Back to Journals » International Medical Case Reports Journal » Volume 19
Stand-Alone Carboxytherapy Followed by Consolidation with Oral Hydrolyzed Marine Collagen Fragments: A Potential Sequential Bioregenerative Strategy for Hypertrophic Scars: A Case Report
Authors Fraone N, Trocchi G, Bartoletti E, Di Castro M, Lo Re F, Raichi M ![]()
Received 26 March 2026
Accepted for publication 2 June 2026
Published 11 June 2026 Volume 2026:19 609171
DOI https://doi.org/10.2147/IMCRJ.S609171
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Thomas E Hutson
Nadia Fraone,1 Gloria Trocchi,1 Emanuele Bartoletti,1 Myriam Di Castro,1 Federica Lo Re,1 Mauro Raichi2
1Department of Aesthetic Medicine, Fatebenefratelli Isola Tiberina-Gemelli Hospital, Rome, Italy; 2Clinical Pharmacology Academic Consultant and Medical Director, Astéria Pharma Srl, Milan, Italy
Correspondence: Nadia Fraone, Department of Aesthetic Medicine, Fatebenefratelli Isola Tiberina-Gemelli Hospital, Rome, Italy, Email [email protected]
Introduction: Carboxytherapy, via the Bohr effect, a denser dermal environment, and preserved fibroblast function, along with oral administration of bioactive marine collagen fragments that target fibroblasts, are regenerative strategies that could improve scar elasticity, thickness, and hydration. Their sequential combination might be an innovative approach.
Methods: In March 2024, a 56-year-old woman began treatment of a large, hypertrophic, partially retracted post-surgical scar in the nasojugal area at the level of the right nasal wing. Ablative techniques were strictly contraindicated; therefore, a regenerative, restructuring approach via carboxytherapy was chosen. A six-session carboxytherapy cycle was performed from October 10, 2024 (T0) to April 3, 2025 (T6). Each session, performed every 15 days, lasted approximately 10 minutes (flow rate: 60 mL/min, 30-G needle, temperature 45°C). Evaluations were conducted after the third (T3) and last (T6) sessions, using the Antera 3D device (quantitative three-dimensional objective analysis of scar depth, texture, erythrosis, and pigmentation) and the POSAS investigator and subject scoring scales. A final injection of persistent hyaluronic acid was performed on April 3, 2025. To support and strengthen the normalization of the scarring process, the first of a twice-yearly oral cycle of hydrolyzed marine collagen fragments began on October 23, 2025.
Results: Over the six-month carboxytherapy treatment cycle, the scarred skin area showed significant improvement toward a normal appearance. The vascularity POSAS score (observer component) decreased from 7 at baseline to 3 at T6; the thickness and flexibility scores improved from 5 to 2 and from 7 to 3, respectively. Additionally, the POSAS pain and itching scores (patient component) decreased from 6 to 1.
Conclusion: Stand-alone carboxytherapy again appears to be an effective option for hypertrophic, structurally abnormal scars. While further investigations are underway, supplementation with hydrolyzed marine collagen fragments may help maintain the benefits of prior carboxytherapy.
Plain Language Summary: Managing postsurgical scars, especially hypertrophic scars, is challenging. Carboxytherapy, the intradermal or subcutaneous administration of carbon dioxide, is well known for reducing the aesthetic and psychological burden of scars. It promotes local vasodilation, improves tissue oxygenation, and induces the production of new, well-organized collagen in the scar area.
Emerging research on the skin-restructuring properties of orally absorbed fragments of marine collagen suggests that these bioactive small peptides may also contribute to scar management. These small collagen peptides, produced at the end of the collagen lifecycle when skin collagen breaks down, stimulate skin fibroblasts to produce new collagen. Several marine collagen fragments are identical to the small, bioactive peptides generated by collagen breakdown and likely act similarly.
For the first time, the authors tested an innovative regenerative strategy that sequentially combines six sessions of carboxytherapy with long-term supplementation with hydrolyzed marine collagen in a 56-year-old woman. The woman sought treatment for a disfiguring hypertrophic scar on the right nasal wing following surgery for a skin carcinoma.
The outcomes of this innovative treatment strategy appear encouraging, though preliminary, as the woman has completed only her first at-home cycle of oral marine collagen supplementation.
Progress in the appearance of the disfiguring scar was monitored using a quantitative three-dimensional skin analysis device and the Patient and Observer Scar Assessment Scale (POSAS). Definitive conclusions from any experience with a single patient must await the results of well-designed clinical studies, some of which are already underway.
Keywords: carboxytherapy, hydrolyzed marine collagen, hypertrophic scar, postsurgical scar, regenerative medicine, scar management
Introduction
Minor wounds that leave small scars are common throughout life, from childhood onward. Uncovering the molecular events underlying this universal response to trauma, surgical wounds, or even adolescent acne vulgaris is ongoing. Immediately after the initial inflammatory phase of injury, fibroblasts become the primary drivers of the subsequent proliferative and remodeling phases of scarring. However, fibroblasts are not a uniform population in their roles in wound healing and their potential to scar.1,2 Fibroblasts involved in scarring belong to the Engrailed-1-positive lineages (EPFs). The role of Engrailed-1 lineage-negative fibroblasts (ENFs) is only partially understood. A dermal ENF subpopulation can activate Engrailed-1 expression after birth during wound healing; mechanical tension triggers mechanotransduction.2
Blocking this mechanotransduction pathway in genetically engineered animal models prevents Engrailed-1 activation and promotes ENF-driven wound regeneration. This leads to visible and ultrastructural recovery of skin, dermal structures, and appendages, along with restored mechanical strength.2 Therefore, reducing mechanical tension during postnatal wound healing could help shift the response from a fibrotic, EPF-driven process to a more regenerative, ENF-driven one. Understanding the network of molecular signals that regulate the replacement of the initial Type-III collagen with Type-I collagen and promote myofibroblast apoptosis during scar remodeling could open new avenues for strategies to prevent fibrosis and promote regenerative scarring.
The Role of Regenerative Medicine in Scar Management
The challenges faced by the aesthetic medicine specialist and the aesthetic plastic surgeon extend beyond those previously discussed. A primary question is how to minimize the impact of a hypertrophic scar, which is often pruritic yet remains within the original wound’s boundaries, or of a disfiguring keloid that exceeds those topographic limits, has a high tendency to recur, and shows disorganized collagen deposition.3–5 These lesions differ visibly and clinically. They also share overlapping molecular mechanisms, including a dysregulated balance between Transforming Growth Factor (TGF)-ß1/TGF-ß2 (pro-fibrotic) and TGF-ß3 (anti-fibrotic) activities, as well as abnormal activation of the Integrin-FAK (Focal Adhesion Kinase) and Wnt/ß-catenin pathways.4,5 Most importantly, these aberrant scarring lesions share the aesthetic, functional, and psychological burdens they impose.6 Facial hypertrophic scars, which account for up to 27% of all scars and impair mimic muscle function, can be especially troublesome, often beyond their aesthetic concern.6
Available evidence suggests that a regenerative medicine approach improves the management of abnormal scars by enhancing scar elasticity, thickness, and hydration. For instance, these improvements are observed after treatment with Platelet-Rich Plasma (PRP), especially when used as an adjunct rather than a stand-alone therapy.7 Centrifuged PRP is rich in growth factors that stimulate fibroblast regeneration and neoangiogenesis, including Platelet-Derived Growth Factor (PDGF), TGF-ß, and Vascular Endothelial Growth Factor (VEGF).7,8
The rationale for the regenerative effects of intradermal or subcutaneous administration of medical-grade CO2 via minimally invasive microinjections (carboxytherapy) is equally sound. Short-term microcirculatory vasodilation and the Bohr effect (a rightward shift of the O2 hemoglobin dissociation curve with increased oxygenation induced by local acidification) are essential components of the complex bioregenerative process that results in a denser microcirculatory network, improved blood flow, preserved fibroblast function, more uniform scar texture, and reduced local mechanical tension.9,10
The emerging dermal and subdermal biorestructurative properties of orally bioavailable marine collagen fragments may also contribute to scar management.11 The literature on this new addition to regenerative wound management is still scarce but suggestive, indicating that further studies may better elucidate the likely role of these bioactive fragments in wound management. Hydrolyzed oligopeptides promote fibroblast growth and enhance skin hydration by activating the HAS2 transcription pathway in dermal fibroblasts and stimulating hyaluronic acid synthesis.12,13 Hydrolyzed marine collagen fragments likely affect fibroblasts by mimicking and supplementing the physiological effects of collagen breakdown oligopeptides, known as matrikines, which are released in the dermis and subdermal tissues at the end of the matrix collagen lifecycle.14,15
This case report details the progression and outcomes of a regenerative treatment strategy that sequentially combines carboxytherapy with long-term consolidation using hydrolyzed marine collagen—an innovative approach not previously tested—for a hypertrophic scar that developed in 2023 following surgical removal of an epithelioma in the nasojugal region. All activities were within the approved regulatory indications for ambulatory carboxytherapy and at-home intake of hydrolyzed marine collagen, thereby legally allowing the waiver of prior Institutional Review Board approval.
Material and Methods
Baseline Clinical Situation and Evolution Before Carboxytherapy
In mid-March 2024, a 56-year-old woman sought specialist advice and treatment, with the requirement to avoid ablative techniques, for an aesthetically bothersome, star-shaped scar measuring approximately 6 cm in the nasojugal area at the level of the right nasal wing. The scar was hypertrophic, partially retracted, and mildly pruritic. It followed the removal of a basal cell carcinoma and a severe local infectious complication six months earlier, in late October 2023. It was associated with slight atrophy of the right malar groove and recurrent episodes of right suborbital edema, resulting in closure of the palpebral rim. Standard systemic therapy with corticosteroids and antibiotics effectively controlled minor post-surgical fever and periocular edema within ten days. In her medical history, the woman reported an additive mastoplasty at age 40, a left hip prosthetic replacement at age 41, and a more recent history of Hodgkin lymphoma treated with radiotherapy in 2022. She had undergone frequent microinvasive mesotherapy (vitamins, amino acids, microelements, nucleosides, and antioxidants) and filler sessions (hyaluronic acid) since age 40, particularly in the zygomatic and nasolabial areas. At the time of surgery, she reported taking nutritional supplements; she had also attempted, without success, to reduce the visual impact of the scar with topical corticosteroids and a cream containing hyaluronic acid, dimethicone, and essential oils to improve scar elasticity.
During the mid-March baseline assessment, ultrasound of the dermis, subdermis, and subcutaneous tissues using an 18 MHz probe revealed a large hypoechoic, edematous area extending from the dermis to the superficial subdermis, followed by a hyperechoic area reaching the bone layer on deeper probing. In the nasolabial region, the scan revealed numerous small hypoechoic zones surrounded by intense tissue hyperechogenicity, likely due to previous injection sessions. Bilaterally in the suborbital areas, ultrasound imaging showed mild hyperechogenicity (approximately 8 mm), likely representing an edematous region undergoing active, chaotic restructuring, suggesting that a regenerative medicine strategy would have been more likely to yield benefits.
At this point, the woman agreed, by signing a detailed informed consent form, to undergo a carboxytherapy treatment cycle. Table 1 outlines the sequence of events, beginning with the October 2023 removal of the skin carcinoma, followed by the infectious complication and the mid-March baseline assessment.
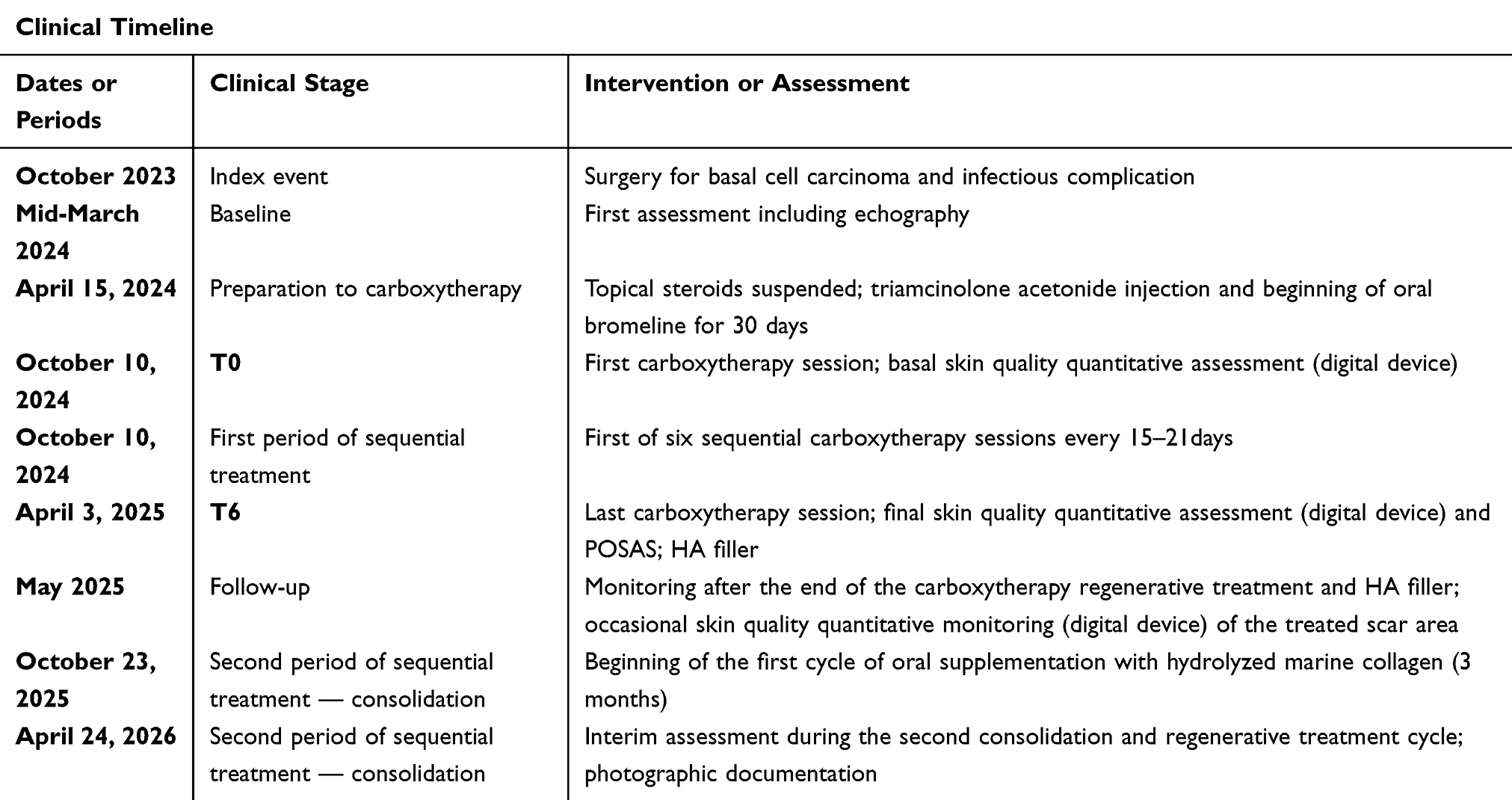 |
Table 1 Timeline of Events Following the Initial Index Event (Surgery for Basal Cell Carcinoma and the Infectious Complication, October 2023): Details of Dates (Dates or Periods), Corresponding Events/Clinical Status (Clinical Stage), and Procedures Performed (Intervention or Assessment) |
After discontinuing topical corticosteroids on April 15, 2024, the woman began carboxytherapy preparation with a triamcinolone acetonide injection (0.1 mL with 0.1 mL of lidocaine) and oral bromelain (500 mg daily for 30 days). On June 10, 2024, the hypertrophic nasojugal scar and right suborbital edema remained unchanged; another triamcinolone acetonide injection and daily bromelain were continued for an additional 30 days.
The Carboxytherapy Treatment Cycle
On October 10, 2024 (T0), the woman underwent the first carboxytherapy session (device: Carbomed CO2 Taumed®, flow rate: 60 mL per minute, 30-G needle, temperature controlled at 45°C). She completed the six-session cycle, with one session (about 10 minutes total) every few weeks, by April 3, 2025 (approximately 120 cc per session until visual evidence of transient paleness). Figure 1 shows the baseline condition of the disfiguring scar immediately before starting CO2 injection.
 |
Figure 1 Baseline (T0) presentation of the hypertrophic scar before the first carboxytherapy session on October 10, 2024. |
Monitoring and Assessment Techniques
After the T0 baseline evaluation on October 10, 2024, the evolution of the hypertrophic scar was assessed after three sessions (T3) and at the end of the six-session cycle (T6), using both objective measures (quantitative Antera 3D® digital three-dimensional imaging and analysis of superficial groove depths, texture, erythrosis, and pigmentation of the hypertrophic scar and adjacent skin) and clinical assessments (POSAS investigator and subject scoring scales, Figure 2).16–19 All digital photographs at T0, T3, and T6 were taken under standardized lighting and subject positioning. Occasional Antera 3D® digital monitoring of the carboxytherapy-treated area continued after the six-session carboxytherapy cycle until mid-October 2023.
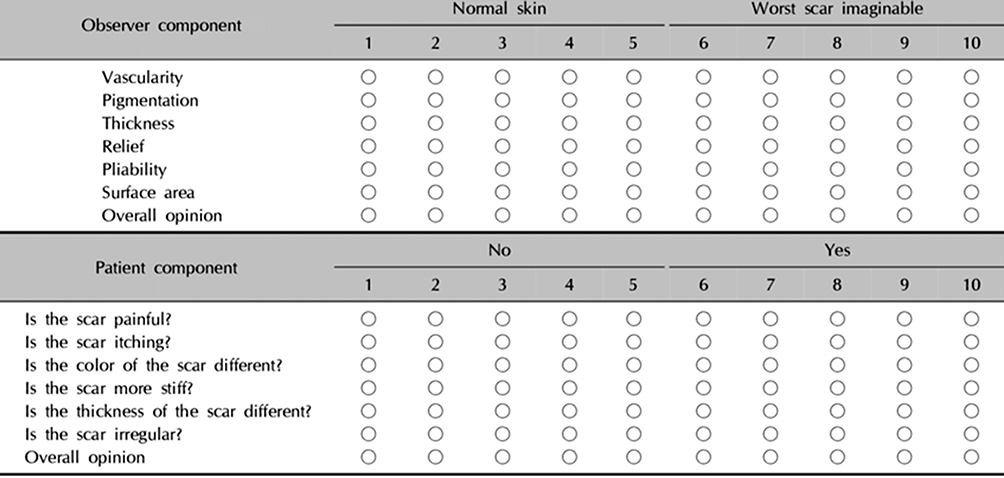 |
Figure 2 The observer and patient components of the Patient and Observer Scar Assessment Scale (POSAS). In the observer component, all parameters consisted of an additional category: Vascularity: pale, pink, red, purple, or mix; Pigmentation: hypopigmentation, hyperpigmentation, or mix; Thickness: thicker or thinner; Relief: supple, stiff, or mix; surface area: expansion, contraction, or mix. Credit: Draaijers LJ et al (Ref19). |
Several months after completing the planned carboxytherapy cycle, the need to enhance and strengthen the results achieved so far prompted a second, less invasive regenerative medicine strategy based on hydrolyzed marine collagens and their highly bioavailable, orally bioactive oligopeptides.11 On October 23, 2025, following a monitoring visit, the woman began taking 5 g of hydrolyzed marine collagen oligopeptides daily as a dietary supplement (Nashira COLLAGEN, Astéria Pharma, Milan, Italy) for three months. The most recent monitoring visit and visual documentation of the scar’s evolution occurred on February 20. Oral intake of bioactive marine collagen fragments will be repeated every 6 to 9 months.
Results
On October 10, 2024, as expected, the treated scar area showed mild inflammation immediately after the carboxytherapy session (Figure 3). This irritation resolved quickly, and the recommendation was to continue applying the same soothing cream, containing hyaluronic acid, dimethicone, and essential oils, twice daily. All six carboxytherapy sessions proceeded without delays or safety concerns. The hypertrophic nasojugal scar’s disfiguring appearance gradually improved over the six treatments. The complete set of images is available upon reasonable request.
 |
Figure 3 Mild inflammation in the hypertrophic scar area after the first carboxytherapy session on October 10, 2024. |
Figure 4 shows the final overall aesthetic result after session six on April 23, 2025, approximately 6 months after the first carboxy therapy session. After the last CO2 infiltration, a vial of persistent, highly flexible hyaluronic acid gel was injected: first superficially with a needle, then more deeply with a cannula. Figure 5 shows the acne scar area on the same day, immediately after the hyaluronic acid injection.
 |
Figure 4 Final evidence of the originally partially retracted hypertrophic scar immediately after the sixth and final carboxytherapy session on T6 (April 3, 2025), immediately before the injection of persistent hyaluronic acid that concluded the six-session carboxytherapy cycle. |
 |
Figure 5 Condition of the scarred skin area on the last day of the carboxytherapy cycle, after the final hyaluronic acid injection. |
Table 2 presents the quantitative changes in the three-dimensional digital analysis parameters during the six-month carboxytherapy sessions and the evaluation period. Figure 6 illustrates the visual improvements in erythrosis and the depth of superficial scar grooves over the same period, indicating structural remodeling of the hypertrophic scar and surrounding skin. During this period, the vascularity POSAS score (observer component) improved from 7 at baseline to 3 at T6; the thickness and flexibility scores improved from 5 to 2 and from 7 to 3, respectively. Additionally, the POSAS scores for pain and itching (patient component) improved from 6 to 1.
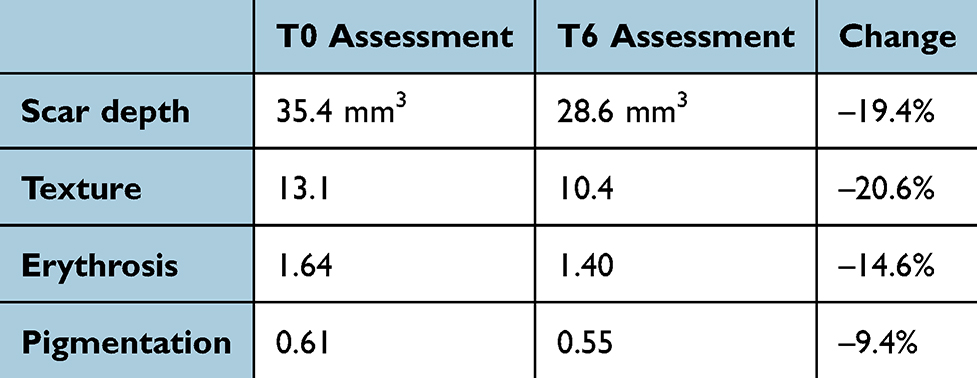 |
Table 2 Changes in Digitally Measured Three-Dimensional Scar Parameters from Baseline to the Final Assessment After the Six-Session Carboxytherapy Cycle. Absolute Values are Reported for Texture, Erythrosis, and Pigmentation |
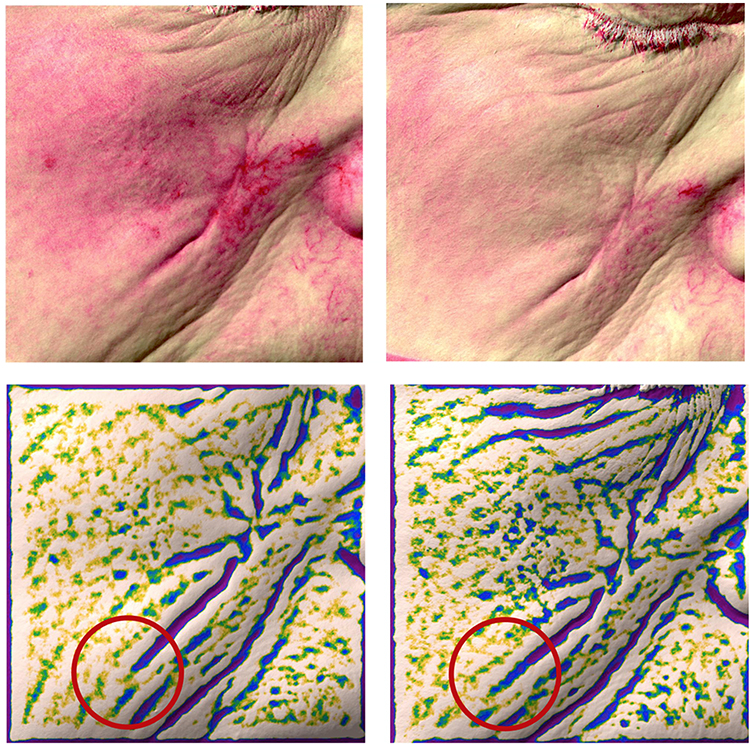 |
Figure 6 Changes from T0 to T6 in erythrosis (top left and right images, respectively) and in the depth of superficial grooves (bottom left and right images, respectively) of the nasojugal scar and surrounding skin. Groove depth is proportional to color intensity (from green to blue to purple): the disappearance of the purple color code, as evidenced within the two comparative red circles, indicates shallower grooves than at baseline. |
Figure 7 shows, on the left, the scarred skin area almost two months after the hyaluronic acid injection (May 29, 2025), and on the right, the same area on October 23, 2025. That October date marks the beginning of the second skin-restructuring treatment course, based on the regenerative properties of hydrolyzed marine collagen fragments (Figure 8), to help support and strengthen the normalization of the scarring process. The first of a twice-yearly cycle of three-month daily intake of bioactive marine collagen hydrolysates began in late October 2025 and ended in late January 2026.
 |
Figure 7 Left snapshot (May 29, 2025): Follow-up monitoring of possible aesthetic changes in the scarred area one month after the final hyaluronic acid infiltration and almost two months after the last carboxytherapy session. Right snapshot (October 23, 2025): condition of the scarred area at the start of the second skin-restructuring treatment course using bioregenerative hydrolyzed marine collagen fragments. |
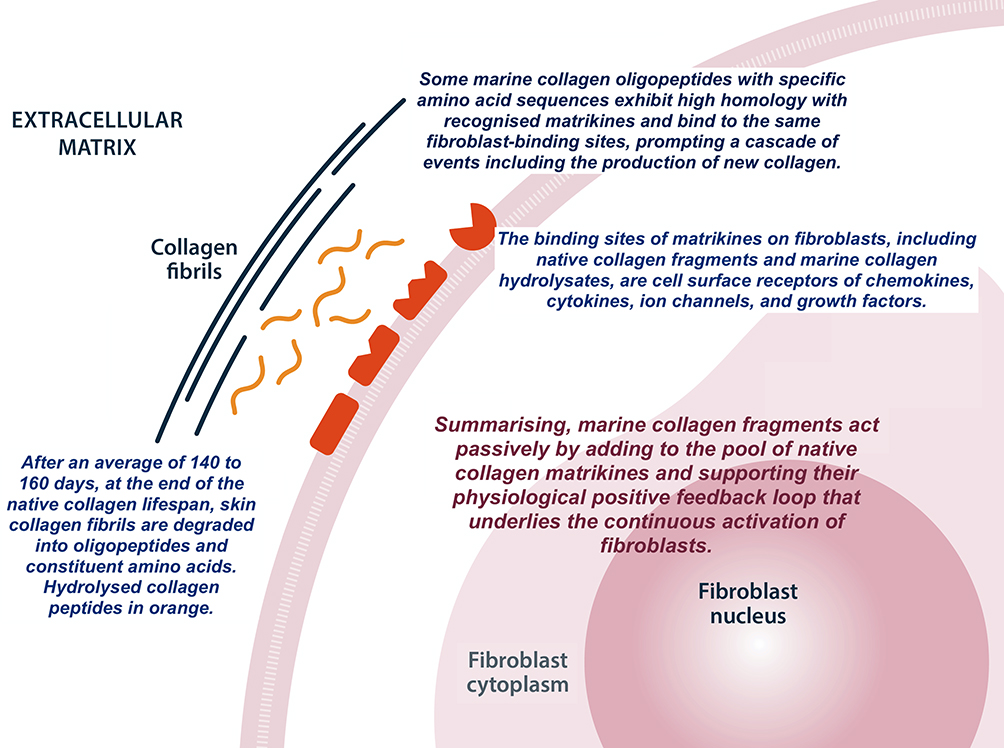 |
Figure 8 The effects of hydrolyzed marine collagen on fibroblasts mimic and enhance those of physiological matrikines as native collagen reaches the end of its lifespan in the dermis and subdermal tissues. Reproduced and adapted from Bartoletti E et al (Ref11) under a Creative Commons CC BY-NC 4.0 License. |
Figure 9 shows the appearance of the hypertrophic scar area on April 24, 2026, the most recent control visit to date, approximately six months after starting oral intake of bioactive marine collagen fragments. The area appears well-preserved. The woman was and remains grateful for the aesthetic result achieved to date. She reports marked improvement in her self-image, self-esteem, and confidence in social interactions.
 |
Figure 9 Follow-up interim control of the hypertrophic scar area on April 2, 2026, the most recent monitoring visit, approximately nine and a half months after the last carboxytherapy session and six months after the second skin-restructuring treatment course with bioactive hydrolyzed marine collagen fragments began. |
Discussion
Excavated dermal depressions resulting from collagen destruction after severe inflammation are a hallmark of atrophic scars. Their clinical appearance varies. Most are narrow, sharply defined, V-shaped fibrous lesions that extend deep into the dermis and account for 60% to 70% of atrophic scars. Wider U-shaped scars with vertical edges reach 0.1 to 0.5 mm into the dermis and make up 20% to 30%. Irregularly rolling scars with fibrous tethering of the dermis to the subcutis account for 15% to 25%.20
The literature provides a solid and reasonable basis for the regenerative effects of subdermal carboxytherapy in treating depressed and hypertrophic scars, and the case report seems to confirm these effects, with notable results at the end of the six-session treatment cycle in early April 2025. Carboxytherapy can be used as a stand-alone treatment or combined with other biorestructuring strategies, such as PRP; the mechanisms by which it exerts its regenerative effects in the skin are reasonably well understood.9,21 Carboxytherapy increases Matrix Metalloproteinase-1 (MMP-1) expression compared with PRP.22 Carboxytherapy produces a short-lived microcirculatory vasodilatory effect that lasts only a few minutes. The locally decreased pH and the Bohr effect activate dermal fibroblasts through the acknowledged action of pro-inflammatory cytokines such as interleukin (IL)-6 and tumor necrosis factor (TNF)-α.9,23 This leads to increased production of collagen and extracellular matrix, microcirculatory vasodilation with improved local blood flow, and long-term increased oxygenation. It also results in reduced scar volume with better morphometry, decreased local mechanical tension, and the release of local growth factors that promote angiogenesis, lipolysis, and skin regeneration.9,23
In addition to biochemical mechanisms, mechanical effects of pressure and CO2 flow in the dermis and subcutaneous tissue activate fibroblasts via internal mechanotransduction pathways.23 A preliminary course of corticosteroid infiltrations, performed between April and May 2025, reduced inflammation and collagen overproduction.24 The marked aesthetic improvement, improved scar texture (digitally estimated at 45%), and volume reduction (60–70%) of the disfiguring hypertrophic scar between autumn 2024 and spring 2025 attest to the bioregenerative and restructuring properties of microinvasive carboxytherapy. Treatment was associated with minimal, temporary discomfort. Erythema lasted no more than 30 minutes. Decreased pigmentation is somewhat unexpected. Although there is currently a lack of gold-standard, evidence-based treatments for pigmentation issues, carboxytherapy has already been shown to be effective, for instance, for periorbital hyperpigmentation.25
Confounding Factors and Limits to More Definitive Conclusions
The three-month maintenance course using marine collagen hydrolysates aligns with the favorable expectations regarding their dermal-restructuring effects; however, definitive confirmation remains premature.
The role of these bioactive fragments remains the central point of debate in this case report, which should be regarded only as hypothesis-generating. Any discussion of observed outcomes in a single patient without a control group is only preliminary; more definitive conclusions must await the results of well-designed, randomized, controlled prospective clinical studies, some of which are already underway. Any pretense of a conclusion beyond a simple suggestion aligned with available evidence is vulnerable to interference from several confounding factors. First, oral maintenance with marine collagen fragments, begun only four months after initiating bioactive hydrolysates, is still in its very early stages. A more confident judgment should wait at least a second maintenance course and several more months, namely, at least eight to twelve months after the last carboxytherapy session. A second potentially powerful confounding factor, at least in these early months after the end of the carboxytherapy course, is the persistent volumetric effect of the final hyaluronic acid injection administered immediately after the last CO2 infiltration. The confounding effect of this late infiltration of flexible hyaluronic acid, if any, will become clear only in the next months.
The authors acknowledge that neither of their two regenerative treatments is novel. The novelty lies in their sequential combination to sustain the results of carboxytherapy over time.23,26 Stand-alone carboxytherapy remains a viable and effective treatment option for hypertrophic, structurally abnormal scars. Properly designed clinical studies may, in the future, confirm that boactive hydrolyzed marine collagen fragments are a sound choice for preserving and strengthening results achieved with prior carboxytherapy, as suggested by experimental evidence. Randomized controlled trials with long-term follow-up are also warranted to optimize dosages, duration, and technical parameters of this potentially innovative sequential regenerative approach for the management of abnormal scars. Well-designed studies would also be welcome to elucidate the cytokine and, more generally, biochemical changes that occur after carboxytherapy and during chronic intake of marine collagen hydrolyzates.
Conclusions
The rationale for using bioactive marine collagen fragments, taken orally months after carboxytherapy sessions to reinforce and sustain previously achieved results, appears reasonably well supported by the experimental literature, although clinical evidence remains lacking and should be developed as soon as possible.11 They appear to efficiently inhibit abnormal fibrosis in experimental models, probably because they are similar, if not identical, to physiological collagen matrikines derived from native dermal collagen at the end of its lifecycle. Examples include fibrosis induced by collagen I-derived C-1158/59 and endostatin, the C-terminal end of collagen XVIII.15 These bioactive collagen fragments have high systemic bioavailability, comparable to proline, and their bioregenerative and biorestructuring properties are associated with minimal antigenic potential and a low risk of Type 1 immediate hypersensitivity.27,28 Across all clinical studies conducted to date in aesthetic medicine rather than wound management, their safety profile appears comparable to that of a placebo.11 Notably, aesthetic benefits, such as improved appearance of wrinkles, are associated with increased subepidermal echogenicity, a normalized collagen texture with fewer huddled and coarse collagen fibers, and reduced elastosis.29
Data Sharing Statement
The minutes of clinical activities from the initial assessment visit and the six-session carboxytherapy treatment cycle are archived and available upon reasonable request from the Corresponding Author.
Ethical Statement
All activities conducted by the Corresponding Author and the study investigator adhered to the approved regulatory indications for ambulatory treatment with the carboxytherapy medical device and for at-home intake of hydrolyzed marine collagen, as detailed in the authorized User Manual (for the carboxytherapy device) and the Patient Information Leaflet (for the dietary supplement). In accordance with applicable regulatory requirements (i.e., Articles 62 to 82 of the European Union Regulation MDR 2017/745 and Article 16 of Legislative Decree 137/2022), these guidelines permit a waiver of prior Institutional Review Board approval. The authors are responsible for the clinical and editorial accuracy and integrity of the manuscript submitted to the International Medical Case Reports Journal. They confirm adherence to the journal’s ethical policies, as outlined in the author guidelines. The signed and dated informed consent forms, completed before each treatment session and outlining the purpose, procedures, risks, benefits, and alternative options, are available upon request. These forms explicitly include a section granting permission to publish the case history and related photographic documentation.
Acknowledgments
The authors thank Astéria Pharma Srl, Milan, Italy (https://asteriapharma.com/), for its generous, unrestricted support toward open-access publication costs. They also thank the woman described in their case report for granting permission to reproduce her photographs in the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The corporate sponsor, Astéria Pharma Srl, Milan, Italy, will be the sole source of funding for the article processing charges required by the International Medical Case Reports Journal.
Disclosure
No author received funding or other benefits related to the clinical activities or the design of the case report manuscript. They have no paid or unpaid relationships with industry manufacturers, publishers, or other companies associated with the submission. Dr. Nadia Fraone, the Corresponding Author, received research grants while serving on R&D steering boards. She has also served as a lecturer and tutor in continuing medical education and as an investigator in clinical studies, including those sponsored by manufacturers of carboxytherapy devices. Dr. Mauro Raichi is the medical director of a company that markets a widely used hydrolyzed marine collagen nutritional supplement. He made every effort to serve solely as a clinical pharmacology consultant, ensuring that his role did not influence his judgments. The authors declare no other conflicts of interest in this work.
References
1. Eming SA, Martin P, Tomic-Canic M. Wound repair and regeneration: mechanisms, signaling, and translation. Sci Transl Med. 2014;6(265):265sr6. doi:10.1126/scitranslmed.3009337
2. Mascharak S, desJardins-Park HE, Davitt MF, et al. Preventing Engrailed-1 activation in fibroblasts yields wound regeneration without scarring. Science. 2021;372(6540):eaba2374. doi:10.1126/science.aba2374
3. Ancuța DL, Văduva M, Coman C, Caraș I. Recent advances in animal models for pathological scar research: a comprehensive review of experimental approaches and translational relevance. Animal Model Exp Med. 2026;9(1):59–13. doi:10.1002/ame2.70115
4. Fang X, Wang Y, Chen H, et al. Hypertrophic Scarring and keloids: epidemiology, molecular pathogenesis, and therapeutic interventions. MedComm. 2025;6(10):e70381. doi:10.1002/mco2.70381
5. Kohlhauser M, Mayrhofer M, Kamolz LP, Smolle C. An update on molecular mechanisms of scarring–A narrative review. Int J Mol Sci. 2024;25(21):11579. doi:10.3390/ijms252111579
6. Van Loey NE, Van Son MJ. Psychopathology and psychological problems in patients with burn scars: epidemiology and management. Am J Clin Dermatol. 2003;4(4):245–272. doi:10.2165/00128071-200304040-00004
7. Gawdat HI, Hegazy RA, Fawzy MM, Fathy M. Autologous platelet-rich plasma: topical versus intradermal after fractional ablative carbon dioxide laser treatment of atrophic acne scars. Dermatol Surg. 2014;40(2):152–161. doi:10.1111/dsu.12392
8. Cho EB, Park GS, Park SS, et al. Effect of platelet-rich plasma on proliferation and migration in human dermal fibroblasts. J Cosmet Dermatol. 2019;18(4):1105–11112. doi:10.1111/jocd.12780
9. Bagherani N, Smoller BR, Tavoosidan G, et al. An overview of the role of carboxytherapy in dermatology. J Cosmet Dermatol. 2023;22(9):2399–2407. doi:10.1111/jocd.15741
10. Jarzabek-Perz S, Wrzosek M. Carboxytherapy in the management of selected skin conditions–applications in monotherapy and combined treatments. Appl Sci. 2025;15(17):9236. doi:10.3390/app15179236
11. Bartoletti E, Cavallini C, Klinger MEA, Lim TS, Llorca Pérez VM, Raichi M. Hydrolyzed marine collagen: emerging evidence of benefits via the oral route - review and insights for medical aesthetics practitioners. Clin Cosmet Invest Dermatol. 2025;18:3339–3356. doi:10.2147/CCID.S562518
12. Shigemura Y, Iwai K, Morimatsu F, et al. Effect of prolyl-hydroxyproline (Pro-Hyp), a food-derived collagen peptide in human blood, on the growth of fibroblasts from mouse skin. J Agric Food Chem. 2009;57(2):444–449. doi:10.1021/jf802785h
13. Kim D-U, Chung H-C, Choi J, Sakai Y, Lee B-Y. Oral intake of low-molecular-weight collagen peptide improves hydration, elasticity, and wrinkling in human skin: a randomized, double-blind, placebo-controlled study. Nutrients. 2018;10(7):826. doi:10.3390/nu10070826
14. Kisling A, Lust RM, Katwa LC. What is the role of peptide fragments of collagen I and IV in health and disease? Life Sci. 2019;2019(228):30–34. doi:10.1016/j.lfs.2019.04.042
15. Jariwala N, Ozols M, Bell M, et al. Matrikines as mediators of tissue remodelling. Adv Drug Deliv Rev. 2022;185:114240. doi:10.1016/j.addr.2022.114240
16. Fearmonti R, Bond J, Erdmann D, Levinson H. A review of scar scales and scar measuring devices. Eplasty. 2010;10:e43.
17. Zhang N, Shi K, Hong L, et al. Antera 3D camera: a novel method for evaluating the therapeutic efficacy of fractional CO2 laser for surgical incision scars. J Cosmet Dermatol. 2018;17(6):1041–1045. doi:10.1111/jocd.12738
18. Ruccia F, Zoccali G, Cooper L, et al. A three-dimensional scar assessment tool for keloid scars: volume, erythema and melanin quantified. Skin Res Technol. 2021;27(6):1007–1016. doi:10.1111/srt.13050
19. Draaijers LJ, Tempelman FRH, Botman YAM, et al. The patient and observer scar assessment scale: a reliable and feasible tool for scar evaluation. Plast Reconstr Surg. 2004;113(7):1960–1965. doi:10.1097/01.prs.0000122207.28773.56
20. Holland DB, Jeremy AH. The role of inflammation in the pathogenesis of acne and acne scarring. Semin Cutan Med Surg. 2005;24(2):79–83. doi:10.1016/j.sder.2005.03.004
21. Araco A, Araco F, Raichi M. An exploratory study of PN HPT for treating postsurgical atrophic and depressed scar. J Cosmet Dermatol. 2025;24(1):e16764. doi:10.1111/jocd.16764
22. Nassar SO, Eltatawy RAR, Hassan GFR. Safety and efficacy of platelet-rich plasma vs carboxytherapy in the treatment of atrophic scar: a comparative clinical and histopathological study. Dermatol Ther. 2020;33(6):e13942. doi:10.1111/dth.1394218
23. Stolecka-Warzecha A, Chmielewski Ł, Deda A, et al. The Influence of carboxytherapy on scar reduction. Clin Cosmet Invest Dermatol. 2022;15:2855–2872. doi:10.2147/CCID.S389380
24. Zhuang ZH, Li YT, Wei XJ. The safety and efficacy of intralesional triamcinolone acetonide for keloids and hypertrophic scars: a systematic review and meta-analysis. Burns. 2021;47(5):987–998. doi:10.1016/j.burns.2021.02.013
25. Seirafianpour F, Atefi N, Amin NG, et al. Effectiveness, safety, and patient satisfaction of carboxytherapy as an adjunctive treatment for periorbital hyperpigmentation. Skin Res Technol. 2004;30(3):e13651. doi:10.1111/srt.13651
26. Delgado-Miguel C, Miguel-Ferrero M. Preliminary results of the use of carboxytherapy in the treatment of pathologic scars: a minimally invasive alternative. J Pediatr Surg. 2023;58(4):679–683. doi:10.1016/j.jpedsurg.2022.12.008
27. Sibilla S, Godfrey M, Brewer S, Budh-Raja A, Genovese L. An overview of the beneficial effects of hydrolysed collagen as a nutraceutical on skin properties: scientific background and clinical studies. Open Nutraceut J. 2015;8(1):29–42. doi:10.2174/1876396001508010029
28. Rahman A, Rehmani R, Pirvu DG, Huang SM, Puri S, Arcos M. Unlocking the therapeutic potential of marine collagen: a scientific exploration for delaying skin aging. Mar Drugs. 2024;22(4):159. doi:10.3390/md22040159
29. Maia Campos PMBG, Scarpino Barboza Franco R, Kakuda L, Cadioli GF, D’Angelo Costa GM, Bouvret E. Oral supplementation with hydrolyzed fish cartilage improves the morphological and structural characteristics of the skin: a double-blind, placebo-controlled clinical study. Molecules. 2021;26(16):4880. doi:10.3390/molecules2616488
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.