Back to Journals » Clinical Ophthalmology » Volume 19
Ocular Manifestations of Perinatal HIV Infection in Kenyan Children on HAART: A Cross-Sectional Comparative Study
Authors Alisi L ![]() , Armentano M, Visioli G
, Armentano M, Visioli G ![]() , Mingaine MS
, Mingaine MS ![]() , Albanese GM
, Albanese GM ![]() , Lucchino L
, Lucchino L ![]() , Bruscolini A
, Bruscolini A
Received 25 March 2025
Accepted for publication 4 July 2025
Published 8 July 2025 Volume 2025:19 Pages 2143—2151
DOI https://doi.org/10.2147/OPTH.S530332
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ludovico Alisi,1,2,* Marta Armentano,1,2,* Giacomo Visioli,1 Mpekethu Sam Mingaine,3 Giuseppe Maria Albanese,1 Luca Lucchino,1 Alice Bruscolini1
1Department of Sense Organs, Sapienza University of Rome, Rome, Italy; 2AINA Children’s Home, Meru Town, Kenya; 3Eye Clinic, Meru Teaching and Referral Hospital, Meru Town, Kenya
*These authors contributed equally to this work
Correspondence: Giacomo Visioli, Department of Sense Organs, Sapienza University of Rome, Viale del Policlinico 155, Rome, 00161, Italy, Email [email protected]
Introduction: Human Immunodeficiency Virus (HIV) remains a global health concern, particularly in Africa. Highly Active Antiretroviral Therapy (HAART) has transformed HIV into a manageable chronic condition, but potential side effects, including ocular manifestations, are recognized. While ophthalmic complications in the pre-HAART era are well-documented, the current landscape in perinatally acquired HIV requires further investigation. This study aims to report the prevalence of ocular involvement in a cohort of children with perinatally acquired HIV.
Methods: This cross-sectional study recruited 73 HIV-positive and 59 HIV-negative age-matched children in Kenya. All HIV+ children were on HAART. Comprehensive ophthalmological examinations included visual acuity, stereopsis, ocular motility assessment, tear film tests (BUT, Schirmer, Oxford staining), corneal esthesiometry, and an ocular allergy questionnaire. Clinical data on HIV parameters and HAART regimens were collected for the HIV+ group.
Results: Visual acuity was comparable between groups. Both groups’ ocular surface parameters (BUT, Schirmer, Oxford score) were within normal limits. Ocular allergy prevalence was similar, but HIV+ children reported fewer symptoms (p=0.030). Strabismus was significantly more frequent in the HIV+ group (24.7% vs 8.5%, p=0.015), particularly in patients in treatment with abacavir (p=0.026). No significant correlation was found between HIV-related parameters and ocular surface findings.
Conclusion: This study suggests that in the HAART era, perinatally HIV-infected children with well-managed viral loads show visual function and largely normal ocular surface health, contrasting with pre-HAART literature. The increased frequency of strabismus in HIV+ children and its potential association with abacavir warrant further investigation into HAART-related ocular motility side effects.
Keywords: HIV, ocular motility, HAART, ocular surface, keratoconjunctivitis sicca, ocular allergy
Introduction
Human immunodeficiency virus (HIV) is currently a global health burden. Around 39.9 million people live with HIV as of 2023, more than 65% of them in African countries. HIV has become a manageable chronic disease in the era of highly active antiretroviral therapy (HAART).1 Nowadays, patients undergoing continuous therapy can maintain a normal CD4 count and substantially live free from complications directly related to the viral infection. However, it has been recognized that several drugs encompassed in HAART protocols can have detrimental effects on the cardiovascular system as well as a reduction in bone density and renal function.2
Ophthalmic manifestations are a significant concern in HIV-infected individuals, encompassing a spectrum of conditions from common issues like keratoconjunctivitis sicca (KCS) to sight-threatening diseases. These pathologies are related to the acquired immune deficiency syndrome (AIDS) condition and include cytomegalovirus (CMV) retinitis, acute retinal necrosis (ARN), progressive outer retinal necrosis (PORN), HIV-related ischaemic microvasculopathy, ocular syphilis, tuberculosis, cryptococcal meningitis, alongside other infectious, immune, and neoplastic conditions. Notably, the presentation of these manifestations can vary between adults and children and geographically.3 Several studies report that the cumulative risk of blindness is between 5 and 25%. In children with perinatally acquired HIV, ocular manifestations remain an important clinical issue. KCS is reported as one of the more common manifestations, involving up to 30% of children.4 Other ocular complications in this population include retinal microvasculopathy and infections, although data remain limited and partially outdated. Despite these consistent numbers, most of the available literature refers to the pre-ART era, and therefore, it may be considerably overstated in the current global scenario.5
Moreover, several antiretroviral drugs are emerging as potential causative agents for ocular disorders. Didanosine has been linked to retinal toxicity, while tenofovir and lamivudine/abacavir have been associated with the development of chronic progressive external ophthalmoplegia.6,7
The purpose of the current study is to report the occurrence of potential ocular surface, motility, or retinal diseases in the eyes of a selected cohort of children with perinatally acquired HIV. Moreover, we looked into the potential effects of HAART therapy on ocular structures and function. The results were compared to a cohort of HIV-negative children.
Materials and Methods
Between December 2024 and January 2025, we conducted a cross-sectional study in a children’s home located in Meru County, Kenya. We recruited a cohort of consecutive HIV-positive (HIV+) pediatric patients. All the children had congenital or perinatal HIV confirmed by laboratory test, acquired from their mothers during childbirth or breastfeeding. A control group of HIV-negative (HIV-) age-matched subjects were randomly recruited from the local school. The study was approved by the internal ethical committee of AINA Children’s Home. All legal representatives of the patients signed an informed consent; the study followed the tenets of the Declaration of Helsinki.
All the patients underwent a comprehensive ophthalmological evaluation, comprising best corrected visual acuity (BCVA) measurement with a 6-meter Snellen chart, stereopsis assessment with Lang II test, ocular motility examination, and cover test. The anterior segment and posterior fundus examination were performed under mydriasis. The Oxford grading8 was calculated following Lissamine green staining, and the tear film break-up time (BUT) was measured after fluorescein drop instillation. Schirmer test type I was performed with calibrated strips. Corneal esthesiometry was performed using the Cochet-Bonnet esthesiometer. Values obtained were averaged between the two eyes.
Additionally, a questionnaire on ocular allergy (OA) signs and symptoms was proposed for all the children.9 The questionnaire included five items for symptoms (score range 0–15) and seven items for signs (0–21), determined after the slit lamp evaluation. If the children were unable to respond about their symptoms, we asked the parents for the HIV- group and the house parents for the HIV+ group to answer on their behalf, based on the behaviors they observed. The house-parents are staff members who work in the children’s home and take on the role of parents. To reduce the proxy symptoms reporting bias, parents and house-parents were specifically instructed to report based on observable behaviors rather than subjective interpretations of the child’s feelings. This approach aimed to standardize the reporting framework as much as possible.
Moreover, clinical data on the time of HAART therapy, types of drugs included in HAART, prophylactic therapy, concomitant or previous tubercular infection, viral load (calculated as the average of the last 18 months), AIDS stage at diagnosis according to the WHO clinical staging system were collected, for the HIV+ group.10
Statistical analysis was conducted with JASP software (ver 0.19.3).11 Continuous variables, reported as mean ± SD, were tested for normality using the Shapiro–Wilk test. Parametric comparisons used the unpaired t-test, while non-parametric comparisons used the Mann–Whitney test. Pearson or Spearman’s rank correlation was used for bivariate correlations, as appropriate. Categorical variables, reported as counts and percentages, were analyzed using the Chi-square test or Fisher’s exact test with Freeman-Halton extension when appropriate. A p-value <0.05 was considered the threshold for significance.
Results
Clinical Data
We recruited a total of 132 pediatric patients, divided into 59 HIV- and 73 HIV+. The HIV+ group had a mean age of 11.64 ± 4.13, whereas the HIV- group presented a mean age of 11.42±3.48. The female percentage was 54.8% (n=49) in the HIV+ group and 67.8% (n=40) in the HIV- group. The HIV+ children have been on HAART for a mean time of 112.96± 40.19 months. The mean BCVA was comparable in the two groups, being 0.01±0.04 LogMar. The clinical characteristics of the recruited patients are reported in Table 1, no significant differences were observed in the demographic data between the two groups. Notably, none of the included patients had chronic systemic or genetic conditions that could have influenced the ocular examination. Further data regarding the HIV+ subgroup were collected. The viral load was undetectable in 65 children (89.0%), detectable (> 40 copies/mL) in 7 patients (9.6%), and unknown in 1 patient (1.4%). This last child was admitted to the children’s home the previous week and data about her viral load was not available yet. No patient presented a viral load superior to 173 copies/mL. The HAART therapy schemes and prophylactic systemic treatments are summarized in Table 2.
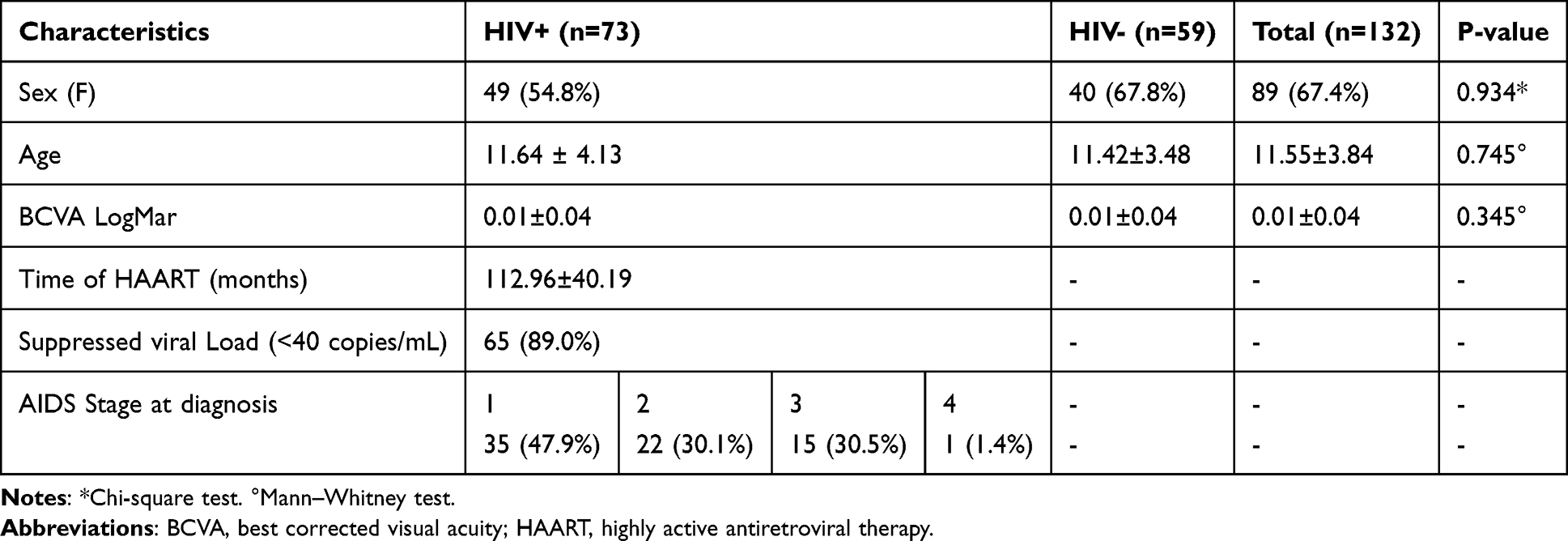 |
Table 1 Description of the Demographic and Clinical Characteristics of the Studied Population |
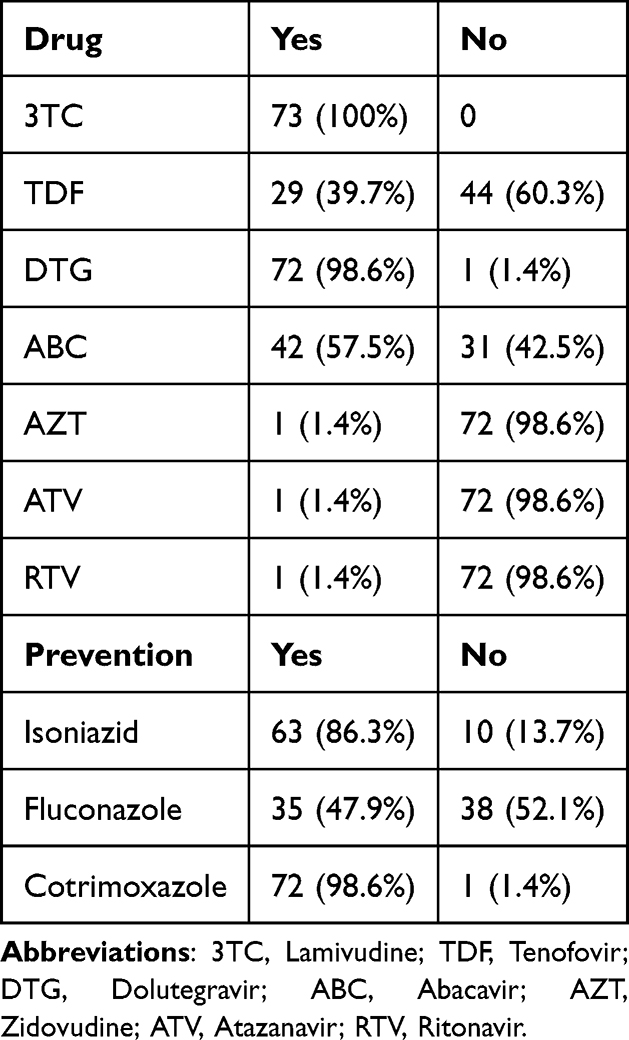 |
Table 2 Therapeutic and Prophylactic Schemes Followed by the HIV+ Patients |
Ocular Motility
The stereopsis was found to be complete in 72 (98.6%) of the HIV+ and 57 (96.6%) of the HIV- (p=0.439). Significant differences between the two groups in terms of ocular motility were identified; in the HIV+ group, 18 (24.6%) patients showed altered motility, while only 5 (8.4%) patients in the HIV- group (p=0.015). More in-depth variable degrees of exophoria were observed, in particular in 15 HIV+ subjects (20.5%) and 4 HIV- subjects (6.8%). Two cases of manifest exotropia in the HIV+ group were also described (2.7%). Esotropia was observed in 1 patient of the HIV+ group (1.3%) and 1 patient of the HIV- group.
Ocular Surface
Signs of allergy were observed in 18 patients from the HIV+ group (24.7%) and in 17 patients from the HIV- group (28.8%). Among this allergic subgroup, 4 children (5.5%) from the HIV+ group and 2 (3.4%) from the HIV- group were diagnosed with vernal keratoconjunctivitis (VKC). No significant differences between the two groups in terms of allergy (p=0.591) and VKC (p=0.567) frequencies were detected. Schirmer test (HIV+: 27.05±4.58, HIV-: 25.12±4.95) and BUT (HIV+: 18.41±2.69, HIV-: 17.39±2.63) resulted within the normal limits in all the cohorts. Corneal esthesiometry was preserved in all study subjects. The frequencies of Oxford scale scoring did not differ between the two groups. Data on OA symptoms reporting showed a significant difference between the two groups with HIV- reporting a larger number of symptoms (1.07±1.56 vs 0.51±1.41; p=0.03). Corneal esthesiometry was conserved in all the patients (sensation perceived with the nylon monofilament extended to 6 cm). Data on anterior segment involvement are summarized in Table 3.
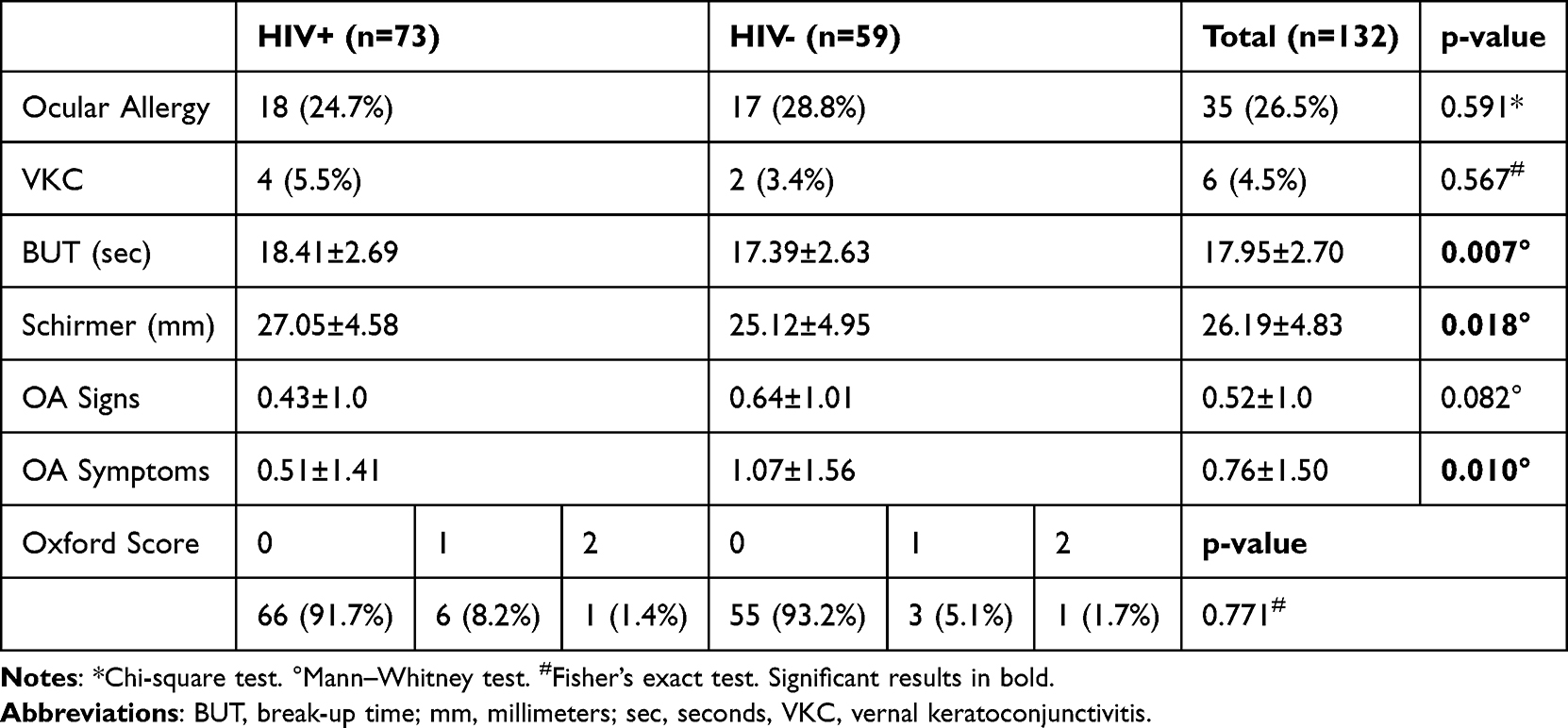 |
Table 3 Anterior Segment Characteristics for the Study Groups |
Uveal and Retinal Involvement
Three patients (4.1%) from the HIV+ group presented corneal signs of previous anterior uveitis. In particular, they showed pigmented endothelial precipitates in the inferior corneal quadrants, without signs of acute inflammation in the anterior chamber. All the patients living in the children’s home had complex and mostly unknown family and past clinical histories, so we could not be aware of previous inflammatory, infectious, or autoimmune conditions. The only test that is routinely performed on all children is TB-gold for tuberculosis. The three patients with signs of past anterior uveitis were negative for tuberculosis. We were able to collect data involving previous or actual tuberculosis only in the HIV+ subgroup, showing a total of 15 children (20.5%) who contracted the infection without apparent ocular involvement. The anterior chamber was within the normal limits in 100% of the patients in both groups.
Two patients from the HIV+ group (2.7%) had chorio-retinal scars outside the posterior pole, which were consistent with previous retinal toxoplasmosis.
Correlation Between Ocular and HIV Parameters
A further subanalysis was conducted on the HIV+ group to evaluate the impact of HAART therapy and the ocular parameters. No significant correlation was found between the clinical HIV parameters (time of therapy, viral load, and stage of AIDS at diagnosis) and the anterior segment parameters (Table 4).
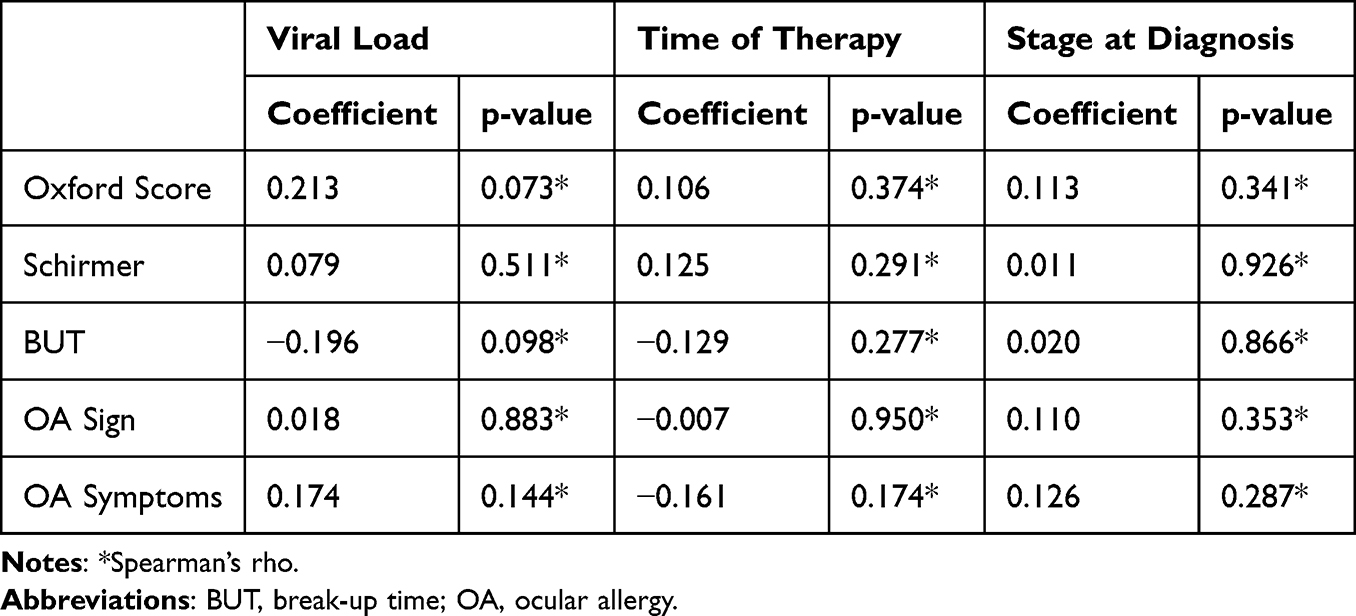 |
Table 4 Correlation Coefficients Between the Ocular Surface Parameters and the HIV-Related Parameters |
Lastly, the potential involvement of HIV drug regimens on ocular motility was investigated. Interestingly, patients who were administered abacavir in both the 120 and 600 mg doses showed a higher frequency of ocular motility disorders than the other patients. On the other hand, patients undergoing tenofovir therapy showed an inverse trend (Table 5).
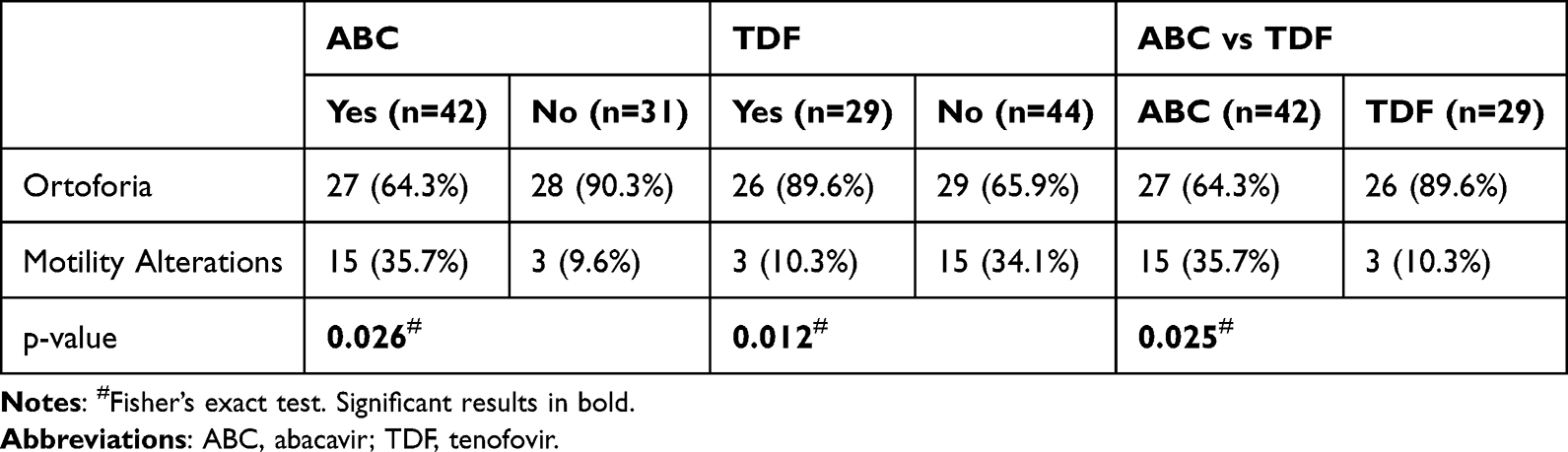 |
Table 5 Frequency of Ocular Motility Disorders in Patients Undergoing Therapy with Abacavir and Tenofovir |
Discussion
Findings from this cross-sectional study of 73 Kenyan paediatric patients with perinatally acquired HIV indicate that patients receiving optimized HIV treatment can maintain visual function and ocular surface homeostasis on par with those of healthy children. As expected, given that all patients were on HAART, strictly monitored, and had suppressed or very low viral loads, we did not identify typical AIDS-related findings.
Visual acuity was substantially preserved in both study groups (0.01 LogMar). Our cohort did not show any signs of current infectious diseases.
We did not report any cases of KCS and all the children in both groups showed normal BUT and Schirmer tests. Only a few patients had a positive Oxford staining without significant differences between the two groups. In our cohort, no correlation was found between the duration of HAART, recent viral load, and ocular surface parameters. Moreover, no sensory corneal alterations were found in the HIV+ group. In the literature, KCS is reported among frequent findings in HIV patients.
Due to chronological and geographic differences, numerous works have been published on the topic with extremely variable results. Kim et al reported 14.2% of patients with KCS without apparent link to the CD4+ count.12 Other studies have reported variable incidences of KCS ranging from 9% to 38.8%.4,13 These wide ranges can be attributed to the considerable variability in the diagnosis of KCS itself and the strong impact of age, living conditions, and hormone status on the ocular surface. HIV infection was often associated with autoimmune phenomena, including Sjogren’s-like syndrome. The pathogenesis of this syndrome in HIV involves aberrant lymphocytic infiltration of the salivary glands and likely extends to the lacrimal gland.4,14 While some authors propose Epstein-Barr Virus (EBV) as a potential risk factor for aqueous tear deficiency, a definitive link between HIV, EBV, and ocular surface remains unproven.15,16 It has been recognized that the anterior surface involvement during the HIV infection, as well as the Sjogren-like syndrome, has been almost completely eradicated by the HAART.17 Cicalini et al reported the case of an HIV-infected patient who developed Behcet's disease and KCS. Both conditions disappeared spontaneously after the introduction of the HAART therapy, together with the normalization of the CD4+ count. This case supports the hypothesis of HIV-related KCS as an expression of the autoimmune dysregulation linked to the virus.18 The absence of KCS can be ascribed to the young age of our cohort and the effective control of HIV replication.
Another dominant problem diffused in both infantile and adult African populations is represented by ocular allergy. Epidemiological data regarding the worldwide distribution of ocular allergy indicate that the highest prevalence is detected in Africa, involving about 18% of the population. Among African countries, Ghana showed the highest prevalence, reaching 39.9%.19 In Kenya, allergic conjunctivitis accounts for 27% of the outpatient visits.20 Our results showed that 24.7% of HIV+ and 28.8% of HIV- patients developed signs of allergy with no significant difference. The only difference between the two groups was found in the OA symptoms report. The HIV+ children may report fewer symptoms as they live in a protected environment with less exposure to irritants (eg firewood cooking or dust). No data are currently available in the literature on potential interactions between HIV infection and the development of allergic conjunctivitis.
A particular allergic manifestation classically described in the literature in HIV+ patients is VKC, but surprisingly we did not find an increased prevalence in our cohort. An Indian study on HIV-infected children reported a prevalence of VKC in around 87% of patients. The authors also found a connection between the incidence and the severity of this pathology and the CD4+ cell count, being associated with a compromised immune status.21 An interesting theory regarding the pathogenesis of VKC in HIV+ patients involves a possible immune shift from Th1 to Th2. CD4+ Th1 cells are the primary target of HIV- infection, and their depletion in the advanced stages of the disease leads to a shift in the immune response toward Th2 cells, which are primarily involved in regulating allergic reactions. Th2s are in fact responsible for the release of cytokines such as IL-5, IL-4, and IL-13, specifically involved in the allergic processes. The balance between Th1 and Th2 can be restored with the recovery of immunocompetence, resulting in the regression of pathological manifestations.22,23 In line with these studies, Kritzinger et al reported a high prevalence of VKC-like disease in a cohort of adult HIV+ patients. They confirmed the connection between these ocular manifestations and the severity of the immune deficiency according to CD4+ count. The authors also hypothesized immune dysregulation as a potential trigger.24 In our study, VKC was found in 5.5% of HIV+ patients while it only occurred in 3.4% of healthy subjects, although the difference was not significant. All the cases were characterized by the involvement of the limbus, with almost no involvement of the tarsal conjunctiva. These results are in line with the literature that shows a prevalence of 4–5% among the African pediatric population.25,26 The main reason why our patients showed a low prevalence of VKC compared with the literature results could be that all the children in our cohort were immunocompetent with a suppressed viral replication, and we can perhaps suppose the absence of immune dysregulation. Moreover, the prevalence of VKC, apart from HIV, is generally higher in Africa compared to European children, where it remains a rare disease (3.2 cases in 10.000).27
Ocular motility disorders in association with HIV are occasionally reported, and most of them are case reports related to cerebral complications of AIDS.28,29 Adhikari et al described an 11-year-old child with perinatally acquired HIV on long-term HAART, who presented with esotropia, limited ocular motility, and horizontal jerk nystagmus in lateral gaze.30 Few cases of opsoclonus-myoclonus-ataxia (OMA) syndrome have been described in HIV+ children. The pathology is considered the expression of the immune dysregulation and disequilibrium between CD4+ and CD8+ populations, which can be responsible for brainstem dysfunction. OMA syndrome can develop when the CD4+ cells are at a low critical level or during the immune restoration after the HAART introduction.31,32 Rutar et al reported that 18% of their HIV+ cohort developed strabismus while other studies report a prevalence of 6.3%.4,33 In our cohort, strabismus was found to be more common in the HIV+ group than the HIV- group (24.6% vs 8.4%). Interestingly, we report a higher frequency of ocular motility disorders in patients undergoing abacavir therapy (35.5% vs 9.6%). Currently, no clear data are available to explain these findings of a higher frequency of strabismus development in HIV patients. However, mitochondrial toxicity has been described in association with HIV infection and HAART therapy. Chronic progressive external ophthalmoplegia (CPEO) and ptosis can represent the expression of mitochondrial dysfunction involving the ocular district. This collateral effect has been reported particularly in association with nucleoside analogues therapy.34–36 Interestingly, abacavir was found in vitro to be considerably more toxic on muscle-skeletal cells than tenofovir.37 Also, in vivo, it is recognized that abacavir and other purine analogues can determine mitochondrial dysfunction.38,39 Based on our limited data, we can currently only speculate that the higher prevalence of strabismus in HIV+ patients may also be linked to a toxic effect on the extraocular muscles. As a future direction, it would be valuable to further investigate this novel finding, ideally by expanding the study to include a larger and more diverse population, including adults, to confirm the observed trend.
One of the main limitations of our study is the short duration of the observation period. Unfortunately, the three-month timeframe was relatively limited and restricted to the climatic conditions typical of the Kenyan summer season. This constraint was due to the limited time we were able to spend in the country to conduct the examinations. A second limitation, also representing a significant selection bias, is that all HIV+ children were recruited from the same children’s home, sharing the same living environment and being exposed to the same allergens within the enclosed setting of the facility. In contrast, all HIV-controls were recruited externally and came from a variety of home environments, potentially introducing confounding environmental differences. Another important limitation is the lack of photographic equipment, which prevented us from documenting the clinical findings. Moreover, we acknowledge the potential reporting bias from proxy symptom reporting for the OA questionnaire.
Conclusion
In the post-HAART era, long-term survivors of perinatally acquired HIV showed a low incidence of vision-threatening ocular diseases. Based on our data, the development of ocular surface diseases in patients with perinatally acquired HIV who have adequate viral load suppression does not differ from that in the healthy paediatric population. However, strabismus may be more frequently encountered in this cohort compared to the general population. The impact of the ocular side effects of HAART is considerably understudied and warrants more analysis.
Acknowledgments
We thank Vittoria Quondamatteo, nomad of love, for dedicating her life to helping those most in need.
Disclosure
The authors report no conflicts of interest in this work.
References
1. HIV and AIDS. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids.
2. Matza LS, Chung KC, Kim KJ, et al. Risks associated with antiretroviral treatment for human immunodeficiency virus (HIV): qualitative analysis of social media data and health state utility valuation. Qual Life Res Int J Qual Life Asp Treat Care Rehabil. 2017;26(7):1785–1798. doi:10.1007/s11136-017-1519-3
3. Kestelyn PG, Cunningham ET. HIV/AIDS and blindness. Bull World Health Organ. 2001;79(3):208–213.
4. Rutar T, Youm J, Porco T, et al. Ophthalmic manifestations of perinatally acquired HIV in a US cohort of long-term survivors. Br J Ophthalmol. 2015;99(5):650–653. doi:10.1136/bjophthalmol-2014-305557
5. Feroze KB, Wang J. Ocular manifestations of HIV. In: StatPearls. StatPearls Publishing; 2025. Available from: http://www.ncbi.nlm.nih.gov/books/NBK441926/.
6. Lenis TL, Botsford BW, Sarraf D, Papakostas TD. Didanosine-associated retinal toxicity in a patient with a mutation in the CRB1 gene. J Vitreoretin Dis. 2022;6(4):329–331. doi:10.1177/24741264211044599
7. Jones AM, Starte J, Dunn H, Ahmad K, Tan K. Surgical technique for pulled in two syndrome: three cases with chronic progressive external ophthalmoplegia. J Pediatr Ophthalmol Strabismus. 2017;54:e83–e87. doi:10.3928/01913913-20171017-01
8. Bron AJ, Evans VE, Smith JA. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea. 2003;22(7):640–650. doi:10.1097/00003226-200310000-00008
9. Ozcan AA, Ersoz TR, Dulger E. Management of severe allergic conjunctivitis with topical cyclosporin a 0.05% eyedrops. Cornea. 2007;26(9):1035–1038. doi:10.1097/ICO.0b013e31812dfab3
10. Weinberg JL, Kovarik CL. The WHO clinical staging system for HIV/AIDS. Virtual Mentor. 2010;12(3):202–206. doi:10.1001/virtualmentor.2010.12.3.cprl1-1003
11. Download JASP. JASP - free and user-friendly statistical software. Available from: https://jasp-stats.org/download/.
12. Kim YS, Sun HJ, Kim TH, Kang KD, Lee SJ. Ocular manifestations of acquired immunodeficiency syndrome. Korean J Ophthalmol. 2015;29(4):241–248. doi:10.3341/kjo.2015.29.4.241
13. Radhakrishnan N, Smit D, Venkatesh Prajna N, et al. Corneal involvement in HIV-infected individuals. Ocul Immunol Inflamm. 2021;29(6):1177–1182. doi:10.1080/09273948.2021.1887283
14. Ong Beng Seng M, Meyer D, Gichuhi S, et al. Ocular surface disorders in patients with human immunodeficiency virus (HIV) infection. Ocul Immunol Inflamm. 2020;28(7):1015–1021. doi:10.1080/09273948.2020.1757122
15. Pflugfelder SC, Tseng SCG, Pepose JS, Fletcher MA, Klimas N, Feuer W. Epstein-Barr Virus infection and Immunologic dysfunction in patients with aqueous tear deficiency. Ophthalmology. 1990;97(3):313–323. doi:10.1016/S0161-6420(90)32595-2
16. Lee-Wing MW, Hodge WG, Diaz-Mitoma F. Investigating a viral etiology for keratoconjunctivitis sicca among patients who are positive for human immunodeficiency virus. Cornea. 1999;18(6):671–674. doi:10.1097/00003226-199911000-00008
17. Panayiotakopoulos GD, Aroni K, Kyriaki D, et al. Paucity of Sjogren-like syndrome in a cohort of HIV-1-positive patients in the HAART era. Part II. Rheumatol Oxf Engl. 2003;42(10):1164–1167. doi:10.1093/rheumatology/keg316
18. Cicalini S, Gigli B, Palmieri F, Boumis E, Froio N, Petrosillo N. Remission of Behçet’s disease and keratoconjunctivitis sicca in an HIV-infected patient treated with HAART. Int J STD AIDS. 2004;15(2):139–140. doi:10.1258/095646204322764352
19. Miyazaki D, Fukagawa K, Okamoto S, et al. Epidemiological aspects of allergic conjunctivitis. Allergol Int off J Jpn Soc Allergol. 2020;69(4):487–495. doi:10.1016/j.alit.2020.06.004
20. Rashid ZA, Mashige KP, Moodley VR. Prevalence and demographic profile of keratoconus among high school students in Kenya. Int Ophthalmol. 2025;45(1):21. doi:10.1007/s10792-024-03370-9
21. Une VL, Jadhav SM. Occurrence of vernal keratoconjunctivitis in children infected with human immunodeficiency virus. Indian J Ophthalmol. 2022;70(2):497–499. doi:10.4103/ijo.IJO_1853_21
22. Agarwal S, Srinivasan B, Iyer G, Sudharshan S, Kalaivani K. Vernal keratoconjunctivitis in human immunodeficiency virus – the possible role of T-helper 1–T-helper 2 shift. Indian J Ophthalmol. 2018;66(7):1004–1006. doi:10.4103/ijo.IJO_76_18
23. Farias RJ, Gama ME, Mendes R, Lobão NT. Vernal Keratoconjunctivitis as the Only Clinical Manifestation of HIV Infection. Ocul Immunol Inflamm. 2022;30(6):1530–1532. doi:10.1080/09273948.2021.1891442
24. Kritzinger A, Zaborowski AG, Sibanda W, Visser L. The role of human immunodeficiency virus in the pathogenesis of vernal keratoconjunctivitis-like disease in adults: a demographic and epidemiological study. Indian J Ophthalmol. 2020;68(8):1551–1554. doi:10.4103/ijo.IJO_1608_19
25. Kyei S, Nkansah M, Asiedu K, Asiamah R, Zaabaar E, Afrifa‐Yamoah E. Prevalence and risk factors of Vernal Keratoconjunctivitis among a Ghanaian clinical cohort: a case-control study. Health Sci Rep. 2024;7(3):e1957. doi:10.1002/hsr2.1957
26. De Smedt SK, Nkurikiye J, Fonteyne YS, Tuft SJ, Gilbert CE, Kestelyn P. Vernal keratoconjunctivitis in school children in Rwanda: clinical presentation, impact on school attendance, and access to medical care. Ophthalmology. 2012;119(9):1766–1772. doi:10.1016/j.ophtha.2012.03.041
27. Nebbioso M, Alisi L, Giovannetti F, Armentano M, Lambiase A. Eye drop emulsion containing 0.1% cyclosporin (1 mg/mL) for the treatment of severe vernal keratoconjunctivitis: an evidence-based review and place in therapy. Clin Ophthalmol Auckl NZ. 2019;13:1147–1155. doi:10.2147/OPTH.S181811
28. Rival G, Okorji O, Kern R, Patel P, Fradeneck K, Cullen D. Bilateral cranial nerve VI Palsies in cryptococcal meningitis, HIV, and Syphilis: a case report. Clin Pract Cases Emerg Med. 2021;5(4):515–518. doi:10.5811/cpcem.2021.8.53347
29. Martins AI, Jorge AF, Galego OD, Nunes CP, Gonçalves RS, Lemos JM. Acute convergence and divergence paralysis in HIV-related rhombencephalitis. J Neuro-Ophthalmol off J North Am Neuro-Ophthalmol Soc. 2021;41(2):e197–e199. doi:10.1097/WNO.0000000000001036
30. Adhikari P, Chettry P. Cataract, strabismus and chorioretinal coloboma in paediatric HIV infection. J Optom. 2017;10(4):268–270. doi:10.1016/j.optom.2016.11.003
31. Pereira NMD, Shah I, Kulkarni S. Opsoclonus-myoclonus-ataxia syndrome in an HIV-infected child. Oxf Med Case Rep. 2016;2016(10):omw077. doi:10.1093/omcr/omw077
32. van Toorn R, Rabie H, Warwick JM. Opsoclonus-myoclonus in an HIV-infected child on antiretroviral therapy—possible immune reconstitution inflammatory syndrome. Eur J Paediatr Neurol. 2005;9(6):423–426. doi:10.1016/j.ejpn.2005.06.007
33. Cunningham ET, Kestelyn P, Pavesio CE. Ocular manifestations of HIV/AIDS in children. In: Hoyt C, Taylor D, editors. Pediatric ophthalmology and Strabismus.
34. Pfeffer G, Côté HCF, Montaner JS, Li CC, Jitratkosol M, Mezei MM. Ophthalmoplegia and ptosis: mitochondrial toxicity in patients receiving HIV therapy. Neurology. 2009;73(1):71–72. doi:10.1212/WNL.0b013e3181aae814
35. Ananworanich J, Nuesch R, Côté HCF, et al. Changes in metabolic toxicity after switching from stavudine/didanosine to tenofovir/lamivudine--a Staccato trial substudy. J Antimicrob Chemother. 2008;61(6):1340–1343. doi:10.1093/jac/dkn097
36. Silkiss RZ, Lee H, Gills Ray VL. Highly active antiretroviral therapy-associated ptosis in patients with human immunodeficiency virus. Arch Ophthalmol Chic Ill. 2009;127(3):345–346. doi:10.1001/archophthalmol.2009.11
37. Cihlar T, Birkus G, Greenwalt DE, Hitchcock MJM. Tenofovir exhibits low cytotoxicity in various human cell types: comparison with other nucleoside reverse transcriptase inhibitors. Antiviral Res. 2002;54(1):37–45. doi:10.1016/s0166-3542(01)00210-8
38. Wallace J, Gonzalez H, Rajan R, et al. Anti-HIV drugs cause mitochondrial dysfunction in monocyte-derived macrophages. Antimicrob Agents Chemother. 2022;66(4):e0194121. doi:10.1128/aac.01941-21
39. Blas-García A, Martí-Rodrigo A, Víctor VM, et al. The purine analogues Abacavir and didanosine increase acetaminophen-induced hepatotoxicity by enhancing mitochondrial dysfunction. J Antimicrob Chemother. 2016;71(4):916–926. doi:10.1093/jac/dkv424
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Immuno-Haematological Abnormalities of HIV-Infected Patients Before and After Initiation of Highly Active Antiretroviral Therapy in the Antiretroviral Therapy Clinics of Six Health Facilities at Dessie Town, Northeast Ethiopia
Tilahun M, Gedefie A, Ebrahim E, Seid A, Ali A, Shibabaw A, Belete MA, Fiseha M, Tesfaye M, Ebrahim H, Abera A
Journal of Blood Medicine 2022, 13:243-253
Published Date: 11 May 2022
Magnitude and Factors Associated with Cytopenia Among Children on Highly Active Antiretroviral Therapy at Hawassa University College of Medicine and Health Science, Sidama Region, Southern Ethiopia
Mohammed Nuru M, Bizuayehu Wube T, Fenta DA
HIV/AIDS - Research and Palliative Care 2023, 15:145-155
Published Date: 1 April 2023
Contemporary Anti-Retroviral Drugs (ARVDs) Disrupt Follicular Development in Female Wistar Rats
Ohihoin AG, Ohihoin EN, Ujomu I, Bakare A, Olanrewaju O, Okafor A, Ojetunde M, Ayoola JB, Aina O, Ajibaye O, Taylor-Robinson SD
Journal of Experimental Pharmacology 2023, 15:267-278
Published Date: 3 July 2023