Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
The Burden of Analgesics Overprescription for Chronic Headache: Impacts on Patients, Healthcare System and Countries
Authors Alshareef MH ![]() , Alsanosi SM
, Alsanosi SM ![]()
Received 8 June 2025
Accepted for publication 29 October 2025
Published 4 November 2025 Volume 2025:18 Pages 7193—7202
DOI https://doi.org/10.2147/JMDH.S545515
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Maram H Alshareef,1 Safaa M Alsanosi2
1Department of Community Medicine and Pilgrims Health Care, Faculty of Medicine, Umm Al Qura University, Makkah, Saudi Arabia; 2Department of Pharmacology and Toxicology, Faculty of Medicine, Umm Al Qura University, Makkah, Saudi Arabia
Correspondence: Maram H Alshareef, Department of Community Medicine and Pilgrims Health Care, Faculty of Medicine, Umm Al-Qura University, Makkah, 21955, Saudi Arabia, Email [email protected]
Abstract: Chronic headache (CH) is a leading cause of debilitating disorders, with many headache types remaining undiagnosed due to improper medication use. This misuse not only worsens the underlying condition but also leads to a secondary problem: medication overuse headache (MOH). This creates a cycle of increasingly complex headache cases, posing significant challenges for patients, healthcare providers, and the healthcare system as a whole. Physicians often contribute to this issue by prescribing analgesics without proper assessment or adequately educating patients on their correct use, thereby increasing the risk of MOH. However, MOH is a preventable condition. Prevention relies on educating both healthcare providers—through adherence to headache management guidelines—and patients, empowering them to use medications appropriately. This article provides a comprehensive review of the consequences of overprescription analgesics for CH population, and effective prevention strategies to mitigate its impact.
Keywords: medication overuse headache, chronic headache, impacts, patients, health care facilities
Introduction
CH, defined as a headache occurring on 15 or more days per month for at least three months. It is a debilitating condition that affects millions of people worldwide.1 It encompasses various headache disorders, including chronic migraine, chronic tension-type headache, and medication-overuse headache, each presenting unique challenges in diagnosis and treatment.2 It significantly impacts quality of life, contributing to persistent pain, psychological distress, and functional impairment. Unlike episodic headaches, which occur sporadically, CH has a continuous presence that disrupts daily activities and often requires long-term management.3,4 Although the precise mechanisms leading to CH remain under investigation, factors like genetic predisposition, stress, lifestyle, and medication overuse are known contributors.5,6 Treatment typically involves a combination of preventive medications, lifestyle modifications, and non-pharmacological therapies, aiming to reduce headache frequency and improve quality of life.7
In this review, we searched the impacts of over prescription of acute pain control analgesics for headache disorders on patient, health care facilities and countries to explore the burden of overprescription and open the eyes of health care provider to the importance of following the guideline for headache management.
Methods and Materials
Published articles in the scientific literature examining the impacts of analgesics overprescription on CH disorders. We searched for relevant publications, including retrospective cohort studies, prospective studies, randomised controlled trials, systematic reviews and meta-analyses, using PubMed, Embase, Google Scholar and Web of Science. We used the following keywords and search terms: [medication overuse headache], [chronic headache], [effects], [impact], [effect], [healthcare system], [health care provider], [countries], [physicians], and [patients].
To maintain methodological rigour and transparency, the inclusion criteria encompassed peer-reviewed studies conducted on human participants, published in English, and explicitly examining the association between analgesic use, overprescription, and outcomes related to chronic headache (CH) or medication-overuse headache (MOH). The exclusion criteria eliminated non-original publications, including commentaries, conference abstracts lacking full texts, and studies unrelated to headache disorders.
The initial database search identified 248 records, of which 76 studies satisfied the inclusion criteria following a multi-stage screening process based on titles, keywords, abstracts, and full texts. All eligible articles were restricted to the English language, with no limitations placed on publication date, ensuring a comprehensive and unbiased representation of the available evidence.
Result
The pathophysiology of CH disorders varies across different headache types, primarily chronic migraine (CM), chronic tension-type headache (CTTH), and medication-overuse headache (MOH). The management of CH depends on the headache type, there is different prophylaxis treatment for each type that help to prevent or lessen the acute attacks and in order reduce the over the counter medication use. Understanding these differences provides insight into the complex mechanisms of CH and guides targeted treatments.
Chronic Migraine (CM)
CM defined as headache attacks more than 15 days per month eight of them associated with migraine features.8 The prevalence of this condition is around 2%.9 The pathophysiology involves neurological, vascular, and inflammatory components. It is thought to be a result from central sensitization, a process where repeated migraine episodes increase sensitivity to pain due to heightened neural response in the trigeminal pain pathway and central nervous system structures, including the brainstem and cortex.10 Changes in cortical excitability and disruptions in pain-modulating pathways are also associated with chronic migraine, leading to the perception of pain even in response to non-painful stimuli.11 This chronic state may be perpetuated by hormonal factors, environmental triggers, and genetic predispositions that predispose individuals to chronicity.12
Chronic Tension-Type Headache (CTTH)
CTTH defined as bilateral pressure or band like pain attacks for 15 days per month last for hours or days not associated with migraine or cluster features. Several literatures showed that the prevalence of CTTH is around 4%.13 The pathophysiology of CTTH believed to stem from peripheral muscle tension and central sensitization mechanisms, similar to those in chronic migraine but with distinct pain pathways.14 In CTTH, nociceptive signals from pericranial muscles are thought to contribute to pain, as many patients experience muscular tenderness around the neck and scalp.15 Over time, repetitive peripheral inputs from muscle tension are believed to contribute to central sensitization, resulting in pain sensitivity and lower pain thresholds, even in the absence of muscle tightness.16 Alterations in serotonin and other neurotransmitter systems may also contribute to the pathophysiology of CTTH, suggesting that the headache’s origin is multifactorial and not solely due to muscle strain.17
Medication-Overuse Headache (MOH)
MOH is unique in that it is induced by the overuse of analgesics or migraine-specific drugs (eg, triptans) more than 15 days per month for 3 months or more. It can develop from episodic migraine or tension-type headache.5 The prevalence of MOH near CM which around 2%.5,18 Studies have shown that among patients at specialized headache centers, the prevalence of MOH ranges from 30% to 50%, which is much higher than in the general population. Its prevalence increased among individuals with migraines. Studies indicate that it can reach up to 50% among patients with chronic migraine.19,20 The pathophysiology of MOH is thought to involve changes in pain modulation systems, particularly through altered regulation in the periaqueductal gray and hypothalamus, which are key in the body’s pain inhibition pathways.21 Repeated exposure to pain relief medications may reduce the effectiveness of endogenous pain control, increase pain sensitivity, and lower the pain threshold. The threshold for diagnosing MOH is specified in the International Classification of Headache Disorders (ICHD), which limits overuse to a maximum of 9 days per month for triptans, ergot derivatives, opioids, or combination analgesics, and 14 days per month for simple analgesics (eg NSAIDs, acetaminophen) in patients with a preexisting headache disorder.22 Neurochemical imbalances, including serotonin and dopamine dysregulation, further complicate the pain experience, making the brain more susceptible to pain signals and maintaining the cycle of CH.23
Combined Pathophysiological Insights
While these types of CH differ in underlying mechanisms, CH disorders often share features like central sensitization and altered pain modulation. These changes make the nervous system more reactive to both pain and non-painful stimuli. Structural brain changes, such as reduced gray matter in pain-processing regions, have also been observed in chronic migraine and MOH, suggesting CH may alter the brain structurally as well as functionally.24,25
Management of Headache Disorders
CH disorders, which include conditions like CM, CTTH, and MOH, pose significant challenges due to their complex pathophysiology and considerable impact on patients’ quality of life. Effective management strategies focus on detailed history and examination to elicit the presence of other headache type. Because MOH may complicate cluster headache, posttraumatic headache, idiopathic intracranial hypertension (IIH), and other secondary headaches, health care provider should not limit its assessment to migraine or tension-type headaches only.26 The management should focus on a multidisciplinary approach that combines pharmacological treatments, lifestyle modifications, and non-pharmacological interventions (Table 1). The pharmacological interventions for headache management depend on Preventive medications aim to reduce the frequency and severity of headaches and are particularly recommended for individuals with frequent or debilitating CH.3 Examples for preventive medications are beta blocker, anti-epileptic, Botulinum toxin A and Monoclonal antibodies that target calcitonin gene-related peptide which are used for CM while antidepressant can be used for both CM and CTTH. The preventive therapy is tailored to individual patient profiles, taking into consideration comorbidities, potential side effects, and patient preferences. Regular monitoring and adjustments in dosage are crucial for optimizing outcomes.27 On the other hands, Physicians commonly prescribe analgesics, such as nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, opioids, and triptans, for the acute attacks of CM disorders. These analgesics are frequently considered a first-line treatment option due to their effectiveness in providing immediate pain relief and accessibility for patients.28 However, these medication must be under judicial use as the practice of prescribing these medications, particularly for recurrent or CH patients, has raised concerns due to risks associated with MOH and other adverse outcomes.5
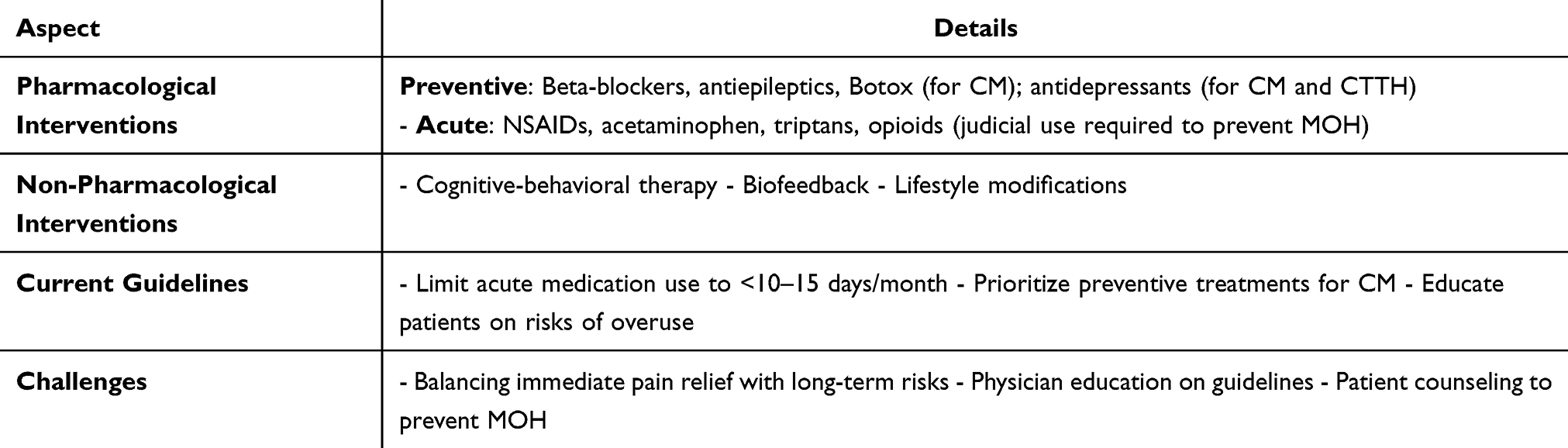 |
Table 1 Management of Chronic Headache Disorders |
Physician Practice and Management Challenges
The decision-making process for headache management involves balancing immediate pain relief with the long-term risks of medication overuse. Physicians face considerable challenges when prescribing for CH patients, as treatment plans need to be revised to avoid over-reliance on analgesics.29 Studies highlight that physician education on the appropriate use of analgesics and patient counseling on the risks of overuse are crucial for preventing MOH.30 There is an increasing emphasis on preventive treatment strategies, such as beta-blockers, antiepileptic drugs, and lifestyle modifications, which can help reduce the frequency of headaches without relying solely on acute pain relievers.31
Current Recommendations and Trends
Guidelines recommend limiting the use of acute headache medications to avoid medication-overuse, suggesting that acute analgesics should be prescribed judiciously with clear instructions to patients.29 The American Headache Society advises that preventive treatments be considered for patients with CM to minimize the risks associated with frequent analgesic use.32 Additionally, non-pharmacological approaches, such as cognitive-behavioral therapy and biofeedback, are increasingly recommended to reduce dependency on analgesics and enhance long-term headache management.33
Unfortunately, due to high prevalence of CH worldwide necessitates its recognition as a public health priority. Effective management strategies can alleviate individual suffering and reduce the societal burden of headache disorders. A review emphasizes that targeting CH is essential for achieving Sustainable Development Goal 3, highlighting the need for comprehensive healthcare approaches which aim to “Ensure healthy lives and promote well-being for all at all ages”.34
Prescribing Concerns and Risks of Medication Overuse
For acute headache episodes, physicians often prescribe NSAIDs and acetaminophen as they are effective, generally well-tolerated, and do not carry the addiction potential associated with opioids.28,35 However, a study showed 6.3% misuse the acetaminophen and exceed the daily dose which can lead to toxicity.36 Acetaminophen overuse was around 41.5%, while 90% of patients with CH use paracetamol.37,38 Triptans are frequently prescribed for migraines due to their specific mechanism of action on serotonin receptors, which can relieve migraine symptoms by constricting blood vessels and reducing inflammation in the brain.35 It accounts up to 30–40% of prescriptions in specialized headache clinics, as they are highly effective for acute migraine attacks. Additionally, opioids are still prescribed for headache management in approximately 10–20% of cases, particularly in emergency settings, despite their association with a high risk of dependency.39–41 However, with recurrent or CH, the line between therapeutic use and potential overuse becomes blurred, as frequent analgesic intake can lead to medication-overuse headache, characterized by a worsening of headache symptoms and dependency on the medication.23 Clinical evidence of followed patients with episodic migraine and observed that those who overused triptans were at a significantly higher risk of developing CM over a year.42
Unfortunately, the prescription of analgesics, particularly for CH patients, has been associated with increased risk for developing medication-overuse headache, especially when usage exceeds recommended limits (ie, more than 10–15 days per month for many analgesics).43 MOH can result from the frequent use of common analgesics, such as NSAIDs and acetaminophen, as well as triptans and opioids.44 Opioid prescription for headache management has come under scrutiny because, while they may provide temporary relief, opioids contribute to higher risks of dependency, addiction and have been shown to be less effective in the long-term management of CH compared to preventive therapies.45 The prescription of analgesics for headache management, while essential for acute pain relief, has raised concerns regarding malpractice, particularly in cases where inappropriate or excessive use leads to CH disorders.46,47 Studies have shown that overprescribing analgesics, particularly opioids, can inadvertently contribute to medication-overuse headache (MOH), thereby worsening the patient’s headache frequency and severity instead of providing lasting relief.5,48 Mismanagement in prescribing practices is often due to a lack of awareness or training among healthcare providers regarding the risks of MOH and the fine line between therapeutic use and overuse.30 Moreover, prescribing pain medication for none headache patient affect CH through the development of MOH.49
Malpractice in this area may involve failing to adhere to recommended guidelines for frequency and dosage of analgesics, as well as neglecting to explore alternative, preventive treatments for CH patients.15 Physicians may over-rely on analgesics, particularly opioids, as a quick fix without adequately educating patients on the risks of medication dependency and MOH. Studies indicate that up to 30% of CH patients experience worsening symptoms due to analgesic overuse, which is often preventable through better physician awareness and patient counseling.43 Furthermore, malpractice cases related to headache management are often linked to a failure to recognize headache patterns early on and to implement preventive therapies that reduce the need for frequent analgesic use.44 Consequently, malpractice related to analgesic prescriptions for headache contributes not only to the persistence of CH disorders but also to a cycle of dependency that complicates effective long-term management32 (Table 2).
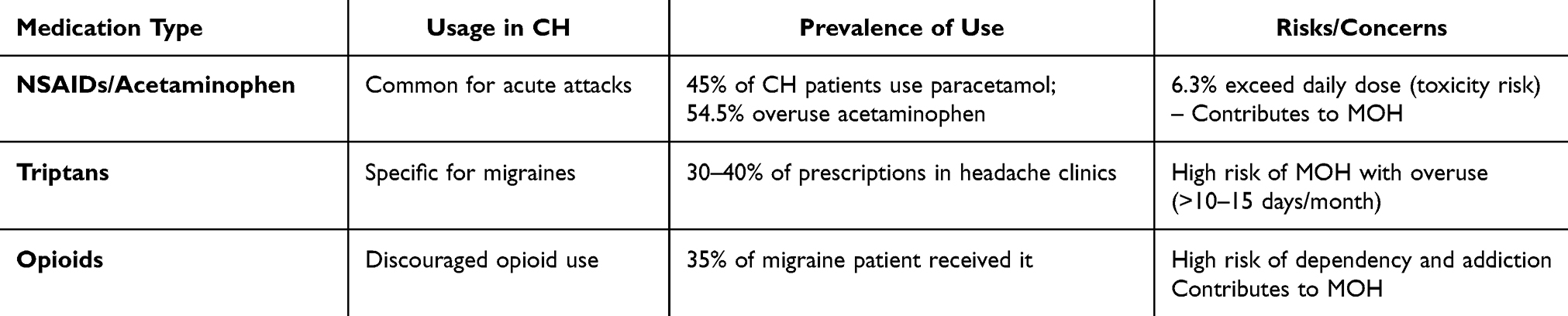 |
Table 2 Prevalence and Prescribing Patterns |
The Impacts of Malpractice of Over-Prescribing
The malpractice practice of overprescribing can have significant repercussions on patients, healthcare facilities, and the economy.50 These effects often arise due to the progression of chronic headache, which may develop from the prescription of analgesics for headache management or other types of pain.39,49
The Impacts on Patients
The malpractice of overprescribing analgesics for headache management can significantly impact patients, particularly those with medication-overuse headache (MOH). One of the primary consequences is the exacerbation of headache frequency and intensity, as the patient becomes trapped in a cycle of dependence on analgesics. This dependence leads to a “rebound” effect, where headaches worsen whenever the medication is not in the system, increasing both physical and psychological suffering.5
Over time, this cycle may lead to chronic daily headaches, which severely impact the patient’s quality of life. CH patients frequently experience reduced productivity, social withdrawal, and difficulties in managing daily responsibilities due to the constant pain and medication dependence.51 CH can have physical, psychological, and social effects on individual lives.52 Furthermore, prolonged overuse of analgesics can lead to adverse physical health outcomes, including gastrointestinal issues, liver toxicity, kidney impairment, fertility effect, and even increased cardiovascular disease risks.53,54
Malpractice in prescribing practices can also diminish trust in healthcare providers, as patients may feel they are not receiving effective long-term solutions but instead becoming dependent on medications that ultimately worsen their condition.55,56
Patients often feel frustrated and may experience psychological effects, including anxiety, depression, isolation and feelings of helplessness, due to the chronic nature of their pain and perceived lack of effective treatment options.51,57 Moreover, patients may be susceptible to stigma and labeling as having a certain headache type without a proper diagnosis.58
Furthermore, the overuse of symptomatic drugs in MOH patients might be related to psychological states such as fear and anticipatory anxiety of forthcoming headache attacks. This anxiety can exacerbate the frequency and severity of headaches, creating a vicious cycle that is challenging to break.59 In addition, reduce productivity, work loss, and reduce income are common findings among migraine population.60,61 Mismanagement also reduces patients’ willingness to seek further medical help, potentially delaying more effective treatments and exacerbating the disorder’s impact on mental and physical well-being.30,52
Impacts of Malpractice on Health Care Facilities, Health Care Providers and Costs
The malpractice of overprescribing analgesics for headache management in medication-overuse headache (MOH) patients not only affects the individuals themselves but also creates significant burdens on healthcare facilities, doctors, and healthcare costs. Healthcare facilities often face increased patient load due to frequent visits from MOH patients seeking relief from chronic pain that worsens due to medication overuse. These patients frequently return to healthcare facilities with recurring headache symptoms, requiring additional consultations, tests, and sometimes emergency care, which puts a strain on healthcare resources.30,62 Repeated visits for a chronic, preventable condition like MOH occupy time and resources that could otherwise be directed toward other critical cases.63
For doctors, the consequences of such malpractice can lead to reputational damage and legal repercussions. Healthcare providers who do not adhere to guidelines for appropriate analgesic prescription for headache management may face professional consequences, as malpractice claims related to chronic pain management and opioid prescriptions have increased in recent years.64 Furthermore, the need to manage patients suffering from the long-term effects of medication overuse can lead to frustration and burnout among healthcare providers, as the cycle of prescribing and dependence can feel counterproductive, ultimately impacting the physician’s professional morale and job satisfaction.5
From a cost perspective, overprescription of analgesics in MOH patients leads to substantial economic implications. The repeated healthcare utilization from frequent patient visits, hospitalizations, and diagnostic procedures contributes significantly to healthcare costs. Studies show that managing CH conditions like MOH is associated with high direct and indirect costs, driven by both the need for long-term care and lost productivity from patients unable to maintain regular employment due to their condition.65 Additionally, overuse of prescription medications, particularly opioids and other costly analgesics, raises pharmaceutical expenses for both healthcare providers and insurance systems, which further escalating overall healthcare costs66 (Table 3).
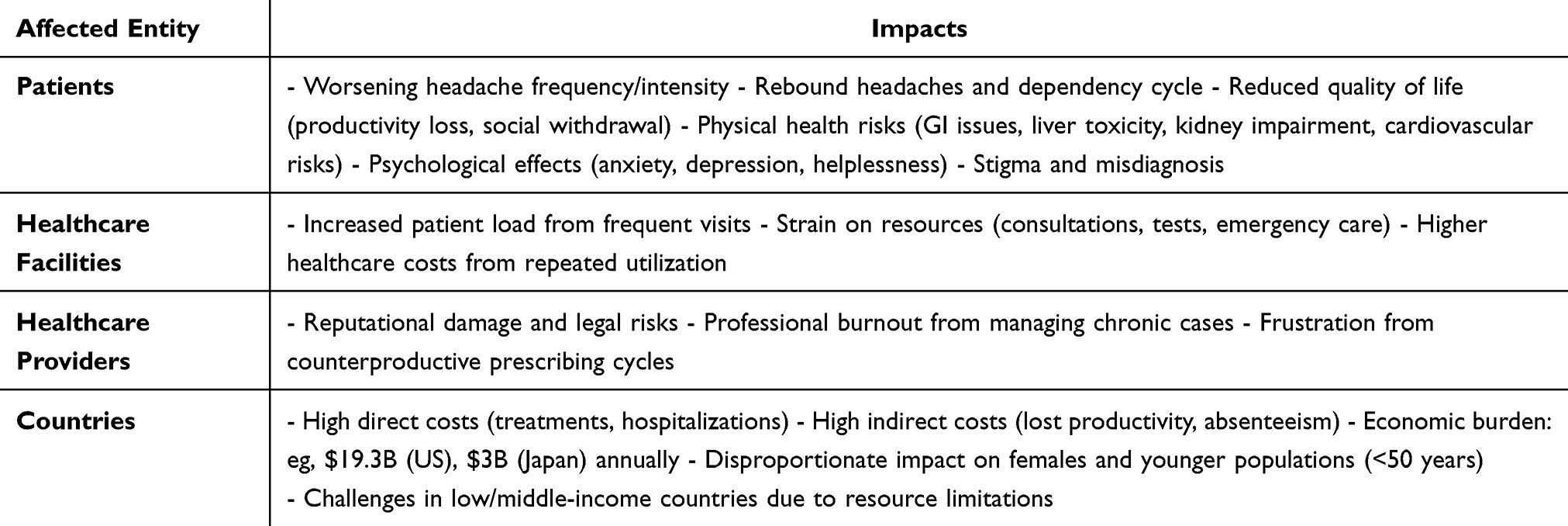 |
Table 3 Impacts of Overprescription and MOH |
Impacts on Countries and Economic Burdens
CH represents a significant burden that transcends individual suffering, affecting economic productivity, public health systems, and societal well-being. They significantly affect individuals and societies worldwide, posing a major public health challenge. According to the Global Burden of Disease (GBD) 2019 study, migraines alone impacted over 500 millions people globally, representing a 16% substantial increase from 1990.67 These conditions account for a significant proportion of years lived with disability (YLDs), with migraines contributing to over 91% of headache-related disability. The burden is disproportionately higher among females, who are more likely to experience severe and chronic forms of headaches. This widespread prevalence makes CH a critical issue for healthcare systems worldwide.68
Economically, the impact of CH is profound. Healthcare systems face high direct costs from treatments, medications, and hospitalizations. For instance, countries in the Organization for Economic Co-operation and Development (OECD) report significant expenditure on headache management. However, the indirect costs, such as lost productivity due to absenteeism or decreased work efficiency, often exceed the direct costs. These indirect effects ripple across national economies, lowering overall workforce output and increasing the financial strain on families and businesses. Intangible costs, such as the emotional toll and social isolation experienced by sufferers, further exacerbate the economic burden.65
CH disorders, particularly migraines, significantly impact employment, especially affect young population less than 50s.69 It leads to increased absenteeism and reduced productivity, leading to substantial economic burdens on both individuals and society. Individuals suffering from CH often experience frequent and severe symptoms that necessitate taking time off work. A study focusing on the US workforce estimated that migraine-related absenteeism and reduced on-the-job productivity could cost large corporations between $21.5 million and $24.4 million annually.70 Furthermore, research indicates that those with CH report an average of 9.7 lost workdays over a three-month period due to headache-related issues.60,71
The financial implications extend beyond individual employers to the broader economy. In the United States, the total indirect costs associated with migraine, including lost productivity, are estimated at $19.3 billion.72 In Japan, migraines are estimated to cost the economy approximately $3 billion annually in lost productivity.73
Globally, the burden of CH is not limited to high-income nations. Low- and middle-income countries like India and China face growing challenges in addressing headache-related disabilities due to limited healthcare resources and awareness. These nations report high prevalence rates of migraines and tension-type headaches, further straining already overburdened healthcare systems. Addressing this global challenge requires tailored solutions that account for regional healthcare disparities, cultural factors, and resource availability.74 CH can also lead to long-term employment challenges. Studies have found that individuals with CH are more likely to be on long-term sick leave, with 33% reporting absences exceeding one year. 60
Additionally, those with chronic migraines may lose about 14% of their annual productivity at work, and 20% report becoming occupationally disabled, unable to perform tasks required by their jobs75 (Table 4).
 |
Table 4 Economic and Societal Burden |
Recommendation
Regular monitoring and follow-up with patients using analgesics can help identify early signs of overuse and allow timely intervention.53 Incorporating artificial intelligence (AI) tools into clinical practice offers a promising solution. AI can assist in patient risk assessment by analyzing patterns in medication use, flagging potential overuse, and suggesting personalized treatment adjustments.76 AI-powered decision-support systems can also guide physicians in adhering to evidence-based protocols and identifying alternative therapies.77
AI can play a role in the diagnosis of chronic headache type and establishment of the preventive therapy for each type can reduce the risk of MOH and improve the outcomes.78 Non-pharmacological treatments, including cognitive-behavioral therapy, relaxation techniques, and lifestyle modifications, should be emphasized as adjuncts or alternatives to medication.79
Additionally, restricting the availability of combination analgesics and opioids, along with implementing policies to promote safer prescribing, can mitigate the risks of MOH. Collaborative care models involving headache specialists, primary care physicians, pharmacists, and AI systems have shown promise in reducing overprescription and improving patient outcomes.80
Conclusion
Overprescription is a prevalent issue among healthcare providers, with repetitive practices contributing to a rise in medication overuse headaches (MOH). This condition leads to a range of physical, psychological, and social challenges for patients, including worsening CH, dependency cycles, and a diminished quality of life, often exacerbated by health complications related to prolonged medication use. MOH also places a significant economic burden on healthcare systems, as recurrent patient visits and treatments for this preventable condition strain resources and increase individual expenditures.
Healthcare providers face additional challenges, including the risk of legal consequences and professional burnout, as they manage chronic pain patients caught in cycles of medication overuse. Economically, MOH generates substantial direct and indirect costs, including ongoing treatments, reduced productivity, and escalating pharmaceutical expenses, impacting both individual practitioners and the broader healthcare system.
Effectively addressing this issue requires strict adherence to established prescribing guidelines, a focus on preventive treatment strategies, and improved provider education. AI could become an essential asset in these measures for curbing overprescription practices, enhancing patient outcomes, and alleviating the broader healthcare and economic burden of MOH.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Olesen J. Headache classification committee of the International Headache Society (IHS) the international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
2. Steiner TJ, Jensen R, Katsarava Z, et al. Aids to management of headache disorders in primary care (2nd edition): on behalf of the European headache federation and lifting the burden: the global campaign against headache. J Headache Pain. 2019;20(1):1–52. doi:10.1186/S10194-018-0899-2/TABLES/20
3. Chronic daily headache: diagnosis and management - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/24784123/.
4. Stewart WF, Wood C, Reed ML, Roy J, Lipton RB. Cumulative lifetime migraine incidence in women and men. Cephalalgia. 2008;28(11):1170–1178. doi:10.1111/J.1468-2982.2008.01666.X/ASSET/IMAGES/LARGE/10.1111_J.1468-2982.2008.01666.X-FIG4.JPEG
5. Kristoffersen ES, Lundqvist C. Medication-overuse headache: epidemiology, diagnosis and treatment. Ther Adv Drug Saf. 2014;5(2):87–99. doi:10.1177/2042098614522683
6. Mungoven TJ, Henderson LA, Meylakh N. Chronic migraine pathophysiology and treatment: a review of current perspectives. Front Pain Res. 2021;2:705276. doi:10.3389/FPAIN.2021.705276
7. Robbins MS, Burch R. Preventive migraine treatment. Continuum. 2021;27(3):613–632. doi:10.1212/CON.0000000000000957
8. Weatherall MW. The diagnosis and treatment of chronic migraine. Ther Adv Chronic Dis. 2015;6(3):115. doi:10.1177/2040622315579627
9. Burch RC, Buse DC, Lipton RB. Migraine: epidemiology, burden, and comorbidity. Neurol Clin. 2019;37(4):631–649. doi:10.1016/J.NCL.2019.06.001
10. Burstein R, Noseda R, Borsook D. Migraine: multiple processes, complex pathophysiology. J Neurosci. 2015;35(17):6619–6629. doi:10.1523/JNEUROSCI.0373-15.2015
11. Schwedt TJ, Schlaggar BL, Mar S, et al. Atypical resting-state functional connectivity of affective pain regions in chronic migraine. Headache. 2013;53(5):737–751. doi:10.1111/HEAD.12081
12. Yeh PK, An YC, Hung KS, Yang FC. Influences of genetic and environmental factors on chronic migraine: a narrative review. Curr Pain Headache Rep. 2024;28(4):169–180. doi:10.1007/S11916-024-01228-4
13. Ghadiri-Sani M, Silver N. Headache (chronic tension-type). BMJ Clin Evid. 2016;2016:1205.
14. Bendtsen L, Jensen R. Tension-type headache. Neurol Clin. 2009;27(2):525–535. doi:10.1016/J.NCL.2008.11.010
15. Yu S, Han X. Update of chronic tension-type headache. Curr Pain Headache Rep. 2014;19(1):1–8. doi:10.1007/S11916-014-0469-5/METRICS
16. Repiso-Guardeño Á, Moreno-Morales N, Labajos-Manzanares MT, Rodríguez-Martínez MC, Armenta-Peinado JA. Does tension headache have a central or peripheral origin? Current state of affairs. Curr Pain Headache Rep. 2023;27(11):801–810. doi:10.1007/S11916-023-01179-2/METRICS
17. Ashina S, Bendtsen L, Ashina M. Pathophysiology of migraine and tension-type headache. Tech Reg Anesth Pain Manag. 2012;16(1):14–18. doi:10.1053/J.TRAP.2012.11.002
18. Katsuki M, Yamagishi C, Matsumori Y, et al. Questionnaire-based survey on the prevalence of medication-overuse headache in Japanese one city—Itoigawa study. Neurol Sci. 2022;43(6):3811–3822. doi:10.1007/S10072-021-05831-W/TABLES/4
19. Krymchantowski A, Jevoux C, Krymchantowski AG, Ramos LB, Barbosa JSS, Silva-Neto RP. Medication-overuse headache—a review of different treatment strategies. Front Pain Res. 2023;4:1103497. doi:10.3389/FPAIN.2023.1103497/BIBTEX
20. Gosalia H, Moreno-Ajona D, Goadsby PJ. Medication-overuse headache: a narrative review. J Headache Pain. 2024;25(1):1–9. doi:10.1186/S10194-024-01755-W/FIGURES/1
21. May A, Burstein R. Hypothalamic regulation of headache and migraine. Cephalalgia. 2019;39(13):1710. doi:10.1177/0333102419867280
22. 8.2 Medication-overuse headache (MOH) - ICHD-3. Available from: https://ichd-3.org/8-headache-attributed-to-a-substance-or-its-withdrawal/8-2-medication-overuse-headache-moh/?utm_source=chatgpt.com.
23. Andreou AP, Edvinsson L. Mechanisms of migraine as a chronic evolutive condition. J Headache Pain. 2019;20(1):1–17. doi:10.1186/S10194-019-1066-0
24. Chen W, Li H, Hou X, Jia X. Gray matter alteration in medication overuse headache: a coordinates-based activation likelihood estimation meta-analysis. Brain Imaging Behav. 2022;16(5):2307–2319. doi:10.1007/S11682-022-00634-9/FIGURES/4
25. Chong CD, Schwedt TJ, Hougaard A. Brain functional connectivity in headache disorders: a narrative review of MRI investigations. J Cereb Blood Flow Metab. 2017;39(4):650. doi:10.1177/0271678X17740794
26. Ashina S, Terwindt GM, Steiner TJ, et al. Medication overuse headache. Nature Reviews Disease Primers. 2023;9(1):1–20. doi:10.1038/s41572-022-00415-0
27. Murphy C, Hameed S. Chronic headaches. StatPearls. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559083/.
28. Robbins MS. Diagnosis and management of headache: a review. JAMA. 2021;325(18):1874–1885. doi:10.1001/JAMA.2021.1640
29. Ford B, Dore M, Harris E. Outpatient primary care management of headaches: guidelines from the VA/DoD. Am Fam Physician. 2021;104(2):316–320.
30. Bigal ME, Serrano D, Reed M, Lipton RB. Chronic migraine in the population: burden, diagnosis, and satisfaction with treatment. Neurology. 2008;71(8):559–566. doi:10.1212/01.WNL.0000323925.29520.E7
31. Dodick DW. Pearls: headache. Semin Neurol. 2010;30(1):74–81. doi:10.1055/S-0029-1245000
32. American Headache Society. The American Headache Society Position Statement On Integrating New Migraine Treatments Into Clinical Practice. Headache. 2019;59(1):1–18. doi:10.1111/HEAD.13456
33. Buse DC, Reed ML, Fanning KM, Bostic RC, Lipton RB. Demographics, headache features, and comorbidity profiles in relation to headache frequency in people with migraine: results of the American Migraine Prevalence and Prevention (AMPP) study. Headache. 2020;60(10):2340–2356. doi:10.1111/HEAD.13966
34. Martelletti P, Leonardi M, Ashina M, et al. Rethinking headache as a global public health case model for reaching the SDG 3 HEALTH by 2030. J Headache Pain. 2023;24(1):1–17. doi:10.1186/S10194-023-01666-2/TABLES/1
35. Kelley NE, Tepper DE. Rescue therapy for acute migraine, part 1: triptans, dihydroergotamine, and magnesium. Headache. 2012;52(1):114–128. doi:10.1111/J.1526-4610.2011.02062.X
36. Shiffman S, Battista DR, Kelly JP, Malone MK, Weinstein RB, Kaufman DW. Prevalence of exceeding maximum daily dose of paracetamol, and seasonal variations in cold-flu season. Br J Clin Pharmacol. 2018;84(6):1250–1257. doi:10.1111/BCP.13551
37. Westergaard ML, Lau CJ, Allesøe K, Gjendal ST, Jensen RH. Monitoring chronic headache and medication-overuse headache prevalence in Denmark. 2020;40(1):6–18. doi:10.1177/0333102419876909
38. Fahmi Issa L, Mohammmed W, Qurashi A, et al. Awareness of paracetamol overuse headache among Saudi’s population in Taif city, Saudi Arabia. doi:10.54905/disssi/v26i130/ms551e2610
39. Bigal ME, Lipton RB. Excessive acute migraine medication use and migraine progression. Neurology. 2008;71(22):1821–1828. doi:10.1212/01.WNL.0000335946.53860.1D
40. Evers S, Jensen R. Treatment of medication overuse headache--guideline of the EFNS headache panel. Eur J Neurol. 2011;18(9):1115–1121. doi:10.1111/J.1468-1331.2011.03497.X
41. Diener HC, Holle D, Solbach K, Gaul C. Medication-overuse headache: risk factors, pathophysiology and management. Nat Rev Neurol. 2016;12(10):575–583. doi:10.1038/NRNEUROL.2016.124
42. Schwedt TJ, Buse DC, Argoff CE, et al. Medication overuse and headache burden: results from the CaMEO study. Neurol Clin Pract. 2021;11(3):216–226. doi:10.1212/CPJ.0000000000001037/ASSET/D9003757-43B7-4BAF-82B4-1FDD1A046B29/ASSETS/GRAPHIC/6TTU1.JPEG
43. Fischer MA, Jan A. Medication-overuse headache. StatPearls. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538150/.
44. Silberstein SD, Lipton RB, Solomon S, Mathew NT. Classification of daily and near-daily headaches: proposed revisions to the IHS criteria. Headache. 1994;34(1):1–7. doi:10.1111/J.1526-4610.1994.HED3401001.X
45. Diener HC, Dodick D, Evers S, et al. Pathophysiology, prevention, and treatment of medication overuse headache. Lancet Neurol. 2019;18(9):891–902. doi:10.1016/S1474-4422(19)30146-2/ATTACHMENT/B9530A5C-7BD9-4C7A-A9CB-44FCE166091B/MMC1.PDF
46. Fernández-De-Las-Peñas C, Palacios-Ceña M, Castaldo M, et al. Variables associated with use of symptomatic medication during a headache attack in individuals with tension-type headache: a European study. BMC Neurol. 2020;20(1):1–10. doi:10.1186/S12883-020-1624-8/TABLES/6
47. Pero A, Pace A, Dhamoon MS. Triptan medication use among patients with migraine with contraindications in the US. Headache. 2022;62(7):883–889. doi:10.1111/HEAD.14327
48. Shao Q, Rascati KL, Lawson KA, Barner JC, Sonawane KB, Rousseau JF. Real-world opioid use among patients with migraine enrolled in US commercial insurance and risk factors associated with migraine progression. J Manag Care Spec Pharm. 2022;28(11):1272–1281. doi:10.18553/JMCP.2022.28.11.1272/ASSET/IMAGES/FIG1B.JPG
49. Westergaard ML, Hansen EH, Glümer C, Jensen RH. Prescription pain medications and chronic headache in Denmark: implications for preventing medication overuse. Eur J Clin Pharmacol. 2015;71(7):851–860. doi:10.1007/S00228-015-1858-3
50. Stovner LJ, Nichols E, Steiner TJ, et al. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2018;17(11):954. doi:10.1016/S1474-4422(18)30322-3
51. Abu Bakar N, Tanprawate S, Lambru G, Torkamani M, Jahanshahi M, Matharu MS. Quality of life in primary headache disorders: a review. Cephalalgia. 2016;36(1):67–91. doi:10.1177/0333102415580099/ASSET/IMAGES/LARGE/10.1177_0333102415580099-FIG2.JPEG
52. Nichols VP, Ellard DR, Griffiths FE, Kamal A, Underwood M, Taylor SJC. The lived experience of chronic headache: a systematic review and synthesis of the qualitative literature. BMJ Open. 2017;7(12):e019929. doi:10.1136/BMJOPEN-2017-019929
53. Milani DAQ, Davis DD. Pain management medications. StatPearls. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560692/..
54. Kristensen DM, Mazaud-Guittot S, Gaudriault P, et al. Analgesic use - prevalence, biomonitoring and endocrine and reproductive effects. Nat Rev Endocrinol. 2016;12(7):381–393. doi:10.1038/NRENDO.2016.55
55. Palos GR, Mendoza TR, Cantor SB, Aday LA, Cleeland CS. Perceptions of analgesic use and side effects: what the public values in pain management. J Pain Symptom Manage. 2004;28(5):460–473. doi:10.1016/J.JPAINSYMMAN.2004.02.016
56. Raja MAG, Al-Shammari SS, Al-Otaibi N, Amjad MW. Public attitude and perception about analgesic and their side effects. Available from: http://imsear.searo.who.int/handle/123456789/215900.
57. Buse DC, Fanning KM, Reed ML, et al. Life with migraine: effects on relationships, career, and finances from the chronic migraine epidemiology and outcomes (CaMEO) study. Headache. 2019;59(8):1286. doi:10.1111/HEAD.13613
58. Tana C, Raffaelli B, Souza MNP, et al. Health equity, care access and quality in headache – part 1. J Headache Pain. 2024;25(1):1–12. doi:10.1186/S10194-024-01712-7
59. Romozzi M, Di Tella S, Rollo E, et al. Theory of mind in migraine and medication-overuse headache: a cross-sectional study. Front Neurol. 2022;13:968111. doi:10.3389/FNEUR.2022.968111
60. Kristoffersen ES, Stavem K, Lundqvist C, Russell MB. Impact of chronic headache on workdays, unemployment and disutility in the general population. J Epidemiol Community Health. 2019;73(4):360–367. doi:10.1136/JECH-2018-211127
61. Shimizu T, Sakai F, Miyake H, et al. Disability, quality of life, productivity impairment and employer costs of migraine in the workplace. J Headache Pain. 2021;22(1):1–11. doi:10.1186/S10194-021-01243-5/FIGURES/2
62. Shao Q, Rascati KL, Barner JC, Lawson KA, Sonawane KB, Rousseau JF. Healthcare utilization and costs among patients with chronic migraine, episodic migraine, and tension-type headache enrolled in commercial insurance plans. Headache. 2022;62(2):141–158. doi:10.1111/HEAD.14247
63. Bonafede M, Cai Q, Cappell K, et al. Factors associated with direct health care costs among patients with Migraine. J Manag Care Spec Pharm. 2017;23(11):1169–1176. doi:10.18553/JMCP.2017.23.11.1169/ASSET/IMAGES/LARGE/1169FIG1.JPEG
64. Fitzgibbon DR, Rathmell JP, Michna E, Stephens LS, Posner KL, Domino KB. Malpractice claims associated with medication management for chronic pain. Anesthesiology. 2010;112(4):948–956. doi:10.1097/ALN.0B013E3181CDEF98
65. Eltrafi A, Shrestha S, Ahmed A, Mistry H, Paudyal V, Khanal S. Economic burden of chronic migraine in OECD countries: a systematic review. Health Econ Rev. 2023;13(1):1–10. doi:10.1186/S13561-023-00459-2/TABLES/2
66. Munakata J, Hazard E, Serrano D, et al. Economic burden of transformed migraine: results from the American migraine prevalence and prevention (AMPP) study. Headache. 2009;49(4):498–508. doi:10.1111/J.1526-4610.2009.01369.X
67. Li XY, Yang CH, Lv JJ, et al. Global, regional, and national epidemiology of migraine and tension-type headache in youths and young adults aged 15-39 years from 1990 to 2019: findings from the global burden of disease study 2019. J Headache Pain. 2023;24(1). doi:10.1186/S10194-023-01659-1
68. Amiri P, Kazeminasab S, Nejadghaderi SA, et al. Migraine: a review on its history, global epidemiology, risk factors, and comorbidities. Front Neurol. 2022;12:800605. doi:10.3389/FNEUR.2021.800605
69. Meng W, Sui L. Headache disorders: a persistent public health challenge for the under 50s. Front Neurol. 2024;15:1501749. doi:10.3389/FNEUR.2024.1501749/BIBTEX
70. Burton WN, Conti DJ, Chen CY, Schultz AB, Edington DW. The economic burden of lost productivity due to migraine headache: a specific worksite analysis. J Occup Environ Med. 2002;44(6):523–529. doi:10.1097/00043764-200206000-00013
71. Wong LP, Alias H, Bhoo-Pathy N, et al. Impact of migraine on workplace productivity and monetary loss: a study of employees in banking sector in Malaysia. J Headache Pain. 2020;21(1). doi:10.1186/s10194-020-01144-z
72. Yucel A, Thach A, Kumar S, et al. Estimating the economic burden of migraine on US employers. Am J Manag Care. 2020;26(12):E403–E408. doi:10.37765/AJMC.2020.88547
73. A closer look at the cost of migraine – global patient Advocacy coalition. Available from: https://gpacmigraine.org/a-closer-look-at-the-cost-of-migraine/?utm_source=chatgpt.com.
74. Zhang YJ, Li XY, Guo ZL. Temporal trends of migraine and tension-type headache burden across the BRICS: implications from the Global Burden of Disease study 2019. Front Neurol. 2023;14:1307413. doi:10.3389/FNEUR.2023.1307413/BIBTEX
75. Riggins N, Paris L. Legal aspects of migraine in the workplace. Curr Pain Headache Rep. 2022;26(12):863. doi:10.1007/S11916-022-01095-X
76. Alsanosi SM, Padmanabhan S. Potential applications of artificial intelligence (AI) in managing polypharmacy in Saudi Arabia: a narrative review. 2024. doi:10.3390/healthcare12070788
77. Antel R, Whitelaw S, Gore G, Ingelmo P. Moving towards the use of artificial intelligence in pain management. Eur. J. Pain. 2024;00:1–22. doi:10.1002/EJP.4748
78. Petrušić I, Chiang CC, Garcia-Azorin D, et al. Influence of next-generation artificial intelligence on headache research, diagnosis and treatment: the junior editorial board members’ vision – part 2. J Headache Pain. 2025;26(1):2. doi:10.1186/S10194-024-01944-7
79. Licina E, Radojicic A, Jeremic M, Tomic A, Mijajlovic M. Non-pharmacological treatment of primary headaches—a focused review. Brain Sci. 2023;13(10):1432. doi:10.3390/BRAINSCI13101432
80. Petrušić I, Ha WS, Labastida-Ramirez A, et al. Influence of next-generation artificial intelligence on headache research, diagnosis and treatment: the junior editorial board members’ vision – part 1. J Headache Pain. 2024;25(1):1–12. doi:10.1186/S10194-024-01847-7
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.