Back to Journals » Clinical Optometry » Volume 11
Calibrated measurement of acuity, color and stereopsis on a Nintendo® 3DS™ game console
Authors Smith KA ![]() , Damarjian AG
, Damarjian AG ![]() , Molina A, Arnold RW
, Molina A, Arnold RW ![]()
Received 31 December 2018
Accepted for publication 1 March 2019
Published 30 April 2019 Volume 2019:11 Pages 47—55
DOI https://doi.org/10.2147/OPTO.S199992
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Supplementary video S1: Demonstration of the use of the PDI Check game for the Nintendo® 3DS™.
Views: 7049
Kyle A Smith,1 Alex G Damarjian,2 Aaron Molina,3 Robert W Arnold4
1Clinical Optometry Department, Accurate Vision Clinic, Anchorage, AK, USA; 2Technology and Humanities Department, Illinois Institute of Technology, Chicago, IL, USA; 3Programming Department, PDI Check, Anchorage, AK, USA; 4The Alaska Blind Child Discovery, Alaska Children’s EYE & Strabismus, Anchorage, AK, USA
Significance: A Nintendo® 3DS™ game can reliably test monocular near acuity, stereopsis and color without the need for occlusion patches or goggles.
Purpose: We developed dynamic, forced-multiple choice games to measure monocular near acuity, color vision and stereopsis on the autostereoscopic barrier screen of the Nintendo 3DS gaming system.
Methods: In an institutional review board-approved study, pediatric and adult patients and normal subjects performed routine patched near visual acuity, Ishahara’s color test and Stereo Fly tests. Then each subject performed a two-phase orientation and testing game, “PDI Check”, on a Nintendo 3DS.
Results: Forty-five patients aged 5–60 years completed the routine and Nintendo near tests, resulting in positive, consistent, discriminatory correlation functions. From ROC curves, referral criteria were determined to separate poor from fair-to-normal monocular acuity with 98% sensitivity and 100% specificity, stereoacuity with 80% sensitivity and 97% specificity, and color with 83% sensitivity and 100% specificity.
Conclusion: The Nintendo 3DS game PDI Check can provide consistent near vision testing via a dynamic, randomized method that does not require goggles for stereo, and does not require patching to assure monocular testing.
Keywords: near sensory testing, video game, autostereoscopic barrier screen, monocular visual acuity, stereopsis, dynamic color test
Introduction
Important components of a comprehensive pediatric or adult eye examination include monocular near acuity, stereopsis and color vision. There are challenges associated with near vision testing. Some individuals are averse to wearing goggles required for certain stereo presentation,1 or eye patches to assure monocular testing. It is possible for some individuals to memorize a chart or book, allowing a visually deficient individual to falsely pass.
The Nintendo® 3DS™ gaming system (Kyoto, Japan) consists of an autostereoscopic parallax barrier color display screen that does not require goggles to confer a three-dimensional (3D) impression and does not require patching to ensure monocular presentation.
We developed a game, “PDI Check”, for the Nintendo 3DS, capable of testing stereo, color and monocular near acuity. We believe this game has practical clinical potential for pediatric ophthalmologists and other eye doctors by overcoming barriers of acquisition time, efficiency and motivation for some patients and testing environments. It may also have research benefits since it addresses binocular, simultaneous presentation of dynamic images. This report is the initial calibration study in the ongoing development of the game.
Methods
This prospective, Health Insurance Portability and Accountability Act (HIPAA)-compliant study has received approval through the institutional review board at Pacific University, Forest Grove, OR, USA, and follows tenets of the Declaration of Helsinki. All subjects or their parents/guardians signed informed consent; older children (>16 years) also gave written informed assent. The study complies with Good Clinical Practices through the National Institute on Drug Abuse Clinical Trials Network.
Subjects with normal vision and patients with known or suspected amblyopia, strabismus, presbyopia and color deficiency were recruited from a pediatric eye/adult strabismus practice. Data were collected on patient age, gender, dominant eye, refraction and best corrected monocular distant acuity. The database was later de-identified.
Baseline near vision was collected by conventional clinical methods. Rosenbaum near card Sloan acuity was performed with the non-tested eye patched. Stereo vision was tested using polarized goggles and arc seconds of disparity by the Stereo Optical (Chicago, IL, USA) Stereo Fly test, which is commonly used in clinical practice even though it can present some monocular cues. Color was tested binocularly using Ishihara’s Test for Color Deficiency – Concise Edition (Kanehara & Co, Tokyo, Japan) with conventional illumination. To score the Ishahara, we counted 1 point if all correct, 0.5 points if partially correct and 0 points if all plates were missed. The range of possible missed scores therefore was from 0 (perfect color) to 13 missed. Thresholds for defining deficient near vision were visual acuity ≤20/70, Stereo ≤100 arc seconds and Ishihara concise missing three or more plates.
The Nintendo 3DS game is programmed to be a forced, multiple-choice dynamic near test of monocular visual acuity, stereopsis and color. The game, currently version 0.1.0, has two phases; orientation and testing. Each patient underwent baseline conventional testing and Nintendo 3DS testing on the same day.
During the orientation phase, the patient views the upper, color, autostereoscopic barrier liquid crystal display (LCD) screen with four identical objects in each of four quadrants corresponding to the interactive second, lower screen on the clam-shell game console. At the press (with finger or stylus) of a “start” button on the lower interactive screen, one of the four objects instantaneously changes by a substantial amount, and a “lag-time” is recorded from the initial random object change to the time the patient presses the correct, corresponding quadrant on the lower screen. The objects during orientation for near acuity are binocular “Landholt C” type optotypes, initially all “C”, with one randomly changing to a “U”. The dynamic change means that the “C”, which is a circle with an open region centered about 0°, is instantaneously rotated so that the identical circle open region is oriented to 90° (
During the testing phase, one random quadrant has a dynamic change from subtle to coarse values of monocular visual acuity, stereopsis and color. In monocular acuity, four, small “C” optotypes are presented in corresponding quadrants of the upper screen, then the right eye only of one random quadrant is instantly switched to a “U” and each optotype is gradually enlarged until the patient is able to discern a difference and press the corresponding quadrant of the lower screen. The subsequent test only changes the left eye of a random “C” optotype to a “U” in one quadrant. For color testing, all four quadrants start with equal hue, deutan confusion axis colors, then one random disc continuously changes hue until the patient can signal the correct, corresponding quadrant on the lower touch screen. For stereopsis, all four discs start at equal perceived height, then one gradually and linearly levitates until the patient signals their perception of depth on the lower touch screen.
Although this is a calibration study, mathematical formulae were derived relating direct time and/or screen distance output to scores on the conventional clinical tests. From these, test–retest reliability was assessed using Cronbach’s alpha. Interrater reliability was assessed with Bland–Altman analysis and Kendall’s W, with alpha of 0.05.
Receiver operating characteristic (ROC) curves were generated for each visual function, from which preferred PDI Check referral criteria were determined for calculations of sensitivity and specificity.
Results
Forty-five patients, mean age 35±17 SD years (median 37 years, range 5–60 years), including 26 females, participated. Seven were under the age of 20. The prescreening probability of deficiency was deliberately enhanced for the calibration (we sought extra subjects who had subnormal near vision): 8% with amblyopia or presbyopia near visual acuity loss, 14% with strabismus, and 14% with deuteranomaly color deficiency. For each of the near visual functions tested, a positive correlation was noted such that poor vision on the PDI Check corresponded with poor vision on conventional tests (Table 1).
 | Table 1 Regression curves to relate linear PDI Check values with corresponding conventional tests of the near visual functions with R-squared goodness of fit, and associated validation statistics from the ideal portion of the receiver operating characteristics curves |
Figure 1 shows the relationship between PDI Check estimation of monocular acuity versus patched Rosenbaum near-card acuity. Figure 2 shows the relationship between PDI Check stereo acuity (mm of displacement) and Stereo Fly acuity. Figure 3 shows the relationship between PDI Check color discrimination in elapsed time versus the number of missed plates on Ishihara’s Concise test.
 | Figure 1 Relationship between near monocular acuity measured with barrier screen–monocular acuity on the Nintendo® 3DS™ game PDI Check (abscissa) and the patched Rosenbaum near card (ordinate). Note: The arrow indicates chosen referral criteria from the receiver operating characteristics curve in Figure 4. |
 | Figure 2 Relationship between autostereoscopic screen, dynamic stereo game on the Nintendo® 3DS™ (abscissa) and Stereo Fly circles stereopsis in arc seconds (ordinate). Note: The arrow indicates chosen referral criteria from the receiver operating characteristics curve in Figure 5. |
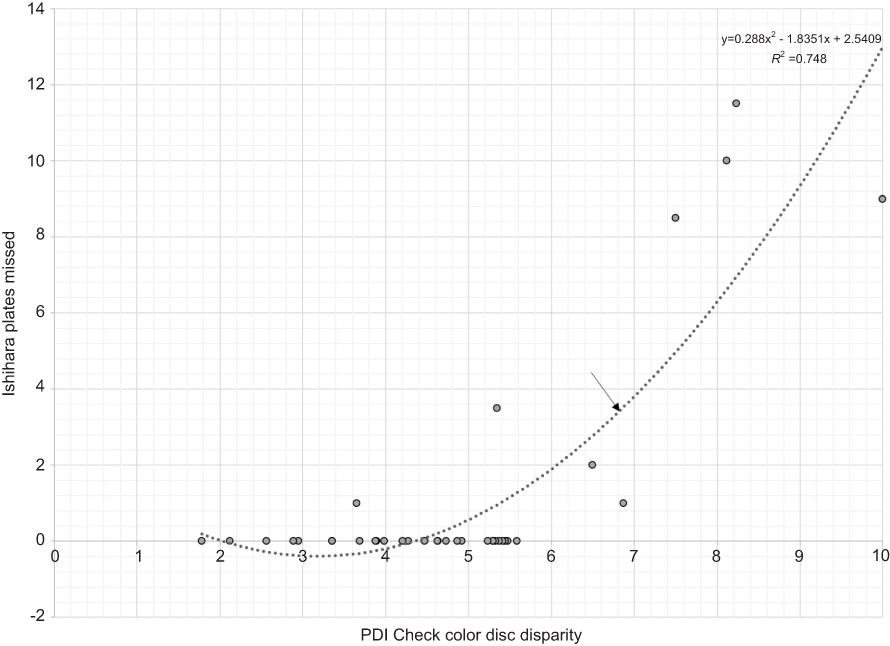 | Figure 3 Relationship between dynamic deutanopic confusion axis color game on the Nintendo® 3DS™ (abscissa) and Ishihara’s concise color test missed plates (ordinate). Note: The arrow indicates chosen referral criteria from the receiver operating characteristics curve in Figure 6. |
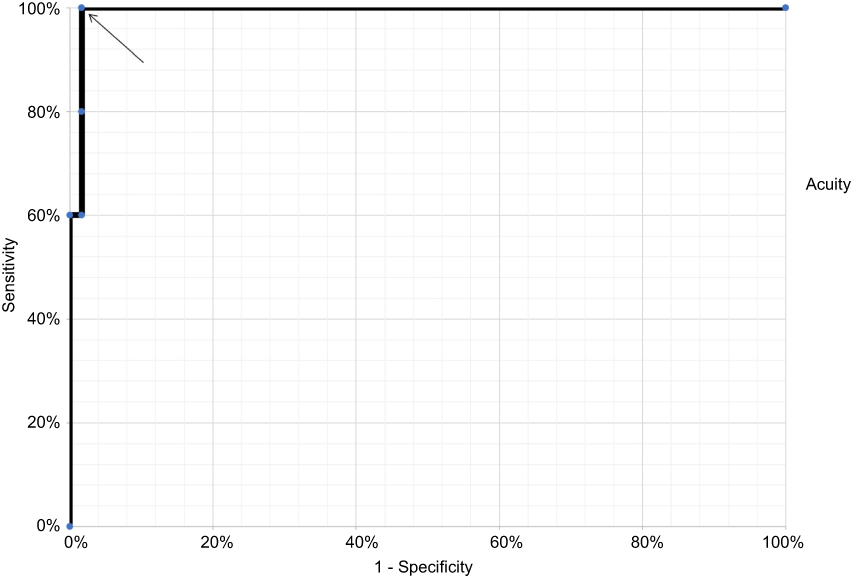 | Figure 4 Receiver operating characteristics curve for near monocular visual acuity with the PDI Check game compared to Rosenbaum pocket visual acuity with non-tested eye patched.Note: Arrow indicates the selected referral criteria. |
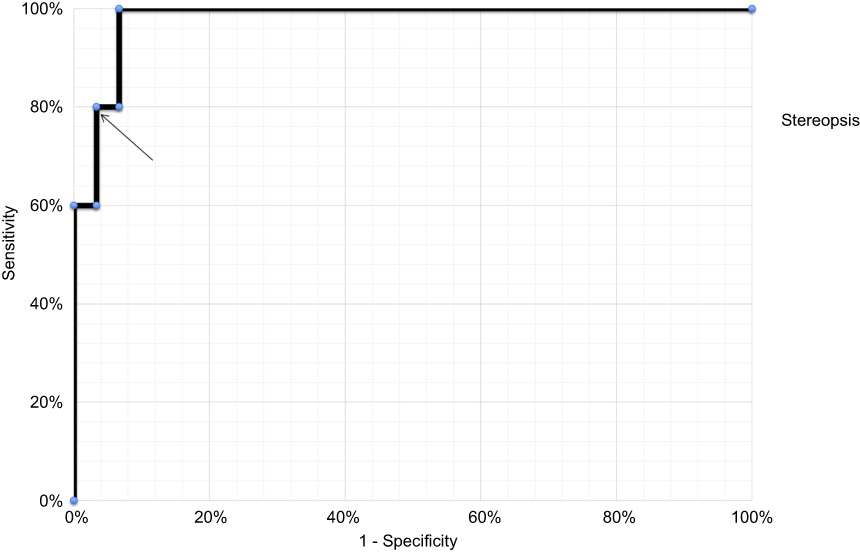 | Figure 5 Receiver operating characteristics curve for stereopsis with the PDI Check game compared to Titmus Stereo Fly circle with polarized goggles.Note: Arrow indicates the selected referral criteria. |
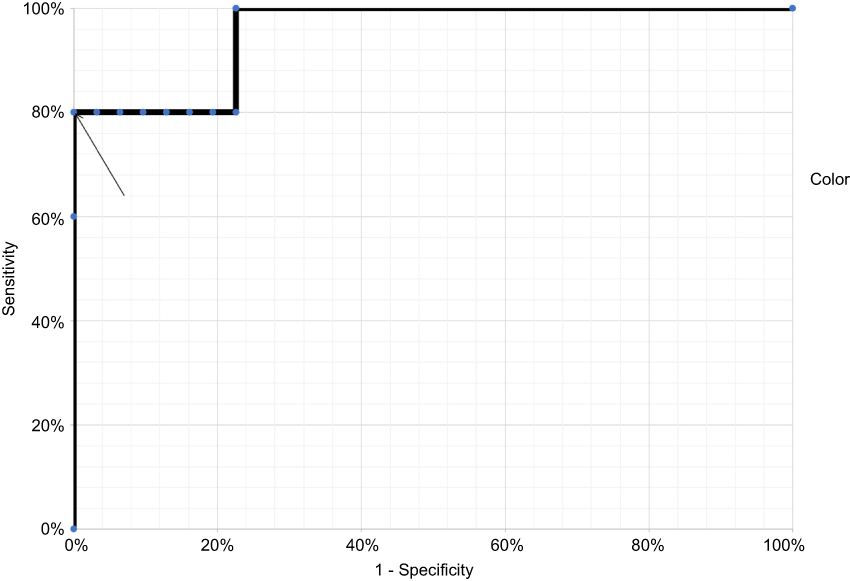 | Figure 6 Receiver operating characteristics curve for typical color vision deficiency with PDI Check dynamic game compared to missed color plates on the Ishihara concise test. Note: Arrow indicates the selected referral criteria. |
Figures 4–6 show ROC curves for visual acuity, stereopsis and color vision with the PDI Check compared to conventional testing. With a threshold of elapsed PDI Check acuity of 16.5 seconds, corresponding to a 13 mm optotype, this game is capable of sorting poor acuity from fair–good acuity with 100% sensitivity and 98% specificity. Utilizing a threshold of 0.4 mm, the PDI Check had the ability to sort poor from fair–good stereopsis with sensitivity 80% and specificity 97%. With a threshold of 7 discs, the PDI Check was able to sort color-deficient from normal color individuals with 80% sensitivity and 100% specificity.
From derived mathematical formulae relating PDI Check time scores, clinical values of near visual acuity, stereopsis and green color deficiency were calculated and then compared to each subject’s clinical score. Good reliability was shown on Bland–Altman analysis, with Kendall’s coefficient of concordance as follows: visual acuity (W=5.3, chi-square=38, p=6E-10), stereopsis (W=0.19, chi-square=7.1, p=0.007) and color (W=0.50, chi-square=20.5, p=6E-6).
Figure 7 shows test–retest values for stereo in six normal subjects and three uncorrected presbyopic patients using PDI Check. All the normal subjects scored 40 second arc on Stereo Fly. The relative SD (SD/mean) was less than 0.3 for all normal subjects over 18 repeated tests. There was good test–retest reliability, with overall Cronbach’s alpha=0.74, and for each of the nine subjects ranging from 0.76 to 0.96.
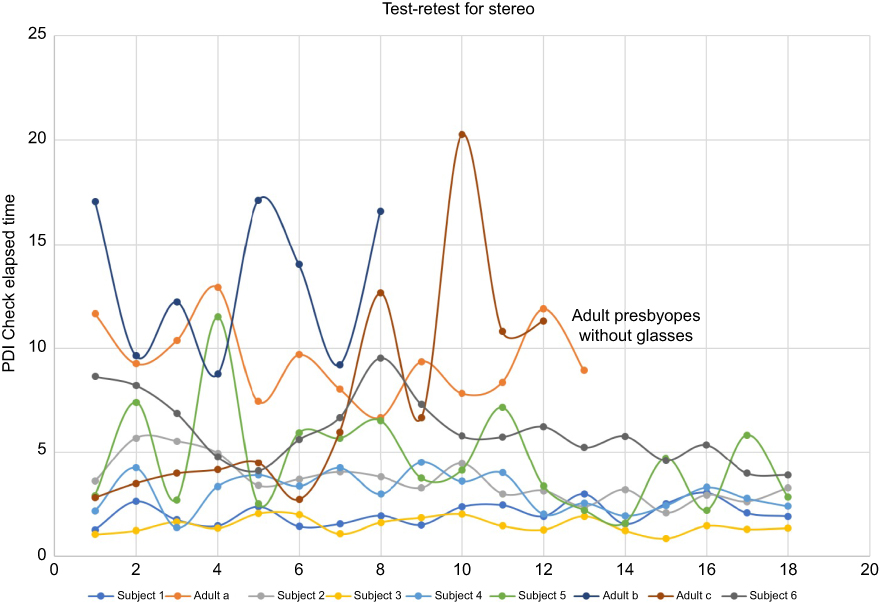 | Figure 7 Test–retest for stereo testing on the Nintendo® 3DS™ game PDI Check for three uncorrected presbyopic patients and six normal subjects, over 18 repeated presentations. |
Discussion
A new game for the autostereoscopic screen on the Nintendo 3DS provided results that correlated well with conventional clinical tests of monocular near visual acuity, stereopsis and red–green color deficiency. Normal subjects and patients provided an enhanced prescreening prevalence population over a wide range of normal and subnormal vision for consistent data, so continuous, mathematical relationships between dynamic game output and clinical values of near acuity, stereopsis and color vision could be quickly generated for the next version of the Nintendo 3DS game, PDI Check. This current version obtains timed data from each dynamic presentation in the game; the next version should output clinically relevant values from the mathematical functions thus derived.
Not all acuity and stereo tests have the same validity and reliability in young children.2 Testability for young children varies from 71% to 91% depending on the preschool stereo test.3 Conjecture surrounds any postulated, potential harm from viewing a Nintendo 3DS screen but therapeutic benefit has also been speculated.4,5 The Nintendo 3DS has been studied using 3D) movies and altering monocular blur from normal to suppression; when one viewing eye perceived the increasingly blurred image, 3D sensation remained robust until, with sufficiently blurred image, suppression occurred.6
Strengths of our study include a wide range of patient age, visual performance and clinical diagnoses. Comparisons were made between the new Nintendo game and conventional tests on the same day. We employed common clinically used conventional tests, each of which has known deficiencies, such as monocular cues for the Stereo Fly test compared to random-dot presentation.1 A weakness is that this is still a calibration study, the results of which are already giving rise to new game versions and subsequent validation studies. Another weakness is that this study did not include children with developmental delay or nystagmus. We did not gather time-efficiency data for all cases comparing conventional near vision testing to PDI Check, but further study on this important characteristic is underway.
Normal subjects had repeatable results on the Nintendo 3DS. We found reliable and repeatable results for stereopsis with finer resolution than the 40 second arc optimum for our comparative clinical test. Future trials will employ clinical tests such as the Randot test, which is capable of discerning higher grade stereopsis. The Nintendo was easily able to render depth without goggles and monocular testing without patching. As a result, this game has potential for clinical and research use with potential benefit for patients with developmental delay, autism, nystagmus, goggle and patch aversion, and also for patients who would tend to memorize certain tests during repeat testing.
Conclusion
By employing the unique, autostereoscopic screen of the Nintendo 3DS video game console, the PDI Check game reliably correlates with conventional clinical test methods for near visual acuity, stereopsis and color deficiency.
Acknowledgment
The paper was presented as a poster at the American Association for Pediatric Ophthalmology and Strabismus (AAPOS) Meeting, Washington, DC, USA, March 18, 2018.
Disclosure
The authors are board members of PDI Check, LLC, which markets the patent-pending game “PDI Check” for the Nintendo 3DS. Kyle A Smith reports no other conflicts outside PDI Check, LLC, outside the submitted work. Alex G Damarjian has nothing to disclose. Aaron Molina has nothing to disclose. Robert W Arnold reports that, in addition to PDI Check, being a board member of Glacier Medical Software, coordinating the Alaska Blind Child Discovery and being a protocol developer and investigator for the Pediatric Eye Disease Investigator Group (PEDIG). In addition, There is a PDI Check patent pending for Robert W Arnold and Alex G Damarjian. The authors report no other conflicts of interest in this work.
References
1. O’Connor AR, Tidbury LP. Stereopsis: are we assessing it in enough depth? Clin Exp Optom. 2018;101(4):485–494. doi:10.1111/cxo.12655
2. Moganeswari D, Thomas J, Srinivasan K, Jacob GP. Test re-test reliability and validity of different visual acuity and stereoacuity charts used in preschool children. J Clin Diagn Res. 2015;9(11):NC01–05. doi:10.7860/JCDR/2015/14407.6747
3. Cyert L, Schmidt P, Maguire M, Moore B, Dobson V, Quinn G. Threshold visual acuity testing of preschool children using the crowded HOTV and Lea Symbols acuity tests. J Aapos. 2003;7(6):396–399. doi:10.1016/S1091853103002118
4. Pallas A, Meyer CH, Mojon D. [Nintendo 3DS: technology, physiology and possible risks for children’s eyes]. Ophthalmologe. 2013;110(3):263–266. doi:10.1007/s00347-012-2696-7
5. Arnold RW, Davidson S, Madigan WP. Stereopsis and 3-d movies. J Pediatr Ophthalmol Strabismus. 2011;48(4):199–201. doi:10.3928/01913913-20110504-01
6. Tidbury L, Black R, O’Connor A. Assessment of stereoacuity and 3-D stereoscopic entertainment. Strabismus. 2015;23(4):164–169. doi:10.3109/09273972.2015.1107600
Supplementary material
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.