For example, for patients with immunodeficiency and some autoimmune conditions, subcutaneous (SC) infusions of immunoglobulin (SCIg) may be used as an alternative to intravenous (IV) immunoglobulin (IVIg).1 Similarly, the tumor necrosis factor inhibitor (TNFi) class of therapies, widely used in the treatment of autoimmune conditions, includes both infliximab, administered as an IV infusion, and multiple agents which are administered by SC injection (eg adalimumab and etanercept).2
In situations where different therapies are expected to have generally similar efficacy and safety, patients’ individual preferences are an important factor in deciding which treatment to use. Matching treatment attributes to patients’ individual preferences has been associated with increased treatment satisfaction and adherence, and with improved health-related quality of life (HRQoL).3,4 Involvement of patients in treatment choices is also central to shared decision making approaches.5,6
In the case of SC formulations of therapies, one potential advantage is the possibility of patients administering their own treatment at home, without needing to depend on a healthcare provider for administration of the therapy. Home self-administration of treatment may be beneficial to patients, by improving convenience, and to healthcare systems, by reducing costs.7 The desire for patients and providers to minimize hospital exposure or in-person contact is especially relevant within the context of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic. It is possible that some preferences established during the pandemic will persist even when vaccination for the virus becomes widely available.
The objective of this systematic literature review (SLR) is to provide evidence to inform discussions about available treatments by summarizing the available literature regarding the preferences of patients with chronic immune system disorders for IV infusion, SC infusion or SC injection.
Methods
Data Sources and Search Strategy
Electronic database searches were conducted on 24 February 2021. The included databases were MEDLINE (via the US National Library of Medicine PubMed tool; pubmed.ncbi.nlm.nih.gov), Embase (via embase.com) and the Cochrane Library (via cochranelibrary.com). The searches were designed to capture all studies reporting patient preferences between subcutaneous and intravenous therapy. Search strings are shown in Supplementary Tables 1–3.
Screening
EndNote (Clarivate Analytics; Philadelphia, PA, USA) was used to combine search results and remove duplicates. For all citations identified in the electronic searches, titles and abstracts were screened by two reviewers (PMO and Claire Mulligan, Beacon Medical Communications Ltd, Brighton, UK) to assess the potential relevance of the study according to prespecified eligibility criteria. For potentially relevant citations, full-text articles were obtained and reviewed to confirm inclusion in the SLR. The reference lists of SLRs identified in the database searches were checked for potentially relevant references, which were included in the review.
Eligibility Criteria
Studies were eligible for inclusion in the SLR if they reported primary data on patients’ preferences for SC infusion or SC injection versus IV infusion of any therapy, or of hypothetical interventions. Studies were included if they described patient preferences for the treatment of chronic immune system disorders (Supplementary Table 4); other indications were excluded. Both pediatric and adult populations were included.
Relevant studies were limited to those in which the mode of administration, including treatment frequency and setting, was the main difference between comparators (ie comparisons between therapies with different efficacy or safety profiles were not included). For studies describing relevant patient preferences, preferences for treatment setting (home vs hospital) and reasons given by patients for preferring each mode of administration were also investigated.
All relevant study designs were included, and no date restriction was applied. Articles published in languages other than English were excluded, except where English-language abstracts contained relevant evidence. Relevant conference abstracts indexed in the databases were included unless the studies described were also published as journal articles.
Data Extraction and Analysis
For the included publications, data on patient preferences were extracted into predefined tables. Classification of SC administration as infusion or injection was based on the term used in the relevant publication. Where data were available for subgroups of patients currently using IV or SC therapies, these were extracted separately. Where reasons given by patients for preferring IV or SC administration, these were also extracted. Reasons for preferences were analyzed semi-quantitatively by grouping the reported reasons into categories and calculating the proportion of studies reporting preferences for IV or SC administration in which each category was mentioned as a main driver of preferences or reported by ≥ 20% of patients.
Risk of Bias Assessment
Risk of bias in the included studies was assessed using the McMaster University CLARITY group Risk of Bias Instrument for Cross-Sectional Surveys of Attitudes and Practices.8
Results
Study Selection
The study selection process is summarized in Figure 1. In total, 1719 citations were identified in the searches. After removal of 507 duplicates, 1212 citations were screened. Full-text versions of 56 articles, as well as 92 conference abstracts, were assessed for eligibility. Searching the bibliographies of seven identified SLRs9–13 identified eight additional relevant articles, which were included in the review. In total, 49 studies,14–62 comprising 38 full papers14–51 and 11 conference abstracts,52–62 were included in the review.
 |
Figure 1 Study selection flow chart.Abbreviations: PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; SLR, systematic literature review. |
Description of the Included Studies
Eighteen studies were identified that compared IV and SC infusion of immunoglobulin (IVIg or SCIg).14–28,52–54 Of these, four studies were randomized controlled trials (RCTs);14–17 six were non-randomized interventional studies;18–22,52 four were observational studies;23–25,53 and four were surveys.26–28,54 The indication in the majority of included studies of SCIg (13 studies in total) was immunodeficiency, mostly primary immunodeficiency (PID).14,15,18–20,23,24,26–28,52–54 The remaining studies comprised four studies of patients with multifocal motor neuropathy (MMN)16,21,22,25 and two studies of patients with chronic inflammatory demyelinating polyneuropathy (CIDP)17,25 (one study included both MMN and CIDP groups).25
The remaining 31 studies compared administration routes for a range of non-immunoglobulin therapies, and described preferences for IV infusion or SC injection.29–51,55–62 Of these, 29 studies were patient surveys,29–50,55–61 of which 22 were straightforward preference questionnaires29–47,55–57 and seven involved conjoint analyses or discrete choice experiments.48–50,58–61 The remaining studies were a non-randomized interventional study51 and a retrospective analysis of treatment choices.62
The most common indication in the included studies of non-immunoglobulin therapies was rheumatoid arthritis (RA; 11 studies).29–36,46,48,58 An additional ten studies involved patients with inflammatory bowel disease (IBD, comprising Crohn’s disease [CD], ulcerative colitis or a mixture of the two);37,38,45,47,49,55,57,59,61,62 two studies were conducted among patients with systemic lupus erythematosus (SLE);39,51 two among patients with severe asthma;40,41 and one each among patients with multiple sclerosis (MS),60 psoriasis50 and axial spondyloarthritis.56 Three studies included patients with a range of conditions (most commonly RA or IBD).42–44
Risk of Bias
The risk of bias assessment of the included studies is shown in Supplementary Table 5. Most studies had some risk of bias, mostly with regard to whether the included population was representative of the overall patient population.
Preferences for IVIg or SCIg
The 18 studies that compared IVIg with SCIg are described in Table 1,14–28,52–54 with overall preferences, where reported, summarized in Figure 2A.14–24,52–54 A single Phase 3 trial – PATH – was identified.17 In this study patients with CIDP using IVIg were randomized to one of two SCIg doses or placebo for 24 weeks. Among the 85 patients treated with SCIg who completed a preference questionnaire at the end of the study, 61 (72%) preferred SCIg, 21 (25%) preferred IVIg and 3 (4%) had no preference.17 A total of three randomized crossover studies were identified.14–16 In two of these, the majority of patients (56% and 91%) who had used IVIg and SCIg during the study reported preferring SCIg;14,16 in the third study, 5 of 10 and 11 of 20 patients in cohorts in the UK and Sweden, respectively, preferred IVIg therapy.15
 | 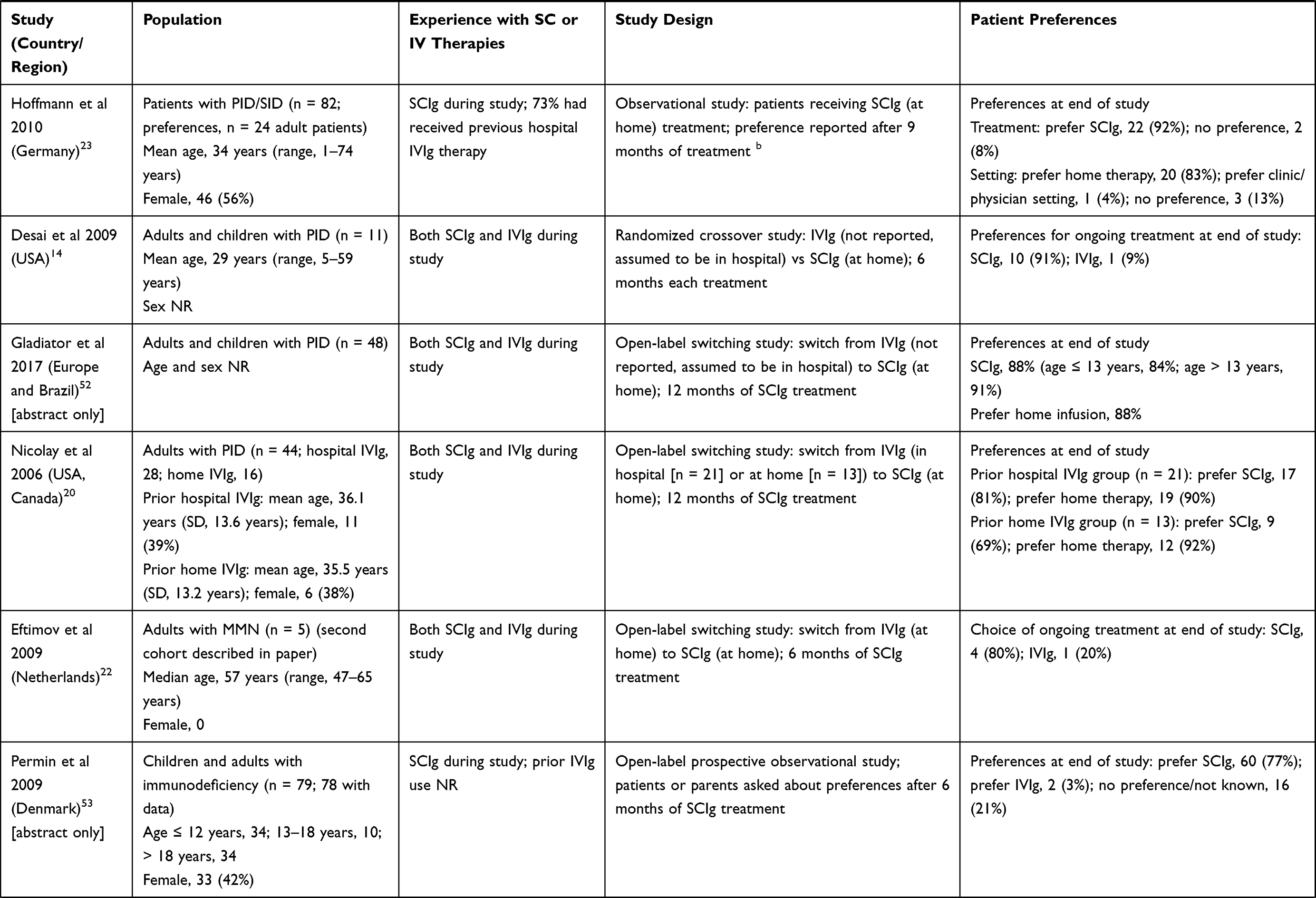 | 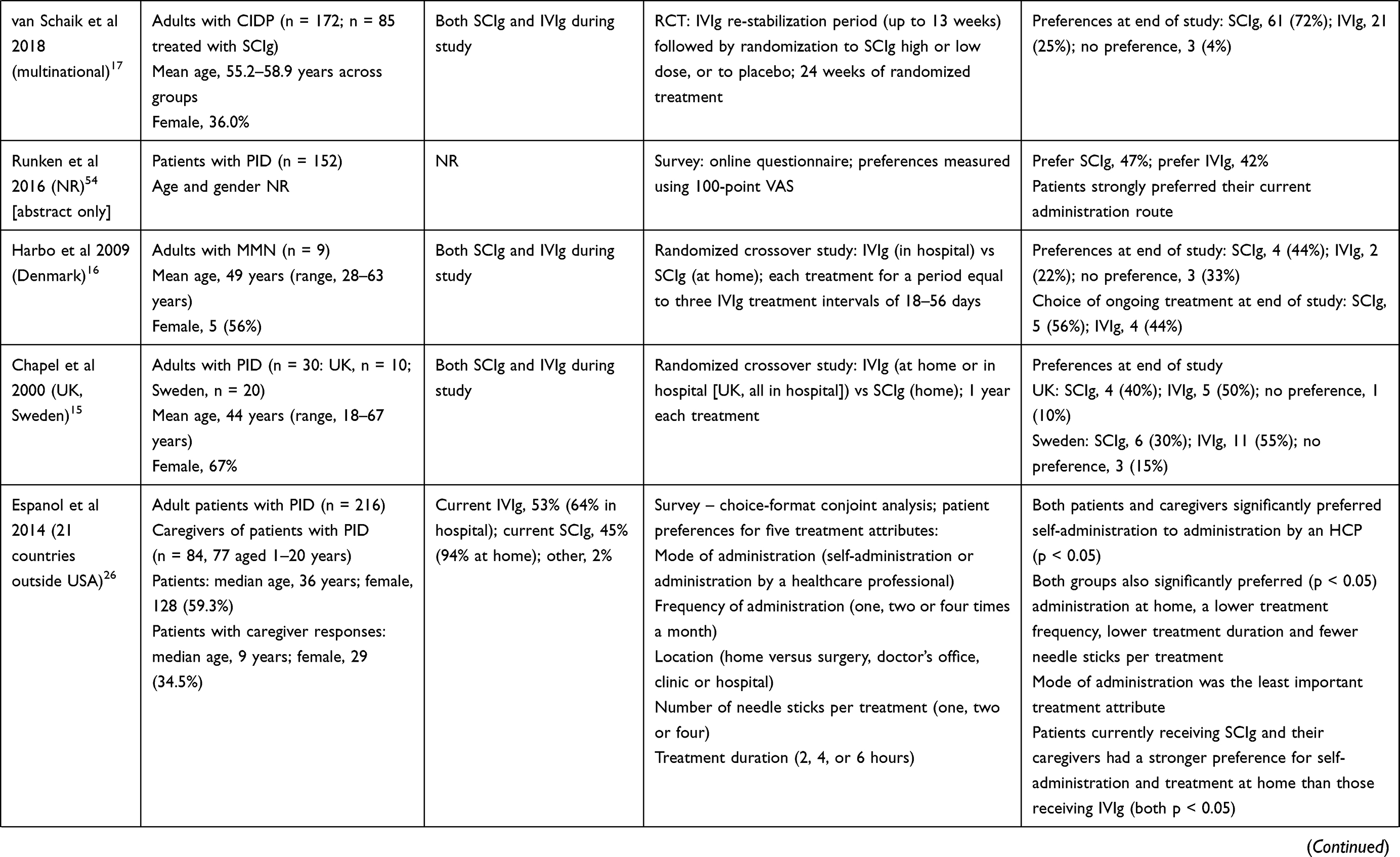 |  |
Table 1 Summary of Included Studies Comparing IV Infusion to SC Infusion |
 |
Figure 2 Summary of patient preferences for (A) IVIg or SCIg and (B) IV infusion or SC injection of non-immunoglobulin therapies. Data are patients’ expressed preferences or actual treatment choices (shown in italics). Eight studies in which percentage preferences were not reported were excluded.25–28,48–50,58 In some studies not all patients expressed a preference, or preferences were not reported for one alternative; therefore, not all lines add up to 100%. |
Six open-label interventional studies of patients switching from IVIg to SCIg were included.18–22,52 These studies were typically small (range, n = 5 to n = 48), and comprised two studies of adult patients with MMN21,22 and four studies of adults or children with PID.18–20,52 In all seven studies, most patients (76–100%) preferred SCIg therapy.18–22,52 Preferences among patients switching from IVIg to SCIg were also investigated in two small observational studies, conducted in the UK (n = 8) and Germany (n = 24).23,25 Both of these studies found strong preferences for SCIg, measured using visual analog scale scores in the UK study25 and directly elicited preferences in the Germany study, in which 22 of 24 patients preferred SCIg.23
A Canadian observational study followed therapy choices made by children with PID (n = 143).24 Among patients already on IVIg who were offered a choice of treatment, 50 of 51 chose to switch to SCIg, and 44 were still on SCIg after an average follow-up period of 52 months.24 Of 92 newly diagnosed patients offered a choice between IVIg and SCIg, 44 initially chose SCIg; of these, 42 were still on SCIg after an average of 33 months of follow-up. By contrast, of the 48 newly diagnosed patients who chose IVIg, 35 switched to SCIg during the follow-up period.24 A further observational study, conducted in Denmark, found that of 78 children and adults with immunodeficiency who used SCIg for 6 months, 77% reported preferring SCIg at the end of the study, compared with 3% who preferred IVIg.53
Two similar conjoint analyses investigated patient preferences for multiple attributes of immunoglobulin treatment. In both a US study and an international cohort, adult patients and parents of children with PID significantly preferred self-administration of SCIg to IVIg administered by a healthcare professional (p < 0.05 for all groups except US patients).26,27 By contrast, a Canadian survey of 91 patients receiving hospital IVIg treatment found that although the majority would be willing to switch to home IVIg or home SCIg, respectively, after consulting with their immunologist, participants were significantly more likely to switch to home IVIg than home SCIg (p = 0.01).28 A further survey of patients with PID found a small overall preference for SCIg over IVIg (47% vs 42%).54
Preferences for IV Infusion or SC Injection of Non-Immunoglobulin Therapies
The 31 studies that compared IV infusion or SC injection of therapies other than immunoglobulin are summarized in Table 229–47,51,55–57,59,61,62 and, where overall preferences were reported, in Figure 2B.29–47,51,55–57,59,61,62 Two clinical studies of patient preferences for IV infusion compared with SC injection were identified.51,62 The first was an open-label switching study, conducted in the USA, in which patients with SLE treated with IV infusions of belimumab (n = 43) switched to SC belimumab, administered using an autoinjector.51 After 8 weeks of treatment, 32 of 42 patients (76%) expressed a preference for the autoinjector over IV administration.51 The second was a retrospective analysis of treatment choices made by children with CD and their families when initiating TNFi therapy (n = 37).62 Most chose SC adalimumab (89%), with 11% opting for IV infliximab.62
 |  |  |  |  |  |  |
Table 2 Summary of Included Studies Comparing IV Administration to SC Injection |
Among the 23 surveys of preferences for IV infusion or SC injection, 12 studies enrolled patients with RA, or populations in which most patients had RA.29–36,42,46,48,58 Of these, eight studies found that more patients preferred SC injection than preferred IV administration.29–33,46,48,58 IV infusion was preferred to SC injection in two studies,34,42 while two studies reported an even split of preferences.35,36
Ten studies enrolled patients with IBD.37,38,45,47,49,55,57,59,61,62 The results of these studies were mixed, with five reporting that patients preferred SC injection,38,45,57,59,61,62 three describing an overall preference for IV infusion37,45,55 and two finding similar preferences for the two options.47,49
Both of the included surveys of patients with severe asthma found strong preferences for SC injection over IV infusion, with 81.3% and 100% of patients preferring the SC administration route.40,41
A discrete choice experiment survey conducted among patients with psoriasis found that patients preferred SC injections to IV infusions (p = 0.014); this preference was significant only for patients with mild disease (p = 0.005) and not for those with moderate or severe disease (p = 0.477).50 An Italian survey of patients with SLE (n = 548) and an Argentinian survey of patients with axial spondyloarthritis (n = 70) also found a preference for SC injection over IV infusion (41.2% vs 36.9% and 41% vs 3%, respectively).39,56 A further two surveys, of patients with MS and of patients with a range of autoimmune conditions, both found that patients preferred IV administration to SC injections.43,60 The final study, conducted among patients using TNFi therapies, found an overall preference for SC injections.44
Preferences According to Current Therapy
Nine studies described preferences among patients naïve to IV or SC therapies. Of these, five studies found patients to prefer SC injection,29,33,38,46,47,62 two found patients to prefer IV infusion,42,55 and two found similar preferences for the two administration routes.35,47
A total of 23 studies described preferences among patients currently using IV or SC therapies. Of these, nine studies assessed preferences among patients currently using SCIg (seven studies),17–22,52 those currently using IVIg (one study),24 or a mixture (one study).54 All seven studies of current SCIg users or patients who had switched from IVIg to SCIg as part of the study found that the majority (69–100%) of patients preferred the SCIg route.17–22,52 In another study, patients already on IVIg were offered a choice between staying on IVIg and switching to SCIg: 50 of 51 patients chose to switch.24 The final study, conducted in a mixed population of SCIg and IVIg use, reported that patients strongly preferred their current administration route.54
Of 14 reports of preferences for IV infusion or SC injection among current users of relevant non-immunoglobulin therapies, 13 found that patients preferred their current treatment.30–34,41–44,57 Seven studies reported that patients receiving treatment by IV infusion preferred the IV administration route.31–34,42–44 Similarly, in six studies patients using SC therapies expressed a preference for that option.31–33,41,44,57 The exceptions were two surveys, conducted in France and Portugal.30,57 In the French study, 54.2% of 201 patients with RA using IV biologics expressed a preference to switch to SC injections.30 Similarly, in the Portuguese survey, 11 of 21 patients with CD using IV infliximab reported preferring to change to SC adalimumab.57
Patient Preferences for Frequency and Setting Separate from Those for Administration Route
Only nine of the included studies separated preferences for treatment at home versus in hospital from choices about administration route.19,20,23,35,40,44,50,59 Four studies reported that patients separately preferred SCIg over IVIg, and home treatment over hospital administration.19,20,23,56 A further study found that among patients with CD who preferred SC injection over IV infusion, the majority (68.7%) preferred home treatment over hospital administration.59 By contrast, two surveys, which investigated multiple aspects of treatment for psoriasis and severe asthma, found patients to prefer SC injection over IV infusion, and also to prefer administration by a healthcare professional in a clinical setting.40,50 Two final studies found that patient preferences varied between those currently using or preferring SC TNFi therapies, who preferred home administration, and those receiving or preferring IV TNFi agents, who preferred hospital treatment.35,44 In two studies, a minority of patients (18% and 44%) preferring SC injections indicated that they would prefer the injections to be performed by a nurse.30,33
All ten studies that separately assessed preferences for administration route from those for treatment frequency found patients to prefer less frequent treatment options.26,27,29,33,36,40,48,50,60,61
Reasons for Treatment Preferences
A total of 16 studies reported patients’ main reasons for preferring particular administration routes (Table 3 and Figure 3).17,28,30,33,35,37,39,41,43,45–47,52,54–56 The main reasons given by patients for preferring IV infusion were the lower frequency of IV infusions compared with SC administration, the presence of healthcare professionals and resulting feelings of safety, and a dislike of self-injecting. By contrast, patients preferring SC treatment cited the convenience and comfort of home treatment and the avoidance of having to attend hospital, as well as the reduced time requirement and greater independence associated with SC administration.
 |
Table 3 Reported Reasons for Preferences |
 |
Figure 3 Summary of reported reasons for preferring SC or IV administration. Data are the proportion of studies reporting preferences for SC or IV administration (n = 14 and n = 13, respectively) in which each category was mentioned as a main driver of preferences or reported by ≥ 20% of patients. |
Discussion
This SLR identified 49 studies that described patient preferences for IV or SC administration of treatments for chronic immune system disorders. The included studies covered a range of indications and comparisons between both IVIg and SCIg, and IV infusion and SC injection of non-immunoglobulin therapies. Overall, the literature suggests that patients with chronic immune system disorders are more likely to choose SC administration over IV infusion, although the results of individual studies varied. Preferences toward SC administration were most consistent in the studies comparing methods of immunoglobulin administration (ie IVIg vs SCIg). These observations speak to the importance of developing and maintaining a diverse suite of treatment options for patients, such that the unique preferences of any individual patient can be accommodated. Patients who favored IV infusions frequently cited the relative infrequency of treatment and feelings of safety due to hospital administration as desirable attributes. By contrast, patients preferring SC therapies tended to like the convenience and independence associated with self-injection at home.
No clear trends were identified according to indication, including whether the disease in question might be expected to affect patients’ ability to self-inject. The most common indication in the included studies was immunodeficiency (mostly PID), for which 11 of 13 studies found an overall preference for SCIg over IVIg.14,15,18–20,23,24,26–28,52–54 This is consistent with studies of patients with arthritis (in nine of 11 studies reporting an overall preference this was in favor of SC administration),29–34,42,46,48,56,58 asthma40,41 and SLE39,51 (for both two of two studies favored SC administration). The preference toward SC therapies was slightly weaker in studies of patients with IBD, but an overall preference for SC treatment was still seen in the majority of studies (5 of 8 studies reporting an overall preference).37,38,45,55,57,59,61,62
Preference toward SC therapies was seen in studies of both adult and pediatric populations. Notably, all of the seven studies of preferences in specific populations of children found an overall preference for SC therapies.18,19,24,26,27,53,62 Of these, six studies compared IVIg and SCIg for the treatment of PID.18,19,24,26,27,53 The final study reviewed treatment choices among children with CD (or their families).62 Interestingly, while 89% of the group offered a choice (n = 37) opted for SC adalimumab over IV infliximab, 72% of those in a parallel group (n = 29) who were not given a choice were treated with IV infliximab. This highlights the potential for treatment preferences to differ between patients and physicians, which may have implications for treatment satisfaction and HRQoL.62
There was a clear tendency for patients to prefer their current treatment administration route over administration routes with which they did not have experience. The exceptions to this were two studies that found patients currently using IV therapies would prefer to switch to SC alternatives.24,30 One of these studies, reported by Samaan et al, illustrates the importance of experience in patients’ decision making.24 A group of IVIg-experienced children strongly preferred to switch to SCIg, and most (88%) remained on SCIg after an average follow-up period of 52 months. By contrast, when a further cohort of children, newly diagnosed with PID and naïve to immunoglobulin replacement therapy, were offered a free choice of IV or SC administration, approximately half selected each administration route. However, by the end of an average of 33 months’ follow-up, 80% were using SCIg.24 Consistent with these observations, preferences expressed by patients as part of clinical studies tended to favor SC administration more strongly than the results of surveys. This difference may reflect many survey respondents not having experience of self-injecting or administering treatment at home. For these patients, training in the use of self-administered therapies is important, as are homecare support structures and patients having sufficient information to make informed treatment choices.
It remains challenging to compare patients’ preferences between IV and SC administration, given there are differences in treatment setting and frequency as well as in route, and the relative importance of different aspects may vary among patients. For example, some patients might consider treatment twice-weekly by SC injection to be too frequent, even though in principle they prefer SC administration to IV infusion. There were only limited data in the literature on preferences for treatment administration route separate from treatment setting. Where such data were identified they were consistent with patients preferring SC administration to take place at home, and IV administration to take place in hospital, with the exception of two studies in which both SC injection and administration by a healthcare professional in a clinic were preferred.40,50 Many of the reasons patients gave for preferring IV treatment were related to receiving treatment in hospital, while many of the reasons given for preferring SC administration were related to receiving treatment at home. It is possible that some patients’ preferences for hospital versus home treatment may change following the SARS-Cov-2 pandemic. During the pandemic, home treatment (including immunoglobulin replacement for myasthenia gravis)63 and remote consultations64,65 were widely used in place of hospital visits; in the case of remote consultations, two surveys have suggested that around half of patients would be open to continuing with this approach at least some of the time.64,65
The findings of this review are consistent with previously published SLRs, most of which focused on specific patient groups. SLRs reported by Jones et al and Abolhassani et al found preferences for SCIg over IVIg among patients with primary immunodeficiency.9,12 A recent SLR of patient preferences for RA treatments, described by Durand et al, included five studies that compared SC injection with IV infusion;10 in four of the five, patients preferred SC administration.10 As in this review, patients’ preferences tended to reflect their current treatment route.10 In addition, a more general SLR reported by Stoner et al found patients in four of the six studies preferred SC therapy over IV administration.13
In addition to managing patients’ clinical condition, a major goal of treatment is to improve patients’ HRQoL. A recent study has shown that, over an entire population of patients with PID, IVIg and SCIg use are associated with similar HRQoL.68 Personal preferences may therefore be an important part of matching each patient to the more appropriate therapy, potentially maximizing HRQoL for each individual. Inconvenience, travel and a lack of flexibility are frequently cited as reasons for preferring home treatment to hospital IV therapy,30,33,69 suggesting that patients’ work schedules, or distance from hospital, may play a part. Conversely, patients preferring hospital IV therapy frequently describe feelings of safety with hospital treatment, underlining the importance of psychological factors.33 Patients’ individual preferences may also be influenced by other clinical factors. For example, a recent survey of patients with SLE found that use of non-steroidal anti-inflammatory drugs was associated with an increased likelihood of choosing SC injection over IV infusion.70 Understanding how other aspects of patients’ treatment may affect the choice of the most appropriate therapy for each patient may be important for maximizing HRQoL.
This review has several limitations. First, all of the studies comparing IV infusion to SC infusion assessed preferences for IVIg versus SCIg; no data were identified comparing SC infusion of other therapies with IV alternatives. Second, the comparison between IV infusion and SC injection covers a range of different treatments and indications, but all except two of the included studies were surveys, and the evidence from clinical studies is limited. Third, no studies comparing SC infusion and SC injection were identified, although this reflects the lack of therapies that might potentially be administered by both of those routes. Fourth, the included evidence was limited to studies published in English; although no citations were excluded on the basis of language (for one study published in German, data were extracted only from the English-language abstract), the possibility of additional relevant literature published in other languages cannot be excluded. Fifth, the review was limited to chronic immune system disorders; accordingly, evidence from recent studies of IV and SC versions of several oncology therapies was therefore excluded. This focus was chosen because patient preferences for oncology therapies, which are taken for a limited period of time, typically in the context of multiple hospital visits, were considered not to be readily comparable with those for treatments for chronic disorders. Sixth, the multitude of variables that contribute to patients’ preferences cannot be accounted for in this review. For example, SC infusion by automated pump has been shown to be preferred to rapid push administration using a syringe.71 As the individual characteristics of the IV, SC infusion, and SC injection administration routes evolve, so too may patient preferences. Seventh, many of the results come from clinical trial data. Patients entering a clinical trial may have an inherent bias toward preference for a study medication that cannot be extrapolated to routine clinical care. Eighth, several recent studies have investigated the relative efficacy and safety of SC and IV therapies.66,67 Although not the focus of this SLR, differences in efficacy or safety would be expected to influence patients’ preferences for particular treatment options. Ninth, many of the included studies were not designed to assess preferences among patients who were necessarily representative of the overall patient populations, and most had some risk of bias. Caution should therefore be taken when extrapolating from these results to other patient groups; however, given the similarity of findings across indications a systematic bias toward preferences for one administration route or another can be considered to be unlikely.
Conclusion
The goal of treatment for chronic immune system disorders is to improve patients’ disease state, functionality and HRQoL. It is important that the method of treatment administration does not add to the burden of their disease, which in many cases can be substantial. Overall, while there is some variability among individual studies, patients with chronic immune system disorders – particularly those using immunoglobulin therapy – tend to be more likely to choose SC administration than IV infusion. Patients tend to prefer their existing therapy, and some choices may reflect lack of experience of alternatives. Many patients may therefore benefit from training and support structures, and from being provided with the information they need to make informed decisions. Patients’ choices appear to reflect the frequency and setting of treatment options as much as differences in administration route – the relative importance of the lower frequency of IV infusions and the convenience of home SC administration may vary among patients. The results of this SLR may help inform discussions about the available treatments, and decisions as to the most appropriate choice of therapy for individual patients.
Acknowledgments
This study was funded by UCB Pharma. The authors acknowledge Veronica Porkess of UCB Pharma, for publication and editorial support, and Claire Mulligan of Beacon Medical Communications Ltd, for systematic review screening.
Disclosure
Jeffrey Allen has acted as a consultant for Argenx, Akcea Therapeutics, CSL Behring and Grifols. He has also received grants from CSL Behring, personal fees from Grifols, and personal fees from Argenx, outside the submitted work. Paul Overton is a director of Beacon Medical Communications Ltd, which received funding for this project from UCB Pharma, and additional project funding from UCB Pharma, outside the submitted work. He also received personal fees from Beacon Medical Communications Ltd, during the conduct of the study. Natalie Shalet is a director of NAS HealthCare solutions Ltd, which provided consultancy services to UCB Pharma during this project. Fabian Somers is an employee of UCB Pharma. The authors report no other conflicts of interest in this work.
References
1. Perez EE, Orange JS, Bonilla F, et al. Update on the use of immunoglobulin in human disease: a review of evidence. J Allergy Clin Immunol. 2017;139(3s):S1–S46.
2. Mantravadi S, Ogdie A, Kraft WK. Tumor necrosis factor inhibitors in psoriatic arthritis. Expert Rev Clin Pharmacol. 2017;10(8):899–910. doi:10.1080/17512433.2017.1329009
3. Schwartzman S, Morgan GJ
4. Wilson SR, Strub P, Buist AS, et al. Shared treatment decision making improves adherence and outcomes in poorly controlled asthma. Am J Respir Crit Care Med. 2010;181(6):566–577. doi:10.1164/rccm.200906-0907OC
5. Kennedy T, McCabe C, Struthers G, et al. BSR guidelines on standards of care for persons with rheumatoid arthritis. Rheumatology. 2005;44(4):553–556. doi:10.1093/rheumatology/keh554
6. Strohal R, Prinz JC, Girolomoni G, Nast A. A patient-centred approach to biological treatment decision making for psoriasis: an expert consensus. J Eur Acad Dermatol Venereol. 2015;29(12):2390–2398. doi:10.1111/jdv.13248
7. Fu LW, Song C, Isaranuwatchai W, Betschel S. Home-based subcutaneous immunoglobulin therapy vs hospital-based intravenous immunoglobulin therapy: a prospective economic analysis. Ann Allergy Asthma Immunol. 2018;120(2):195–199. doi:10.1016/j.anai.2017.11.002
8. Agarwal A, Guyatt G, Busse J. Risk of bias instrument for cross-sectional surveys of attitudes and practices. 2017; Available from: https://www.evidencepartners.com/resources/methodological-resources/risk-of-bias-cross-sectional-surveys-of-attitudes-and-practices/.
9. Abolhassani H, Sadaghiani MS, Aghamohammadi A, Ochs HD, Rezaei N. Home-based subcutaneous immunoglobulin versus hospital-based intravenous immunoglobulin in treatment of primary antibody deficiencies: systematic review and meta analysis. J Clin Immunol. 2012;32(6):1180–1192. doi:10.1007/s10875-012-9720-1
10. Durand C, Eldoma M, Marshall DA, Bansback N, Hazlewood GS. Patient preferences for disease-modifying antirheumatic drug treatment in rheumatoid arthritis: a systematic review. J Rheumatol. 2020;47(2):176–187. doi:10.3899/jrheum.181165
11. Health Quality Ontario. Home-based subcutaneous infusion of immunoglobulin for primary and secondary immunodeficiencies: a health technology assessment. Ont Health Technol Assess Ser. 2017;17(16):1–86.
12. Jones GL, Vogt KS, Chambers D, Clowes M, Shrimpton A. What is the burden of immunoglobulin replacement therapy in adult patients with primary immunodeficiencies? A systematic review. Front Immunol. 2018;9:1308. doi:10.3389/fimmu.2018.01308
13. Stoner KL, Harder H, Fallowfield LJ, Jenkins VA. Intravenous versus subcutaneous drug administration. Which do patients prefer? A systematic review. Patient. 2014. doi:10.1007/s40271-014-0075-y
14. Desai SH, Chouksey A, Poll J, Berger M. A pilot study of equal doses of 10% IGIV given intravenously or subcutaneously. J Allergy Clin Immunol. 2009;124(4):854–856. doi:10.1016/j.jaci.2009.07.051
15. Chapel HM, Spickett GP, Ericson D, Engl W, Eibl MM, Bjorkander J. The comparison of the efficacy and safety of intravenous versus subcutaneous immunoglobulin replacement therapy. J Clin Immunol. 2000;20(2):94–100. doi:10.1023/A:1006678312925
16. Harbo T, Andersen H, Hess A, Hansen K, Sindrup SH, Jakobsen J. Subcutaneous versus intravenous immunoglobulin in multifocal motor neuropathy: a randomized, single-blinded cross-over trial. Eur J Neurol. 2009;16(5):631–638. doi:10.1111/j.1468-1331.2009.02568.x
17. van Schaik IN, Bril V, van Geloven N, et al. Subcutaneous immunoglobulin for maintenance treatment in chronic inflammatory demyelinating polyneuropathy (PATH): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Neurol. 2018;17(1):35–46. doi:10.1016/S1474-4422(17)30378-2
18. Fasth A, Nystrom J. Safety and efficacy of subcutaneous human immunoglobulin in children with primary immunodeficiency. Acta Paediatr. 2007;96(10):1474–1478. doi:10.1111/j.1651-2227.2007.00485.x
19. Gardulf A, Nicolay U, Math D, et al. Children and adults with primary antibody deficiencies gain quality of life by subcutaneous IgG self-infusions at home. J Allergy Clin Immunol. 2004;114(4):936–942. doi:10.1016/j.jaci.2004.06.053
20. Nicolay U, Kiessling P, Berger M, et al. Health-related quality of life and treatment satisfaction in North American patients with primary immunedeficiency diseases receiving subcutaneous IgG self-infusions at home. J Clin Immunol. 2006;26(1):65–72. doi:10.1007/s10875-006-8905-x
21. Misbah SA, Baumann A, Fazio R, et al. A smooth transition protocol for patients with multifocal motor neuropathy going from intravenous to subcutaneous immunoglobulin therapy: an open-label proof-of-concept study. J Peripher Nerv Syst. 2011;16(2):92–97. doi:10.1111/j.1529-8027.2011.00330.x
22. Eftimov F, Vermeulen M, de Haan RJ, van den Berg LH, van Schaik IN. Subcutaneous immunoglobulin therapy for multifocal motor neuropathy. J Peripher Nerv Syst. 2009;14(2):93–100. doi:10.1111/j.1529-8027.2009.00218.x
23. Hoffmann F, Grimbacher B, Thiel J, Peter HH, Belohradsky BH, Vivaglobin Study G. Home-based subcutaneous immunoglobulin G replacement therapy under real-life conditions in children and adults with antibody deficiency. Eur J Med Res. 2010;15(6):238–245. doi:10.1186/2047-783X-15-6-238
24. Samaan K, Levasseur MC, Decaluwe H, et al. SCIg vs. IVIg: let’s give patients the choice! J Clin Immunol. 2014;34(6):611–614. doi:10.1007/s10875-014-0057-9
25. Hadden RD, Marreno F. Switch from intravenous to subcutaneous immunoglobulin in CIDP and MMN: improved tolerability and patient satisfaction. Ther Adv Neurol Disord. 2015;8(1):14–19. doi:10.1177/1756285614563056
26. Espanol T, Prevot J, Drabwell J, Sondhi S, Olding L. Improving current immunoglobulin therapy for patients with primary immunodeficiency: quality of life and views on treatment. Patient Prefer Adherence. 2014;8:621–629. doi:10.2147/PPA.S60771
27. Mohamed AF, Kilambi V, Luo MP, Iyer RG, Li-McLeod JM. Patient and parent preferences for immunoglobulin treatments: a conjoint analysis. J Med Econ. 2012;15(6):1183–1191. doi:10.3111/13696998.2012.716804
28. Reid B, Pires L. Home gammaglobulin therapy: a patient survey of intravenous and subcutaneous options in Canada. LymphoSign J. 2014;1(1):27–37. doi:10.14785/lpsn-2014-0001
29. Bolge SC, Goren A, Brown D, Ginsberg S, Allen I. Openness to and preference for attributes of biologic therapy prior to initiation among patients with rheumatoid arthritis: patient and rheumatologist perspectives and implications for decision making. Patient Prefer Adherence. 2016;10:1079–1090. doi:10.2147/PPA.S107790
30. Desplats M, Pascart T, Jelin G, et al. Are abatacept and tocilizumab intravenous users willing to switch for the subcutaneous route of administration? A questionnaire-based study. Clin Rheumatol. 2017;36(6):1395–1400. doi:10.1007/s10067-017-3587-8
31. Edel Y, Sagy I, Pokroy-Shapira E, et al. A cross-sectional survey on the preference of patients with rheumatoid arthritis for route of administration of disease-modifying anti-rheumatic drugs: oral target-specific versus parenteral biologic. Isr Med Assoc J. 2020;22(3):154–159.
32. Emadi SA, Hammoudeh M, Mounir M, Mueller RB, Wells AF, Sarakbi HA. An assessment of the current treatment landscape for rheumatology patients in Qatar: recognising unmet needs and moving towards solutions. J Int Med Res. 2017;45(2):733–743. doi:10.1177/0300060516686872
33. Huynh TK, Ostergaard A, Egsmose C, Madsen OR. Preferences of patients and health professionals for route and frequency of administration of biologic agents in the treatment of rheumatoid arthritis. Patient Prefer Adherence. 2014;8:93–99. doi:10.2147/PPA.S55156
34. Willeke P, Becker H, Wassenberg S, Pavenstädt H, Jacobi AM. Patient/rheumatologist evaluation of infusion treatment for rheumatoid arthritis. Z Rheumatol. 2011;70(3):232–238. doi:10.1007/s00393-011-0752-3
35. Scarpato S, Antivalle M, Favalli EG, et al. Patient preferences in the choice of anti-TNF therapies in rheumatoid arthritis. Results from a questionnaire survey (RIVIERA study). Rheumatology. 2010;49(2):289–294. doi:10.1093/rheumatology/kep354
36. Tłustochowicz M, Tłustochowicz W. Patients’ preferences regarding biological treatment in doctors’ and patients’ opinions-the results of the RAISE questionnaire survey. Reumatologia. 2013;51(2):113–118. doi:10.5114/reum.2013.34819
37. Cha JM, Park DI, Park SH, Shin JE, Kim WS, Yang SK. Physicians should provide shared decision-making for anti-TNF therapy to inflammatory bowel disease patients. J Korean Med Sci. 2017;32(1):85–94. doi:10.3346/jkms.2017.32.1.85
38. Kariburyo MF, Xie L, Teeple A, Tan H, Ingham M. Predicting pre-emptive discussions of biologic treatment: results from an openness and preference survey of inflammatory bowel disease patients and their prescribers. Adv Ther. 2017;34(6):1398–1410. doi:10.1007/s12325-017-0545-4
39. Falanga M, Canzona A, Mazzoni D. Preference for subcutaneous injection or intravenous infusion of biological therapy among Italian patients with SLE. J Patient Exp. 2019;6(1):41–45. doi:10.1177/2374373518770811
40. Gelhorn HL, Balantac Z, Ambrose CS, Chung YN, Stone B. Patient and physician preferences for attributes of biologic medications for severe asthma. Patient Prefer Adherence. 2019;13:1253–1268. doi:10.2147/PPA.S198953
41. Santus P, Ferrando M, Baiardini I, Radovanovic D, Fattori A, Braido F. Patients beliefs on intravenous and subcutaneous routes of administration of biologics for severe asthma treatment: a cross-sectional observational survey study. World Allergy Organ J. 2019;12(4):100030. doi:10.1016/j.waojou.2019.100030
42. Grisanti L, Kwiatkowski A, Dyrda P, et al. Patient perspectives on intravenous biologics for rheumatologic disease. Arthritis Care Res. 2019;71(9):1234–1242. doi:10.1002/acr.23758
43. Bolge SC, Eldridge HM, Lofland JH, Ravin C, Hart PJ, Ingham MP. Patient experience with intravenous biologic therapies for ankylosing spondylitis, crohn’s disease, psoriatic arthritis, psoriasis, rheumatoid arthritis, and ulcerative colitis. Patient Prefer Adherence. 2017;11:661–669. doi:10.2147/PPA.S121032
44. Sylwestrzak G, Liu J, Stephenson JJ, Ruggieri AP, DeVries A. Considering patient preferences when selecting anti-tumor necrosis factor therapeutic options. Am Health Drug Benefits. 2014;7(2):71–81.
45. Allen PB, Lindsay H, Tham TC. How do patients with inflammatory bowel disease want their biological therapy administered? BMC Gastroenterol. 2010;10:1. doi:10.1186/1471-230X-10-1
46. Chilton F, Collett RA. Treatment choices, preferences and decision-making by patients with rheumatoid arthritis. Musculoskeletal Care. 2008;6(1):1–14. doi:10.1002/msc.110
47. Wu AA, Barros JR, Ramdeen M, Baima JP, Saad-Hossne R, Sassaki LY. Factors associated with patient´s preference in choosing their therapy for inflammatory bowel disease in Brazil. Arq Gastroenterol. 2020;57(4):491–497. doi:10.1590/s0004-2803.202000000-86
48. Louder AM, Singh A, Saverno K, et al. Patient preferences regarding rheumatoid arthritis therapies: a conjoint analysis. Am Health Drug Benefits. 2016;9(2):84–93.
49. Boeri M, Myers K, Ervin C, et al. Patient and physician preferences for ulcerative colitis treatments in the United States. Clin Exp Gastroenterol. 2019;12:263–278. doi:10.2147/CEG.S206970
50. Bolt T, Kobayashi H, Mahlich J. Patient and physician preferences for therapy characteristics for psoriasis: a discrete choice experiment in Japan. Pharmacoecon Open. 2019;3(2):255–264. doi:10.1007/s41669-018-0104-1
51. Dashiell-Aje E, Harding G, Pascoe K, DeVries J, Berry P, Ramachandran S. Patient evaluation of satisfaction and outcomes with an autoinjector for self-administration of subcutaneous belimumab in patients with systemic lupus erythematosus. Patient. 2018;11(1):119–129. doi:10.1007/s40271-017-0276-2
52. Gladiator A, Meckley L, Berner T, Engl W, Ito D, Yel L. Treatment preference on the new subcutaneous immunoglobulin 20% (SCIG 20%) treatment in patients with Primary Immunodeficiency Diseases (PID) in Europe (EU). Swiss Med Wkly. 2017;147:57S.
53. Permin H, Herlin T, Gajek H, Mattauch M, Gustafson R. Safety profile of subcuvia from post-authorisation safety surveillance (PASS). Eur J Immunol. 2009;39:S454–S455.
54. Runken MC, Wasserman D, Gelinas D. Patient and physician beliefs regarding immunoglobulin therapy route of administration. J Clin Immunol. 2016;36(3):245.
55. Nagahori M, Saitoh E, Morio J, Fujii T, Naganuma M, Watanabe M. Patient preferences in the choice of anti-TNF treatments in inflammatory bowel diseases: a questionnaire survey at an academic IBD center in Japan. Inflamm Bowel Dis. 2011;17:S32–S33. doi:10.1097/00054725-201112002-00103
56. Capelusnik D, Schneeberger E, Oviedo LLM, Gutierrez JMS, Citera G. Treatment preferences in patients with axial spondyloarthritis. Arthritis Rheumatol. 2019;71:3983–3984.
57. Fernandes C, Pais T, Ribeiro I, et al. Satisfaction and concerns about anti-TNF alpha therapy in crohn’s disease-the patient’s perspective in a Portuguese population. J Crohns Colitis. 2014;8:S213. doi:10.1016/S1873-9946(14)60474-8
58. Husni ME, Griffith J, Betts K, Song Y, Ganguli A. Thresholds of benefit-risk trade-offs from the patient perspective for treatment decisions in moderate-to-severe rheumatoid arthritis. Arthritis Rheumatol. 2016;68:3338–3340.
59. Borruel N, Riestra S, Castro J, et al. Attributes of anti-TNF treatment that impact on preferences of patients with crohn’s disease candidates for biological treatment (IMPLICA Study). J Crohns Colitis. 2015;9:S120.
60. Adlard NE, Panpurina A, Patel VJ, Khurana V, Medin J, Kubara A. Patient preferences for different modes and frequency of administration of multiple sclerosis disease modifying therapies. Value Health. 2018;21:S351. doi:10.1016/j.jval.2018.09.2096
61. Van Deen WK, Khalil C, Almario C, et al. Patients’ preferences for subcutaneous or intravenous administration methods in inflammatory bowel diseases. Am J Gastroenterol. 2020;115(SUPPL):S417.
62. Pérez JG, Muncunill GP, Osorio JM, Cuerva BG, Miravet VV, De Carpi JM. Shared decision making in the choice of anti-TNF alpha in pediatric Crohn's disease. J Pediatr Gastroenterol Nutr. 2017;65:S54–S55.
63. Solé G, Salort-Campana E, Pereon Y, et al. Guidance for the care of neuromuscular patients during the COVID-19 pandemic outbreak from the French rare health care for neuromuscular diseases network. Rev Neurol (Paris). 2020;176(6):507–515. doi:10.1016/j.neurol.2020.04.004
64. Conde Blanco E, Manzanares I, Centeno M, et al. Epilepsy and lockdown: a survey of patients normally attending a Spanish centre. Acta Neurol Scand. 2021;143(2):206–209.
65. Gilbert AW, Billany JCT, Adam R, et al. Rapid implementation of virtual clinics due to COVID-19: report and early evaluation of a quality improvement initiative. BMJ Open Qual. 2020;9(2):e000985. doi:10.1136/bmjoq-2020-000985
66. Caporali R, Allanore Y, Alten R, et al. Efficacy and safety of subcutaneous infliximab versus adalimumab, etanercept and intravenous infliximab in patients with rheumatoid arthritis: a systematic literature review and meta-analysis. Expert Rev Clin Immunol. 2021;17(1):85–99. doi:10.1080/1744666X.2020.1858803
67. Lauper K, Mongin D, Iannone F, et al. Comparative effectiveness of subcutaneous tocilizumab versus intravenous tocilizumab in a pan-European collaboration of registries. RMD Open. 2018;4(2):e000809. doi:10.1136/rmdopen-2018-000809
68. Anterasian C, Duong R, Gruenemeier P, Ernst C, Kitsen J, Geng B. Quality of life differences for primary immunodeficiency patients on home SCIG versus IVIG. J Clin Immunol. 2019;39(8):814–822. doi:10.1007/s10875-019-00705-5
69. Kittner JM, Grimbacher B, Wulff W, Jager B, Schmidt RE. Patients’ attitude to subcutaneous immunoglobulin substitution as home therapy. J Clin Immunol. 2006;26(4):400–405. doi:10.1007/s10875-006-9031-5
70. Bell CF, Lau M, Lee M, Poulos C. Insights into the choice between intravenous infusion and subcutaneous injection: physician and patient characteristics driving treatment in SLE. Clin Rheumatol. 2020.
71. Cozon GJN, Clerson P, Dokhan A, Fardini Y, Sala TP, Crave JC. In-depth interviews of patients with primary immunodeficiency who have experienced pump and rapid push subcutaneous infusions of immunoglobulins reveal new insights on their preference and expectations. Patient Prefer Adherence. 2018;12:423–429. doi:10.2147/PPA.S156983
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.