Back to Journals » Clinical and Experimental Gastroenterology » Volume 19
Real-Life Use of Subcutaneous Biologicals and JAK Inhibitors in IBD Maintenance Therapy: Treatment Continuation, Switching Patterns, and Concomitant Medications
Authors Koivusalo M, Jokelainen J, Huhtinen A ![]() , Kovac B
, Kovac B ![]() , Silvola S, Torvinen S, Ylisaukko-oja T, Arkkila P
, Silvola S, Torvinen S, Ylisaukko-oja T, Arkkila P ![]()
Received 28 October 2025
Accepted for publication 31 December 2025
Published 23 January 2026 Volume 2026:19 576384
DOI https://doi.org/10.2147/CEG.S576384
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Santosh Shenoy
Mirkka Koivusalo,1 Jari Jokelainen,1 Anna Huhtinen,1 Bianca Kovac,2 Saija Silvola,2 Saku Torvinen,1 Tero Ylisaukko-oja,1 Perttu Arkkila3
1MedEngine Oy, Helsinki, Uusimaa, Finland; 2Takeda Oy, Helsinki, Uusimaa, Finland; 3Department of Gastroenterology, University of Helsinki and Helsinki University Hospital, Helsinki, Uusimaa, Finland
Correspondence: Mirkka Koivusalo, Email [email protected]
Objective: Combining biologicals or Janus kinase inhibitors (JAKis) with conventional medications and switching therapies is common in moderate-to-severe inflammatory bowel disease (IBD) treatment. This study assessed the use of conventional medications, treatment continuation, switching, and factors associated with switching during IBD maintenance therapy with subcutaneous (SC) biologicals or JAKis.
Materials and Methods: This Finnish nationwide, retrospective registry study included adult Crohn’s disease (CD) and ulcerative colitis (UC) patients on SC biological/JAKi maintenance therapy (≥ 6 months on treatment) during 2003– 2023. Pharmacy dispensation data were collected from The Social Insurance Institution.
Results: Among 7,707 individuals, use of corticosteroids (CS), immunosuppressants (IS) and 5-aminosalicylates (5-ASA) was less common after SC biological/JAKi initiation. At 24 months, treatment continuation rates were 51– 57% for adalimumab, golimumab, ustekinumab and tofacitinib (in UC); and 71– 80% for infliximab, vedolizumab and ustekinumab (in CD). Overall, 16% of treatments were switched—most commonly from golimumab (28%), tofacitinib (24%) and adalimumab (21%) to ustekinumab (42% of switches) or vedolizumab (17% of switches). Prior golimumab (adjusted OR, 1.73; 95% CI, 1.42– 2.09) or tofacitinib (1.48; 1.16– 1.86) use was associated with a higher risk of switching (p< 0.001), while prior infliximab (0.12; 0.09– 0.16), vedolizumab (0.35; 0.26– 0.46), IS (0.52; 0.45– 0.57), or 5-ASA (0.62; 0.55– 0.70) use was associated with lower risk (p< 0.001).
Conclusion: Treatment continuation rates during maintenance reached up to 80%. Most switches involved a different mode-of-action. While conventional medications were tapered, IS and 5-ASA may support treatment continuation.
Keywords: IBD, subcutaneous biologicals, JAK inhibitors, conventional medication, treatment continuation, treatment switching
Introduction
The management of inflammatory bowel disease (IBD) has significantly advanced over the past two decades with the introduction of biologicals and small molecule therapies, particularly Janus kinase inhibitors (JAKis).1–3 These agents are used to induce and maintain remission in patients with moderate to severe Crohn’s disease (CD) and ulcerative colitis (UC) who are refractory or intolerant to conventional therapies (corticosteroids, CS; 5-aminosalicylates, 5-ASA; and immunosuppressants, IS).
Anti-tumor necrosis factor (anti-TNF) agents, such as adalimumab and infliximab, are commonly used as first-line biologicals. However, approximately 10–30% of patients fail to respond to induction therapy and up to two-thirds lose response over time.4–6 Second-line biologicals, ustekinumab (interleukin-12/23 antagonist) and vedolizumab (α4β7-integrin antagonist), have shown efficacy in both unresponsive anti-TNF-experienced and anti-TNF-naive patients.1,2,7–11 Orally administered JAKis are approved primarily for the treatment of UC patients with an inadequate response or intolerance to conventional therapies or biologicals.3,12 In patients refractory to a biological or JAKi, treatment strategies often include dose escalation before switching to next-line agents.13–19
Despite advances in treatment, conventional medications are often continued alongside a biological or JAKis in real-life settings.13,20–22 While combining IS with anti-TNF agents can enhance the induction of clinical remission and prevent anti-drug antibody formation,1,23–26 it may also increase the risk of adverse events, including infections and malignancies.27,28 Similarly, 5-ASA agents are often co-administered with biologicals despite limited evidence supporting their clinical benefit.21,29 CS can be used in combination with biologicals to induce remission, but are unsuitable for long-term use due to their adverse effect profiles.30 Notably, real-world studies have demonstrated a steroid-sparing effect for both biologicals and JAKis.13,14,21,31,32
Treatment switching patterns between biologicals, and factors associated with switching, have been investigated utilizing real-world data, but analyses following the emergence of non-anti-TNF therapies remain scarce.33–37 Studies examining factors associated with biological discontinuation and switching show somewhat conflicting findings. Factors associated with a higher risk of switching include prior infections, hospitalizations, a higher comorbidity index, use of IS, 5-ASA, and high-dose CS, and anti-TNF dose escalation.34–37 Conversely, anti-TNF dose escalation and IS use have also been reported to decrease the risk of switching.35
Previously, we reported the real-world utilization of subcutaneous (SC) adalimumab, golimumab, and ustekinumab in Finland, based on reimbursed pharmacy dispensations up to 2018.16 Since then, SC infliximab, vedolizumab, and JAKis have become available. Therefore, updated real-world evidence is needed to understand treatment patterns better and to improve treatment choices and overall IBD management. Our aim was to evaluate the following parameters during IBD maintenance therapy with SC biologicals/JAKis: the use of conventional medications, treatment continuation, switching patterns, and factors associated with switching.
Materials and Methods
Study Design and Population
This nationwide, retrospective registry study utilized data from The Register for Reimbursement Entitlements and The Register for Reimbursed Drugs (The Social Insurance Institution of Finland). The study population included all individuals with an IBD-related reimbursement entitlement, and is thus expected to cover all prevalent IBD cases.38 Additional inclusion criteria included: a diagnosis for CD (10th revision of the International Classification of Diseases, ICD-10: K50) or UC (ICD-10: K51), ≥1 pharmacy dispensation(s) of SC biologicals (adalimumab, golimumab, infliximab, vedolizumab, ustekinumab, risankizumab) or JAKis (tofacitinib, upadacitinib, filgotinib), and aged ≥18 years at the time of the first dispensation between 2003 and 2023 (Supplementary Table 1). Only patients on maintenance therapy (treatment duration ≥6 months) and with on-label indications were included in the analyses.
Follow-Up and Data Collection
Follow-up began at first SC biological/JAKi dispensation (index date) and ended at treatment discontinuation or the study period’s conclusion. The period from the first IBD-related reimbursement entitlement during study period to the index date was defined as baseline. Collected variables included diagnosis for entitlement (if a person had both CD and UC diagnoses, the more recent diagnosis was chosen), sex, age at first IBD-related reimbursement entitlement during study period, geographic area, IBD-related medications (Supplementary Table 1) and associated dispensation dates, number of claimed packages, package size, and Nordic product number (VNR) indicating product strength.
Treatment Periods
Treatment initiation was defined as the first pharmacy dispensation. Hospital administered intravenous (IV) medications were not captured; therefore, IV induction doses specified in the summary of product characteristics (SmPC) for infliximab, vedolizumab, and ustekinumab were not included. Treatment discontinuation was defined as the end of treatment effect (ie, the date when the last purchased amount would be used up, per SmPC) plus a 12-week grace period (24 weeks for ustekinumab).
Outcome Measures
Basic demographic and clinical characteristics were described at baseline. Baseline use of conventional medications, including IS (azathioprine, mercaptopurine, methotrexate, cyclosporine), 5-ASA (mesalazine, sulfasalazine, olsalazine), and CS (prednisolone, prednisone, methylprednisolone, hydrocortisone, betamethasone, budesonide), was assessed within 12 months of the first IBD reimbursement entitlement during the study period.
All other outcomes were analyzed for treatment periods with ≥6 months of persistence to ensure an adequate response time. Conventional medication use was reported as the number and proportion of treatment periods with concomitant IS, 5-ASA, or CS use during the six months before and after initiation of an SC biological/JAKi. Treatment continuation was reported as the proportion of persistent treatment periods at 12, 18, and 24 months after initiation. Switching patterns, regardless of treatment line, were reported as the number and proportion of switches from and to each medication. Associations between explanatory variables (sex, age, diagnosis, use of IS, 5-ASA, or CS within 0–6 months prior to a switch, preceding SC biological/JAKi treatment, calendar quarter, and University Hospital Catchment Area) with switching were analyzed. Switches to and from IV infliximab and vedolizumab (prior to SC formulations) were not captured.
Statistical Analysis
Descriptive statistics were used to report numbers and percentages for categorical variables, and mean with standard deviation (SD) and median with quartiles (Q1, Q3) for continuous variables. Statistical comparisons were performed using the McNemar test. Kaplan-Meier survival analysis was used to assess treatment persistence, and the Log rank test to compare survival estimates between diagnoses. P-values <0.05 were considered statistically significant. Treatment continuation rates were calculated as probabilities with 95% confidence intervals (CIs).
Factors associated with switching were examined by comparing treatment periods that were switched to those that were not. Crude odds ratios (ORs) with 95% CIs were calculated using univariate logistic regression, and adjusted ORs (aORs) using multivariate logistic regression. All analyses were performed using R version 4.0.3 (https://www.r-project.org/).
Ethical Considerations
The study was approved by the Social Insurance Institution (Kela, 24/522/2024). Ethics approval or informed consent were not required under Finnish legislation, as patients were not contacted, treatment was unaffected, and only pseudonymized data were used.
Results
Patient Characteristics
Between 2003 and 2023, 70,173 adults were granted reimbursement entitlement for IBD, of whom 16,689 individuals had CD and 43,023 had UC. Of these individuals, 8,557 received at least one pharmacy dispensation of an SC biological/JAKi, and 7,707 had a treatment period of >6 months.
In CD, where the sex distribution was approximately equal, a higher proportion of male patients (51–66%) received all treatments except for filgotinib and ustekinumab (Table 1). The mean age at the time of the first IBD reimbursement entitlement during the study period, among treatment groups (drug) in each disease (CD and UC), was 31.7–43.5 years, with the lowest for filgotinib in UC, and the highest for vedolizumab in CD. At baseline, 36–67% of patients used IS, with the lowest use observed in golimumab users in UC and the highest in upadacitinib users in UC. Baseline use of CS or 5-ASA appeared to be more common in UC (CS: 53–73% of patients; 5-ASA: 64–77%) than in CD (CS: 31–46%; 5-ASA: 25–31%).
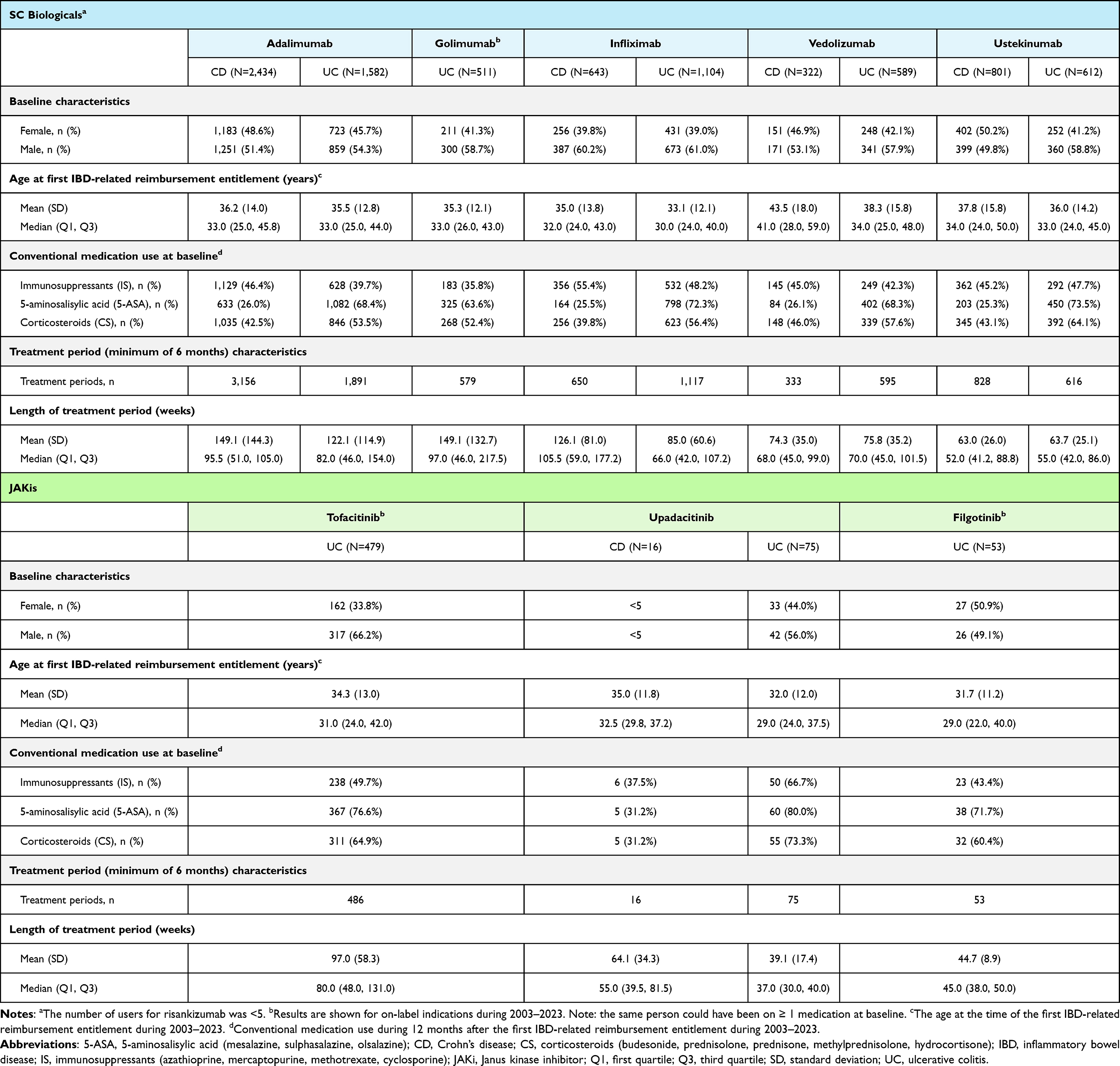 |
Table 1 Patient Characteristics |
Adalimumab was the most frequently prescribed therapy during the study period, with 3,156 treatment periods for CD and 1,891 for UC. Adalimumab and golimumab were associated with the longest treatment periods (122.1–149.1 weeks), followed by infliximab in CD (126.1 weeks) (Table 1).
Use of Conventional Medications
For most SC biologicals and JAKis, the use of IS, 5-ASA, and CS was significantly less common during the six months after treatment initiation compared to the six months before (Figure 1). The proportion of treatment periods with IS use (IS dispensed from pharmacies after JAKi initiation) decreased by 8–38% after initiation of SC biologicals, with the largest difference observed for ustekinumab in UC (34% before vs 21% after initiation, p<0.001). After initiation of JAKi, the proportion of treatment periods with IS use decreased by 31–80%. The largest changes were observed in UC patients on tofacitinib (49% before vs 10% after initiation, p<0.001) and upadacitinib (28% vs 8%, p<0.01).
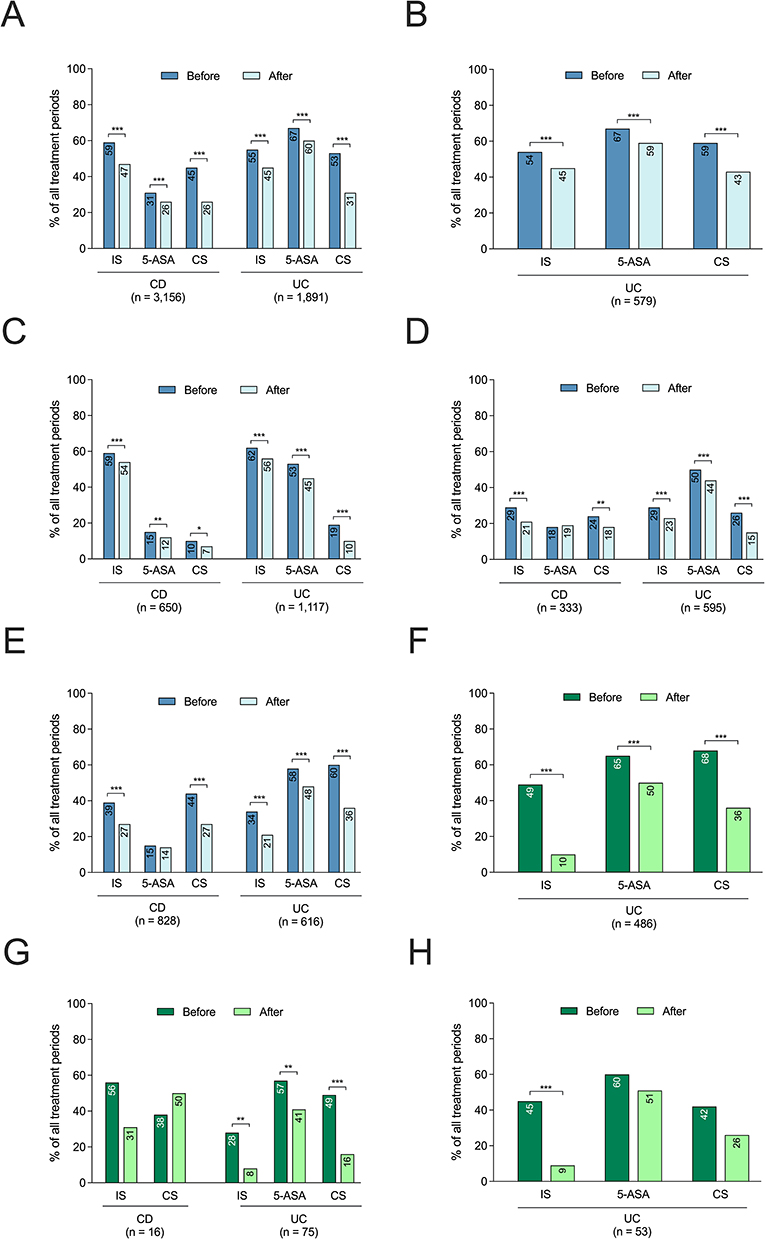 |
Figure 1 Use of conventional medications (IS, 5-ASA, and CS) during the 6 months before and after initiation of SC biological or JAKi treatment periods. SC biologicals included (A) adalimumab, (B) golimumab, (C) infliximab, (D) vedolizumab, and (E) ustekinumab, and JAKis included (F) tofacitinib, (G) upadacitinib, and (H) filgotinib. Medication use before initiation may coincide with previously used other biological or JAKi treatments. Results are shown for on-label indications during 2003–2023. Abbreviations: 5-ASA, 5-aminosalicylic acid (mesalazine, sulfasalazine, olsalazine); CD, Crohn’s disease; CS, corticosteroid (budesonide, prednisolone, prednisone, methylprednisolone, hydrocortisone,); IS, immunosuppressant (azathioprine, methotrexate, mercaptopurine, cyclosporine); JAKi, Janus kinase inhibitor; SC, subcutaneous; UC, ulcerative colitis. Notes: * p<0.05, ** p<0.01, *** p<0.001 between the number of treatment periods with conventional medication use before and after initiation of a SC biological/JAKi. |
There was a 10–28% decrease in the proportion of treatment periods with 5-ASA use after SC biological/JAKi initiation. However, in UC, the proportion of treatment periods with 5-ASA use remained at 41–60% after SC biological/JAKi initiation.
The reduction in proportion of SC biological/JAKi treatment periods with use of CS was prominent, ranging from 36 to 69%. The largest decreases in CS use were observed in UC patients on tofacitinib (60% vs 36% of treatment periods with CS use before vs after initiation, p<0.001) and upadacitinib (49% vs 16%, p<0.001).
The number and proportion of treatment periods with individual medication use are shown in Supplementary Table 2.
Treatment Continuation Rate
Similar treatment continuation rates were observed for adalimumab, golimumab, ustekinumab (in UC), and tofacitinib. Between 6 and 12 months, 70–74% of treatment periods continued, while only approximately half (51–57%) continued at month 24 (Table 2 and Supplementary Figure 1). For infliximab and vedolizumab, continuation rates were higher, 84–90% at month 12 and 71–80% at month 24. For upadacitinib and filgotinib, the assessment of continuation rates (78–88% and 74%, respectively) was limited due to the short follow-up period available (Supplementary Table 1).
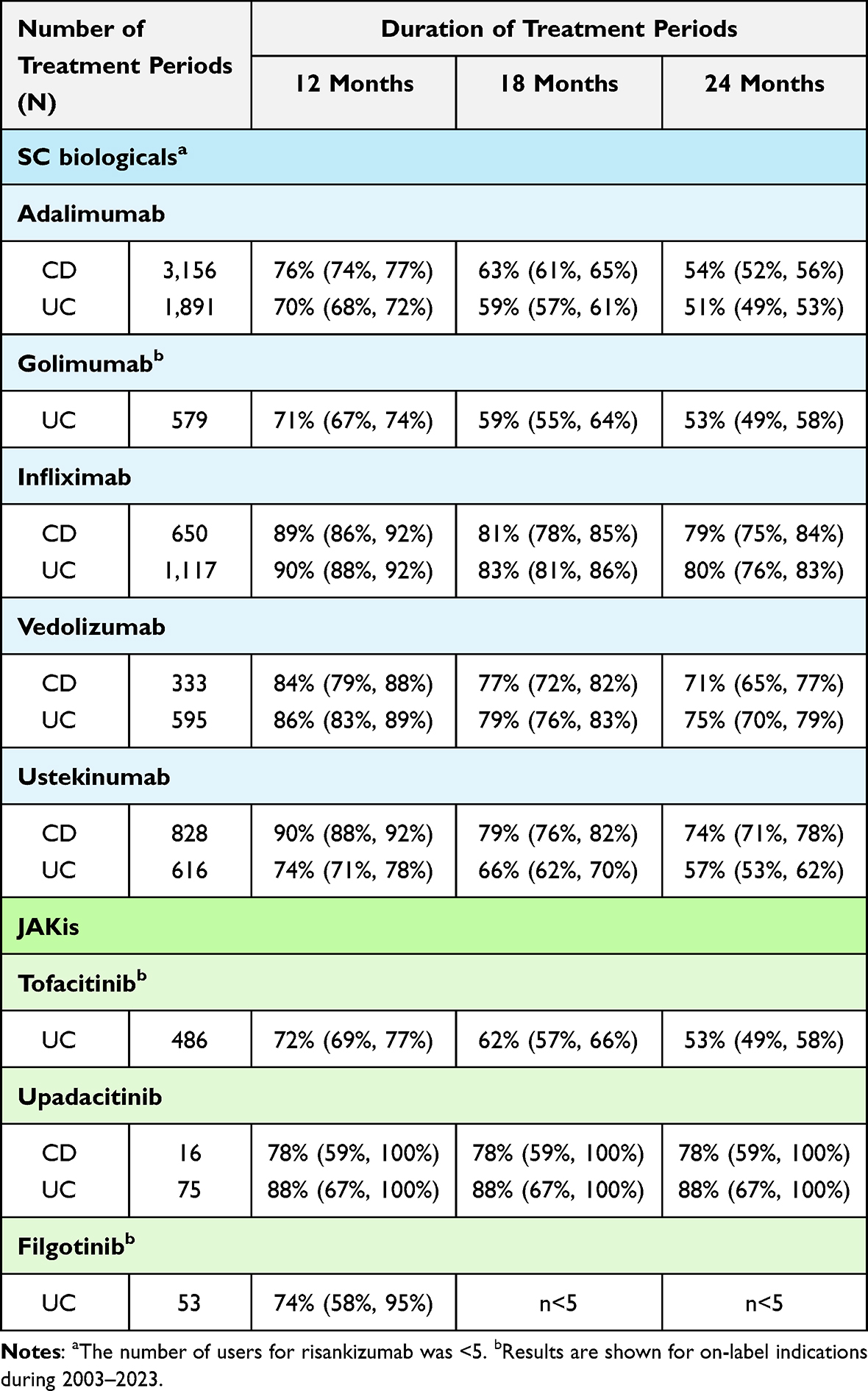 |
Table 2 Treatment Continuation Rates, Presented as Probabilities (with 95% CI), of Subcutaneous (SC) Biologicals and JAK Inhibitors (JAKis) in Crohn’s Disease (CD) and Ulcerative Colitis (UC) Patients in Maintenance Therapy Who Continued Treatment for ≥6 months, Over a Follow-up-Period of 24 months and Independent of the Treatment Line |
Medication Switching Patterns and Associated Factors
Out of all SC biological/JAKi treatment periods, 16% involved a switch to another treatment during the study period (Table 3). The treatments most frequently switched from were golimumab (28% of golimumab treatment periods), tofacitinib (24%), and adalimumab (21%), while infliximab had the lowest switching rate (3%). The most common treatments switched to (from any treatment type) were ustekinumab (42% of all switches), vedolizumab (17%) and tofacitinib (17%), with upadacitinib being the least common (3%).
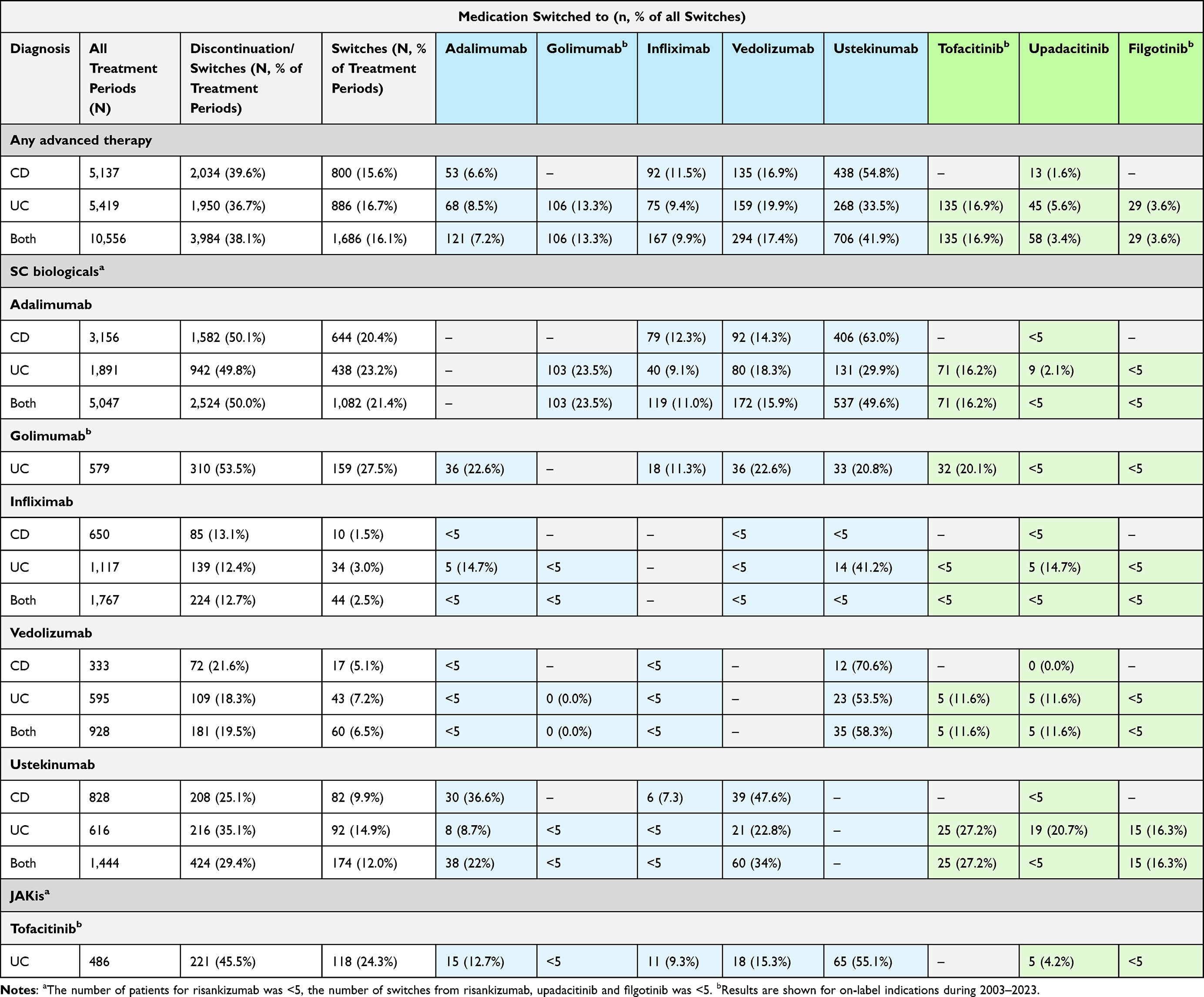 |
Table 3 Medication Switches Between Subcutaneous (SC) Biologicals or JAK Inhibitors (JAKis) Independent of Treatment Line During the Study Period (2003–2023). |
Among the three most common medications that patients switched from, the switching patterns were as follows: from golimumab, patients switched to adalimumab, vedolizumab, and ustekinumab in equal proportions (21–23%); from tofacitinib, most switched to ustekinumab (55%), followed by vedolizumab (15%) and adalimumab (12%); and from adalimumab, switches were most often to ustekinumab (50%), golimumab (24%) and vedolizumab (16%).
Factors associated with an increased risk of switching to another SC biological/JAKi included prior use of golimumab (aOR, 1.73; 95% CI, 1.42–2.09; p<0.001) or tofacitinib (1.48; 1.16–1.86; p<0.001), and a diagnosis of UC (1.25; 1.10–1.42; p=0.001) (Figure 2 and Supplementary Table 3). Conversely, prior use of infliximab (0.13; 0.09–0.16) or vedolizumab (0.35; 0.26–0.46), as well as the use of an IS (0.51; 0.45–0.57; p<0.001), 5-ASA (0.62; 0.55–0.70; p<0.001), or CS (0.84; 0.75–0.95; p=0.003) within six months prior to switching, were associated with a lower risk of transitioning to another SC biological/JAKi (p<0.001).
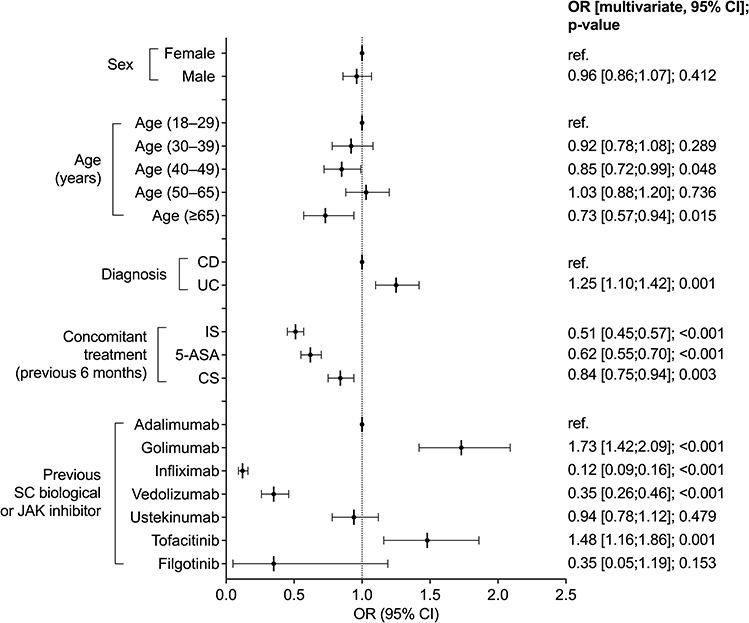 |
Figure 2 Factors associated with SC biological or JAKi medication switching shown as adjusted odds ratios (ORs) with 95% CI. Results are shown for on-label indications during 2003–2023. Abbreviations: 5-ASA, 5-aminosalicylic acid (mesalazine, sulfasalazine, olsalazine); CD, Crohn’s disease; CI, confidence interval; CS, corticosteroid (budesonide, prednisolone, prednisone, methylprednisolone, hydrocortisone,); IS, immunosuppressant (azathioprine, methotrexate, mercaptopurine, cyclosporine); JAKi, Janus kinase inhibitor; ref., reference; SC, subcutaneous; UC, ulcerative colitis. |
Discussion
This nationwide registry study assessed conventional medication use, treatment continuation, and switching in IBD patients receiving SC biological or JAKi maintenance therapy during a 20-year period. Up to 80% of treatment periods continued at month 24, while 16% involved a switch, most often from golimumab, adalimumab, and tofacitinib, to therapies with a different mode-of-action, such as ustekinumab or vedolizumab. Use of conventional medications was less common after treatment initiation, and prior use of an IS and/or 5-ASA was associated with a decreased risk of switching, suggesting a role in supporting the efficacy of the biologicals.
Our data showed that IS use was less common following initiation of any SC biological, with an 8–38% reduction in the proportion of treatment periods with IS use, and with the largest reduction observed for ustekinumab (in UC). The differences in IS use between biologicals may partly reflect variations in disease activity at the time of treatment initiation. Additionally, it should be noted that infliximab and vedolizumab users may also include patients that received IV treatment before their first SC dispensation. In such cases, both the “before” and “after” periods could reflect a stable treatment phase rather than a true treatment initiation. Nonetheless, previous real-world studies in Finland reported similar findings or no major changes in IS use after initiation of biologicals.13,21 While combining IS with anti-TNF agents may improve treatment persistence and enhance remission,25,35,39–41 some studies have shown limited benefit of combination therapy in the induction or maintenance of remission.41–45 The potential for increased risk of infection necessitates careful consideration when combining JAKis with IS.3,46,47 In our analysis, IS use decreased substantially after JAKi initiation, with an up to 80% reduction in the proportion of treatment periods with IS use, and approximately 10% of patients remaining on IS, consistent with previous real-world findings.48 Although these dispensations may reflect residual use, continued IS use during JAKi therapy warrants careful monitoring.
5-ASA is commonly administered together with biologicals, even though the clinical benefit may be limited, especially in CD patients.21,29,49 We found that the overall proportion of treatment periods involving 5-ASA use decreased by 10–28% after SC biological/JAKi initiation. In CD, 5-ASA use continued in 26% of treatment periods with adalimumab but only in 12% and 19% with infliximab and vedolizumab, respectively—possibly reflecting the wider adoption of guidelines discouraging 5-ASA use in CD by the time SC formulations of infliximab and vedolizumab became available. In UC, 5-ASA use remained substantially higher, with up to 60% of treatment periods still involving 5-ASA.
Meanwhile, we observed a significant reduction in CS use, with up to a 70% reduction in the proportion of treatment periods involving CS following SC biological/JAKi initiation. The most pronounced reductions were observed with JAKis. Reducing CS use is a key treatment goal in the long-term management of IBD due to their well-documented adverse effects.30,31,50 Our findings are in line with real-world studies demonstrating a CS-sparing effect and high CS-free remission rates with biologicals/JAKis.17,20–22,31,32,51 Given that JAKis are often prescribed for patients with more severe disease and prior treatment failures,3,12 their the CS-sparing effect is particularly valuable in minimizing additional treatment-related adverse effects.
In our study, treatment continuation rates were analyzed for treatment periods of ≥6 months to ensure a stable clinical response. Direct comparisons with other studies should therefore be interpreted cautiously. At month 24, only approximately half of the treatment periods continued for adalimumab, golimumab, and ustekinumab (in UC), while vedolizumab, infliximab, and ustekinumab (in CD) had higher continuation rates (71–80%), consistent with other studies.13,20,37 It should be noted that the patient populations on infliximab and vedolizumab also include those initiated on hospital-administered IV treatment during previous years. These patients were likely to already have good persistence and remission at the time of starting the SC medication, and also maintain remission thereafter, as suggested by a recent Finnish study.52 Treatment continuation rate for tofacitinib (62%) at month 12 was comparable to other studies,14,17 even though higher persistence was reported in a Korean study.37
Switching occurred in 16% of treatment periods during 2003–2023. For comparison, switching rates of 10–32% over follow-up periods of 3–10 years have been reported,34,36,37 and rates ranging from 4–70% in a review of 21 studies with follow-up durations of 1–2 years.33 Previous assessments of switching patterns have shown frequent switches from infliximab to adalimumab.33–35,37 Here, only 10% of infliximab treatment periods were switched, but this may be largely affected by the exclusion of IV-administered infliximab. According to prior reports, adalimumab was also commonly switched to infliximab, followed by switching to vedolizumab, certolizumab pegol, golimumab, and ustekinumab.34–36 Consistent with this, we also demonstrate that adalimumab was frequently switched from, along with golimumab and tofacitinib. The low switching rates from vedolizumab and ustekinumab support their high treatment persistence.20,37,53 Notably, most switches from any treatment were to ustekinumab, likely because it was the first SC non-anti-TNF therapy that became available, followed by vedolizumab and tofacitinib. These results align with treatment guidelines favoring a different mode-of-action.1,2,37
Several factors were associated with the risk of treatment switching. Prior golimumab or tofacitinib use was associated with an increased risk of switching when compared to adalimumab which was used as the reference in the analysis. Accordingly, golimumab has been shown to be associated with an increased risk of treatment non-persistence.36,37 With tofacitinib, treatment switching may be affected by safety concerns in certain patients, and treatment persistence has been shown to be lower for tofacitinib compared to, for example, vedolizumab.54,55 Prior evidence shows a higher risk of non-persistence and switching in UC than in CD.11,36,37 Similarly, CS use has been linked to an increased risk of switching.34–36 While we did not observe significant associations between diagnosis or CS use with risk of switching in the unadjusted analysis, the association became significant in the multivariate model, suggesting that confounding variables were masking the true relationship.
Conversely, vedolizumab or infliximab as the previous medication decreased the risk of switching, aligning with their high treatment continuation rates. Similarly, prior IS or 5-ASA use decreased the risk of switching, consistent with findings by Chen et al.35 Plausible explanations include the benefits of combination therapy between IS and anti-TNFs,24–26,39,40 and the benefit of 5-ASA during induction in particular in UC.2 However, there are also contrasting findings showing that IS and 5-ASA use have been associated with an increased risk of treatment switching.34–37
The main strengths of this study are the real-world setting, nationwide coverage of patients due to the Finnish reimbursement system, which ensures equal access to medications, the long study period, and the efficient implementation of international treatment guidelines and introduction of new therapies (early switching to SC products). The main limitation is the lack of data on hospital-administered IV biologicals. Therefore, the first induction doses (based on SmPC for ustekinumab, infliximab, and vedolizumab) and the IV administration periods of infliximab and vedolizumab were not captured. As a result, the infliximab and vedolizumab populations also include patients who transitioned from IV to SC maintenance therapy, limiting insight into initial treatment starting points and switching patterns. In addition, reasons for discontinuations and switching are unknown, the first reimbursement entitlement for IBD could have been received before the start of the study period, and the short follow-up time available for medications with the most recent reimbursement status (upadacitinib, filgotinib, and risankizumab) limited their analyses. Furthermore, the true relationships were masked by confounding variables in the univariate unadjusted analysis but were revealed in the multivariate analysis.
In conclusion, our findings of high treatment continuation rates suggest good remission rates in patients on maintenance therapy. When treatments were switched –most commonly from golimumab, tofacitinib or adalimumab– the new therapy most often had a different mode-of-action. There was a decreasing reliance on conventional medications alongside advanced therapies, though IS and 5-ASA may support treatment persistence in some cases, possibly by enhancing the efficacy of biologicals. These findings help characterize real-world treatment patterns and may inform clinical decision-making in IBD management, particularly regarding the selection and sequencing of advanced therapies, although further long-term data on JAKi use and other newer treatments are still needed.
Data Sharing Statement
The data underlying this article cannot be shared publicly to protect the privacy of individuals that participated in the study. The study protocol will be shared on reasonable request to the corresponding author.
Acknowledgments
We thank Mónica Ferreira and Harlan Barker from MedEngine Oy for medical writing support and language review. Takeda Oy (Helsinki, Finland) is acknowledged for financial support of this study.
Funding
This study was supported by Takeda Oy.
Disclosure
Mirkka Koivusalo, Jari Jokelainen, Anna Huhtinen and Saku Torvinen are employees of MedEngine. Tero Ylisaukko-oja is the owner of MedEngine. Bianca Kovac and Saija Silvola are employees of Takeda Oy. Perttu Arkkila is a stock owner of Orion Pharma Oy and a consultant for Takeda Oy, Celltrion Oy, and Johnson & Johnsson Oy. The authors report no other conflicts of interest in this work.
References
1. Torres J, Bonovas S, Doherty G, et al. ECCO guidelines on therapeutics in crohn’s disease: medical treatment. J Crohns Colitis. 2020;14:4–14. doi:10.1093/ecco-jcc/jjz180
2. Raine T, Bonovas S, Burisch J, et al. ECCO guidelines on therapeutics in ulcerative colitis: medical treatment. J Crohns Colitis. 2022;16:2–17. doi:10.1093/ecco-jcc/jjab178
3. Herrera-deGuise C, Serra-Ruiz X, Lastiri E, Borruel N. JAK inhibitors: a new Dawn for oral therapies in inflammatory bowel diseases. Front Med. 2023;10:1089099. doi:10.3389/fmed.2023.1089099
4. Roda G, Jharap B, Neeraj N, Colombel JF. Loss of response to anti-tnfs: definition, epidemiology, and management. Clin Transl Gastroenterol. 2016;7:e135. doi:10.1038/ctg.2015.63
5. Chanchlani N, Lin S, Bewshea C, et al. Mechanisms and management of loss of response to anti-TNF therapy for patients with Crohn’s disease: 3-year data from the prospective, multicentre PANTS cohort study. Lancet Gastroenterol Hepatol. 2024;9:521–538. doi:10.1016/S2468-1253(24)00044-X
6. Hirten RP, Iacucci M, Shah S, Ghosh S, Colombel JF. combining biologics in inflammatory bowel disease and other immune mediated inflammatory disorders. Clin Gastroenterol Hepatol. 2018;16:1374–1384. doi:10.1016/j.cgh.2018.02.024
7. Sands BE, Peyrin-Biroulet L, Loftus EV, et al. Vedolizumab versus Adalimumab for Moderate-to-Severe Ulcerative Colitis. N Engl J Med. 2019;381:1215–1226. doi:10.1056/NEJMoa1905725
8. Feagan BG, Sandborn WJ, Gasink C, et al. Ustekinumab as Induction and maintenance therapy for crohn’s disease. N Engl J Med. 2016;375:1946–1960. doi:10.1056/NEJMoa1602773
9. Feagan BG, Lasch K, Lissoos T, et al. Rapid response to vedolizumab therapy in biologic-naive patients with inflammatory bowel diseases. Clin Gastroenterol Hepatol. 2019;17:130–138.e7. doi:10.1016/j.cgh.2018.05.026
10. Parra RS, Chebli JMF, Queiroz NSF, et al. Long-term effectiveness and safety of ustekinumab in bio-naïve and bio-experienced anti-tumor necrosis factor patients with Crohn’s disease: a real-world multicenter Brazilian study. BMC Gastroenterol. 2022;22:199. doi:10.1186/s12876-022-02280-3
11. Ylisaukko-oja T, Af Björkesten CG, Eberl A, et al. Real-life treatment persistence and treatment outcomes of Finnish patients with inflammatory bowel disease receiving vedolizumab as first-line biological treatment. Heliyon. 2024;
12. Honap S, Agorogianni A, Colwill MJ, et al. JAK inhibitors for inflammatory bowel disease: recent advances. Frontline Gastroenterol. 2024;15:59–69. doi:10.1136/flgastro-2023-102400
13. Sipponen T, Af Björkesten CG, Hallinen T, et al. A nationwide real-world study on dynamic ustekinumab dosing and concomitant medication use among Crohn’s disease patients in Finland. Scand J Gastroenterol. 2021;56:661–670. doi:10.1080/00365521.2021.1906315
14. Farkas B, Bessissow T, Limdi JK, et al. Real-world effectiveness and safety of selective jak inhibitors in ulcerative colitis and crohn’s disease: a retrospective, multicentre study. J Clin Med. 2024;13:7804. doi:10.3390/jcm13247804
15. Panaccione R, Lee WJ, Clark R, et al. Dose escalation patterns of advanced therapies in crohn’s disease and ulcerative colitis: a systematic literature review. Adv Ther. 2023;40:2051–2081. doi:10.1007/s12325-023-02457-6
16. Ylisaukko-Oja T, Puttonen M, Jokelainen J, et al. Dose-escalation of Adalimumab, golimumab or ustekinumab in inflammatory bowel diseases: characterization and implications in real-life clinical practice. Scand J Gastroenterol. 2022;57:415–423. doi:10.1080/00365521.2021.2014950
17. Honap S, Chee D, Chapman TP, et al. Real-world effectiveness of tofacitinib for moderate to severe ulcerative colitis: a multicentre uk experience. J Crohns Colitis. 2020;14:1385–1393. doi:10.1093/ecco-jcc/jjaa075
18. Armuzzi A, daCosta DM, Tarallo M, et al. Treatment patterns among patients with moderate-to-severe ulcerative colitis in the United States and Europe. PLoS One. 2020;15:e0227914. doi:10.1371/journal.pone.0227914
19. Privitera G, Pugliese D, Lopetuso LR, et al. Novel trends with biologics in inflammatory bowel disease: sequential and combined approaches. Ther Adv Gastroenterol. 2021;14:17562848211006669. doi:10.1177/17562848211006669
20. Eberl A, Hallinen T, Af Björkesten CG, et al. Ustekinumab for Crohn’s disease: a nationwide real-life cohort study from Finland (FINUSTE). Scand J Gastroenterol. 2019;54:718–725. doi:10.1080/00365521.2019.1624817
21. Ylisaukko-Oja T, Torvinen S, Aaltonen J, et al. Characterization of inflammatory bowel disease management by vedolizumab and concomitant treatments in real-life clinical practice. Biol J Int Assoc Biol Stand. 2019;58:50–56.
22. Molander P, Kosunen M, Eronen H, et al. Tofacitinib real-world experience in ulcerative colitis in Finland (FinTofUC): a retrospective non-interventional multicenter patient chart data study. Scand J Gastroenterol. 2024;59:425–432. doi:10.1080/00365521.2023.2298361
23. Vermeire S, Gils A, Accossato P, Lula S, Marren A. Immunogenicity of biologics in inflammatory bowel disease. Ther Adv Gastroenterol. 2018;11:1756283X17750355. doi:10.1177/1756283X17750355
24. Fousekis FS, Papamichael K, Kourtis G, et al. The efficacy of immunomodulators in the prevention and suppression of anti-drug antibodies to anti-tumor necrosis factor therapy in inflammatory bowel disease. Ann Gastroenterol. 2022;35:1–7. doi:10.20524/aog.2021.0682
25. Sultan KS, Berkowitz JC, Khan S. Combination therapy for inflammatory bowel disease. World J Gastrointest Pharmacol Ther. 2017;8:103. doi:10.4292/wjgpt.v8.i2.103
26. Roblin X, Williet N, Boschetti G, et al. Addition of azathioprine to the switch of anti-TNF in patients with IBD in clinical relapse with undetectable anti-TNF trough levels and antidrug antibodies: a prospective randomised trial. Gut. 2020;69:1206–1212. doi:10.1136/gutjnl-2019-319758
27. Lemaitre M, Kirchgesner J, Rudnichi A, et al. Association between use of thiopurines or tumor necrosis factor antagonists alone or in combination and risk of lymphoma in patients with inflammatory bowel disease. JAMA. 2017;318:1679.
28. Dai C, Huang YH, Jiang M. Combination therapy in inflammatory bowel disease: current evidence and perspectives. Int Immunopharmacol. 2023;114:109545. doi:10.1016/j.intimp.2022.109545
29. Bernstein CN, Tenakoon A, Singh H, Targownik LE. Continued 5ASA use after initiation of anti-TNF or immunomodulator confers no benefit in IBD: a population-based study. Aliment Pharmacol Ther. 2021;54:814–832. doi:10.1111/apt.16518
30. Dubois-Camacho K, Ottum PA, Franco-Muñoz D, et al. Glucocorticosteroid therapy in inflammatory bowel diseases: from clinical practice to molecular biology. World J Gastroenterol. 2017;23:6628–6638. doi:10.3748/wjg.v23.i36.6628
31. Jeuring SFG, Biemans VBC, van den Heuvel TRA, et al. Corticosteroid sparing in inflammatory bowel disease is more often achieved in the immunomodulator and biological era-results from the dutch population-based IBDSL cohort. Am J Gastroenterol. 2018;113:384–395. doi:10.1038/ajg.2017.482
32. Barreiro-de Acosta M, Lorenzo A, Mera J, Dominguez-Muñoz JE. Mucosal healing and steroid-sparing associated with infliximab for steroid-dependent ulcerative colitis. J Crohns Colitis. 2009;3:271–276. doi:10.1016/j.crohns.2009.06.003
33. Singh H, Wilson L, Tencer T, Kumar J. Systematic literature review of real-world evidence on dose escalation and treatment switching in ulcerative colitis. Clin Outcomes Res. 2023;15:125–138. doi:10.2147/CEOR.S391413
34. Meijboom RW, Gardarsdottir H, Becker ML, et al. Switching TNFα inhibitors: patterns and determinants. Pharmacol Res Perspect. 2021;
35. Chen C, Hartzema AG, Xiao H, et al. Real-world pattern of biologic use in patients with inflammatory bowel disease: treatment persistence, switching, and importance of concurrent immunosuppressive therapy. Inflamm Bowel Dis. 2019;25:1417–1427.
36. Jung YS, Han M, Park S, Cheon JH. Biologic use patterns and predictors for non-persistence and switching of biologics in patients with inflammatory bowel disease: a nationwide population-based study. Dig Dis Sci. 2020;65:1436–1444. doi:10.1007/s10620-019-05867-1
37. Koo HM, Jun YK, Choi Y, et al. 10 years of biologic use patterns in patients with inflammatory bowel disease: treatment persistence, switching and dose intensification – a nationwide population-based study. Ther Adv Gastroenterol. 2023;16:17562848231201728. doi:10.1177/17562848231201728
38. Kontola K, Oksanen P, Huhtala H, Jussila A. Increasing Incidence of inflammatory bowel disease, with greatest change among the elderly: a nationwide study in Finland, 2000–2020. J Crohns Colitis. 2023;17:706–711. doi:10.1093/ecco-jcc/jjac177
39. Vermeire S, Noman M, Van Assche G, Baert F, D’Haens G, Rutgeerts P. Effectiveness of concomitant immunosuppressive therapy in suppressing the formation of antibodies to infliximab in Crohn’s disease. Gut. 2007;56:1226–1231. doi:10.1136/gut.2006.099978
40. Strik AS, van den Brink GR, Ponsioen C, Mathot R, Löwenberg M, D’Haens GR. Suppression of anti-drug antibodies to infliximab or Adalimumab with the addition of an immunomodulator in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2017;45:1128–1134. doi:10.1111/apt.13994
41. Ko Y, Paramsothy S, Yau Y, Leong RW. Superior treatment persistence with ustekinumab in Crohn’s disease and vedolizumab in ulcerative colitis compared with anti-TNF biological agents: real-world registry data from the Persistence Australian National IBD Cohort (PANIC) study. Aliment Pharmacol Ther. 2021;54:292–301. doi:10.1111/apt.16436
42. Feagan BG, McDonald JWD, Panaccione R, et al. Methotrexate in combination with infliximab is no more effective than infliximab alone in patients with crohn’s disease. Gastroenterology. 2014;146:681–688.e1. doi:10.1053/j.gastro.2013.11.024
43. Matsumoto T, Motoya S, Watanabe K, et al. Adalimumab monotherapy and a combination with azathioprine for crohn’s disease: a prospective, randomized trial. J Crohns Colitis. 2016;10:1259–1266. doi:10.1093/ecco-jcc/jjw152
44. Yzet C, Diouf M, Singh S, et al. No benefit of concomitant immunomodulator therapy on efficacy of biologics that are not tumor necrosis factor antagonists in patients with inflammatory bowel diseases: a meta-analysis. clin. Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. 2021;19:668–679.e8.
45. Hu A, Kotze PG, Burgevin A, et al. Combination therapy does not improve rate of clinical or endoscopic remission in patients with inflammatory bowel diseases treated with vedolizumab or ustekinumab. clin. Gastroenterol Hepatol. 2021;19:1366–1376.e2.
46. Hanzel J, Ma C, Jairath V. Upadacitinib for the treatment of moderate-to-severe crohn’s disease. Immunotherapy. 2024;16:345–357. doi:10.2217/imt-2023-0293
47. Sedano R, Ma C, Jairath V, Feagan BG. Janus kinase inhibitors for the management of patients with inflammatory bowel disease. Gastroenterol Hepatol. 2022;18:14–27.
48. Lucaciu LA, Constantine-Cooke N, Plevris N, et al. Real-world experience with tofacitinib in ulcerative colitis: a systematic review and meta-analysis. Ther Adv Gastroenterol. 2021;14:17562848211064004. doi:10.1177/17562848211064004
49. Singh S, Proudfoot JA, Dulai PS, et al. No benefit of concomitant 5-aminosalicylates in patients with ulcerative colitis escalated to biologic therapy: pooled analysis of individual participant data from clinical trials. Am J Gastroenterol. 2018;113:1197–1205. doi:10.1038/s41395-018-0144-2
50. Buchman AL. Side effects of corticosteroid therapy. J Clin Gastroenterol. 2001;33:289–294. doi:10.1097/00004836-200110000-00006
51. Wu H, Xie T, Yu Q, et al. An analysis of the effectiveness and safety of upadacitinib in the treatment of inflammatory bowel disease: a multicenter real-world study. Biomedicines. 2025;13:190. doi:10.3390/biomedicines13010190
52. Kolehmainen S, Rautakorpi J, Löyttyniemi E, et al. Real-life experiences of switching from intravenous to subcutaneous vedolizumab maintenance therapy in patients with inflammatory bowel disease. Eur J Gastroenterol Hepatol. 2024;36:1193–1201. doi:10.1097/MEG.0000000000002816
53. Ylisaukko-Oja T, Aaltonen J, Nuutinen H, et al. High treatment persistence rate and significant endoscopic healing among real-life patients treated with vedolizumab - a Finnish Nationwide Inflammatory Bowel Disease Cohort Study (FINVEDO). Scand J Gastroenterol. 2018;53:158–167. doi:10.1080/00365521.2017.1416160
54. Honap S, Irving PM, Samaan MA. JAK inhibitors for the treatment of inflammatory bowel disease: results of an international survey of perceptions, attitudes, and clinical practice. Eur J Gastroenterol Hepatol. 2023;35:1270–1277. doi:10.1097/MEG.0000000000002650
55. Adimadhyam S, Lewis JD, Simon AL, et al. Real-world evidence comparing tofacitinib and vedolizumab in anti-tnf-experienced patients with ulcerative colitis. Inflamm Bowel Dis. 2024;30:554–562. doi:10.1093/ibd/izad115
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.