")
Back to Journals » Journal of Blood Medicine » Volume 13
Immuno-Haematological Abnormalities of HIV-Infected Patients Before and After Initiation of Highly Active Antiretroviral Therapy in the Antiretroviral Therapy Clinics of Six Health Facilities at Dessie Town, Northeast Ethiopia
Authors Tilahun M , Gedefie A , Ebrahim E , Seid A, Ali A, Shibabaw A , Belete MA , Fiseha M , Tesfaye M, Ebrahim H , Abera A
Received 2 March 2022
Accepted for publication 5 May 2022
Published 11 May 2022 Volume 2022:13 Pages 243—253
DOI https://doi.org/10.2147/JBM.S364700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin H Bluth
Mihret Tilahun,1 Alemu Gedefie,1 Endris Ebrahim,1 Abdurahaman Seid,1 Abdurrahman Ali,1 Agumas Shibabaw,1 Melaku Ashagrie Belete,1 Mesfin Fiseha,1 Melkam Tesfaye,1 Hussen Ebrahim,1 Admasu Abera2
1Department of Medical Laboratory Sciences, College of Medicine and Health Science, Wollo University, Dessie, Ethiopia; 2Department of Medical Laboratory Science, Debre Birhan health Science college, North Showa, Ethiopia
Correspondence: Mihret Tilahun, Department of Medical Laboratory Science College of Medicine and Health Sciences, Wollo University, Po.Box: 1145, Dessie, Ethiopia, Tel +251-920988307, Fax +251 333115250, Email [email protected]
Background: In people living with the human immunodeficiency virus, haematological abnormalities have been linked to an increased risk of disease progression and mortality. Hematological parameters may have a positive or negative impact on antiretroviral therapy. The aim of this study was to assess the immuno-haematological abnormalities of HIV-infected patients before and after the initiation of highly active antiretroviral therapy in the antiretroviral therapy clinics of six health facilities in Dessie, Northeast Ethiopia.
Methods: A facility-based cross-sectional study was conducted from April to May 30, 2021, at the antiretroviral therapy clinics of six health facilities in Dessie Town. A total of 378 HIV-infected patients taking highly active antiretroviral treatment for at least 6 months by using a consecutive sampling technique were included. A well-organized questionnaire was used to collect socio-demographic and clinical information. Immune-haematological parameters were tested using a Mindray BS-300 hematology analyzer and a BD FACS count CD4 analyzer. Statistical analysis was performed using SPSS version 25 statistical software. Statistical significance was defined as a P-value of 0.05 with a 95% confidence interval.
Results: Leukopenia was found in 26.7% and 16.5%, neutropenia in 16.5% and 9.4%, lymphopenia in 20% and 3.1%, and thrombocytopenia in 25.9% and 7.1% of HIV patients before and after HAART initiation, respectively. There was a significant difference in total white blood cell, absolute neutrophil, red blood cell, hemoglobin value, mean cell volume, mean cell haemoglobin, mean cell haemoglobin concentration, red cell distribution width, platelet and CD4+ T cell counts in HIV patients before and after the initiation of HAART with P < 0.05.
Conclusion and Recommendation: Anemia, leukopenia, neutropenia, lymphopenia, and thrombocytopenia were the most common haematological abnormalities found in this study before and after HAART initiation. The prevalence of thrombocytopenia, immunosuppression, and viral load was reduced considerably after starting HAART.
Keywords: HIV, anemia, leukopenia, thrombocytopenia, HAART
Introduction
Acquired Immunodeficiency Syndrome (AIDS) is an immunological disease caused by the Human Immunodeficiency Virus (HIV), which infects cells and causes malfunctions of the immune system. It results in immune-hematological abnormalities, secondary and/or opportunistic infections, and tumors.1 In addition, extreme weakness and progressive harm of cellular and humoral immune responses are one of the characteristics of HIV.2 HIV was a global public health issue that claimed the lives of 770,000 people living with HIV (PLWHIV) at the end of 2018. From the HIV-infected personnel, more than two-thirds of the 37.9 million people were lived in Africa.3 In Ethiopia 2017 census indicated that a higher prevalence rate of HIV was found in Amhara, Oromia, and Addis Ababa, which accounted for 16.2% (613,000/37,900,000).4
Hematological abnormalities and/or cytopenia are the most common HIV-AIDS consequences and the leading predictors of HIV infection in PLWHIV, which has been linked to an elevated risk of illness progression and death.2,5 In PLWHIV, cytopenia can be caused by the adverse effect of HIV infection targeting lymphocytes, monocytes, and macrophages, resulting in irregularities in cytokine production, which in turn affects hematopoiesis.6 Thus, anemia, leucopenia, neutropenia, lymphopenia, and thrombocytopenia are the common complications associated with AIDS epidemics.7,8
Lower CD4 counts, immunological failure, viral load increment, advanced WHO clinical stages, HBV coinfection and side effects of highly antiretroviral therapy are all major risk factors for cytopenia in HIV patients.9 Therefore, management of hematological abnormalities in HIV patients and early initiation of ART is important to reduce the burden of immune-hematological problems. HIV not only affects the immune system and immunological dysfunction, but it also damages the hematopoietic system and causes cytopenia in infected people.10
Different studies indicated that 4–40% of Thrombocytopenia has been found to be associated with all stages of the HIV/AIDS disease11,12 and has been associated with an increased morbidity and mortality of HIV associated with risks of bleeding in various tissues.13–15 Platelet dysfunction includes immune-mediated platelet destruction and impaired hematopoiesis.13,15–17 Platelet destruction by antibodies and HIV direct infection of megakaryocytes has resulted in decreased platelet output from these progenitor cells.
Despite the fact that these hematological abnormalities have a significant impact on patient well-being, treatment and care, particularly in developing countries where access to health facilities is limited and people may only seek treatment after the disease has progressed to a serious stage and is accompanied by multiple immune-hematological abnormalities.21 For better treatment of HIV/AIDS patients, assessing the extent and severity of immune-hematological abnormalities is therefore very critical. The purpose of this study was therefore to determine the immune-hematological abnormalities in HIV-infected individuals presenting at selected health facilities of Dessie town, Northeastern Ethiopia, before and after commencing HAART.
Materials and Methods
Study Area
This study was conducted in the ART clinics of six health facilities at Dessie town, South Wollo zone of Amhara Regional state, Northeast Ethiopia. The town is situated in the mountainous ridge and has relatively cold weather. It has a total area of 15.08km2 (5.82 sq. Mi) and 401 km far from the capital city of the county, Addis Ababa, and 471 km far from Bahir Dar, the capital city of Amhara regional state. In Dessie town, there is one comprehensive specialized hospital, one general hospital, eight health centres, three private general hospitals and five higher private clinics, which provide ART services (offer HIV/AIDS prevention, treatment, care and support to the most vulnerable population). There are around 7350 HIV patients at Dessie Comprehensive Specialized Hospital, 250 at Selam General Hospital, 900 at Borumeda General Hospital, 650 at Dessie Health Centre and 500 at Ethio and Bati General Hospitals.
Study Design and Period
Health facility-based cross-sectional study was conducted from April 1 to May 30, 2021.
Population
Source Population
All HIV positive patients who visited ART clinics of the selected health facilities were the source population.
Study Population
HIV-positive patients who visited the ART clinics during the study period and those who fulfilled the eligibility criteria were included in the study.
Inclusion and Exclusion Criteria
HIV patients having complete haematological value at the baseline (at the time of ART initiation), those who were on ART for at least six months, and those who were volunteered to participate in the study were included. Those who were severely ill due to other medical conditions, those who were on medication, those who had known cancer or haematological abnormalities, those taking vitamins and iron supplementation at the time of sampling and pregnant women were excluded from the study.
Sample Size and Sampling Technique
Based on the following assumptions, the sample size was estimated using a single population proportional formula: In the previous study, the prevalence of leukopenia was 35.9%,11 marginal error was 5%, level of confidence was 95%, and the source population was 10,000 people, so the correction formula was used. Using the preceding assumptions, a minimum sample size of 304 was computed, with a 10% non-response rate, resulting in a final sample size of 334 but to increase the accuracy we included 378 participants in the study.
Data Collection and Laboratory Methods
With the aid of a structured questionnaire, relevant socio-demographic information was gathered from each participant. A skilled laboratory technician collected about 4 mL of venous blood from the forearm antecubital vein using vacuum collection in a tube containing a salt ethylene diamine tetra acetate (EDTA) anticoagulant were stored at 25–30°C for 30 minutes and analyzed within two hours of collection time. The samples stored for more than 48 hours were not processed. The Mindray 3000 plus hematology analyzer was used for complete blood count analysis,18 and the BD facscount CD4 analyzer (Becton Dickinson and Company, California, USA) was used for CD4+ T cell count.19 The result was collected within six hours and filled in the data collection format.
Operational Definitions
The WHO hematologic toxicity grading system was used to identify anemia, neutropenia, and thrombocytopenia. Anemia was defined as a hemoglobin (Hgb) concentration of less than 10.5 g/dL in all children, and severity was graded as follows:20 Thrombocytopenia is described as a platelet count of less than 150,000 per milliliter of blood. Platelet count >450,000/mm3 is considered thrombocytosis.21 White blood cell (WBC) count of less than 4000/mm3 is considered leukopenia. WBC count >12,000/mm3 is considered leukocytosis. Lymphopenia is defined as a lymphocyte count of less than 1500/mm3. Neutropenia is defined as an absolute neutrophil count (ANC) of less than 1500/mm3 with severity levels ranging from mild to severe.22
Data Entry and Analysis
The data was gathered utilizing a well-organized and pre-tested structured questionnaire, as well as laboratory results obtained from the hematology department and the patient’s registration card. SPSS version 25 was used to enter and evaluate the data. To display descriptive statistics, tables and graphs were calculated and used. Skewness and Kurtosis normality tests were used to determine the kind of distribution. Results were compared between categorical variables using parametric tests and ANOVA for continuous variables based on the distribution of the data. A paired t-test was employed to compare the means of each hematological parameter before and after 6 months of HAART imitation. A P-value of less than 0.05 is deemed statistically significant.
Quality Assurance and Quality Control
Starting from the data collection period to the sample processing, the lead investigator reviewed the accuracy and completeness of the gathered data every day during the post-analytical phase. All specimens were collected according to standard operating procedure, the specimen quality was confirmed, and all laboratory procedures were performed according to the manufacturer’s instructions. Quality control was carried out at the pre-analytical and analytical stages, which included the appropriate use of hematological investigations, as well as the collection, storage, and transportation of blood specimens. Furthermore, patient samples were evaluated alongside analytical stage quality control checks, which included quality control materials (Normal, Low, and High) to detect if analytic errors had occurred.
Ethical Approval
The study protocol was evaluated and approved by the Research Ethics Review Committee (RERC 0247/2021) of Wollo University, College of Health Sciences, and ethical clearance was obtained. Official letters of cooperation were submitted to the respective health facilities, and permission was obtained. Moreover, prior to commencing the study, a written informed consent was obtained from each study participant. Study participants aged less than 18 years were asked an assent, and written consent was taken from their parents or legal guardians. Throughout the study, confidentiality and any unique data security needs were maintained and ensured. Moreover, this study was conducted in accordance with the Declaration of Helsinki.
Result
General Characteristics of the Study Participants
In this study, a total of 378 HIV-positive people were included. From the total participants, females accounted for about half of the group 191 (50.5%). The age range of study participants was from 10 to 70 years, with a mean age (±SD) 40.09 (±12.24), while the median (IQR) age was 43 (35–54) years. The majority 174 (46%) of the study participants were between the 31–41 age group. Most of the study participants were urban dwellers with frequency of 289 (76.5%). About 318 (84.1%) of the participants were married. About 168 (44.4%) of the study participants were under WHO clinical stage III and half of 190 (50.5%) the study participants had <350 CD4 Cells/mm3 count (Table 1).
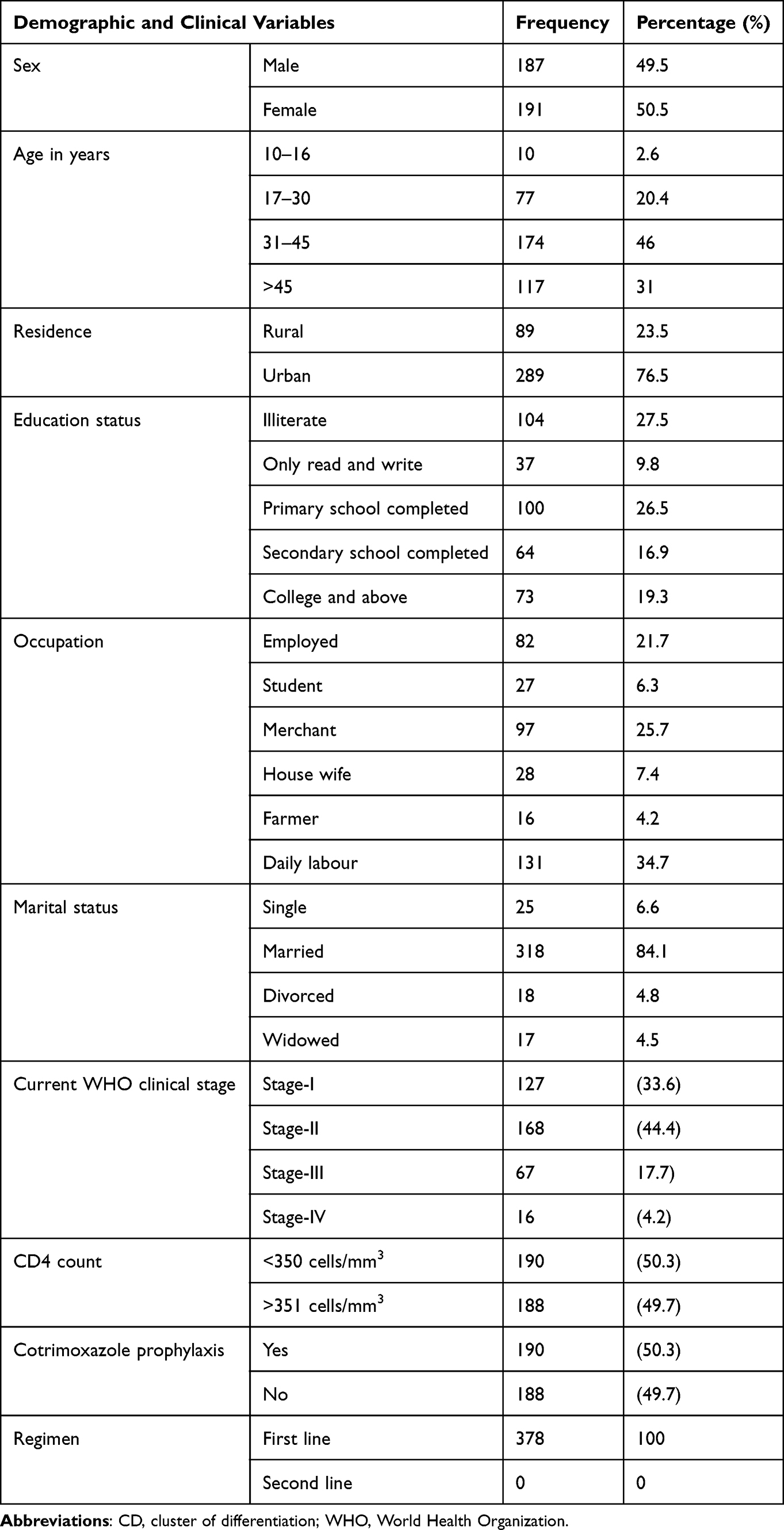 |
Table 1 Sociodemographic and Clinical Characteristics from April to May 30, 2021 |
Immuno-Haematological Values Before and After Initiation of HAART
The mean value of total white blood cell counts before starting of HAART (baseline) and after at 6 months of receiving HAART was 5.8 ± 2.7 × 103/μL, 4.7 ± 1.9 × 103/μL, respectively. Similarly, the amount of Neutrophil was 2.55 ± 1.56 × 103 and 2.45 ± 1.53 × 103/μL and lymphocyte were 2.12 ± 1.1 × 103/μL and 2.56 ± 1.3 × 103/μL, respectively. The mean value of WBC, ANC and TLC before initiation of HAART were 5.8 (4.09 −7.2) x103 /μL, 2.55 (1.5–3.4) x103 /μL and 2.12 (1.6–2.99) x103 /μL respectively and after at 6 months of HAART initiation 4.7 (3.5–6.69) x103 /μL, 2.45 (1.4 −2.9) x103 /μL and 2.56 (2.3–4.5) x103 /μL respectively (Table 2).
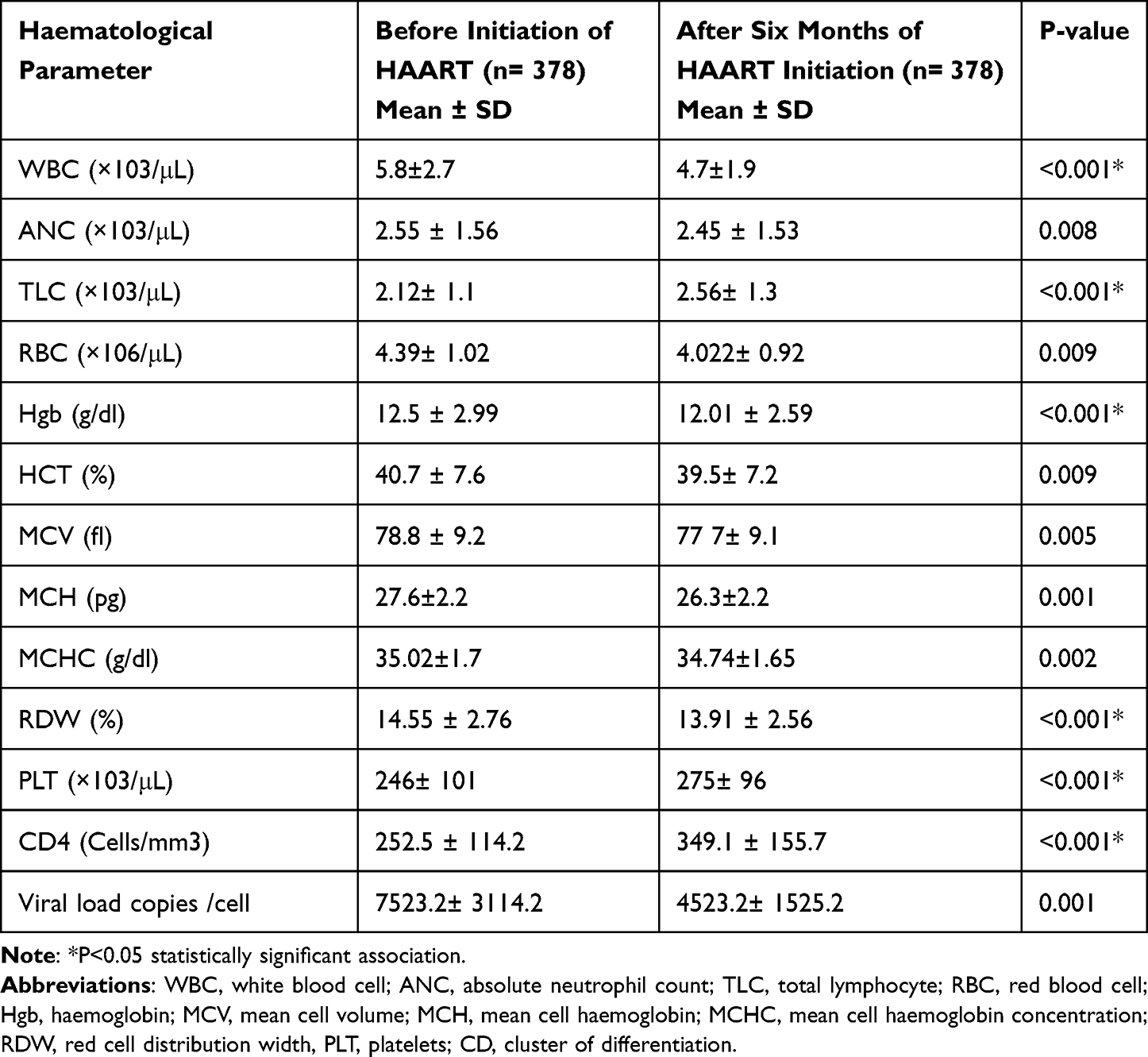 |
Table 2 Haematological and Immunological Values Before and After Initiation of HAART from April to May 30, 2021 |
The mean values of WBC and ANC after at least 6 months of HAART initiation were decreased with significant valve (p < 0.001 for WBC and p = 0.008 for ANC), respectively, whereas the mean values of TLC after at least 6 months of HAART initiation were increased with significant valve (p < 0.001). The mean RBC count was 4.39 ± 1.02 × 106/μL at the time before HAART initiation and 4.022± 0.92×106/μL after 6 months of taking HAART. The mean Hgb concentration was decreased and found to be 12.5 ± 2.99 g/dl before HAART initiation and 12.01 ± 2.59 g/dl after 6 months of HAART. Concerning the RBC indices, the mean values of MCV, MCH, MCHC and RDW before initiation HAART were 78.8 ± 9.2fl, 27.6 ± 2.2pg, 35.02 ± 1.7g/dl and 14.55 ± 2.76%, respectively, and after 6 months of HAART initiation the mean values of MCV, MCH, MCHC and RDW were 77 7± 9.16fl, 26.3 ± 2.2pg, 34.74 ± 1.65g/dl and 13.91 ± 2.56%, respectively.
The mean value of RBC (p = 0.009), Hgb (p < 0.001*), MCV (p = 0.005), MCH (p=0.001), and RDW (<0.001*) were significantly increased after 6 months of HAART initiation as compared to the patients who were before HAART initiation and their mean values were decreased, whereas the mean value of MCHC (p = 0.002) was increase as compared to patients who were before HAART initiation.
The mean platelet count of the study participants before HAART initiation was 246± 101×103/μL and 275± 96×103/μL after 6 months of HAART initiation, respectively. The amount of platelet count was significantly increased with a p value <0.001*.
The mean CD4 count of the study participants was 252.5 ± 114.2 (Cells/mm3) and 349.1 ± 155.7 (Cells/mm3) at the baseline and after 6 months of HAART initiation, respectively. The amount count was significantly increased with a p value <0.001*. The mean viral copies of the study participants were 7523.2± 3114.2 Viral load copies/cell and 4523.2± 1525.2 Viral load copies/cell at before HAART initiation and after 6 months of HAART initiation, respectively. The decrease of platelet count was significant with a p value <0.001* (Table 2).
Prevalence of Immuno-Haematological Abnormalities
In the current study, before and after treatment of HAART, hematological abnormalities were observed. The common haematological abnormalities were leukopenia, which accounted for 26.7% and 16.5%, neutropenia, which accounted for 16.5% and 9.4%, lymphopenia, which accounted for 20% and 3.1%, and thrombocytopenia, which accounted for 25.9% and 7.1% of the study participants before and after the initiation of HAART, respectively. Concerning immunological failure of study participants, the amount of CD4 count (Cells/mm3) before and after initiation of HAART were 73% and 55%, respectively, whereas, regarding the viral copies, 48.8% and 37.6% of the study subjects were greater than 1000 copies/cell before and after initiation of HAART, respectively (Figure 1).
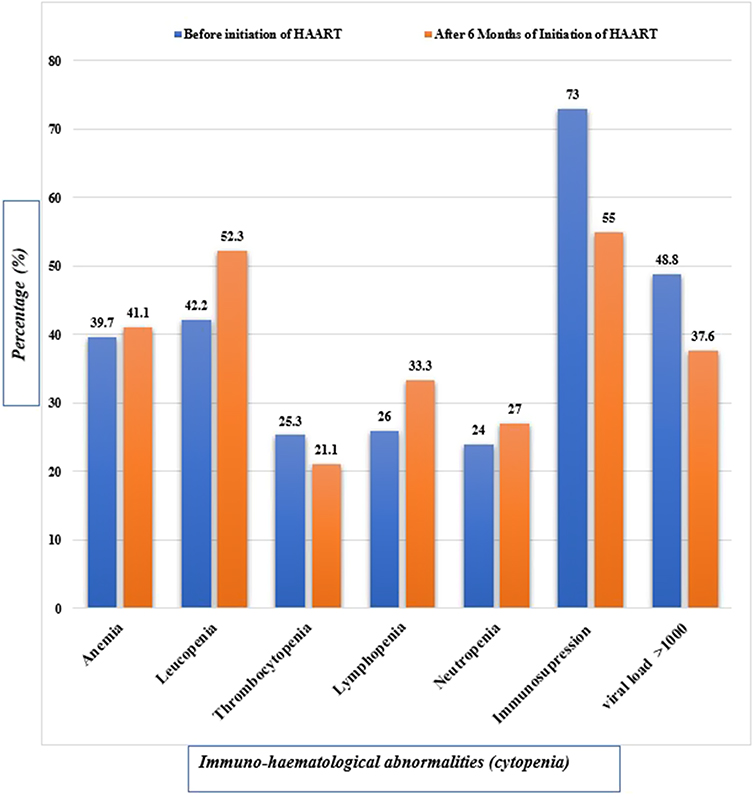 |
Figure 1 Immuno-haematological abnormalities among study participants. N.B Immunosuppression: Abnormal CD4 count range 50–500 cells per cubic millimeter. It means weakened immune system and may be infected with HIV and specifically below 350 cells per cubic millimeter. Viral copies: high HIV viral load generally indicates that HIV is present and replicating. |
Discussion
The current study looked at immune-haematological abnormalities in 378 HIV-positive patients who had been on HAART for more than six months at ART facilities managed by governmental and non-governmental healthcare systems in Dessie town. Anemia, leukopenia, neutropenia, lymphopenia, thrombocytopenia, and immunosuppression linked with HAART were the most common haematological abnormalities observed in the current study. Thrombocytopenia and immunosuppression became less common once HAART was initiated. Another study found an increase in the prevalence of anemia, leukopenia, neutropenia, and lymphopenia.23 This could be owing to the reduced blood cell counts associated with advanced HIV/AIDS. Sex, race/ethnicity, geographic location, and comorbidities like tuberculosis, hepatitis B infection, fever, and oral candidiasis have all been connected to cytopenia and an increase in the incidence of bone marrow transplantation.
Among the investigated haematological abnormalities, the mean ± SD white blood cell count was 5.8 ± 2.7 × 103/μL before HAART initiation and it was decreased to 4.7 ± 1.9 × 103/μL after 6 months of HAART initiation. This finding was supported by a similar study that reported decreased WBC count for HIV patients on HAART, conducted in Gondar, Ethiopia.24,25 This difference might be due to a short duration of ART intake as in the initial stage of ART initiations, WBC count will be low which gradually corrects itself over a period of time.24 In the current study, the prevalence of leukopenia was 42.2% at baseline and 52.3% after six months of HAART initiation, respectively (Figure 1). The current finding is comparable with a study from Gondar, Ethiopia, which found a prevalence of 34.2% before HAART initiation and 35.9% for leukopenia after HAART.11 However, the current study discovered a difference in a Nigerian study that discovered the prevalence of leukopenia before and after HAART was 6.1% and 1.7%, respectively.26 This discrepancy could be explained by a difference in the defining value for leukopenia. Additionally, cancer and other diseases that wreak havoc on the bone marrow are autoimmune diseases that cause the destruction of white blood cells or bone marrow cells. Antibiotics and other medications that destroy white blood cells.
In the present study, absolute neutrophil count also presented a decrease from 2.55 ± 1.56 × 103/μL to 2.45 ± 1.53 × 103/μL before HAART initiation and after 6 months of HAART initiation, respectively. The prevalence of Neutropenia was found to be present in 24% and 27% of patients before and after the start of HAART, respectively. It differs from a study conducted in Gondar, Ethiopia, which discovered 14.8% and 28% neutropenia before and after therapy, respectively.11 This variance could be attributed to variations in the study population, sample size, research design, and clinical situations. Furthermore, certain pharmaceuticals, such as antibiotics and blood pressure medications, may suppress or limit the synthesis of granulocyte macrophage and granulocyte colony-stimulating factor, both of which are critical in granulocyte activation.
In this study, haematological parameters (the mean value) of RBC count were 4.39± 1.02 (×106/μL) and 4.022± 0.92 (×106/μL) before HAART initiation and after 6 months of HAAART initiation (Table 2). These findings were comparable with a study conducted at Jimma, Ethiopia reported that a mean value of RBC count was 4.95 ± 0.57 ×106/μL and 4.14 ± 0.07×106/μL27 and in Addis Ababa with a mean value of RBC count (4.41 ± 0.71 × 106/μL and 4.28 ± 0.59 × 106/μL before HAART initiation and after at least six months of receiving antiretroviral therapy, respectively.28 However, a higher mean value of RBC count before HAART than after the treatment was also reported by another study.29 This could be due to the unfavourable effect of Zidovudine, which is commonly indicated for RBC depletion in HAART patients, which could possibly account for the current data. The unfavourable HAART treatment of Zidovudine might suppress bone marrow production of RBC, which could possibly account for the current data.30
The present study also showed that the amount of haemoglobin value was decreased after HAART initiation. The mean values of haemoglobin were 12.5 ± 2.99 g/dl and 12.01 ± 2.59 g/dl before HAART initiation and after six months of HAART initiation, respectively (Table 2). This finding is in agreement with other studies.25,27,31 This could be due to HAART treatment, which can cause lead poisoning, immunological dysregulation, red blood cell destruction (haemolysis), or insufficient red blood cell formation, all of which are influenced by spleen or circulatory system issues.
Anemia was found to be prevalent in 39.7% and increased to 41.1% before HAART initiation and after HAAART 6 months HAART initiation. This finding is consistent with a research conducted in Europe and North America,32 Addis Ababa, Ethiopia (34.6%),33 Jimma, Ethiopia (43.1%),23 Brazil (37.5%),34 and 46% Ghana.35 The treatment of Zidovudine (ZDV) might be responsible for the increase in anemia following HAART commencement.36 Immune dysregulation can increase the risk of anemia with HIV infection by the death of red blood cells or insufficient red blood cell production.37 Furthermore, previous studies have shown that smoking increases hemoglobin levels and reduces the detection of anemia by lowering the oxygen carrying capacity of red blood cells.38 In contrast to our study, study done showed that the prevalence of anemia in Gondar, Ethiopia, 29.7% and 11.7%,11 in Addis Ababa, 41.9% and 11.4%,28 Nigeria reported 57.5% and 24.3%,26 and Ghana 63% and 46%35 were reduced before and after the start of HAART, respectively. This gap could be attributed to a number of factors, including differences in the study population, sample size, study design, socio-demographic characteristics of study participants, and anemia definition discrepancies.
In the current study, the mean value of red cell indices (MCV, MCH, and MCHC and RDW) were decreased significantly following starting of HAART (p < 0.001). This was concurrent with the results of earlier investigations.39 However, the current finding was different from studies done in which the amount of red cell indices (MCV, MCH, and MCHC) was increased.11,28,40 This might be due to failure of the bone marrow. The primary cause of anemia in patients with chronic renal disease is erythropoietin deficiency.
The amount of CD4+ T cells counts 252.5 ± 114.2 cells/μL were increased to 349.1 ± 155.7 cells/μL after 6-month initiation of HAART. This finding was in agreement with the study conducted at Addis Ababa, Ethiopia31,41,42 and in Maryland43 stated that the mean value of CD4+ was increased after HAART initiation. This may be due to the fact that HIV infection is thought to be caused by the destruction of mature CD4+ T lymphocytes in the peripheral lymphoid system, and HIV may also inhibit the maturation of lymphoid precursors such as lymphoid-restricted T cell progenitors in the thymus and/or clonally distributed memory T cells in peripheral lymphoid organs. Increased CD4+ T cell production is linked to HAART-induced viral replication suppression.44
The current study showed that the prevalence of immunosuppression was 73% and 55% at the baseline and after HAART initiation, respectively (Figure 1). This finding is supported by studies conducted in India where 89.2% of the cases had a CD4 count of fewer than 200 cells/l at the time of diagnosis45 and Maharashtra where 89.2% of the cases had immunosuppression at baseline.46 This could be due to the fact that the majority of the patients were severely immunocompromised at the outset of the research. Furthermore, HIV’s cytotoxic effect on T helper cells might cause immunosuppression, resulting in a low CD4 level. Immunosuppression is reduced after starting treatment because HAART enhances immune function by lowering HIV viral replication and increasing CD4+ T-cell numbers.47
This study showed that platelet counts were significantly increased from 246 ± 101 (×103/μL) to 275± 96 (×103/μL) after 6 months of the treatment (Table 2). The prevalence of thrombocytopenia was 25.3% at baseline and 21.1% after six months of HAART initiation. This finding was comparable with studies conducted in Gondar,11 Addis Ababa 25% to 5.7%,28 Gondar, 4.1% and 9.1%,11 Goba Ethiopia 11.4% to 4.5%,48 Uganda 17.8% to 13.0%49 which collectively showed that the prevalence of thrombocytopenia decreased after initiation of HAART. Another study in systematic review and meta-analysis showed that the prevalence of thrombocytopenia was 21% and 11.64% before and after initiation of highly active antiretroviral therapy (HAART), respectively.50 This variation could be due to hematopoiesis-related disorders, opportunistic infections, and immune-suppression factors related to HIV which subsequently lead to low platelet count.51 Furthermore, there are differences in the definition of thrombocytopenia, study design, and study population size.
Conclusion and Recommendations
In this study, statistically significant variations in haematological parameters were observed from the baseline and after HAART initiation. The magnitude of hematological abnormalities, before and after initiation of HAART, was leukopenia (26.7% and 16.5%), neutropenia, (16.5% and 9.4%), lymphopenia (20% and 3.1%), and thrombocytopenia (25.9% and 7.1%), respectively. Before and after HAART, there were statistically significant differences in total WBC count, neutrophils, lymphocytes, Hgb, MCV, MCH, MCHC, and platelets. The study subjects exhibited high and low CD4 counts and viral copies before and after starting HAART, respectively, in terms of CD4 count, immunological failure, and viral copy. According to existing data, a significant proportion of HIV patients remained anemic after six months of antiretroviral therapy (ART), emphasizing the need for routine anemia screening and treatment to prevent the harmful effects of anemia.
Abbreviations
AIDS, acquired immune deficiency syndrome; ART, antiretroviral therapy; ANC, absolute neutrophil count; AZT/ZDV, Azidothymidine/Zidovudine; CBC, Complete blood count; CD4, cluster of differentiation 4; EDTA, Ethylene diamine tetra acetate; HAART, highly active antiretroviral therapy; HGB, Haemoglobin concentration; IQC, Internal quality control; LYM, Lymphocyte; MCH, Mean Corpuscular Haemoglobin; MCHC, Mean Corpuscular Haemoglobin Concentration; MCV, Mean Corpuscular Volume; NEUT, Neutrophils; PCV, Packed Cell Volume; PLT, Platelets; RBC, Red Blood Cells; SPSS, Statistical Package for Social Sciences; WBC, White Blood Cell; WHO, World Health Organization.
Data Sharing Statement
Data supplementary to the conclusions of this article are within the manuscript.
Acknowledgment
The authors would like to acknowledge the Department of Medical Microbiology, School of Biomedical and Laboratory Sciences, College of Medicine and Health Sciences, University of Gondar Hospital, for giving me the opportunity to conduct this thesis work. All the study participants, APHI staffs especially Microbiology Department and the staffs of DRH are for their participation and support during the sample collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors state that they have no conflicts of interest in this research work.
References
1. Levy JA. HIV pathogenesis: 25 years of progress and persistent challenges. Aids. 2009;23(2):147–160. doi:10.1097/QAD.0b013e3283217f9f
2. Rudnicka D, Schwartz O. Intrusive HIV-1-infected cells. Nat Immunol. 2009;10(9):933–934. doi:10.1038/ni0909-933
3. Wamala K, Nuwamanya R, Muwanga M. Prevalence of HIV and associated risk factors among infants born to HIV positive mothers attending Entebbe regional referral hospital. SJHR Africa. 2021;2(3):11.
4. Worku ED, Asemahagn MA, Endalifer ML. Epidemiology of HIV infection in the Amhara region of Ethiopia, 2015 to 2018 surveillance data analysis. HIV/AIDS. 2020;12:307.
5. Anastos K, Shi Q, French AL, et al. Total lymphocyte count, hemoglobin, and delayed-type hypersensitivity as predictors of death and AIDS illness in HIV-1–infected women receiving highly active antiretroviral therapy. JAIDS. 2004;35(4):383–392. doi:10.1097/00126334-200404010-00008
6. Gunda DW, Godfrey KG, Kilonzo SB, Mpondo BC. Cytopenias among ART-naive patients with advanced HIV disease on enrolment to care and treatment services at a tertiary hospital in Tanzania: a crosssectional study. Malawi Med J. 2017;29(1):43–52. doi:10.4314/mmj.v29i1.9
7. Scaradavou A. HIV-related thrombocytopenia. Blood Rev. 2002;16(1):73–76. doi:10.1054/blre.2001.0188
8. Opie J. Haematological complications of HIV infection: forum-review. S Afr Med J. 2012;102(6):465–468. doi:10.7196/SAMJ.5595
9. Shiferaw MB, Endalamaw D, Hussien M, et al. Viral suppression rate among children tested for HIV viral load at the Amhara Public Health Institute, Bahir Dar, Ethiopia. BMC Infect Dis. 2019;19(1):1–6. doi:10.1186/s12879-019-4058-4
10. Durandt C, Potgieter J, Khoosal R, et al. HIV and haematopoiesis. S Afr Med J. 2019;109(8 Supplement 1):S41–S6. doi:10.7196/SAMJ.2019.v109i8b.13829
11. Enawgaw B, Alem M, Addis Z, Melku M. Determination of hematological and immunological parameters among HIV positive patients taking highly active antiretroviral treatment and treatment naïve in the antiretroviral therapy clinic of Gondar University Hospital, Gondar, Northwest Ethiopia: a comparative cross-sectional study. BMC Hematol. 2014;14(1):1–7.
12. Firnhaber C, Smeaton L, Saukila N, et al. Comparisons of anemia, thrombocytopenia, and neutropenia at initiation of HIV antiretroviral therapy in Africa, Asia, and the Americas. Int J Infect Dis. 2010;14(12):e1088–e1092. doi:10.1016/j.ijid.2010.08.002
13. Li Z, Nardi MA, Karpatkin S. Role of molecular mimicry to HIV-1 peptides in HIV-1–related immunologic thrombocytopenia. Blood. 2005;106(2):572–576. doi:10.1182/blood-2005-01-0243
14. Marks KM, Clarke RM, Bussel JB, Talal AH, Glesby MJ. Brief report: risk factors for thrombocytopenia in HIV-infected persons in the era of potent antiretroviral therapy. J Acquir Immune Defic Syndr. 2009;52(5):595. doi:10.1097/QAI.0b013e3181b79aff
15. Alexaki A, Wigdahl BHIV-1. infection of bone marrow hematopoietic progenitor cells and their role in trafficking and viral dissemination. PLoS Pathog. 2008;4(12):e1000215. doi:10.1371/journal.ppat.1000215
16. Wondimeneh Y, Muluye D, Ferede G. Prevalence and associated factors of thrombocytopenia among HAART naive HIV positive patients at Gondar University Hospital, northwest Ethiopia. BMC Res Notes. 2014;7(1):1–4. doi:10.1186/1756-0500-7-5
17. Akinbami A, Oshinaike O, Adeyemo T, et al. Hematologic abnormalities in treatment-naive HIV patients. Infect Dis. 2010;3(IDRT):S6033.
18. Oudatzis G, Tsagarakis NJ, Paterakis G, et al. Evaluation of automated capillary complete blood counts for routine clinical decision making in a large cohort of hematological patients, using Mindray BC‐3000 Plus Auto and Sysmex XE‐5000 hematology analyzers. Int J Lab Hematol. 2020;42(5):565–572. doi:10.1111/ijlh.13237
19. Tagoe DNA, Boachie J. Assessment of the impact of malaria on CD4+ T Cells and haemoglobin levels of HIV-malaria co-infected patients. J Infect Dev Ctries. 2012;6(09):660–663. doi:10.3855/jidc.2124
20. World Health Organization. WHO Guideline on Use of Ferritin Concentrations to Assess Iron Status in Individuals and Populations; 2020.
21. CHeCK Q. Eosinophilia, Leukocytosis, thrombocytopenia, thrombocytosis, Anemia, Hepatic Function Abnormalities. In: The Clozapine Handbook: Stahl’s Handbooks. Cambridge University Press; 2019.
22. Fan L, Li C, Zhao H. Prevalence and risk factors of cytopenia in HIV-infected patients before and after the initiation of HAART. Biomed Res Int. 2020;2020. doi:10.1155/2020/3132589
23. Fekene TE, Juhar LH, Mengesha CH, Worku DK. Prevalence of cytopenias in both HAART and HAART naïve HIV infected adult patients in Ethiopia: a cross sectional study. BMC Hematol. 2018;18(1):1–11. doi:10.1186/s12878-018-0102-7
24. Wanjari A, Acharya S, Singh AP, Rathi C. A study of hematological profile in HIV/AIDS. AIDS. 2013;8:9.
25. Tesfaye Z, Enawgaw B. Prevalence of anemia before and after initiation of highly active antiretroviral therapy among HIV positive patients in Northwest Ethiopia: a retrospective study. BMC Res Notes. 2014;7(1):1–5. doi:10.1186/1756-0500-7-745
26. Denue BA, Kida IM, Hammagabdo A, Dayar A, Sahabi MA. Prevalence of anemia and immunological markers in HIV-infected patients on highly active antiretroviral therapy in Northeastern Nigeria. Infect Dis. 2013;6(IDRT):S10477.
27. Gedefaw L, Yemane T, Sahlemariam Z, Yilma D. Anemia and risk factors in HAART naive and HAART experienced HIV positive persons in south west Ethiopia: a comparative study. PLoS One. 2013;8(8):e72202. doi:10.1371/journal.pone.0072202
28. Woldeamanuel GG, Wondimu DH. Prevalence of thrombocytopenia before and after initiation of HAART among HIV infected patients at black lion specialized hospital, Addis Ababa, Ethiopia: a cross sectional study. BMC Hematol. 2018;18(1):1–6. doi:10.1186/s12878-018-0097-0
29. Melku M, Addis Z, Alem M, Enawgaw B. Prevalence and predictors of maternal anemia during pregnancy in Gondar, Northwest Ethiopia: an institutional based cross-sectional study. Anemia. 2014;2014. doi:10.1155/2014/108593
30. Jam S, Ramezani A, Sabzevari D, et al. A cross-sectional study of anemia in human immunodeficiency virus-infected patients in Iran; 2009.
31. Amegor O, Bigila D, Oyesola O, Oyesola T, Buseni S. Hematological changes in HIV patients placed on anti retroviral therapy in Markurdi, Benue State of Nigeria. Asian J Epidemiol. 2009;2(4):97–103. doi:10.3923/aje.2009.97.103
32. Harris RJ, Sterne JA, Abgrall S, et al. Prognostic importance of anaemia in HIV-1 infected patients starting antiretroviral therapy: collaborative analysis of prospective cohort studies in industrialized countries. Antivir Ther. 2008;13(8):959. doi:10.1177/135965350801300802
33. Gebremedhin KB, Haye TB. Factors associated with anemia among people living with HIV/AIDS taking ART in Ethiopia. Adv Hematol. 2019;2019. doi:10.1155/2019/9614205
34. De Santis GC, Brunetta DM, Vilar FC, et al. Hematological abnormalities in HIV-infected patients. Int J Infect Dis. 2011;15(12):e808–e811. doi:10.1016/j.ijid.2011.08.001
35. Quaye W, Addai-Mensah A. Prevalence of anaemia and immunological markers among Ghanaian HAART-naïve HIV-patients and those on HAART. Afr Health Sci. 2011;11:1.
36. Meidani M, Rezaei F, Maracy MR, Avijgan M, Tayeri K. Prevalence, severity, and related factors of anemia in HIV/AIDS patients. J Res Med Sci. 2012;17(2):138.
37. Kerkhoff AD, Wood R, Cobelens FG, Gupta-Wright A, Bekker L-G, Lawn SD. Resolution of anaemia in a cohort of HIV-infected patients with a high prevalence and incidence of tuberculosis receiving antiretroviral therapy in South Africa. BMC Infect Dis. 2014;14(1):1–12. doi:10.1186/s12879-014-0702-1
38. Nordenberg D, Yip R, Binkin NJ. The effect of cigarette smoking on hemoglobin levels and anemia screening. JAMA. 1990;264(12):1556–1559. doi:10.1001/jama.1990.03450120068031
39. Gebreweld A, Fiseha T, Girma N, Haileslasie H, Gebretsadik D. Prevalence of cytopenia and its associated factors among HIV infected adults on highly active antiretroviral therapy at Mehal Meda Hospital, North Shewa Zone, Ethiopia. PLoS One. 2020;15(9):e0239215. doi:10.1371/journal.pone.0239215
40. Rezaei E, Ebrahim-Saraie HS, Heidari H, et al. Impact of vitamin supplements on HAART related hematological abnormalities in HIV-infected patients. Med J Islam Repub Iran. 2016;30:350.
41. Huruy K, Kassu A, Mulu A, Wondie Y. Immune restoration disease and changes in CD4+ T-cell count in HIV-infected patients during highly active antiretroviral therapy at Zewditu Memorial Hospital, Addis Ababa, Ethiopia. AIDS Res Ther. 2010;7(1):1–7. doi:10.1186/1742-6405-7-46
42. Derbe M, Monga D, Daka D. Immunological response among HIV/AIDS patients before and after ART therapy at Zewuditu Hospital Addis Ababa, Ethiopia. Am J Res Commun. 2013;1(1):103–115.
43. Moore RD, Keruly JC. CD4+ cell count 6 years after commencement of highly active antiretroviral therapy in persons with sustained virologic suppression. Clin Infect Dis. 2007;44(3):441–446. doi:10.1086/510746
44. Vidya Vijayan K, Karthigeyan KP, Tripathi SP, Hanna LE. Pathophysiology of CD4+ T-cell depletion in HIV-1 and HIV-2 infections. Front Immunol. 2017;8:580. doi:10.3389/fimmu.2017.00580
45. Gautam H, Bhalla P, Saini S, Dewan R. Correlation between baseline CD4+ T-Lymphocyte count and plasma viral load in AIDS patients and their early clinical and immunological response to HAART: a preliminary study. Indian J Med Microbiol. 2008;26(3):256–258. doi:10.4103/0255-0857.42039
46. Patil SS, Patil VS. Correlation of blood profile and CD4 count in AIDS patients before and after HAART, Study in Western Maharashtra. Biomed Pharmacol J. 2020;13(1):101–105. doi:10.13005/bpj/1866
47. Sokoya T, Steel HC, Nieuwoudt M, Rossouw TM. HIV as a cause of immune activation and immunosenescence. Mediators Inflamm. 2017;2017. doi:10.1155/2017/6825493
48. Duguma N, Kiya GT, Maleko WA, Bimerew LG. Hematological parameters abnormalities and associated factors in HIV-positive adults before and after highly active antiretroviral treatment in Goba Referral Hospital, southeast Ethiopia: a cross-sectional study. SAGE Open Med. 2021;9:20503121211020175. doi:10.1177/20503121211020175
49. Taremwa IM, Muyindike WR, Muwanguzi E, Boum Y. Prevalence of HIV-related thrombocytopenia among clients at Mbarara Regional Referral Hospital, Mbarara, southwestern Uganda. J Blood Med. 2015;6:109. doi:10.2147/JBM.S80857
50. Getawa S, Aynalem M, Bayleyegn B, Adane T. The global prevalence of Thrombocytopenia among HIV infected adults: a systematic Review and Meta-analysis. Int J Infect Dis. 2021;105:495–504. doi:10.1016/j.ijid.2021.02.118
51. Nascimento FG, Tanaka PY. Thrombocytopenia in HIV-infected patients. Indian J Hematol Blood Transfus. 2012;28(2):109–111. doi:10.1007/s12288-011-0124-9
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.