Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Adaptation and Validation of the Iraqi Diabetic Health Literacy Questionnaire (IDHLQ): A Rasch and Factor Analysis Study
Authors Al-Qerem W ![]() , Alsajri AH, Jarab A
, Alsajri AH, Jarab A ![]() , Eberhardt J
, Eberhardt J ![]() , Baaj R, Sawaftah L, Al-Sa’di L, Mahdi II NS, Hasan Agha MI
, Baaj R, Sawaftah L, Al-Sa’di L, Mahdi II NS, Hasan Agha MI ![]() , Hassan II AM, Atiya II BA
, Hassan II AM, Atiya II BA
Received 29 October 2025
Accepted for publication 5 February 2026
Published 12 February 2026 Volume 2026:19 572563
DOI https://doi.org/10.2147/DMSO.S572563
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ernesto Maddaloni
Walid Al-Qerem,1 Alaa Hussein Alsajri,2 Anan Jarab,3 Judith Eberhardt,4 Ramah Baaj,5 Lama Sawaftah,1 Lujain Al-Sa’di,1 Nabaa Saeed Mahdi II,2 Mhd Isam Hasan Agha,6 Ayat Mohamed Hassan II,2 Batoul Ayad Atiya II2
1Department of Pharmacy, Faculty of Pharmacy, Al-Zaytoonah University of Jordan, Amman, Jordan; 2Department of Pharmacy, Al-Rasheed University College, Baghdad, Iraq; 3Department of Clinical Pharmacy, Faculty of Pharmacy, Jordan University of Science and Technology, Irbid, 22110, Jordan; 4Department of Psychology, School of Social Sciences, Humanities and Law, Teesside University, Middlesbrough, UK; 5Department of Biochemistry, Faculty of Pharmacy, Alrasheed Private University, Daraa, Syria; 6Department of Pharmacy, Faculty of Pharmacy, Damascus University, Damascus, Syria
Correspondence: Mhd Isam Hasan Agha, Email [email protected]
Introduction: Diabetes prevalence in Iraq is high, yet culturally adapted and psychometrically validated health literacy (HL) tools for people with diabetes remain limited. The Jordanian Diabetic Health Literacy Questionnaire (JDHLQ) assesses informational and communicative HL but omits numeracy.
Purpose: To adapt and validate the Iraqi Diabetic Health Literacy Questionnaire (IDHLQ), based on the JDHLQ, which incorporates a numeracy domain, for use among adults with type 2 diabetes in Iraq.
Patients and Methods: A cross-sectional study recruited 473 adults with type 2 diabetes from endocrinology clinics across Iraq. Participants were 52.7% female with a median age of 50 years (IQR: 31– 60). The 11-item IDHLQ was validated using exploratory factor analysis, Rasch modeling, and Cronbach’s alpha. Linear regression examined sociodemographic predictors.
Results: A three-factor model emerged, representing informational, numeracy, and communicative health literacy, with internal consistency ranging from α = 0.70 to 0.86. Rasch analysis showed item separation reliability of 0.87– 0.95 and person reliability of 0.65– 0.82. The median score was 33 (IQR: 28– 36) out of 44. Monthly income predicted HL (β = 0.16, p = 0.003), while age, gender, education, and marital status were nonsignificant.
Conclusion: The adapted IDHLQ is a reliable and valid instrument for assessing multidimensional diabetic health literacy among Iraqi adults. Its use in clinical and public health settings could inform patient education strategies and guide policy development to reduce disparities in diabetes outcomes.
Keywords: diabetes mellitus, health literacy, IDHLQ, validation, Iraq
Introduction
Diabetes mellitus (DM) is a growing global public health problem and one of the most common chronic diseases, with prevalence projected to reach 642 million by 2040.1 The World Health Organization (WHO) defines DM as a chronic metabolic disorder characterized by high blood glucose levels and impaired insulin production, function, or both.2 In the Middle East and North Africa, diabetes is estimated to affect more than 70 million people by 2040.1 In Iraq, as in many countries in the region, diabetes rates have increased significantly. Estimates indicate that about 17% of adults are affected, with 8.1% undiagnosed. This highlights the urgent need for effective disease management strategies that emphasize patient-centered education and active involvement.3
The effective management of type 2 diabetes mellitus (T2DM) depends on patients’ ability to understand and act on health information, a concept known as health literacy (HL).4 Diabetic HL and numeracy involve a wide range of cognitive and social skills, including understanding educational materials, communicating with healthcare providers, and performing numerical tasks such as adjusting medication doses, calculating carbohydrate intake, and interpreting blood glucose monitoring results.5 The burden of managing T2DM and its potential for severe complications such as blindness, heart attacks, strokes, kidney failure, reduced lung function, and lower extremity amputations,6–9 highlights the significant impact of HL and numeracy in the proper management of T2DM. Effective disease control requires consistent self-care efforts, including maintaining a healthy diet, adhering to prescribed medications, exercising regularly, and achieving optimal blood sugar control.10,11 HL and numeracy play a pivotal role in enhancing patients’ ability to understand complex aspects of their disease management, improve their emotional well-being, and gain the essential knowledge needed to manage their condition. Existing evidence consistently demonstrates that inadequate health literacy and numeracy are associated with poorer medication adherence, suboptimal glycemic control, increased complication rates, and higher healthcare utilization.12 On the other hand, interventions targeting diabetes health literacy and numeracy have been shown to improve self-care behaviors, treatment adherence, and clinical outcomes, supporting the need for culturally adapted and psychometrically validated assessment tools.13
Previous studies have also demonstrated that higher levels of HL are linked to more informed decision-making and better quality of life.14,15
Despite the critical role of HL in diabetes outcomes, there is a lack of culturally and linguistically tailored tools to assess HL in Arabic-speaking populations such as the Iraqi population. Moreover, the currently available tools often fail to capture the full spectrum of these skills. The Jordanian Diabetic Health Literacy Questionnaire (JDHLQ) was developed and validated to address this gap within the Jordanian context, covering two important domains: the informative domain, which assesses the ability to understand and evaluate diabetes-related information, and the communicative domain, which evaluates patients’ ability to express and exchange information with healthcare providers.13 While the JDHLQ represents a significant advancement in enhancing HL among Arabic-speaking diabetic patients, it does not assess numeracy, which is a fundamental component of diabetic self-care.12 Additionally, the generalizability of this tool to other Arabic-speaking populations, such as Iraq, with variations in healthcare systems, remains to be explored. Therefore, cross-cultural validation is crucial before the JDHLQ items can be effectively used in Iraq, as even subtle cultural and linguistic differences can affect how respondents understand questionnaire items.16
Previous research has demonstrated that even when questionnaires are developed in linguistically similar settings, cross-cultural adaptation remains essential due to differences in healthcare systems, educational structures, and patient–provider interactions.17 According to an established methodological guideline for the process of cross-cultural adaptation, translation alone is insufficient, as self-report health measures are highly influenced by healthcare organization, patient education programs, and cultural norms.16 Studies that have adapted diabetes-related health literacy tools have shown that variations in diabetes education, access to healthcare, and communication practices can significantly influence how patients interpret questionnaire items.13,18 There are notable differences between diabetes education and care practices in Jordan and Iraq. In Iraq, the development and validation of a culturally specific diabetes self-management education and support (DSMES) program has been driven by the recognition that poor diabetes knowledge among patients is largely attributable to the lack of existing structured education resources and support programs.19 In contrast, diabetes care and education in Jordan are more systematically incorporated into routine clinical practice, evidenced by documented quality of care study that describe organized patient education, routine follow-up in which more than 80% of patients reported that they could reach the health facility easily, and team-based support.20
Given Iraq’s high prevalence of diabetes and the need for better management strategies, there is a clear need for a validated tool that reflects the full range of HL skills. Therefore, the present study aimed to validate the Iraqi Diabetic Health Literacy Questionnaire (IDHLQ) for use among Iraqi adults with type 2 diabetes, through adapting the existing Jordanian Diabetic Health Literacy Questionnaire (JDHLQ) and expanding its scope by incorporating a numeracy domain relevant to diabetes self-management. In addition, the study evaluated the questionnaire’s psychometric properties using exploratory factor analysis and Rasch modeling. To the best of our knowledge, this is the first study to cross-culturally adapt and validate a multidimensional diabetic health literacy instrument for the Iraqi population while explicitly integrating numeracy as a core component, providing a comprehensive tool that captures informational, communicative, and numeracy skills essential to effectively assess diabetes self-management. This expanded tool offers a more comprehensive and culturally relevant measure, enabling clinicians to identify patients with limited HL and implement tailored interventions to improve diabetes management.
Materials and Methods
Participants and Data Collection
This cross-sectional study involved recruiting diabetic patients who were visiting endocrinology outpatient clinics at various hospitals in different regions of Iraq. Data collection was conducted between January and August 2025 through face-to-face administration of the questionnaire by trained researchers during routine clinic visits. Participants completed the questionnaire independently, with assistance provided when necessary to clarify item wording without influencing responses. Clinical data (including HbA1c values) were obtained from patients’ medical records on the day of the clinic visit.
Participants were selected using convenience sampling. The inclusion criteria included a confirmed diagnosis of type 2 diabetes mellitus for at least one year, age ≥18 years, and the ability to read and understand Arabic. Patients with cognitive impairment, severe acute illness, or incomplete questionnaire responses were excluded. The final dataset included 473 adults with type 2 diabetes. Prior to enrollment, the study’s aims and protocol were explained to participants, and they were informed of their right to withdraw from the study at any time. They were assured that the information collected would remain confidential. No personally identifiable information (such as names, addresses, or contact details) was recorded in the study database and questionnaires were stored in locked cabinets accessible only to the research team. All participants signed an informed consent form. The following assumptions were made during data collection: (1) participants provided honest and accurate responses, and (2) DM patients attending the clinic were representative of adults with type 2 diabetes receiving outpatient care in Iraq. Ethical approval was obtained from the Institutional Review Board and the Deanship of Research at Al-Rasheed University (reference number RUCPD10012507). This study followed the Declaration of Helsinki ethical guidelines.
Data Collection and Study Instruments
The questionnaire had two parts. The first collected demographic information, and the second included the Iraqi Diabetic Health Literacy Questionnaire (IDHLQ). The IDHLQ comprised three domains. The first domain, informational health literacy, evaluated patients’ ability to assess, understand, and use information about T2DM. The second domain, numeracy, assessed their ability to perform numerical tasks such as interpreting carbohydrate content on food labels, understanding risk probabilities, and determining whether blood sugar levels were within the normal range. The third domain, communicative health literacy, assessed patients’ ability to effectively communicate about their disease. This included their capacity to explain the rationale for a diabetic diet, describe their own condition, and ask healthcare providers pertinent questions about T2DM. The questionnaire included eleven items on a 1–4 Likert scale, with higher scores indicating greater ability. The maximum possible score was 44. Additional information was retrieved from patients’ files, including HbA1c readings on the day of the visit and current medications.
Sample Size Calculation
The determination of an adequate sample size for factor analysis was guided by the subject-to-item ratio, a common heuristic in psychometric research. For this study, a ratio of 20 participants per questionnaire item was adopted, as recommended for achieving stable factor structures.21 Because the instrument contained 11 items, this guideline indicated a minimum recruitment target of 220 participants. To enhance reliability, generalizability, and validity, the present study recruited a larger sample of 473 participants.
Tool Validation
Content and face validity were evaluated by an expert panel consisting of two endocrinologists and a clinical pharmacist. A pilot study with diabetic patients was conducted to confirm the questionnaire’s clarity and comprehensibility for Iraqi participants. Data from the pilot study were excluded from the final statistical analysis. Exploratory Factor Analysis (EFA) was conducted to evaluate the questionnaire’s construct validity, and Cronbach’s alpha values were examined to ensure internal consistency for each factor. Rasch analysis was also performed to assess the tool’s ability to distinguish between patients’ abilities and to evaluate the difficulty level of each questionnaire item.
Statistical Analysis
Statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS) version 26 and R software (version 4.3.3), with the Test Analysis Modules (TAM, v. 4.1–4) and Psycho (v. 0.6–1) packages. The factorability of the dataset was examined with a polychoric correlation matrix. Adequacy was assessed using the Kaiser–Meyer–Olkin (KMO) index and per-variable Measures of Sampling Adequacy (MSA). Bartlett’s test of sphericity was also applied to this matrix. The optimal number of factors was determined through parallel analysis. Items were removed if they had communalities below 0.3, factor loadings below 0.4, or significant cross-loadings (loadings greater than 0.4 on more than one factor).
Subsequently, a multi-factorial Rasch analysis for polytomous responses was performed. To evaluate the model’s utility, person and item separation reliability indices were computed. Model fit was further assessed using infit and outfit mean square (MSQ) statistics, with values between 0.5 and 1.5 considered acceptable At the item level, Thurstonian thresholds were calculated to verify the logical ordering of response categories. A Differential Item Functioning (DIF) analysis was conducted to examine gender-based variance, using Z-statistics to compare item difficulty between the sexes relative to the standard error. Finally, Targeting was examined using Wright (person–item) maps, a standard Rasch graphical diagnostic that locates respondents and item/threshold parameters on the same logit metric to evaluate coverage of the latent trait and the alignment between respondent ability and item difficulty.
Floor and ceiling effects were examined for the total IDHLQ score and each domain, defined as >15% of respondents achieving the minimum or maximum possible score. Linear regression was used to model IDHLQ score. Predictors included age (years), gender, educational level (low vs high), marital status (unmarried vs married), private insurance (yes vs no), and monthly income coded 1–3 (low to high) to test for a linear trend. Model assumptions were assessed using standardized residuals versus fitted values, normal P–P plots, studentized deleted residuals, leverage, Cook’s distance, and the Durbin–Watson statistic. Collinearity was assessed using tolerance and variance inflation factors (VIF), with a threshold of VIF > 5. A two-sided α = 0.05 was used.
Results
Table 1 presents participants’ sociodemographic profiles. A total of 473 diabetic patients were included in the study; the majority were female (52.7%), with a median age of 50 years (IQR: 31–60). Most participants had a university or college degree (58%), were married (69.9%), and did not have private health insurance (89.2%). Finally, 46.7% of participants were on insulin.
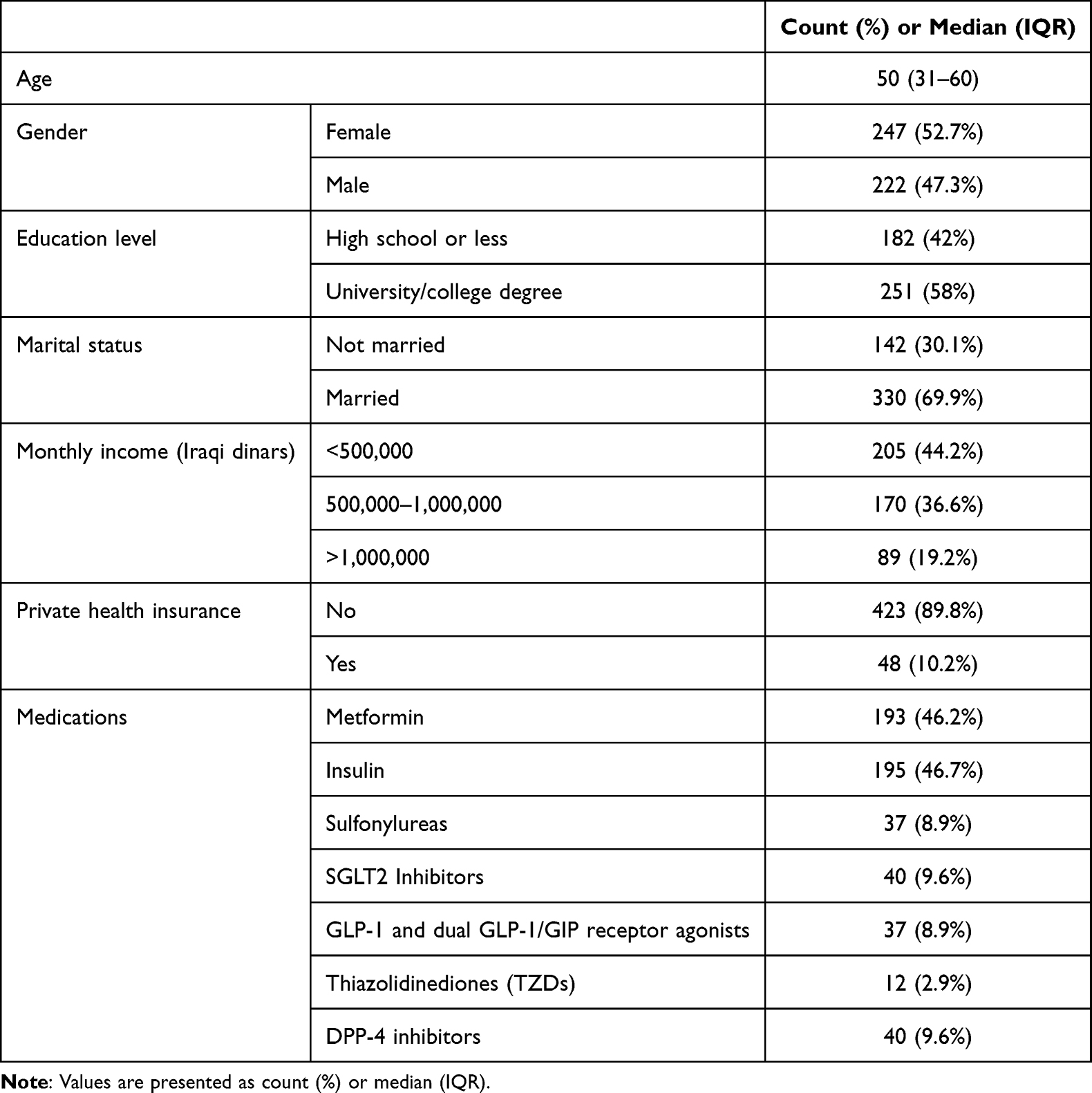 |
Table 1 Participant Socioeconomic Profiles |
Participants’ responses to the health literacy items are shown in Table 2. For the informational factor, the highest “Often” response was to the item “Do you understand the information from the doctor about how to control diabetes?” (49.5%). For the numeracy factor, the highest “Often” response was “Do you have the ability to know whether your blood sugar level is within the normal range?” (39.1%). For the communicative factor, the highest “Often” response was “Do you ask your doctor diabetes-related questions?” (45.7%). The median health literacy score was 33 (IQR: 28–36) out of a maximum of 44 (75%).
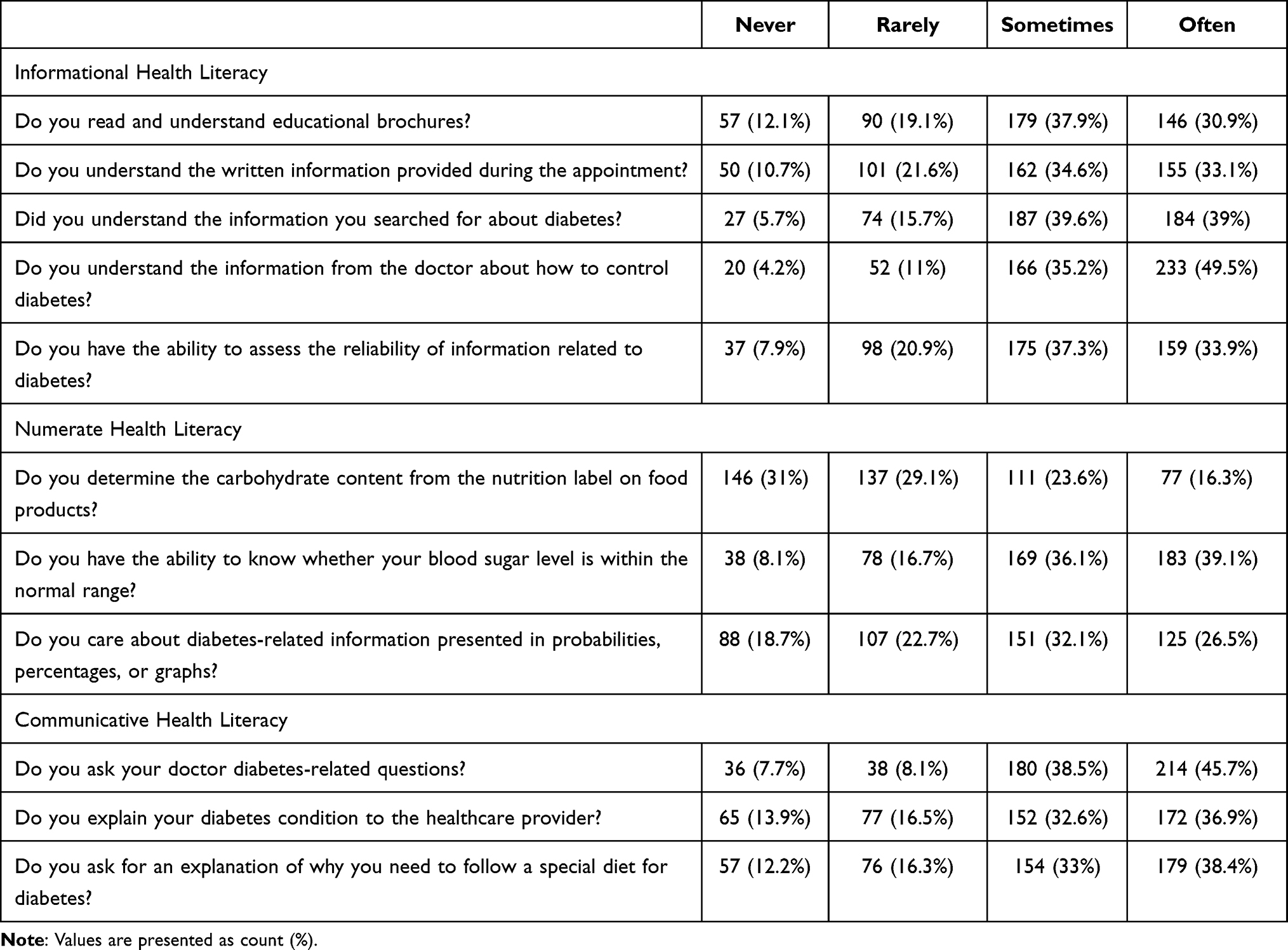 |
Table 2 Participants’ Responses to the Iraqi Diabetic Health Literacy Questionnaire (IDHLQ) |
The results of EFA and Rasch analysis are presented in Table 3. A KMO value of 0.822 was obtained, with MSAs ranging from 0.739 to 0.902, indicating sufficient common variance among items. Bartlett’s test was significant, χ2(55) = 2166.207, p < 0.001, supporting factor extraction. Parallel analysis indicated that the 11-item, 3-factor model was suitable for the present study. These factors were identified as Informational Health Literacy, Numerate Health Literacy, and Communicative Health Literacy, with Cronbach’s alpha values of 0.86, 0.84, and 0.70, respectively. The highest factor loadings were observed for Q10, followed by Q3, while the lowest loading was observed for Q7. The highest communality was for Q10 (0.70), while the lowest was for Q6 (0.30).
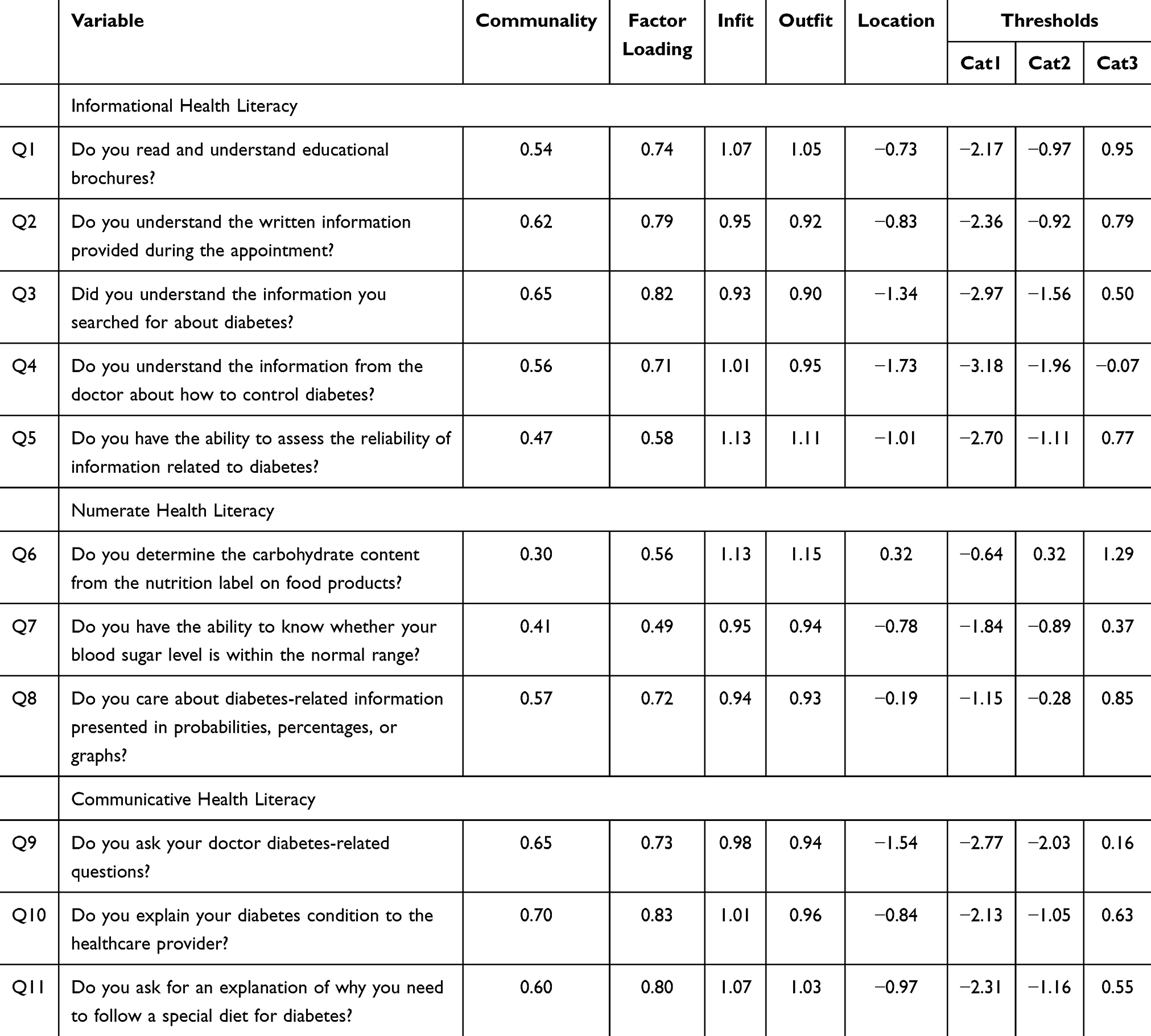 |
Table 3 Factor Loadings, Infit and Outfit Statistics, Item Locations, and Rasch Thresh |
Rasch analysis was performed, and the item separation reliabilities for the three factors were 0.866, 0.845, and 0.949, while the person separation reliabilities were 0.815, 0.761, and 0.647. All items across the three health literacy factors had infit and outfit values within the acceptable range, supporting the item hierarchy and confirming the model’s ability to differentiate between varying levels of health literacy among participants. Item difficulty analysis indicated that Q6 (location = 0.32) was the most difficult item, whereas Q4 (location = –1.73) was the least difficult.
All thresholds were appropriately ordered. The lowest threshold was the first threshold for Q4 (–3.18) in the informational health literacy factor, while the highest was the third threshold for Q6 (1.29) in the numeracy factor.
The Wright map is displayed in Figure 1. It shows that respondent abilities for informational, numeracy, and communicative health literacy had a unimodal distribution centered just below 0 logits, with tails ranging from approximately –3 to +2. Item step thresholds covered a similar range and were most concentrated between –1 and 0 logits, indicating generally acceptable targeting.
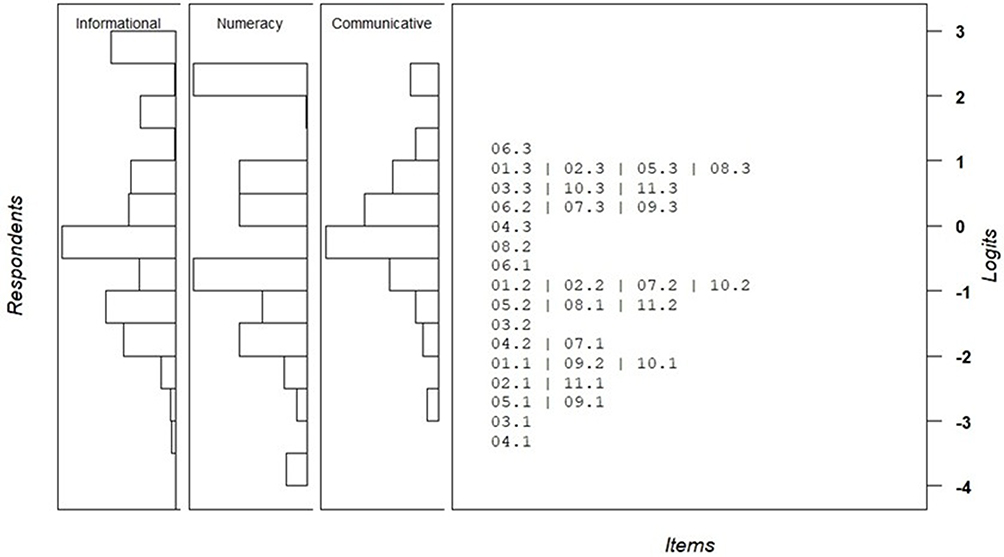 |
Figure 1 Wright (person–item) map for the Iraqi Diabetic Health Literacy Questionnaire (IDHLQ). Respondent locations (left; by domain) and item step-threshold locations (right) are displayed on the same logit scale. Higher logit values indicate higher health literacy (respondents) and greater difficulty (items/thresholds). |
Differential item functioning (DIF) between the sexes was evaluated as shown in Figure 2. The results indicated that a significant difference between males and females was observed only for item 4. Floor and ceiling effects were examined for the total IDHLQ score and each domain, and the results indicated that the flooring and ceiling effects were limited for the total IDHLQ score, with 3.8% of participants scoring the minimum possible value (11/44; 17/450) and none scoring the maximum (44/44; 0/450). At the domain level, floor effects ranged from 5.6% to 12.8% across the numeracy, informational, and communicative subscales, while ceiling effects were absent in all domains (0.0%). Overall, these findings indicate no evidence of problematic score compression at the extremes based on the prespecified >15% criterion.
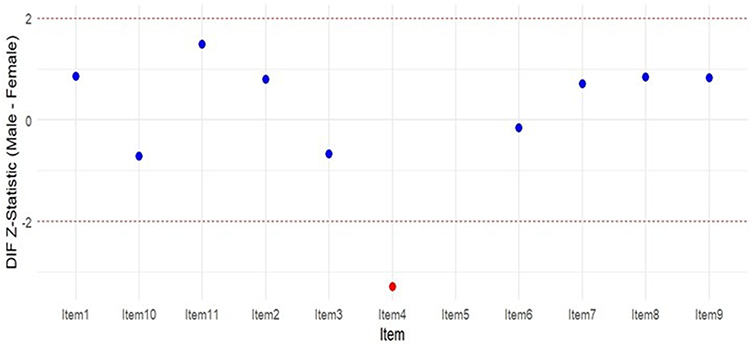 |
Figure 2 Differential item functioning (DIF) between sexes. |
Linear regression assumptions were checked, and diagnostic plots supported linearity and homoscedasticity. No influential observations exceeded conventional cutoffs. VIFs ranged from 1.02 to 1.71, and the Durbin–Watson statistic was 1.770. Monthly income was the only significant predictor of IDHLQ score (B = 1.318, SE = 0.445, β = 0.159, 95% CI: 0.45–2.19, p = 0.003). Age, gender, educational level, and marital status were not significant (all p > 0.27). The R2 value was 0.038, indicating that the model explained only 3.7% of the outcome variance.
Discussion
This study aimed to validate the IDHLQ, which included two domains from the JDHLQ and incorporated a new numeracy domain to better assess diabetic health literacy across all its dimensions. The development of a reliable and culturally appropriate tool can be used to better assess patients’ health literacy needs and ultimately enhance diabetes management in this population. By doing so, this study addressed an important gap in diabetes care. Overall, the results confirmed the reliability and validity of the IDHLQ, demonstrating strong psychometric properties within the three-factor model that encompassed the informational, communicative, and numeracy domains.
Several instruments that assess health literacy and numeracy in diabetic patients have been developed and used in the literature; however, the present study specifically employed the Iraqi Diabetic Health Literacy Questionnaire (IDHLQ), which was adapted from the Jordanian Diabetic Health Literacy Questionnaire (JDHLQ). The JDHLQ was selected as the foundational instrument because it was originally developed and validated in an Arabic-speaking population and showed strong psychometric properties in assessing informational and communicative health literacy domains relevant to diabetes care.
Alternative instruments, such as general health literacy scales and the Diabetes Numeracy Test (DNT),22 have been widely used in diabetes research. While these are valuable tools, they present certain limitations in the context of the present study. General health literacy instruments often lack disease-specific sensitivity, whereas the DNT focuses exclusively on numeracy skills without addressing informational comprehension or patient–provider communication. In contrast, the IDHLQ integrates informational, communicative, and numeracy domains within a single instrument, allowing for a more comprehensive assessment of diabetes-specific health literacy. From a psychometric point of view, the IDHLQ demonstrated reliability and construct validity comparable to those reported for other diabetes-related health literacy tools. The internal consistency values observed in this study were consistent with those reported for the JDHLQ and for diabetes numeracy instruments validated in other populations. Moreover, the application of Rasch modeling in the present study provides additional evidence of measurement robustness, supporting the IDHLQ’s ability to distinguish between varying levels of patient ability, a feature not consistently evaluated in earlier tools.
The three-factor structure identified in the IDHLQ, informational, numeracy, and communicative health literacy, is consistent with established conceptual models of health literacy and mirrors the structure reported in the original Jordanian Diabetic Health Literacy Questionnaire (JDHLQ), in which the informational and communicative domains demonstrated strong psychometric performance.13 Similar to the JDHLQ validation study, the informational domain in the present study showed the highest internal consistency, which points to the central role of information comprehension in diabetes self-management.
The EFA and Rasch analysis supported the construct validity of the tool, as all items showed acceptable infit and outfit values. Cronbach’s alpha values for each domain indicated satisfactory internal consistency, suggesting that items within each domain reliably measured their intended constructs. These findings align with the original validation of the JDHLQ in Jordan, where the informational and communicative domains demonstrated strong psychometric properties.13 This study, however, expands the JDHLQ by incorporating the numeracy domain, which is a vital component of effective diabetes management.12
Additionally, when compared with other studies, the Cronbach’s alpha values observed in this study (α = 0.70–0.86) are consistent with those reported for other diabetes-specific health literacy and numeracy tools validated in diverse populations.12 Furthermore, the use of Rasch analysis in the present study revealed acceptable item fit statistics and well-ordered response thresholds, findings that align with prior Rasch-based validation studies and support the structural robustness of the IDHLQ across varying levels of patient ability.16
The inclusion of a numeracy domain represents a key advancement over earlier instruments that primarily focused on informational or communicative skills. Consistent with previous research, numeracy-related items in the IDHLQ exhibited higher difficulty levels compared with other domains, reflecting the previously documented challenges patients face when interpreting numerical health information.23 These findings reinforce evidence that numeracy represents a critical component of diabetes self-management that needs independent assessment.
Previous studies have shown that patients with limited numeracy skills are more prone to poor glycemic control and treatment errors. A cross-sectional study of 398 adults with type 1 or type 2 diabetes found that lower numeracy skills, measured with the Diabetes Numeracy Test, were associated with poorer glycemic control and reduced perceived self-efficacy, as reflected by errors in interpreting glucose levels and miscalculating medication dosages.23 Another study of diabetic adults from three medical centers in Tennessee, United States, reported that numeracy skills strongly influence self-efficacy, which in turn profoundly affects glycemic control.12 Therefore, integrating numeracy into health literacy assessments provides deeper insight into patients’ ability to manage their disease.
In this study, numeracy items had higher difficulty levels than those in other domains. For example, interpreting carbohydrate content on food labels and understanding risk probabilities were among the most challenging tasks for participants. These findings are consistent with previous studies showing that diabetic patients often struggle more with numeracy skills, which are essential for daily self-care.12 Interestingly, the highest-scoring item in the numeracy domain was the “ability to know whether blood sugar is within the normal range,” suggesting that while some basic numerical understanding is present among Iraqi patients, more complex tasks such as carbohydrate counting remain a challenge. This highlights a critical area for targeted interventions focusing on the numeracy component of diabetes self-management education programs.
The median IDHLQ score was 33 out of 44 (75%), suggesting moderate diabetic health literacy among participants. This finding is consistent with studies assessing HL in other countries, such as Jordan and Saudi Arabia, where similar moderate scores were reported.13,24 These results point to the persistent challenges in achieving optimal HL. Monthly income was a significant contributor to this trend in both the present and previous studies. However, the regression model in this study had very weak explanatory power, and future research should examine additional predictors. Overall, our findings suggest that the expanded IDHLQ is a culturally relevant and psychometrically sound tool for assessing diabetic health literacy in the Iraqi population. The inclusion of a numeracy domain provides a broader understanding of patients’ skills, enabling clinicians to tailor educational strategies more effectively to individual needs. Additionally, the tool could be highly valuable in supporting national initiatives to address the growing burden of diabetes through patient-centered care and the development of population-specific interventions.
Strengths, Limitations and Future Directions
This study has several strengths. First, it is the first to validate the communicative and informative domains of the JDHLQ in the Iraqi population, providing evidence for its cross-cultural applicability in an Arabic-speaking context, given the linguistic, healthcare system, and cultural differences that may influence how patients understand and respond to health literacy questions. Second, it introduced and psychometrically validated a numeracy domain within the IDHLQ, recognizing the central role of numeracy in diabetes self-management. Finally, the study employed multiple validation techniques, including EFA, internal consistency testing (Cronbach’s alpha), and Rasch modeling. This comprehensive approach ensured both the statistical validity of the adapted tool and its practical relevance in clinical settings.
However, this study also has limitations. First, data collection relied on self-reported surveys, which may be subject to recall and social desirability biases. Second, a convenience sampling approach was adopted, which may have introduced selection bias.
Future research should implement longitudinal designs, which would be particularly valuable for evaluating how targeted educational interventions influence disease management. Additionally, examining variations in health literacy across demographic subgroups, such as education level or gender, may provide insights for developing health policies and patient-centered education programs in Iraq that address specific population needs.
Conclusion
This study validated the IDHLQ in the Iraqi population, incorporating a numeracy domain alongside.
This study validated the 11-item Iraqi Diabetic Health Literacy Questionnaire (IDHLQ), expanding the JDHLQ by incorporating a numeracy domain alongside the informational and communicative components. Exploratory factor analysis supported a three-factor structure, and internal consistency was acceptable across domains (α = 0.70–0.86). Rasch analysis further supported measurement performance, with item separation reliability of 0.87–0.95 and person reliability of 0.65–0.82. Collectively, these findings indicate that the IDHLQ is a reliable and valid instrument for assessing multidimensional diabetes-related health literacy among Arabic-speaking adults in Iraq, and its use in clinical and public health settings may support identification of patients with limited health literacy and inform targeted education strategies.
Data Sharing Statement
The dataset supporting the conclusions of this article is available in the Zenodo repository: https://doi.org/10.5281/zenodo.17095198.
Author Contributions
Conceptualization, W.Q. and A.A.; methodology, W.Q.; software, W.A.-Q.; validation, J.E. and A.J.; formal analysis, W.A.-Q., A.J., and A.A.; investigation, A.A., N.M, A.H., and B.A.; data curation, W.Q., A.J., B.A., and A.H.; writing - original draft and writing - review and editing, all authors; visualization, W.Q.; supervision, W.Q.; project administration, A.A. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was conducted without any external funding or financial support.
Disclosure
The authors declare that there is no conflict of interest.
References
1. Ogurtsova K, da Rocha Fernandes JD, Huang Y. et al. IDF Diabetes Atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabet Res Clin Pract. 2017;128:40–11. doi:10.1016/j.diabres.2017.03.024
2. Alberti KGMM, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus. Provisional report of a WHO consultation. Diabetic Med. 1998;15(7):539–553. doi:10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
3. Pengpid S, Peltzer K. Prevalence and factors associated with undiagnosed type 2 diabetes among adults in Iraq: analysis of cross-sectional data from the 2015 STEPS survey. BMJ Open. 2022;12(11). doi:10.1136/BMJOPEN-2022-064293
4. Ad Hoc Committee on Health Literacy for the Council on Scientific Affairs AMA. Health Literacy: report of the Council on Scientific Affairs. JAMA. 1999;281(6):552–557. doi:10.1001/JAMA.281.6.552.
5. White RO, Wolff K, Cavanaugh KL, Rothman R. Addressing health literacy and numeracy to improve diabetes education and care. Diabetes Spectr. 2010;23(4):238–243. doi:10.2337/DIASPECT.23.4.238
6. Harding JL, Pavkov ME, Magliano DJ, Shaw JE, Gregg EW. Global trends in diabetes complications: a review of current evidence. Diabetologia. 2019;62(1):3–16. doi:10.1007/S00125-018-4711-2
7. Ahmad MN, Farah AI, Al-Qirim TM. The cardiovascular complications of diabetes: a striking link through protein glycation. Rom J Intern Med. 2020;58(4):188–198. doi:10.2478/RJIM-2020-0021
8. Irfan M, Jabbar A, Haque AS, Awan S, Hussain SF. Pulmonary functions in patients with diabetes mellitus. Lung India. 2011;28(2):89–92. doi:10.4103/0970-2113.80314
9. Vollset SE, Ababneh HS, Abate YH, et al. Burden of disease scenarios for 204 countries and territories, 2022–2050: a forecasting analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2204–2256. doi:10.1016/S0140-6736(24)00685-8
10. Ahmad F, Joshi SH. Self-care practices and their role in the control of diabetes: a narrative review. Cureus. 2023;15(7). doi:10.7759/CUREUS.41409
11. Chittooru CS, Gorantla Ananda K, Panati DD, Chaudhuri S, Prahalad H. Self-care practices and its determinants among diabetic population in rural Andhra Pradesh, India: a cross-sectional study. Clin Epidemiol Glob Health. 2022;16:101102. doi:10.1016/j.cegh.2022.101102
12. Osborn CY, Cavanaugh K, Wallston KA, Rothman RL. Self-efficacy links health literacy and numeracy to glycemic control. J Health Commun. 2010;15 Suppl 2(Suppl 2):146–158. doi:10.1080/10810730.2010.499980
13. Al-Qerem W, Jarab A, Eberhardt J, Alasmari F, Alkaee SM, Alsabaa ZH. Development and validation of the jordanian diabetic health literacy questionnaire: enhancing diabetes management in arabic-speaking populations. Healthcare. 2024;12(7). doi:10.3390/healthcare12070801
14. Shrivastava SRBL, Shrivastava PS, Ramasamy J. Role of self-care in management of diabetes mellitus. J Diabetes Metab Disord. 2013;12(1). doi:10.1186/2251-6581-12-14
15. Al-Qerem W, Jarab AS, Badinjki M, Hyassat D, Qarqaz R. Exploring variables associated with medication non-adherence in patients with type 2 diabetes mellitus. PLoS One. 2021;16(8 August). doi:10.1371/JOURNAL.PONE.0256666
16. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi:10.1097/00007632-200012150-00014
17. Costa FA, Duggan C, Bates I. A systematic approach to cross-cultural adaptation of survey tools. Pharm Pract. 2007;5(3):115–124. doi:10.4321/S1886-36552007000300004
18. White RO, Wolff K, Cavanaugh KL, Rothman R. Addressing health literacy and numeracy to improve diabetes education and care. Diabetes Spectr. 2010;23(4):238. doi:10.2337/DIASPECT.23.4.238
19. Mikhael E, Hassali M, Hussain S. Validation of newly developed culturally specific diabetes self-management education and support program for Iraqi type 2 diabetes mellitus patients. J Educ Health Promot. 2021;10(1). doi:10.4103/JEHP.JEHP_311_21
20. Saadeh R, Alsmadi H, Batieha A, et al. Quality of care for type 2 diabetes in Jordan: a national study. Med Int. 2023;3(3):27. doi:10.3892/MI.2023.87
21. Hair JF. Multivariate Data Analysis: A Global Perspective. Pearson Education; 2010.
22. Huizinga MM, Elasy TA, Wallston KA, et al. Development and validation of the Diabetes Numeracy Test (DNT). BMC Health Serv Res. 2008;8:96. doi:10.1186/1472-6963-8-96
23. Cavanaugh K, Huizinga MM, Wallston KA, et al. Association of numeracy and diabetes control. Ann Intern Med. 2008;148(10):737–746. doi:10.7326/0003-4819-148-10-200805200-00006
24. Abdel-Latif MMM, Saad SY. Health literacy among Saudi population: a cross-sectional study. Health Promot Int. 2019;34(1):60–70. doi:10.1093/HEAPRO/DAX043
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.