Back to Journals » Clinical Ophthalmology » Volume 20
Influence of Preoperative Contact Lens Wearing Patterns on Corneal Endothelial Cell Density After Implantable Collamer Lens Implantation
Authors Gotoda S ![]() , Horai R, Sakai Y, Nishida T, Ichikawa K, Ichikawa K
, Horai R, Sakai Y, Nishida T, Ichikawa K, Ichikawa K ![]()
Received 6 March 2026
Accepted for publication 16 April 2026
Published 21 April 2026 Volume 2026:20 607456
DOI https://doi.org/10.2147/OPTH.S607456
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sotiria Palioura
Satoshi Gotoda,1 Rie Horai,1 Yukihiro Sakai,1 Tomoya Nishida,1 Kei Ichikawa,1,2 Kazuo Ichikawa1
1Department of Ophthalmology, Chukyo Eye Clinic, Nagoya, Aichi, Japan; 2Department of Ophthalmology, Aoyama General Hospital, Toyokawa, Aichi, Japan
Correspondence: Satoshi Gotoda, Department of Ophthalmology, Chukyo Eye Clinic, 12-22 Sanbonmatsu-cho, Atsuta-ku, Nagoya, Aichi, 456-0032, Japan, Tel +81-52-883-1543, Email [email protected]
Purpose: To determine the influence of preoperative contact lens (CL) wearing history on early postoperative corneal endothelial cell density (CD) and endothelial morphology following implantable Collamer lens (ICL) implantation.
Patients and Methods: In this retrospective study, 230 eyes that underwent ICL implantation at Chukyo Eye Clinic (mean age 34.4 ± 8.24 years) were analyzed. Based on preoperative interviews, eyes were categorized into four groups: no CL wear (78 eyes), hard CL wear (HCL; 29 eyes), non-daily soft CL wear ≤ 10 h/day (NSCL; 48 eyes), and daily soft CL wear ≥ 10 h/day (OSCL; 75 eyes). CD, coefficient of variation (CV), and percentage of hexagonal cells (6A) were assessed preoperatively and at 1 and 3 months postoperatively. The primary outcome was the between-group comparison of CD change from baseline to 1 month.
Results: No significant between-group differences were observed in CD changes at 1 month (p = 0.458) or 3 months (p = 0.149). Within-group analyses demonstrated significant CD reduction at 1 month in the NSCL and OSCL groups (both p = 0.04); this reduction persisted at 3 months only in the OSCL group (p = 0.04). No significant CD changes were observed in the no CL or HCL groups. No significant between- or within-group differences were found in CV or 6A at any time point.
Conclusion: Preoperative soft CL wear, particularly long-duration daily wear, may be associated with a tendency toward early postoperative endothelial cell density reduction after ICL implantation. Endothelial morphology remained stable, suggesting no evidence of irreversible structural compromise. Careful assessment of preoperative CL wear patterns may help optimize perioperative endothelial monitoring.
Keywords: implantable collamer lens, corneal endothelial cell density, contact lens wear, endothelial cell morphology, early postoperative changes
Introduction
Implantable Collamer Lens (ICL; STAAR Surgical) implantation is widely performed as a phakic intraocular lens procedure for the correction of myopia and astigmatism. It has been established as a refractive surgical option with a broad correction range, high predictability, and a favorable safety profile.1–5 Previous clinical studies have reported that good refractive stability and safety are maintained for over 10 years after ICL implantation,4,5 establishing the procedure as a standard refractive surgical option in clinical practice.1
In recent years, the prevalence of myopia has been particularly notable in East Asia, including Japan, with an increase in highly myopic cases from young to middle-aged populations.6 Consequently, the number of patients seeking ICL implantation is expected to further increase. Many candidates for ICL surgery have a prolonged history of preoperative contact lens (CL) wear, reflecting the substantial global population of CL users.7 Therefore, CL wearing history is a highly common and clinically relevant background factor among patients undergoing ICL implantation.
The corneal endothelium is crucial for maintaining corneal transparency and fluid homeostasis and is indispensable for stable visual function.8 It consists of a monolayer of hexagonal cells that regulates fluid and solute transport between the aqueous humor and corneal stroma.9,10 However, because human corneal endothelial cells have limited regenerative capacity, they are susceptible to aging and various insults such as intraocular surgery and CL wear.11–13
ICL implantation is an intraocular procedure, and although its impact on endothelial cells is generally less pronounced than that of anterior chamber phakic intraocular lenses,14 it involves corneal incision, intraocular manipulation, ICL insertion, and positioning, which may impose physical and metabolic stress on the corneal endothelium.15 In intraocular surgeries such as cataract surgery, an early, transient postoperative decrease in corneal endothelial cell density (CD) is common,16–18 and preoperative endothelial status may influence postoperative outcomes. Previous studies have also reported relatively small early postoperative decreases in endothelial cell density after ICL implantation compared with cataract surgery.15,19
CL wear may disrupt corneal homeostasis, affecting not only corneal shape and epithelium but also the endothelium. Prolonged, daily soft contact lens (SCL) wear may induce chronic hypoxia, which can increase metabolic stress on endothelial cells and potentially result in reduced endothelial cell density and morphological changes such as polymegathism and pleomorphism.20–22 Moreover, SCLs may induce greater hypoxic stress than hard CLs (HCLs) because of lower oxygen transmissibility. Nevertheless, few studies have comprehensively classified CL-wearing conditions and investigated how preoperative CL wear and its specific patterns affect postoperative CD and endothelial morphology after ICL implantation.
Therefore, this study examined the presence and detailed patterns of preoperative CL wear (type, duration, and frequency) and aimed to retrospectively evaluate their effects on postoperative CD and endothelial morphology. Early postoperative endothelial evaluation (1–3 months) may provide important insights into transient surgical stress and the early recovery process of endothelial cells after ICL implantation. Therefore, this study aimed to provide new insights into the clinical significance of CL wearing history in the preoperative assessment for ICL implantation, particularly with respect to endothelial protection. We hypothesized that different preoperative CL wearing patterns, particularly prolonged SCL wear, may influence early postoperative corneal CD after ICL implantation.
Materials and Methods
Study Design and Patients
This retrospective study included 230 eyes from 116 patients (mean age, 34.4 ± 8.24 years) that underwent ICL implantation at Chukyo Eye Clinic between October 1, 2019, and December 1, 2024.
As this was a retrospective exploratory study with a relatively limited sample size, the analyses were performed on an eye-based dataset. Adjustment for inter-eye correlation was not applied, consistent with approaches commonly adopted in similar ophthalmic studies. Based on preoperative interviews, eyes were categorized into four groups by CL wear patterns: no CL wear (No CL group; 78 eyes), hard CL wear (HCL group; 29 eyes), non-daily SCL wear ≤10 h/day (NSCL group, 48 eyes), and daily SCL wear ≥10 h/day (OSCL group, 75 eyes). CD, uncorrected distance visual acuity (UDVA), and manifest refraction spherical equivalent (MRSE) were evaluated retrospectively at baseline, 1 month postoperatively, and 3 months postoperatively.
CL wear history was obtained from a routine pre-visit questionnaire completed by patients and confirmed during the clinical interview.
CL discontinuation before preoperative examinations was performed according to routine clinical practice at our institution. Patients were instructed to discontinue SCL use for 1–2 weeks and HCL use for 3 weeks before the preoperative measurements used for surgical planning. In addition, all patients discontinued CL wear from 3 days before surgery.
Exclusion criteria were CL wear not meeting predefined classification criteria (≥10 h/day but non-daily wear, or ≤10 h/day but daily wear), organic ocular diseases other than refractive error (keratoconus, ocular inflammatory/infectious diseases, cataract, glaucoma, retinal diseases, etc.), history of other ocular surgery, intraoperative deviation from the standard ICL procedure due to unexpected events, or other conditions deemed inappropriate by the surgeon (Figure 1). This study adhered to the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of Chukyo Eye Clinic (approval number: 20241220089). Given the retrospective design, we adopted an opt-out approach approved by the ethics committee of Chukyo Eye Clinic instead of obtaining written informed consent.
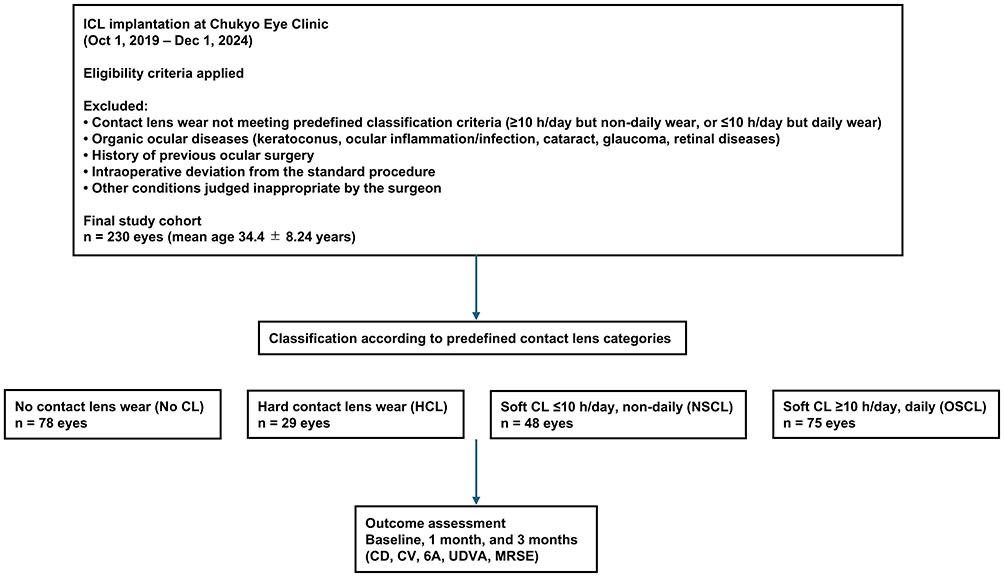 |
Figure 1 Study Flow Diagram Illustrating Patient Selection and Group Allocation. Data are presented as mean ± standard deviation. |
Assessment and Outcome Measures
Preoperative interviews confirmed CL wear status and type (SCL or HCL), wearing duration (≥10 h/day), and wearing frequency (daily wear). Eyes were classified into four groups: No CL (n=78), HCL (n=29), NSCL (n=48), and OSCL (n=75).
The study outcomes included CD, coefficient of variation in cell size (CV), and percentage of hexagonal cells (6A). The primary outcome was the change in CD from baseline to 1 month postoperatively, reflecting early postoperative endothelial changes. The change in CD from baseline to 3 months served as a secondary endpoint to assess the persistence of endothelial cell loss. CV and 6A were analyzed as secondary outcomes to evaluate changes in endothelial morphology from baseline to 1 month and 3 months. UDVA and spherical equivalent were secondary outcomes for refractive stability and were evaluated with both within-group and between-group comparisons (Figure 1).
All corneal endothelial measurements were obtained using a non-contact specular microscope (CEM-530, NIDEK Co., Ltd., Gamagori, Japan).
Surgical Procedure
After ocular surface preparation and draping, a side-port incision was created with a 1.1-mm knife (MANI, Japan), and 1% lidocaine was injected into the anterior chamber. After filling the anterior chamber with an ophthalmic viscosurgical device (Opegan®, Santen Pharmaceutical, Japan), a 3.2-mm corneal single-plane main incision was made using a KOJO knife (BVI, USA), and the ICL was inserted using the dedicated injector.
The ICL was positioned beneath the iris within the ciliary sulcus using an Ichikawa double-ended manipulator (ASICO, USA). The ophthalmic viscosurgical device was removed for 1–2 minutes using an Irrigation/Aspiration (I/A) handpiece (Alcon, USA). Miosis was induced with acetylcholine chloride (Obisot®, Daiichi Sankyo, Japan), and appropriate lens position and wound closure were confirmed. No intraoperative complications occurred, and all surgeries were completed using the standardized procedure. All included procedures were performed by a single surgeon (K.I). Postoperatively, patients received 0.1% betamethasone, 1.5% levofloxacin, and 0.1% bromfenac eye drops for approximately 1 month.
Cases with intraoperative complications or clinically significant postoperative complications were excluded from the analysis.
Statistical Analysis
Between-group comparisons of baseline characteristics and outcomes were performed using the Kruskal–Wallis test. The primary outcome was the change in CD from baseline to 1 month. Changes from baseline to 3 months, endothelial morphology indices (CV and 6A), and refractive outcomes were analyzed as secondary outcomes. When significant, post hoc pairwise comparisons were conducted using the Dunn test with Holm correction.
Within-group longitudinal changes were evaluated using the Friedman test. When significant, post hoc comparisons between baseline and 1 month and between baseline and 3 months were performed using the Wilcoxon signed-rank test with Holm correction for multiple comparisons.
All analyses were two-sided, with p < 0.05 considered statistically significant. Statistical analyses were conducted using EZR (Jichi Medical University, Tochigi, Japan) version 1.68, a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria) that incorporates commonly used biostatistical functions.23
Results
Baseline Characteristics
Among the 230 eyes, 78 were assigned to the No CL group, 29 to the HCL group, 48 to the NSCL group, and 75 to the OSCL group. Age differed significantly across the four groups (Kruskal–Wallis test, p = 0.005). Post hoc analyses demonstrated that the NSCL group was significantly younger than the No CL and HCL groups (Dunn test with Holm correction, p < 0.05), whereas no significant differences were observed between the OSCL group and the others.
UDVA and MRSE also varied significantly among the four groups (p = 0.009 and p = 0.003, respectively). Post hoc analyses indicated that the HCL group had worse preoperative visual acuity and significantly higher myopic refractive error than the No CL group (p < 0.05 for both). No significant between-group differences were observed in baseline CD, CV, or 6A (p = 0.477, p = 0.238, and p = 0.569, respectively) (Table 1).
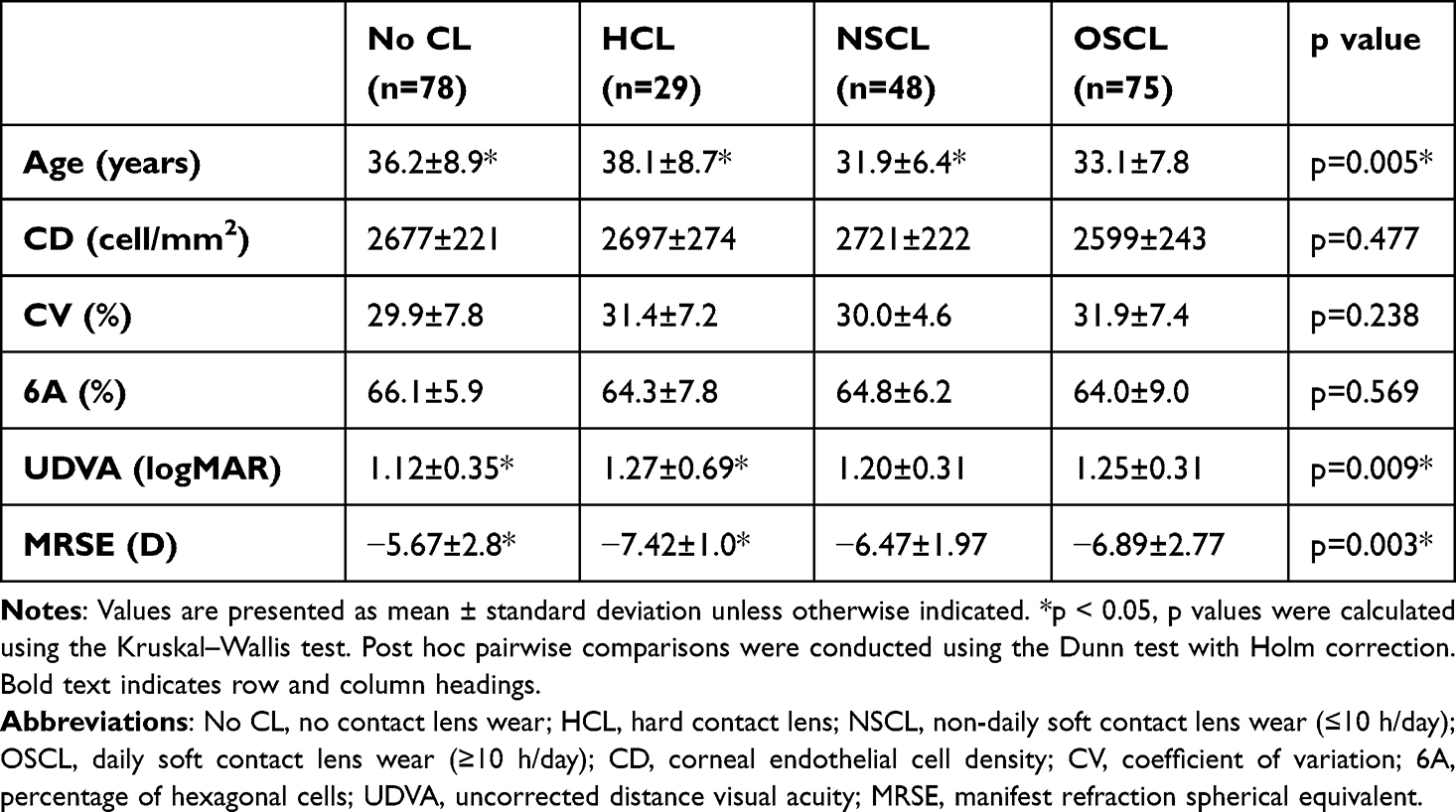 |
Table 1 Baseline Demographic and Ocular Characteristics of the Study Groups |
Changes in Corneal Endothelial Cell Density
No significant between-group differences in changes in CD from baseline to 1 month were observed (Kruskal–Wallis test, p = 0.458). Similarly, no significant between-group differences were observed in the change in CD from baseline to 3 months (p = 0.149). In contrast, within-group analyses revealed significant CD reductions at 1 month in the NSCL and OSCL groups (Friedman test: p = 0.04 and p = 0.01). Post hoc Wilcoxon signed-rank tests with Holm correction confirmed significant decreases from baseline to 1 month in both groups (both p = 0.04). In addition, the OSCL group exhibited persistent CD reduction at 3 months (p = 0.04). No significant changes in CD were observed at either postoperative time point in the No CL and HCL groups (p = 0.37 and p = 0.725, respectively) (Table 2 and Figure 2).
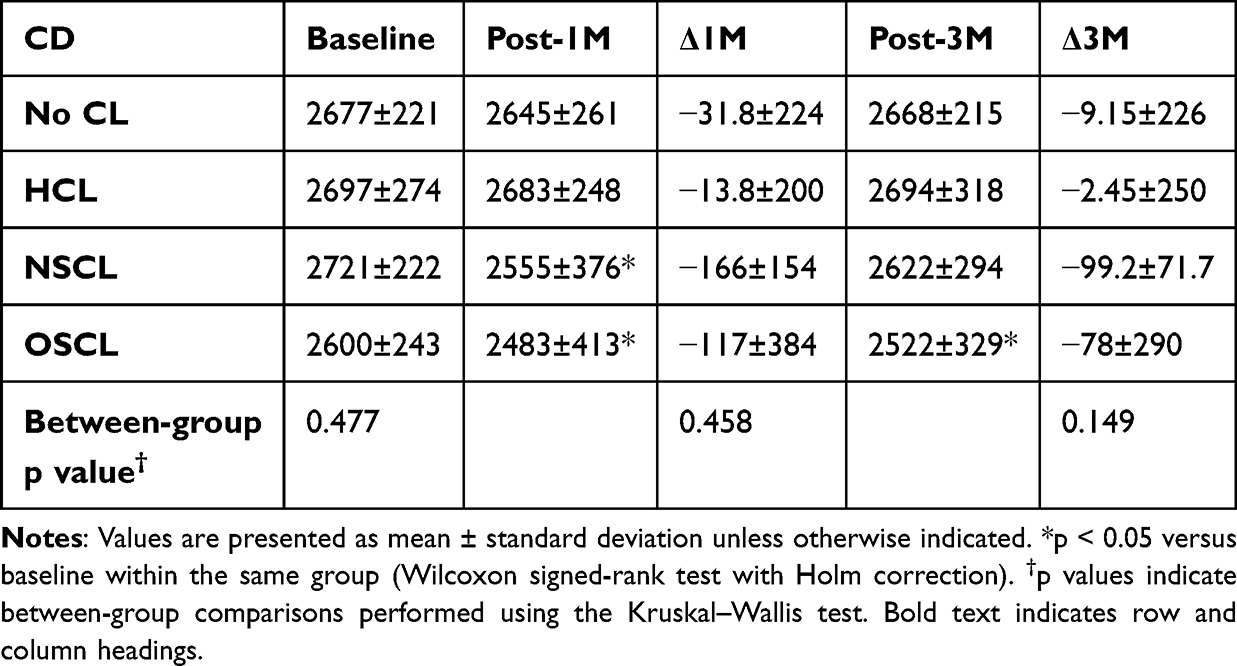 |
Table 2 Changes in Corneal Endothelial Cell Density from Baseline to 1 and 3 Months Postoperatively |
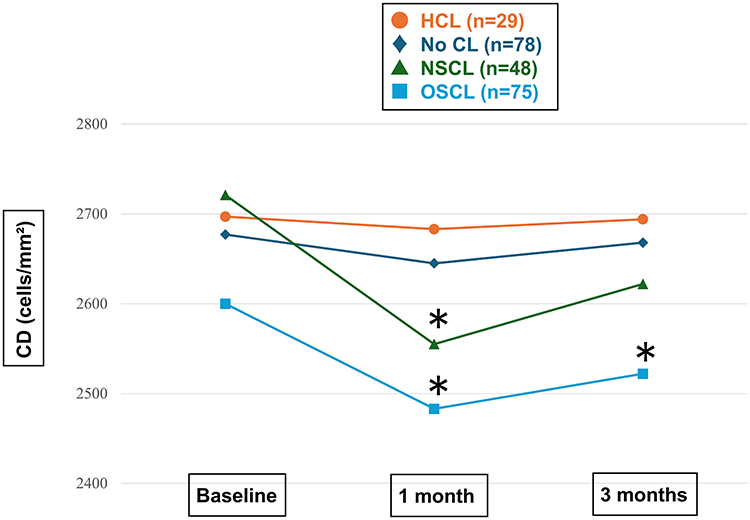 |
Figure 2 Longitudinal Changes in Corneal Endothelial Cell Density (CD) After Implantable Collamer Lens (ICL) Implantation Stratified by Contact Lens Wearing History. No significant between-group differences were observed at any time point (Kruskal–Wallis test). Within-group comparisons were performed using the Wilcoxon signed-rank test. *p < 0.05. |
Changes in Coefficient of Variation
No significant between-group differences were observed in the change in CV from baseline to 1 month (Kruskal–Wallis test, p = 0.627) or from baseline to 3 months (p = 0.715). Within-group analyses also showed no significant longitudinal changes in CV in any group (Table 3 and Figure 3).
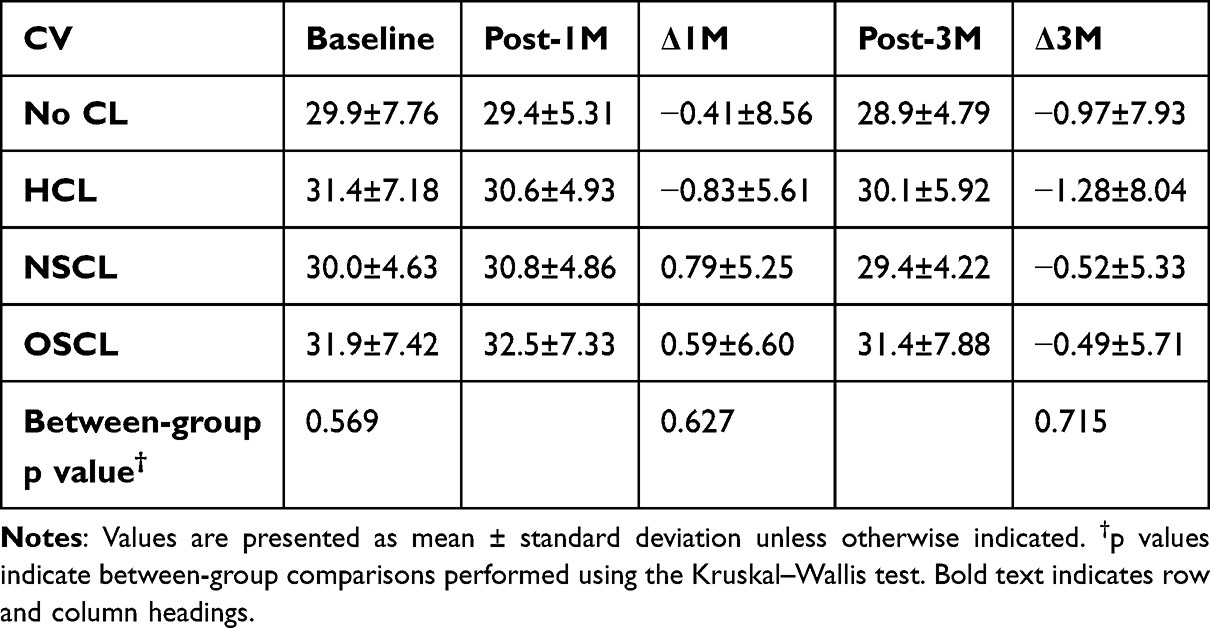 |
Table 3 Changes in Coefficient of Variation from Baseline to 1 and 3 Months Postoperatively |
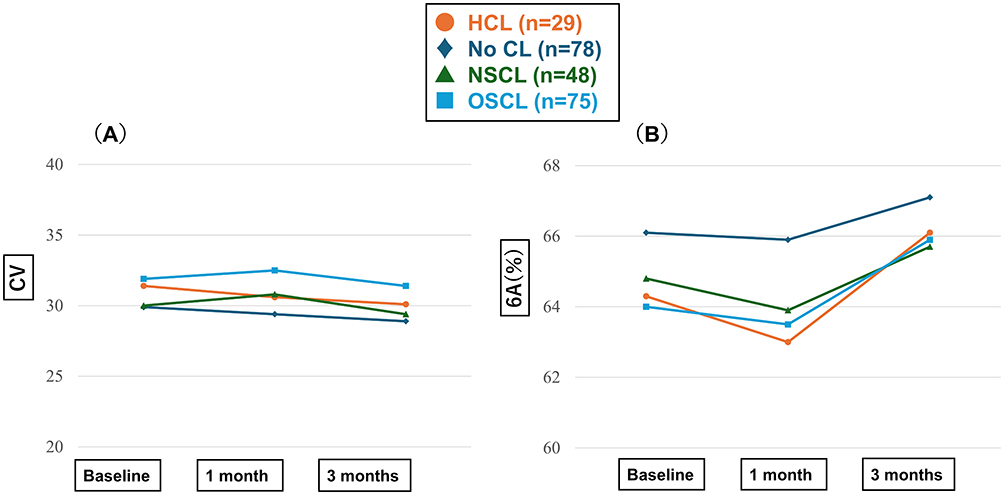 |
Figure 3 Longitudinal Changes in Corneal Endothelial Morphology Parameters (CV and 6A) After ICL Implantation. (A) Coefficient of Variation (CV). No significant between-group differences were detected at any time point (Kruskal–Wallis test). No significant within-group differences were observed over time (Wilcoxon signed-rank test). (B) Percentage of Hexagonal Cells (6A). No significant between-group differences were observed at any time point (Kruskal–Wallis test). No significant within-group differences were observed over time (Wilcoxon signed-rank test). |
Changes in Percentage of Hexagonal Cells
No significant between-group differences were observed in the change in 6A from baseline to 1 month (Kruskal–Wallis test, p = 0.818) or from baseline to 3 months (p = 0.918). Within-group analyses also demonstrated no significant changes in 6A over time in any group (Table 4 and Figure 3).
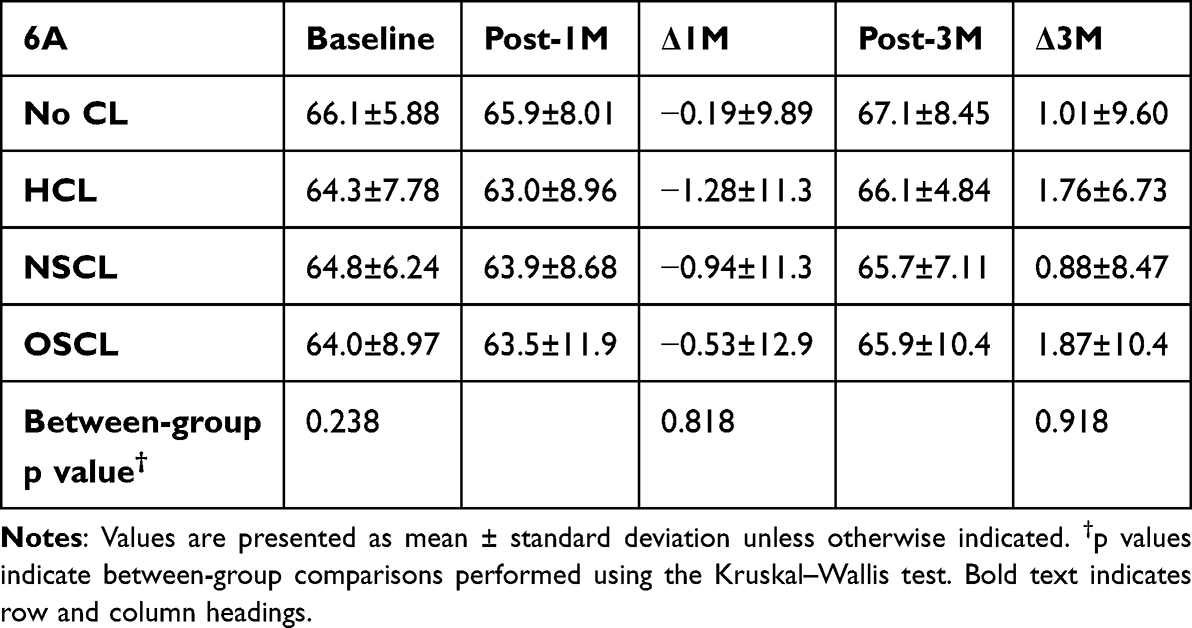 |
Table 4 Changes in Percentage of Hexagonal Cells from Baseline to 1 and 3 Months Postoperatively |
Changes in Uncorrected Distance Visual Acuity and Manifest Refraction Spherical Equivalent
Within-group analyses showed significant improvements in UDVA and MRSE at 1 month, which were sustained at 3 months compared with baseline (all p < 0.05). No significant changes occurred between 1 and 3 months (p > 0.05). Between-group comparisons revealed no statistically significant differences at any time point (p > 0.05) (Tables 5 and 6).
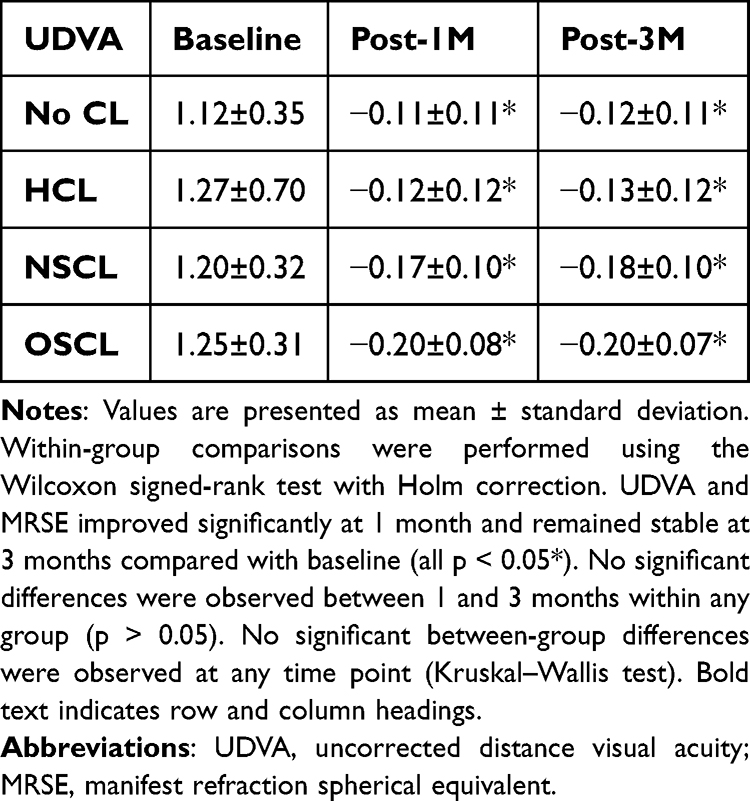 |
Table 5 Changes in UDVA After ICL Implantation |
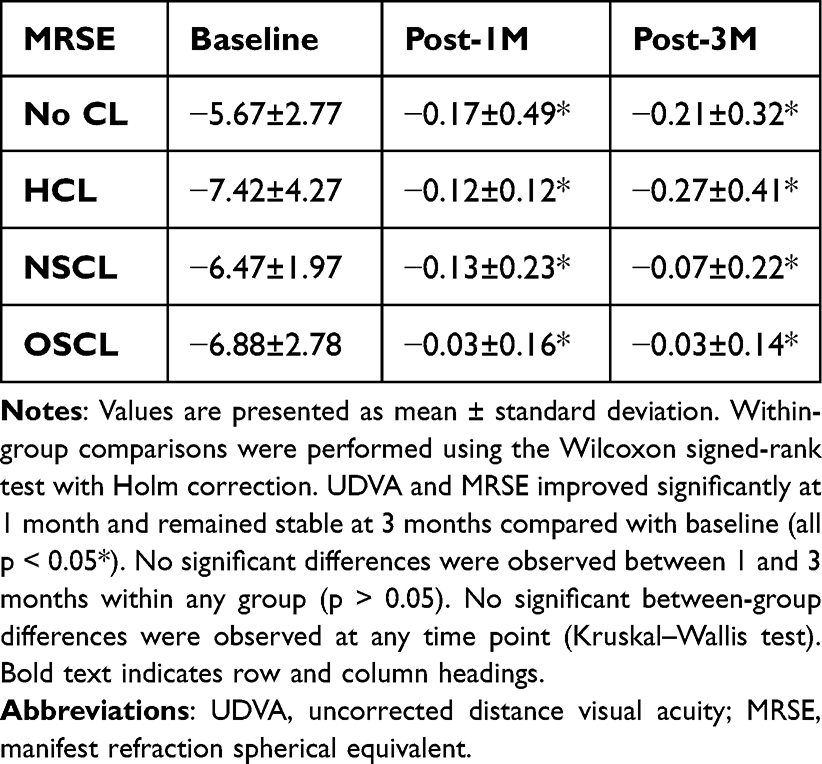 |
Table 6 Changes in MRSE After ICL Implantation |
Discussion
This study evaluated the impact of preoperative CL wearing patterns on early postoperative CD and endothelial morphology after ICL implantation. Changes in CD from baseline to 1 month and 3 months did not differ significantly among the four groups at either time point. However, within-group analyses demonstrated significant early postoperative CD reduction in SCL-wearing groups, with persistent CD reduction at 3 months in the OSCL group. Because the primary between-group comparisons were not statistically significant, these findings should be interpreted cautiously. Carlson et al reported that CL-wearing eyes, regardless of lens type, had a higher risk of reduced CD, with significantly increased CV and decreased 6A compared with non-wearing eyes.9 Aljaberi et al also reported that longer-term SCL wear was associated with a higher risk of reduced CD, increased CV, and decreased 6A.22 In the present study, although the OSCL group tended to have lower baseline CD than other groups, the between-group comparison did not reach statistical significance. Baseline CD, CV, and 6A did not differ significantly among the four groups, and no findings suggested OSCL-specific preoperative endothelial impairment. This may reflect inter-individual variability in endothelial cell density as well as the relatively limited sample size in each subgroup.
Although significant between-group differences were observed in age, UDVA, and refractive error at baseline, these variables were not significantly imbalanced in the OSCL group. Because this was a retrospective exploratory study with a relatively limited sample size, multivariable adjustment for these baseline differences was not performed. Therefore, the observed tendency toward lower baseline endothelial indices in the OSCL group is unlikely to be attributable primarily to age or refractive status.
These results should be interpreted considering the retrospective design and the limited sample size, as well as inter-individual variability in endothelial reserve. Accordingly, it remains difficult to draw definitive conclusions regarding the association between OSCL wear and baseline CD based on the present data alone. Larger prospective studies are warranted. The finding that significant early postoperative CD reduction occurred only in the SCL groups may suggest that the corneal endothelium in SCL wearers could have been subjected to chronic stress preoperatively. Long-term SCL wear may induce chronic hypoxia, increasing metabolic demand on endothelial cells and potentially rendering endothelial function more vulnerable.20–22 Our findings suggest that transient physical and metabolic stress during ICL implantation may partially explain the observed early postoperative CD decline. In the OSCL group, particularly, longer-duration daily wear may have accumulated greater endothelial burden, possibly explaining the persistent reduction observed at 3 months.
ICL implantation is an intraocular procedure involving corneal incision and anterior chamber manipulation, and early postoperative transient CD reduction has been reported.15,19 In cataract surgery, early postoperative endothelial losses of approximately 11.5–12.3% at 1 month and 11.7–12.4% at 3 months have been reported, with no significant changes in CV or hexagonality.18 In contrast, endothelial loss after ICL implantation has been reported to be approximately 2.1% at 3 months.19 Considering our results (absolute CD reduction of approximately 9–99 cells/mm2, corresponding to 0.09–3.64%) together with previous reports, ICL implantation may be associated with a lower rate of postoperative endothelial loss than that observed after cataract surgery.
Long-term outcomes after ICL implantation have demonstrated endothelial loss rates of 7.5% at 5 years24 and 6.2% at 8 years.25 Such long-term data support the preservation of corneal health after ICL implantation. Longer follow-up in our cohort is therefore warranted. In this study, no significant changes were observed in endothelial morphology indices (CV and 6A). This suggests that the observed CD reduction was not accompanied by irreversible structural endothelial damage and may represent a relatively reversible change. Edelhauser et al reported that although CD decreased over 3 years after ICL implantation, CV tended to decrease, and hexagonality increased slightly.19 They proposed that postoperative CD reduction may be better explained by long-term corneal remodeling rather than continuous endothelial cell loss. Our findings are consistent with this interpretation; however, because our follow-up was limited to 3 months, longer observation may reveal different trajectories for CV and 6A.
UDVA and MRSE improved in all groups and remained stable after 1 month. In addition, no significant between-group differences were observed for these visual and refractive outcomes. Therefore, within the observation period, the observed endothelial cell density changes were not associated with clinically meaningful deterioration in visual function. This finding supports the safety and efficacy of ICL implantation.1
This study has some limitations. First, this study relied on self-reported CL wearing history, including daily wearing duration, which may be subject to recall bias. Second, detailed information regarding CL material, oxygen transmissibility, and duration of wear was unavailable. This may also have contributed to heterogeneity within the CL groups, particularly among SCL users. Third, high vault has been identified as a potential risk factor for CD reduction after ICL implantation.26 However, detailed analyses of ICL sizing and postoperative vault were not performed in the present study. Because of the retrospective design, stratified analyses or longitudinal evaluation of vault were not included. Finally, the follow-up period was limited to 3 months, and long-term endothelial safety could not be assessed. Therefore, the present findings should be interpreted as short-term postoperative endothelial changes. Future prospective studies incorporating vault as a key variable with longer follow-up duration are needed to further clarify endothelial outcomes after ICL implantation.
Conclusions
Preoperative SCL wear, particularly long-duration daily use, may be associated with a tendency toward early postoperative reduction in corneal CD after ICL implantation. In contrast, endothelial morphology indices remained stable, and no evidence of irreversible structural endothelial damage or associated visual functional decline was observed.
However, because no significant between-group differences were identified, these findings should be interpreted cautiously, and should be considered exploratory and hypothesis-generating rather than definitive. In addition, the present results reflect short-term postoperative outcomes up to 3 months and do not necessarily indicate long-term endothelial safety. Therefore, careful assessment of preoperative CL wearing history—especially SCL wearing duration and frequency—and close early postoperative endothelial monitoring may be advisable in patients with a high CL wearing burden.
Abbreviations
ICL, implantable Collamer lens; CL, contact lens; CD, corneal endothelial cell density; CV, coefficient of variation; 6A, percentage of hexagonal cells; HCL, hard contact lens; NSCL, non-daily soft contact lens wear (≤10 h/day); OSCL, daily soft contact lens wear (≥10 h/day); UDVA, uncorrected distance visual acuity; MRSE, manifest refraction spherical equivalent; I/A, irrigation/aspiration.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study adhered to the tenets of the Declaration of Helsinki and received approval from the institutional ethics committee (approval number: 20241220089). Because this study was retrospective, an opt-out approach approved by the ethics committee was used instead of the acquisition of written informed consent.
Acknowledgments
The authors thank the clinical staff of Chukyo Eye Clinic for their assistance with patient care and data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
Satoshi Gotoda reports personal fees from Lumenis Be Ltd., personal fees from Santen Pharmaceutical Co., Ltd., personal fees from Senju Pharmaceutical Co., Ltd., personal fees from Tomey Corporation, outside the submitted work. Kazuo Ichikawa reports grants, personal fees, consulting/lecture fee from STAAR Surgical, non-financial support, provision of equipment from Rxsight, personal fees, consulting/lecture fee from Alcon, personal fees from KOWA Company, Ltd., personal fees from WAKAMOTO PHARMACEUTICAL CO., LTD., personal fees from Lumenis Japan Co. Ltd., outside the submitted work; In addition, Dr Kazuo Ichikawa has a patent 2025-232333 pending to None. The authors report no conflicts of interest related to this work.
References
1. Packer M. Meta-analysis and review: effectiveness, safety, and central port design of the intraocular collamer lens. Clin Ophthalmol. 2016;10:1059–11. doi:10.2147/OPTH.S111620
2. Russo A, Filini O, Mertens E, et al. Immediate sequential bilateral implantable collamer lens surgery is safe and effective. J Refract Surg. 2024;40(5):e313–e320. doi:10.3928/1081597X-20240326-01
3. Parkhurst G, Brinton JP, Faulkner A, et al. Three year results from the United States FDA prospective multicenter clinical study of the EVO/EVO+ implantable collamer lens. Clin Ophthalmol. 2025;19:3237–3248. doi:10.2147/OPTH.S537739
4. Alfonso-Bartolozzi B, Fernández-Vega-Cueto L, Lisa C, Palacios A, Madrid-Costa D, Alfonso JF. Ten-year follow-up of posterior chamber phakic intraocular lens with central port design in patients with low and normal vault. J Cataract Refract Surg. 2024;50(5):441–447. doi:10.1097/j.jcrs.0000000000001379
5. Chung B, Choi JY, Kang DSY, Kim K, Kim BY, Kim TI. Ten-year clinical outcomes of V4c implantable collamer lens implantation: longitudinal analysis of visual acuity, endothelial cell density, and vault dynamics. Am J Ophthalmol. 2025;269:1–10. doi:10.1016/j.ajo.2024.08.007
6. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
7. Dumbleton K, Caffery B, Dogru M, et al. The TFOS International Workshop on Contact Lens Discomfort: report of the subcommittee on epidemiology. Invest Ophthalmol Vis Sci. 2013;54(11):TFOS20–TFOS36. doi:10.1167/iovs.13-13125
8. Holden BA, Sweeney DF, Vannas A, Nilsson KT, Efron N. Effects of long-term extended contact lens wear on the human cornea. Invest Ophthalmol Vis Sci. 1985;26(11):1489–1501.
9. Carlson KH, Bourne WM, Brubaker RF. Effect of long-term contact lens wear on corneal endothelial cell morphology and function. Invest Ophthalmol Vis Sci. 1988;29(2):185–193.
10. Sweeney DF. Have silicone hydrogel lenses eliminated hypoxia? Eye Contact Lens. 2013;39(1):53–60. doi:10.1097/ICL.0B013e31827c7899
11. Harvitt DM, Bonanno JA. Re-evaluation of the oxygen diffusion model for predicting minimum contact lens Dk/t values needed to avoid corneal anoxia. Optom Vis Sci. 1999;76(10):712–719. doi:10.1097/00006324-199910000-00023
12. Dumbleton KA, Chalmers RL, Richter DB, Fonn D. Vascular response to extended wear of hydrogel lenses with high and low oxygen permeability. Optom Vis Sci. 2001;78(3):147–151. doi:10.1097/00006324-200103000-00006
13. Chalmers RL, Dillehay S, Long B, et al. Impact of previous extended and daily wear schedules on signs and symptoms with high Dk lotrafilcon A lenses. Optom Vis Sci. 2005;82(6):549–554. doi:10.1097/00006324-200506000-00019
14. Saif PS, Okasha MG, Mahmoud H, Samir A, Abdelmonagy Ibrahim MA. Impact of Veriflex and ICL on corneal biomechanics and endothelial cell density. Sci Rep. 2025;15(1):31553. doi:10.1038/s41598-025-14330-3
15. Yang W, Zhao J, Sun L, et al. Four-year observation of the changes in corneal endothelium cell density and correlated factors after Implantable Collamer Lens V4c implantation. Br J Ophthalmol. 2021;105(5):625–630. doi:10.1136/bjophthalmol-2020-316144
16. Hayashi K, Hayashi H, Nakao F, Hayashi F. Risk factors for corneal endothelial injury during phacoemulsification. J Cataract Refract Surg. 1996;22(8):1079–1084. PMID: 8915805. doi:10.1016/S0886-3350(96)80121-0
17. Dewan T, Malik PK, Kumari R. Comparison of effective phacoemulsification time and corneal endothelial cell loss using 2 ultrasound frequencies. J Cataract Refract Surg. 2019;45(9):1285–1293. doi:10.1016/j.jcrs.2019.04.015
18. Vital MC, Jong KY, Trinh CE, Starck T, Sretavan D. Endothelial cell loss following cataract surgery using continuous curvilinear capsulorhexis or precision pulse capsulotomy. Clin Ophthalmol. 2023;17:1701–1708. doi:10.2147/OPTH.S411454
19. Edelhauser HF, Sanders DR, Azar R, Lamielle H; ICL in Treatment of Myopia Study Group. Corneal endothelial assessment after ICL implantation. J Cataract Refract Surg. 2004;30(3):576–583. doi:10.1016/j.jcrs.2003.09.047
20. Bourne WM, Holtan SB, Hodge DO. Morphologic changes in corneal endothelial cells during 3 years of fluorocarbon contact lens wear. Cornea. 1999;18(1):29–33. doi:10.1097/00003226-199901000-00006
21. Patel SV, McLaren JW, Hodge DO, Bourne WM. Confocal microscopy in vivo in corneas of long-term contact lens wearers. Invest Ophthalmol Vis Sci. 2002;43(4):995–1003.
22. Aljaberi HA, Rahmani S, Muhammad GA. Effect of soft contact lens wear on corneal endothelial cell characteristics. Cont Lens Anterior Eye. 2025;48(5):102441. doi:10.1016/j.clae.2025.102441
23. Kanda Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013;48(3):452–458. doi:10.1038/bmt.2012.244
24. Alfonso JF, Baamonde B, Fernández-Vega L, Fernandes P, González-Méijome JM, Montés-Micó R. Posterior chamber collagen copolymer phakic intraocular lenses to correct myopia: five-year follow-up. J Cataract Refract Surg. 2011;37(5):873–880. doi:10.1016/j.jcrs.2010.11.040
25. Igarashi A, Shimizu K, Kamiya K. Eight-year follow-up of posterior chamber phakic intraocular lens implantation for moderate to high myopia. Am J Ophthalmol. 2014;157(3):532–9.e1. doi:10.1016/j.ajo.2013.11.006
26. Choi H, Lee SY, Lee BY, Cho HJ, Yoo TK. Paired-eye comparison of endothelial cell density and vault height after implantable collamer lens implantation. Sci Rep. 2024;14(1):27643. doi:10.1038/s41598-024-79613-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.