Back to Journals » Advances in Medical Education and Practice » Volume 16
Knowledge, Perspectives, and Interests of Dental Surgery Students Towards Oral Health Policy of Malawi
Authors Kafera G ![]() , Bagg J, Chimimba P, Mchenga JM, Chiwaya D, Samonte GC, Bwanali AN
, Bagg J, Chimimba P, Mchenga JM, Chiwaya D, Samonte GC, Bwanali AN ![]() , Ham E, Chung J, Choi Y, Park SY
, Ham E, Chung J, Choi Y, Park SY ![]() , Lee SS, Chung SJ, Lubanga AF
, Lee SS, Chung SJ, Lubanga AF
Received 29 July 2025
Accepted for publication 5 December 2025
Published 10 December 2025 Volume 2025:16 Pages 2299—2305
DOI https://doi.org/10.2147/AMEP.S552782
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sateesh Arja
George Kafera,1 Jeremy Bagg,2 Peter Chimimba,1 James Maurice Mchenga,1 Don Chiwaya,1 Gian Carlo Samonte,3 Akim Nelson Bwanali,4 Emily Ham,5 Jaeha Chung,5 Yeonho Choi,5 So Yeon Park,5 Simon SangWon Lee,5 Sung Jae Chung,5 Adriano Focus Lubanga4
1School of Medicine and Oral Health, Kamuzu University of Health Sciences, Blantyre, Malawi; 2School of Medicine, Dentistry and Nursing, University of Glasgow, Glasgow, UK; 3Ministry of Health, Kamuzu Central Hospital, Lilongwe, Malawi; 4Research & Development, Clinical Research Education and Management Services, Lilongwe, Malawi; 5Research, Youth with Talents, Fairfax, VA, USA
Correspondence: George Kafera, Kamuzu University of Health Sciences, Post Office Box 360, Chichiri, Blantyre 3, Malawi, Tel +265 991 379 603, Email [email protected]
Background: The development of Malawi’s first National Oral Health Policy (MNOHP) in 2022 marked a milestone in strengthening the country’s oral health system. However, the extent to which future oral health professionals are aware of and prepared to implement this policy remains unclear. This study explored the knowledge, perspectives, and interest of dental surgery students in Malawi regarding the MNOHP, with the aim of identifying educational and policy engagement gaps.
Methods: A descriptive cross-sectional exploratory survey was conducted among all willing clinical-year dental students enrolled in Malawi’s sole Bachelor of Dental Surgery (BDS) program at Kamuzu University of Health Sciences. Data were collected using a structured, self-administered questionnaire developed from validated tools and refined through expert review and piloting. Descriptive analyses summarized participants’ demographic characteristics, policy knowledge, exposure, and perspectives on curriculum integration. Ethical approval was obtained from the College of Medicine Research and Ethics Committee (P.11/24-1270).
Results: A total of 43 students participated (response rate 95.6%). Most participants were male (60.5%) and enrolled in Year 3 or 4. Awareness of the MNOHP was limited: only 27.9% correctly identified its launch year (2022) and 9.8% knew it had seven priority areas. Although 85.0% had never read the policy and 97.6% reported not being taught about it, all respondents expressed strong interest in learning more and participating in policy development. A majority (88.4%) believed oral health policy education should be compulsory, and over half (51.2%) preferred that it be introduced during the clinical years.
Conclusion: Malawian dental students exhibit enthusiasm to engage in oral health policy but lack foundational knowledge of the MNOHP. Integrating structured policy education within the dental curriculum covering the policy’s seven priority areas of leadership, prevention, access, workforce, financing, infrastructure, and research could bridge this gap. Building policy literacy among future dentists is essential for effective policy implementation and long-term improvement of oral health outcomes in Malawi.
Keywords: curriculum development, dental education, dental students, Malawi, oral health policy, policy awareness
Introduction
Oral health policy is a cornerstone of effective health-system governance because it links -preventive, educational, and clinical strategies to population well-being.1–4 High-quality oral health systems contribute directly to universal health coverage and to the achievement of the Sustainable Development Goals.5 To achieve these goals, countries must align the training of oral-health professionals with national priorities and ensure that future dentists and dental teams understand how policy translates into practice.6
In sub-Saharan Africa, oral diseases remain a major public-health concern, yet policy awareness and implementation capacity within the health workforce are limited.7,8 Although the World Health Organization (WHO) has long advocated for national oral-health policies, only a few African countries have developed and operationalized them.8 Even where policies exist, dissemination and integration into dental education are often weak. Recent studies in Ghana, South Africa, and Rwanda reveal low levels of oral-health policy awareness and limited curricular emphasis on health-policy issues among students and practitioners.9–11 These findings highlight a regional gap between policy formulation and implementation, driven partly by limited exposure of trainees to policy content.
Malawi has recently made important progress through the development of the National Oral Health Policy (NOHP), officially disseminated in 2022 under the MalDent Project.7,12 The policy has seven priority areas to guide implementation and help achieve its objectives. These are: (1) Leadership and Governance; (2) Dental Public Health; (3) Clinical Practice and Patient Access; (4) Human Resources for Oral Health; (5) Oral Health Financing; (6) Infrastructure and Equipment; and (7) Research, Data and Information Management.13
Each priority area addresses a fundamental dimension of the oral health system: leadership and governance focus on oversight and regulation; dental public health emphasizes prevention and population-based approaches; clinical practice and access ensure that dental services reach those in need; human resources encompass training, deployment and retention of dental personnel; financing covers resource allocation and sustainability; infrastructure and equipment pertain to physical and technological capacity; and research/data management ensures evidence-based decision making.13
By foregrounding these priority areas, the MNOHP provides a comprehensive roadmap for aligning education, service delivery and policy implementation in Malawi’s oral health sector. However, the extent to which future oral-health professionals are aware of, or prepared to implement, this policy has not yet been studied. The Bachelor of Dental Surgery (BDS) programme, introduced in 2019 at Kamuzu University of Health Sciences, represents Malawi’s first and only dental-training pathway.14 Understanding the knowledge and perspectives of its students is therefore critical for successful policy implementation and curriculum strengthening.
Despite global and regional research on students’ exposure to health policy,15–18 no study in Malawi has examined dental students’ familiarity with or attitudes toward the national oral-health policy. This exploratory study therefore investigated Malawian dental surgery students’ knowledge, perspectives, and interest in the MNOHP. By identifying educational and systemic gaps, the findings can inform curriculum review, guide faculty development, and provide locally grounded evidence to support the ongoing implementation of the MNOHP.
Materials and Methods
Study Design and Setting
This exploratory cross-sectional survey targeted all willing clinical-year (Years 3 to 5), dental surgery students at Kamuzu University of Health Sciences both male and female enrolled. This is the only accredited dental training programme in Malawi during the study period Data collection occurred in the month of April, 2025. Because the national BDS programme is newly established (first clinical cohort graduated in 2025), the accessible population of clinical students was small; therefore, we elected all willing students, rather than a sample-based approach.14
Sample Size and Sampling Approach
The total number of eligible clinical-year (Years 3–5) students at the time of the study was approximately 50.19 Given the limited cohort size, a conventional sample-size calculation for hypothesis testing would not be meaningful; instead, the study is positioned as exploratory/pilot research describing knowledge and perspectives in the entire accessible cohort.
Questionnaire Development and Validation
The survey instrument was adapted from validated and published KAP and health-policy awareness questionnaires used in related studies and then tailored to the Malawi context.12,14,15 To enhance content validity, the draft instrument underwent expert review by three senior oral health academicians and clinicians who recommended modifications to improve cultural and contextual relevance. The revised instrument was then piloted with a small group of dental students who were not included in the final dataset; pilot feedback informed wording and response-option adjustments.
We did not compute internal consistency measures (eg, Cronbach’s alpha) because the tool was comprised mainly discrete factual and attitudinal items rather than multi-item psychometric scales, and the study was exploratory and used expert review plus piloting to establish acceptable face and content validity. The questionnaire included demographic characteristics (2 items) capturing participants’ gender and year of study, Knowledge of the MNOHP (4 items) assessing familiarity with the policy’s launch year, number of priority areas, the last part of the questionnaire, comprised of its main purpose and Interests and perspectives toward oral health policy (5 items) exploring whether students had read or been taught about the MNOHP, their interest in learning more, willingness to participate in policy development, and views on integrating policy education into the dental curriculum.
Data Collection Procedure
The questionnaire was distributed in person to all eligible students with informed consent. Participation was voluntary and anonymous; reminders were issued to maximise response. Data collectors provided clarifications when requested but did not influence responses.
Data Analysis
Given that the BDS program in Malawi currently enrolls a very small number. Hence, the study’s strength lies in its style descriptive design, not in inferential generalization. We have therefore focused on presenting descriptive summaries and frequency distributions to capture these valuable baseline insights for future, larger-scale studies.
Ethical Considerations
Ethical approval was obtained from the College of Medicine Research and Ethics Committee (COMREC) (reference P.11/24-1270).
Results
Participant Flow and Characteristics
A total of 45 dental surgery students were initially invited to participate in the study. Two questionnaires were excluded from the analysis due to missing key demographic information (gender and year of study). The final analytic sample therefore comprised 43 participants, representing a response rate of 95.6%.
Table 1 shows that, of these 43 participants, 60.5% (n = 26) were male and 39.5% (n = 17) were female. In terms of academic year, 44.2% (n = 19) were third-year students, 41.9% (n = 18) were in fourth year, and 14.0% (n = 6) were in fifth year. The mean age of the students was not collected, but all were within the typical age range for undergraduate dental trainees (20–28 years). There were no missing data for gender and academic year among the included participants.
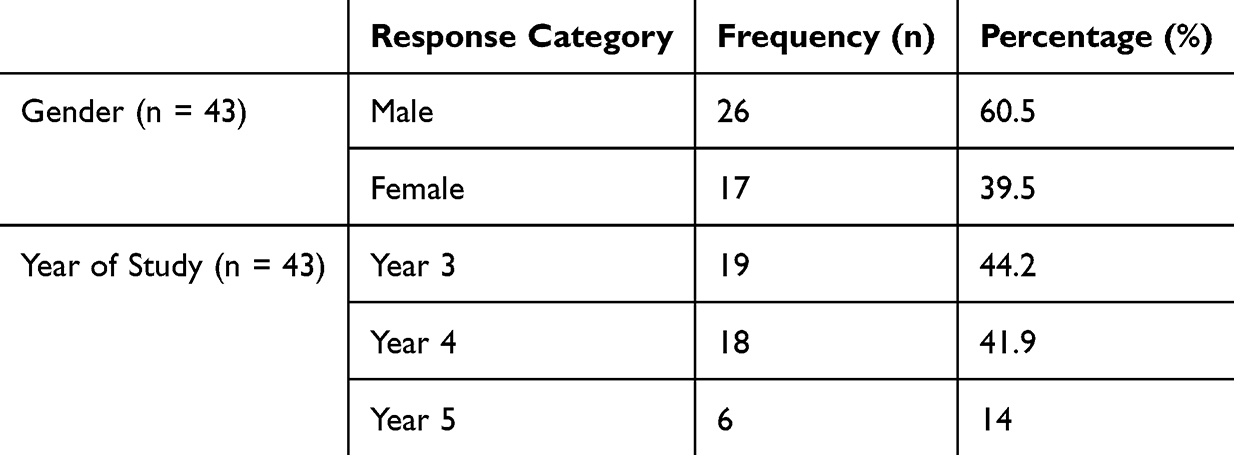 |
Table 1 Demographic Characteristics of the Participants |
Knowledge of the Malawi National Oral Health Policy (MNOHP)
Table 2 summarizes participants’ knowledge of the MNOHP.
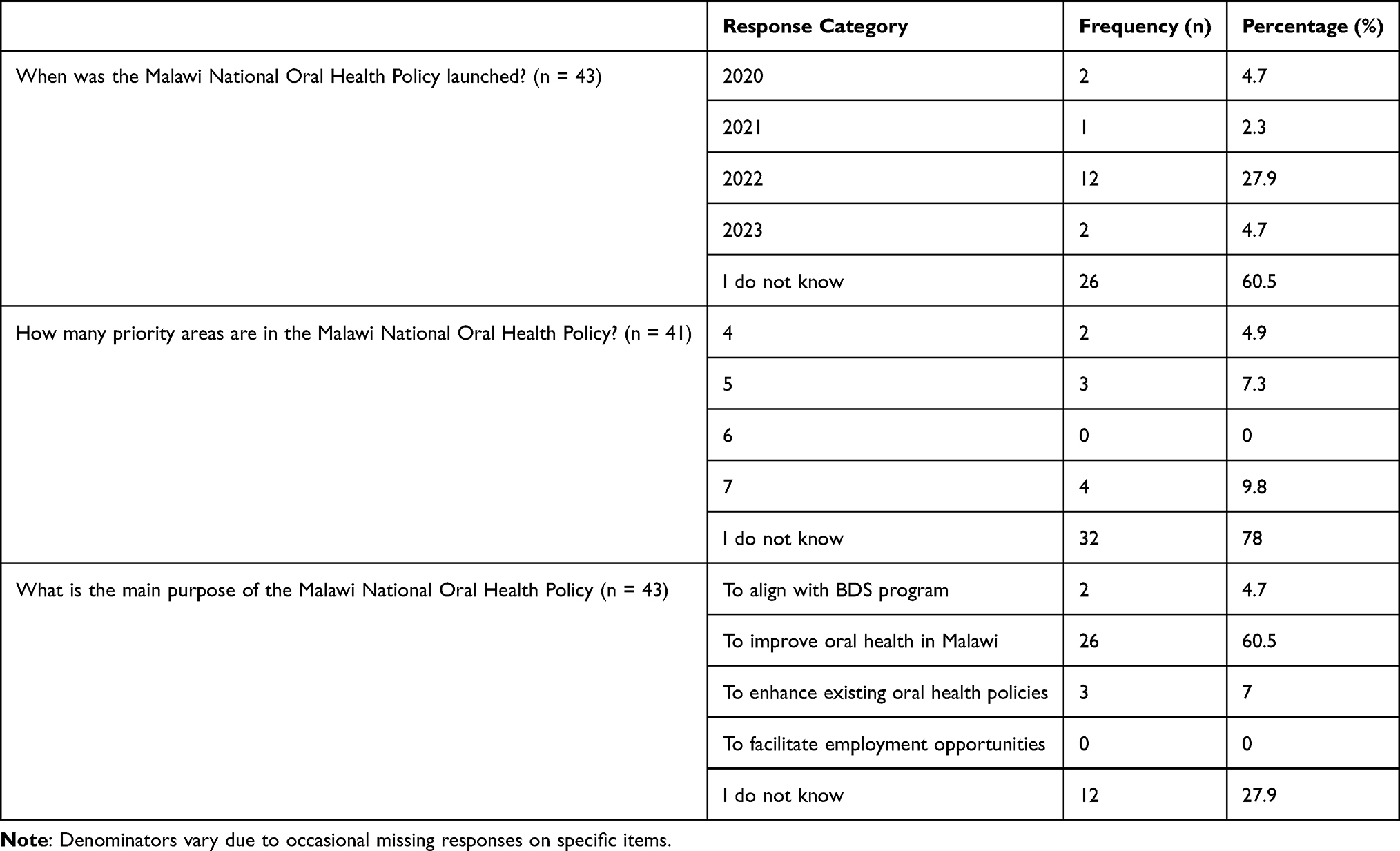 |
Table 2 Knowledge of the Malawi National Oral Health Policy (MNOHP) |
The majority of respondents (60.5%, n = 26) reported that they were unsure when the policy was launched, whereas 27.9% (n = 12) correctly identified 2022 as the launch year. A small number (11.6%, n = 5) gave incorrect responses, indicating 2020, 2021, or 2023.
When asked about the number of priority areas outlined in the MNOHP, 78.0% (n = 32) indicated they were unsure, while only 9.8% (n = 4) correctly reported that the policy includes seven priority areas. The remaining respondents provided incorrect answers, most commonly “four” or “five”.
Regarding the main purpose of the MNOHP, 60.5% (n = 26) correctly identified it as a framework for improving oral health in Malawi. A smaller proportion (27.9%, n = 12) were uncertain, and the remainder selected incorrect alternatives such as enhancing existing policies or aligning with the Bachelor of Dental Surgery (BDS) program.
Perspectives and Interests Towards Malawi National Oral Health Policy
Most participants (85.0%, n = 34) indicated that they had never read the MNOHP document. Similarly, nearly all (97.6%, n = 40) reported that oral health policy content had not been included in their current dental school curriculum (Table 3).
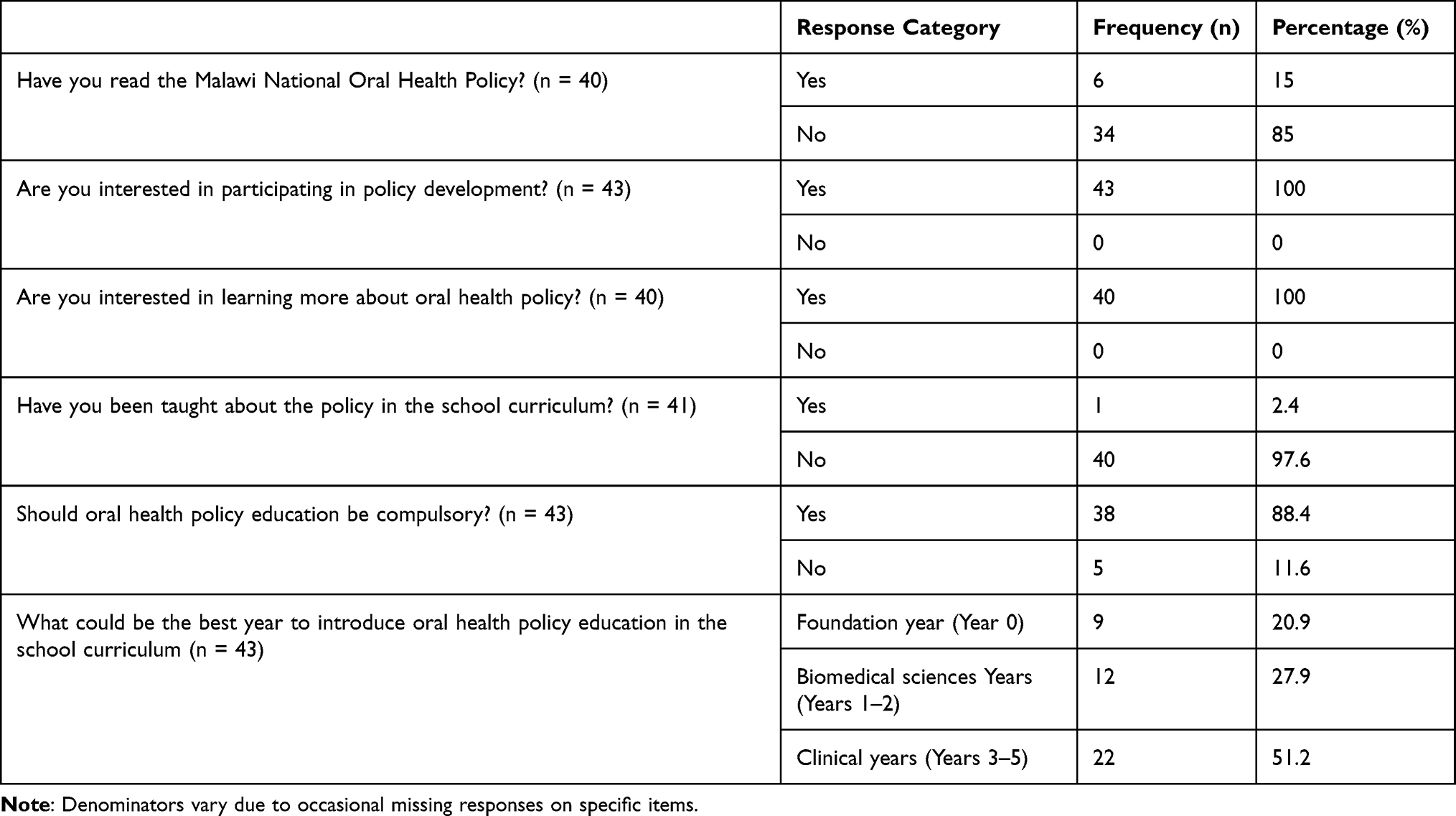 |
Table 3 Perspectives and Interests Towards Malawi National Oral Health Policy |
Despite this limited exposure, enthusiasm for learning about and participating in oral health policy was universal. All respondents (100%, n = 40) expressed a strong interest in learning more about the MNOHP, and all (100%, n = 37) stated their willingness to contribute to oral health policy development in the future. As shown in Table 3, the large majority (88.4%, n = 38) believed that oral health policy should be a compulsory component of the dental curriculum. When asked about the most suitable time for policy integration in the school curriculum, 51.2% (n = 22) recommended introducing it during the clinical years (Years 3–5). Another 27.9% (n = 12) preferred it to be taught during the biomedical sciences phase (Years 1–2), while 20.9% (n = 9) favored inclusion during the foundation year (Year 0).
Discussion
This study examined the knowledge, perspectives, and engagement of dental surgery students in Malawi regarding the Malawi National Oral Health Policy (MNOHP). The findings demonstrate a substantial gap in students’ awareness of the policy’s core components, such as its launch year and priority areas, reflecting a broader disconnect between national policy frameworks and dental education in Malawi.
The limited knowledge observed among participants may stem from several structural factors. First, dissemination of the MNOHP within academic and professional circles remains inadequate. Many students may have had no formal introduction to the policy, and faculty members themselves may not yet be fully conversant with its contents or implementation strategies. Second, the Bachelor of Dental Surgery (BDS) curriculum, launched only in 2019, is still evolving, and currently lacks systematic integration of health policy or oral health systems management content. Similar gaps have been reported in Kenya and Rwanda, where weak institutional links between training institutions and health ministries have constrained students’ understanding of national health strategies.20 Moreover, oral health policy in many African countries has historically received low visibility compared to clinical training priorities.21
Despite these deficits, the study found encouraging levels of enthusiasm among students to learn about and engage with oral health policy. This enthusiasm represents an important educational opportunity. Introducing structured learning experiences such as policy seminars, guest lectures from Ministry of Health officials, or interdisciplinary policy simulation exercises could strengthen students’ health systems literacy. Studies from South Africa and Nigeria have demonstrated that including health systems and policy modules in dental and medical training enhances students’ ability to connect clinical practice to national development goals.22,23
The finding that knowledge gaps were consistent across all years of study highlights that policy education should not be restricted to senior clinical stages. Instead, oral health policy concepts should be integrated throughout the curriculum, beginning from foundational years. Early exposure can build a progressive understanding of how governance, financing, and policy frameworks shape service delivery and population oral health. This approach aligns with recommendations by the WHO Regional Office for Africa, which emphasizes embedding oral health policy education within undergraduate training to support effective policy implementation and advocacy.24
These findings correspond with global trends showing limited health policy awareness among students in both high- and low-income countries. However, in Malawi, the issue is accentuated by resource limitations, a young dental education system, and recent policy adoption. Strengthening oral health policy literacy among students not only aligns education with national goals but also contributes to building a new generation of dental professionals capable of engaging in evidence-informed decision-making and leadership within Malawi’s oral health system.
Limitations and Future Perspectives
This study was limited by its small sample size and single-institution design, which restricts generalizability. However, it represents the almost full cohort of clinical dental surgery students in Malawi at the time, providing nationally relevant baseline insights. The questionnaire was expert-reviewed and piloted but not formally tested for reliability. Future studies involving multiple institutions and larger cohorts are recommended to validate and expand these findings and to explore qualitative perspectives on how students engage with national oral health policy.
Conclusion
This study demonstrates that although dental surgery students in Malawi are keen and motivated to engage with oral health policy, their knowledge of the Malawi National Oral Health Policy remains limited. This gap underscores the urgent need for educational strategies that integrate policy literacy into the dental curriculum, ensuring future practitioners understand and actively contribute to national oral health objectives.
The findings highlight opportunities to strengthen each domain of policy priorities through targeted training, resources and institutional support. To transform interest into impact, stakeholders should: incorporate policy modules into the BDS curriculum, provide accessible policy documents and case-studies, facilitate mentorship linking students with oral health policy actors, and monitor progress through national oral health data systems. Equipping next-generation dentists with both clinical skills and policy fluency empowers them not just as service providers but as agents of change. Only by doing so can Malawi move from policy development to effective implementation and improved oral health outcomes across the population.
Data Sharing Statement
The data used in this study can be found on: Doc II.csv - Google Drive.
Acknowledgments
The authors would like to express their sincere gratitude to Prof. Jeremy Bagg for his guidance in the development of the data collection tool and his mentorship throughout the study. Special thanks also go to Dr. Adriano Lubanga for his mentorship, administrative support, and for inspiring and introducing the lead author to research—a role he continues to play as a key mentor. The authors also acknowledge Dr. James Mchenga, the Head of the Department of Oral Health Sciences at Kamuzu University of Health Sciences, for granting approval to engage dental students in the study. Finally, we extend our appreciation COMREC at Kamuzu University of Health Sciences for approving the study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Health systems governance for universal health coverage action plan: department of health systems governance and financing. Geneva: World Health Organization; 2014. Available from: https://iris.who.int/rest/bitstreams/1346130/retrieve.
2. Moutselos K, Maglogiannis I. Evidence-based public health policy models development and evaluation using big data analytics and web technologies. Med Arch. 2020;74(1):47. doi:10.5455/medarh.2020.74.47-53
3. Dang A, Likhar N, Alok U. Importance of economic evaluation in health care: an Indian perspective. Value Health Reg Issues. 2016;9:78–83. doi:10.1016/j.vhri.2015.11.005
4. Bhattacharya D, Bhatt J. Seven foundational principles of population health policy. Popul Health Manag. 2017;20(5):383–388. doi:10.1089/pop.2016.0148
5. Thapa G, Jhalani M, García-Saisó S, Malata A, Roder-DeWan S, Leslie HH. High quality health systems in the SDG era: country-specific priorities for improving quality of care. PLoS Med. 2019;16(10):e1002946. doi:10.1371/journal.pmed.1002946
6. Busse R, Panteli D, Quentin W. An introduction to healthcare quality: defining and explaining its role in health systems. In: Busse R, Klazinga N, Panteli D, Quentin W, editors. Improving Healthcare Quality in Europe: Characteristics, Effectiveness and Implementation of Different Strategies. Copenhagen: WHO Regional Office for Europe; 2019.
7. The MalDent Project. Successful National Oral Health Policy dissemination & implementation workshop. 2022. Available from: https://themaldentproject.com/2022/12/04/successful-national-oral-health-policy-dissemination-implementation-workshop/.
8. World Health Organization. Writing oral health policy: a manual for oral health managers in the WHO African region. Brazzaville: WHO Regional Office for Africa; 2005. Available from: https://apps.who.int/iris/bitstream/handle/10665/204462/AFR_ORH_05.1.pdf.
9. Appiah EO, Arthur N, Asiamah V, et al. Oral health knowledge and behaviour among Ghanaian teachers. Int J Dent. 2020;2020:6458512.
10. Mfolo T, Madiba TK, Bhayat A. Oral health knowledge, attitudes and practices among school teachers in Tshwane District, South Africa. S Afr Dent J. 2021;76(5):250–256. doi:10.17159/10.17159/2519-0105/2021/v76no6a3
11. Munyaneza E, Gishoma J, Ntaganda E, et al. Oral health attitudes and training gaps among schoolteachers in Rwanda. Int J Health Sci Res. 2021;11(3):36–41.
12. Matanhire-Zihanzu CN, Chambers S, Bagg J, Chimimba P. Assessing Malawi’s recent development of a national oral health policy–learning for the future. J Glob Health Rep. 2022;6:e2022062.
13. Government of the Republic of Malawi. National Oral Health Policy (Revised Final VR12). Lilongwe: Ministry of Health, Malawi; 2022. Available from: https://themaldentproject.com/wp-content/uploads/2022/05/National-Oral-Health-Policy-Vr-12-Revised-Final-PRINT-VERSION-17-03-22-1.pdf.
14. Kamuzu University of Health Sciences (KUHeS). Medicine and Oral Health – the only institution training doctors and dentists in Malawi. Lilongwe/Blantyre: KUHeS; [cited July 2025]. Available from: https://www.kuhes.ac.mw/medicine-and-oral-health.
15. Malik B, Ojha U, Khan H, Begum F, Khan H, Malik Q. Medical student involvement in health policy roles. Adv Med Educ Pract. 2017;8:735–743. doi:10.2147/AMEP.S147212
16. Haque M, Rahman NA, Rahman S, et al. Medical students’ perception regarding health policy teaching and their participation in health policy roles: a survey at a public university in Malaysia. Healthcare. 2022;10(6):967. doi:10.3390/healthcare10060967
17. Agrawal JR, Huebner J, Hedgecock J, Sehgal AR, Jung P, Simon SR. Medical students’ knowledge of the US health care system and their preferences for curricular change: a national survey. Acad Med. 2005;80(5):484–488. doi:10.1097/00001888-200505000-00017
18. Patel MS, Lypson ML, Davis MM. Medical student perceptions of education in health care systems. Acad Med. 2009;84(9):1301–1306. doi:10.1097/ACM.0b013e3181b17e3e
19. Infodent International. “Joint working between 2017 and 2019 allowed the creation of a BDS curriculum … This total of 52 dental students is greater than the number of dentists in the country.” 2023; (IDS 2023 2):94. Available from: https://www.infomedixinternational.com/magazine/download/ids_2023_2.pd.
20. Chikte UM, Brand AA, Lewis HA. Attitudes and perceptions of dental students to the inclusion of dental public health in the curriculum. Oral Epidemiol. 1990;18(3):134–137.
21. Okeigbemen SA, Ehizele AO. Dental public health education in Nigerian dental schools: a review of curriculum and training needs. Ann Med Health Sci Res. 2015;5(4):275–281.
22. Moodley R, Naidoo S. The role of dental education in promoting health systems understanding in South Africa. S Afr Dent J. 2021;76(8):402–408.
23. Ibekwe TS, Olatosi OO, Folayan MO. Oral health policy awareness and education among Nigerian dental students. BMC Oral Health. 2019;19:114. doi:10.1186/s12903-019-0811-8
24. World Health Organization Regional Office for Africa. Writing Oral Health Policy: A Manual for Oral Health Managers in the WHO African Region. Brazzaville: WHO-AFRO; 2005.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.